
Abstract
The human genome was once thought to be a redundant sequence containing few functional regions coding for proteins. This teaching is being rewritten as we continue to understand the vast complexity of the noncoding regions of the genetic code. These regions we now understand are transcribed into small single-stranded segments or microRNAs (miRNAs) that participate in the regulation of gene expression. miRNAs interact across many pathways and thus have the potential as targets for oncologic therapies. Their efficacy is limited because methods to traverse the many biologic barriers are yet to be developed. In order to achieve effective therapeutic levels at the site of interest, the tumor, the miRNA must be shuttled to the site and simultaneously be protected from the body’s defensive mechanisms. To this end, scientists have developed many vehicles for delivery at both the micro- and nanoscale using both synthetic and biologically derived vectors. Viral vectors continue to be the most commonly used vehicles, but are plagued by complications related to the vector itself. These inadequacies led researchers to explore synthetic materials such aspolylactic co-glycolic-acid (PLGA), silicon, gold, and liposomes to overcome the biobarriers of our body. While these vehicles have shown promise, problems such as high clearance rates, poor tumor accumulation and targeting, and adverse reactions have limited their translation into the clinic. In order to overcome these problems, a multistage theory was developed. By decoupling the tasks required of the carrier system, the multistage delivery system is able to simultaneously protect the payload, target the site of interest, and deliver the payload in therapeutic concentrations. This presents a paradigm shift in the concept of drug delivery and may provide the solution to the limited translational gene therapy in oncology.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
In the past, it was believed that the only functional product of any given gene was a protein, and that the noncoding sequences in the genome were nothing but remnants of evolutionary redundancy. This principle of the central dogma taught for years was revolutionized with the discovery of lin-4, a gene of the Caenorhabditis elegans larvae found in development that represses LIN-14 protein expression and thus developmental timing [1, 2]. The lin-4 gene does not encode a protein, but instead a pair of small RNA molecules with sequence complementarity to lin-14, and in fact represses its expression through RNA–RNA interaction [1].
The functionality of therapeutic RNAs is based on the catalytic process of naturally occurring 15–22-nt single-stranded RNA that couples with the cytoplasmic multiprotein complex RNA-inducing silencing complex (RISC) to pair with messenger RNAs (mRNAs) carrying complementary sequences to repress gene expression [3, 4]. The discovery of these small RNAs, later known as microRNA (miRNA) , by Victor Ambrose represented the first example of gene expression regulation by endogenously produced RNA molecules.
Since the discovery of lin-4, miRNAs have been identified in organisms ranging from plants to humans. It has been shown that up to 3 % of human genes encode for miRNAs and that up to 30 % of human protein-coding genes are regulated by miRNAs [5, 6]. The interconnectivity of the regulation of protein expression and miRNA regulation has yet to be fully elucidated. What is clear is the opportunity for miRNAs to be used as both diagnostic and therapeutic entities. The frequent aberrant expression and functional implication of miRNAs in human disease have elevated these molecules from the ranks of redundant cellular components to preferred drug targets [7–9]. With approximately 1,400 human miRNAs known to date, a new pool of therapeutic targets with a new mechanism has emerged [6]. Additionally, acting not only as targets, but also as agents themselves, miRNAs possess the capability to suppress a broad range of oncogenes and oncogenic pathways deregulated in cancer [8]. As our view of cancer evolves as a heterogeneous disease process unable to be successfully treated by attacking a single gene or gene product, so does the therapeutic potential of miRNA as multifaceted multitarget agents capable of disabling systems rather than select cellular components [7, 10–12].
Because cancer genesis and progression involve the loss of endogenous regulatory controls of essential cellular processes, the treatment of malignancies is extremely challenging. Current chemotherapeutic regimens continue to rely on heavy dosing to overcome their low cancer specificity and poor penetration [13–15]. Immunotargeting strategies have aided tumor targeting, but they still fall short of being substantially efficacious across a wide range of tumor types and are often limited in their scope because of the specificity of their targets [16, 17]. Because they interact with multiple pathways and convergence points of tumor suppression, miRNAs are ideal candidates for delivery.
Several advancements in cancer treatment have been developed over the last century to control and eradicate the disease [18]. Currently, the leading treatments for cancer are surgery, chemotherapy, and radiotherapy [11, 19, 20]. Further innovations have been made over the years to overcome weaknesses and side effects that may arise with these treatments [21]. While many novel approaches to the noninvasive diagnosis and treatment of cancer have emerged, effective penetration of the tumor and specific cancer cell targeting remains an obstacle, resulting in multiple administrations of current therapeutics, and for prolonged periods. This could lead to renal, cardiac, hepatic, and neurologic toxicities.
To overcome these disadvantages and enable a greater efficacy of treatment, novel drug delivery systems have emerged as prospective vehicles to carry and deliver the therapeutic payload. Vectors derived from natural and synthetic materials have been used to deliver oligonucleotide fragments with inhibitory and restorative functions to cancer cells in hopes of achieving greater therapeutic efficacy than the currently commercially available drugs, which are fraught with side effects and shortcomings.
2 MicroRNA as Pharmaceutical Agents
2.1 MicroRNA Characteristics, Comparisons, and Biogenesis
The discovery and characterization of several classes of small (~ 20–30 nt), noncoding RNAs during the last decade changed the field of molecular biology. This family of RNA is capable of regulating gene expression and can be classified into three main categories: miRNAs , short-interfering RNAs (siRNAs), and piwi-interacting RNAs (piRNAs). The piRNAs are single strands found mainly in animals; they act primarily in the germline and will not be discussed [22, 23]. In contrast, siRNAs and miRNAs show similarities with regard to structure, biogenesis, and repression of translation. However, it is the diminutive differences between siRNAs and miRNAs that point to disparities in function and therapeutic potential.
Both siRNAs and miRNAs are ~ 21–23 nt long, have double-stranded precursors (double-stranded RNA, dsRNA) of a guide strand (miRNA strand) and passenger strand (miRNA* strand) [22, 24]. These precursors undergo extensive splicing and refinement via their respective RISC before interacting with target mRNA [22, 25]. Both classes’ biogenesis is utterly dependent upon two protein families composed of specific domains: dicer enzymes (PAZ, 0–2 dsRNA-binding domains (dsRBDs), and tandem RNase III domains) to separate them from their precursors, and Argonaut (Ago) proteins (PAZ, PIWI, N-terminal (N), and middle (Mid) domains) that are central to the RISC and allow the complex unwinding, base pairing, and cleavage described later (Fig. 19.1) [22, 26–28]. Additionally, both classes have highly reprogrammable silencing effects due to predictable Watson–Crick base pairing recognition of gene targets, and both can dynamically redirect such silencing depending on changing genomic demands (miRNA) or threats (siRNA) [22, 29–31]. Both siRNAs and miRNAs have nuclear and cytoplasmic phases of refinement, but they preferentially exist/function in the cytoplasm, lose their aforementioned passenger strand during unwinding in the RISC, and can act by direct nucleolytic degradation, histone methylation, or heterochromatin formation [22, 25, 26, 28, 30, 32–36]. These two classes do, however, have notable differences.

Schematic of miRNA processing in the cell cytoplasm. As the primary mRNA transcript is shuttled from the nucleus to the cytoplasm, it associates with the DCR complex, where the double strand is extensively spliced. Following splicing and refinement, the precursors then associate with the RISC complex before interacting with their target mRNA. (Reproduced from [28] with permission from Nature Publishing Group)
Differentiation of miRNAs/siRNAs has classically and simply been based on their origin and precursor characteristics. The sources of siRNAs are extensive, but the majority are exogenous linear, base-paired dsRNA like viruses, transgenes, transposons, etc. that are either directly introduced into the cytoplasm or actively taken into the cell as an endosome from the environment and are thought to function as guardians of genomic integrity [22, 24, 37, 38]. This was classically viewed in stark contrast to miRNAs —perceived as intentional, endogenous products of a host genome in response to an inherent genomic need, and far more conserved across related organisms [3]. However, recent evidence shows that endogenous siRNAs can be derived from hairpin RNAs, centromeres/telomeres, naturally occurring sense–antisense pairs like convergent mRNA transcripts or pseudogene antisense/mRNA sense transcript duplexes [22, 37, 39, 40]. While siRNAs are cleaved from long, complementary dsRNAs, miRNAs are refined from incomplete dsRNA primary miRNAs (pri-miRNA) in what is called a “stem loop” with important flanking segments [3, 22, 23]. Additional differences have been discovered in the structure, processing, and mechanisms of repression by siRNAs and miRNAs.
A central difference between most siRNAs and miRNAs is the exactness of their 3′ and 5′ ends, as miRNA duplexes have very precise ends, with siRNAs showing much greater variability [3, 22]. It is this feature that is believed to afford miRNA its enhanced target specificity despite often imperfect central base pairing. Conversely, siRNA typically depends on perfect substrate complementarity for silencing, but may still function in the face of mismatches in an miRNA-like manner, despite suppressed endonucleolytic cleavage activity [22, 25, 26, 37, 40]. Often, siRNAs undergo amplification, with secondary siRNA generation via RNA-dependent RNA polymerase (RdRP) enzymes, causing a sustained response [22, 28]. This has been studied most extensively in other eukaryotes. miRNAs are unique in the fact that they may arise from either a dedicated transcription unit or one that makes several products, they may be cotranscribed with a protein within an intron, and they exhibit combinatorial regulation—target specificity across a variable number of mRNAs and the sharing of a common mRNA target by several different miRNAs [22, 33, 41, 42]. The broad possible effect on multiple cellular pathways allowed by miRNA is quite different than the target specificity required for RNA interference (RNAi) by siRNA. Finally, miRNA–RISC (miRISC) complexes require additional proteins like GW182 for silencing activity and are believed to repress genes by additional mechanisms to the canonical cleavage and nuclease degradation preferred by siRNA, such as deadenylation/decapping, inhibition of mRNA circularization, and premature ribosomal dissociation [25, 31, 36, 43, 44].
2.2 Mechanisms of Silencing
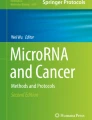
Although the steps and machinery required for miRNA biogenesis and refinement have been well characterized, more robust theoretical debate has surrounded its functional mechanisms of genomic silencing. We know that a pri-miRNA first travels to the nucleus for a critically precise cleavage of its stem loop from surrounding RNA by an RNase III/dsRBD complex (Droscha/DGCR8 in mammals) before travelling to the cytoplasm, where the Dicer enzyme separates the terminal loop from its pre-miRNA stem, making a duplex of mature miRNA that is ~ 22 bp in length [3, 22, 45, 46]. This miRNA is quickly unwound when assembled with Ago and associated proteins in the miRISC, which guide it to mRNA targets with variable complementarity, so they may be silenced and/or degraded [31, 47]. Protein expression is repressed by miRNA through degradation and decay, inhibition of translation initiation, inhibition of translation elongation, and translation abruption via ribosomal dissociation (Fig. 19.2) [28, 31, 48].

Mechanisms of miRNA silencing. Silencing by miRNA can occur through several mechanisms at different points throughout the protein translation phase. Posttranslational inhibition of protein elongation or posttranslational protein degradation may be affected (a, b). Interference with the formation of the ribosomal translational unit will inhibit translation (c, d). Pretranslation modifications, such as deadenylation or decapping, will prevent proper translational processing and result in early degradation (e, f). (Reproduced from [31] with permission from Elsevier)
Target mRNAs with exact complementarity to the guide miRNA strand can undergo Ago-catalyzed cleavage/degradation, while those containing centrally located mismatches have their translation repressed by another mechanism. These mismatched targets may be sequestered for decay within cytoplasmic P bodies—containing Argonaut proteins, GW182, deadenylase complexes, decapping machinery, and an RNA helicase [30, 31, 49, 50]. Recent evidence suggests that such a destabilization of mRNA target transcripts accounts for a greater percentage of the diminished protein production observed [51, 52]. Studies have shown that miRNA can halt translation before it begins initiation by binding the essential cap-binding protein eIF4E to central phenylalanine residues on Argonaut, or competitive inhibition at the methylated cap structure [31, 53]. Finally, miRNA is believed to inhibit early translation by the binding of eIF4E, subunit recruitment, causing their early dissociation, as well as interfering with translation elongation [22, 31, 48]. Until recently, the timing and contribution of these mechanisms were unknown. Ribosomal and initiation effects are now confirmed to occur early before decay, while translational repression is the primary mechanism observed on new targets and confirmed to occur prior to deadenylation or decapping causes of degradation, which are prominent mechanisms at steady state [48, 50, 54–56].
2.3 Dysregulation of miRNA in Cancer and Its Potential Clinical Implications
Given their ability to affect protein production at the genomic level, it is not surprising that miRNAs play significant roles in nearly every cellular process from development through apoptotic death. Indeed, several in vitro and in vivo studies have proved this to be true, demonstrating key regulatory roles for miRNA in: embryological development, stem cell proliferation and differentiation, organogenesis, metabolism, apoptosis, angiogenesis, muscular, neuronal and immune cell development and function, and more [3, 47, 57–60]. Such intertwining of miRNA and normal cellular function thus makes their dysregulation a prime suspect in the genesis of both benign and malignant diseases. Experimental evidence has confirmed this suspicion and generated useful databases, revealing links between miRNA dysfunction and many benign diseases, from cardiovascular disease to myasthenia gravis, and from Tourette syndrome to scleroderma [61–66]. Likewise, altered miRNA expression in human cancer is the rule rather than the exception.
Numerous associations exist between various cancer subtypes and specific miRNA aberrances, and we now know the potential of miRNA to serve as an early biomarker of disease and predict cancer stage, outcomes, and predilection for metastasis. Genomic mapping and miRNA profiling have generated expression signatures (miRNome) of many cancer tissue types and validated the presence of several miRNAs in chromosomal loci with known cancer-associated abnormalities. These include oncogene/tumor suppressor networks that harbor fragile sites, mutations, or deletions as exemplified by miR-15a and miR-16-1 in chronic lymphocytic leukemia (CLL), single nucleotide polymorphisms (SNPs) as seen in lung cancer, changes in promoter site transcription factor activity as seen with miR-34 and p53, or amplifications [67–71]. Key miRNAs in the structure of such networks were first coined “oncomirs” in 2005, and their expression profiles parallel respective cancer pathophysiological features, while serving as attractive potential targets of directed anticancer therapy [72, 73]. These oncomirs reciprocally modulate oncogenes or tumor suppressor genes by way of amplification or deletion/repression, respectively, to affect oncogenesis [74–76]. Introducing or repressing a single miRNA has proven sufficient for oncogenesis, best shown by miR-155 [68, 77, 78].
Altered methylation is well documented in human cancer and serves as its best epigenetic marker. The discovery of global hypomethylation compared to normal tissues was followed by observations of tumor suppressor gene inactivation via hypermethylation of promoter cytosines preceding guanines (CpG) islands, which we now know occur as “hypermethylome” profiles that are specific to cancer types and may enhance diagnosis, prognosis, and following treatment response [79–83]. Likewise, over half of the miRNAs are linked with CpG islands, and dysregulated miRNA expression in cancer is often plagued by epigenetic changes in either methylation or histone deacetylation (HDAC) and defects in miRNA biogenesis machinery (e.g., Drosha, Dicer, DCGR8, Lin-28) [84–87]. Examples include hypermethylated (downregulated) tumor suppressor miRNAs (TS-miRNAs), like miR-9-1 in breast cancer, miR-34b/c in colon cancer, and miR-127 in several cancers including both those of the breast and colon, as well as conversely hypomethylated oncogenic miRNAs (oncomiRNAs) like miR-21 in ovarian cancer [68, 70, 86, 88–90]. Since methylation and histone alterations are reversible events, further targeting the existing armament of demethylating agents and HDAC inhibitors to restore endogenous miRNA function represents an interesting potential shift in future cancer chemotherapy.
The oncogenic or tumor suppressive ability of several miRNAs has been clearly elucidated, and specific miRNAs are connected to essential cellular hallmarks of cancer (Fig. 19.3), thus establishing the need for these small entities as central substrates in our knowledge pursuit and therapeutic goals within the cancer paradigm going forward. The original TS-miRNAs described were members of the let-7 family, found to be modulated by p53 and downregulated in many cancer types with compromised interactions with several putative targets (MYC, RAS, HMGA2, FOS) [84, 87, 91]. The archetypal oncomiRNA is represented by miRNA-17-92 cluster, nicknamed “oncomiR-1.” This oncomiR is linked to several cancer types with putative targets, such as MYC, Bim, tsp-1, and phosphatase and tensin homolog (PTEN) [68, 71, 72, 85]. Several other oncomirs have subsequently been identified studied to provide “signatures” for human cancers (Tab. 19.1) [8]. Breast cancer is one of the best characterized for miRNA signatures [68, 73, 91–93]. A similar signature has also been developed for lung cancer [68, 73, 91, 92, 94, 95]. These targets show great promise for therapy and biomarkers for diagnosis, prognosis, treatment response, and predicting invasion/metastasis.

MicroRNAs involved in targeting the hallmarks of cancer. (Reproduced from [68] with permission from John Wiley and Sons Publishing Group)
The stability of miRNA in vitro, degree of conservation in vivo, and verified presence in circulating serum make it a good theoretical agent for diagnosis [91]. miRNA profiling has proven to be more accurate than mRNA in reliably classifying tissues of origin in both primary and metastatic tumors due to their similarly conserved miRNA expression, showing great potential for diagnosing the origin of metastasis of unknown primary origin [68, 96]. Many miRNAs have demonstrated links with cancer aggressiveness and outcomes as well. The first link was shown in 2005 between prognosis and progression of CLL and a unique 13-gene miRNA signature [97]. High miR-193a and low miR-191 levels are associated with shorter survival in melanomas [68, 98]. Additionally, it was later discovered that downregulation of miR-17-5p, -381, and let-7 and upregulation of miR-155 are predictive of poor prognosis/survival in lung cancer [99–101]. Certain miRNAs either promote (miR-10b and -21) or reduce (miR-200 family, -205) invasion and metastasis in breast cancer, and silencing miR-10b in mice successfully inhibits metastasis [68, 94, 102–104]. Both miR-126 and miR-335 suppress the “epithelial–mesenchymal transition” (EMT) necessary for metastasis in breast and lung cancer [92].
Even hormone receptor (ER) status and predictive response (PR) to hormone-based therapies in breast cancer can be predicted by miRNA. Various patterns of decreased miR-145/-125b and increased miR-21/-34/-155/-375 together can mirror tumor ER/PR expression, stage, proliferation index, or vascular invasion [73, 105–107]. Overexpression of miR-221/-222 is responsible for resistance to antiestrogenic therapies, while improved responsiveness to tyrosine kinase inhibitors via HER3 targeting is seen with ectopic expression of TSmiR-205 [108, 109]. These far-reaching and “awe-inspiring” data provide a wide base of validity and enumerable targets for pursuing novel miRNA-based cancer therapies or diagnostic modalities. However, as is often the case, the question looms just how far behind our technical ability trails our current knowledge base.
3 Mimicry vs. Antagonism
Theoretically, miRNA therapy represents a superior approach to multi-pathway disease such as cancer, since multiple genes can be affected by targeting a single miRNA. Given the nature of miRNA as a natural inhibitor of gene/protein production and function, it follows that there are two possible approaches for miRNA-based therapies: mimicry (replacement) or antagonism. At the phenotypic level of cellular machinery, these are experienced as loss or gain of function effects, respectively; and pertaining specifically to cancer, they represent repression of oncogene or restoration of tumor suppressor activity. Technically speaking, antagonists act upstream from the RISC outside of P bodies and mechanistically resemble siRNA or small-molecule inhibition, while mimicry is likened to traditional gene therapy and acts via miRNA replacement downstream of the RISC [7, 110]. The effect(s) of either mimics or antagonists can be followed by functional studies of their target genes and individual or genome-wide miRNA expression profiling [91].
miRNA mimics are either single- or double-stranded RNA molecules, which form a complex with RISC to suppress the target genes on the intended target of native miRNA. Double-stranded mimics are preferred due to 100–1000-fold greater potency as compared to single-stranded versions, as the passenger (miRNA*) strand may interact with either the mature miRNA or its precursor form [77, 111]. Although likened to gene therapy, miRNA mimicry has potential advantages due to its smaller size, ability for systemic administration, and the need for cytosolic entry for functional changes [77]. In addition, miRNA profiling of cancers indicated changes in miRNAs, suggesting their roles in oncogenesis. miRNAs could be tumor suppressors since their inhibition resulted in enhanced tumorigenesis. Since the miR mimics are identical to endogenous miRNA, the mimics should target the same mRNAs, making off-target cytotoxic cellular effects less likely. One mimic has been shown to modulate multiple oncogenic targets and pathways [9, 77, 112].
Evidence from animal studies has demonstrated the potential validity of miRNA replacement therapy. The miRNA let-7 suppresses RAS and is decreased in breast and non-small cell lung cancer (NSCLC), and replacement therapy with mimics in mouse models reduces existing tumor growth and stops proliferation of cancer cells [77, 84, 113–116]. Similar mimicry of miR-34a, a transcriptional target of p53 that is lost or repressed in most cancer types, showed inhibition of lung tumor growth in existing tumors with low miR-34a levels and protection from tumorigenesis in cells with normal levels, implying a protective role [7, 77, 117, 118]. Numerous other examples exist, including miR-16 and prostate cancer, miR-205 and breast cancer, and miR-26a and hepatocellular cancer [93, 119, 120].
Antagonists inhibit oncomiRNA that has acquired a gain of function. They are collectively known as anti-miR oligonucleotides (AMOs) and may take the form of anti-miRs, antagomiRs, or locked nucleic acids (LNAs) and are also useful in functional studies confirming miRNA target sites [121–123]. Similar to RNAi using siRNA, efficient antagonism depends on sufficient binding specificity for inhibition/degradation. The most common method uses antisense single-stranded oligonucleotides containing complementary, sugar/phosphate chemically modified backbone analogs (e.g., 2′-O-methyl, 2′NH2, phosphorothioates) with enhanced RNase protection and affinity for endogenous miRNA that sequester it from its RISC processing and promote degradation [7, 52, 121, 123]. Their length and composition can be fine-tuned for improved circulation time, cellular internalization, etc., and endogenous miRNA targets can act as biomarkers of efficacy and optimization [7]. “AntagomiRs” are analogs with a 3′ cholesterol moiety that were first coined in 2005 with evidence of their inhibition in mice [124]. Important antagomiR characterization has been done using antagomiR-16 and its target miR-122 in vivo in mice, demonstrating: dose and time dependency, a minimum length of 19 nt required for silencing, extensive target degradation that is “independent” of exonucleases, and interaction with miRNA in cytosol “outside” of P bodies [110]. AntagomiRs also display high sequence specificity with impaired silencing possible by only a single position-dependent mismatch [110]. AMOs are capable of downregulating the abundant miR-122 in the liver, which has two target sites within the hepatitis C viral (HCV) genome, and the first human clinical trial has been conducted using LNA anti-miR [68]. However, effective delivery is a main impediment to therapeutic mimicry/antagonism, with great potential for improvement.
4 Negotiating Biological Barriers in miRNA Delivery
The promise of in vitro efficacy of miRNA for cancers is dampened by the limitation to effectively deliver the miRNA to the site of interest [125–128]. The body’s natural protective barriers such as serum nucleases, vascular endothelium, interstitial and oncotic pressure, and the cell wall have made the targeting and treatment of tumor cells particularly challenging (Fig. 19.4) [128, 129]. The great obstacle in engineering therapeutics, though, is often not the synthesis and characterization of the agent, but rather overcoming the many biobarriers of the body without damaging the integrity of the payload, in this case miRNA. By understanding the critical barriers to overcome, one could exploit these mechanisms to develop solutions that preferentially direct the activity of therapeutic agents and sequentially negotiate those barriers for effective targeting and treatment. Because of these hurdles, the successful application of miRNAs as a cancer therapy has been limited [119, 130, 131].

The highly efficient biological barriers of the body present themselves as obstacles to the delivery of injected chemicals, biomolecules, nanoparticles, and any other therapeutic foreign agents from reaching their site of action. The barriers include the reticulo-–endothelial system, endothelial/epithelial membranes, complex networks of blood vessels, abnormal flow of blood, and interstitial pressure gradients (a). The tumor cells also pose additional barriers: cellular/nuclear membranes and ionic/molecular pumps that can expel drugs from the cancerous cells creating drug resistance (b). (Reproduced from [129] with permission from Nature Publishing Group)
The site of action of miRNA therapeutics occurs in the cytosol. The barriers to successful delivery of miRNA to the point of action in the cytosol or the nucleus are many and depend on the targeted organ and the route of administration. Locoregional administration of miRNA has fewer barriers compared to systemic delivery. For example, intranasal delivery of viral particles with let-7 miRNA in a Kras G1D/ + autochronous NSCLC mouse reduced tumor burden [115]. The efficacy of this delivery route was comparable to systemic delivery of let-7 in a neutral lipid emulsion in the same NSCLC model [132]. Many times this is not the case and one requires an understanding of the complex barriers to be able to achieve effective systemic delivery of miRNA.
4.1 Challenges: Serum Nucleases
The intravenous injection of miRNA poses significant challenges, beginning at the site of intravascular injection where the miRNA can be degraded. The first of many barriers encountered by delivered miRNA therapeutics are serum nucleases [133]. The major class of these nucleases includes 3′ exonuclease, although internucleotide cleavage of bonds has been reported [134]. Naked oligonucleotides can be degraded by serum nucleases. Modifications of miRNAs were attempted to protect them from systemic nucleases. These included the addition of adenosine or uracil residues to the 3′ end of the RNA [135–137]. In other methods, the delivery vehicles such as polymers have also been shown to protect the miRNAs. Endogenous miRNAs have been found intact in serum bound to RISC proteins such as Ago2 protein and within exosomes [138]. Thus, an understanding of endogenous protection could lead to a rational design of molecules capable of evading serum nuclease activity.
4.2 Biodistribution and Renal Clearance
In order to achieve an effective therapeutic index, a proposed agent must accumulate within the system or at the site of interest in sufficient amounts so as to have a therapeutic effect [139]. In the design of oligonucleotides administered as individual molecules or encapsulated within polymers, consideration must be given to the clearance mechanisms of the liver and kidney. The liver’s role in clearance is more prominent when the oligonucleotides are associated with nanoparticles [140] . Clearance by the kidney, on the other hand, has been demonstrated in nanoparticle and non-nanoparticle-based miRNA therapeutics [141]. Studies that characterized the clearance of antisense oligonucleotides were extensively reported during the 1990s [142–144]. Many of these studies were focused on protein-bound oligonucleotides or those with a phosphorothioate backbone. While protein bound, the main route of elimination was found to be in the urine, and the major organ of accumulation was found to be the kidney. Important features of oligonucleotide pharmacokinetics emerged from these studies. These include the following: (1) The biphasic plasma half-lives of oligonucleotides are in the range of minutes for the distributional phase and in the range of minutes to hours in the elimination phase. This indicates that without targeting or protection from nonspecific organ accumulation, miRNAs may be eliminated before any desired effect. (2) Oligonucleotides are accumulated in the liver and kidney but not the central nervous system. (3) In general, the information on the pharmacokinetic studies of phosphorothioate oligonucleotides in lower animal models such as rodents can be applicable to humans [145]. Animal models reported that the biodistribution of siRNA duplexes was similar to single-stranded antisense molecules, with highest uptake in kidney followed by liver [146, 147]. Interestingly, although found circulating in the blood bound to protein or within exosomic vesicles, these circulating miRNAs are not cleared by hemodialysis, suggesting these mechanisms as potential vehicles for effective protection of antisense oligonucleotides in the blood [148]. Clearly, uptake by the reticuloendothelial system (RES) plays a critical role in the delivery of miRNAs and other oligonucleotides. Further understanding the mechanisms that govern uptake into these RES-rich organs will allow us to design and deliver oligonucleotide carriers to achieve greater efficacy.
4.3 Clearance by the RES
In addition to circulating nucleases and renal clearance, a major barrier to effective in vivo delivery of antisense drugs is clearance by the RES [133]. Phagocytic cells, including circulating monocytes and tissue macrophages, whose physiological functions are to clear the body of foreign pathogens, remove cellular debris that is generated during tissue remodeling, and clear cells that have undergone apoptosis comprise the RES [149]. These cells, named Kupffer cells in the liver, or known simply as splenic macrophages, can detect and eliminate antisense oligonucleotides, such as miRNAs or siRNAs . Further, these same cells are capable of eliminating the nanoparticle carriers into which antisense drugs may be loaded [150]. This clearance may occur through various opsonization mechanisms including immunoglobulins, complement components, and other serum proteins.
Following administration, nanoparticles are detected by the immune system and tagged by proteins identifying them as foreign bodies and sequestering them for elimination. Several factors such as carrier surface charge, size, and surface characteristics may affect RES uptake [151, 152]. These characteristics have been used to target drug carriers to RES organs [153, 154]. Sites outside this system, though, continue to be elusive in their targeting. Immunoglobulin opsonization leads to Fc receptor activation and internalization characterized by cytoskeletal rearrangement, pseudopodia extension, and engulfment of the opsonized particle [155]. Complementopsonized particles are internalized by complement receptors such as CR1, CR3, and CR4, members of the integrin family of heterotrimeric membrane proteins. While CR1 is involved in particle binding to the macrophage membrane, CR3 and CR4 mediate internalization. Lastly, lipopolysaccharide (LPS) and modified lipoprotein opsonization not only targets particles, but also targets naked oligonucleotides. The scavenger receptors that recognize these ligands found in the liver and spleen are suggested to be responsible for the uptake of monomolecular oligonucleotides [156, 157].
4.4 Endothelial Barrier
The endothelial cells lining the vascular lumen present both a barrier and an opportunity for oligonucleotide-based therapeutics [133]. Endothelial cells line the vasculature, adhering tightly to the underlying extracellular matrix largely via integrins and forming junctions with each other via several types of cell–cell adhesion molecules, including vascular endothelial (VE)-cadherin, junctional adhesion molecule (JAM), occludins, claudins, and platelet endothelial cell adhesion molecule (PECAM) [158]. The integrity of the endothelial junctions is influenced by complex signal transduction processes that respond to a variety of mediators. For example, microvascular transport of macromolecules increases during inflammation [159]. This process, often driven by diffusion, is due to shifts in the concentration gradients between the inside and outside of the vessel wall. Transvascular fluid transport is driven by the difference in hydrostatic and osmotic pressures between the blood vessel and interstitial space. When delivering particulates, the upper size limit of diffusion is limited by the pore size of the capillary. In the case of inflammation, these pore sizes can increase, altering the normal gradients and allowing greater diffusion [160–162].
Angiogenesis is a known and widely accepted mechanism of tumor growth and survival. A mixture of heterogeneous precursor cells and preexisting normal vasculature makes up the new sprouting vessels [163]. The tumor blood vessels generated from aberrant mechanisms of tumor survival are structurally and architecturally different from the normal vasculature [164]. The combination of constitutively activated genes and heterogeneous cell populations develops abnormal vasculature marked by precocious capillary sprouting, convoluted and excessive vessel branching, distorted and enlarged vessels, erratic blood flow, microhemorrhaging, leakiness, and abnormal levels of endothelial cell proliferation and apoptosis [165]. Structurally, the dense vascular networks are not organized into venules, arterioles, and capillaries as seen in normal anatomy, but rather are a chaotic organization of loops and arcs that encircle clusters of cancer cells. Architecturally, the vessels themselves have an atypical basement membrane, a high percentage of hyperproliferative endothelial-like cells, and a decreased number of pericytes [166]. Directed by the cancer cells, the resulting vessels have large intercellular openings between the endothelial cells that are not present in normal continuous vasculature [167–169]. These fenestrations are known to range in size from 100 nm to 10 µm and are exploited in many nanomaterial-based therapies [170, 171]. Due to the leakiness of these vessels, the major pathway of drug transport across tumor microvasculature is by extravasation via diffusion and/or convection through the discontinuous endothelial junctions, whereas transcytosis plays a relatively minor role. This leakiness promotes not only drug carrier extravasation, but also protein transport, leading to high interstitial compartment pressures and reduced transvascular transport [169, 172].
4.5 Extracellular Matrix Compartment and Subcellular Distribution
The interstitial compartment of solid tumors is mainly composed of extracellular matrix proteins, interstitial fluid, and a random organization of poorly formed vessels. The distinguishing feature of the interstitium is the high pressure resulting from the lack of sufficient lymphatic drainage. The movement of small molecules in the interstitial space is governed by diffusion, while the movement of large molecules, such as drug carriers, is governed by convection [173]. While diffusion relies on diffusion coeffecients and concentration gradient, the convection depends on hydraulic conductivity and pressure difference. While the enhanced permeability and retention (EPR) effect allows the particles to accumulate to the tumor loci, it is the high interstitium pressure that allows extravasated particles to be pushed into the margin of the tumor [174, 175]. This characteristic presents an additional biobarrier to the penetration of therapeutic agents into the tumor core as the transport is governed by the physical properties (charge, pH, lipophilicity, size, structure) of the subcompartment and of the drug [173, 176]. This phenomenon of EPR within tumor stroma elucidated by Maeda et al. supports the use of silicon microparticles as drug carriers because of the passive accumulation in solid tumor after intravenous administration [139, 169, 177, 178].
4.6 Inefficient Endocytosis and Endosomal Release
The cellular subcompartment represents the final barrier to therapeutic delivery. Efficient endocytosis and endosomal release are required to bring the payload to the site of action in the cytosol. Mechanisms like phospholipid bilayer, lysozomal and endosomal degradation, and efflux glycoprotein channels are particularly crucial to intracellular delivery of agents as small interfering RNAs and miRNAs, where cytoplasmic delivery is critical and endogenous degradation pathways prevent that delivery. Targets such as the previously mentioned TP53 pathway, Ras/Raf pathway, and other various growth factor signal transduction pathways require this intracellular delivery.
The plasma membrane is a significant barrier for miRNA uptake [179]. Despite their small size, the charge and hydrophilicity of miRNA molecules prevent them from readily crossing the plasma membrane [180]. While complexing to nanoparticles or other delivery mechanism may target them to the cell itself, the entry of the system into the cell is critical for function. The integration of the payload into nanoparticles that are uptaking by cells may present an efficient of innovative mechanism for delivery.
The final barrier to effective targeting of miRNA is the release form the endosome [180]. Whether delivery by cationic lipids, nanoparticles, or cell-type-specific delivery reagents, the intracellular trafficking of miRNA begins in the early endosomal vesicles [180]. These early vesicles fuse with late endosomes with increasingly acidic environments until, ultimately, they fuse with the lysosome [181]. The lysosomal compartment is the most acidic environment and will lead to the degradation of any nucleic acids that may find themselves in that environment. The fate of the internalized molecules inside the fused vesicle depends on the specific type of bound receptors and includes the following: recycling back to the cell surface, degradation in lysosomes, or release into the cytosol to interact with other intracellular components [182–185]. The endosomal entrapment contributes to the low transfection efficacy of non-viral carriers and represents a final but significant hurdle to overcome in delivery. Various strategies such as liposomal delivery, hydrogen sponges, and cell-penetrating peptides have been developed to facilitate the release of oligonucleotides from the endosomal compartment in order to avoid lysosomal degradation [186–188].
5 Vehicles of Delivery
5.1 Non-Nanoparticle Therapeutic Delivery
Successfully delivering miRNA mimics or antagonists to the tissue of interest while preserving their structural integrity remains a principal challenge [189, 190]. Several technologies have proven effective in delivering miRNAs to tissues: vector based (adenoviral and lentiviral (let-7)), atelocollagen, liposomes , porous silica, gold, and polylactic co-glycolic-acid (PLGA). Development of clinically relevant miRNA formulations frequently involves a thorough evaluation of existing technologies to identify those that are amenable to miRNA and its chemistry. Although synthetic modifications provide some degree of protection from nucleases and promotion of necessary cellular internalization as stated above, naked RNAs in biological fluids rapidly undergo nuclease destruction. This fact limits many therapeutic RNAi platforms to local administration only, allowing a restricted number of amenable tissues and, often, only a fraction of diseased cells get adequate drug exposure. Systemic administration has many theoretical advantages, but besides nucleases, a horde of other in vivo barriers, from macrophages to renal clearance, impedes successful miRNA delivery (Tab. 19.2). Critical criteria in the evaluation process are: (1) sufficient delivery to induce a therapeutic effect and (2) a significant safety margin at therapeutic levels. Since the size and base chemical structure of miRNA are virtually identical to siRNA, many of the same therapeutic delivery platforms pioneered by siRNA-based RNAi show great promise for miRNA therapy. Methods of in vivo delivery have witnessed varied levels of success and side effects and are basically classified as either viral or non-viral, including but not limited to conjugated RNAs, viral vector-based systems, and liposomal or polymer-based systems (Fig. 19.5).

Current approaches to in vivo miRNA targeting. Because of the body’s multiple levels of biobarriers, researchers have investigated multiple animal models for delivery. miRNA targeting has evolved to include local injection, systemic, and intranasal delivery. (Reproduced from [68] with permission from John Wiley and Sons Publishing Group)
The degree of nuclease degradation limits naked dsRNA use to local injection in the eye, skin, or tumor, and even this local application has largely given way to newer conjugated or packaged iterations [191]. The cholesterol conjugation used with some AMOs is a simple mechanism to improve in vivo performance. Cholesterol enhances cell surface membrane receptor binding via associations with high-density (BI receptor) and low-density (LDL receptor) lipoproteins [191]. In addition to examples previously cited, such formulations are capable of inhibiting miRNA in liver, lung, kidney, heart, intestine, fat, skin, bone marrow, muscle, ovaries, and adrenal glands, albeit at high doses [110, 123, 124, 191]. Such need for higher doses may be secondary to the propensity for these molecules to be sequestered from the cytoplasm by phagolysosomes [191]. AMOs also have difficulty reaching targets beyond certain biological barriers, illustrated by antagomiR-16’s ability to specifically inhibit miR-16 in brain cortex when directly applied, but inability to reach these tissues via intravascular injection [124, 192].
5.2 Vector-Based Delivery: Lentiviruses and Adenoviruses
Vector-based therapies exhibit significant anti-cancer activity both locally and systemically. There are essentially two vectors for the delivery of genetic material: viral based and non-viral based. Because many of the constructs used to deliver miRNA have been viral based, we will focus on those vectors. Because viruses have evolved to develop machinery to enter the cell, deliver, and integrate genetic material, they are excellent candidates for a vehicle to deliver miRNA [193–195]. Several viruses have been explored to deliver genetic material: retroviruses or lentiviruses like human immunodeficiency virus 1 (HIV-1), adeno- and adeno-associated viral vectors , herpes simplex, and poxviruses to name a few. Viruses with miRNA activity can be used as mimics or antagonists, and miRNA transcripts can augment classic gene therapy. Currently, the most commonly used vector for transport of miRNA or other oligonucleotides are adeno-associated virus (AAV) vectors and lentiviral vectors.
Lentiviruses are members of the viral family Retroviridae (retroviruses) that are characterized by the use of viral reverse transcriptase and integrase to stably insert into the gene [196]. Lentiviruses replicate in nondividing cells and can lyse the host cell if there is excessive replication [197, 198]. Lentiviruses can show differences in genome structure, pathogenicity, and receptor usage, depending on the species [199–201]. In most cases, viral delivery of genes is based on HIV-1.
HIV is a single-stranded positive-sense RNA of approximately 9 kb [202]. The three main open reading frames encode the major structural machinery of the virus: gag, pol, env. The gag gene encodes viral core proteins. The pol gene encodes the enzyme required for viral replication and env encodes the viral surface glycoprotein gp160 [196, 197]. In addition, the Tat and Rev genes encode proteins that control viral transcription, splicing, and nuclear exports of viral transcripts. HIV-1 is effective with regard to delivering genetic material into cells as compared to its nurine leukemia virus counterpart (Fig. 19.6) [203]. The HIV-1 has since become a vehicle for therapeutic delivery of genes.

Viral vector antagonism. Schematic of a vector or virus to inhibit a miRNA. (a) The vector encodes multiple copies of perfectly complementary or bulged target sites (as shown) for a miRNA or miRNA family. The target sites are expressed at high levels by a strong RNA polymerase II or III promoter or by introducing a large number of vectors into a cell. (b) The target containing transcripts bind to the cognate miRNA, and because of excess target concentration saturate the miRNA. This limits the availability of the miRNA, and inhibits the regulation of its natural target mRNAs. The processing body (P body) is a region rich in enzymes involved in miRNA turnover. niRNP, niRNA ribonucleoprotein complex. Reproduced from [29] with permission from Nature Publishing Group.
As the complex molecular mechanisms of cancer continue to evolve, so do targets and therapies to treat cancer. miRNAs show promise for cancer therapy because they can target multi-pathways with the possibility of reduced toxicity [42, 204]. As discussed above, the mimic or antagomiR can easily be incorporated into virus for cellular delivery [124, 205–207]. Experimentally, lentiviral vector overexpressing miRNAs was shown to demonstrate loss of function of specific genes in a myelomoncytic cell line [208, 209]. Transgenes engineered to express miRNA-binding transcripts are called “miRNA sponges” or “decoys,” to compete with endogenous miRNAs [68, 191, 210]. The sponges can be inserted into chromosomes and then induced to be expressed (“miRZips”) [191]. The expression of miRNA in rats caused organ failure and death, indicating that toxicity could be confound in miRNA therapy [191, 211].
In addition to the potential of using lentiviral vector-based miRNA for cancer, there is potential for other pathologies, such as abdominal aortic aneurysms and hypercholesterolemia [205, 212, 213]. Lentiviral delivery of miR-33 in mice was shown to lower HDL by repression adenosine triphosphate-binding cassette (ABC) transporter, ABCA1 [213]. Systemic injection of a locked nucleic acid-modified antagomiR targeting miR-21 diminished the pro-proliferative impact of downregulated PTEN, leading to a marked increase in the size of AAA. Similar results were seen in mice with AAA augmented by nicotine and in human aortic tissue samples from patients undergoing surgical repair of AAA (with more pronounced effects observed in smokers) [205, 214, 215].
AAV vectors belong to the Parvoviridae family and are part of the Dependovirus genus. Twelve human serotypes (AAV serotype 1 (AAV-1) to AAV-12 have been reported in addition to the more than 100 serotypes from nonhuman primates [215–217]. The nonenveloped virus that packages a single-stranded DNA genome can only occur in the presence of another virus, such as adenovirus or herpesvirus [218]. In the absence of a helper virus, the AAV and specifically the serotype 2 can set up latency by integrating into the chromosome 19q13.4. This characteristic has made it the only mammalian DNA virus known to be capable of site-specific integration. Due to its lack of pathogenicity, its persistence, and availability of many serotypes, the translational potential of AAVs has soared for a variety of therapeutic applications [218].
Tumors are characterized by the global miRNA patterns [8, 89, 219, 220]. This presents a unique opportunity for therapeutic intervention that may span several tumor types at once, as many of the mechanisms that induce the tumorigenesis have commonalities in the miRNA patterns [221]. For example, therapeutic miRNA delivery of miR-26 through AAV in a murine model of liver tumorigenesis found a decrease in the proliferation of cancer, induced apoptosis with no evidence of toxicity [119]. Adenovirus-expressing miR-133 was shown to reduce cardiomegaly and intranasal administration of adenovirus-expressing let-7a reduced tumor formation in a K-ras mouse lung cancer model [130, 222].
Retroviruses and lentiviruses incorporate their DNA into the host genome without specificity, making insertional mutagenesis or oncogene activation serious theoretical off-target effects of gene therapy, in addition to their immunogenicity [68]. The method of using virus for gene delivery can be adopted for miRNA by incorporating the transcripts or target sites into the 3′ untranslated region (UTR) of vectors. This has been demonstrated in studies using oncolytic viruses and miR-122 in the liver, and miR-124 in neurons/glial cells [191, 223, 224].
The path for the successful use of viruses as vectors for gene therapy has been fraught with troubles, such as the death of a recipient in 1999 following the administration of high doses of adenovirus for gene therapy [225]. Since that unfortunate event, many advances and optimizations to the technology have occurred. But we must not forget that our interventions carry significant consequences and we must judge our therapies with intense scrutiny before we consider their translation into humans.
5.3 Polymer-Based Delivery
Polymer-based oligonucleotide and gene delivery are considered to be safer than viral-based mechanisms for gene silencing with reduced insertional mutagenesis and phenotoxicity [226–228]. The advent of polymers/copolymers and lipid-based platforms expanded horizons in the world of biotechnology and bioengineering due to their favorable plasticity. Applied to RNAi, they overcome inherent (naked) miRNA physicochemical deficiencies and present advantages of biocompatibility/degradability, easy tailoring of particle size, functional targeting ability, protection from nucleases, and release from endosomes.
The most widely studied/used polymer for RNAi is polyethyleneimine (PEI), but many others exist (e.g., PLGA, chitosan, gelatin) [229]. PEI is a polycation polymer capable of complexing with DNA and protecting nucleic acids from nuclease degradation. PEI polymers can be synthesized in the nanoscale allowing for cellular endocytosis and also allowing for pH-buffering capability [230]. The number of positive charges in the polymer and negative phosphate groups within the RNA determines the size and structure of the resulting complexes (termed “polyplexes” or “polymersomes”). The polyplexes act as a “proton sponge” to protect the RNA from degradation and to stimulate necessary endosomal rupture within the cytosol [229]. Decreased cancer cell proliferation and increased apoptosis have been achieved in vivo using atellocollagen/miR-34a and PEI/miR-145/-33a formulations, respectively [231, 232]. In other studies, combinations of the cationic effects of PEI with the biocompatibility and physicochemical properties of polyurethanes (PUs) formed a PU–PEI polymer complex to deliver miR145 to treat lung adenocarcinoma (LAC) [233]. MiR145 was also identified as a candidate for therapy for LAC-associated cancer stem cells (CSCs). Experimental studies with nude mice treated LAC with PU–PEI-miR145 in combination with radiotherapy and cisplatin and this resulted in maximal inhibition of tumor growth [234].
Other biodegradable polymers have been investigated to deliver miRNAs. PLGA seemed to be one of the most successful biodegradable polymers currently used in translational research (Fig. 19.7). PLGA is approved by the Federal Drug Administration (FDA) and the European Medicine Agency (EMA) for drug delivery [235] . One advantage of PLGA is the control attainable by altering the co-polymeric ratios to achieve long-term release [236]. PLGA, which is 50 % lactic acid and 50 % glycolic acid, is released when PLGA undergoes biodegradation. These monomers are quickly metabolized through the Krebs cycle resulting in minimal toxicity [237]. While extremely biocompatible, the hydrophobic residues on the surface as well as the nanoparticle size make PLGA particle targets for the RES. Cells in the RES organs sequester PLGA particles by opsonization, leading to payload loss. Surface modifications with other polymers such as polyethylene glycol (PEG) have led to increased circulating half-life by several orders of magnitude [238]. PLGA drug delivery has been used with antibiotics to treat infections, growth factors for tissue engineering applications, and polymeric stent coverage in cardiovascular disease [239–243].

Workflow schematic of alternative splicing and miRNA inhibition induced by non-arginine-coated nanoparticles (ARG-NPs) that deliver charge-neutral oligonucleotide analogs. ARG-NPs comprise a spherical PLGA core coated with PEGylated ARG. Dehydrated ARG-NPs were visualized by scanning electron microscopy (SEM), intracellular uptake of osmium tetroxide-loaded ARG-NPs was visualized by transmission electron microscopy (TEM); scale bars for SEM and TEM micrographs represent 1 µm. (Adapted with permission from [316]. Copyright 2013 American Chemical Society)
PLGA has also served as an effective delivery system for miRNA in cancer therapeutics. Because of its favorable biocompatibility and ability to be targeted, PLGA encapsulation of miRNA has shown great efficacy [244, 245]. AntagomiRs loaded in PLGA nanoparticles have been used to inhibit miR155 in a mouse model for lymphoma and showed slowing of pre-B cell tumors in vivo [245]. Because of the mechanism of internalization leading to endolysosomal compartment targeting, PLGA nanoparticles can be used to deliver miRNA to the regulatory proteins responsible for the ultimate action of miRNA in the cell [237, 246]. Gomes et al. have shown that PLGA can be used not only to deliver miR132 to endothelial and mononuclear cells, but also as a vehicle to carry perfluoro-1,5-crown ether (PFCE), a labeling compound used to track survival of cells [246]. Delivery of miR132 resulted in a threefold survival of endothelial cells transplanted in vivo and a 3.5-fold increase in blood perfusion in ischemic limbs following transplantation of miR132-treated endothelial cells. While PLGA delivery of miRNA and RNAi therapeutics is still early in development, the potential application and speed to translation are apparent given its previous success in the clinic.
5.4 Lipid-Based Delivery
Similar to PLGA, lipid-based carriers have been approved by the FDA for use in humans. There is a great diversity in the types of lipid-based carriers used for miRNA delivery. The most widely studied are exosomes [247–249]. These naturally occurring vesicles are derived from intracellular compartments and are released through fusion of the multi-vesicular endosomes with the plasma membrane [249]. These lipid-based carriers are capable of both transport and protection of the payload from the harsh extracellular environment [249]. Our understanding of exosomes has given us insight into the nature of intercellular miRNA communications and has led researchers to investigate other lipid-based vehicles for miRNA delivery, namely liposomes . Liposomes represent a major sector of nanomedicines and consist of spherical lipid vesicles 30–200 nm composed of lipid bilayers encapsulating hydrophilic chemotherapeutics, such as doxorubicin or danorubucin [250]. Doxil® and Myocet®DaunoXome® are three anthracycline-carrying anticancer liposome formulations approved by the FDA and have been used in clinics for more than a decade [251, 252]. The lipid bilayer of liposomal formulations permits avoidance of renal clearance and improved intracellular delivery. Examples abound as RNAi delivery vehicles, including PEGylated liposomes, lipoplexes, lipoids, and lipidoids [229, 253]. Liposomal carriers alter the biodistribution of the drug, increasing the circulation time and decreasing the cardiotoxicity commonly associated with chemotherapeutics [254, 255]. Micelles are spheres, roughly 20 nm in diameter, consisting of a single lipid or amphiphilic polymer layer, with a hydrophilic exterior and hydrophobic lumen (Fig. 19.8) [256]. Lipid- and polymer-based nanoparticles for systemic delivery of siRNAs have been developed and tested. While lipid-based delivery of miRNA is efficient, it tends to induce an inflammatory response. On the other hand, biodegradable polymers induce less inflammation, but deliver less efficiently and have shorter effects.

The evolution of liposomes. Simple liposomal vesicles are constructed of a lipid bilayer shell. a Liposomes can trap molecules (red sphere) up to a few nanometers in diameter within the hydrophobic region, while the hydrophilic region can trap molecules up to several hundred nanometers in size (green star). In order to negotiate biobarriers, “stealth” liposomes were constructed for drug delivery applications. (b) Polymers attached to the lipid bilayer can be modified with targeting moieties (blue rectangle) that enable specific cellular targeting. (c) Cationic liposomes, able to carry DNA (purple circles), are constructed in an onion-like fashion with the DNA sandwiches between the cationic membranes. (d) In the most recent evolution, the bilayer is assembled from cavitands where hydrophobic and hydrophilic chains can be attached. Within the cavitands angstrom-sized molecules (yellow diamond) can be trapped on the surface. This enables molecules of different sizes or configurations, such as miRNA, to be carried and protected. (Reproduced from [256] with permission from Nature Publishing Group)
Lipoplexes contain cationic lipids in their bilayer that interact with the negatively charged anionic nucleic acid molecules. The hydrophilicity of the nucleic acids is offset by the cationic lipids and a net positive charge results, which allows the liposomes to bind to anionic cell surface molecules [191]. These particles can be further modified to facilitate fusion with extra/intracellular membranes and foster endosomal release once inside the cell via attributes like a pH-sensitive lipid head group that causes endosomal membrane disruption, releasing the RNA payload. Such later-generation formulations have proven to be 100 times more effective than typical lipid-based carriers, requiring a fraction of the RNA for equal effect [191].
One study used a lung cancer model to compare the efficacy of a lipoplex/miR-133 formulation with a reputable transfection agent and found that the lipoplex application caused over a twofold increase in miR-133 expression, nearly a twofold difference in target protein downregulation, and a 50-fold greater accumulation in the target lung tissue without toxic effects [257]. Similar results were seen using a lipid-based tumor suppressor miR-34a formulation in a mouse model of lung cancer when administered locally or systemically [118]. Despite their safety and easy preparation, liposomal formulations have less tumor specificity and lower transfection efficiency than viral vector-based therapies, but the addition of surface ligands and/or nanotechnology hybridization can enhance this property greatly [258] . The Holy Grail in delivery of miRNA-based cancer therapy is a product capable of delicately negotiating the many biological barriers to efficiently deliver an RNAi payload with great tissue specificity, complete transfection, and no negative off-target effects on healthy tissue. A combination of today’s most advanced biotechnology, such as nanomedicine, and biocompatible lipid- or polymer-based carriers may just make this dream a reality.
5.5 Protein-Based Delivery
Nonlipid protein-based delivery mechanisms have also been used as drug delivery systems for oligonucleotides. Atelocollagen is a processed natural biomaterial produced from bovine type I collagen [259]. Because it is derived from naturally occurring collagen, it retains the characteristics of high biocompatibility and high biodegradability [260]. The mixture of atelocollagen and oligonucleotides results in complexes, 200 nm–10 μm [260]. Atelocollagen protects the nucleic material from serum nucleases, which is a major biological barrier known to degrade nucleic acids. [261]. Atelocollagen forms bonds with the nucleic acids in the miRNA or siRNA, where hydrogen bonds are formed between the phosphate groups of the oligonucleotides and the CH groups of the collagen (Fig. 19.9) [262]. By controlling the size as potentially adding targeting moieties to the atelocollagen itself, this system presents itself as an appealing and biologically inspired alternative to synthetic polymer nanoparticle delivery systems.

The molecular model of atelocollagen–siRNA complex. Hydrogen bonds arise between CH and phosphate groups. 1,3 phosphate groups are situated on the first chain of ds-siRNA and the other 2,4 phosphate groups (which are below the 1,3 phosphate groups) are situated on another chain. H-bonds are created between 1,3 ↔ 11,31 and 2,4 ↔ 21,41 groups 11,31,21,41 are CH groups of Gly and Pro amino acids situated on the triple helix of collagen and 21,41 CH groups are situated below of 11,31 CH groups (“hydrogen bonding without water molecules”). On the “hydrogen bonding with water molecules” are shown water-mediated intermolecular contacts between atelocollagen and siRNA which are restricted to the backbone phosphates and sugar 2′-OH groups (are shown hydrogen bonding between one layer of phosphate groups and CH groups of collagen). (Reproduced from [262] with permission from Elsevier)
Atelocollagen has found utility as a drug delivery system in both oncologic and tissue engineering applications [263–269] . As an oncologic drug delivery system, atelocollagen has proven effective in delivering miRNAs to target tissues. In one model of lung metastasis of osteosarcoma, Osaki et al. seeded luciferase-tagged human osteosarcoma subclone cell line in the knee of athymic mice and allowed lung metastasis to develop. Once metastasis was confirmed, the investigators complexed miR-143 with atelocollagen for systemic delivery every 3 days for 19 days. At 1 week, the only lesions detected were those at the primary osteosarcoma site in the knee. Following the course of treatment, only two often mice injected with miR-143 atelocollagen showed lung metastasis [268]. Similarly, in a model of metastatic prostate cancer, miR-16 delivery via atelocollagen systemic delivery resulted in significant reduction of bone metastatic growth [264]. The tumor-suppressive effects of atelocollagen miRNA have also been demonstrated in a xenograft tumor model of human colon cancer in athymic mice. miR-34a was identified as a potential miRNA capable of growth arrest and growth suppression through quantitative polymerase chain reaction analysis. The miRNA was then complexed with atelocollagen for systemic delivery and then administered intravenously to the xenograft mice. miR-34a atelocollagen administration resulted in upregulation of p53 and 36 % of cancer tissues demonstrated downregulation of miR-34a [265]. As a delivery mechanism in oncologic treatments, atelocollagen has demonstrated efficacy, but its utility has also been investigated in tissue engineering applications. In a rat model of ligamentous healing, Shoji et al. demonstrated that intra-articular injection of atelocollagen complexed miR-210 prompted healing of a partially torn anterior cruciate ligament through enhancement of angiogenesis via upregulation of vascular endothelial growth factor and fibroblast growth factor-2 [269]. In sum, the delivery of miRNA and other RNAi nucleotides has been demonstrated using atelocollagen as a delivery mechanism.
5.6 Metallic Core Nanoparticles
Cancer therapeutic strategies include gene delivery to target cancer cells in order to replace dysfunctional tumor suppressor genes, elicit immune rejection, or drive tumor cells into apoptotic pathways. To date, several biological delivery vehicles, including DNA, cationic liposomes, viral vectors , and siRNA nanoparticles, have been used with advantages and limitations [270–272]. Other vehicles have thus been investigated to overcome the inefficiencies of the previously described vehicles. To this end, investigators have begun to look into metal-based nanoparticles , namely gold nanoparticles for systemic miRNA delivery [273, 274] .
Gold nanoparticles have received attention because of their unique physicochemical properties such as shape, surface area, amphiphilicity, biocompatibility, and safe carrier capabilities essential for effective nucleotide delivery [275–278]. However, the nucleotide cargo, often siRNA, had to be modified to facilitate delivery [279–281]. These modifications would likely alter the activity of miRNA and would therefore not be possible in their delivery. Recognizing the need to efficiently deliver unmodified miRNA investigators has used gold nanoparticle–miRNA complexing to form stable delivery vehicles. Crew et al. demonstrated that through conjugation miRNA could be immobilized to the surface of gold nanoparticles and efficiently transfected into cells for gene knockdown [282]. Similarly, Ghosh et al. developed a system where unmodified miRNA would be bound to the gold nanoparticles, then covered in a PEG layer to allow for protection from serum nucleases (Fig. 19.10). In vitro functional characterization demonstrated that this system was capable of efficiently delivering miRNA into cells resulting in significant target gene downregulation and decreased cell proliferation [276]. While this delivery system appears promising, true in vivo translation has yet to be realized.

Synthesis, delivery, and characterization of gold nanoparticles (AuNPs) and miR-AuNP-S-PEG polyelectrolyte complexes. a Schematic diagram of the miR-AuNP synthesis and uptake through endocytosis pathway. b TEM image of dialyzed cationic AuNPs that were prepared by chemical reduction of chloroauric acid (HAuCl4) using sodium borohydride (NaBH4) in the presence of cysteamine hydrochloride (HS–CH2CH2–NH3 + Cl−) followed by dialysis against RNAse-free water in a Spectra/Por dialysis membrane with a molecular weight cutoff of 10 kDa. c Gel retardation assay: TBE-Urea gel electrophoresis of miR-AuNP polyelectrolyte complexes. In each case, 1 μg of miRNA was loaded to observe polyelectrolyte complex formation with AuNPs. (Reproduced from [276] with permission from Elsevier)
6 Future Perspectives on Drug Delivery: Multistage Theory
The targeting of genetic materials, since their inception, has found difficulty in efficient targeting. Naked oligonucleotides are rapidly cleared by nucleases and encapsulation in lipid-based carriers, while effective, also suffer from rapid clearance in addition to their immunogenicity [283, 284]. Opsonin recognition to lipid nanoparticles and complement-mediated clearance can trigger toll-like receptor activation and transgene silencing. While viral vehicles for delivery have the potential for mass reproduction of carried genes and have shown some efficacy, they too are troubled with limitations that have prevented their full translation into the clinic [285, 286]. In some cases, the inflammatory response generated from the vector itself may enhance its clearance and thus decrease the payload delivery and therapeutic efficacy [287]. Polymeric nanoparticles similarly are troubled by clearance from the system [288]. While the mechanisms of clearance vary, the end result is the same in decreased payload delivery and increased immunogenic response. Because of the ability to effectively target polymer nanoparticles to the cell, they are capable of entry but release from the endosome results in endosomal content leakage and intracellular damage [289] . Further, their accumulation in RES organs such as the lung, liver, and spleen makes them difficult to target elsewhere. Because of their recognition by the host as foreign, antibodies are made and further dosing results in more decreased delivery as well as stimulating the body to reject any cells transduced by the foreign viral particles [290–293].
To summarize, there are many limitations to the success and efficacy of current delivery systems for RNAi and specifically miRNA delivery . These shortcomings include inadequate targeting, poor tumor accumulation, systemic toxicity, and most importantly, inadequate clinical translation and efficacy. A paradigm shift is needed in the fundamental principles of how to target and deliver miRNA and other RNAi oligonucleotides effectively to the site of interest. Since no single agent truly possesses the ability to overcome the plethora of obstacles to therapeutic delivery, a multistage delivery approach proposes the use a nested multicomponent construct, engineered to sequentially avoid biological barriers [178, 294]. According to the multistage dogma, biobarrier avoidance, recognition, and cytotoxicity interdependence are reduced, yet acting in efficacious operational synchrony [295, 296].
7 Mesoporous Silicon and Therapeutic Applications
The rationale of the multistage theory is to decouple the multiplicity of tasks in targeting to preferentially negotiate bio-barriers, sequester the vehicle at the site of interest, and then deliver the payload. By enabling the slow, controlled, and persistent release of a drug, one could potentially reduce toxicities and heighten the therapeutic efficacy of the molecule. Through this mechanism, drugs with great therapeutic efficacy, but previously deemed too toxic for systemic therapy, can be considered for clinical use. Additionally, other barriers such as the blood-–brain -barriers and the RES, previously thought to be unavoidable, may be negotiated. These barriers have presented the most challenging obstacles to current oligonucleotide- based therapies and present opportunities for improvement through multistage delivery .
Despite the vast assortment of nanomaterials, the majority of the nanocarriers rely on molecules functionalized on their surface for biological recognition or protection from the RES. Polyethylene glycol-coated nanoparticles have been used to hide the payload from elimination, but in doing so lose their targeting abilities . Conversely, targeted particles, while preferentially finding their site of action, are quickly cleared by the body’s defensive mechanisms. Unfortunately, the overall activity of biological barriers ultimately prevents these carriers from localizing at a specific site in adequate therapeutic concentrations [297, 298]. As nanocarriers evolved from generation to generation, so did their ability to in overcome biobarriers. First-generation nanocarriers, relying on passively homing to diseased sites through the enhanced permeability and retention, resulted in extravasation through the tumor’s diseased vasculature. Second-generation nanocarriers possessed greater functionality through the conjugation of targeting moieties and thus could selectively concentrate at the site of interest. Liposomes and other targeted nanomaterials such as gold are examples of delivery systems [299–301]. Third-generation nanocarriers are characterized by their ability to carry both therapeutic and diagnostic multifunctional components with logic-embedded functions. This system focuses on negotiating the body’s biobarriers, accumulating at the target site, and delivering the protected payload to the target site. To accomplish these combined operations, third-generation nanocarriers are comprised of nanoparticles loaded into a nanostructured carrier [302–304]. Third-generation systems are comprised of multiple components assembled with embedded instructions to act in a synergistic, preprogrammable, and sequential manner. The multistage delivery system (MDS) is an emblematic system for third-generation carriers and may be a potential solution to the shortcomings of current miRNA delivery mechanisms .
Multistage Delivery System
In order to negotiate biological barriers and fully utilize the advantages of a third-generation nanocarrier, our laboratory envisioned and engineered the MDS (Fig. 19.11). The MDS aimed to decouple the tasks required of the carrier system into vehicle, nanocarrier, and therapeutic agent. By shielding the nanocarrier and payload from the serum nucleases in the intravascular space, the MDS vehicles can transport millions of loaded nanoparticles to the site of diseased tissue. The rational design, based on mathematical modeling of blood flow within diseased vessels, allows the micron-sized mesoporous silicon particles to exploit aberrant blood flow of tumor vasculature and land itself in the tissue to selectively deliver a nanoparticle-carrying payload. The governing principle of the MDS involves the loading of nanoparticles into first-stage micron-sized particle that can be finely tuned to achieve precise targeting. Tuning refers to changing the physical properties of the particle to specialize it for the intended application and payload. Pore size, porosity, shape, and size can all be calibrated based on the desired function, target, and ultimate destination. With this approach, the first-stage silicon carrier is optimized for the navigation through the bloodstream, avoidance of the RES and nucleases, recognition of a diseased site, as well as retention and protection of a payload. The second-stage nanoparticle, which can be a liposome, gold nanoparticle, or a viral vector , is then capable of extravasation through the tumor’s fenestrations and into the target microenvironment. Silicon , the precursor element to mesoporous silicon and one of Earth’s richest elements, was strategically chosen to fabricate this first-stage carrier because of its biodegradability and biocompatibility [305–307]. Porous silicon particles have shown considerable advantageous properties, such as increased drug solubility, bioavailability, biocompatibility, and sustained localized release. Through the direct release of the therapeutic agent at the site, one could potentially increase the amount of drug actually penetrating the tumor.

SEM micrographs of PSPs. a Digital composition of three distinct SEM micrographs showing the nucleation side of a 3.2 μm, 1.6 μm, and 0.97 μm PSP:the external corona (1) and the nucleation site (2). b Digital composition of three distinct SEM micrographs showing the release side of a 3.2 μm, 1.6 μm, and 0.97 μm PSP. Section along the diameter and the lateral view of: a flat disk PSP obtained by wet etch of the masking layer (c, d, respectively); a discoidal PSP obtained by trench formation by CF4 RIE (e, f, respectively); a hemispherical PSP obtained by trench formation by SF6 RIE (g, h, respectively); a tubular PSP obtained by trench formation by combination of HBr and SF6 RIE (i, j, respectively); a XLP1 PSP (k, l, respectively). (m) Close-up view of the multilayer structure of an XLP1 particle, from top to bottom: 1 SP layer, 2 transitional layer, 3 XLP layer. (c – m) Nucleation side is at the top of the figure and release side at the bottom. All scale bars are 200 nm. (Reproduced from [314] with permission from John Wiley and Sons Publishing Group)
To effectively target therapeutic agents, it is necessary to develop a delivery system that is simultaneously able to negotiate biological barriers, while protecting the payload, and then only at the site of interest effectively release its payload [178, 308–310]. Designed to exploit the body’s natural environment, the discoid shape was chosen for the MDS to allow for greater blood margination and improved cell surface adhesion to the leaky vasculature of a tumor [308, 311]. The pores’ tunable size enables control of surface area, density, the degradation rate, and thus of the dose of drug released [312, 313]. The ability to customize the pore size also permits the loading of nanoparticles of different sizes within the porous matrix [314]. Through the employment of these unique features, therapeutic and imaging agents can be loaded into the MDS and transported in an effective manner. As this technology evolves and the capabilities of first-stage nanoparticle loading improve, so does the potential for therapeutic and diagnostic applications.
8 Conclusion
Since the discovery of lin-4, miRNA has been shown to be a novel and multifunctional target in many disease processes. Although the interconnectivity of gene expression, protein synthesis, and miRNA interaction has yet to be elucidated, the utility of miRNA targeting or delivery has been demonstrated [315]. Many obstacles, though, confront the true translation of these ubiquitously expressed small, noncoding RNAs to the clinic. Effective negotiation of the body’s biological barriers of serum nucleases, renal and hepatic clearance, vascular endothelium, cellular membranes, and endosomal release is paramount to the success of these molecules and effective therapeutic agents. To that end, investigators have developed and tested many delivery systems ranging from synthetic to naturally occurring polymers, as well as viral vectors for targeted delivery of the oligonucleotide payload. These delivery systems have shown some success, but are limited by their poor clinical translation. Although many advances in polymer chemistry and interdisciplinary approaches have been utilized, a new paradigm for drug delivery could potentially revolutionize the effective delivery of miRNA. Through multistage delivery, miRNA could be shielded from the degradation and sequestration, while not sacrificing targeting or organ specificity. Taken together, there is great potential for miRNA to have a great impact in the clinic, and with a proper understanding of the obstacles to overcome and tools in our armament to negotiate these barriers, it will find true translation into the clinic.
References
Lee RC, RL Feinbaum, Ambros V. The C. elegans heterochronic gene lin-4 encodes small RNAs with antisense complementarity to lin-14. Cell. 1993;75(5):843–54.
Wightman B, Ha I, Ruvkun G. Posttranscriptional regulation of the heterochronic gene lin-14 by lin-4 mediates temporal pattern formation in C. elegans. Cell. 1993;75(5):855–62.
Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004;116(2):281–97.
Baek D, et al. The impact of microRNAs on protein output. Nature. 2008;455(7209):64–71.
Lewis BP, Burge CB, Bartel DP. Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell. 2005;120(1):15–20.
Lewis BP, et al. Prediction of mammalian microRNA targets. Cell. 2003;115(7):787–98.
Bader AG et al. Developing therapeutic microRNAs for cancer. Gene Ther. 2011;18(12):1121–6.
Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat Rev Cancer. 2006;6(11):857–66.
Esquela-Kerscher A, Slack FJ. Oncomirs – microRNAs with a role in cancer. Nature reviews. Cancer. 2006;6(4):259–69.
Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. 2000;100(1):57–70.
Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–74.
Check Hayden E. Cancer complexity slows quest for cure. Nature. 2008;455(7210):148.
Hogberg T. Chemotherapy: current drugs still have potential in advanced ovarian cancer. Nat Rev Clin Oncol. 2010;7(4):191–3.
Nahleh Z. Neoadjuvant chemotherapy for “triple negative” breast cancer: a review of current practice and future outlook. Med Oncol. 2010;27(2):531–9.
Ohtsu A. Current status and future prospects of chemotherapy for metastatic gastric cancer: a review. Gastric cancer: official journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association. 2005;8(2):95–102.
Imai K, Takaoka A. Comparing antibody and small-molecule therapies for cancer. Nat Rev Cancer. 2006;6(9):714–27.
Aggarwal S, et al. A dimeric peptide that binds selectively to prostate-specific membrane antigen and inhibits its enzymatic activity. Cancer Res. 2006;66(18):9171–7.
Le Pechoux C. Role of postoperative radiotherapy in resected non-small cell lung cancer: a reassessment based on new data. Oncologist. 2011;16(5):672–81.
Buchholz TA. Radiation therapy for early-stage breast cancer after breast-conserving surgery. N Engl J Med. 2009;360(1):63–70.
Recht A, et al. The sequencing of chemotherapy and radiation therapy after conservative surgery for early-stage breast cancer. N Engl J Med. 1996;334(21):1356–61.
McCahill L, Ferrell B. Palliative surgery for cancer pain. West J Med. 2002;176(2):107–10.
Carthew RW, Sontheimer EJ. Origins and mechanisms of miRNAs and siRNAs. Cell. 2009;136(4):642–55.
Couvillion MT, et al. Sequence, biogenesis, and function of diverse small RNA classes bound to the Piwi family proteins of Tetrahymena thermophila. Genes Dev. 2009;23(17):2016–32.
Sontheimer EJ, Carthew RW. Silence from within: endogenous siRNAs and miRNAs. Cell. 2005;122(1):9–12.
Hammond SM, et al. An RNA-directed nuclease mediates post-transcriptional gene silencing in Drosophila cells. Nature. 2000;404(6775):293–6.
Meister G, et al. Human Argonaute2 mediates RNA cleavage targeted by miRNAs and siRNAs. Mol Cell. 2004;15(2):185–97.
Meister G, et al. Identification of novel argonaute-associated proteins. Curr Biol. 2005;15(23):2149–55.
Meister G, Tuschl T. Mechanisms of gene silencing by double-stranded RNA. Nature. 2004;431(7006):343–9.
Brown BD, Naldini L. Exploiting and antagonizing microRNA regulation for therapeutic and experimental applications. Nature reviews. Genetics. 2009;10(8):578–85.
Cai Y, et al. A brief review on the mechanisms of miRNA regulation. Genomics, Proteomics Bioinformatics. 2009;7(4):147–54.
Eulalio A, Huntzinger E, Izaurralde E. Getting to the root of miRNA-mediated gene silencing. Cell. 2008;132(1):9–14.
Guang S, et al. An Argonaute transports siRNAs from the cytoplasm to the nucleus. Science. 2008;321(5888):537–41.
Lu J, et al. The birth and death of microRNA genes in Drosophila. Nat Genet. 2008;40(3):351–5.
Moazed D. Small RNAs in transcriptional gene silencing and genome defence. Nature. 2009;457(7228):413–20.
Ohrt T, et al. Fluorescence correlation spectroscopy and fluorescence cross-correlation spectroscopy reveal the cytoplasmic origination of loaded nuclear RISC in vivo in human cells. Nucleic Acids Res. 2008;36(20):6439–49.
Wu L, Fan J, Belasco JG. MicroRNAs direct rapid deadenylation of mRNA. Proc Natl Acad Sci USA. 2006;103(11):4034–9.
Golden DE, Gerbasi VR, Sontheimer EJ. An inside job for siRNAs. Mol Cell. 2008;31(3):309–12.
Mello CC, Conte D Jr. Revealing the world of RNA interference. Nature. 2004;431(7006):338–42.
Dunoyer P, et al. An endogenous, systemic RNAi pathway in plants. EMBO J. 2010;29(10):1699–712.
Fagegaltier D, et al. The endogenous siRNA pathway is involved in heterochromatin formation in Drosophila. Proc Natl Acad Sci USA. 2009;106(50):21258–63.
Krek A, et al. Combinatorial microRNA target predictions. Nat Genet. 2005;37(5):495–500.
Rajewsky N. microRNA target predictions in animals. Nat Genet. 2006;38(Suppl):S8–13.
Ding XC, Grosshans H. Repression of C. elegans microRNA targets at the initiation level of translation requires GW182 proteins. EMBO J. 2009;28(3):213–22.
Wakiyama M, et al. Let-7 microRNA-mediated mRNA deadenylation and translational repression in a mammalian cell-free system. Genes Dev. 2007;21(15):1857–62.
Han J, et al. Molecular basis for the recognition of primary microRNAs by the Drosha-DGCR8 complex. Cell. 2006;125(5):887–901.
Kim VN. MicroRNA biogenesis: coordinated cropping and dicing. Nat Rev Mol Cell Biol. 2005;6(5):376–85.
Bushati N, Cohen SM. microRNA functions. Annu Rev Cell Dev Biol. 2007;23:175–205.
Fabian MR, Sonenberg N. The mechanics of miRNA-mediated gene silencing: a look under the hood of miRISC. Nat Struct Mol Biol. 2012;19(6):586–93.
Behm-Ansmant I, et al. mRNA degradation by miRNAs and GW182 requires both CCR4:NOT deadenylase and DCP1:DCP2 decapping complexes. Genes Dev. 2006;20(14):1885–98.
Mishima Y, et al. Translational inhibition by deadenylation-independent mechanisms is central to microRNA-mediated silencing in zebrafish. Proc Natl Acad Sci USA. 2012;109(4):1104–9.
Guo H, et al. Mammalian microRNAs predominantly act to decrease target mRNA levels. Nature. 2010;466(7308):835–40.
Huntzinger E, Izaurralde E. Gene silencing by microRNAs: contributions of translational repression and mRNA decay. Nat Rev Genet. 2011;12(2):99–110.
Kiriakidou M, et al. An mRNA m7G cap binding-like motif within human Ago2 represses translation. Cell. 2007;129(6):1141–51.
Bazzini AA, Lee MT, Giraldez AJ. Ribosome profiling shows that miR-430 reduces translation before causing mRNA decay in zebrafish. Science. 2012;336(6078):233–7.
Bethune J, Artus-Revel CG, Filipowicz W. Kinetic analysis reveals successive steps leading to miRNA-mediated silencing in mammalian cells. EMBO Rep. 2012;13(8):716–23.
Djuranovic S, Nahvi A, Green R. miRNA-mediated gene silencing by translational repression followed by mRNA deadenylation and decay. Science. 2012. 336(6078):237–40.
Baltimore D, et al. MicroRNAs: new regulators of immune cell development and function. Nat Immunol. 2008;9(8):839–45.
Huang Y, et al. Biological functions of microRNAs: a review. J Physiology Biochem. 2011;67(1):129–39.
Kloosterman WP, et al. Targeted inhibition of miRNA maturation with morpholinos reveals a role for miR-375 in pancreatic islet development. PLoS Biol. 2007;5(8):e203.
Neilson JR, et al. Dynamic regulation of miRNA expression in ordered stages of cellular development. Genes Dev. 2007;21(5):578–589.
Cheng Y, Zhang C. MicroRNA-21 in cardiovascular disease. J Cardiovasc Transl Res. 2010;3(3):251–5.
Cheng Z, et al. MiR-320a is downregulated in patients with myasthenia gravis and modulates inflammatory cytokines production by targeting mitogen-activated protein kinase 1. J Clin Immunol. 2013;33(3):567–76.
Esau CC, Monia BP. Therapeutic potential for microRNAs. Adv Drug Deliv Rev. 2007;59(2–3):101–14.
Jazbutyte V, Thum T. MicroRNA-21: from cancer to cardiovascular disease. Curr Drug Targets. 2010;11(8):926–35.
Lu M, et al. An analysis of human microRNA and disease associations. PLoS One. 2008;3(10):e3420.
Small EM, Frost RJ, Olson EN. MicroRNAs add a new dimension to cardiovascular disease. Circulation. 2010;121(8):1022–32.
Calin GA, et al. Human microRNA genes are frequently located at fragile sites and genomic regions involved in cancers. Proc Natl Acad Sci USA. 2004;101(9):2999–3004.
Iorio MV, Croce CM. MicroRNA dysregulation in cancer: diagnostics, monitoring and therapeutics. A comprehensive review. EMBO Mol Med. 2012;4(3):143–59.
Zhang L, et al. microRNAs exhibit high frequency genomic alterations in human cancer. Proc Natl Acad Sci USA. 2006;103(24):9136–41.
Brueckner B, et al. The human let-7a-3 locus contains an epigenetically regulated microRNA gene with oncogenic function. Cancer Res. 2007;67(4):1419–23.
Ota A, et al. Identification and characterization of a novel gene, C13orf25, as a target for 13q31-q32 amplification in malignant lymphoma. Cancer Res. 2004;64(9):3087–95.
He L, et al. A microRNA polycistron as a potential human oncogene. Nature. 2005;435(7043):828–33.
Tong AW, Nemunaitis J. Modulation of miRNA activity in human cancer: a new paradigm for cancer gene therapy? Cancer Gene Ther. 2008;15(6):341–55.
Hammond SM. MicroRNAs as oncogenes. Curr Opin Genet Dev. 2006;16(1):4–9.
Zhang B, et al. microRNAs as oncogenes and tumor suppressors. Dev Biol. 2007;302(1):1–12.
Croce CM. Oncogenes and cancer. N Engl J Med. 2008. 358(5):502–11.
Bader AG, Brown D, Winkler M. The promise of microRNA replacement therapy. Cancer Res. 2010;70(18):7027–30.
Costinean S, et al. Pre-B cell proliferation and lymphoblastic leukemia/high-grade lymphoma in E(mu)-miR155 transgenic mice. Proc Natl Acad Sci USA. 2006;103(18):7024–9.
Esteller M. Epigenetics in cancer. N Engl J Med. 2008;358(11):1148–59.
Feinberg AP, Vogelstein B. Hypomethylation distinguishes genes of some human cancers from their normal counterparts. Nature. 1983;301(5895):89–92.
Gonzalez-Zulueta M, et al. Methylation of the 5’ CpG island of the p16/CDKN2 tumor suppressor gene in normal and transformed human tissues correlates with gene silencing. Cancer Res. 1995;55(20):4531–5.
Herman JG, et al. Inactivation of the CDKN2/p16/MTS1 gene is frequently associated with aberrant DNA methylation in all common human cancers. Cancer Res. 1995;55(20):4525–30.
Sakai T, et al. Allele-specific hypermethylation of the retinoblastoma tumor-suppressor gene. Am J Hum Gen. 1991;48(5):880–8.
Johnson SM, et al. RAS is regulated by the let-7 microRNA family. Cell. 2005;120(5):635–47.
Garzon R, et al. MicroRNA signatures associated with cytogenetics and prognosis in acute myeloid leukemia. Blood. 2008;111(6):3183–9.
Toyota M, et al. Epigenetic silencing of microRNA-34b/c and B-cell translocation gene 4 is associated with CpG island methylation in colorectal cancer. Cancer Res. 2008;68(11):4123–32.
Wang T, et al. A micro-RNA signature associated with race, tumor size, and target gene activity in human uterine leiomyomas. Genes Chromosomes Cancer. 2007;46(4):336–47.
Iorio MV, et al. MicroRNA gene expression deregulation in human breast cancer. Cancer Res. 2005;65(16):7065–70.
Iorio MV, et al. MicroRNA signatures in human ovarian cancer. Cancer Res. 2007;67(18):8699–707.
Lehmann U, et al. Epigenetic inactivation of microRNA gene hsa-mir-9–1 in human breast cancer. J Pathol. 2008;214(1):17–24.
Blenkiron C, Miska EA. miRNAs in cancer: approaches, aetiology, diagnostics and therapy. Human Mol Genet. 2007;16(Spec No 1):R106–13.
Tavazoie SF, et al. Endogenous human microRNAs that suppress breast cancer metastasis. Nature. 2008;451(7175):147–52.
Tang J, Ahmad A, Sarkar FH. The Role of MicroRNAs in Breast Cancer Migration, Invasion and Metastasis. Int J Mol Sci. 2012;13(10):13414–37.
Wu H, Zhu S, Mo YY. Suppression of cell growth and invasion by miR-205 in breast cancer. Cell Res. 2009;19(4):439–48.
Mishra PJ, Merlino G. MicroRNA reexpression as differentiation therapy in cancer. J Clin Invest. 2009;119(8):2119–23.
Rosenfeld N, et al. MicroRNAs accurately identify cancer tissue origin. Nat Biotechnol. 2008;26(4):462–9.
Calin GA, et al. A MicroRNA signature associated with prognosis and progression in chronic lymphocytic leukemia. N Engl J Med. 2005;353(17):1793–801.
Caramuta S, et al. MicroRNA expression profiles associated with mutational status and survival in malignant melanoma. J Invest Dermatol. 2010;130(8):2062–70.
Chen Q, et al. Prognostic significance of serum miR-17–5p in lung cancer. Med Oncol. 2013;30(1):353.
Rothschild SI, et al. MicroRNA-381 represses ID1 and is deregulated in lung adenocarcinoma. J Thorac Oncol: official publication of the International Association for the Study of Lung Cancer. 2012;7(7):1069–77.
Yanaihara N, et al. Unique microRNA molecular profiles in lung cancer diagnosis and prognosis. Cancer Cell. 2006;9(3):189–98.
Gregory PA, et al. MicroRNAs as regulators of epithelial-mesenchymal transition. Cell Cycle. 2008;7(20):3112–8.
Ma L, et al. Therapeutic silencing of miR-10b inhibits metastasis in a mouse mammary tumor model. Nat Biotechnol. 2010;28(4):341–7.
Zhu S, et al. MicroRNA-21 targets tumor suppressor genes in invasion and metastasis. Cell Res. 2008;18(3):350–9.
Ma L, Teruya-Feldstein J, Weinberg RA. Tumour invasion and metastasis initiated by microRNA-10b in breast cancer. Nature. 2007;449(7163):682–8.
Sahab ZJ, et al. Putative biomarkers and targets of estrogen receptor negative human breast cancer. Int J Mol Sci. 2011;12(7):4504–4521.
Simonini PdSR, et al. Epigenetically deregulated microRNA-375 is involved in a positive feedback loop with estrogen receptor α in breast cancer cells. Cancer Res. 2010;70(22):9175–9184.
Miller TE, et al. MicroRNA-221/222 confers tamoxifen resistance in breast cancer by targeting p27Kip1. J Biol Chem. 2008;283(44):29897–903.
Zhao JJ, et al. MicroRNA-221/222 negatively regulates estrogen receptor alpha and is associated with tamoxifen resistance in breast cancer. J Biol Chem. 2008;283(45):31079–86.
Krutzfeldt J, et al. Specificity, duplex degradation and subcellular localization of antagomirs. Nucleic Acids Res. 2007;35(9):2885–92.
Schwarz DS, et al. Asymmetry in the assembly of the RNAi enzyme complex. Cell. 2003;115(2):199–208.
Kumar MS, et al. Impaired microRNA processing enhances cellular transformation and tumorigenesis. Nat Genet. 2007;39(5):673–7.
Johnson CD, et al. The let-7 microRNA represses cell proliferation pathways in human cells. Cancer Res. 2007;67(16):7713–22.
Kumar MS, et al. Suppression of non-small cell lung tumor development by the let-7 microRNA family. Proc Natl Acad Sci USA. 2008;105(10):3903–8.
Trang P, et al. Regression of murine lung tumors by the let-7 microRNA. Oncogene. 2010;29(11):1580–7.
Yu F, et al. let-7 regulates self renewal and tumorigenicity of breast cancer cells. Cell. 2007;131(6):1109–23.
He L, et al. microRNAs join the p53 network–another piece in the tumour-suppression puzzle. Nature reviews. Cancer. 2007;7(11):819–22.
Wiggins JF, et al. Development of a lung cancer therapeutic based on the tumor suppressor microRNA-34. Cancer Res. 2010;70(14):5923–30.
Kota J, et al. Therapeutic microRNA delivery suppresses tumorigenesis in a murine liver cancer model. Cell. 2009;137(6):1005–17.
Takeshita F, et al. Systemic delivery of synthetic microRNA-16 inhibits the growth of metastatic prostate tumors via downregulation of multiple cell-cycle genes. Mol Ther. 2010;18(1):181–7.
Hutvagner G, et al. Sequence-specific inhibition of small RNA function. PLoS Biol. 2004;2(4):E98.
Meister G, et al. Sequence-specific inhibition of microRNA- and siRNA-induced RNA silencing. RNA. 2004;10(3):544–50.
Orom UA, Kauppinen S, Lund AH. LNA-modified oligonucleotides mediate specific inhibition of microRNA function. Gene. 2006;372:137–41.
Krutzfeldt J, et al. Silencing of microRNAs in vivo with ‘antagomirs’. Nature. 2005;438(7068):685–9.
Shen H, Sun T, Ferrari M. Nanovector delivery of siRNA for cancer therapy. Cancer Gene Ther. 2012;19(6):367–373.
Ganta S, et al. A review of multifunctional nanoemulsion systems to overcome oral and CNS drug delivery barriers. Molecular Membrane Biology. 2010;27(7):260–273.
Tanaka T, et al. Nanotechnology for breast cancer therapy. Biomed Microdevices. 2009;11(1):49–63.
Wakai Y, et al. Effective cancer targeting using an anti-tumor tissue vascular endothelium-specific monoclonal antibody (TES-23). Jpn J Cancer Res. 2000;91(12):1319–1325.
Sanhai WR, et al. Seven challenges for nanomedicine. Nat Nanotechnol. 2008;3(5):242–4.
Esquela-Kerscher A, et al. The let-7 microRNA reduces tumor growth in mouse models of lung cancer. Cell Cycle. 2008;7(6):759–64.
Liu C, et al. The microRNA miR-34a inhibits prostate cancer stem cells and metastasis by directly repressing CD44. Nat Med. 2011;17(2):211–5.
Trang P, et al. Systemic delivery of tumor suppressor microRNA mimics using a neutral lipid emulsion inhibits lung tumors in mice. Mol Ther: the journal of the American Society of Gene Therapy. 2011;19(6):1116–22.
Juliano R, et al. Biological barriers to therapy with antisense and siRNA oligonucleotides. Mol Pharm. 2009;6(3):686–95.
Yang XC, et al. Studies of the 5’ exonuclease and endonuclease activities of CPSF-73 in histone pre-mRNA processing. Mol Cell Biol. 2009;29(1):31–42.
Krol J, Loedige I, Filipowicz W. The widespread regulation of microRNA biogenesis, function and decay. Nat Rev Genet. 2010;11(9):597–610.
Katoh T, et al. Selective stabilization of mammalian microRNAs by 3’ adenylation mediated by the cytoplasmic poly(A) polymerase GLD-2. Genes Dev. 2009;23(4):433–8.
Ramachandran V, Chen X. Degradation of microRNAs by a family of exoribonucleases in Arabidopsis. Science. 2008;321(5895):1490–2.
Turchinovich A, et al. Characterization of extracellular circulating microRNA. Nucleic Acids Res. 2011;39(16):7223–33.
Matsumura Y, Maeda H. A new concept for macromolecular therapeutics in cancer chemotherapy: mechanism of tumoritropic accumulation of proteins and the antitumor agent smancs. Cancer Res. 1986;46(12 Pt 1):6387–92.
Shinohara N., Danno N., Ichinose T., Sasaki T., Fukui H., Honda K., and Gamo M. Tissue distribution and clearance of intravenously administered titanium dioxide (TiO2) nanoparticles. Nanotoxicology. 2013;8(2):132–141.
Sa LT, et al. Biodistribution of nanoparticles: initial considerations. J Pharm Biomed Anal. 2012. 70:602–4.
Kang YS, Boado RJ, Pardridge WM. Pharmacokinetics and organ clearance of a 3’-biotinylated, internally [32P]-labeled phosphodiester oligodeoxynucleotide coupled to a neutral avidin/monoclonal antibody conjugate. Drug Metab Dispos. 1995;23(1):55–9.
Rifai A, et al. Clearance kinetics, biodistribution, and organ saturability of phosphorothioate oligodeoxynucleotides in mice. Am J Pathol. 1996;149(2):717–25.
Gutierrez-Puente Y, et al. Safety, pharmacokinetics, and tissue distribution of liposomal P-ethoxy antisense oligonucleotides targeted to Bcl-2. J Pharm Exp Ther. 1999;291(2):865–9.
Juliano RL, et al. Antisense pharmacodynamics: critical issues in the transport and delivery of antisense oligonucleotides. Pharm Res. 1999;16(4):494–502.
Merkel OM, et al. In vivo SPECT and real-time gamma camera imaging of biodistribution and pharmacokinetics of siRNA delivery using an optimized radiolabeling and purification procedure. Bioconjug Chem. 2009;20(1):174–82.
van de Water FM, et al. Intravenously administered short interfering RNA accumulates in the kidney and selectively suppresses gene function in renal proximal tubules. Drug Metab. Dispos. 2006;34(8):1393–7.
Martino, F., et al., Circulating microRNAs are not eliminated by hemodialysis. PloS one. 2012;7(6):e38269.
Mosser DM, Edwards JP. Exploring the full spectrum of macrophage activation. Nature Rev Immunol. 2008;8(12):958–69.
Alexis F, et al. Factors affecting the clearance and biodistribution of polymeric nanoparticles. Mol Pharm. 2008;5(4):505–15.
Yadav KS, et al. Effect of size on the biodistribution and blood clearance of etoposide-loaded PLGA nanoparticles. PDA J Pharm Sci Technol. 2011;65(2):131–9.
Xiao K, et al. The effect of surface charge on in vivo biodistribution of PEG-oligocholic acid based micellar nanoparticles. Biomaterials. 2011;32(13):3435–46.
Talegaonkar S, Vyas SP. Inverse targeting of diclofenac sodium to reticuloendothelial system-rich organs by sphere-in-oil-in-water (s/o/w) multiple emulsion containing poloxamer 403. J Drug Target. 2005;13(3):173–8.
Li P, et al. Targeting study of gelatin adsorbed clodronate in reticuloendothelial system and its potential application in immune thrombocytopenic purpura of rat model. J Control Release: official journal of the Controlled Release Society. 2006;114(2):202–8.
Underhill DM, Ozinsky A. Phagocytosis of microbes: complexity in action. Annu Rev Immunol. 2002;20:825–52.
Nolting A, et al. Hepatic distribution and clearance of antisense oligonucleotides in the isolated perfused rat liver. Pharm Res. 1997;14(4):516–21.
Thomas LL, Price CM. Cellular uptake, distribution, and degradation of phosphorothioate oligonucleotides in Euplotes crassus. Ann N Y Acad Sci. 1992;660:328–30.
Dejana E, Simionescu M, Wolburg H. Endothelial cell biology and pathology. Cell Tissue Res. 2009;335(1):1–3.
Szekanecz Z, Koch AE. Vascular endothelium and immune responses: implications for inflammation and angiogenesis. Rheum Dis Clin North Am. 2004;30(1):97–114.
Chorianopoulos E, et al. The role of endothelial cell biology in endocarditis. Cell Tissue Res. 2009;335(1):153–63.
Pate M, et al. Endothelial cell biology: role in the inflammatory response. Adv Clin Chem. 2010;52:109–30.
Cid MC. Endothelial cell biology, perivascular inflammation, and vasculitis. Cleve Clin J Med. 2002;69(Suppl 2):SII45–9.
Furuya M, Yonemitsu Y. Cancer neovascularization and proinflammatory microenvironments. Current Cancer Drug Targets. 2008;8(4):253–65.
van der Wijk T, et al. Osmotic swelling-induced activation of the extracellular-signal-regulated protein kinases Erk-1 and Erk-2 in intestine 407 cells involves the Ras/Raf-signalling pathway. Biochem J. 1998;331(Pt 3):863–9.
Baeriswyl V, Christofori G. The angiogenic switch in carcinogenesis. Semin Cancer Biol. 2009;19(5):329–37.
Hendrix MJ, et al. Vasculogenic mimicry and tumour-cell plasticity: lessons from melanoma. Nature Rev Cancer. 2003;3(6):411–21.
Hashizume H, et al. Openings between defective endothelial cells explain tumor vessel leakiness. Am J Clin Pathol. 2000;156(4):1363–80.
Dvorak AM, Feng D. The vesiculo-vacuolar organelle (VVO). A new endothelial cell permeability organelle. J Histochemistry Cytochem: official journal of the Histochemistry Society. 2001;49(4):419–32.
Dreher MR, et al. Tumor vascular permeability, accumulation, and penetration of macromolecular drug carriers. J Natl Cancer Inst. 2006;98(5):335–44.
Folkman J. Fundamental concepts of the angiogenic process. Curr Mol Med. 2003;3(7):643–51.
Caron WP, et al. Interpatient pharmacokinetic and pharmacodynamic variability of carrier-mediated anticancer agents. Clin Pharmacol Ther. 2012;91(5):802–12.
Dvorak HF, et al. Identification and characterization of the blood vessels of solid tumors that are leaky to circulating macromolecules. Am J Pathol. 1988;133(1):95–109.
Jain RK. Transport of molecules in the tumor interstitium: a review. Cancer Res. 1987;47(12):3039–51.
Prabhakar U, et al. Challenges and key considerations of the enhanced permeability and retention effect for nanomedicine drug delivery in oncology. Cancer Res. 2013;73(8):2412–7.
Azzopardi EA, Ferguson EL, Thomas DW. The enhanced permeability retention effect: a new paradigm for drug targeting in infection. J Antimicrob Chemother. 2013;68(2):257–74.
Netti PA, et al. Role of extracellular matrix assembly in interstitial transport in solid tumors. Cancer Res. 2000;60(9):2497–503.
Liu W, et al. Tumor accumulation, degradation and pharmacokinetics of elastin-like polypeptides in nude mice. J Control Release: official journal of the Controlled Release Society. 2006;116(2):170–8.
Tasciotti E, et al. Mesoporous silicon particles as a multistage delivery system for imaging and therapeutic applications. Nat Nanotechnol. 2008;3(3):151–7.
Khatri N, et al. In vivo delivery aspects of miRNA, shRNA and siRNA. Crit Rev Ther Drug Carrier Syst. 2012;29(6):487–527.
Dominska M, Dykxhoorn DM. Breaking down the barriers: siRNA delivery and endosome escape. J Cell Sci. 2010;123(Pt 8):1183–9.
Park B, et al. Proteolytic cleavage in an endolysosomal compartment is required for activation of Toll-like receptor 9. Nat Immunol. 2008;9(12):1407–14.
Thompson DB, et al. Cellular uptake mechanisms and endosomal trafficking of supercharged proteins. Chem Biol. 2012;19(7):831–43.
Hierro A, et al. Structure of the ESCRT-II endosomal trafficking complex. Nature. 2004;431(7005):221–5.
Kelly EE, et al. The role of endosomal-recycling in long-term potentiation. Cell Mol Life Sci. 2011;68(2):185–94.
Puthenveedu MA, et al. Sequence-dependent sorting of recycling proteins by actin-stabilized endosomal microdomains. Cell. 2010;143(5):761–73.
Endoh T, Ohtsuki T. Cellular siRNA delivery using cell-penetrating peptides modified for endosomal escape. Adv Drug Deliv Rev. 2009;61(9):704–9.
Endoh T, Ohtsuki T. Cellular siRNA delivery using TatU1A and photo-induced RNA interference. Methods Mol Biol. 2010;623:271–81.
Tseng YC, Huang L. Self-assembled lipid nanomedicines for siRNA tumor targeting. J Biomed Nanotechnol. 2009;5(4):351–63.
Akhtar S, Benter IF. Nonviral delivery of synthetic siRNAs in vivo. J Clin Invest. 2007;117(12):3623–32.
Castanotto D, Rossi JJ. The promises and pitfalls of RNA-interference-based therapeutics. Nature. 2009;457(7228):426–33.
Broderick JA, Zamore PD. MicroRNA therapeutics. Gene Ther. 2011;18(12):1104–10.
Krutzfeldt J, Poy MN, Stoffel M. Strategies to determine the biological function of microRNAs. Nat Genet. 2006;38 Suppl:S14–9.
Varble A, ten Oever BR. Implications of RNA virus-produced miRNAs. RNA Biol. 2011;8(2):190–4.
Miyazaki Y, et al. Viral delivery of miR-196a ameliorates the SBMA phenotype via the silencing of CELF2. Nat Med. 2012;18(7):1136–41.
Chistiakov DA, Sobenin IA, Orekhov AN. Strategies to deliver microRNAs as potential therapeutics in the treatment of cardiovascular pathology. Drug Deliv. 2012;19(8):392–405.
Sakuma T, Barry MA, Ikeda Y. Lentiviral vectors: basic to translational. Biochem J. 2012;443(3):603–18.
Bukrinsky MI, et al. A nuclear localization signal within HIV-1 matrix protein that governs infection of non-dividing cells. Nature. 1993;365(6447):666–9.
Freed EO, Martin MA. HIV-1 infection of non-dividing cells. Nature. 1994;369(6476):107–8.
Klimatcheva E, Rosenblatt JD, Planelles V. Lentiviral vectors and gene therapy. Front Biosci: a journal and virtual library. 1999;4:D481–96.
Modlich U, Baum C. Preventing and exploiting the oncogenic potential of integrating gene vectors. J Clin Invest. 2009;119(4):755–8.
Zufferey R, et al. Multiply attenuated lentiviral vector achieves efficient gene delivery in vivo. Nat Biotechnol. 1997;15(9):871–5.
Lehmann-Che J, Saib A. Early stages of HIV replication: how to hijack cellular functions for a successful infection. AIDS Rev. 2004;6(4):199–207.
Naldini L, et al. In vivo gene delivery and stable transduction of nondividing cells by a lentiviral vector. Science. 1996;272(5259):263–7.
Kong YW, et al. microRNAs in cancer management. Lancet Oncol. 2012;13(6):e249–58.
Maegdefessel L, et al. MicroRNA-21 blocks abdominal aortic aneurysm development and nicotine-augmented expansion. Sci Transl Med. 2012;4(122):122ra22.
Craig VJ, et al. Epigenetic silencing of microRNA-203 dysregulates ABL1 expression and drives Helicobacter-associated gastric lymphomagenesis. Cancer Res. 2011;71(10):3616–24.
Liu QS, et al. Lentiviral-mediated miRNA against liver-intestine cadherin suppresses tumor growth and invasiveness of human gastric cancer. Cancer Sci. 2010;101(8):1807–12.
Gentner B, et al. Stable knockdown of microRNA in vivo by lentiviral vectors. Nat Methods. 2009;6(1):63–6.
Brown BD, et al. Endogenous microRNA can be broadly exploited to regulate transgene expression according to tissue, lineage and differentiation state. Nat Biotechnol. 2007;25(12):1457–67.
Ebert MS, Neilson JR, Sharp PA. MicroRNA sponges: competitive inhibitors of small RNAs in mammalian cells. Nat methods. 2007;4(9):721–6.
Grimm D, et al. Argonaute proteins are key determinants of RNAi efficacy, toxicity, and persistence in the adult mouse liver. J Clin Invest. 2010;120(9):3106–19.
Cavazzana-Calvo M, et al. Transfusion independence and HMGA2 activation after gene therapy of human beta-thalassaemia. Nature. 2010;467(7313):318–22.
Rayner KJ, et al. MiR-33 contributes to the regulation of cholesterol homeostasis. Science. 2010;328(5985):1570–3.
Stevenson SC, et al. Human adenovirus serotypes 3 and 5 bind to two different cellular receptors via the ol head domain. J Virol. 1995;69(5):2850–7.
Shashkova EV, May SM, Barry MA. Characterization of human adenovirus serotypes 5, 6, 11, and 35 as anticancer agents. Virology. 2009;394(2):311–20.
Fu J, Li L, Bouvier M. Adenovirus E3–19K proteins of different serotypes and subgroups have similar, yet distinct, immunomodulatory functions toward major histocompatibility class I molecules. J Biol Chem. 2011;286(20):17631–9.
Grimm D, et al. Fatality in mice due to oversaturation of cellular microRNA/short hairpin RNA pathways. Nature. 2006;441(7092):537–41.
Daya S, Berns KI. Gene therapy using adeno-associated virus vectors. Clin Microbiol Rev. 2008;21(4):583–93.
Han Y, et al. MicroRNA expression signatures of bladder cancer revealed by deep sequencing. PloS one. 2011;6(3):e18286.
Grady WM, Tewari M. The next thing in prognostic molecular markers: microRNA signatures of cancer. Gut. 2010;59(6):706–8.
Calin GA, Croce CM. MicroRNAs and chromosomal abnormalities in cancer cells. Oncogene. 2006;25(46):6202–10.
Care A, et al. MicroRNA-133 controls cardiac hypertrophy. Nat Med. 2007;13(5):613–8.
Colin A, et al. Engineered lentiviral vector targeting astrocytes in vivo. Glia. 2009;57(6):667–79.
Leja J, et al. Double-detargeted oncolytic adenovirus shows replication arrest in liver cells and retains neuroendocrine cell killing ability. PLoS One. 2010;5(1):e8916.
Thomas CE, Ehrhardt A, Kay MA. Progress and problems with the use of viral vectors for gene therapy. Nat Rev Genet. 2003;4(5):346–58.
Mingozzi F, High KA. Therapeutic in vivo gene transfer for genetic disease using AAV: progress and challenges. Nat Rev Genet. 2011;12(5):341–55.
Kang EM, et al. Retrovirus gene therapy for X-linked chronic granulomatous disease can achieve stable long-term correction of oxidase activity in peripheral blood neutrophils. Blood. 2010;115(4):783–91.
Hacein-Bey-Abina S, et al. Insertional oncogenesis in 4 patients after retrovirus-mediated gene therapy of SCID-X1. J Clin Invest. 2008;118(9):3132–42.
Wang J, et al. Delivery of siRNA therapeutics: barriers and carriers. The AAPS J. 2010;12(4):492–503.
Kline KK, Tucker SA. Spectroscopic characterization of core-based hyperbranched poly(ethyleneimine) and dendritic poly(propyleneimine) as selective uptake devices. J Phys Chem A. 2010;114(27):7338–44.
Ibrahim AF, et al. MicroRNA replacement therapy for miR-145 and miR-33a is efficacious in a model of colon carcinoma. Cancer Res. 2011;71(15):5214–24.
Tazawa H, et al. Tumor-suppressive miR-34a induces senescence-like growth arrest through modulation of the E2F pathway in human colon cancer cells. Proc Natl Acad Sci USA. 2007;104(39):15472–7.
Chiou GY, et al. Cationic polyurethanes-short branch PEI-mediated delivery of Mir145 inhibited epithelial-mesenchymal transdifferentiation and cancer stem-like properties and in lung adenocarcinoma. J Control Release: official journal of the Controlled Release Society. 2012;159(2):240–50.
Chiou SH, et al. Coexpression of Oct4 and Nanog enhances malignancy in lung adenocarcinoma by inducing cancer stem cell-like properties and epithelial-mesenchymal transdifferentiation. Cancer Res. 2010;70(24):10433–44.
Danhier F, et al. PLGA-based nanoparticles: an overview of biomedical applications. J Control Release: official journal of the Controlled Release Society. 2012;161(2):505–22.
Prokop A, Davidson JM. Nanovehicular intracellular delivery systems. J Pharm Sci. 2008;97(9):3518–90.
Kumari A, Yadav SK, Yadav SC. Biodegradable polymeric nanoparticles based drug delivery systems. Colloids Surf B Biointerfaces. 2010;75(1):1–18.
Owens DE 3rd, Peppas NA. Opsonization, biodistribution, and pharmacokinetics of polymeric nanoparticles. Int J Pharm. 2006;307(1):93–102.
Klugherz BD, et al. Gene delivery from a DNA controlled-release stent in porcine coronary arteries. Nat Biotechnol. 2000;18(11):1181–4.
Gupta H, et al. Sparfloxacin-loaded PLGA nanoparticles for sustained ocular drug delivery. Nanomedicine. 2010;6(2):324–33.
Pillai RR, et al. Nafcillin-loaded PLGA nanoparticles for treatment of osteomyelitis. Biomed Mater. 2008;3(3):034114.
Golub JS, et al. Sustained VEGF delivery via PLGA nanoparticles promotes vascular growth. Am J Physiol Heart Circ Physiol. 2010;298(6):H1959–65.
Yilgor P, Hasirci N, Hasirci V. Sequential BMP-2/BMP-7 delivery from polyester nanocapsules. J Biomed Mater Res A. 2010;93(2):528–36.
Liang G. F., Zhu Y. L., Sun B., Hu F. H., Tian T., Li S. C., and Xiao Z. D. PLGA-based gene delivering nanoparticle enhance suppression effect of miRNA in HePG2 cells. Nanoscale research letters. 2011;6(1):1–9.
Babar IA, et al. Nanoparticle-based therapy in an in vivo microRNA-155 (miR-155)-dependent mouse model of lymphoma. Proc Natl Acad Sci USA. 2012;109(26):E1695–704.
Gomes RS, et al. Efficient pro-survival/angiogenic miRNA delivery by an MRI-detectable nanomaterial. ACS Nano. 2013;7(4):3362–72.
Kosaka N, et al. Secretory mechanisms and intercellular transfer of microRNAs in living cells. J Biol Chem. 2010;285(23):17442–52.
Ohshima K, et al. Let-7 microRNA family is selectively secreted into the extracellular environment via exosomes in a metastatic gastric cancer cell line. PloS one. 2010;5(10):e13247.
Théry C. Exosomes: secreted vesicles and intercellular communications. F1000 Biol Rep. 2011;3(15):130.
Torchilin VP. Lipid-core micelles for targeted drug delivery. Curr Drug Deliv. 2005;2(4):319–27.
Markman M. Pegylated liposomal doxorubicin in the treatment of cancers of the breast and ovary. Expert Opin Pharmacother. 2006;7(11):1469–74.
Strother R, Matei D. Pegylated liposomal doxorubicin in ovarian cancer. Ther Clin Risk Manag. 2009;5(3):639–50.
Akinc A, et al. A combinatorial library of lipid-like materials for delivery of RNAi therapeutics. Nat Biotechnol. 2008;26(5):561–9.
Muggia FM. Clinical efficacy and prospects for use of pegylated liposomal doxorubicin in the treatment of ovarian and breast cancers. Drugs. 1997;54(Suppl 4):22–9.
Muggia FM, et al. Phase II study of liposomal doxorubicin in refractory ovarian cancer: antitumor activity and toxicity modification by liposomal encapsulation. J Clin Oncol: official journal of the American Society of Clinical Oncology. 1997;15(3):987–93.
Safinya CR, Ewert KK. Materials chemistry: Liposomes derived from molecular vases. Nature. 2012;489(7416):372–4.
Wu Y, et al. MicroRNA delivery by cationic lipoplexes for lung cancer therapy. Mol Pharm. 2011;8(4):1381–9.
DeSano JT, Xu L. MicroRNA regulation of cancer stem cells and therapeutic implications. AAPS J. 2009;11(4):682–92.
Hanai K, et al. Atelocollagen-mediated systemic DDS for nucleic acid medicines. Ann N Y Acad Sci. 2006;1082:9–17.
Miyata T, Taira T, Noishiki Y. Collagen engineering for biomaterial use. Clin Mater. 1992;9(3–4):139–48.
Minakuchi Y, et al. Atelocollagen-mediated synthetic small interfering RNA delivery for effective gene silencing in vitro and in vivo. Nucleic Acids Res. 2004;32(13):e109.
Svintradze DV, Mrevlishvili GM. Fiber molecular model of atelocollagen-small interfering RNA (siRNA) complex. Int J Biol Macromol. 2005;37(5):283–6.
Nakasa T, et al. Acceleration of muscle regeneration by local injection of muscle-specific microRNAs in rat skeletal muscle injury model. J Cell Mol Med. 2010;14(10):2495–505.
Takeshita F, et al. Systemic delivery of synthetic microRNA-16 inhibits the growth of metastatic prostate tumors via downregulation of multiple cell-cycle genes. Mol Ther: the journal of the American Society of Gene Therapy. 2010;18(1):181–7.
Tazawa H, et al. Tumor-suppressive miR-34a induces senescence-like growth arrest through modulation of the E2F pathway in human colon cancer cells. Proc Natl Acad Sci USA. 2007;104(39):15472–7.
Nagata Y, et al. Induction of apoptosis in the synovium of mice with autoantibody-mediated arthritis by the intraarticular injection of double-stranded MicroRNA-15a. Arthritis Rheum. 2009;60(9):2677–83.
Takei Y, et al. The metastasis-associated microRNA miR-516a-3p is a novel therapeutic target for inhibiting peritoneal dissemination of human scirrhous gastric cancer. Cancer Res. 2011;71(4):1442–53.
Osaki M, et al. MicroRNA-143 regulates human osteosarcoma metastasis by regulating matrix metalloprotease-13 expression. Mol Ther: the journal of the American Society of Gene Therapy. 2011;19(6):1123–30.
Shoji T, et al. The effect of intra-articular injection of microRNA-210 on ligament healing in a rat model. Am J Sports Med. 2012;40(11):2470–8.
Kaasgaard T, Andresen TL. Liposomal cancer therapy: exploiting tumor characteristics. Expert Opin Drug Deliv. 2010;7(2):225–43.
Kato Y, Sawata SY, Inoue A. A lentiviral vector encoding two fluorescent proteins enables imaging of adenoviral infection via adenovirus-encoded miRNAs in single living cells. J Biochem. 2010;147(1):63–71.
Wang Y, et al. Nanoparticle-based delivery system for application of siRNA in vivo. Curr Drug Metab. 2010;11(2):182–96.
Bergen JM, et al. Gold nanoparticles as a versatile platform for optimizing physicochemical parameters for targeted drug delivery. Macromol Biosci. 2006;6(7):506–16.
Han G, Ghosh P, Rotello VM. Multi-functional gold nanoparticles for drug delivery. Adv Exp Med Biol. 2007;620:48–56.
Papasani MR, Wang G, Hill RA. Gold nanoparticles: the importance of physiological principles to devise strategies for targeted drug delivery. Nanomedicine. 2012;8(6):804–14.
Ghosh R, et al. A gold nanoparticle platform for the delivery of functional microRNAs into cancer cells. Biomaterials. 2013;34(3):807–16.
Shan Y, et al. Gene delivery using dendrimer-entrapped gold nanoparticles as nonviral vectors. Biomaterials. 2012;33(10):3025–35.
Shukla R, et al. Biocompatibility of gold nanoparticles and their endocytotic fate inside the cellular compartment: a microscopic overview. Langmuir: the ACS journal of surfaces and colloids. 2005;21(23):10644–54.
Rosi NL, et al. Oligonucleotide-modified gold nanoparticles for intracellular gene regulation. Science. 2006;312(5776):1027–30.
Demers LM, et al. A fluorescence-based method for determining the surface coverage and hybridization efficiency of thiol-capped oligonucleotides bound to gold thin films and nanoparticles. Anal Chem. 2000;72(22):5535–41.
Giljohann DA, et al. Oligonucleotide loading determines cellular uptake of DNA-modified gold nanoparticles. Nano Lett. 2007;7(12):3818–21.
Crew E, et al. MicroRNA conjugated gold nanoparticles and cell transfection. Anal Chem. 2012;84(1):26–9.
Bravo V, et al. Instability of miRNA and cDNAs derivatives in RNA preparations. Biochem Biophys Res Commun. 2007;353(4):1052–5.
van Etten EW, et al. Administration of liposomal agents and blood clearance capacity of the mononuclear phagocyte system. Antimicrob Agents Chemother. 1998;42(7):1677–81.
Baum C, et al. Mutagenesis and oncogenesis by chromosomal insertion of gene transfer vectors. Hum Gene Ther. 2006;17(3):253–63.
Bouard D, Alazard-Dany D, Cosset FL. Viral vectors: from virology to transgene expression. Br J Pharmacol. 2009;157(2):153–65.
Brown BD, et al. In vivo administration of lentiviral vectors triggers a type I interferon response that restricts hepatocyte gene transfer and promotes vector clearance. Blood. 2007;109(7):2797–805.
Lesina E, Dames P, Rudolph C. The effect of CpG motifs on gene expression and clearance kinetics of aerosol administered polyethylenimine (PEI)-plasmid DNA complexes in the lung. J Control Release: official journal of the Controlled Release Society. 2010;143(2):243–50.
Mizrak A, et al. Genetically engineered microvesicles carrying suicide mRNA/protein inhibit schwannoma tumor growth. Mol Ther: the journal of the American Society of Gene Therapy. 2013;21(1):101–8.
Zintchenko A, et al. Drug nanocarriers labeled with near-infrared-emitting quantum dots (quantoplexes): imaging fast dynamics of distribution in living animals. Mol Ther: the journal of the American Society of Gene Therapy. 2009;17(11):1849–56.
Merdan T, et al. PEGylation of poly(ethylene imine) affects stability of complexes with plasmid DNA under in vivo conditions in a dose-dependent manner after intravenous injection into mice. Bioconjug Chem. 2005;16(4):785–92.
Kang E, Yun CO. Current advances in adenovirus nanocomplexes: more specificity and less immunogenicity. BMB Rep. 2010;43(12):781–8.
Arnberg N. Adenovirus receptors: implications for tropism, treatment and targeting. Rev Med Virol. 2009;19(3):165–78.
Godin B, et al. Multistage nanovectors: from concept to novel imaging contrast agents and therapeutics. Acc Chem Res. 2011;44(10):979–89.
Serda RE, et al. Multi-stage delivery nano-particle systems for therapeutic applications. Biochim Biophys Acta. 2011;1810(3):317–29.
Godin B, et al. multistage nanovectors: from concept to novel imaging contrast agents and therapeutics. Acc Chem Res. 2011;44(10):979–989.
Ferrari M. Cancer nanotechnology: opportunities and challenges. Nature reviews. Cancer. 2005;5(3):161–71.
Sakamoto J, et al. Antibiological barrier nanovector technology for cancer applications. Expert Opin Drug Deliv. 2007;4(4):359–69.
Geers B., De Wever O., Demeester J., Bracke M., De Smedt S. C., and Lentacker I. Targeted Liposome‐Loaded Microbubbles for Cell‐Specific Ultrasound‐Triggered Drug Delivery. Small. 2013;9(23):4027–4035.
Vader P, et al. Targeted delivery of small interfering RNA to angiogenic endothelial cells with liposome-polycation-DNA particles. J Control Release: official journal of the Controlled Release Society. 2012;160(2):211–6.
Geng J, et al. Conjugated polymer and gold nanoparticle co-loaded PLGA nanocomposites with eccentric internal nanostructure for dual-modal targeted cellular imaging. Small. 2012;8(15):2421–9.
Ferrari M. Vectoring siRNA therapeutics into the clinic. Nat Rev Clin Oncol. 2010;7(9):485–6.
Sengupta S, et al. Temporal targeting of tumour cells and neovasculature with a nanoscale delivery system. Nature. 2005;436(7050):568–72.
Chen JD, Wang Y, Chen X. In situ fabrication of nano-hydroxyapatite in a macroporous chitosan scaffold for tissue engineering. J Biomater Sci Polym Ed. 2009;20(11):1555–65.
Martin FJ, et al. Acute toxicity of intravenously administered microfabricated silicon dioxide drug delivery particles in mice: preliminary findings. Drugs R D. 2005;6(2):71–81.
Low SP, et al. Evaluation of mammalian cell adhesion on surface-modified porous silicon. Biomaterials. 2006. 27(26):4538–46.
Goh AS, et al. A novel approach to brachytherapy in hepatocellular carcinoma using a phosphorous32 (32P) brachytherapy delivery device–a first-in-man study. Int J Radiat Oncol Biol Phys. 2007;67(3):786–92.
Decuzzi P, Ferrari M. Design maps for nanoparticles targeting the diseased microvasculature. Biomaterials. 2008;29(3):377–84.
Decuzzi P, et al. A theoretical model for the margination of particles within blood vessels. Ann Biomed Eng. 2005;33(2):179–90.
Decuzzi P, et al. Intravascular delivery of particulate systems: does geometry really matter? Pharm Res. 2009;26(1):235–43.
Godin B, et al. An integrated approach for the rational design of nanovectors for biomedical imaging and therapy. Adv Genet. 2010;69:31–64.
Anderson SHC, et al. Dissolution of different forms of partially porous silicon wafers under simulated physiological conditions. physica status solidi (a). 2003;197(2):331–335.
Canham LT, et al. Derivatized mesoporous silicon with dramatically improved stability in simulated human blood plasma. Adv Mater. 1999;11(18):1505–1507.
Chiappini C, et al. Tailored porous silicon microparticles: fabrication and properties. Chemphyschem. 2010;11(5):1029–35.
Kasinski AL, Slack FJ. Epigenetics and genetics. MicroRNAs en route to the clinic: progress in validating and targeting microRNAs for cancer therapy. Nat Rev Cancer. 2011;11(12):849–64.
Cheng CJ, Saltzman WM. Polymer nanoparticle-mediated delivery of microRNA inhibition and alternative splicing. Mol Pharm. 2012 May 7;9(5):1481–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Fernandez-Moure, J., Van Eps, J., Weiner, B., Ferrari, M., Tasciotti, E. (2014). MicroRNA and Drug Delivery. In: Singh, S., Rameshwar, P. (eds) MicroRNA in Development and in the Progression of Cancer. Springer, New York, NY. https://doi.org/10.1007/978-1-4899-8065-6_19
Download citation
DOI: https://doi.org/10.1007/978-1-4899-8065-6_19
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4899-8064-9
Online ISBN: 978-1-4899-8065-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)