
Abstract
We studied 58 cases of linear scleroderma of the face: 20 of them showed transition into progressive facial hemiatrophy (PFH). In several cases a distinction between these two conditions was not possible since the atrophic changes were arranged along the previous indurations, usually along the branches of trigeminal nerve. Neurological manifestations, most often epilepsy, were found in about 10% cases of PFH, and were similar in childhood cases of scleroderma en coup de sabre. The shrinking of deeper tissue and bone deformities were observed by early onset of the disease, not infrequently after trauma. In both scleroderma en coup de sabre and PFH, neurological complications are probably related to vascular involvement.
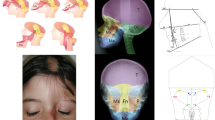
The double lines at the frontal area in 4 children were associated with epilepsy and usually pronounced deformities, whereas double lines in young adults did not produce evident wasting and shrinking.
Our study showed a close relationship of PFH with linear scleroderma of the face, and deep atrophies were comparable to the shrinking of subcutis and muscle in profound linear scleroderma of the limbs. There are however rare cases of PFH associated with atrophy of the brain and severe neurological manifestations. Their relationship with scleroderma is not known.
Progressive facial hemiatrophy (PFH) is a sporadic disease characterized by unilateral shrinking and deformity of the face, and which is associated at least in 10% of cases with central nervous system involvement [1,2]. The etiology of this condition is unknown. A frequent coexistence with linear scleroderma of the face, morphea and linear scleroderma on various sites of the body suggests a close relationship of these conditions. [3-5].
In several cases overlapping symptoms of both conditions made a definite distinction impossible [6]. It is believed that while in PFH the primary disorder is atrophy of the subcutaneous tissue, muscle and bone without skin induration, in scleroderma sclerosis and atrophy affect primarily the skin and subcutaneous tissues, and only later pass to the deeper tissue. The atrophic changes tend to be band-like and arranged along the previous indurations, whereas in PFH they are often more confluent. However not infrequently the lesions recognized as PFH occupied limited areas resembling involutionary scleroderma. Neurological manifestations, epilepsy and occasional ocular and auditory complications, my be similar in both diseases [7–9], and in both may involve various levels of cerebrospinal and sympathetic nervous system [10–12]. PFH, both secondary to scleroderma and seemingly idiopathic, is localized mainly along branches of trigeminal nerve, with involvement of sympathetic fibers of this nerve and cervical sympathetic ganglia (1, 13). Cerebral changes both in scleroderma en coup de sabre and PFH are mainly related to vascular involvement (neurovasculitis) [2, 13].
We present 4 children with double lines of scleroderma en coup de sabre at the frontal area (Figure 1). In all of these children the disease started at the very early age, in most of them after trauma, believed to be responsible for neurologic injury [14]. Linear scleroderma of the face, by its onset in infancy, has a greater tendency to produce deep atrophy and bone deformities with not infrequent transformation into PFH. In all children with double lines epilepsy appeared in infancy. Only in one girl, did the double lines appear at the age of 14 years, 7 years after trauma due to a car accident, concurrently with epilepsy (Table 1). Epilepsy was also present in a girl with a single, but very deep and large line. When the onset of scleroderma en coup de sabre occurs later in life (Figure 2), the wasting of the tissue and bone deformities were less pronounced, and the central nervous system involvement slight and unusual (Table 2). Thus epilepsy is associated with scleroderma en coup de sabre or PFH occurs mostly in childhood onset of the diseases.
The wasting of the subcutaneous tissue, muscle and bones in PFH is similar to the shrinking and deformities of the limbs that occur in profound linear scleroderma. PFH with no preceding indurations might be a counterpart of primary profound atrophic morphea. Deep subcutaneous atrophy as well as atrophy of the muscles of the trunk, limited to the C3-T2 dermatome, but with no involvement of the face, has been described as PFH [15]. Such primary profound atrophy at various sites of the body may be arbitrarily classified either under primary atrophic scleroderma or PFH. Thus, the majority of PFH cases could be recognized as involutionary linear scleroderma. Prognosis should be guarded when onset of the disease occurs at infancy and following trauma. Appearance of double lines, concurrently or consecutively, is associated with a more severe course in children, whereas in adults this does not appear to affect the course of the disease.
Although the most cases of PFH are closely related with scleroderma en coup de sabre, there are rare cases of primary hemiatrophy associated with brain atrophy, and severe neurological manifestations (such as facial palsy, hemiplegia, enophtalmos etc.)
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
Preview
Unable to display preview. Download preview PDF.
Similar content being viewed by others


References
Terstagge K, Henkes H, Kunath B, Felber S, Uhrmeister P, Kern A. Zerebrale Manifestation der progressive fazialen Hemiatrophie (Romberg-Erkrankung). Radiologe 33: 585–595 (1993)
Terstagge K, Kunath B, Felber S, Speciali JG, Henkens H, Hosten N. MR of brain involvement in progressive facial hemiatrophy (Romberg’s disease): reconsideration of a syndrome. Am J Neuroradiol 15: 145–150(1994)
Jablonska S. Facial hemiatrophy and its relation to localized scleroderma. In: Jablonska S. Scleroderma and Pseudoscleroderma. PZWL, Warszawa pp. 537–548 (1975)
Jablonska S, Rodnan GR Localized scleroderma. Clin Rheum Dis 5: 215–241 (1976)
Menni S, Marzano AV, Passoni E. Neurologic abnormalities in two patients with facial hemiatrophy and sclerosis coexisting with morphea. Pediatric Dermatol 14: 113–116 (1997)
Lehman TJA. The Parry Romberg syndrome of progressive facial hemiatrophy and linear scleroderma en coup de sabre. Mistaken diagnosis or overlapping conditions. J Rheum 19: 844–845 (1992)
Fry JA, Alvarellos A, Fink CW, Blow ME, Roach ES. Intracranial findings in progressive facial hemiatrophy. J Rheum 19: 956–958 (1992)
David J, Wilson J, Woo P. Scleroderma „en coup de sabre“. Ann Rheum Dis 50: 260–262 (1991)
Luer W, Jockei D, Henze T, Schipper HI. Progressive inflammatory lesions of the brain parenchyma in localized scleroderma of the head. J Neurol 237: 379–381 (1990)
Resende LA, Dal Pai V, Alves A. Étude expérimentale de l’hémiatrophie facial progressive effects de la sympathectomie cervical chez l’animal. Rev. Neurol 147: 609–611 (1991).
Cerinic MM, Generini S, Pignone A, Casale R. The nervous system in systemic sclerosis (scleroderma). Rheum Dis Clin North America 22: 879–892 (1996)
Averbuch-Heller L, Steiner I, Abramsky O. Neurologic manifestations of progressive systemic sclerosis. Arch Neurol 49: 1292–1295 (1992)
Pensler JM, Murrphy GF, Mulliken JB. Clinical and ultrastructural studies of Romberg’s hemifacial atrophy. Plas Reconstr Surg 85: 669–674 (1990).
Littman BH. Linear scleroderma: a response to neurologic injury? Report and literature review. J Rheumatol 16: 1135–1140 (1989)
Jappe U, Ring J. Parry-Romberg-Syndrom. Hautarzt 47: 599–603 (1996).
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 1999 Springer Science+Business Media New York
About this chapter
Cite this chapter
Blaszczyk, M., Jablonska, S. (1999). Linear Scleroderma En Coup De Sabre. In: Mallia, C., Uitto, J. (eds) Rheumaderm. Advances in Experimental Medicine and Biology, vol 455. Springer, Boston, MA. https://doi.org/10.1007/978-1-4615-4857-7_14
Download citation
DOI: https://doi.org/10.1007/978-1-4615-4857-7_14
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4613-7203-5
Online ISBN: 978-1-4615-4857-7
eBook Packages: Springer Book Archive