
Abstract
Pancreatic cancer, one of the deadliest malignancies, is a complex disease consisting of heterogeneous cancer cells with deregulated signaling pathways and a myriad of microenvironment cells, including infiltrating immune cells and fibroblasts, that impact tumor growth and susceptibility to conventional chemotherapy. Understanding the signaling pathways that drive pancreatic cancer is crucial to the development of novel targeted therapies to combat the disease, which is largely refractory to conventional therapeutic options. Among these pathways are the Hedgehog, NOTCH, Wnt, MET, and TGF-β pathways that control not only bulk tumor growth, but also self-renewal of cancer stem cells and maintenance of the desmoplastic stroma characteristic of the disease. In addition to altered signaling pathways, many cells within the tumor microenvironment promote both tumor growth and serve as a barrier to chemotherapy. Here we will discuss how targeting these components of the disease may increase the efficacy with which it is treated.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Pancreatic Cancer
- Cancer Stem Cell
- Hepatocyte Growth Factor
- Epithelial Mesenchymal Transition
- Pancreatic Cancer Cell
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
The lethality of pancreatic can be attributed to the absence of early detection, the inherent aggressive nature of the tumor, and resistance to currently available standard therapies. Gemcitabine has historically been the cornerstone of systemic chemotherapy, with limited improvement with the addition of other cytotoxic chemotherapies. Recently, a three-drug regimen, FOLFIRINOX, was shown to improve clinical outcomes in a clinically significant way but at a cost of toxicity that limits broad application (Conroy et al. 2011). Despite these therapeutic options, the duration of response to chemotherapy is limited in patients with pancreatic cancer, indicating a need to develop novel therapies against the disease. In this chapter we will focus on developmental signaling pathways that play a critical role in pancreatic cancer which may serve as promising therapeutic targets. We will also discuss how we may potentially improve therapeutic efficacy and clinical outcomes by targeting the desmoplastic stroma characteristic of pancreatic cancer as well as the particularly virulent pancreatic cancer stem cell (CSC) subpopulation.
Targeting Developmental Signaling Pathways
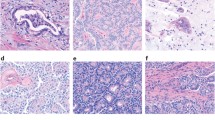
There is a distinct pattern of histologic changes in pancreatic tumorigenesis that begins with precursor pancreatic intraepithelial neoplasm (PanIN) lesions that eventually progress to invasive pancreatic ductal adenocarcinoma (PDAC). Specific mutations accompany these histologic changes, including KRAS mutations which can be found in the earliest PanIN lesions (i.e., PanIN-1) (Hezel et al. 2006). Ultimately, KRAS is mutated in greater than 95 % of pancreatic carcinomas. Other genetic changes commonly found in invasive pancreatic cancers such as mutations or deletions in the tumor suppressor genes p16/INK4A, p53, DPC4/SMAD4 also occur during PanIN progression to pancreatic cancer (Hezel et al. 2006). In addition to these and other genetic changes, there are molecular changes in pancreatic cancers that involve reactivation of developmental signaling pathways such as Hedgehog, NOTCH and Wnt. These developmental signaling pathways are included in a set of 12 core signaling pathways determined to be altered in pancreatic cancers through a comprehensive global genomic analysis (Jones et al. 2008). An average of 63 genetic alterations was found in pancreatic cancers, a majority of which were point mutations but also included deletions and amplifications. While distinct individual changes were seen within any given tumor, the specific alterations could be grouped into a set of 12 core signaling pathways including KRAS, TGF-β, Wnt/NOTCH/Hedgehog, cell cycle, and DNA repair genes (Jones et al. 2008). In the following section, we will discuss several of the developmental signaling pathways aberrantly activated in pancreatic cancer and describe their potential to serve as therapeutic targets.
The Hedgehog Signaling Pathway
The Hedgehog signaling pathway is vital for spatial patterning during embryonic development (Ingham and McMahon 2001). Hedgehog signaling has been shown to regulate cell fate specification (heart, skin, eye), cell proliferation (lung, muscle, neural crest), and cell survival (gonad) in different target cells (Ingham and McMahon 2001; Ruiz i Altaba et al. 2002a, b; Berman et al. 2003). Canonical activation of the Hedgehog signaling pathway begins with binding of one of the three hedgehog (HH) ligands (Sonic, Indian, and Desert) to the 12-transmembrane protein Patched (PTCH). In the absence of HH ligand, PTCH actively represses the activity of Smoothened (SMO), a seven transmembrane receptor-like protein (Fig. 1). HH ligand binding to PTCH inhibits its repression of SMO, allowing SMO to then transduce the signal internally via the GLI family of transcription factors (Rubin and de Sauvage 2006; Gupta et al. 2010). This results in transcriptional activation of hedgehog transcriptional genes such PTCH, GLI and Hedgehog Interaction protein HHIP.

The HH signaling pathway. The hedgehog signaling pathway is shown in three relevant scenarios: unstimulated cells (left), stimulated cells (middle), and pancreatic cancer cells (right). In unstimulated cells, PTCH inhibits the activity of SMO, resulting in inhibition of GLI-mediated transcription. In the presence of ligand (SHH), PTCH no longer inhibits SMO, which in turn inhibits SUFU and Cos2, resulting in GLI translocation to the nucleus and transcriptional activation of hedgehog signaling target genes. In pancreatic cancer cells, SHH is upregulated by oncogenic KRAS, which also blocks autonomous GLI activation through its effector, DYRK1B. Pancreatic cancer cell-secreted SHH stimulates neighboring cells, including pancreatic stellate cells
Aberrant Hedgehog signaling has been associated with cancer through several different mechanisms (Scales and de Sauvage 2009; Rubin and de Sauvage 2006). One mechanism of aberrant pathway activation is through mutation of a pathway component that allows for constitutive pathway activation in a ligand-independent manner. This is the pattern of activation seen in basal cell carcinomas, medulloblastomas, and rhabdomyosarcomas. Mutation of PTCH prevents it from its usual active inhibition of SMO, resulting in constitutive activation of SMO. By contrast, overexpression of HH ligand activates the HH signaling pathway in a ligand-dependent mechanism. This aberrant activation mechanism has been shown in multiple solid tumors including lung, stomach, esophagus, prostate, breast, liver, and pancreatic cancers (Rubin and de Sauvage 2006; Scales and de Sauvage 2009). While some early studies suggested potential autocrine activation of pancreatic tumor cells in response to increased HH ligand, a paracrine mechanism is now currently favored. In this model, tumor cells secrete Hedgehog ligand which binds to PTCH on neighboring cells in the tumor microenvironment in which Hedgehog signaling is then activated (Nolan-Stevaux et al. 2009).
In pancreatic cancer, ligand-dependent, canonical HH pathway activity is restricted to the stromal compartment (Lauth et al. 2010). In the tumor epithelial compartment of pancreatic cancer, the HH pathway appears to be activated by noncanonical upregulation of the effector transcription factor GLI1. Pancreatic cancer cells appear to be insensitive to HH ligand and in fact SMO is not required for pancreatic tumorigenesis (Nolan-Stevaux et al. 2009). Instead, GLI1 expression in pancreatic cancer epithelial cells is regulated by KRAS via its effector molecule DYRK1B, as well as by TGF-β signaling (Lauth et al. 2010; Nolan-Stevaux et al. 2009). While TGF-β signaling promotes the expression of GLI1 in pancreatic cancer cells, oncogenic KRAS and DYRK1B suppress its expression, limiting cell autonomous HH-signaling in pancreatic cancer cells (Lauth et al. 2010).
The normal adult pancreas does not normally express HH ligand, while expression of HH is a common feature of pancreatic cancer (Kim and Simeone 2011). Aberrant expression of HH ligand has been shown to occur as early as PanIn 1 lesions, with increasing levels expressed as these lesions progress to PDAC (Thayer et al. 2003). Sonic HH (SHH) is the dominant HH ligand expressed in pancreatic cancer and is aberrantly expressed in 70 % of patient tumors. A causal role for this aberrant SHH expression in pancreatic tumorigenesis is supported by evidence from a genetically engineered mouse model (Pdx-Shh) in which SHH is expressed in the pancreatic endoderm, resulting in development of abnormal tubular structures similar to human PanIN-1 and 2 lesions (Thayer et al. 2003). SHH has also been shown to play a critical role in formation and maintenance of the desmoplasia characteristic of pancreatic cancers (Bailey et al. 2008). Overexpression of SHH expression in a pancreatic epithelial cell line that forms xenograft tumors results in enhanced fibroblast infiltration. This fibrotic infiltration is accompanied by increased expression of the acellular components of the desmoplastic stroma, including collagen I and fibronectin (Bailey et al. 2008). HH signaling thus appears to play a role in the generation of the dense stroma that is seen in primary pancreatic tumors.
The formation of the dense stroma characteristic of pancreatic cancers appears to contribute to virulence of the cancer cells by promoting metastatic progression. It may also pose a physical barrier to drug delivery and contribute to the apparent resistance of pancreatic cancers to drug therapy. Given the above described role of the HH signaling pathway in the stroma of pancreatic cancers, blocking this pathway may facilitate improvement in drug efficacy by simply allowing greater penetration and drug delivery into tumor. Several novel agents that target the HH signaling pathway currently are in clinical development and share the general approach of inhibiting the SMO protein. HH pathway inhibition using a SMO antagonist has been studied in the KPC (KrasLSL.G12D/+; p53R172H/+; PdxCre) mouse model of pancreatic cancer, a well-studied model of pancreatic cancer that recapitulates human tumors, including formation of desmoplastic stroma (Olive et al. 2009; Hingorani et al. 2005). Treatment of KPC mice with the smoothened antagonist IPI-926, given in combination with the standard chemotherapy drug gemcitabine, produced a transient increase in tumor vascularity and intratumoral concentration of gemcitabine, leading to transient stabilization of disease (Olive et al. 2009). KPC mice treated with gemcitabine alone or IPI-926 alone showed no survival benefit in comparison with vehicle-treated controls; however, combination treatment with IPI-926 and gemcitabine extended the median survival of KPC mice from 11 to 25 days (p = 0.001) (Olive et al. 2009). Although the effects were transient, these results provided preclinical evidence that targeting the Hedgehog signaling pathway may increase response to chemotherapy. There are a number of other HH pathway inhibitors in clinical development which all target SMO, including LDE225 (Novartis), LEQ506 (Novartis), GDC-0449 (Genentech), and IPI-926 (Infinity Pharmaceuticals). These novel agents are currently being studied in early phase trials for patients with advanced pancreatic cancer in combination with chemotherapy (www.clinicaltrials.gov).
The NOTCH Signaling Pathway
NOTCH signaling plays an important role in cell fate and differentiation through effects on cell proliferation, survival and apoptosis (Artavanis-Tsakonas et al. 1995; D’Souza et al. 2008; Fiuza and Arias 2007). This pathway also regulates adult stem cell homeostasis and maintenance (Gridley 1997, 2003). The NOTCH signaling pathway involves activation of the NOTCH receptor by ligand. Five NOTCH ligands have been identified to date, which include Dll-1 (Delta-like1), Dll-3 (Delta-like3), Dll-4 (Delta-like4) (Bettenhausen et al. 1995; Dunwoodie et al. 1997; Shutter et al. 2000), Jagged-1, and Jagged-2 (Lindsell et al. 1995; Shawber et al. 1996). Four members of the NOTCH family of receptors have been identified, NOTCH1-4. Upon activation by one of these ligands, the NOTCH receptor is cleaved by the metalloprotease tumor necrosis factor α-convertase enzyme (TACE) and γ-secretase, releasing the intracellular domain of NOTCH (ICD) (Fig. 2). ICD translocates from the cell surface to the nucleus and binds the transcription factor CSL. In the absence of NOTCH pathway activation, CSL is free to bind to co-repressors which inhibit transcription (Kao et al. 1998; Hsieh et al. 1999; Morel et al. 2001). NOTCH pathway activation allows ICD to compete with inhibitory proteins to bind to CSL and to recruit co-activators, including p300, mastermind-like 1–3 (MAML1-3), and histone acetyltransferases. This process converts CSL from a transcriptional repressor to transcriptional activator (Zhou et al. 2000; Kurooka and Honjo 2000; Fryer et al. 2002, 2004). Several NOTCH target genes have been identified, including HES1 (hairy/enhancer of Split), c-Myc, cyclin D3, and p21WAF1 (Blaumueller et al. 1997).

The NOTCH signaling pathway. In NOTCH signaling, ligand-presenting cells stimulate the extracellular domain of NOTCH proteins (here on a pancreatic cancer cell) with either Delta-like (DLL) or Jagged family ligands. Upon stimulation, TACE and γ-secretase cleave NOTCH proteins, and the intracellular domain (ICD) translocates to the nucleus where it binds the transcription factor CSL and recruits coactivators like MAML. This promotes the transcription of NOTCH target genes
NOTCH1 was first characterized as an oncogene in human T-cell acute lymphoblastic leukemia (Reynolds et al. 1987) and subsequently in several epithelial tumors (Gallahan and Callahan 1997; Gallahan et al. 1996; Jhappan et al. 1992), including head and neck, breast, renal, lung, and colon cancers (Radtke and Raj 2003). In the pancreas, NOTCH signaling is normally suppressed in early development (Apelqvist et al. 1999; Jensen et al. 2000) but has been found to be upregulated in pancreatic cancer (Miyamoto et al. 2003). Further evidence supporting a causal role for aberrant NOTCH pathway activation in pancreatic cancer can be found from genetically engineered mouse models of pancreatic cancer. In the KRAS mouse model of pancreas cancer, NOTCH pathway activation can be seen in PanIN lesions (Hingorani et al. 2003). Co-expression of NOTCH1 with oncogenic KRAS in pancreatic acinar cells results in rapid and widespread transformation of acinar cells to duct-like cells and progression to aggressive, high-grade lesions (De La O et al. 2008).
Based on evidence of upregulation of NOTCH signaling in pancreatic cancer, targeting this pathway is of clinical interest for therapeutic application to patients with pancreatic cancer. The primary target for therapeutic intervention in the NOTCH signaling pathway thus far has been the enzyme γ-secretase, responsible for the last cleavage step of the NOTCH receptor that releases ICD. In preclinical studies, inhibition of NOTCH signaling by down regulation of NOTCH1 receptors using specific siRNA or γ-secretase inhibitors (GSI) reduced proliferation, increased apoptosis and decreased invasion of pancreatic cancer cells (Plentz et al. 2009; Mullendore et al. 2009; Wang et al. 2006). In KPC mice, treatment with the GSI, MRK-003 (Merck), attenuated the progression of PanIN lesions to PDAC (Plentz et al. 2009). A recent study exploring the effects of MRK-003 and gemcitabine in the same KPC mouse model of pancreatic cancer found the combined treatment reduced the proliferation of neoplastic cells, significantly induced endothelial cell death and reduced the density of intratumoral vessels (Cook et al. 2012). In this study it was proposed that the hypoxia caused by endothelial cell death sensitized the tumor cells to the effects of GSI by activating target genes such as survivin and NOTCH3 (Cook et al. 2012). This combination of MRK003/gemcitabine is currently being tested in an ongoing clinical trial in the United Kingdom. Another GSI, MK-0752 (Merck), is being tested in combination with gemcitabine in patients with advanced pancreatic cancer (www.clinicaltrials.gov).
The Wnt Signaling Pathway
Wnt-β-catenin signaling is required for morphogenesis, proliferation and differentiation of many organs. Wnt genes encode small, secreted proteins that are involved in many aspects of embryonic development and also control homeostatic self-renewal in a number of adult tissues (Clevers 2006; Willert and Jones 2006). To initiate pathway signaling, Wnt ligands (19 family members) bind to receptors of the Frizzled (Fzd) family (10 members), which in turn interact with transmembrane co-receptors LRP5/6 (Fig. 3). Activated LRP5/6 then recruits the protein, Dishevelled (Dsh), at which point Wnt signaling can branch into two different pathways, a canonical and noncanonical pathway. In the canonical pathway (Fig. 3), in the absence of Wnt, unstimulated cells regulate β-catenin levels by a multiprotein complex which phosphorylates β-catenin, leading to its subsequent ubiquitination and degradation. This β-catenin degradation complex consists of the adenomatous polyposis coli (APC) tumor suppressor protein, Axin, and the glycogen synthase kinase, GSK3β. Binding of Wnt to Fzd leads to inactivation of the degradation complex and accumulation of unphosphorylated β-catenin, which localizes to the nucleus. In the nucleus, β-catenin binds to TCF/LEF (T-cell factor/lymphoid enhancing factor) to activate downstream target genes (Willert and Jones 2006; Clevers 2006) (Fig. 3).

The Wnt signaling pathway. In canonical Wnt signaling, cells exist in either an unstimulated (left) or stimulated (right) state. In unstimulated cells, β-catenin is mostly complexed with E-cadherin, while free β-catenin is phosphorylated and degraded by a complex consisting of APC, Axin, and GSK3β. Upon stimulation by Wnt proteins, the Frizzled receptors and LRP5/6 co-receptors activate disheveled (Dsh), which inhibits the degradation complex, allowing β-catenin to translocate to the nucleus, bind to LEF/TCF, and promote target gene transcription. In pancreatic cancer, upregulation of ATDC promotes β-catenin stability through binding and stabilization of Dsh
Wnt also is activated by the “noncanonical” pathway which is independent of TCF/LEF and β-catenin. The “noncanonical” pathway is divided into two types: the Planar Cell Polarity (PCP) pathway and Wnt-Calcium pathway. In the PCP pathway, which has mostly been studied in Drosophila, Wnt signaling is transduced through Fzd independent of the co-receptors LRP5/6, leading to the activation of Dsh (Nishimura et al. 2012). Dsh, through Daam1 (Dishevelled associated activator of morphogenesis), mediates activation of Rho, Rock and JNK, inducing cytoskeletal changes important for cell polarization and motility during gastrulation (Nishimura et al. 2012; Kohn and Moon 2005). In the Wnt-Ca pathway, Wnt 5a and Wnt11, through activation of Fzd receptors, can stimulate intracellular Ca2+ release from the endoplasmic reticulum, which activates G-proteins without affecting β-catenin stabilization (Kohn and Moon 2005).
Several studies have proposed a role for the canonical Wnt pathway in pancreatic organogenesis. Evidence that Wnt/β-catenin signaling is important for the developing pancreas came from Heller et al. and others who have demonstrated expression of Wnt2b, Wnt 4, Wnt5a, Wnt7b and Frizzled receptors in the developing pancreas (Heller et al. 2002; Murtaugh et al. 2005). Later in development, the Wnt signaling pathway appears to promote proliferation and/or differentiation of acinar cells (Murtaugh et al. 2005; Wells et al. 2007; Morris et al. 2010). Wnt/β-catenin signaling may also be involved in maintaining normal islet cell development (Dessimoz et al. 2005).
The Wnt β-catenin pathway has been implicated as playing a key role in initiation and progression of cancer in many tissue types. The best studied pathway mutations are the inherited and sporadic mutations in the tumor suppressor APC. Monoallelic inactivating mutations in APC result in familial adenomatous polyposis (FAP), an inherited autosomal dominant condition leading to the development of multiple adenomas in the colorectum (Groden et al. 1991; Nishisho et al. 1991). Additionally, mutations in the gene encoding β-catenin (CTNNB1) are present in approximately 10 % of the remaining CRC tumors, mostly in early or smaller, less aggressive tumors (Samowitz et al. 1999). Loss of function mutations in APC or gain of function mutations in β-catenin are both rare in pancreatic cancer, except in the setting of pseudopapillary tumors in the pancreas, where mutations in β-catenin are driver mutations for the disease (Abraham et al. 2002). The contribution of aberrant Wnt signaling to pancreatic tumorigenesis was first demonstrated by Pasca di Magliano and colleagues, where they showed that the canonical arm of the Wnt pathway is induced in human PDA as well as in mouse models of pancreatic cancer. Wnt inhibition could block proliferation and apoptosis in cultured pancreatic adenocarcinoma cells (Pasca di Magliano et al. 2007).
In addition to the core components of canonical and noncanonical Wnt signaling, other novel regulators of Wnt signaling have been identified in pancreatic cancer. A recently identified oncogene in pancreatic cancer, the ataxia telangiectasia Group D associated gene (ATDC), has been shown to promote pancreatic tumor growth and metastasis, at least in part, through upregulation of the β-catenin signaling pathway (Wang et al. 2009a). ATDC was shown to bind and stabilize Disheveled-2, bringing it to the β-catenin degradation complex. Binding of ATDC and Disheveled-2 to the degradation complex results in inhibition of degradation complex, release of β catenin from the complex, and subsequent activation of the downstream target genes (Wang et al. 2009a). Another mechanism of activating the Wnt signaling pathway in pancreatic cancer involves Sulfs. The extracellular sulfatases, Sulf1 and Sulf2, act on internal glucosamine-6-sulfate (6S) modifications within heparan sulfate proteoglycans (HSPGs) and modulate HSPG interactions with various signaling molecules, including Wnt ligands (Nawroth et al. 2007).
The Wnt pathway can be potentially targeted at multiple levels, either by antibodies against Fzd or by the use of Wnt inhibitors. Antibodies directed against Fzd6 (clone 23M2) and Fzd5 (clone 44M13) have been shown to have antitumor properties (Deonarain et al. 2009). The inhibitor PRI-724 (Prism Biolabs), which blocks the interaction of β-catenin with CBP and is being tested in a phase 1 clinical trial in patients with advanced solid tumors, including pancreatic cancer (www.clinicaltrials.gov).
The MET Signaling Pathway
Embryogenesis, tissue repair, organ regeneration, and cancer invasion involves epithelial mesenchymal transition (EMT) (Kalluri 2009). This is stimulated by extracellular signaling which leads to modification of cellular proteins, intercellular junctional molecules and the cell cytoskeleton, leading to ordered cell migration and morphogenesis of new structures. One of the key signaling pathway that participates in these events is the hepatocyte growth factor (HGF) ligand and its receptor MET.
MET (also known as c-Met) is an integral plasma membrane protein that relays signals from the extracellular environment into the cytoplasm. MET, which is expressed by progenitors as well as epithelial and endothelial cells, is activated when its extracellular domain binds to HGF, also known as scatter factor (Sonnenberg et al. 1993). HGF is secreted predominantly by mesenchymal cells and bound in an inactive form to heparin proteoglycans within the extracellular matrix (Kobayashi et al. 1994; Lyon et al. 1994). HGF mRNA is also found in fibroblasts, smooth muscle cells, mast cells, macrophages, endothelial cells, leukocytes, and megakaryocytes (Zarnegar and Michalopoulos 1995). The HGF polypeptide is inactive in its initial form and must be cleaved into a disulfide-linked α-β heterodimer by an extracellular protease to acquire MET-binding activity (Zarnegar and Michalopoulos 1995).
Once HGF binds MET, its kinase activity is switched on by receptor dimerization and trans-phosphorylation of two catalytic tyrosine residues (Tyr1234 and Tyr1235) within the kinase activation loop (Trusolino et al. 2010). This leads to phosphorylation of two additional docking tyrosines in the carboxyl terminal tail; this site acts as a harbor for recruitment of several other signaling molecules. MET is negatively regulated by several protein-tyrosine phosphatases (PTP) which dephosphorylate either the catalytic or the docking tyrosines (PTP1, 2, 3) which prevents engagement of binding partners as well as downstream signaling (Trusolino et al. 2010) (Fig. 4).

The MET signaling pathway. In MET signaling, stromal (right) cell-secreted HGF binds to the MET receptor on pancreatic cancer cells (left). Upon ligand binding, MET dimerizes, autophosphorylates itself, and promotes signal transduction. Docking of GAB1 to phosphorylated MET promotes additional signal transduction. The cell surface molecule CD44 can promote MET signaling by interacting with MET and HGF outside the cell, as well as promoting RAS-signaling inside the cell. MET signaling ultimately drives metastasis, proliferation, and self-renewal of pancreatic cancer cells
MET signaling is augmented by a few other scaffolding partners, including GRB2-associated protein (GAB1) and CD44. GAB1 has a unique binding site for MET; upon binding and phosphorylation by MET receptor, GAB1 provides extra adapter sites for PI3K, SHP2, CRK, PLCγ1, and p120 Ras-GAP (Maroun et al. 2003; Maroun et al. 2000; Weidner et al. 1996). CD44 is a transmembrane cell adhesion molecule that activates MET in two ways; the extracellular domain tethers MET, HGF, and CD44, while the cytoplasmic tail helps to transduce signal from MET to Ras (Orian-Rousseau et al. 2002). Recently, ICAM-1 was identified as a new co-receptor for MET (Olaku et al. 2011), although the exact signaling mechanism has not yet been elucidated. Thus the basic signaling machinery of MET is regulated by a complex group of signal modifiers.
MET activates a cascade of downstream signaling pathways that include the MAP kinase PI3K-AKT, STAT, and NF-κB pathways (Trusolino et al. 2010) which function to modulate downstream gene expression. The mesenchymal-epithelial communication mediated by HGF-MET signaling integrates several pathways that control cell proliferation essential for normal processes such as embryogenesis, organ regeneration, and wound healing (Bhowmick et al. 2004; Boccaccio and Comoglio 2006). A role of MET in cancer was first noted in 1984, when it was cloned as a fusion oncogene from a human osteosarcoma cell line (Cooper et al. 1984). Germ line mutations in MET were observed in hereditary kidney cancer (Schmidt et al. 1997) and MET-activating mutations have also been observed in sporadic papillary renal cancer (Schmidt et al. 1997), childhood hepatocellular cancer (Park et al. 1999), and gastric cancer (Soman et al. 1991). More frequently, MET is overexpressed rather than mutated in cancer, as in colorectal (Takeuchi et al. 2003; Di Renzo et al. 1995a), hepatocellular (Suzuki et al. 1994), gastric (Amemiya et al. 2002), prostate (Humphrey et al. 1995), breast (Beviglia et al. 1997; Ghoussoub et al. 1998; Lee et al. 2005), and pancreatic cancers (Di Renzo et al. 1995b).
Evidence of MET/HGF upregulation in pancreatic cancer came from work in pancreatic cancer cell lines which showed that MET and HGF were overexpressed in a panel of 31 pancreatic cancer cell lines and were responsible for a “ductal” phenotype (Di Renzo et al. 1995b).In most pancreatic cancers, MET expression is transcriptionally upregulated and has been shown to be induced by hypoxia (Pennacchietti et al. 2003) and/or inflammatory cytokines in the tumor stroma (Bhowmick et al. 2004). The interaction between HGF and the MET receptor increases the rate of proliferation, invasion, migration, and angiogenesis of pancreatic cancer cells, and data suggest MET activation is a relatively late event in tumorigenesis that adds to the aggressiveness of the tumor by its proliferative, pro-apoptotic and pro-migratory signals (Trusolino et al. 2010).
MET is considered to be an important target in anticancer therapy because of its role in oncogenesis and cancer progression (Trusolino et al. 2010; Migliore and Giordano 2008; Sierra and Tsao 2011). Preclinical studies have shown that in animal models, the inhibition of MET or neutralization of its ligand impairs tumorigenic and metastatic properties of cancer cells (Li et al. 2011; Corso et al. 2008; McDermott et al. 2007). Recently, Li, and colleagues evaluated the role of MET in pancreatic cancer stem cell (CSC, reviewed later in the chapter) function (Li et al. 2011). Pancreatic cancer cells expressing high levels of MET cells had increased tumorigenic potential in mice, and cells that expressed MET and CD44 (0.5–5 % of the pancreatic cancer cells) had the capability for self-renewal and the highest tumorigenic potential of all cell populations studied. MET inhibition using the pharmacologic inhibitor XL184 or knockdown by shRNA slowed tumor growth and reduced the population of CSCs, either alone or in combination with gemcitabine. Additionally, targeting of MET prevented the development of metastases (Li et al. 2011). Based on this data, clinical trials targeting MET are currently in development.
The TGF-b Signaling Pathway
TGF-β is a multifunctional cytokine that controls cell growth, differentiation, proliferation, and angiogenesis, both during embryonic development and in adult tissues (Massague 1998). The TGF-β family contains two subfamilies, the TGF-β/Activin/Nodal subfamily and the bone morphogenetic protein (BMP)/growth and differentiation factor (GDF)/Muellerian inhibiting substance (MIS) subfamily, as defined by sequence similarity and the specific signaling pathways that they activate. The ligand family is comprised of three isoforms, TGF-β1, TGF-β2, and TGF-β3 (Massague 1998). TGF-β1 is expressed in epithelial, endothelial, hematopoietic and connective tissue cells; TGF-β2 is expressed in epithelial and neuronal cells and TGF-β3 is expressed in mesenchymal cells (Pasche 2001). There is 70–80 % homology among TGF-β isoforms which have different binding affinities to their tissue-specific receptors (Massague 1998). In general, they exhibit similar functions in vitro on cell growth regulation, ECM production and immune modulation. However, each ligand has distinct activities in vivo (Pasche 2001; Massague 1998).
To initiate signaling, TGF-β ligands interact with two receptors, TGFβRI and TGFβRII. TGF-β binds to TGFβRII, which then recruits and phosphorylates TGFβRI (Fig. 5). This allows activation and phosphorylation of SMAD2 and SMAD3. Phosphorylated SMAD2 and 3 then combine with SMAD4 to translocate into the nucleus (Massague 1998). Once in the nucleus, the SMAD complex can associate with cofactors to transcriptionally regulate target genes. In addition to SMAD dependent signaling pathways, TGF-β also activates many other signaling pathways such as PI3K (Krymskaya et al. 1997), MAPK (Hartsough and Mulder 1995), and the small GTPases Rho (Bhowmick et al. 2001), Cdc42 (Edlund et al. 2002), and Rac1 (Mucsi et al. 1996).

The TGF-β signaling pathway. Binding of TGF-β to TGFβRII promotes dimerization with and phosphorylation of TGFβRI. This leads to recruitment and phosphorylation of SMAD2/3, which in turn bind to SMAD4 and translocate to the nucleus to promote transcription of target genes. Additionally, repressor SMADs, like SMAD7, inhibit TGF-β signaling. In addition to driving transcription through SMAD2/3/4, TGF-β signaling also activates small GTPases like Rho, Rac1, and CDC42, which regulate cytoskeletal dynamics
SMAD4 (or Deleted in Pancreatic Cancer, locus 4/DPC4) inactivation through homozygous deletion or intragenic mutations are found in more than half of pancreatic cancers, (Jaffee et al. 2002). It is thought that loss of the SMAD4 expression is a rather late event in the pathogenesis of pancreatic cancer, with loss of SMAD4 expression occurring in 14.3 % of stage I pancreatic cancers and increasing to 60.0 % of stage IV pancreatic cancers (Hua et al. 2003). In a separate study, SMAD4 gene expression was found to be normal in PanIN1 and 2 lesions with loss of expression seen in 31 % of cases with PanIN3 (Wilentz et al. 2000).
Loss of expression of SMAD4 in pancreatic cancers has been associated with worse prognosis. Patients with cancers expressing the SMAD4 protein had significantly longer survival following surgical resection than patients in which SMAD4 expression was absent in their tumors (median survival of 19.2 months vs. 14.7 months; p = 0.03) (Tascilar et al. 2001). To further examine the role of SMAD4 in pancreatic tumorigenesis, several groups have used pancreatic-specific Cre recombinase strategies to study the role of SMAD4 loss in both initiation and promotion of pancreatic cancer (Izeradjene et al. 2007; Bardeesy et al. 2006). SMAD4 loss markedly promoted tumor development initiated by KrasG12D activation and KrasG12D/Smad4−/− tumors exhibited both increased proliferation and tumor stromal formation. These studies demonstrate that SMAD4 loss cannot alone initiate pancreatic tumor formation, but promotes pancreatic tumor progression and metastasis independent of TGF-β-mediated EMT (Malkoski and Wang 2012).
In addition to SMAD family members like SMAD4 that transduce TGF-β signaling, some SMAD family members, like SMAD6 and SMAD7, are inhibitory. SMAD7 has been shown to be overexpressed in greater than 50 % of pancreatic cancers (Arnold et al. 2004). Interestingly, low expression of SMAD7 in pancreatic tumors correlated with lymph node metastasis, liver metastasis after surgery, a poor survival rate and high MMP2 expression (p = 0.0004) (Wang et al. 2009b). These results would suggest a more complicated role for SMAD7 in pancreatic cancer, and not simply one of an oncogene. Several other molecules, like KLF11, retinoblastoma, and thioredoxin have been associated with SMAD7-dependent aggressiveness of pancreatic cancer (Ellenrieder et al. 2004; Arnold et al. 2004).
TGF-β signaling is complex in tumor development as it appears to have dual roles, with growth inhibitory function in early tumor development but apparent promotion of invasion and metastasis later in tumorigenesis. This latter role of TGF-β is the basis for interest in targeting this pathway in pancreatic cancer. Several inhibitory approaches have shown efficacy in preclinical and clinical studies. These include blocking production of TGF-β ligands with antisense molecules, small-molecule inhibitors of the kinase activity of TGFβRI and TGFβRII, monoclonal antibodies that block TGF-β signaling and soluble forms of TGFβRII and TGFβRIII that function as ligand traps (Flavell et al. 2010; Rowland-Goldsmith et al. 2001, 2002; Kelly and Morris 2010). In addition, combined therapies of small-molecule inhibitors with immune-stimulating vaccines represents an additional therapeutic approach that is being tested (Terabe et al. 2009). Another agent being utilized to target the TGF-β pathway in pancreatic cancer is trabedersen (AP 12009), a phosphorothioate antisense mRNA targeting TGF-β2 (Schlingensiepen et al. 2011). Using an orthotopic xenograft model, trabedersen was effective at inhibiting tumor cell growth and cell migration, while reversing TGF-β2-mediated immunosuppression of lymphokine activated killer (LAK) cells (Schlingensiepen et al. 2011). These data support the idea that the TGF-β is a desirable target in pancreatic cancer; however, further evaluation of these TGF-β inhibitory agents is necessary to assess actual efficacy in controlled clinical trials.
Stromal Biology and Therapeutic Targets
Pancreatic cancer characteristically has an abundantly dense stroma composed of a mixture of both cellular and acellular components including extracellular matrix proteins (ECM), growth factors, cytokines. The different cellular components include cells of mesenchymal and immune origin. In the following section, we will describe how these stromal cells contribute to pancreatic cancer growth and how they may be targeted.
Cancer-Associated Fibroblasts
The dense stroma found in pancreatic cancer appears to be formed through the actions of cancer-associated fibroblasts (CAFs) (Apte et al. 2004; Hwang et al. 2008). Current understanding of the actual cell of origin for CAFs is incomplete and although the term CAF is often used interchangeably with activated pancreatic stellate cells (PSCs), CAFs may also be derived from other cell types including infiltrating cells from the bone marrow (Direkze et al. 2004). Further demonstrating the complexity of CAFs is a recent study in human pancreatic tumors that identified a subpopulation of CAFs that are CD10+ which more robustly support tumor growth, highlighting the fact that CAFS represent a heterogeneous population of cells (Ikenaga et al. 2010). In addition to supporting enhanced tumorigenicity, CAFs appear to also contribute to resistance of pancreatic cancer cells to chemotherapy and radiation and promote metastatic spread (Hwang et al. 2008).
There have been multiple mechanisms proposed by which CAFS contribute to the tumor progression, including signaling pathways such as SDF-1/CXCR4 axis, the Hedgehog pathway (discussed previously), hypoxia-mediated signaling, and innate immunity. Stromal cell-derived factor-1 (SDF-1) is a member of the CXC subfamily of chemokines and interacts with its receptor CXCR4. SDF1-CXCR4 signaling has been implicated in the process of local invasion and distant metastasis of pancreatic cancer (Hermann et al. 2007). CAFs have been shown to express SDF-1, whereas CXCR4 is expressed by pancreatic cancer cells (Koshiba et al. 2000). Increased proliferation and metastatic spread of pancreatic cancer cells expressing CXCR4 can be abrogated by anti-SDF-1 neutralizing antibodies or the CXCR4 inhibitor AMD3100/plerixafor (Johnson Matthey), suggesting that the SDF-1/CXCR4 axis contributes to CAF stimulation of pancreatic cancer cells (Gao et al. 2010). In one study, pancreatic cancer cell lines treated with recombinant SDF-1 were resistant to gemcitabine, and this effect was reversed by blocking CXCR4 with AMD3100 (Singh et al. 2010). In addition, a potential important role of CXCR4 has been described in pancreatic CSCs, in which a subpopulation of CSCs expressing CD133 and CXCR4 were found to be highly invasive and responsible for metastasis (Hermann et al. 2007), further supporting the rationale for exploring SDF-1/CXCR4 for therapeutic targeting.
In addition to provided growth factors and chemoattractants that promote pancreatic cancer cell growth, the extremely dense stroma of pancreatic cancer serves to protect cells from chemotherapy by “crushing” blood vessels. Using a murine pancreatic cancer model, Olive and colleagues showed that the dense tumor stroma was driven by tumor cell-derived SHH which activated the Hedgehog pathway in stromal cells (Olive et al. 2009). By inhibiting SMO with IPI-926, blood vessels could be transiently reopened by decreasing the stroma, which allowed for enhanced efficacy of gemcitabine treatment (Olive et al. 2009). In addition to being driven by paracrine SHH signaling, the desmoplastic tumor stroma has also been shown to be sustained by excessive amounts of the extracellular matrix component, hyaluronic acid (hyaluronan) (Provenzano et al. 2012; Jacobetz et al. 2013). Provenzano and Jacobetz and their colleagues simultaneously reported that in murine pancreatic cancer models, hyaluronic acid in the stroma led to the collapse of tumor vasculature, which impeded drug delivery. Using a PEGylated form of the hyaluronic acid-degrading enzyme, PH20 hyaluronidase (PEGPH20), the authors were able to restore a normalized stroma and tumor vasculature. When combined with gemcitabine, PEGPH20 was able to substantially reduce tumor burden and extend animal survival (Provenzano et al. 2012; Jacobetz et al. 2013). Based on these findings, the tumor stroma can be thought of as both nurturing and protecting pancreatic cancer cells and a valuable target in pancreatic cancer therapy.
Hypoxia-Driven Signaling Pathways
Hypoxia is a common condition in zones of rapidly proliferating tumors which influences signaling pathways that control cell proliferation, angiogenesis, and apoptosis (Harris 2002). Hypoxia is also believed to be a prevalent state in pancreatic tumors due to hypovascularity that is concomitantly found within the dense stroma. Hypoxic conditions are also associated with resistance to chemotherapy and radiation therapy (Harris 2002; Yokoi and Fidler 2004). In pancreatic cancer, hypoxia confers multidrug resistance primarily through the PI3K/AKT/NF-κB pathway and partially through the MAPK signaling pathway (Yokoi and Fidler 2004). Inhibition of PI3K with the inhibitor LY294002 (Eli Lilly), in combination with a Chk1 inhibitor, UCN-01 (Tokyo Research Laboratories), has been shown to partially sensitize pancreatic cancer cells to cytotoxic chemotherapy under hypoxic conditions (Onozuka et al. 2011).
Immune Cells
Immune cells form an integral part of the tumor stroma and various types of immune cells have either tumor-promoting or tumor-antagonistic properties. The balance between these two properties contributes to tumor growth. Tumor-promoting cells include macrophages, mast cells, neutrophils, T and B lymphocytes (Ruffell et al. 2010; DeNardo et al. 2010). These cells are activated by a number of signaling molecules that have been extensively studied in different cell systems (Ruffell et al. 2010; Murdoch et al. 2008; Qian and Pollard 2010). Infiltration with immune cells has been observed in all stages of pancreatic cancer, from PanIN lesions to invasive cancer (Clark et al. 2007). These immune cells secrete a number of molecules that modulate tumor and stromal growth, including VEGF, FGF2, chemokines and cytokines, pro-angiogenic factors such as MMP-9 and other matrix metalloproteases, and heparinase (Murdoch et al. 2008; Qian and Pollard 2010; Hanahan and Weinberg 2011). Kraman and colleagues identified a specific subpopulation of stromal cells expressing fibroblast activation protein (FAP) that play a role in suppressing antitumor immunity (Kraman et al. 2010). Depletion of this subpopulation led to IFNγ and TNFα mediated modulation of tumor growth (Kraman et al. 2010). Pancreatic cancer cells are also responsible for recruiting immune cells to suppress the antitumor activity of CD8(+) T cells. Using murine models for pancreatic cancer, two groups simultaneously found that oncogenic KRAS results in the secretion of GM-CSF by pancreatic cancer cells, which in turn attracts Gr-1(+) CD11b(+) cells that can inhibit the activity of CD8(+) T cells in the tumor (Bayne et al. 2012; Pylayeva-Gupta et al. 2012). These data emphasize the complex nature of the immune system and tumor development and represent a venue to target to alter the immune suppressive environment that exists in pancreatic cancer.
Cancer Stem Cells
A subset of cancer cells has been identified in many solid tumors which has the capacity to efficiently propagate a new tumor with the heterogeneity and pathologic features of the original cancer. These cells are called CSCs because they share normal stem cell features such as self-renewal and the ability to undergo both symmetric and asymmetric cell division (Reya et al. 2001). Conventional therapies are directed at eliminating bulk tumor cells; however, these therapies are usually short-lived, and tumors eventually reestablish themselves. One reason for this phenomenon is that the CSCs are intrinsically resistant to cytotoxic chemotherapy and persist despite apparent response in bulk tumor (Kim and Simeone 2011). Therefore, understanding differences between CSCs and bulk tumor cells is relevant to improving overall efficacy of treatment.
CSCs were first described in acute myeloid leukemia (AML) as a distinct CD34+/CD38− population capable of both self-renewal and distinct progeny (Bonnet and Dick 1997). Subsequently, CSCs have been identified by surface marker analysis in solid tumors, including pancreatic cancer, with a first report demonstrating a subset of CD44+/CD24+/ESA + pancreatic CSCs (Li et al. 2007). Additionally, both CD133 and ALDH have been identified as potential independent markers for pancreatic CSCs (Hermann et al. 2007; Jimeno et al. 2009). Most recently, c-Met+/CD44+ pancreatic cancer cells have been described to potently enrich for a population of pancreatic CSCs (Li et al. 2011).
Although tumorigenesis is generally considered a clonal process, there is ultimately genetic diversity within an individual tumor (Marusyk and Polyak 2010). Recent detailed analysis of tumor cells from different metastatic sites within an individual patient confirmed that there are subclonal populations due to genomic instability (Campbell et al. 2010). We currently lack a detailed understanding of how genetic heterogeneity of pancreatic cancer correlates with the hierarchy of CSCs. Although one could view the complexity of genetic heterogeneity as an insurmountable barrier to the development of targeted therapies, an alternate view in the context of CSCs is that identifying the dominant signaling pathways in the CSC subpopulation is the key to eliminating the subpopulation of cells that may be most important for clinical progression and recurrence of disease. Based on this latter view, we describe below the results of increased attention focused on CSC biology, including the role of developmental signaling pathways and commonalities between CSC and cancer cells that have undergone EMT.
There are multiple signaling pathways that are upregulated in pancreatic CSCs that represent possible therapeutic targets. MET has recently been described as a potent marker for identifying pancreatic CSCs when studied in combination with CD44 expression (Li et al. 2011). This selective feature of CSC is now being targeted therapeutically with agents that inhibit MET. Treatment with the MET inhibitor XL184 has been shown in preclinical studies to reduce the percentage of pancreatic CSCs, decrease tumorsphere-forming capacity, and decrease in vivo tumorigenicity (Li et al. 2011). In addition to high levels of MET expression, Lonardo and colleagues found Nodal/Activin signaling to be elevated in pancreatic CSCs (Lonardo et al. 2011). By inhibiting the Nodal/Activin receptors Alk4/7 with the chemical inhibitor SB431542 or targeted siRNA, CSCs could be ablated in vitro. Additionally, the combination of SB431542 with gemcitabine and the SMO inhibitor CUR199691 could effectively ablate tumor growth in vivo (Lonardo et al. 2011). Together, HGF/MET and Nodal/Activin/Alk4 represent signaling pathways that may allow for the development of CSC-targeted therapies that can potentially be used in combination with standard chemotherapeutic regimens to reduce disease recurrence by specifically eliminating CSCs.
CSCs have also found to be resistant to chemotherapy and radiotherapy as evidenced by the increased percentage of CSC isolated following treatment. Cells that have undergone EMT share some of the same characteristics. Induction of EMT has been shown in breast cancer to cause transition to development of a CSC marker profile with associated phenotypic changes such as increased ability to form tumorspheres (Mani et al. 2008). In pancreatic cancer, recent gene expression profiling analysis of human and murine pancreatic cancer cell samples revealed three distinct tumor types: classical epithelial, quasimesenchymal, and endocrine-like type (Collisson et al. 2011). The most EMT-like quasimesenchymal tumors were associated with poor patient prognosis (Collisson et al. 2011). It has also been reported in preclinical studies that gemcitabine-resistant cells appear to undergo EMT with associated phenotypic changes of increased invasiveness and migration (Wang et al. 2009c). These resistant cells correspondingly had an increased population of pancreatic CSCs (Wang et al. 2009c). Although these data do not prove equivalence of CSC with cancer cells that have undergone EMT, the correlation between EMT and CSCs may provide insight into shared phenotypes of chemoresistance and allow for identification of new targets for therapy.
Conclusions
From the analyses of the complex pathways present in pancreatic cancer and evolving evidence of tumor heterogeneity, it is evident that in pancreatic tumors, changes are not often due to a single driver mutation, but more often a combination of many mutations collaborating together. Therefore, targeting a single pathway or molecule is unlikely to be successful. Adding to this complexity is the genetic clonal variation within the tumor itself. It is also becoming more apparent that in order to effectively treat pancreatic cancer, other cells in the tumor microenvironment must also be targeted, such as CAFs and immune cells that nourish and protect pancreatic cancer cells from chemotherapies. Ultimately, effective treatment of pancreatic cancer will need to combine means of normalizing the tumor stroma, removing bulk tumor cells, and eliminating elusive pancreatic CSCs that might drive tumor reestablishment and disease relapse. By achieving these goals, pancreatic cancer may someday become a manageable condition rather than a certain death sentence.
References
Abraham SC, Klimstra DS, Wilentz RE, Yeo CJ, Conlon K, Brennan M, Cameron JL, Wu TT, Hruban RH (2002) Solid-pseudopapillary tumors of the pancreas are genetically distinct from pancreatic ductal adenocarcinomas and almost always harbor beta-catenin mutations. Am J Pathol 160(4):1361–1369
Amemiya H, Kono K, Itakura J, Tang RF, Takahashi A, An FQ, Kamei S, Iizuka H, Fujii H, Matsumoto Y (2002) c-Met expression in gastric cancer with liver metastasis. Oncology 63(3):286–296. doi: ocl63286 [pii]
Apelqvist A, Li H, Sommer L, Beatus P, Anderson DJ, Honjo T, Hrabe de Angelis M, Lendahl U, Edlund H (1999) Notch signalling controls pancreatic cell differentiation. Nature 400(6747):877–881
Apte MV, Park S, Phillips PA, Santucci N, Goldstein D, Kumar RK, Ramm GA, Buchler M, Friess H, McCarroll JA, Keogh G, Merrett N, Pirola R, Wilson JS (2004) Desmoplastic reaction in pancreatic cancer: role of pancreatic stellate cells. Pancreas 29(3):179–187
Arnold NB, Ketterer K, Kleeff J, Friess H, Buchler MW, Korc M (2004) Thioredoxin is downstream of Smad7 in a pathway that promotes growth and suppresses cisplatin-induced apoptosis in pancreatic cancer. Cancer Res 64(10):3599–3606. doi: 10.1158/0008-5472.CAN-03-2999 64/10/3599 [pii]
Artavanis-Tsakonas S, Matsuno K, Fortini ME (1995) Notch signaling. Science 268(5208):225–232
Bailey JM, Swanson BJ, Hamada T, Eggers JP, Singh PK, Caffery T, Ouellette MM, Hollingsworth MA (2008) Sonic hedgehog promotes desmoplasia in pancreatic cancer. Clin Cancer Res 14(19):5995–6004. doi: 14/19/5995 [pii] 10.1158/1078-0432.CCR-08-0291
Bardeesy N, Cheng KH, Berger JH, Chu GC, Pahler J, Olson P, Hezel AF, Horner J, Lauwers GY, Hanahan D, DePinho RA (2006) Smad4 is dispensable for normal pancreas development yet critical in progression and tumor biology of pancreas cancer. Genes Dev 20(22):3130–3146. doi: 20/22/3130 [pii] 10.1101/gad.1478706
Bayne LJ, Beatty GL, Jhala N, Clark CE, Rhim AD, Stanger BZ, Vonderheide RH (2012) Tumor-derived granulocyte-macrophage colony-stimulating factor regulates myeloid inflammation and T cell immunity in pancreatic cancer. Cancer Cell 21(6):822–835. doi: 10.1016/j.ccr.2012.04.025
Berman DM, Karhadkar SS, Maitra A, Montes De Oca R, Gerstenblith MR, Briggs K, Parker AR, Shimada Y, Eshleman JR, Watkins DN, Beachy PA (2003) Widespread requirement for Hedgehog ligand stimulation in growth of digestive tract tumours. Nature 425(6960):846–851. doi: 10.1038/nature01972 nature01972 [pii]
Bettenhausen B, Hrabe de Angelis M, Simon D, Guenet JL, Gossler A (1995) Transient and restricted expression during mouse embryogenesis of Dll1, a murine gene closely related to Drosophila Delta. Development 121(8):2407–2418
Beviglia L, Matsumoto K, Lin CS, Ziober BL, Kramer RH (1997) Expression of the c-Met/HGF receptor in human breast carcinoma: correlation with tumor progression. Int J Cancer 74(3):301–309. doi:10.1002/(SICI)1097-0215(19970620)74:3<301::AID-IJC12>3.0.CO;2-E [pii]
Bhowmick NA, Ghiassi M, Bakin A, Aakre M, Lundquist CA, Engel ME, Arteaga CL, Moses HL (2001) Transforming growth factor-beta1 mediates epithelial to mesenchymal transdifferentiation through a RhoA-dependent mechanism. Mol Biol Cell 12(1):27–36
Bhowmick NA, Neilson EG, Moses HL (2004) Stromal fibroblasts in cancer initiation and progression. Nature 432(7015):332–337. doi: nature03096 [pii] 10.1038/nature03096
Blaumueller CM, Qi H, Zagouras P, Artavanis-Tsakonas S (1997) Intracellular cleavage of Notch leads to a heterodimeric receptor on the plasma membrane. Cell 90(2):281–291. doi: S0092-8674(00)80336-0 [pii]
Boccaccio C, Comoglio PM (2006) Invasive growth: a MET-driven genetic programme for cancer and stem cells. Nat Rev Cancer 6(8):637–645. doi: nrc1912 [pii] 10.1038/nrc1912
Bonnet D, Dick JE (1997) Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med 3(7):730–737
Campbell PJ, Yachida S, Mudie LJ, Stephens PJ, Pleasance ED, Stebbings LA, Morsberger LA, Latimer C, McLaren S, Lin ML, McBride DJ, Varela I, Nik-Zainal SA, Leroy C, Jia M, Menzies A, Butler AP, Teague JW, Griffin CA, Burton J, Swerdlow H, Quail MA, Stratton MR, Iacobuzio-Donahue C, Futreal PA (2010) The patterns and dynamics of genomic instability in metastatic pancreatic cancer. Nature 467(7319):1109–1113. doi: nature09460 [pii] 10.1038/nature09460
Clark CE, Hingorani SR, Mick R, Combs C, Tuveson DA, Vonderheide RH (2007) Dynamics of the immune reaction to pancreatic cancer from inception to invasion. Cancer Res 67(19):9518–9527. doi: 67/19/9518 [pii] 10.1158/0008-5472.CAN-07-0175
Clevers H (2006) Wnt/beta-catenin signaling in development and disease. Cell 127(3):469–480. doi: S0092-8674(06)01344-4 [pii] 10.1016/j.cell.2006.10.018
Collisson EA, Sadanandam A, Olson P, Gibb WJ, Truitt M, Gu S, Cooc J, Weinkle J, Kim GE, Jakkula L, Feiler HS, Ko AH, Olshen AB, Danenberg KL, Tempero MA, Spellman PT, Hanahan D, Gray JW (2011) Subtypes of pancreatic ductal adenocarcinoma and their differing responses to therapy. Nat Med 17(4):500–503. doi: nm.2344 [pii] 10.1038/nm.2344
Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de la Fouchardière C, Bennouna J, Bachet JB, Khemissa-Akouz F, Péré-Vergé D, Delbaldo C, Assenat E, Chauffert B, Michel P, Montoto-Grillot C, Ducreux M (2011) FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 364(19):1817–1825. doi: doi:10.1056/NEJMoa1011923
Cook N, Frese KK, Bapiro TE, Jacobetz MA, Gopinathan A, Miller JL, Rao SS, Demuth T, Howat WJ, Jodrell DI, Tuveson DA (2012) Gamma secretase inhibition promotes hypoxic necrosis in mouse pancreatic ductal adenocarcinoma. J Exp Med 209(3):437–444. doi: jem.20111923 [pii] 10.1084/jem.20111923
Cooper CS, Park M, Blair DG, Tainsky MA, Huebner K, Croce CM, Vande Woude GF (1984) Molecular cloning of a new transforming gene from a chemically transformed human cell line. Nature 311(5981):29–33
Corso S, Migliore C, Ghiso E, De Rosa G, Comoglio PM, Giordano S (2008) Silencing the MET oncogene leads to regression of experimental tumors and metastases. Oncogene 27(5):684–693. doi: 1210697 [pii] 10.1038/sj.onc.1210697
D’Souza B, Miyamoto A, Weinmaster G (2008) The many facets of Notch ligands. Oncogene 27(38):5148–5167. doi: onc2008229 [pii] 10.1038/onc.2008.229
De La O JP, Emerson LL, Goodman JL, Froebe SC, Illum BE, Curtis AB, Murtaugh LC (2008) Notch and Kras reprogram pancreatic acinar cells to ductal intraepithelial neoplasia. Proc Natl Acad Sci U S A 105(48):18907–18912. doi: 0810111105 [pii] 10.1073/pnas.0810111105
DeNardo DG, Andreu P, Coussens LM (2010) Interactions between lymphocytes and myeloid cells regulate pro- versus anti-tumor immunity. Cancer Metastasis Rev 29(2):309–316. doi: 10.1007/s10555-010-9223-6
Deonarain MP, Kousparou CA, Epenetos AA (2009) Antibodies targeting cancer stem cells: a new paradigm in immunotherapy? MAbs 1(1):12–25
Dessimoz J, Bonnard C, Huelsken J, Grapin-Botton A (2005) Pancreas-specific deletion of beta-catenin reveals Wnt-dependent and Wnt-independent functions during development. Curr Biol 15(18):1677–1683. doi: 10.1016/j.cub.2005.08.037
Di Renzo MF, Olivero M, Giacomini A, Porte H, Chastre E, Mirossay L, Nordlinger B, Bretti S, Bottardi S, Giordano S et al (1995a) Overexpression and amplification of the met/HGF receptor gene during the progression of colorectal cancer. Clin Cancer Res 1(2):147–154
Di Renzo MF, Poulsom R, Olivero M, Comoglio PM, Lemoine NR (1995b) Expression of the Met/hepatocyte growth factor receptor in human pancreatic cancer. Cancer Res 55(5):1129–1138
Direkze NC, Hodivala-Dilke K, Jeffery R, Hunt T, Poulsom R, Oukrif D, Alison MR, Wright NA (2004) Bone marrow contribution to tumor-associated myofibroblasts and fibroblasts. Cancer Res 64(23):8492–8495. doi: 10.1158/0008-5472.can-04-1708
Dunwoodie SL, Henrique D, Harrison SM, Beddington RS (1997) Mouse Dll3: a novel divergent Delta gene which may complement the function of other Delta homologues during early pattern formation in the mouse embryo. Development 124(16):3065–3076
Edlund S, Landström M, Heldin CH, Aspenström P (2002) Transforming growth factor-beta-induced mobilization of actin cytoskeleton requires signaling by small GTPases Cdc42 and RhoA. Mol Biol Cell 13(3):902–914. doi: 10.1091/mbc.01-08-0398
Ellenrieder V, Buck A, Harth A, Jungert K, Buchholz M, Adler G, Urrutia R, Gress TM (2004) KLF11 mediates a critical mechanism in TGF-beta signaling that is inactivated by Erk-MAPK in pancreatic cancer cells. Gastroenterology 127(2):607–620. doi: S0016508504008649 [pii]
Fiuza UM, Arias AM (2007) Cell and molecular biology of Notch. J Endocrinol 194(3):459–474. doi: 194/3/459 [pii] 10.1677/JOE-07-0242
Flavell RA, Sanjabi S, Wrzesinski SH, Licona-Limon P (2010) The polarization of immune cells in the tumour environment by TGFbeta. Nat Rev Immunol 10(8):554–567. doi: nri2808 [pii] 10.1038/nri2808
Fryer CJ, Lamar E, Turbachova I, Kintner C, Jones KA (2002) Mastermind mediates chromatin-specific transcription and turnover of the Notch enhancer complex. Genes Dev 16(11):1397–1411. doi: 10.1101/gad.991602
Fryer CJ, White JB, Jones KA (2004) Mastermind recruits CycC:CDK8 to phosphorylate the Notch ICD and coordinate activation with turnover. Mol Cell 16(4):509–520. doi: S1097276504006409 [pii] 10.1016/j.molcel.2004.10.014
Gallahan D, Callahan R (1997) The mouse mammary tumor associated gene INT3 is a unique member of the NOTCH gene family (NOTCH4). Oncogene 14(16):1883–1890. doi: 10.1038/sj.onc.1201035
Gallahan D, Jhappan C, Robinson G, Hennighausen L, Sharp R, Kordon E, Callahan R, Merlino G, Smith GH (1996) Expression of a truncated Int3 gene in developing secretory mammary epithelium specifically retards lobular differentiation resulting in tumorigenesis. Cancer Res 56(8):1775–1785
Gao Z, Wang X, Wu K, Zhao Y, Hu G (2010) Pancreatic stellate cells increase the invasion of human pancreatic cancer cells through the stromal cell-derived factor-1/CXCR4 axis. Pancreatology 10(2–3):186–193. doi: 10.1159/000236012
Ghoussoub RA, Dillon DA, D’Aquila T, Rimm EB, Fearon ER, Rimm DL (1998) Expression of c-met is a strong independent prognostic factor in breast carcinoma. Cancer 82(8):1513–1520. doi:10.1002/(SICI)1097-0142(19980415)82:8<1513::AID-CNCR13>3.0.CO;2-7 [pii]
Gridley T (1997) Notch signaling in vertebrate development and disease. Mol Cell Neurosci 9(2):103–108. doi: S1044-7431(97)90610-2 [pii] 10.1006/mcne.1997.0610
Gridley T (2003) Notch signaling and inherited disease syndromes. Hum Mol Genet 12 Spec No. 1:R9–R13
Groden J, Thliveris A, Samowitz W, Carlson M, Gelbert L, Albertsen H, Joslyn G, Stevens J, Spirio L, Robertson M et al (1991) Identification and characterization of the familial adenomatous polyposis coli gene. Cell 66(3):589–600
Gupta S, Takebe N, Lorusso P (2010) Targeting the Hedgehog pathway in cancer. Ther Adv Med Oncol 2(4):237–250. doi: 10.1177/1758834010366430 10.1177_1758834010366430 [pii]
Hanahan D, Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144(5):646–674. doi: S0092-8674(11)00127-9 [pii] 10.1016/j.cell.2011.02.013
Harris AL (2002) Hypoxia—a key regulatory factor in tumour growth. Nat Rev Cancer 2(1):38–47. doi: http://www.nature.com/nrc/journal/v2/n1/suppinfo/nrc704_S1.html
Hartsough MT, Mulder KM (1995) Transforming growth factor beta activation of p44mapk in proliferating cultures of epithelial cells. J Biol Chem 270(13):7117–7124. doi: 10.1074/jbc.270.13.7117
Heller RS, Dichmann DS, Jensen J, Miller C, Wong G, Madsen OD, Serup P (2002) Expression patterns of Wnts, Frizzleds, sFRPs, and misexpression in transgenic mice suggesting a role for Wnts in pancreas and foregut pattern formation. Dev Dyn 225(3):260–270. doi: 10.1002/dvdy.10157
Hermann PC, Huber SL, Herrler T, Aicher A, Ellwart JW, Guba M, Bruns CJ, Heeschen C (2007) Distinct populations of cancer stem cells determine tumor growth and metastatic activity in human pancreatic cancer. Cell Stem Cell 1(3):313–323. doi: S1934-5909(07)00066-5 [pii] 10.1016/j.stem.2007.06.002
Hezel AF, Kimmelman AC, Stanger BZ, Bardeesy N, Depinho RA (2006) Genetics and biology of pancreatic ductal adenocarcinoma. Genes Dev 20(10):1218–1249. doi: 20/10/1218 [pii] 10.1101/gad.1415606
Hingorani SR, Petricoin EF, Maitra A, Rajapakse V, King C, Jacobetz MA, Ross S, Conrads TP, Veenstra TD, Hitt BA, Kawaguchi Y, Johann D, Liotta LA, Crawford HC, Putt ME, Jacks T, Wright CV, Hruban RH, Lowy AM, Tuveson DA (2003) Preinvasive and invasive ductal pancreatic cancer and its early detection in the mouse. Cancer Cell 4(6):437–450. doi: S153561080300309X [pii]
Hingorani SR, Wang L, Multani AS, Combs C, Deramaudt TB, Hruban RH, Rustgi AK, Chang S, Tuveson DA (2005) Trp53R172H and KrasG12D cooperate to promote chromosomal instability and widely metastatic pancreatic ductal adenocarcinoma in mice. Cancer Cell 7(5):469–483. doi: S1535-6108(05)00128-5 [pii] 10.1016/j.ccr.2005.04.023
Hsieh JJ, Zhou S, Chen L, Young DB, Hayward SD (1999) CIR, a corepressor linking the DNA binding factor CBF1 to the histone deacetylase complex. Proc Natl Acad Sci USA 96(1):23–28
Hua Z, Zhang YC, Hu XM, Jia ZG (2003) Loss of DPC4 expression and its correlation with clinicopathological parameters in pancreatic carcinoma. World J Gastroenterol 9(12):2764–2767
Humphrey PA, Zhu X, Zarnegar R, Swanson PE, Ratliff TL, Vollmer RT, Day ML (1995) Hepatocyte growth factor and its receptor (c-MET) in prostatic carcinoma. Am J Pathol 147(2):386–396
Hwang RF, Moore T, Arumugam T, Ramachandran V, Amos KD, Rivera A, Ji B, Evans DB, Logsdon CD (2008) Cancer-associated stromal fibroblasts promote pancreatic tumor progression. Cancer Res 68(3):918–926. doi: 68/3/918 [pii] 10.1158/0008-5472.CAN-07-5714
Ikenaga N, Ohuchida K, Mizumoto K, Cui L, Kayashima T, Morimatsu K, Moriyama T, Nakata K, Fujita H, Tanaka M (2010) CD10+ pancreatic stellate cells enhance the progression of pancreatic cancer. Gastroenterology 139(3):1041–1051. doi: S0016-5085(10)00849-8 [pii] 10.1053/j.gastro.2010.05.084, 1051.e1–8
Ingham PW, McMahon AP (2001) Hedgehog signaling in animal development: paradigms and principles. Genes Dev 15(23):3059–3087. doi: 10.1101/gad.938601
Izeradjene K, Combs C, Best M, Gopinathan A, Wagner A, Grady WM, Deng CX, Hruban RH, Adsay NV, Tuveson DA, Hingorani SR (2007) Kras(G12D) and Smad4/Dpc4 haploinsufficiency cooperate to induce mucinous cystic neoplasms and invasive adenocarcinoma of the pancreas. Cancer Cell 11(3):229–243. doi: S1535-6108(07)00057-8 [pii] 10.1016/j.ccr.2007.01.017
Jacobetz MA, Chan DS, Neesse A, Bapiro TE, Cook N, Frese KK, Feig C, Nakagawa T, Caldwell ME, Zecchini HI, Lolkema MP, Jiang P, Kultti A, Thompson CB, Maneval DC, Jodrell DI, Frost GI, Shepard HM, Skepper JN, Tuveson DA (2013) Hyaluronan impairs vascular function and drug delivery in a mouse model of pancreatic cancer. Gut 62(1):112–120. doi: 10.1136/gutjnl-2012-302529
Jaffee EM, Hruban RH, Canto M, Kern SE (2002) Focus on pancreas cancer. Cancer Cell 2(1):25–28. doi: 10.1016/s1535-6108(02)00093-4
Jensen J, Heller RS, Funder-Nielsen T, Pedersen EE, Lindsell C, Weinmaster G, Madsen OD, Serup P (2000) Independent development of pancreatic alpha- and beta-cells from neurogenin3-expressing precursors: a role for the notch pathway in repression of premature differentiation. Diabetes 49(2):163–176
Jhappan C, Gallahan D, Stahle C, Chu E, Smith GH, Merlino G, Callahan R (1992) Expression of an activated Notch-related int-3 transgene interferes with cell differentiation and induces neoplastic transformation in mammary and salivary glands. Genes Dev 6(3):345–355
Jimeno A, Feldmann G, Suárez-Gauthier A, Rasheed Z, Solomon A, Zou GM, Rubio-Viqueira B, García-García E, López-Ríos F, Matsui W, Maitra A, Hidalgo M (2009) A direct pancreatic cancer xenograft model as a platform for cancer stem cell therapeutic development. Mol Cancer Ther 8(2):310–314
Jones S, Zhang X, Parsons DW, Lin JC, Leary RJ, Angenendt P, Mankoo P, Carter H, Kamiyama H, Jimeno A, Hong SM, Fu B, Lin MT, Calhoun ES, Kamiyama M, Walter K, Nikolskaya T, Nikolsky Y, Hartigan J, Smith DR, Hidalgo M, Leach SD, Klein AP, Jaffee EM, Goggins M, Maitra A, Iacobuzio-Donahue C, Eshleman JR, Kern SE, Hruban RH, Karchin R, Papadopoulos N, Parmigiani G, Vogelstein B, Velculescu VE, Kinzler KW (2008) Core signaling pathways in human pancreatic cancers revealed by global genomic analyses. Science 321(5897):1801–1806. doi: 10.1126/science.1164368
Kalluri R (2009) EMT: when epithelial cells decide to become mesenchymal-like cells. J Clin Invest 119(6):1417–1419. doi: 10.1172/jci39675
Kao HY, Ordentlich P, Koyano-Nakagawa N, Tang Z, Downes M, Kintner CR, Evans RM, Kadesch T (1998) A histone deacetylase corepressor complex regulates the Notch signal transduction pathway. Genes Dev 12(15):2269–2277
Kelly RJ, Morris JC (2010) Transforming growth factor-beta: a target for cancer therapy. J Immunotoxicol 7(1):15–26. doi: 10.3109/15476910903389920
Kim EJ, Simeone DM (2011) Advances in pancreatic cancer. Curr Opin Gastroenterol 27(5):460–466. doi: 10.1097/MOG.0b013e328349e31f
Kobayashi T, Honke K, Gasa S, Miyazaki T, Tajima H, Matsumoto K, Nakamura T, Makita A (1994) Hepatocyte growth factor elevates the activity levels of glycolipid sulfotransferases in renal cell carcinoma cells. Eur J Biochem 219(1–2):407–413
Kohn AD, Moon RT (2005) Wnt and calcium signaling: beta-catenin-independent pathways. Cell Calcium 38(3–4):439–446. doi: 10.1016/j.ceca.2005.06.022
Koshiba T, Hosotani R, Miyamoto Y, Ida J, Tsuji S, Nakajima S, Kawaguchi M, Kobayashi H, Doi R, Hori T, Fujii N, Imamura M (2000) Expression of stromal cell-derived factor 1 and CXCR4 ligand receptor system in pancreatic cancer: a possible role for tumor progression. Clin Cancer Res 6(9):3530–3535
Kraman M, Bambrough PJ, Arnold JN, Roberts EW, Magiera L, Jones JO, Gopinathan A, Tuveson DA, Fearon DT (2010) Suppression of antitumor immunity by stromal cells expressing fibroblast activation protein-alpha. Science 330(6005):827–830. doi: 330/6005/827 [pii] 10.1126/science.1195300
Krymskaya VP, Hoffman R, Eszterhas A, Ciocca V, Panettieri RA (1997) TGF-β1 modulates EGF-stimulated phosphatidylinositol 3-kinase activity in human airway smooth muscle cells. Am J Physiol 273(6):L1220–L1227
Kurooka H, Honjo T (2000) Functional interaction between the mouse notch1 intracellular region and histone acetyltransferases PCAF and GCN5. J Biol Chem 275(22):17211–17220. doi: 10.1074/jbc.M000909200 M000909200 [pii]
Lauth M, Bergstrom A, Shimokawa T, Tostar U, Jin Q, Fendrich V, Guerra C, Barbacid M, Toftgard R (2010) DYRK1B-dependent autocrine-to-paracrine shift of Hedgehog signaling by mutant RAS. Nat Struct Mol Biol 17(6):718–725. doi: nsmb.1833 [pii] 10.1038/nsmb.1833
Lee WY, Chen HH, Chow NH, Su WC, Lin PW, Guo HR (2005) Prognostic significance of co-expression of RON and MET receptors in node-negative breast cancer patients. Clin Cancer Res 11(6):2222–2228. doi: 11/6/2222 [pii] 10.1158/1078-0432.CCR-04-1761
Li C, Heidt DG, Dalerba P, Burant CF, Zhang L, Adsay V, Wicha M, Clarke MF, Simeone DM (2007) Identification of pancreatic cancer stem cells. Cancer Res 67(3):1030–1037. doi: 67/3/1030 [pii] 10.1158/0008-5472.CAN-06-2030
Li C, Wu JJ, Hynes M, Dosch J, Sarkar B, Welling TH, Pasca di Magliano M, Simeone DM (2011) c-Met is a marker of pancreatic cancer stem cells and therapeutic target. Gastroenterology 141(6):2218.e5–2227.e5. doi: S0016-5085(11)01157-7 [pii] 10.1053/j.gastro.2011.08.009
Lindsell CE, Shawber CJ, Boulter J, Weinmaster G (1995) Jagged: a mammalian ligand that activates Notch1. Cell 80(6):909–917. doi: 0092-8674(95)90294-5 [pii]
Lonardo E, Hermann PC, Mueller MT, Huber S, Balic A, Miranda-Lorenzo I, Zagorac S, Alcala S, Rodriguez-Arabaolaza I, Ramirez JC, Torres-Ruíz R, Garcia E, Hidalgo M, Cebrián DÁ, Heuchel R, Löhr M, Berger F, Bartenstein P, Aicher A, Heeschen C (2011) Nodal/Activin signaling drives self-renewal and tumorigenicity of pancreatic cancer stem cells and provides a target for combined drug therapy. Cell Stem Cell 9(5):433–446
Lyon M, Deakin JA, Mizuno K, Nakamura T, Gallagher JT (1994) Interaction of hepatocyte growth factor with heparan sulfate. Elucidation of the major heparan sulfate structural determinants. J Biol Chem 269(15):11216–11223
Malkoski SP, Wang XJ (2012) Two sides of the story? Smad4 loss in pancreatic cancer versus head-and-neck cancer. FEBS Lett. doi: S0014-5793(12)00101-9 [pii] 10.1016/j.febslet.2012.01.054
Mani SA, Guo W, Liao MJ, Eaton EN, Ayyanan A, Zhou AY, Brooks M, Reinhard F, Zhang CC, Shipitsin M, Campbell LL, Polyak K, Brisken C, Yang J, Weinberg RA (2008) The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell 133(4):704–715. doi: S0092-8674(08)00444-3 [pii] 10.1016/j.cell.2008.03.027
Maroun CR, Naujokas MA, Holgado-Madruga M, Wong AJ, Park M (2000) The tyrosine phosphatase SHP-2 is required for sustained activation of extracellular signal-regulated kinase and epithelial morphogenesis downstream from the met receptor tyrosine kinase. Mol Cell Biol 20(22):8513–8525
Maroun CR, Naujokas MA, Park M (2003) Membrane targeting of Grb2-associated binder-1 (Gab1) scaffolding protein through Src myristoylation sequence substitutes for Gab1 pleckstrin homology domain and switches an epidermal growth factor response to an invasive morphogenic program. Mol Biol Cell 14(4):1691–1708. doi: 10.1091/mbc.E02-06-0352
Marusyk A, Polyak K (2010) Tumor heterogeneity: causes and consequences. Biochim Biophys Acta 1805(1):105–117. doi: S0304-419X(09)00074-2 [pii] 10.1016/j.bbcan.2009.11.002
Massague J (1998) TGF-beta signal transduction. Annu Rev Biochem 67:753–791. doi: 10.1146/annurev.biochem.67.1.753
McDermott U, Sharma SV, Dowell L, Greninger P, Montagut C, Lamb J, Archibald H, Raudales R, Tam A, Lee D, Rothenberg SM, Supko JG, Sordella R, Ulkus LE, Iafrate AJ, Maheswaran S, Njauw CN, Tsao H, Drew L, Hanke JH, Ma XJ, Erlander MG, Gray NS, Haber DA, Settleman J (2007) Identification of genotype-correlated sensitivity to selective kinase inhibitors by using high-throughput tumor cell line profiling. Proc Natl Acad Sci USA 104(50):19936–19941. doi: 0707498104 [pii] 10.1073/pnas.0707498104
Migliore C, Giordano S (2008) Molecular cancer therapy: can our expectation be MET? Eur J Cancer 44(5):641–651. doi: S0959-8049(08)00067-1 [pii] 10.1016/j.ejca.2008.01.022
Miyamoto Y, Maitra A, Ghosh B, Zechner U, Argani P, Iacobuzio-Donahue CA, Sriuranpong V, Iso T, Meszoely IM, Wolfe MS, Hruban RH, Ball DW, Schmid RM, Leach SD (2003) Notch mediates TGF alpha-induced changes in epithelial differentiation during pancreatic tumorigenesis. Cancer Cell 3(6):565–576. doi: S1535610803001405 [pii]
Morel V, Lecourtois M, Massiani O, Maier D, Preiss A, Schweisguth F (2001) Transcriptional repression by suppressor of hairless involves the binding of a hairless-dCtBP complex in Drosophila. Curr Biol 11(10):789–792. doi: S0960-9822(01)00224-X [pii]
Morris JP 4th, Cano DA, Sekine S, Wang SC, Hebrok M (2010) Beta-catenin blocks Kras-dependent reprogramming of acini into pancreatic cancer precursor lesions in mice. J Clin Invest 120(2):508–520. doi: 10.1172/JCI40045 40045 [pii]
Mucsi I, Skorecki KL, Goldberg HJ (1996) Extracellular signal-regulated kinase and the small GTP-binding protein, Rac, contribute to the effects of transforming growth factor-beta1 on gene expression. J Biol Chem 271(28):16567–16572. doi: 10.1074/jbc.271.28.16567
Mullendore ME, Koorstra JB, Li YM, Offerhaus GJ, Fan X, Henderson CM, Matsui W, Eberhart CG, Maitra A, Feldmann G (2009) Ligand-dependent Notch signaling is involved in tumor initiation and tumor maintenance in pancreatic cancer. Clin Cancer Res 15(7):2291–2301. doi: 1078-0432.CCR-08-2004 [pii] 10.1158/1078-0432.CCR-08-2004
Murdoch C, Muthana M, Coffelt SB, Lewis CE (2008) The role of myeloid cells in the promotion of tumour angiogenesis. Nat Rev Cancer 8(8):618–631. doi: nrc2444 [pii] 10.1038/nrc2444
Murtaugh LC, Law AC, Dor Y, Melton DA (2005) Beta-catenin is essential for pancreatic acinar but not islet development. Development 132(21):4663–4674. doi: 10.1242/dev.02063
Nawroth R, van Zante A, Cervantes S, McManus M, Hebrok M, Rosen SD (2007) Extracellular sulfatases, elements of the Wnt signaling pathway, positively regulate growth and tumorigenicity of human pancreatic cancer cells. PLoS One 2(4):e392. doi: 10.1371/journal.pone.0000392
Nishimura T, Honda H, Takeichi M (2012) Planar cell polarity links axes of spatial dynamics in neural-tube closure. Cell 149(5):1084–1097
Nishisho I, Nakamura Y, Miyoshi Y, Miki Y, Ando H, Horii A, Koyama K, Utsunomiya J, Baba S, Hedge P (1991) Mutations of chromosome 5q21 genes in FAP and colorectal cancer patients. Science 253(5020):665–669
Nolan-Stevaux O, Lau J, Truitt ML, Chu GC, Hebrok M, Fernandez-Zapico ME, Hanahan D (2009) GLI1 is regulated through Smoothened-independent mechanisms in neoplastic pancreatic ducts and mediates PDAC cell survival and transformation. Genes Dev 23(1):24–36. doi: 23/1/24 [pii] 10.1101/gad.1753809
Olaku V, Matzke A, Mitchell C, Hasenauer S, Sakkaravarthi A, Pace G, Ponta H, Orian-Rousseau V (2011) c-Met recruits ICAM-1 as a coreceptor to compensate for the loss of CD44 in Cd44 null mice. Mol Biol Cell 22(15):2777–2786. doi: mbc.E11-02-0134 [pii] 10.1091/mbc.E11-02-0134
Olive KP, Jacobetz MA, Davidson CJ, Gopinathan A, McIntyre D, Honess D, Madhu B, Goldgraben MA, Caldwell ME, Allard D, Frese KK, DeNicola G, Feig C, Combs C, Winter SP, Ireland-Zecchini H, Reichelt S, Howat WJ, Chang A, Dhara M, Wang L, Rückert F, Grützmann R, Pilarsky C, Izeradjene K, Hingorani SR, Huang P, Davies SE, Plunkett W, Egorin M, Hruban RH, Whitebread N, McGovern K, Adams J, Iacobuzio-Donahue C, Griffiths J, Tuveson DA (2009) Inhibition of Hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science 324(5933):1457–1461. doi: 10.1126/science.1171362
Onozuka H, Tsuchihara K, Esumi H (2011) Hypoglycemic/hypoxic condition in vitro mimicking the tumor microenvironment markedly reduced the efficacy of anticancer drugs. Cancer Sci 102(5):975–982. doi: 10.1111/j.1349-7006.2011.01880.x
Orian-Rousseau V, Chen L, Sleeman JP, Herrlich P, Ponta H (2002) CD44 is required for two consecutive steps in HGF/c-Met signaling. Genes Dev 16(23):3074–3086. doi: 10.1101/gad.242602
Park WS, Dong SM, Kim SY, Na EY, Shin MS, Pi JH, Kim BJ, Bae JH, Hong YK, Lee KS, Lee SH, Yoo NJ, Jang JJ, Pack S, Zhuang Z, Schmidt L, Zbar B, Lee JY (1999) Somatic mutations in the kinase domain of the Met/hepatocyte growth factor receptor gene in childhood hepatocellular carcinomas. Cancer Res 59(2):307–310
Pasca di Magliano M, Biankin AV, Heiser PW, Cano DA, Gutierrez PJ, Deramaudt T, Segara D, Dawson AC, Kench JG, Henshall SM, Sutherland RL, Dlugosz A, Rustgi AK, Hebrok M (2007) Common activation of canonical Wnt signaling in pancreatic adenocarcinoma. PLoS One 2(11):e1155. doi: 10.1371/journal.pone.0001155
Pasche B (2001) Role of transforming growth factor beta in cancer. J Cell Physiol 186(2):153–168. doi:10.1002/1097-4652(200002)186:2<153::aid-jcp1016>3.0.co;2-j
Pennacchietti S, Michieli P, Galluzzo M, Mazzone M, Giordano S, Comoglio PM (2003) Hypoxia promotes invasive growth by transcriptional activation of the met protooncogene. Cancer Cell 3(4):347–361. doi: S1535610803000850 [pii]
Plentz R, Park JS, Rhim AD, Abravanel D, Hezel AF, Sharma SV, Gurumurthy S, Deshpande V, Kenific C, Settleman J, Majumder PK, Stanger BZ, Bardeesy N (2009) Inhibition of gamma-secretase activity inhibits tumor progression in a mouse model of pancreatic ductal adenocarcinoma. Gastroenterology 136(5):1741.e6–1749.e6. doi: S0016-5085(09)00014-6 [pii] 10.1053/j.gastro.2009.01.008
Provenzano PP, Cuevas C, Chang AE, Goel VK, Von Hoff DD, Hingorani SR (2012) Enzymatic targeting of the stroma ablates physical barriers to treatment of pancreatic ductal adenocarcinoma. Cancer Cell 21(3):418–429
Pylayeva-Gupta Y, Lee KE, Hajdu CH, Miller G, Bar-Sagi D (2012) Oncogenic Kras-induced GM-CSF production promotes the development of pancreatic neoplasia. Cancer Cell 21(6):836–847. doi: 10.1016/j.ccr.2012.04.024
Qian BZ, Pollard JW (2010) Macrophage diversity enhances tumor progression and metastasis. Cell 141(1):39–51. doi: S0092-8674(10)00287-4 [pii] 10.1016/j.cell.2010.03.014
Radtke F, Raj K (2003) The role of Notch in tumorigenesis: oncogene or tumour suppressor? Nat Rev Cancer 3(10):756–767. doi: 10.1038/nrc1186
Reya T, Morrison SJ, Clarke MF, Weissman IL (2001) Stem cells, cancer, and cancer stem cells. Nature 414(6859):105–111. doi: 10.1038/35102167 35102167 [pii]
Reynolds TC, Smith SD, Sklar J (1987) Analysis of DNA surrounding the breakpoints of chromosomal translocations involving the beta T cell receptor gene in human lymphoblastic neoplasms. Cell 50(1):107–117. doi: 0092-8674(87)90667-2 [pii]
Rowland-Goldsmith MA, Maruyama H, Kusama T, Ralli S, Korc M (2001) Soluble type II transforming growth factor-beta (TGF-beta) receptor inhibits TGF-beta signaling in COLO-357 pancreatic cancer cells in vitro and attenuates tumor formation. Clin Cancer Res 7(9): 2931–2940
Rowland-Goldsmith MA, Maruyama H, Matsuda K, Idezawa T, Ralli M, Ralli S, Korc M (2002) Soluble type II transforming growth factor-beta receptor attenuates expression of metastasis-associated genes and suppresses pancreatic cancer cell metastasis. Mol Cancer Ther 1(3): 161–167
Rubin LL, de Sauvage FJ (2006) Targeting the Hedgehog pathway in cancer. Nat Rev Drug Discov 5(12):1026–1033. doi: nrd2086 [pii] 10.1038/nrd2086
Ruffell B, DeNardo DG, Affara NI, Coussens LM (2010) Lymphocytes in cancer development: polarization towards pro-tumor immunity. Cytokine Growth Factor Rev 21(1):3–10. doi: S1359-6101(09)00109-9 [pii] 10.1016/j.cytogfr.2009.11.002
Ruiz i Altaba A, Palma V, Dahmane N (2002a) Hedgehog-Gli signalling and the growth of the brain. Nat Rev Neurosci 3(1):24–33. doi: 10.1038/nrn704 nrn704 [pii]
Ruiz i Altaba A, Sanchez P, Dahmane N (2002b) Gli and hedgehog in cancer: tumours, embryos and stem cells. Nat Rev Cancer 2(5):361–372. doi: 10.1038/nrc796
Samowitz WS, Powers MD, Spirio LN, Nollet F, van Roy F, Slattery ML (1999) Beta-catenin mutations are more frequent in small colorectal adenomas than in larger adenomas and invasive carcinomas. Cancer Res 59(7):1442–1444
Scales SJ, de Sauvage FJ (2009) Mechanisms of Hedgehog pathway activation in cancer and implications for therapy. Trends Pharmacol Sci 30(6):303–312. doi: S0165-6147(09)00069-8 [pii] 10.1016/j.tips.2009.03.007
Schlingensiepen KH, Jaschinski F, Lang SA, Moser C, Geissler EK, Schlitt HJ, Kielmanowicz M, Schneider A (2011) Transforming growth factor-beta 2 gene silencing with trabedersen (AP 12009) in pancreatic cancer. Cancer Sci 102(6):1193–1200. doi: 10.1111/j.1349-7006.2011.01917.x
Schmidt L, Duh FM, Chen F, Kishida T, Glenn G, Choyke P, Scherer SW, Zhuang Z, Lubensky I, Dean M, Allikmets R, Chidambaram A, Bergerheim UR, Feltis JT, Casadevall C, Zamarron A, Bernues M, Richard S, Lips CJ, Walther MM, Tsui LC, Geil L, Orcutt ML, Stackhouse T, Lipan J, Slife L, Brauch H, Decker J, Niehans G, Hughson MD, Moch H, Storkel S, Lerman MI, Linehan WM, Zbar B (1997) Germline and somatic mutations in the tyrosine kinase domain of the MET proto-oncogene in papillary renal carcinomas. Nat Genet 16(1):68–73. doi: 10.1038/ng0597-68
Shawber C, Boulter J, Lindsell CE, Weinmaster G (1996) Jagged2: a serrate-like gene expressed during rat embryogenesis. Dev Biol 180(1):370–376. doi: S0012-1606(96)90310-3 [pii] 10.1006/dbio.1996.0310
Shutter JR, Scully S, Fan W, Richards WG, Kitajewski J, Deblandre GA, Kintner CR, Stark KL (2000) Dll4, a novel Notch ligand expressed in arterial endothelium. Genes Dev 14(11): 1313–1318
Sierra JR, Tsao MS (2011) c-MET as a potential therapeutic target and biomarker in cancer. Ther Adv Med Oncol 3(1 Suppl):S21–S35. doi: 10.1177/1758834011422557 10.1177_ 1758834011422557 [pii]
Singh S, Srivastava SK, Bhardwaj A, Owen LB, Singh AP (2010) CXCL12-CXCR4 signalling axis confers gemcitabine resistance to pancreatic cancer cells: a novel target for therapy. Br J Cancer 103(11):1671–1679. doi: http://www.nature.com/bjc/journal/v103/n11/suppinfo/6605968s1.html
Soman NR, Correa P, Ruiz BA, Wogan GN (1991) The TPR-MET oncogenic rearrangement is present and expressed in human gastric carcinoma and precursor lesions. Proc Natl Acad Sci U S A 88(11):4892–4896
Sonnenberg E, Meyer D, Weidner KM, Birchmeier C (1993) Scatter factor/hepatocyte growth factor and its receptor, the c-met tyrosine kinase, can mediate a signal exchange between mesenchyme and epithelia during mouse development. J Cell Biol 123(1):223–235
Suzuki K, Hayashi N, Yamada Y, Yoshihara H, Miyamoto Y, Ito Y, Ito T, Katayama K, Sasaki Y, Ito A et al (1994) Expression of the c-met protooncogene in human hepatocellular carcinoma. Hepatology 20(5):1231–1236. doi: S0270913994003459 [pii]
Takeuchi H, Bilchik A, Saha S, Turner R, Wiese D, Tanaka M, Kuo C, Wang HJ, Hoon DS (2003) c-MET expression level in primary colon cancer: a predictor of tumor invasion and lymph node metastases. Clin Cancer Res 9(4):1480–1488
Tascilar M, Skinner HG, Rosty C, Sohn T, Wilentz RE, Offerhaus GJ, Adsay V, Abrams RA, Cameron JL, Kern SE, Yeo CJ, Hruban RH, Goggins M (2001) The SMAD4 protein and prognosis of pancreatic ductal adenocarcinoma. Clin Cancer Res 7(12):4115–4121
Terabe M, Ambrosino E, Takaku S, O’Konek JJ, Venzon D, Lonning S, McPherson JM, Berzofsky JA (2009) Synergistic enhancement of CD8+ T cell-mediated tumor vaccine efficacy by an anti-transforming growth factor-beta monoclonal antibody. Clin Cancer Res 15(21):6560–6569. doi: 1078-0432.CCR-09-1066 [pii] 10.1158/1078-0432.CCR-09-1066
Thayer SP, di Magliano MP, Heiser PW, Nielsen CM, Roberts DJ, Lauwers GY, Qi YP, Gysin S, Fernandez-del Castillo C, Yajnik V, Antoniu B, McMahon M, Warshaw AL, Hebrok M (2003) Hedgehog is an early and late mediator of pancreatic cancer tumorigenesis. Nature 425(6960):851–856. doi: 10.1038/nature02009 nature02009 [pii]
Trusolino L, Bertotti A, Comoglio PM (2010) MET signalling: principles and functions in development, organ regeneration and cancer. Nat Rev Mol Cell Biol 11(12):834–848. doi: nrm3012 [pii] 10.1038/nrm3012
Wang Z, Zhang Y, Li Y, Banerjee S, Liao J, Sarkar FH (2006) Down-regulation of Notch-1 contributes to cell growth inhibition and apoptosis in pancreatic cancer cells. Mol Cancer Ther 5(3):483–493. doi: 5/3/483 [pii] 10.1158/1535-7163.MCT-05-0299
Wang L, Heidt DG, Lee CJ, Yang H, Logsdon CD, Zhang L, Fearon ER, Ljungman M, Simeone DM (2009a) Oncogenic function of ATDC in pancreatic cancer through Wnt pathway activation and beta-catenin stabilization. Cancer Cell 15(3):207–219. doi: 10.1016/j.ccr.2009.01.018
Wang P, Fan J, Chen Z, Meng ZQ, Luo JM, Lin JH, Zhou ZH, Chen H, Wang K, Xu ZD, Liu LM (2009b) Low-level expression of Smad7 correlates with lymph node metastasis and poor prognosis in patients with pancreatic cancer. Ann Surg Oncol 16(4):826–835. doi: 10.1245/s10434-008-0284-5
Wang Z, Li Y, Kong D, Banerjee S, Ahmad A, Azmi AS, Ali S, Abbruzzese JL, Gallick GE, Sarkar FH (2009c) Acquisition of epithelial-mesenchymal transition phenotype of gemcitabine-resistant pancreatic cancer cells is linked with activation of the notch signaling pathway. Cancer Res 69(6):2400–2407. doi: 10.1158/0008-5472.can-08-4312
Weidner KM, Di Cesare S, Sachs M, Brinkmann V, Behrens J, Birchmeier W (1996) Interaction between Gab1 and the c-Met receptor tyrosine kinase is responsible for epithelial morphogenesis. Nature 384(6605):173–176. doi: 10.1038/384173a0
Wells JM, Esni F, Boivin GP, Aronow BJ, Stuart W, Combs C, Sklenka A, Leach SD, Lowy AM (2007) Wnt/beta-catenin signaling is required for development of the exocrine pancreas. BMC Dev Biol 7:4. doi: 10.1186/1471-213X-7-4
Wilentz RE, Iacobuzio-Donahue CA, Argani P, McCarthy DM, Parsons JL, Yeo CJ, Kern SE, Hruban RH (2000) Loss of expression of Dpc4 in pancreatic intraepithelial neoplasia: evidence that DPC4 inactivation occurs late in neoplastic progression. Cancer Res 60(7):2002–2006
Willert K, Jones KA (2006) Wnt signaling: is the party in the nucleus? Genes Dev 20(11):1394–1404. doi: 20/11/1394 [pii] 10.1101/gad.1424006
Yokoi K, Fidler IJ (2004) Hypoxia increases resistance of human pancreatic cancer cells to apoptosis induced by gemcitabine. Clin Cancer Res 10(7):2299–2306. doi: 10.1158/1078-0432.ccr-03-0488
Zarnegar R, Michalopoulos GK (1995) The many faces of hepatocyte growth factor: from hepatopoiesis to hematopoiesis. J Cell Biol 129(5):1177–1180. doi: 10.1083/jcb.129.5.1177
Zhou S, Fujimuro M, Hsieh JJ, Chen L, Miyamoto A, Weinmaster G, Hayward SD (2000) SKIP, a CBF1-associated protein, interacts with the ankyrin repeat domain of NotchIC To facilitate NotchIC function. Mol Cell Biol 20(7):2400–2410
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Kim, E., Abel, E.V., Ghosh, A., Simeone, D.M. (2013). Molecular Targeted Therapies in Pancreatic Cancer. In: Simeone, D., Maitra, A. (eds) Molecular Genetics of Pancreatic Cancer. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-6549-2_6
Download citation
DOI: https://doi.org/10.1007/978-1-4614-6549-2_6
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-6548-5
Online ISBN: 978-1-4614-6549-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)