
Abstract
Fine-needle aspiration (FNA) is the most useful minimally invasive approach in the evaluation of lymphadenopathy. The diagnostic accuracy of the procedure is increased with the use of ultrasound (US) to guide the needle and avoid lymph node cystic areas, select the most abnormal lymph node, evaluate non-palpable lymph nodes, and obtain samples for ancillary tests. This chapter covers briefly lymph node anatomy and histology and clinical considerations as preamble to discuss in detail the various head and neck levels, paramount to facilitate the localization of a particular lymph node. Numerous US images complement the text. US features of benign and malignant lymphadenopathies are also covered in detail and complemented with numerous US images. The FNA diagnosis of lymph nodes is covered using a cell pattern approach, and select reactive, infectious/inflammatory, and neoplastic (lymphomas and metastasis) entities are discussed. Immunophenotype is also included in each lymphoma entity.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Clinical Considerations
Lymph nodes are “absent” by palpation in newborns. They are more numerous in children than in adults and are soft and oval. Anterior cervical, axillary, and inguinal lymph nodes may be found in healthy children and measure <1 cm. The only palpable lymph nodes in adults may be found in the inguinal region and measure <1.5 cm.
Localized or regional lymphadenopathy is defined as lymph node enlargement in contiguous anatomic regions. Generalized lymphadenopathy is defined as the involvement of more than two noncontiguous lymph node regions.
Lymphadenopathy may be the result of a local or systemic etiologic process, i.e., metastases, lymphoma, infection, or inflammation. The clinical differential diagnosis is based on the physical examination, location of the lymph node, and particularly the age of the patient. Although these factors are important, they should not overinfluence the interpretation. The history of immunosuppression, particularly in HIV-positive individuals, contributes to the frequency of certain lymph node-based reactive, malignant, or infectious processes. A nonneoplastic pathologic process is the most common cause of regional or generalized lymphadenopathy in children and adults.
In the pediatric age group, the most common causes of regional lymphadenopathy are viral, bacterial, and mycobacterial processes, depending on the geographic environment; the most frequent malignancies presenting as a cervical lymphadenopathy are small blue cell tumors including, but not limited to, lymphomas and leukemias, followed by solid tumors such as neuroblastoma, rhabdomyosarcoma, and Wilms’ tumor. In the adolescent group, Hodgkin’s and non-Hodgkin’s lymphomas, nasopharyngeal carcinoma, and metastatic germ cell tumors are the predominant malignancies present in a neck lymph node. Metastatic carcinoma, predominantly of the squamous type, from lung and head and neck organs becomes the most common diagnostic consideration in or above the fourth decade of life.
In general, a round, firm, well-defined lymph node present for >8 weeks or a lymph node that is fixed to surrounding tissues including the skin, deep anatomic planes, or other lymph nodes should be considered for FNA regardless of clinical findings. Likewise, a regional or generalized lymphadenopathy associated with constitutional symptoms should be considered for FNA.
Lymph Node Anatomy and Histology
The normal lymph node has a bean shape, measures <1 cm, has a cortex and medulla, and is surrounded by a capsule. The afferent lymphatic vessels penetrate the convex surface of the lymph node, and the efferent vessel exits at the level of the hilum, which is indented, contains the vein and artery, and is contiguous with the medulla.
The cortex contains the lymphoid follicles, which have germinal centers. The medulla contains the sinuses, stroma, and vessels. The sinuses converge in the hilum. The afferent lymphatic vessels drain into the subcapsular sinus, a remarkably important structure because it is the first site of entry for any benign or metastatic process. Reactive lymphoid hyperplasia produces diffuse cortical widening; if the process continues, there is formation of germinal centers in the hilar area, causing widening of the hilum. Metastatic processes produce irregular cortical widening.
US features. The US findings reflect the histology. The cortex is densely cellular with little stroma and appears hypoechoic and essentially avascular on Doppler examination. In contrast, the medulla has more stroma, converging sinuses, and vessels and appears hyperechoic and vascular. Also, since the antigenic stimulus triggers lymph node enlargement, vascular increment, and follicular response, the cortex becomes variably vascular (Fig. 7.1a, b).

Ultrasound anatomy of a reactive lymph node showing cortex (C), medulla (M), and hilum (H) with a prominent vascular pole by Doppler examination (a, b). Anatomic levels of the neck (c)
The Neck Levels, US Examination, and Lymphatic Drainage
There are more than 300 lymph nodes in the head and neck region and range from 3 mm to 3.0 cm in size. The neck has been divided in topographic compartments or levels to facilitate the localization of a particular lymph node. They were first described to map metastases from head and neck squamous cell carcinomas to cervical lymph nodes. The six levels of the neck are: (I) submental and submandibular, (II) upper lateral, (III) mid-lateral, (IV) lower lateral, (V) posterior, and (VI) antero-lateral (Fig. 7.1c). The suprasternal/superior mediastinum is considered level VII.
Level I
Submental (Ia) and submandibular (Ib) area lymph nodes. Level I lymph nodes are important for non-thyroid head and neck carcinomas, particularly those located in the oral cavity.
US examination. For submental nodes, elevate the chin, place the probe transverse to the chin, and scan from the chin down to the hyoid bone. The nodes are superficial in the midline between the anterior bellies of both digastric muscles; they drain the anterior tongue, floor of the mouth, lips, chin, and cheeks (Fig. 7.2). For submandibular nodes, turn the head to the opposite side, place the probe transverse to the neck parallel to the mandible, and scan from the chin back to the angle of the mandible and identify the submandibular gland. The nodes are grouped superior and anterior to the gland and lateral to the anterior belly of the digastric muscle; they drain the anterior face, anterior oral cavity, and floor of the mouth (Fig. 7.3). Of note, there are no lymph nodes within the submandibular gland.


Submental (level 1a) region. The normal anatomy is shown in (a) (transverse view) and (b) (longitudinal view along the midline). A small reactive lymph node between the digastric muscles is seen in (c) (transverse view) and (d) (longitudinal view). Abbreviations: P platysma, aDG digastric muscle, anterior belly, M mandible, GH geniohyoid muscle, MH mylohyoid muscle, LN lymph node

Left submandibular region (level 1b). The transducer is placed parallel to the mandible. There is a small reactive lymph node posterior to the anterior belly of the digastric muscle. Abbreviations: LN lymph node, DG digastric muscle, anterior belly, MH mylohyoid muscle, SmG submaxillary gland
Levels II, III, and IV
These levels correspond to lymph nodes deep to the cervical/internal jugular chain that follows the course of the internal jugular vein extending from the angle of the mandible to the midclavicular region and are the main lymphatic drainage for lesions located in the head and neck, draining the submental, submandibular, parotid, and retropharyngeal nodes. The jugulodigastric node is the most superior and prominent node in the chain, lies behind the submandibular gland, and is virtually visible by US examination in all individuals, measuring up to 4 cm in length in healthy young teenagers.
US examination. Identify the jugulodigastric node with the transducer transversally placed below the angle of the mandible and smoothly sweep down the chain keeping the internal jugular vein in the center of the field while evaluating all levels. In the mid-cervical region, the omohyoid muscle that divides levels III and IV lies deep to the sternocleidomastoid muscle and crosses the vessels mimicking a lymph node; the issue is solved by placement of the transducer in a longitudinal position.
-
Level II. Lymph nodes located from the skull base to the level of the hyoid bone (Fig. 7.4).
Figure 7.4 
Left neck level II. The transducer is placed slightly superior to the carotid bulb and both carotid branches are visualized in (a). The corresponding findings by Doppler examination are seen in (b). Abbreviations: DgM digastric muscle, posterior belly, CAB carotid artery bifurcation, IJV internal jugular vein
-
Level III. Lymph nodes located between the levels of the hyoid bone and the cricoid cartilage (Fig. 7.5).
Figure 7.5 
Left neck level III. Normal US anatomy showing the trachea (T), esophagus (E), left thyroid lobe (Th), strap muscles (SM), omohyoid muscle (OH), common carotid artery (CCA), internal jugular vein (IJV), sternocleidomastoid muscle (SCM), and longus colli (LC). A small lymph node with hilum (LN) and the vagus nerve are also seen
-
Level IV. Lymph nodes located below the levels of the cricoid cartilage and the clavicle (Fig. 7.6).
Figure 7.6 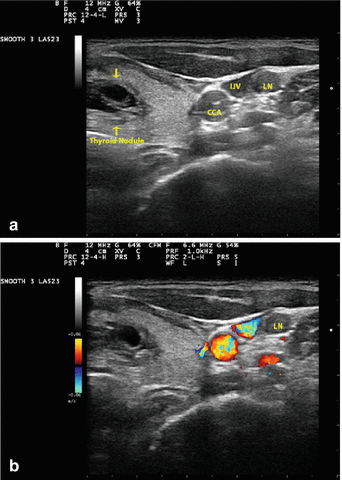
Left neck level IV. US images show a predominantly cystic complex left thyroid nodule, the common carotid artery (CCA), internal jugular vein (IJV), and a round-shaped lymph node (LN) posterior to the IJV (a). Corresponding findings by Doppler exam (b). US-guided FNA of both the thyroid nodule and lymph node showed papillary thyroid carcinoma



Level V
This level corresponds to lymph nodes located in the supraclavicular fossa/transverse cervical chain posterior to the sternocleidomastoid muscle and superior to the subclavian vein and in the posterior triangle. The boundaries of the triangle are the sternocleidomastoid muscle anteriorly, the clavicle inferiorly, and the trapezius muscle posteriorly (Fig. 7.7). The lymph nodes are located superficially within this triangle filled with adipose tissue. Enlargement of the left supraclavicular lymph node (Virchow’s node) often indicates a primary malignancy located below the diaphragm. The posterior triangle lymph nodes drain the skin of the occipital and mastoid regions, posterior scalp, lateral neck, and the postnasal space.

Left neck level V, supraclavicular area. Normal anatomy is seen in this image and include the trapezius muscle (Tr), and anterior, medial, and posterior scalene muscles (ScA, ScM, ScP)
US examination. Scan transversally along the superior border of the midclavicle to the lateral end of the clavicle to evaluate the supraclavicular fossa. The posterior triangle is scanned with the transducer transverse to the mastoid process, moving inferiorly along the posterior border of the sternocleidomastoid muscle toward the acromioclavicular joint and the anterior border of the trapezius.
Level VI
These lymph nodes are located in the anterior central neck compartment. The prelaryngeal and pretracheal lymph nodes are superficial and the paratracheal are lateral to the trachea, medial to the carotid artery, and deeper in the tracheoesophageal groove. The prelaryngeal and pretracheal nodes drain the skin and muscles of the anterior neck and the thyroid gland. The prelaryngeal lymph node drains the subglottic area of the larynx. The paratracheal lymph nodes are difficult to visualize by US because they lie posterior to the thyroid gland; they drain the larynx, the pyriform fossae, the thyroid gland, and the esophagus.
US examination. Scan moving the probe in the transverse plane with the probe in a longitudinal position from the level of the hyoid bone down to the sternal notch.
Level VII
These lymph nodes are located in the suprasternal/superior mediastinum. Best evaluated using a small-footprint curvilinear probe placed above the sternal notch (Fig. 7.8).

Neck level VII. The transducer is placed above the sternal notch and is used for evaluation of suprasternal/superior mediastinum lymph nodes. SCJ sternoclavicular joint
The parotid-area lymph nodes have no numbered level. They drain the skin of the lateral forehead, temple, external auditory meatus, posterior cheek, gums, and buccal mucosa. Likewise, the buccal region lymph nodes are not numbered, lie anterior to masseter muscle adjacent to the facial artery in the buccal fat space, and drain the facial skin from the upper eyelid to the upper lid.
The retroauricular and occipital lymph nodes drain corresponding areas of the scalp and should be examined in cases of scalp malignancy.
US can typically identify between 6 and 20 neck lymph nodes. Most enlarged lymph nodes are reactive secondary to inflammatory or infectious processes located in the head and neck area. Lateral compartment lymph nodes are easier to detect and amenable to USG-FNA. Central-compartment lymph nodes are more difficult to detect by US and sample using US guidance.
US Features in Lymph Node Evaluation
The US features to be evaluated in a lymph node include, size, shape, border, confluence, echogenicity, hilum, calcification, necrosis, parenchymal reticulation, intranodal vascular pattern, and surrounding edema. Because no abnormality of these features by itself is diagnostic of malignancy, a combination of the ultrasound findings helps in predicting malignancy. The lymph node number in a given lymph node chain is a consideration for abnormality when >3 US-abnormal lymph nodes are present.
-
1.
Size. Lymph node size is an important consideration; however, the most important factor is the variation in the lymph node size over a period of time. Size may be of limited value in differentiating benign from malignant nodes. Nodal size is important for TNM cancer staging: N1 <3 cm, N2 3–6 cm, and N3 >6 cm. The lymph node size should be measured transversally and not longitudinally (Fig. 7.9).
Figure 7.9 
Lymph node size. Small oval level III left (a) and right (b) neck lymph nodes. Metastatic papillary thyroid carcinoma (calipers, a) and reactive follicular hyperplasia (b) were the US- guided FNA diagnoses. Abbreviations: LN lymph node, CCA common carotid artery, SM strap muscles, T trachea
-
2.
Shape. A normal node has a flat bean shape. An irregular or round shape is seen in metastasis instead of the oval shape often seen in benign and reactive lymph nodes. An irregular lymph node cortex is suggestive of a subcapsular metastatic deposit. It has been found that 85 % of benign lymph nodes have a ratio of antero posterior (AP) axis/transverse (T) axis < 0.5, and 85 % of malignant nodes have an AP/T axis ratio > 0.5 in the transverse view. Of note, level Ia and Ib benign lymph nodes are often round (Fig. 7.10).
Figure 7.10 
Lymph node shape. Oval (antero posterior/transverse < 0.5) level 1a lymph node (horizontal arrows) with regular borders and prominent hilum (vertical arrow) (a US-guided FNA diagnosis was reactive follicular hyperplasia). Left neck lymph node with heterogeneous echotexture, irregular borders (arrows), and taller than wide (antero posterior/transverse > 0.5) in the transverse view (b US-guided FNA diagnosis was poorly differentiated metastatic squamous cell carcinoma)
-
3.
Border. The border of a normal lymph node is smooth and slightly indistinct from the surrounding tissue. A sharp lymph node border is seen in metastasis and lymphoma instead of an ill-defined border seen in a reactive lymph node. Extracapsular nodal involvement of malignancy and response to radiotherapy also cause ill-defined borders. Ill-defined and spiculated/irregular margins in a metastatic node indicate extranodal metastatic spread (Fig. 7.11).
Figure 7.11 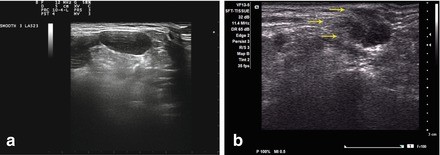
Lymph node borders. Neck lymph node with oval, homogeneous, and slightly lobulated well-defined sharp borders (a Hodgkin lymphoma was the US-guided FNA diagnosis). Neck level 1 lymph node with spiculated borders (arrows) and heterogeneous echotexture (b metastatic breast carcinoma was the US-guided FNA diagnosis)
-
4.
Confluence. Matted lymph nodes can be seen in tuberculosis, postradiation, chemotherapy, metastasis, and lymphoma as a result of perinodal inflammation and fibrosis (Fig. 7.12).
Figure 7.12 
Lymph node confluence. Matted hypoechoic homogeneous lymph nodes. Non-Hodgkin lymphoma was the US-guided FNA diagnosis
-
5.
Echogenicity. Hypoechogenicity is seen in metastatic malignancies; however, metastatic papillary thyroid carcinoma may be hyperechoic when compared with adjacent muscle. A “pseudocystic” pattern (marked hypoechogenicity with posterior acoustic enhancement) is seen in lymphoma when evaluated at conventional US resolution (Fig. 7.13).
Figure 7.13 
Lymph node echogenicity. Hyperechic lymph node in a patient with metastatic Hurthle cell carcinoma of the thyroid gland (a arrow heads). Lymph node with marked hypoechogenicity (“pseudocystic” pattern) and posterior acoustic enhancement in a patient with non-Hodgkin lymphoma (b)
-
6.
Hilum. A vascular hilum is usually seen in 90 % of lymph nodes >5 mm. An enlarged lymph node with a prominent echogenic vascular hilum is probably benign. Metastatic lymph nodes usually lack a hilum; however, a hilum can be seen in metastasis, particularly in early metastatic nodal involvement. Thus, hilum absence in an enlarged lymph node is highly suspicious for malignancy. Of note, tuberculous lymph nodes usually lack a hilum (Fig. 7.14).
Figure 7.14 
Benign lymph node with a prominent hilum (a arrow heads) highlighted by Doppler examination (b)
-
7.
Calcification. Metastasis from papillary thyroid carcinoma, medullary carcinoma, or lymph nodes in patients with a history of radiotherapy or chemotherapy may show foci of macrocalcification. Macrocalcifications are also seen in tuberculous lymphadenitis (Fig. 7.15).
Figure 7.15 
Metastatic thyroid carcinoma to a level V lymph node. Note microcalcifications in the upper part of the node
-
8.
Necrosis. Cystic necrosis can be seen in metastases, i.e., squamous cell carcinoma, papillary thyroid carcinoma, and benign processes such as tuberculosis (Fig. 7.16). A cystic nodal metastasis >3 cm in squamous cell carcinoma appears anechoic and, if it involves the jugulo digastric lymph node, should be differentiated from a branchial cleft cyst, particularly in patients older than 30 years. Coagulative necrosis may appear hyperechoic and may be confused with hilum when located close to the nodal capsule; however, it is not continuous with the perinodal fat as the hilum is.
Figure 7.16 
Necrosis. Tuberculous lymphadenitis with focal necrosis (n) and preserved hilum (a arrow). Level V cervical lymph node with metastatic squamous cell carcinoma with central necrosis (b)
-
9.
Intranodal reticulation. A micronodular reticulated pattern is seen in lymphoma when evaluated with high-resolution US. Under conventional resolution, lymph nodes have a “pseudocystic” appearance with marked hypoechogenicity and posterior acoustic enhancement.
-
10.
Nodal vascular pattern. Normal or reactive lymph nodes usually have no vascularity when they measure <5 mm. Metastatic lymph nodes may have hilar and peripheral (mixed) or peripheral subcapsular flow and perfusion defects (Fig. 7.17a). Peripheral subcapsular flow is also seen in tuberculosis, which disrupts the nodal vascular architecture in a manner similar to malignancy. An exaggerated normal vascular appearance with a branching hilar vascular pattern is often seen in lymphoma (Fig. 7.17b).
Figure 7.17 
Vascular pattern. Metastatic poorly differentiated carcinoma showing a chaotic vascular flow pattern (a). Non-Hodgkin lymphoma showing an exaggerated branching hilar vascular pattern (b)









Thus, the US characteristics and topographic distribution of the lymph nodes, and the clinical scenario including physical examination, are paramount for the cytopathologist to provide a useful microscopic interpretation, which in some instances does not need to be specific but only descriptive. The lack of specific findings is also useful in some cases.
Fine-Needle Aspiration of Lymph Nodes
The clinical history and the characteristics of a lymph node are factors important for deciding on the need for additional diagnostic modalities, i.e., imaging studies and FNA. FNA is the modality of choice for evaluating an abnormal lymph node and, in many instances, avoiding an unnecessary open biopsy. The use of US as an aid in locating and performing FNA of superficial and deep-seated lymph nodes offers significant benefits, i.e., sampling of solid areas in cystic necrosis and reducing nondiagnostic samples, procurement of sample for cultures, and obtain material for flow cytometry in lymphomas. USG-FNA has a sensitivity of 97 % and a specificity of 93 %.
A thorough cytologic evaluation answers questions which the cytopathologist should keep in mind when evaluating lymph node FNAs. The questions include the following: (1) Is it really a lymph node? (2) Adequate? (3) Is it benign or malignant? (4) If benign, is it infectious? Can we identify the infectious agent? (5) If malignant, lymphoma? Metastasis? (6) If lymphoma, non-Hodgkin? Hodgkin?, (7) If non-Hodgkin, B- or T-cell type? Grade? (8) If Hodgkin, subtype? (9) If metastasis, type? Source? Most answers can be based on morphologic evaluation, and others need the support of ancillary tests, i.e., cultures, special stains, flow cytometry, cytogenetics, molecular studies, etc., for reaching a definitive diagnosis.
The use of Romanowsky-type stains (Diff-Quik, Wright, May–Grunwald–Giemsa) performed on air-dried smears is fundamental for FNA cytologic interpretation, because they provide excellent evaluation of cell size, cytoplasmic detail, and background elements. Papanicolaou and hematoxylin and eosin stains performed on alcohol-fixed smears provide excellent visualization of nuclear morphology in both single cells and cell aggregates. Thus, both air-dried and alcohol-fixed stains are complementary. We caution against the use of liquid-based preparations for lymph node FNA because cells appear smaller, cell aggregates are fragmented, lymphocytes may become artificially aggregated, and background elements are difficult to evaluate.
Cell Patterns in Fine-Needle Aspiration of Lymph Nodes
To facilitate the cytologic interpretation, the FNA of lymph nodes can algorithmically be classified in the following smear cell patterns:
-
1.
Polymorphous. Nonspecific reactive lymphoid hyperplasia, early HIV lymphadenitis, primary and secondary syphilis lymphadenitis, toxoplasma and leishmania lymphadenitis, rheumatoid arthritis, Castleman lymphadenopathy plasma cell variant, Kimura lymphadenopathy, early dermatopathic lymphadenopathy, Sézary syndrome, early cat scratch lymphadenitis, follicular lymphoma grade 2, diffuse follicular center cell lymphoma, and nodal marginal B-cell lymphoma
-
2.
Monotonous small size. Quiescent benign lymph node, Castleman disease hyaline vascular variant, B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma, T-cell chronic lymphocytic leukemia, lymphoplasmacytic lymphoma, T-cell/histiocyte-rich diffuse large B-cell lymphoma, and Hodgkin lymphoma lymphocyte-predominant type
-
3.
Monotonous intermediate size. Follicular lymphoma grade 1, diffuse follicle center cell lymphoma grade 1, mantle cell lymphoma, nodal marginal zone lymphoma, Burkitt lymphoma, precursors of B- and T-cell lymphomas, adult T-cell leukemia/lymphoma, peripheral T-cell lymphoma, Sézary syndrome, and metastatic small cell malignancies
-
4.
Monotonous large size. Diffuse large B-cell lymphoma and its variants, follicular lymphoma grade 3, Richter’s transformation of small lymphocytic lymphoma, blastoid variant of mantle cell lymphoma, peripheral T-cell lymphoma, NK-/T-cell lymphoma, granulocytic sarcoma, nodal Langerhans cell histiocytosis, dendritic cell neoplasms, metastatic carcinoma, metastatic melanoma, metastatic sarcoma, and metastatic seminoma
-
5.
Pleomorphic. Hodgkin lymphoma, anaplastic large cell lymphoma, Hodgkin-type Richter’s transformation of small lymphocytic lymphoma/chronic lymphocytic leukemia, diffuse large B-cell lymphoma variants, thymoma, metastatic melanoma, and metastatic mesenchymal malignancies
Select Examples of Lymphadenopathy
Reactive Lymphoid Hyperplasia
Reactive lymphoid hyperplasia is the prototype of a cytologic polymorphous lymphoid cell pattern commonly associated with benign, reactive and reversible, lymphadenopathy. The etiology remains unknown in most cases. Bacteria, viruses, chemicals, and iatrogenic drugs are identified in a minority of cases. The lymph nodes are small, oval, soft, and single or regional, often cervical in children and inguinal in all age groups.
The cytologic pattern reflects the expansion of a particular lymph node area (follicular, paracortical, medullary, sinusoidal), which depends on the antigenic stimulus. Follicular hyperplasia represents a B-cell response and includes the presence of small round lymphocytes, centroblasts, centrocytes, immunoblasts, plasmacytoid lymphocytes, plasma cells, and histiocytes/tingible-body macrophages in various numbers. Paracortical hyperplasia with predominance of immunoblasts represents a T-cell response. An inflammatory pattern is frequently associated with bacteria and fungi. An immune pattern is usually the result of drugs and viruses, and it often elicits a paracortical hyperplasia. Occasionally, the differential diagnosis includes follicular lymphoma grades 2 and 3, and the use of ancillary tests on FNA material is needed.
The smears are cellular and show a polymorphous population of lymphoid cells and lymphohistiocytic aggregates, which are fragments of germinal centers containing centrocytes, centroblasts, dendritic cells, small lymphocytes, and tingible-body macrophages. After a single triggering factor, the smears show a polymorphous pattern lasting 3–4 weeks; progressively, the smear shows a predominance of small round lymphocytes and centrocytes for 3–4 weeks. The background shows histiocytes, scattered plasmacytoid cells, plasma cells, and lymphoglandular bodies (Fig. 7.18).

Reactive lymph node. The smear shows a characteristic polymorphous population of lymphoid cells (a). The US evaluation shows an oval (AP/T < 0.5 in the transverse view), hypoechoic, homogeneous, and well-defined lymph node with regular borders and presence of hilum (b). AP antero posterior axis, T transverse axis)
The immunophenotype shows positive pan-B-cell markers CD19, CD20, CD22, and CD79a with a K/L ratio of 3–5/1 and no light-chain restriction.
Of note, this pattern is seen as a smear background in Hodgkin lymphoma and along with histiocytes in cases of draining lymph nodes in metastatic disease, regardless of the presence or absence of actual metastatic deposits.
Bacterial Lymphadenitis
This process is seen in the head and neck of children draining, an area of bacterial infection. Patients have fever, the lymph node is enlarged and tender, and the overlying skin is usually hyperemic.
The smear pattern shows numerous intact and degenerated neutrophils; degenerated lymphoid cells and macrophages may also be present. This pattern may be seen in systemic lupus erythematosus and rarely in Hodgkin lymphoma. Bacterial organisms may be seen best with Romanowsky-stained smears inside phagocytes and extracellularly (Fig. 7.19).

Bacterial lymphadenitis. Smear shows a purulent smear pattern (a). The US exam shows a lymph node with ill-defined margins, heterogeneous echotexture, and a cystic component (b arrow heads)
Granulomatous Lymphadenitis
Etiologic agents for this smear pattern include infections, foreign body reactions, and sarcoidosis.
Mycobacterium tuberculosis is prevalent in HIV-infected individuals and in foreign-born young immigrants to the US. The most common form of extrapulmonary tuberculosis is lymphadenitis that commonly affects cervical (frequently posterior triangle) chains. The lymph nodes may be matted and markedly necrotic and fluctuant. The M. tuberculosis activates CD4+ T cells and produces tissue necrosis, and the macrophages transform into uni- or multinucleated epithelioid macrophages. Thus, the smears of tuberculous lymphadenitis show epithelioid granulomas, caseation necrosis, lymphocytes, and occasional Langhans-type giant cells. The nuclei of such cells are arranged peripherally in a horseshoe shape rimming in the cytoplasm. The bacilli can be detected by special acid-fast staining and are detected predominantly in the background smear. The bacilli are bright red, slender, and beaded by the Ziehl–Neelsen acid-fast stain; however, only 20 % of culture-positive cases have a positive stain. Culture in Lowenstein–Jensen medium can take up to 6 weeks for a definitive diagnosis, thus delaying treatment. Polymerase chain reaction in fluids, smears, and tissue samples, including paraffin-embedded tissue, can detect the organism in less than 6 h.
Atypical mycobacteria are a cause of chronic granulomatous lymphadenitis in children. In adults, the infection occurs in the presence of immunosuppression. The organisms are widely spread in nature and include M. marinum, M. fortuitum, M. scrofulaceum, and M. kansasii. Commonly affected sites include cervical lymph nodes and may be associated with erythema of the overlying skin and with abscess formation. Mycobacterium avium intracellulare (MAI), found in the soil and in tap water, is highly pathogenetic in patients with AIDS and may produce regional or generalized lymphadenitis and systemic disease. The smears show necrosis, poorly formed granulomas, and numerous large histiocytes with foamy cytoplasm (pseudo-Gaucher cells) filled with bacilli. Occasionally, the histiocytes develop a spindle cell phenotype (MAI spindle cell pseudotumor). The characteristic negative images within the cytoplasm of macrophages and in the background are best seen in Romanowsky-stained smears. The definite diagnosis is made by cultures and polymerase chain reaction in smears and formalin-fixed, paraffin-embedded tissue (Fig. 7.20).

Tuberculous lymphadenitis. Smears show necrosis, damaged inflammatory cells, histiocytes, multinucleated giant cells, and granulomas (a, b Mycobacterium tuberculosis). Atypical mycobacteria with numerous thick and long organisms that appear as “negative images” both in the background of the smear (c) and within histiocytes (“pseudo-Gaucher” cells) (d Mycobacterium avium intracellulare). The US exam shows a large lymph node with hypoechogenicity, smooth distinct margins, foci of cystic degeneration (e arrow heads), and mild central and peripheral vascularity on Doppler examination (f) (a, d DiffQuik stain, medium and high magnification)
The differential diagnosis of granulomatous lymphadenitis includes tuberculosis, histoplasma, Kikuchi and cat scratch lymphadenitis, and sarcoidosis. Non-necrotizing granulomas are often seen in sarcoidosis, which shows tightly packed granulomas and damaged lymphoid cells; cultures are negative. Fungal infections may involve the lymph nodes, particularly when immunocompetency is affected. The prevalence of these infections is influenced by the incidence of mycoses, i.e., histoplasmosis and coccidioidomycosis, in certain geographic areas. The identification of the organism in cytologic material permits the application of early antifungal therapy before culture and serologic results are available.
Cat Scratch Disease
Cat scratch disease is a common cause of chronic lymphadenitis in children and adolescents. In the United States, 55 % of cases occur in patients age 18 years or younger, commonly in the months of September to January. The pathogenic organism is Bartonella henselae, a Gram-negative bacillus transmitted by fleas to kittens and then transmitted to humans by a cat bite or lick.
The patients have enlarged, nodular, and matted regional lymphadenopathy that is fixed to surrounding tissues and commonly occurs in the upper extremities and face. The lymphadenopathy develops 1–3 weeks after the primary skin lesion and is usually accompanied by systemic symptoms. In immunocompetent individuals, the disease is self-limited and resolves in 6–12 weeks in the absence of treatment. Suppuration occurs in 10 % of cases. A systemic life-threatening disease may occur in immunosuppressed patients.
The smears show a reactive lymphoid hyperplasia pattern with monocytoid cells and scattered tingible-body macrophages in the early stages of the disease. A suppurative granulomatous pattern with necrosis, neutrophils, epithelioid histiocytes, granulomas, and rare multinucleated Langhans-type giant cells is seen in more established processes (Fig. 7.21).

Cat scratch disease. Smears show a purulent pattern with necrosis, acute inflammation damaged lymphocytes, and granulomas (a, b). The US exam shows irregularly-shaped, coalescent lymph nodes with necrosis and no vascularity on Doppler examination (c, d) (a, b DiffQuik stain, high magnification)
Microbiologic detection is difficult, and the diagnosis is supported by clinical history, serology, and histopathology. The organisms can be visualized by the Warthin–Starry silver stain, immunoperoxidase stain with anti-B. henselae antibodies in tissue sections, PCR, indirect immunofluorescence, and enzyme immunoassay. The diagnostic sensitivity of all tests is low. The silver stain is the most sensitive, but is the least specific. Lymphogranuloma venereum is cytologically identical, and immunofluorescence and serology are necessary for the diagnosis. The differential cytologic diagnosis also includes bacterial suppurative lymphadenitis, tularemia, and other granulomatous processes, including tuberculosis; special stains and cultures are needed to rule out these processes.
Infectious Mononucleosis
Infectious mononucleosis is an acute self-limited disease caused by the Epstein–Barr virus (EBV) that affects predominantly adolescents and young adults, who have fever, pharyngitis, and cervical or generalized lymphadenopathy. The lymph nodes are enlarged and soft, but not matted. The viral spread is via direct contact with oral secretions. The EBV infects both epithelial cells and B cells in the oropharynx; B cells can be infected via the CD3d complement receptor (CD21) causing an antibody response with cell proliferation during the first week of the disease. Lymphocytosis with atypical lymphocytes is commonly seen in the peripheral blood. The disease resolves in 3–4 weeks in most patients. A life-threatening disease is seen in immunosuppressed individuals.
The cytology preparations show numerous large reactive immunoblasts, large and small lymphocytes, histiocytes, tingible-body macrophages, and rare plasma cells. Numerous mitoses and apoptotic nuclei are also present. The immunoblasts are large and show a basophilic cytoplasm, a large nucleus, and a single central round or polyhedral nucleolus. Necrosis may be present (Fig. 7.22).

Infectious mononucleosis. Smears show numerous reactive immunoblasts with bluish cytoplasm, large nuclei, prominent nucleoli, and scattered mitoses (a). The US exam shows large odd-shaped hypoechoic lymph nodes with predominant medullary and polar vascularity (b, c) (a DiffQuik stain, high magnification)
No light-chain restriction is identified, and the immunostains for B and T cells demonstrate a reactive pattern. EBV can be demonstrated by immunohistochemistry, in situ hybridization, and other types of molecular analysis in tissue sections. The differential diagnosis includes large cell lymphoma, anaplastic large cell lymphoma, nodular lymphocyte predominance Hodgkin lymphoma, and classical Hodgkin lymphoma.
Human Immunodeficiency Virus
The human immunodeficiency virus 1 (HIV-1) is a lentivirus, a subfamily of retroviruses that infects CD4+ lymphocytes, macrophages, and dendritic cells; the first disseminates the virus, and the last two are the reservoirs. In the late stage, the CD4 lymphocytes and the dendritic cells are destroyed, the viremia resurges, and opportunistic infections and tumors develop in the immunosuppressed host.
In the acute and chronic phase of HIV infection, there is generalized lymphadenopathy that harbors processes that may be reactive, infectious (mycobacterial and fungal), or neoplastic (lymphoma, Kaposi’s sarcoma). In the acute phase, the smear shows a florid reactive lymphoid hyperplasia, scattered large monocytoid cells with clear cytoplasm and round nuclei, neutrophils, multinucleated cells (polykaryocytes of Warthin–Finkeldey), and tingible-body macrophages. The smears are less cellular, and the present plasma cells are notorious in the subacute phase of HIV lymphadenitis. Hypocellular smears with a paucity of lymphocytes and predominance of plasma cells are characteristic of the chronic burned-out phase of HIV infection.
The main role of FNA in HIV patients is to rule out opportunistic infections and neoplasms such as lymphoma or Kaposi’s sarcoma.
Ultrasound Features of Reactive and Infectious Lymph Nodes
Reactive lymph nodes usually have the following characteristics: hypoechoic, slightly ill-defined margins, hilum present, hilar vascular pattern except lymph nodes <5 mm, lack of peripheral blood flow by Doppler examination, and flat or oval shape (AP/T axis < 0.5) except lymph nodes involving level I, which may be round. Lymph nodes involved by granulomatous infectious processes including cat scratch disease and tuberculosis may have pronounced cystic necrosis and lymph node confluence in addition to the mentioned findings (Figs. 7.18b, 7.19b, 7.20e, f, 7.21c, d, and 7.22b, c).
Non-Hodgkin Lymphoma (NHL)
The use of FNA cytology for diagnosing NHLs is well established. In fact, most malignant lymphomas can be diagnosed and treated on the basis of cytomorphology and special studies done on FNA material. Judicious use of ancillary tests is paramount, and flow cytometry is most important in the detection of cell surface markers to establish light-chain monoclonality and characterize the clonal proliferation. Normal mature B cells express CD19, CD20, and CD22 and are good markers in B-cell lymphomas. Plasma cells lack such markers; instead, they express CD38 and CD138. CD10 is expressed by both early B- and T-cell progenitor cells and follicular lymphoma. The T-cell markers CD5 and CD43 may normally be expressed in a small percentage of B cells; CD5 is aberrantly coexpressed in some small cell types of B-cell lymphomas. T-cell clonality is difficult to establish by flow cytometry.
The various types of NHLs are defined by their morphology, immunophenotype, cytogenetics, and clinical features (Table 7.3).
Combining cytomorphology and immunophenotype, the diagnosis of NHL can be reached successfully in FNA material. In the following paragraphs, we will briefly review the characteristics of the common NHLs found in clinical practice.
Large Cell Lymphoma
This is one of the most common neoplasms diagnosed by FNA and affects mainly adults in the seventh decade of life. Young adults and children may be affected occasionally. The primary presentation is usually nodal, but extranodal spread or presentation may be seen. B cell is the most common phenotype and is usually diffuse on tissue examination.
The cytology shows monomorphous large lymphoid cells; however, the particular cytomorphology is variable, i.e., centroblasts, centroblasts and immunoblasts, and less frequently true immunoblasts may be seen (Fig. 7.23a–d). Variable anaplasia including large cells with irregular multilobed nuclei can also be seen. The rare anaplastic B-cell lymphoma shows less pleomorphism than does the T-cell counterpart. The T-cell-rich B-cell lymphoma shows rare large pleomorphic tumor cells and a background of numerous small lymphocytes and mimics Hodgkin lymphoma, carcinoma, or melanoma.

Diffuse large B-cell lymphoma. Large monomorphous cells with dark blue cytoplasm, some plasmacytoid features, irregular nuclear contours, mitoses, and apoptotic bodies (a). Large cells with round nuclei, basophilic cytoplasm, and prominent nucleoli are characteristic of immunoblastic lymphoma (b). The US exam shows dysmorphic coalescent lymph nodes with well-defined, margins, marked hypoechogenicity, and intense chaotic hilar blood flow by Doppler examination (c, d) (a From Pambuccian and Bardales (2011). Reprinted with permission)
Cells show light-chain monoclonality and positive B-cell markers CD19, CD20, and CD79a. CD10 is positive in centroblastic lymphoma and CD30 in the anaplastic variants. Large-cell lymphoma has a high proliferation index and frequently expresses bcl-2 and bcl-6. One third of cases show t(14;18).
Follicular (Small Cleaved and Mixed Small Cleaved and Large-Cell) Lymphoma
Follicular lymphomas arise in the lymph node follicular centers and affect mainly middle-aged patients who usually have generalized lymphadenopathy. The lymph nodes in small cleaved follicular lymphoma have a nodular or diffuse histologic pattern that gives the lymphoma a low or intermediate grade, respectively, with prognostic implications. The mixed type is an intermediate-grade lymphoma. Follicular lymphomas need tissue confirmation for precise classification. The clinical course depends on the stage and grade, and cure is rare. Large-cell malignant transformation occurs in 30 % of patients, who have a poor prognosis.
The cytology of the small cell type shows a monotonous population of small lymphocytes (centrocytes) with irregular nuclear contours, i.e., indentations, notches, and clefts, which are best seen in Papanicolaou-stained smears; nucleoli are rarely identified. The mixed cell type shows a polymorphous population of centrocytes and medium-sized atypical lymphocytes with a round nucleus and peripheral nucleoli (centroblasts), usually with predominance of the former; this pattern must be differentiated from that of reactive follicular hyperplasia. Cell aggregates may suggest a nodular pattern when smears are evaluated at low magnification. Small T lymphocytes are also present in the background (Fig. 7.24).

Follicular lymphoma. Smear shows a follicular pattern at screening magnification (a). Cells are monomorphous of small to intermediate size and have irregular nuclear contours (b). The US exam, in this particular case shows coalescent lymph nodes with presence of hilum, thick and irregular cortex, well-defined margins, hypoechogenicity, and hilar vascular blood flow by Doppler examination (c, d) (a, b MGG stain, low and high magnification) (b From Pambuccian and Bardales (2011). Reprinted with permission)
Cells show light-chain monoclonality and CD19, CD20, CD79a, and CD10 positivity. CD5 and CD43 are negative. Cells express bcl-2 in most cases. In 95 % of cases, t(14;18) is seen.
Small Lymphocytic Lymphoma
This mainly B-cell neoplasm is the nodal counterpart of chronic lymphocytic leukemia, affects middle-aged and older populations, involves multiple lymph nodes, and is a low-grade malignancy. The clinical course is indolent; however, in rare instances, it may undergo a high-grade large B-cell transformation (Richter’s lymphoma).
The cytology shows a monotonous pattern of small lymphocytes with a round nucleus, coarse chromatin, and inconspicuous nucleoli. Scattered large cells (paraimmunoblasts and prolymphocytes) can be found. Distinction from other lymphomas of the small cell type is based on flow cytometry and not on pure cytomorphology (Fig. 7.25) (Table 7.4).

Small cell lymphocytic lymphoma. The smear shows a monotonous population of small round lymphoid cells (a). The precise diagnosis is made based on flow cytometric analysis. Large cell lymphoma transformation may occur (Richter lymphoma) and the vacuolated cytoplasm is often the result of prior chemotherapy (b). The US evaluation showed slightly enlarged cervical lymph nodes with linear hilum (c) and minimal blood flow by Doppler exam (d) (a, b DiffQuik, high magnification) (a From Pambuccian and Bardales (2011). Reprinted with permission)
Cells show CD19, CD20, CD23, and CD79a positivity. CD5 positivity is characteristic, and cells are negative for CD10 (positive in follicular lymphoma) and FMC7 (positive in mantle cell lymphoma). Deletion (13q14) is present in 50 % of the patients and is associated with a favorable prognosis. Trisomy 12, t(11;14), and t(14;19) have been described.
Mantle Cell Lymphoma
Mantle cell lymphoma occurs in middle-aged to older individuals, with male predominance. Most patients have generalized lymphadenopathy, hepatosplenomegaly, and GI and bone marrow and peripheral blood involvement. Most patients cannot be cured.
Cytologic preparations show monotonous lymphoid cells of intermediate size with irregular nuclear contours resembling centrocytes with dispersed chromatin and inconspicuous nucleoli; the larger cells may have single small, distinct nucleoli. Rare plasmacytoid lymphocytes may be seen. Scattered epithelioid histiocytes and plasma cells are commonly present (Fig. 7.26).

Mantle cell lymphoma. The smear shows a monotonous population of small slightly irregular lymphoid cells (a). The diagnosis needs flow cytometry evaluation in material obtained by FNA. The US exam shows a lymph node with well-defined margins, hypoechogenicity, homogeneous echotexture, and prominent vascular pattern by Doppler exam (b, c) (a DiffQuik stain, high magnification) (a From Pambuccian and Bardales (2011). Reprinted with permission)
Cell show CD5+, FMC7+, CD43+, BCL2+, BCL6–, and CD10– (Table 7.4). All cases express bcl-2 and cyclin D1. Neoplastic cells showing t(11;14)(q13;q32) with CCND1 translocation are seen in almost all cases.
Marginal Zone Lymphoma
Monocytoid B-cell lymphoma and mucosa-associated lymphoid tissue (MALT) lymphoma have been grouped as nodal and extranodal types of marginal zone lymphoma, respectively, and have identical histology and cytology. The nodal type that comprises <2 % of all non-Hodgkin lymphomas is a primary lymph node B-cell neoplasm without splenic or extranodal involvement and affects mostly adults and older individuals who have asymptomatic regional, often cervical or generalized lymphadenopathy. It is clinically indolent, and most patients survive longer than 5 years. Some patients may have serologic evidence of hepatitis C infection or autoimmune disorders.
The cytology shows monocytoid cells or medium-sized cells with irregular contours (centrocyte-like cells), or cells resembling small-/intermediate-sized round lymphocytes, or a combination of the three in various proportions. Plasma cell differentiation may be prominent in some cases, and scattered eosinophils may be present (Fig. 7.27).

Marginal zone lymphoma. A monotonous population of intermediate size centrocyte-like lymphoid cells with slightly irregular nuclei is seen (a). The precise diagnosis is made by flow cytometry on FNA material. Ultrasound shows coalescent lymph nodes with hypoechogenicity, well-defined margins, and chaotic vascular flow by Doppler exam (b, c) (a DiffQuik stain, high magnification) (a From Pambuccian and Bardales (2011). Reprinted with permission)
As seen in Table 7.4, CD5, CD10, BCL6, and cyclin D1 are negative and bcl-2 is positive. CD23 may be faintly positive. Trisomy 3 (60 %) or t(11;18) may be seen.
Small Non-cleaved Cell (Burkitt) Lymphoma (BL)
Three variants, endemic, sporadic, and immunodeficiency associated, have been described and differ clinically, morphologically, and biologically. Endemic BL occurs in equatorial Africa in areas of endemic malaria and affects predominantly children. Sporadic BL is seen throughout the world, represents <2 % of all non-Hodgkin lymphomas in the United States, and affects predominantly children and young adults. Immunodeficiency-associated BL is often associated with HIV infection. Patients have bulky disease and signs and symptoms of a few weeks’ duration due to the short doubling time of the tumor. Endemic and sporadic BL may be cured with intensive chemotherapy regimens.
The cytology shows tumor cells of medium size with round nuclei and evenly distributed chromatin with multiple nucleoli. The cytoplasm is moderate in amount, deeply basophilic, and usually contains a number of clear-lipid-containing vacuoles. Numerous mitoses are present as well as numerous macrophages with ingested apoptotic tumor cells. The spectrum of BL is wide, and some cases may show tumor cells with plasmacytoid features or nuclear pleomorphism with prominent nucleoli (Fig. 7.28).

Burkitt’s lymphoma. The smear shows a population of intermediate-size cells with multiple nucleoli and distinct minute cytoplasmic vacuoles (DiffQuik stain, high magnification) (From Pambuccian and Bardales (2011). Reprinted with permission)
Tumor cells are monoclonal and CD10, CD19, and CD20 positive. bcl-2 is negative and bcl-6 is positive. The Epstein–Barr virus (EBV) genome is present in the neoplastic cells in all cases of endemic BL and in approximately 30 % of sporadic and immunodeficiency-associated BL. Most cases have an (8;14) translocation.
Precursor B- and T-Cell Lymphomas
The term lymphoblastic lymphoma (LBL) is used when the process is confined to a mass lesion with minimal or no peripheral blood and bone marrow involvement. Whereas the B-cell lineage predominates in lymphoblastic leukemia, only 10 % of LBLs have a B-cell phenotype. In general, LBLs are seen often in children and adolescents. The most frequent sites of involvement in B-LBL are the skin, soft tissue, bone, and lymph nodes. Mediastinal (thymic) involvement is often present in T-LBL and infrequent in B-LBL. Any extranodal site may be involved in T-LBL. Lymphadenopathy, hepatomegaly, and splenomegaly are frequent in B- and T-LBL.
The cytology shows cells of small or intermediate size. The small cells are uniform and have scant cytoplasm; round nuclei with occasional clefting and indentations; homogeneous, fine, and delicate chromatin; and multiple variably prominent nucleoli. When intermediate-sized cells predominate, the pattern shows more anisocytosis; moderate cytoplasm; fine and delicate chromatin; often irregular, clefted, and indented nuclear contours; and two to three small nucleoli. Mitotic figures are often numerous (Fig. 7.29).

Lymphoblastic lymphoma. A monotonous population of intermediate-size lymphoid cells some with slight nuclear irregularities is seen (MGG stain, high magnification)
Tumor cells are positive for the enzyme terminal deoxynucleotidyl transferase (TdT) in most cases of B- and T-LBL. The lymphoblasts in B-LBL are almost always positive for the B-cell markers CD19, CD22, cytoplasmic CD79a, and PAX5. The lymphoblasts in T-LBL are positive for the T-cell markers CD7, CD99, CD34, and CD1a. Almost all cases of B-LBL have cytogenetic abnormalities. T-LBL almost always has T-cell receptor gene rearrangements, commonly of α and δ loci.
Adult T-Cell Leukemia/Lymphoma
The disease is caused by the human T-cell leukemia virus type I (HTLV-I) and is endemic in southwestern Japan, the Caribbean basin, and Central Africa. Most patients have generalized disease with lymph node and peripheral blood involvement. Generalized lymphadenopathy, skin rash, leukocytosis, eosinophilia, and hypercalcemia are common in acute ATLL. Generalized lymphadenopathy without peripheral blood involvement is seen in the lymphomatous variant of ATLL.
The cytology shows neoplastic lymphocytes of intermediate to large size with marked nuclear irregularities, coarse chromatin, and distinct nucleoli. Giant cells with convoluted nuclei may be present.
The tumor cells express T-cell-associated antigens (CD2, CD3, and CD5) and lack CD7. The large cells may be CD30+, but are negative for ALK. The tumor cells frequently express CCR4 and FOXP3. Neoplastic cells have a clonal rearrangement of T-cell-receptor genes and monoclonal integration of HTLV-I.
Peripheral T-Cell Lymphoma
Peripheral T-cell lymphoma (PTCL) is rare and is especially common in African-American males in the sixth decade of life or older. Patients commonly have lymphadenopathy, extranodal (skin, GI tract, liver, spleen, bone marrow) involvement, and systemic symptoms. Pruritus, eosinophilia, and hemophagocytic syndrome may be present, but leukemia is uncommon.
The cytology shows small, intermediate, and large cells in various combinations resulting in a polymorphous pattern or may be monotonous when one cell pattern predominates. The small cell pattern is the least common. Cells exhibit clear cytoplasm, irregular nuclei, prominent nucleoli, and numerous mitoses. Clear cells and Reed–Sternberg-like cells may be seen. In addition, small lymphocytes, histiocytes, eosinophils, and plasma cells are present. Tight sarcoid-like granulomas can be seen.
The neoplastic cells express pan-T-cell and T-cell-associated antigens including CD2, CD3, CD5, CD7, CD43, and CD45RO. Most are CD4+ and express TCR αβ. Ki67 is usually high. T-cell-receptor genes are clonally rearranged in most cases.
Sézary Syndrome
Sézary syndrome is rare and occurs in adults, usually older than 60 years, and has a male predominance. It is an aggressive disease with an overall survival of 20 % at 5 years. Patients have erythroderma and generalized lymphadenopathy. Palmar and plantar hyperkeratosis and onychodystrophy may be present.
The neoplastic T cells are of small to intermediate size, have irregular “cerebriform” nuclei (Sézary cells), and are found in the skin, lymph nodes, and peripheral blood. The cells have moderate amounts of cytoplasm, and the nucleus may have a monocytoid appearance with one to three nucleoli. The smear background may show melanin-laden histiocytes as a manifestation of dermatopathic lymphadenopathy (Fig. 7.30).

Sezary syndrome. Monotonous population of intermediate-size lymphocytes with prominent nuclear irregularities in a background of dermatopathic lymphadenopathy is seen (Papanicolaou stain, high magnification) (Courtesy Dr. Javier Saenz de Santamaria, Badajoz, Spain. From Pambuccian and Bardales (2011). Reprinted with permission)
Tumor cells are CD2+, CD3+, TCRβ+, CD5+, and often CD4+. They express cutaneous lymphocyte antigen (CLA) and the skin-homing receptor CCR4 and have a T-cell-receptor gene rearrangement.
Anaplastic Large Cell Lymphoma
Anaplastic large cell lymphoma (ALCL) is a mature T-cell lymphoma that accounts for approximately 20 % of all T-cell lymphomas and occurs in young adults, but may occur in children. According to the presence or absence of ALK protein expression, it can be divided into the morphologically indistinguishable but clinically distinct ALK+ ALCL (50–80 % of cases) and ALK–ALCL. ALK+ ALCL involves both lymph nodes and extranodal sites (skin, musculoskeletal system, lungs, liver) of young, predominantly male patients, whereas ALK-ALCL tends to affect elderly patients. The response to treatment and the prognosis of patients with ALK+ ALCL are better than that for ALK– ALCL and other peripheral T-cell lymphomas.
ALCL has a number of morphologic variants or patterns, the common (or classic) (75 %), the lymphohistiocytic (10 %), and the small cell (5–10 %). The small cell variant is composed of neoplastic cells that are neither large nor anaplastic and may enter the differential diagnosis of small blue cell tumors and of lymphomas composed of intermediate-sized neoplastic cells.
Common to all morphologic variants of ALCL is the presence of “hallmark” cells, large or very large cells, with horseshoe-shaped or kidney-shaped nuclei, abundant clear or basophilic cytoplasm, and prominent perinuclear clear hofs, corresponding to the Golgi regions. Nucleoli are round or angular and prominent. The cytoplasm may show peripheral blebs and small vacuoles. A continuum of sizes of the abnormal cells can usually be seen. Other characteristic neoplastic cells include “half-doughnut cells,” “doughnut cells,” multinucleated giant “wreath cells,” “embryo cells,” “tennis racket” or “hand mirror” cells, and cells with polylobed nuclei and Reed–Sternberg-like cells. Frequent mitoses and apoptotic cells are present. Erythrophagocytosis or cell cannibalism, reactive lymphocytes, neutrophils, histiocytes, or eosinophils can occasionally be seen (Fig. 7.31).

Anaplastic large cell lymphoma. Large pleomorphic cell population is characteristic of this lymphoma (a). “Doughnut” cells also are some of the pleomorphic cells seen (b arrow head) (DiffQuik stain, high magnification) (a From Pambuccian and Bardales (2011). Reprinted with permission)
Immunohistochemistry is useful in the differentiation of ALCL from Hodgkin lymphoma and metastatic malignancies (Table 7.5). The large, pleomorphic neoplastic cells of ALCL are positive for CD30 in a membranous and Golgi pattern. The vast majority of cases express one or more T-cell markers (CD2, CD4, CD5), but CD3 is frequently lost. The neoplastic cells are consistently CD45 and EMA positive. The t(2;5) or t(1;2) translocation is present in 90 % of systemic cases.
Hodgkin Lymphoma (HL)
Hodgkin lymphoma accounts for 30 % of lymphomas, principally affects adolescents and young adults, and initially involves cervical and mediastinal lymph nodes. Lymph nodes are enlarged and usually non-tender, and patients are usually asymptomatic at diagnosis. The HL tends to spread to contiguous lymph node regions. Constitutional symptoms including fever, night sweats, and weight loss usually occur with widespread disease.
The REAL/WHO classification of HL includes:
-
1.
Nodular lymphocyte-predominant HL (NLPHL) – 5 % of all HL cases
-
2.
Classical Hodgkin lymphoma (cHL) – 95 % of all HL cases
-
(a)
Nodular sclerosis cHL – 65 to 70 % of all HL cases
-
(b)
Mixed-cellularity cHL – 20 % of all HL cases
-
(c)
Lymphocyte-rich cHL – 5 % of all HL cases
-
(d)
Lymphocyte-depleted cHL – 1 % of all HL cases
-
(a)
The neoplastic cells in HL are B cells that have lost most of their B-cell markers. The L&H cells of NLPHL are also named LP or popcorn cells; the mononuclear Hodgkin and multinucleated Reed–Sternberg cells of cHL are collectively called HRS cells. By polymerase chain reaction, it has been demonstrated that HRS cells have immunoglobulin gene rearrangements with somatic mutations that indicate their clonal origin in the germinal center. Likewise, the LP cells of NLPHL have cell rearrangements and mutations similar to those of HRS. However, the B-cell differentiation program is downregulated in HRS cells and fully active in LP cells. Thus, neoplastic cells have lost most B-cell markers in cHL and are preserved in NLPHL. The neoplastic cells of cHL are variably positive for EBV; however, no EBV positivity is found in NLPHL.
Treatment with radiation and chemotherapy results in a >85 % cure rate.
FNA findings. Smears show a background of reactive polymorphous lymphoid cells with predominance of small mature lymphocytes. The cellularity tends to be relatively low, and neoplastic cells are found scattered in the background. The cellularity is the lowest due to fibrosis in nodular sclerosis HL, the most common form of HL. The background also shows variable numbers of eosinophils, plasma cells, and even epithelioid cells to the point that such a finding in a lymph node aspirate should trigger the diligent search for neoplastic cells of HL. A granulomatous response is also seen in HL. These findings may also be present in lymphadenopathies secondary to allergic reactions and parasitic infestations. Occasionally, the background shows numerous neutrophils and simulates bacterial lymphadenitis. Of note, the syncytial variant of nodular sclerosis HL, particularly when present in the mediastinal lymph nodes, must be distinguished from metastatic carcinoma and primary mediastinal large B-cell lymphoma. Large cell T- and B-cell lymphomas, metastatic malignancies, especially melanoma and carcinoma or viral-driven lymphadenitis, should be included in the differential diagnosis.
The FNA diagnosis requires finding the neoplastic cells. Classic Reed–Sternberg cells usually have a moderate amount of pale cytoplasm with two or more eccentrically placed large, complex, or lobulated nuclei exhibiting irregular borders, coarse chromatin, and prominent irregular inclusion-like nucleoli. The mononuclear variants of neoplastic cells show similar nuclear features. Immunoblasts, commonly mistaken for the mononuclear variant, are smaller and show basophilic cytoplasm, a round nucleus, and a prominent but smooth round nucleolus (Fig. 7.32).

Hodgkin lymphoma. The smear shows a polymorphous population of lymphoid cells, rare eosinophils, and plasma cells. Present in this background are Reed-Sternberg cells, mononuclear variants, and multinucleated cells (a–c). Large, matted, and hypoechoic lymph nodes with well-defined margins are seen (d). The vascular pattern is exaggerated and chaotic (e) (a–c DiffQuik stain, high magnification)
Immunoprofile. Table 7.5 summarizes the markers that are useful in the differential diagnosis of HL.
Ultrasound Features of Lymph Nodes Involved by Lymphomas
Lymphomas commonly involve the levels I and V of the neck. Lymph nodes are usually round or oval, very hypoechoic reticulated/micronodular, and rarely necrotic and have sharp margins, and the hilum may be absent or present, usually with an exaggerated vascular pattern (Figs. 7.23c, d, 7.24c, d, 7.25b, c, 7.26b, c, 7.27b, c, and 7.32d, e).
Metastases
Lymph nodes are the most common sites of metastasis, and metastatic malignancies outnumber primary lymphoid malignancies in most lymph node locations. The topography of lymph node chains and their territories of lymphatic drainage are helpful clues for determining the primary site of malignancy and are covered early in this chapter. When possible, the original tumor should be reviewed for comparison of the cytomorphology. In the absence of a known primary malignancy, a metastatic deposit can be correctly classified only by the cytomorphology in many cases. However, poorly differentiated or undifferentiated malignancies, particularly of the small cell type (blue cell tumors), may be difficult to distinguish from each other and from lymphomas. Because distinction is important for management purposes, the use of immunostains is helpful in the diagnosis of carcinoma, lymphoma, melanoma, or other malignancies and can be done preferably in cell block preparations (Table 7.6). It must be noted that no antibody is organ specific and cross-reactivity with other tissues is being reported increasingly. Material from needle rinses may also be used for measurement of thyroglobulin and thyroglobulin antibody levels when differentiated thyroid carcinoma is suspected. Likewise, calcitonin levels in needle rinses are helpful when metastasis from medullary thyroid carcinoma is suspected.
The Table 7.7 summarizes metastatic malignancies by patterns, monotonous and pleomorphic, as an attempt to ease and narrow the differential diagnosis in lymph node aspirates.
Common Metastatic Malignancies in Adults
Metastatic Squamous Cell Carcinoma
This is the most common metastatic malignancy to the head and neck and frequently follows or presents with a primary tumor in the head and neck.
FNA findings. Well-differentiated squamous cell carcinoma shows high cellularity, with keratinized cells exhibiting pyknotic, minimally irregular, and slightly enlarged nuclei, with no mitotic activity (Fig. 7.33). The diagnosis is usually straightforward in these cases. Cystic squamous cell carcinoma shows scant cellularity, anucleated squamous cells, and scattered intermediate squamous cells with hyperchromatic and minimally irregular nuclei in a necrotic and variably inflamed background (Fig. 7.34). Necrosis and granulomatous foreign body-type reaction to the keratin may be seen.

Metastatic squamous carcinoma, well-differentiated. The smears show keratinization with anucleated squamous cells, foreign body type reaction with giant cells “engulfing” keratin flakes (a), and keratinized malignant cells showing cytophagocytosis with clearly malignant nuclear features (b). The US exam shows slightly hyperechoic lymph node with round shape, slightly lobulated borders, and heterogeneous echotexture (c). Minimal peripheral and central vascularity is seen by Doppler examination (d) (a, b MGG stain, high magnification)

Metastatic squamous carcinoma with cystic degeneration. The smears clearly malignant squamous cells with focal keratinization and a background of tissue damage (a, b). The US images show an irregular lymph node with cystic necrosis, ill-defined margins with focal extracapsular invasion (arrowheads), and no vascularity by Doppler exam (c, d) (a MGG stain high magnification; b Papanicolaou stain, high magnification)
The differential diagnosis includes cystic squamous cell carcinomas versus benign inflamed branchial cleft cysts and abscess. Malignant cells with anaplastic nuclei are important for diagnosis. Poorly differentiated squamous carcinomas may be difficult to differentiate from other high-grade neoplasms. Cell block material is useful to perform special stains such as p16, which is a subrogate for HPV-driven squamous carcinomas of the head and neck (Fig. 7.35).

Metastatic squamous carcinoma, poorly differentiated. The smear shows complex aggregates with spiculated ends and no evidence of keratinization (a). The cell block shows scattered aggregates of malignant squamous cells (b). Immunostain or p16 is positive (c). The US exam shows a hypoechoic lymph node with fuzzy margins, extracapsular invasion (arrowheads), and no vascularization by Doppler exam (d, e) (a MGG stain high magnification; b H-E stain, medium magnification; c immunostain for p16, medium magnification)
Metastatic Nasopharyngeal Carcinoma
This is particularly prevalent among the Asian ethnic group, is associated with Epstein–Barr virus infection, and has a bimodal age presentation with one peak between 15 and 25 years and the other between 60 and 70 years. Involvement of level II and III neck lymph nodes are frequent and is the first evidence of the tumor in 90 % of cases. Histologic types include keratinizing, nonkeratinizing, and undifferentiated.
FNA findings. The smears are cellular. The nonkeratinizing type shows numerous tridimensional aggregates and single round or elongated cells with scant cytoplasm, large nuclei, and prominent nucleoli. The undifferentiated type shows single and aggregated basaloid cells and small lymphocytes within the cell aggregates and in the background. Mitosis and necrosis are common (Fig. 7.36). Tumors with similar histomorphology can arise in the palatine and lingual tonsils, thymus, and larynx.

Metastatic nasopharyngeal carcinoma. Non-keratinizing poorly-differentiated carcinoma with spindle cell features admixed with lymphocytes (a, b). US features are not specific and include hypoechoic coalescent lymph nodes with sharp and irregular margins, and minimal vascularity by Doppler exam (c, d) (a DiffQuik stain high magnification; b Papanicolaou stain high magnification)
The differential diagnosis includes large cell lymphoma, carcinomas, and germ cell tumors. Immunocytochemistry for keratin, leukocyte common antigen, alpha-fetoprotein, and β-chorionic gonadotropin is helpful. The neoplastic cells are positive for EBV-associated markers such as EBV-latent membrane protein type 1 and in situ hybridization for EBV small-encoded RNA (EBER).
Metastatic Papillary Thyroid Carcinoma
US is useful in the preoperative evaluation and postsurgical follow-up of patients with well-differentiated thyroid carcinoma, in particular for evaluation of lymphadenopathy in the central and lateral neck compartments. Also, in cases of elevated serum thyroglobulin in post-thyroidectomy patients with thyroid carcinoma, US is used for evaluation of neck lymph nodes and thyroid bed nodules followed by USG-FNA, looking for thyroid carcinoma. Needle rinses looking for thyroglobulin and thyroglobulin antibody levels complement the cytologic evaluation in these cases. Secondary cystic changes are common in both primary and metastatic papillary carcinomas.
FNA findings. Solid lymph node metastases from papillary carcinoma show diagnostic features sufficient for a diagnosis. Aspirates from cystic metastasis show small sheets of monolayered epithelium in a hemorrhagic cystic background; cytoplasmic septate vacuoles and macrophages are often seen, and other cytologic characteristics may be inconspicuous (Fig. 7.37).

Metastatic papillary thyroid carcinoma with cystic degeneration. Metaplastic cells with intranuclear cytoplasmic invaginations (arrows), numerous macrophages, and rare sheets of cells with pale chromatin, nuclear grooves, and intranuclear cytoplasmic invaginations (a, b). US exam shows an oddly-shaped angulated lymph node with marked hypoechogenicity and no vascularity by Doppler exam (c, d) (a MGG stain, high magnification; b Papanicolaou stain, high magnification)
The differential diagnosis includes medullary carcinoma that may exhibit a pseudo-papillary pattern, as well as intranuclear inclusions and nuclear grooves which may be erroneously interpreted as features of papillary carcinoma. Furthermore, amyloid may be mistaken for colloid. Measurements of thyroglobulin and thyroglobulin antibody levels and calcitonin levels in needle rinses are helpful.
Metastatic Breast Carcinoma
The single most important predictor of clinical outcome is the sentinel lymph node, which is the ipsilateral axillary lymph node closest to the breast cancer tumor and likely to be the first to harbor a metastatic deposit. Touch preparation cytology evaluation of a sentinel lymph node is the preferred technique. Alternatively, sampling by means of FNA can be done pre- or intraoperatively at the time of lumpectomy. If the sentinel lymph node is positive, the patient undergoes axillary lymph node dissection. Skip metastasis involving axillary lymph nodes other than the sentinel lymph node occurs in 5 % of cases (Fig. 7.38).

Metastatic breast carcinoma. Neck level I LN. Aggregates of malignant cells with thin cytoplasm, ill-defined cytoplasmic borders, round nucleus and prominent nucleoli are seen (a, b). Comparison with the cytomorphology of the primary tumor is necessary for an accurate diagnosis. The US exam shows a lymph node with ill-defined and spiculated borders, and poor vascularization by Doppler exam (c, d) (a MGG stain high magnification; b Papanicolaou stain, high magnification)
Metastatic Melanoma
If the thickness of a cutaneous melanoma exceeds 0.76 mm, the risk of lymph node metastasis increases in parallel to the tumor thickness. The regional (sentinel) lymph nodes are involved before the melanoma spreads more distally. However, approximately 4 % of melanomas show axillary, cervical, and inguinal lymph node metastases in the absence of a known primary site (spontaneous regression).
FNA findings. The diagnosis is facilitated by the clinical history and the demonstration of melanin pigment in tumor cells or histiocytes (melanophages), but melanin may be entirely absent, and a history of melanoma may not be available. Aspirates are usually cellular, containing round or oval, spindle-shaped, and pleomorphic cells in various proportions. This pleomorphic pattern is characteristic of metastatic melanoma; however, anaplastic nuclei, prominent nucleoli, intranuclear cytoplasmic invaginations, and melanin pigment may not be present in all cell types (Fig. 7.39). Melanoma may mimic the cytomorphology of any neoplasm, including large cell lymphoma, although metastatic melanoma cells are usually larger and more pleomorphic. The rare amelanotic melanoma with lymphocyte-like or plasmacytoid-like cytomorphology may also resemble lymphoma or plasmacytoma; however, the smear background lacks lymphoglandular bodies. The spindle cell type must be distinguished from spindle cell neoplasms (Fig. 7.40). In equivocal cases, stains for S-100 protein, melan-A, and HMB-45 are helpful. Of note, the S-100 protein stain is also positive in the interdigitating reticulum cells of the lymph node.

Metastatic pigmented melanoma. Markedly pleomorphic cells with cytoplasmic brown melanin pigment, prominent nucleoli, and rare large cells with intranuclear cytoplasmic invaginations (a–c). US evaluation shows large round lymph nodes, focal fuzzy margins, extracapsular invasion (arrowhead), and moderate but abnormal vascularity (d, e) (a MGG stain, high magnification; b, c Papanicolaou stain, high magnification)

Metastatic amelanotic melanoma, spindle cell type. Elongated cells with pleomorphic nuclei, prominent nucleoli, and lack of melanin pigment (a, b). US show slightly hypoechoic lymph nodes with ill-defined margins, areas of extranodal invasion (arrowheads), and abnormal vascularity on Doppler examination (c, d) (a, b Papanicolaou stain, moderate and high magnification)
Metastatic Merkel Cell Carcinoma
Merkel cell carcinoma is a rare primary neuroendocrine tumor of the skin which occurs particularly in the head and upper extremities of elderly individuals. This tumor is aggressive and may produce multiple distant metastases, including the lymph nodes.
FNA findings. Aspirates are cellular, composed of intermediate-sized cells with a variable degree of cohesiveness. Cells have uniform round or oval nuclei with fine chromatin and small nucleoli. The cytoplasm is scant and fragile. Cell molding is not a feature. Scattered mitoses and apoptotic nuclei are present, and the background lacks lymphoglandular bodies. The most characteristic feature is the presence of an inconspicuous small spherical perinuclear cytoplasmic aggregate (“button”) of intermediate filaments (keratin). The cells show a positive immunostain for low-molecular-weight keratin, neurofilaments, and NSE. The keratin stain highlights the cytoplasmic condensation (Fig. 7.41).

Metastatic Merkel cell carcinoma. Complex aggregates of intermediate size cells with scan cytoplasm, granular coarse chromatin, and paranuclear dense cytoplasmic round aggregates of intermediate filaments or “buttons” (a, b arrowheads) highlighted by the keratin immunocytochemical stain (c). The US features are not specific and include oval shape hypoechoic lymph node with well-defined margins (d arrow) (a Papanicolaou stain high magnification; b DiffQuik stain high magnification; c immunocytochemical stain for keratin, high magnification)
The differential diagnosis includes small cell carcinoma of salivary gland or lung origin, lymphoma, and solid adenoid cystic carcinoma. The presence of “buttons” and small perinuclear clear zones is important for diagnosing Merkel cell carcinoma. In some cases, the use of special stains is necessary. The demonstration of the Merkel cell polyomavirus is diagnostic.
Metastatic Mesenchymal Malignancies
Lymph node metastases from sarcomas are unusual; however, when they occur, they may mimic carcinomas or lymphomas of Hodgkin or non-Hodgkin type, including anaplastic large cell lymphoma (ALCL) due to the presence of pleomorphic single cells or loose clusters in a lymphoid background. Of the metastatic mesenchymal neoplasms, the most likely to be confused with such entities are metastatic high-grade undifferentiated sarcomas (malignant fibrous histiocytomas), metastatic rhabdomyosarcomas, and metastatic neuroblastomas. Metastatic neuroblastoma may show a spectrum of neuroblastic to ganglion cell differentiation, with large, frequently multinucleated ganglion-like cells which may mimic Hodgkin/Reed–Sternberg cells or ALCL cells. The identification of neutrophil-like material in the background is diagnostically useful. The correct diagnosis is made by clinical correlation and immunostains (desmin and myogenin in rhabdomyosarcoma and NSE in neuroblastoma).
The Virchow’s Lymph Node
The supraclavicular lymph nodes are the most likely site to harbor cancer. Left supraclavicular lymphadenopathy is usually an ominous sign of disseminated disease from a primary site below the diaphragm, including but not restricted to the stomach, prostate, ovary, colon, biliary tract, pancreas, and uterus (Fig. 7.42). It may be the first evidence of disease in patients with prostatic adenocarcinoma.

Virchow’s node. Metastatic anaplastic-type carcinoma showing marked cell pleomorphism (a, b). The US evaluation shows a taller than wide hypoechoic lymph node with microcalcifications, fuzzy margins (c), and abnormal vascularity by Doppler examination (d) (a, b MGG stain, high magnification)
Ultrasound Features of Lymph Nodes Involved by Metastases
Lymph nodes affected by metastases are usually in the territory of lymphatic drainage of the primary tumor, unless in a widely metastatic process. In squamous cell carcinoma, the metastatic lymph node may be as small as 0.5 cm. Lymph nodes often have the following characteristics: round (AP/T axis >0.5 in the transverse view), usually hypoechoic, absent hilum, eccentric cortical hypertrophy, partial or total cystic necrosis, sharp margins, and abnormal peripheral vascularization. The lymph node may be hyperechoic with microcalcifications in metastatic papillary medullary, and anaplastic thyroid carcinoma and ovarian serous papillary carcinoma. The lymph node margins are ill defined and spiculated when there is lymph node extracapsular spread.
Suggested Reading
Cook JR. Nodal and leukemic small B-cell neoplasms. Mod Pathol. 2013;26 Suppl 1:S15–28.
Ioachim HL, Medeiros LJ. Ioachim’s lymph node pathology. Philadelphia: Lippincott Wlliams and Wilkins; 2009.
Pambuccian SE, Bardales RH. Lymph node cytopathology. Philadelphia: Springer; 2011.
Rhys R. Cervical lymph nodes. In: Allan PL, Baxter GM, Weston MJ, editors. Clinical ultrasound, vol. 2. London: Churchill Livingstone Elsevier; 2011. p. 920–37.
Said JW. Aggressive B-cell lymphomas: how many categories do we need? Mod Pathol. 2013;26 Suppl 1:S42–56.
Skoog L, Tani E. FNA cytology in the diagnosis of lymphoma. Basel: Karger; 2009.
Swerdlow SH, Campo E, et al. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC WHO; 2008.
Twist CJ, Link MP. Assessment of lymphadenopathy in children. Pediatr Clin North Am. 2002;49(5):1009–25.
Weiss LM, O’Malley D. Benign lymphadenopathies. Mod Pathol. 2013;26 Suppl 1:S88–96.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Bardales, R.H. (2014). The Lymph Nodes. In: Bardales, R. (eds) The Invasive Cytopathologist. Essentials in Cytopathology, vol 16. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0730-4_7
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0730-4_7
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0729-8
Online ISBN: 978-1-4939-0730-4
eBook Packages: MedicineMedicine (R0)