
Abstract
An imaging phantom is a specially designed physical object that is scanned or imaged in medical imaging to evaluate, analyze, and optimize the performance of various imaging modalities. These phantoms are readily available and provide more consistent results than the use of a living subject or cadaver; their use also serves to avoid subjecting a human subject to unnecessary radiation exposure.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- National Electric Manufacturer Association
- National Electric Manufacturer Association
- Radiochromic Film
- Quality Control Tool
- National Electric Manufacturer Association
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
An imaging phantom is a specially designed physical object that is scanned or imaged in medical imaging to evaluate, analyze, and optimize the performance of various imaging modalities. These phantoms are readily available and provide more consistent results than the use of a living subject or cadaver; their use also serves to avoid subjecting a human subject to unnecessary radiation exposure.
Imaging phantoms were originally designed for use in 2D X-ray-based imaging techniques such as radiography or fluoroscopy, and subsequently phantoms with desired imaging characteristics were developed for 3D imaging modalities such as magnetic resonance imaging (MRI), computed tomography (CT), ultrasound, positron emission tomography (PET), and other imaging modalities.
There are numerous phantoms which have been developed to test a variety of different physical parameters of imaging modalities or techniques. However, there are too many to be comprehensively covered in this chapter. We will focus on selected phantoms which meet the following criteria:
-
1.
Extensively tested with documentation and published data;
-
2.
Commercially and readily available;
-
3.
Recognized by the leading bodies in the medical physics and radiology communities, such as the American Association of Physicists in Medicine (AAPM), Institute of Physics and Engineering in Medicine (IPEM), American College of Radiology (ACR), International Atomic Energy Agency (IAEA), etc.
The construction of each of these phantoms will be discussed briefly followed by specific reference to their role in conventional X-ray imaging applications, including radiography and fluoroscopy. The phantoms are discussed according to the categories of anthropomorphic phantoms, acceptance testing and quality control (QC) phantoms, as well as vendor-specific phantoms. This chapter will end with a brief discussion on research phantoms which have the potential of contributing to diagnostic imaging development. The phantoms discussed in this chapter and their main applications are summarized in Table 6.1.
1 Anthropomorphic Phantom for X-ray Imaging
Anthropomorphic phantoms are ideal substitute for patient selection, monitoring, training, and optimization of scanning parameters of imaging modalities. They are useful for research and development involving in vitro experimental validation prior to clinical application in human. Phantoms permit unlimited repetition of radiation exposure for investigation or training purposes. Optimization of image quality and radiation exposure can be achieved by using suitable phantoms that replicate the human anatomy. Some anthropomorphic phantoms are used as QA tools for initial implementations of an imaging protocol and routine QC for the imaging modality.
1.1 Head/Neck Phantom
1.1.1 CIRS Dental and Diagnostic Head Phantom
The CIRS dental and diagnostic head phantom (CIRS Inc, USA) was designed for the selection, monitoring, training, and verification of scanning parameters common to most radiological procedures requiring fine anatomical details. The phantom is ideal for determining optimum system settings, commissioning new equipment, monitoring system performance, and training in dental and panoramic X-ray, as well as CT and cone beam CT examinations. The phantom is constructed of proprietary tissue-equivalent materials, ATOM Max. It is made of tissue-simulating resins mimicking the X-ray attenuation properties of human tissue for both CT and therapy energy ranges (50 keV to 25 MeV). The phantom approximates the average male human head in both size and structure. The phantom includes detailed 3D anthropomorphic anatomy such as brain, bone, larynx, trachea, sinus, nasal cavities, and teeth. The bones contain both cortical and trabecular separations. The teeth include distinct dentine, enamel, and root structure including the nerve (Fig. 6.1).

a The left lateral view of the CIRS dental and diagnostic head phantom. b Plain X-ray image of the phantom. (Images courtesy of CIRS Inc, USA)
1.2 Torso Phantoms
1.2.1 Alderson Lung/Chest Phantom
The Alderson lung/chest phantom (Radiology Support Device Inc, USA) extends from the neck to below the diaphragm. It is molded around a male skeleton, corresponding to the external body size of a patient, 175 cm tall and weighing 73.5 kg. The materials used to construct the phantom, known as the “RSD materials”, are equivalent to human bone and soft tissues. Animal lungs are selected to match the size of an adult male. Lungs are fixed in the inflated state and are molded to conform to the pleural cavities of the phantom. The pulmonary arteries are injected with a blood-equivalent plastic. The phantom with simulated left coronary artery reveals several areas of coronary artery irregularity and narrowing. The phantom is available either with the diaphragm permanently sealed to the interior of the phantom, fixing the lungs in place, or with a removable diaphragm, which permits the interchange of lungs and provides an unlimited number of configurations and disease simulations. The phantom is equipped with custom pathologies such as different sizes of nodules and pneumonia to demonstrate different pathological conditions of the lungs (Fig. 6.2).

The Alderson lung/chest phantom with removable diaphragm. (Image courtesy of Radiology Support Device Inc, USA)
1.2.2 Kyoto Kagaku Multipurpose Chest Phantom “LUNGMAN”
The Kyoto Kagaku chest phantom, also known as the “LUNGMAN” was developed by Kyoto Kagaku Co, Ltd, Japan. The phantom provides a life-size anatomical model of a human torso. It is a multipurpose phantom which is applicable for both plain radiography and CT imaging. The inner components of the phantom consisting of mediastinum, pulmonary vasculature, and an abdomen block are detachable to allow insertion of mimic tumors or other lesions. The X-ray properties of the soft tissue substitute material and synthetic bones are similar to human tissues. The 3D structure of the phantom allows both posterior–anterior (PA) and lateral images to be obtained (Fig. 6.3).

The multipurpose chest phantom Kyoto Kagaku “LUNGMAN”. a Positioning of the phantom for chest radiography. b The resulting phantom image. c Phantom with the chest plates to simulate a larger body size. d The inner components consisting of mediastinum, pulmonary vasculature, and an abdomen block are easily detachable, allowing insertion of mimic tumors or other lesions. (Images courtesy of Kyoto Kagaku Co, Ltd, Japan)
1.2.3 Gammex 610 Neonatal Chest Phantom
The Gammex 610 (Gammex Inc, USA) is an anthropomorphic neonatal phantom that represents a 1–2 kg neonate in its transmission characteristics, histogram, physical size, and structure. The phantom also contains clinically relevant image quality features for resolution and noise in the form of a lung with simulated pneumothorax with pleural thickening and a lung with simulated hyaline membrane disease. The phantom can be used for QA program for computed and digital radiography. Patient exposure is a concern especially in digital imaging where overexposed images could be post-processed to an acceptable level. The result often referred to as “dose creep” is especially relevant in pediatric imaging where some patients are imaged several times a day (Fig. 6.4).

The Gammex neonatal chest phantom (Model 610, Gammex Inc, USA) used for QA program for computed and digital radiography. (Image courtesy of Gammex Inc, USA)
1.2.4 CIRS 3D Torso Phantom
The CIRS anthropomorphic 3D torso phantom (CIRS Inc, USA) was designed for simulation of an average male torso for medical imaging applications. The removable organs enable the placement of dosimeters such as thermoluminescent dosimeters (TLDs) and contrast agents, etc. The phantom is fabricated using epoxy materials which have the optimal tissue simulation in the diagnostic energy range (40 keV to 20 MeV). The phantom is claimed to simulate the physical density and linear attenuation of actual tissue to within 2 % in the diagnostic energy range.
The phantom contains removable organs such as lungs, heart, liver, pancreas, kidney, and spleen. The lower portion of the phantom contains a removable, soft, bolus material simulating a mixture of 50 % adipose and 50 % muscle tissue. This insert is used to maintain the position of the organs when the phantom is placed upright. Simulated muscle material is used to layer the rib cage and vertebral column. The exterior envelope of the phantom simulates a mixture of 30 % adipose and 70 % muscle tissue. The phantom is sealed at the bottom by an acrylic plate. Water- or blood-mimicking fluid can be used to fill all the interstitial voids within the phantom (Fig. 6.5).

a The CIRS anthropomorphic 3D torso phantom (CIRS Inc, USA). b Plain X-ray image shows the anterior–posterior (AP) projection of the phantom. (Images courtesy of CIRS Inc, USA)
1.3 Whole Body Phantom
1.3.1 RANDO® Phantom
The RANDO® phantoms (The Phantom Laboratory Inc, USA) are constructed with natural human skeleton cast inside tissue-equivalent material. The soft tissue is manufactured with a proprietary urethane formulation with an effective atomic number and mass density that closely simulates muscle tissue with randomly distributed fat. There are two RANDO® models, RANDO® Man and RANDO® Woman. The RANDO® Man represents a 175-cm-tall and 73.5-kg male figure, whereas the RANDO® Woman represents a 163-cm-tall and 54-kg female figure. The RANDO® lungs are molded to fit the contours of the natural human rib cage. The lower density material in the RANDO® lungs is designed to simulate human lungs in a median respiratory state.
The RANDO® phantoms were initially designed for dose mapping applications in radiotherapy. However, its tissue equivalent properties and the whole body anatomy make it a useful phantom for diagnostic imaging applications especially for dose measurement and optimization. In vivo dose measurements can be done using radiochromic films or TLDs. To facilitate dose mapping, RANDO® phantoms are sliced into 2.5 cm sections and equipped with standard, close-fitting Mix D plugs inserted in the holes of each section. The radiochromic films and TLDs can be placed within these sections or holes (Fig. 6.6).

a The RANDO® Man. b The RANDO® Woman (Images courtesy of the Phantom Laboratory, Inc, USA)
2 Phantoms for Acceptance and QC Tests
The phantoms used for acceptance and QC tests are typically composed of material that mimics human tissue in its ability to produce absorption and scattering of radiation, i.e., they mimic radiopacity or radiolucency characteristics of human anatomy. Various phantoms have been developed for QC testing of conventional X-ray systems with respect to optical density, spatial resolution, and contrast detail. For example, a step wedge when radiographed produces a series of nearly uniform film areas with decreasing optical densities: line resolution phantoms that can be visually evaluated to estimate the smallest visible structure on film, and contrast detail phantom consisting of objects of decreasing size and contrast (circles or parallel lines) that can be visually evaluated to assess the detectability of the features on the X-ray image.
The general requirements of an acceptable test phantom are summarized as follows:
-
1.
The phantom material and thickness should simulate X-ray attenuation and scattering of human anatomy;
-
2.
The phantom setup should allow exposure in clinical setting. The phantom should be of appropriate size to represent realistic X-ray field and large enough to cover automatic exposure control (AEC) detectors;
-
3.
An ideal phantom should accommodate exposure or dose measurements during the QC test.
The following sections describe selected commercially available QC phantoms for both radiographic and fluoroscopic imaging systems.
2.1 Radiographic Systems
2.1.1 REX X-ray Test Phantom
The REX X-ray test phantom (PTW, Germany) is a reference phantom for QC of X-ray facilities for radiography and fluoroscopy. The phantom is suitable to be used for constancy tests and acceptance tests of X-ray equipments. It complies with the international standard IEC 61223-3-1 [1]. The phantom is constructed by a compact aluminum test object of 25 × 25 × 2.5 cm dimension with well-defined structures with respect to X-ray attenuation and image quality. The REX phantom provides fast and easy control of properties, adjustment, and stability of X-ray components and imaging systems (Fig. 6.7).

The REX X-ray test phantom (PTW, Germany). (Image courtesy of PTW, Germany)
2.1.2 “Duke” Phantom
The “Duke” phantom (Model 07-646, Nuclear Associates, USA) is a QC phantom for conventional and digital X-ray systems. It provides quantitative measurements for evaluation of image quality and performance of the complete integrated digital system. The “Duke” phantom was developed by Chotas et al. [2] from the Duke University Medical Centre, Durham, USA, in 1997. The phantom is constructed from sheets of copper and aluminum shapes resembling frontal radiographic projections of human thoracic structures (lungs, heart, ribs, and abdomen). The components are oriented and arranged to simulate a projection of a complete thorax and are then sandwiched between additional sheets of aluminum and acrylic. The top two corners of the phantom form “shoulders” which provide a region for direct X-ray exposure of the image receptor. The “Duke” phantom is equipped with regional test objects, contrast–detail test pattern, line-pair test pattern, and stainless steel wire mesh overlaying the entire chest area.
The “Duke” phantom can be used for the following purposes:
-
1.
QC testing of photostimulable storage phosphor CR systems
-
2.
Digital thoracic radiography systems based on a selenium detector
-
3.
Conventional screen–film systems
-
4.
Routine testing of phototimer performance in all chest imaging systems (Fig. 6.8).
Fig. 6.8 
The “Duke” QC phantom for conventional and digital chest X-ray. (Image courtesy of Fluke Biomedical, USA)

2.1.3 CIRS ACR Accreditation Radiography/Fluoroscopy (R/F) QA Phantom
The CIRS ACR accreditation R/F QA phantom (Model 903, CIRS Inc, USA) was designed for a comprehensive review of radiographic and fluoroscopic facilities and image quality programs. It was designed to be an integral part of the ACR R/F Accreditation Program. The phantom can be used for initial QA assessment and routine monthly QC testing to ensure optimal performance of the R/F systems. The phantom is manufactured from poly(methyl methacrylate) (PMMA)-equivalent epoxy that has the same X-ray attenuation properties as acrylic with significantly greater durability. The overall phantom measures 25 × 25 × 20.7 cm and consists of three attenuation plates, one test object plate and a detachable stand for reproducible setup. The test objects include high-resolution copper mesh targets from 12 to 80 lines per inch and two separate contrast detail test objects (Fig. 6.9).

The CIRS ACR accreditation R/F QA phantom (Model 903, CIRS Inc, USA). (Image courtesy of CIRS Inc, USA)
2.1.4 Radiography/Fluoroscopy QC Phantom
The R/F QC phantom (Model 07-647, Nuclear Associates, USA) was designed to provide a reproducible and quantitative method for evaluating the image quality and performance of radiographic and fluoroscopic imaging systems. The design of this phantom is based on the CDRH fluoroscopic phantom (refer Sect. 6.2.1.8). The phantom is used in determining subtle degradation in imaging performance. It can be used for QC of phototimer and automatic brightness control (ABC) consistency, as well as to verify the fluoroscopic monitor contrast and brightness adjustment. The phantom contains a 2 mm copper attenuator, which is simulating the attenuation of an average adult. The center of the phantom consists of pie-shaped wedges of varying mesh sizes for evaluating high-contrast performance. The meshes are surrounded by four low-contrast masses of different diameters ranging from 2 to 8 mm. There is a small “density difference” patch at one edge of the phantom to measure film contrast. At the opposite edge of the phantom, there are two monitor adjustment squares, each having a low-contrast square insert (Fig. 6.10).

The R/F QC phantom (Model 07-647, Nuclear Associates, USA). (Image courtesy of Fluke Biomedical, USA)
2.1.5 Leeds Test Objects
The Leeds test objects (Leeds Test Object Ltd, UK) are a collection of test objects or patterns which are used to assess the performance of a wide variety of X-ray imaging systems, including radiographic, fluoroscopic, digital, and mammographic systems. These objects, the first of which was manufactured in 1955, have been recommended as a clinical standard for establishing the correct operating performance of X-ray systems following their adoption for clinical use by the National Health Service (NHS), UK, in 1973 and as a testing protocol by the IPEM, UK, in 1979.
The general design and purposes of Leeds test tools are listed as following:
-
1.
High-contrast resolution mesh: used for the evaluation of the resolution of fluoroscopic imaging systems. Plastic plates containing eight groups of wire mesh screening. The wire mesh screening should be made of copper or brass in mesh sizes ranging from 9 to 23 lines per cm for conventional fluoroscopic units and from 12 to 39 lines per cm for evaluation of cinefluoroscopy units.
-
2.
Fluoroscopic threshold contrast test tool: used to provide a quantitative evaluation of fluoroscopic threshold contrast. It consists of two 15 × 15 cm × 6.3 mm thick aluminum plates. Each plate contains an array of 1.1 cm targets of varying contrast arranged in three columns. Three 15 × 15 cm × 1 mm copper attenuation sheets are also needed. Tables of target contrast versus kVp permit determination of target contrast at the tested fluoroscopic kVp values.
-
3.
Centering and alignment tool: used to determine perpendicularity of the central ray of the X-ray beam. The device should be a box or cylinder whose sides are perpendicular with its bottom to within 1 degree with a centrally located vertical wire.
-
4.
Beam restriction and sizing evaluation device: an aluminum plate with four sliding brass strips dividing the plate into quarters. Holes, at 12.7 mm intervals, should be drilled in perpendicular lines beneath the sliding brass strips. Recommended minimum size of 23 × 23 cm.
The variety of Leeds test objects with their product code, applications and standard compliance are summarized in Table 6.2.
Some examples of commonly used Leeds test objects are shown in Figs. 6.11, 6.12, 6.13, 6.14.

Examples of threshold contrast test object a TO 10 and b TO 12 for digital spot imaging systems. The test object has 108 details with a range of 12 sizes (ranged 11–0.25 mm) and nine contrasts (range 0.0043–0.540 at 70 kV, 1.0 mm Cu filtration). The results are plotted on a threshold detection index curve. (Images courtesy of Leeds Test Object Ltd, UK)

The TOR CDR phantom used for conventional and non-subtractive digital radiography and fluoroscopy systems. After an initial grayscale check, image quality is measured by counting the number of details detected and the number of bar patterns resolved in the image. It can be used for sensitometric measurement, resolution limit, low-contrast large-detail detectability, and high-contrast small-detail detectability. (Image courtesy of Leeds Test Object Ltd, UK)

a The Leeds test object set for digital subtraction fluorography (DSF). The set consists of four test objects: TO J3 used to check log/linear subtraction analog-to-digital converter (ADC) and digital-to-analog converter (DAC) operation, TO Q3 used to measure dynamic range of imaging capability, TO 20 to assess threshold contrast detail detectability, and TO D3 to detect systematic misregistration artefacts. b The DSF images of the Leeds test object (top left: TO 20; top right: TO D3; bottom left: TO J3; bottom right: TO Q3). (Images courtesy of Leeds Test Object Ltd, UK)

Leeds test object Fluoro-4 phantom used to check image quality performance of digital and conventional fluoroscopy systems. Fluoro-4 should be used with either PMMA/Cu or Al attenuator plates. It can be used for quantitative assessment of limiting spatial resolution, low-contrast resolution and dynamic range of imaging capability. (Image courtesy of Leeds Test Object Ltd, UK)
2.1.6 EZ CR/DR “DIN” Test Tool
The EZ CR/DR “DIN” test tool (Model 07-605-7777, Nuclear Associates, USA) is designed for evaluating the entire CR or DR image acquisition chain including laser beams, photomultiplier tubes, network gateways, and laser printers. It is suitable to be used as a preventive maintenance QC tool by taking regularly scheduled measured data points from the image, such as line-pair resolution measurements, ROIs, and geometry symmetry. The phantom allows a routine check on the dynamic range, contrast resolution, homogeneity, and resolution of the CR/DR systems. Quantitative measurement is applied to evaluate monitor as well as printed film image quality (Fig. 6.15).

Schematic diagram of the EZ CR/DR “DIN” test tool (Model 07-605-7777, Nuclear Associates, USA). (Image courtesy of Fluke Biomedical, USA)
2.1.7 Acrylic Phantoms for Diagnostic X-ray
The Joint Commission (TJC), USA, requires X-ray exposure measurements to be determined for commonly used projections in all radiographic suites [3]. In order to provide this information when using radiographic AEC or fluoroscopy ABC systems, specifically designed phantoms must be used. Attenuating material must be used between the focal spot and AEC or ABC detectors. Since these detectors are energy dependent, measurement of skin entrance exposure requires the use of patient-equivalent phantoms for meaningful results [4].
AAPM has recommended four special patient-equivalent phantoms for use in diagnostic radiology, i.e., chest, abdomen/lumbar spine, skull X-ray, and extremity X-ray phantoms. The phantoms have been developed by the ANSI using acrylic and the CDRH using Lucite and aluminum (LucAl). The phantoms are patient-equivalent and are specifically designed to conform to the AAPM recommendations. The designs of modified ANSI phantoms are summarized in Table 6.3.
2.1.8 CDRH LucAl Phantoms
The comparison between the modified ANSI phantoms and the CDRH phantoms has been carried out and documented in the AAPM Report No. 31. It is noted that the patient equivalency of the CDRH phantoms has been established clinically [4]. The designs and constructions of the CDRH LucAl phantoms are summarized in Table 6.4.
2.1.9 Dual-Energy X-ray Absorptiometry QC Phantom
2.1.9.1 CIRS “Bona Fide Phantom”
The CIRS BFP phantom is a QC tool for DEXA scanners, which features an acrylic-embedded calcium hydroxyapatite (CHA) step wedge. The phantom has a range of densities (0.7–1.5 g cm−2) with respect to clinical range of bone mineral density (BMD). The phantom uses a CHA insert for direct assessment of bone density accuracy. The CHA insert is compliant with Food and Drug Administration (FDA) guidelines for cross-calibration phantoms for clinical trials. The phantom is cast in acrylic and comes with its own carrying case. The case remains on the phantom during scanning and does not affect BMD readings, allowing rapid placement and removal for the phantom from the bed (Fig. 6.16).

The CIRS “Bona Fide Phantom” used for QC test in DEXA systems. (Image courtesy of CIRS Inc, USA)
2.2 Fluoroscopic Systems
2.2.1 CIRS Cardiovascular Fluoroscopic Benchmark Phantom
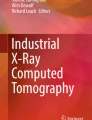
The CIRS cardiovascular fluoroscopic benchmark phantom (Model 901 NEMA-SCA&I, CIRS Inc, USA) was designed to evaluate and standardize catheterization image quality in cardiovascular fluoroscopy. It is the product of collaboration between the Society for Cardiac Angiography and Interventions (SCAI) and the National Electric Manufacturers Association (NEMA). The phantom configuration is compliant with the performance standard of NEMA XR 21 [5]. The phantom is manufactured from PMMA with X-ray absorption properties similar to soft tissue at diagnostic energies. It contains a variety of static and dynamic test targets for objective assessment of resolution, motion unsharpness, and radiation exposure. The sectional design allows for configuration of thicknesses from 5 to 30 cm, simulating PA thicknesses from infants to large adult patients (Fig. 6.17).

a Complete set of the CIRS cardiovascular fluoroscopic benchmark phantom (Model 901, CIRS Inc, USA). b Close-up view of the central target assembly (NE 01) and working thickness plate (NE 03) as part of the assembly of the phantom. (Image courtesy of CIRS Inc, USA)
2.2.2 Fluoroscopic Contrast Imaging Phantom
The fluoroscopic contrast imaging phantom (Model 07-643, Nuclear Associates, USA) is a test tool to evaluate image quality and optimal performance of a fluoroscopy system. It can be used to check the dynamic range of the video system and overall system performance, as well as the radiographic film range and density. The phantom has an outer diameter of 23 cm and thickness of 1.28 cm. It weighs 1.26 kg (Fig. 6.18).

a The fluoroscopy contrast imaging phantom (Model 07-643, Nuclear Associates, USA). b Plain X-ray image of the phantom. (Image courtesy of Fluke Biomedical, USA)
2.2.3 Fluoroscopic Imaging Test Phantom
The fluoroscopic imaging test phantom (Model 07-653, Nuclear Associates, USA) can be used to evaluate, adjust, and optimize fluoroscopic video cameras, brightness systems, and image processing systems. It provides a test pattern enabling the precise adjustment of many critical parameters of the fluoroscopic system such as video level, contrast, peak whites, black level, shading or vignette correction, automatic brightness, sweep linearity, frequency response, and aperture correction. The phantom has an outer diameter of 22.78 cm and thickness of 1.28 cm. It weighs 1.86 kg (Fig. 6.19).

The fluoroscopy imaging test phantom (Model 07-653, Nuclear Associates, USA). (Image courtesy of Fluke Biomedical, USA)
2.2.4 Ludlum Rotating Spoke Test Tool
The rotating spoke test tool (Model L-629, Ludlum Medical Physics, USA) was designed to evaluate the performance of the fluoroscopic imaging systems. The tool demonstrates screen image lag, motion blur, contrast, and related distortions encountered in fluoroscopic examinations. When combined with aluminum or acrylic block attenuators, the rotating spoke test tool enables simulation of the movement of guide wires and radiopaque catheters, seen in angiography or cardiac catheterization patient procedures. The rotating spoke test pattern consists of a circular acrylic disk of 13.97 cm diameter with 12 steel wires arranged on its surface in 30-degree intervals. The wire diameters range from 0.508 to 0.127 mm. There are 2 wires of each size directly opposite to each other on the disk. There are 6 lead objects (labeled with number 1 to 6) on each half of the disk near the perimeter. The disk is mounted on a synchronous motor with a speed of 30 rotations per minute (RPM) to simulate movement of the wires (Fig. 6.20).

The rotating spoke test tool (Model L-629, Ludlum Medical Physics, USA). (Image courtesy of Ludlum)
2.2.5 Ludlum Fluoroscopy Resolution Test Tool
The fluoroscopic resolution test tool (Model L-601, Ludlum Medical Physics, USA) is a square plastic plate (19 × 19 × 0.3 cm) containing eight groups of copper and brass mesh screening. The phantom is used for resolution checks of the fluoroscopic imaging systems There are three models of test tools available, each with different resolutions for standard-, medium-, and high-resolution ranging from 16 to 60 lines per inch, 30 to 100 lines per inch, and 60 to 150 lines per inch. The screens are arranged in an irregular and non-sequential rotation to permit better visualization of the different resolution patterns. The phantom can also be used to optimize television system focus as well as mirror optics and image intensifier settings (Fig. 6.21).

The fluoroscopic resolution test tool (Model L-601, Ludlum Medical Physics, USA). (Image courtesy of Ludlum)
3 Vendor-Specific QA Tools
3.1 Agfa Auto QC Tools
Auto QC2 (Agfa Healthcare, USA) is a QA program for verifying that the Agfa CR systems are working optimally and consistently. Auto QC2 can be used both for acceptance testing when setting up the CR systems, and for constancy testing for periodic QC. The Auto QC2 program includes a special designed phantom (hafnium phantom), positioning template, automated analyzing software, a filter unit, and a light field indicator. This test requires only a single phantom exposure for both spatial and contrast tests. The utilization of a rare-earth hafnium step wedge element in the phantom significantly reduces the exposure control issues that can affect QC tools employing only copper or aluminum. The phantom complies with the AAPM [3], IEC 61267 [6], and IEC 62220-1-1 [7] recommendations.
Auto QC2 can be used for five functional test groups:
-
1.
Acceptance testing: used for the initial setup of the CR system and for establishing an operational baseline standard.
-
2.
Periodic QC: a subset of the acceptance procedure, for monitoring the state of the CR system in routine use.
-
3.
Plate inventory: provides individual and statistical performance data on all imaging plates.
-
4.
Light field indicator: to check collimation accuracy of the X-ray exposure.
-
5.
Monitor check: to check the performance of the monitor in viewing CR images (Fig. 6.22).
Fig. 6.22 
The (a) internal construction and (b) X-ray image of the Hafnium phantom used in the Agfa Auto QC2 QA program. (Image courtesy of Agfa Healthcare, USA)

3.2 Carestream DirectView Total Quality Tool for DR/CR System
The DirectView TQT (Carestream Health Inc, USA) phantom and software provide a method to measure image quality in order to verify that all Carestream DR or CR detectors within a facility are operating within the specified range. This QC system enables performance of objective image tests and QC measurements with the same interface used for examinations. The system is equipped with administrative analysis and reporting software to monitor the IEC exposure index, TQT data, reject rates, and collect and review other data for all Carestream CR, DR, and DRX systems within a healthcare facility. The TQT can also be used to measure and verify the performance of individual cassettes used in the DirectView CR/DR Systems (Fig. 6.23).

The direct view TQT phantom (Carestream Health Inc, USA) used for QC tests for all Carestream DR or CR detectors. (Image courtesy of Carestream Health Inc, USA)
3.3 Fuji FCR 1 Shot Phantom
The Fuji FCR 1 Shot Phantom (Fujifilm, USA) enables a system-wide quality analysis by incorporating eight performance tests into a single exposure. The phantom provides valuable evaluation of the imaging plate, CR image reader, exposure room, hard copy printer, and imaging workstations (Fig. 6.24).

a The FCR 1 Shot Phantom (Fujifilm, USA). b Example of the CR image of the FCR 1 Shot phantom. (Image courtesy of Fujifilm, USA)
3.4 Fuji FCR 1 Shot Phantom Plus
The Fuji FCR 1 Shot Phantom Plus (Fujifilm, USA) is an advanced QC program with automated tests, software, and reports specifically for use with Fujifilm CR and DR systems as well as the QC workstations. This phantom, made of acrylic, is a quality analysis system incorporating extensive test parameters into an automated program. Visual and automated calculations can be performed through the user interface.
3.5 GE Quality Assurance Process
GE QAP (GE Healthcare, UK) is a QA program used primarily to check the overall performance of the digital radiography systems. The QAP consists of a series of tests that should be performed on a scheduled (weekly) basis. Most of the analysis and reporting features are included in the software as automated program. There are two types of quality tests: detector check and a full QAP test that requires exposures to be done on a flat-field phantom (Fig. 6.25).

a The QAP setup for a mobile DR system. The same setup can be used to assess both detector check and the full QAP tests. b The digital X-ray image of the flat-field phantom. (Images courtesy of GE Healthcare, UK)
4 Future Development on Imaging Phantoms
The optimal imaging performance and appropriate radiation dose of X-ray equipment should be routinely tested. However, most of the existing phantoms were developed to test film/screen and image intensifier systems. Recently, the film/screen or image intensifier techniques are being increasingly replaced by flat-panel detectors (FPDs). Unfortunately, the phantoms for the evaluation of such systems are generally vendor-specific and are not comparable across the different system, and their validity cannot be confirmed. Therefore, it is imperative that simple QC phantom be available for easy evaluation of FPD image performance across a variety of different systems.
Chida et al. [8] has recently developed a QC phantom to evaluate the spatial resolution, low-contrast resolution, and dynamic range on single (one-shot) X-ray exposures for FPD radiography and fluoroscopy. The phantom consists of three copper thicknesses (0.5, 1.5, and 3.0 mm), an aluminum step wedge (0.1 to 2.7 mm), and piano wire of various diameters (0.08 to 0.5 mm). The phantom is claimed to be simple, inexpensive, and useful for a routine QC of all FPD systems.
In addition, the use of vendor-specific QC program allows automatic processing and analysis of the radiographic images acquired, hence increases the objectivity of the system evaluation. In a QC program, the quality of the image is very useful to characterize the physical properties of the imaging chain. Therefore, specific phantoms that can be used to evaluate the images of CR or DR systems will be very useful. Mayo et al. [9] have developed a series of phantoms that can be used for this purpose. They have also developed specific software to analyze the phantom images obtained with digital processing techniques based on mathematical algorithms applied to the phantoms. The phantoms should include a wide range of image quality tests such as threshold contrast resolution, limiting spatial resolution, dynamic range, homogeneity zone, alignment accuracy, etc.
As the conventional QC tests are gradually being replaced by the vendor-specific QAP program, there is a need to develop an independent phantom or program to verify and compare across different QAP programs. Currently, there is no known standard protocol available to check the specification and performance of these vendor-specific QA programs. There is also no system capable of capturing QC data for comparison and monitoring across different QAP tools. Thus, it is imperative that an international guidelines or protocol needs to be developed to ensure proper implementation of the system.
There is an increased public awareness of radiation exposures, and therefore, there is a need for developing methods whereby all diagnostic imaging is properly performed in optimally maintained imaging equipment, and all patients’ radiation exposure is monitored. Several phantoms (anthropomorphic as well as mathematical phantoms) have been developed to assess radiation dosimetry in routine clinical examinations. These phantoms associated with calculation software are well established for advanced imaging techniques such as CT, nuclear medicine procedures, etc. At the present, radiographic and fluoroscopic dose records, as well as QC dose report, are almost entirely hand-recorded into paper logbooks typically at the operator’s control console or with DR systems manually retrieved from PACS [10]. However, fetching the whole series of such examinations from the PACS is time consuming, and more importantly, it is not possible to generate user- or protocol-specific radiation dose reports. Therefore, there is a trend toward developing standardized toolkits to automatically capture and integrate radiation dose records, QA, and QC report in a timely fashion [11, 10]. Several commercial dose monitoring and management systems are available today.
References
International Electrotechnical Commission. (1999). Evaluation and routine testing in medical imaging departments. Part 3-1: Acceptance tests—Imaging performance of X-ray equipment for radiographic and radioscopic systems. IEC 61223-3-1, International Electrotechnical Commission, Geneva, Switzerland.
Chotas, H. G., Floyd, C. E, Jr, Johnson, G. A., & Ravin, C. E. (1997). Quality control phantom for digital chest radiography. Radiology, 202, 111–116.
American Association of Physicists in Medicine. (1998). AAPM Report No. 60. Instrumentation requirements of diagnostic radiological physicist, AAPM.
American Association of Physicists in Medicine. (1990). AAPM Report No. 31. Standardized methods for measuring diagnostic X-ray exposures, AAPM.
National Electric Manufacturers Association. (2000). NEMA Standards Publication XR 21-2000: Characteristics of and test procedures for a phantom to benchmark cardiac fluoroscopic and fluorographic performance. In National Electric Manufacturers Association (Ed.), XR 21-2000, National Electric Manufacturers Association, Virginia, USA.
International Electrotechnical Commission. (2005). Medical diagnostic X-ray equipment: Radiation conditions for use in the determination of characteristics, IEC 61267. Geneva, Switzerland: International Electrotechnical Commission.
International Electrotechnical Commission. (2003). Medical electric equipment: Characteristics of digital X-ray imaging devices—Part 1: Determination of the detective quantum efficiency, IEC 62220-1. Geneva, Switzerland: International Electrotechnical Commission.
Chida, K., Kaga, Y., Haga, Y., Takeda, K., & Zuguchi, M. (2013). Quality control phantom for flat panel detector X-ray systems. Health Physics, 104, 97–101.
Mayo, P., Rodnenas, F., Marin, B., Campayo, J., G. V. (2009). Analysis of digital radiographic equipments with development of specific phantoms and software. In J. Sloter, et al. (Eds.), IFMBE Proceedings (pp. 425–428) Berlin, Heidelberg: Springer.
Ng K. H. (2013). Ensuring safety when transitioning to digital radiography in practice. In Proceedings of the international conference on radiation protection in medicine—Setting the scene for the next decade. International Atomic Energy Agency (IAEA), Bonn, Germany, Dec 3–7, 2012.
Wang, S., Pavlicek, W., Roberts, C. C., Langer, S. G., Zhang, M., Hu, M., et al. (2011). An automated DICOM database capable of arbitrary data mining (including radiation dose indicators) for quality monitoring. Journal of Digital Imaging, 24, 223–233.
Conway, B. J., Butler, P. F., Duff, J. E., Fewell, T. R., Gross, R. E., Jennings, R. J., et al. (1984). Beam quality independent attenuation phantom for estimating patient exposure from x-ray automatic exposure controlled chest examinations. Medical Physics, 11, 827–832.
Acknowledgments
We thank the manufacturers and suppliers of the phantoms and test tools described in this chapter for providing us with the necessary information regarding their products.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Web Resources
Web Resources
Majority of the phantoms’ description and specification were obtained from the manufacturers’ or suppliers’ official websites, as listed below:
Manufacturer/supplier | Official Website |
|---|---|
Agfa Healthcare, USA | |
Carestream Health, Inc., USA | |
Computerized Imaging Reference System (CIRS), Inc., USA | |
Fluke Biomedical, USA | |
Fujifilm, USA | |
Gammex, Inc., USA | |
General Electric (GE) Healthcare, UK | |
Kyoto Kagaku Co. Ltd, Japan | |
Leeds Test Objects Ltd, UK | |
Radiology Support Devices (RSD), Inc., USA | |
The Phantom Laboratory, USA |
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Ng, KH., Yeong, CH. (2014). Imaging Phantoms: Conventional X-ray Imaging Applications. In: DeWerd, L., Kissick, M. (eds) The Phantoms of Medical and Health Physics. Biological and Medical Physics, Biomedical Engineering. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8304-5_6
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8304-5_6
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8303-8
Online ISBN: 978-1-4614-8304-5
eBook Packages: Physics and AstronomyPhysics and Astronomy (R0)