
Abstract
Several bacteria that cause human disease can be found in the ocean. The actual incidence of bacterial disease that results from seawater or seafood is not precisely known but is thought to be relatively low in the USA, although some diseases are on the rise. Bacterial disease from the ocean is more prevalent worldwide, especially in developing countries and in countries that derive most of their protein from seafood. Compared to the viruses, bacteria account for a much lower incidence of disease emanating from the ocean, both in the USA and worldwide. However, it is important to understand and mitigate bacterial disease from the ocean, because of such environmental pressures as global warming, antibiotic resistance, pollution, breakdowns in sanitation (e.g., Haiti after the earthquake) and tourism.
This chapter, which has been modified slightly for the purposes of this volume, was originally published as part of the Encyclopedia of Sustainability Science and Technology edited by Robert A. Meyers. DOI:10.1007/978-1-4419-0851-3
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Definition of the Subject and Its Importance
Several bacteria that cause human disease can be found in the ocean. The actual incidence of bacterial disease that results from seawater or seafood is not precisely known but is thought to be relatively low in the USA, although some diseases are on the rise. Bacterial disease from the ocean is more prevalent worldwide, especially in developing countries and in countries that derive most of their protein from seafood. Compared to the viruses, bacteria account for a much lower incidence of disease emanating from the ocean, both in the USA and worldwide. However, it is important to understand and mitigate bacterial disease from the ocean, because of such environmental pressures as global warming, antibiotic resistance, pollution, breakdowns in sanitation (e.g., Haiti after the earthquake) and tourism.
Introduction
Myriad bacteria reside in the ocean and most (>99.9%) have not been isolated and are known only by their unique molecular signatures (e.g., 16 S rRNA sequences) [35, 59]. These bacteria belong to the domain Bacteria which exhibits extensive biodiversity, only exceeded by the biodiversity within the domain Archaea and the viruses. The vast majority of bacteria in the ocean do not cause disease and Archaea are not known to cause any human disease [39]; however, a very small number (percentage) of bacterial species found in the ocean cause pathogenesis in plants and animals. Some of these pathogens are indigenous to the ocean and are defined as autochthonous. Others (allochthonous bacteria) are of exogenous or terrestrial origin and are introduced to the ocean via surface runoff, rivers and streams, atmospheric fallout and ocean disposal of wastes (intentional or accidental); the chapter on enteric viruses (See S.NO.12, J. Woods, Waterborne Diseases of the Ocean, Enteric Viruses, this volume) has a nice discussion of allochthonous sources. This chapter will focus on those allochthonous and autochthonous bacteria that cause waterborne and foodborne disease in humans. Some also cause disease in marine animals (and a few in marine plants) but nonhuman diseases will not be addressed in this chapter.
Autochthonous human pathogens have evolved in the ocean and for largely unknown reasons have the ability to infect and cause disease in humans. Almost all of these diseases result from ingesting seawater, eating seafood, or broken skin contact (swimming, wading, or working in seawater). The allochthonous human pathogens are transients in the ocean with varying abilities to survive in seawater; all of the allochthonous pathogens infect humans via the same routes as autochthonous pathogens, i.e., contaminated seawater, seafood or broken skin contact. There are a few bacteria that may fit both definitions, and there is no current scientific consensus about the place of these bacteria. Examples of these ubiquitous bacteria include the enterococci [159], Staphylococcus aureus (see Allochthonous Pathogens in this chapter) and Pseudomonas aeruginosa [114].
In the following pages, allochthonous and autochthonous marine bacteria that cause disease(s) in humans will be discussed in terms of their biology, ecology, pathogenesis, and epidemiology. Disease treatment will also be discussed but not in clinical detail.
Autochthonous Pathogens
Autochthonous pathogens generally cause one or more diseases in marine animals and if the disease(s) is transmissible to humans it is classified as a zoonosis. It some cases, humans can transmit disease to marine animals.
Vibrio
Vibrios, and specifically Vibrio cholerae, were first observed by Pacini in 1854 and later isolated in pure culture from cholera patients by Robert Koch in 1883 [8, 27]. Today, the Vibrios comprise a large genus (>80 species) and belong to the Gammaproteobacteria [47]. They are gram-negative rods, often slightly curved (e.g., V. cholerae) and most are motile in liquids by means of one or more polar flagella; on solid surfaces they are motile by means of lateral flagella. Unlike most bacteria, Vibrios possess two circular chromosomes (one large and one small) which are of relevance to this chapter because of the distribution of virulence genes on the two chromosomes. The large chromosome is usually referred to as Chromosome 1 (Ch1) and it tends to contain housekeeping genes (DNA replication, transcription, translation, flagellar synthesis, metabolic pathways). Chromosome 2 (Ch2) tends to contain accessory genes (pathogenicity, antibiotic resistance, host defense avoidance, survival in adverse environments). Most of the Vibrios can metabolize a large number of organic compounds, including sugars, amino acids, fatty acids, carbohydrates, proteins, lipids, alcohols, and selected aliphatic and aromatic hydrocarbons. Indeed, prior to the development of molecular biology methods, the Vibrios were largely identified and classified by these diverse and extensive metabolic traits [22].
In addition to metabolic diversity, the pathogenic Vibrios also possess an array of exotoxins, proteases, transport proteins, attachment mechanisms, and lipases that act as virulence factors. Since Vibrios are gram-negative, they also possess endotoxin which differs in toxicity from strain to strain. Indeed, the Vibrios are well equipped to cause disease in their hosts – accidental or otherwise. In general, the Vibrios are opportunistic pathogens – for both humans and marine animals – and they cause systemic infections, skin lesions and gastroenteritis. In fish, the infections often lead to hemorrhagic skin lesions (known as vibriosis) and pathology in the liver, spleen, and kidney. In humans, the diseases arise from contamination of cuts and other skin lesions with seawater (and to a lesser extent marine animals, e.g., stingray barbs and barnacles) and from ingestion of raw, undercooked or cooked but re-contaminated seafood and seawater. Depending on the species, skin infections can remain localized or become systemic and ultimately fatal. Oral ingestion of seafood and seawater leads to various degrees of gastroenteritis and, in some cases (e.g., V. vulnificus) life-threatening systemic infections. Although 12 Vibrio spp. are considered to be human pathogens, the predominant human pathogens are V. cholerae, V. parahaemolyticus and V. vulnificus. Table 4.1 presents a recent compilation of Vibrio diseases in the USA. In addition to the eight species listed in Table 4.1, the other human pathogens include V. cincinnatiensis, Photobacterium damselae (initially named V. damsela), V. furnissii, and V. harveyi; these four Vibrios, along with G. hollisae and V. metschnikovii, will not be discussed in this chapter, due to their low incidence of disease in humans.
All of the Vibrios require NaCl to grow properly, although this requirement is minimal for some species, e.g., V. cholerae and V. mimicus. Most if not all Vibrios use a sodium motive force to drive their polar flagella [94, 157] and at least a few species appear to use a sodium motive force to make ATP [37, 138]. Lateral flagella are produced by Vibrios when they grow on solid surfaces; these flagella are driven by a proton motive force [94] and are responsible for swarming. In addition to a requirement for sodium, most Vibrios are mesophiles and, therefore, do best in warmer waters. Recently, it has been suggested that global warming might increase the incidence of Vibrios worldwide [25, 28]. Interestingly, laboratory-confirmed infections with Vibrio spp. began to exceed those from Salmonella, Shiga toxin-producing Escherichia coli O157, Campylobacter and Listeria in late 2000 and this US trend has increased through 2008 [17]. In 2009, the overall rate of foodborne disease caused by Vibrios was 0.35 per 100,000 population [18]. The relative rates of the other four pathogens have either remained level (Salmonella ) or shown a decrease (Shigella rates decreased 40% and STEC O157 decreased 25%) while Vibrio rates have increased by 47% [17]. Some have suggested that because this trend began just before the El Niño years 2002–2003 and continued through the El Niño years 2006–2007, it was caused by global warming. Intriguing as it may be, this observation is circumstantial and cannot be confirmed. However, in 1991 there was an outbreak of cholera in Peru, a country that had not seen this disease for over 100 years [136]. The source of the 1991 outbreak was never determined and two more outbreaks occurred in 1993–1995 and 1997–1998. Gil et al. [56] very nicely demonstrated that the Peru outbreaks in summer 1998 correlated (linear regression, P < 0.001) with the sea surface temperature peak associated with the strong El Niño that year. Colwell et al. [25] and [28] have made similar observations for the Bay of Bengal. In 2004, an outbreak involving cultured raw oysters and V. parahaemolyticus occurred aboard a cruise ship in Prince Edward Sound [96]. Mean water temperatures had been increasing in Prince William Sound (0.21°C per year) since 1997, and in 2004, for the first time, mean daily temperatures in the sound did not drop below 15°C [96]. Johnson et al. [74] reported that when temperatures drop below 15°C V. parahaemolyticus and V. vulnificus are no longer culturable from water and sediment in Mississippi Sound; similar observations have been reported by others, suggesting that 15°C is a limiting temperature for many of the Vibrios. Clearly, it is beginning to look like increasing ocean temperatures are increasing the incidence of Vibrio disease and as more data become available this Vibrio incidence-climate link may be substantiated. Temperature and sodium preferences for the three principal pathogenic Vibrios are shown in Table 4.2. Finally, in the past decade, scientists are using remotely-sensed satellite data, including temperature and salinity, to predict human health risks from pathogenic vibrios in water and oysters [90, 117].
Vibrio alginolyticus
This Vibrio is very common in estuarine and marine waters worldwide; in fact, it is unusual not to isolate V. alginolyticus when culturing coastal and estuarine water samples. It is known for its ability to swarm on isolation media [141] and it often overgrows desired isolates. Recently, it was demonstrated that V. alginolyticus is capable of quorum sensing and that QS is responsible for biofilm formation (swarming is a prelude to this phenomenon) and development of virulence factors involved with fish disease [64].
The most common disease caused by V. alginolyticus in humans is wound infection. Of the 99 infections reported to the CDC in 2008 (Table 4.1), 64 isolates came from wound infections, 5 from blood, 3 from stools and 27 from other specimens. Most infections are mild and self-limiting, although V. alginolyticus has been demonstrated in a few cases of severe necrotizing fasciitis that involved patients at risk because of cirrhosis [66]. Cases of gastroenteritis caused by V. alginolyticus are rare [140], as indicated in Table 4.1. This Vibrio has also caused eye infections [86].
Vibrio cholerae
During the early cholera pandemics of the 1800s, V. cholerae was responsible for millions of deaths and was feared as the most dangerous waterborne human pathogen known [27, 76]. It still causes several thousand deaths annually [153] and a small number of cases occur in the USA each year (see COVIS report cited in Table 4.1). The World Health Organization recently reported that in 2009 the number of cases worldwide (45 countries reporting) was 221,226 with 4,946 deaths (2.24% case fatality rate) [153]. The number of cases in the USA in 2008 was nine and none of these patients died (see COVIS report, Table 4.1). Although molecular detection is very effective and widely used [102] and the genomes of several strains have been fully sequenced, for documentation and epidemiology purposes isolates are still serogrouped by means of their O antigens. The predominant serogroups causing human disease worldwide are O1 and O139; in the USA, the CDC tests for serogroups O1, O75, O139, and O141 (COVIS report cited in Table 4.1).
The classic disease caused by V. cholerae is a rapidly developing, profuse, watery diarrhea that is usually accompanied by severe dehydration. The cholera diarrhea is often called a “rice-water” stool because as the disease progresses the frequent stools are little more than water containing flecks of mucous abraded from the intestinal mucosa. When death occurs, it is because of the severe dehydration (water loss) and acidic coma (loss of sodium bicarbonate to the diarrhea). Historically, the death rate often exceeded 50% and death could result in as few as 24–36 h after onset of symptoms. As noted above [153] the death rate for cholera is now below 5% and most cases of cholera today are little more than a transient diarrhea. In addition to classic cholera, V. cholerae can also cause self-limiting gastroenteritis and wound infections; it has also been implicated in fish disease (eels and ayu). An interesting and illustrative human case occurred after Hurricanes Katrina and Rita and involved a Louisiana couple who consumed properly cooked (boiled) shrimp that had been placed on the ice used by them to transport the raw shrimp. The husband developed a severe case of cholera that caused renal, pulmonary and cardiac failure. He was given ciprofloxacin and aggressive rehydration therapy and he did not die. Of interest is that the husband had a history of common Vibrio risk factors – history of high blood pressure, alcoholism, diabetes, brain tumor, and renal failure that required frequent dialysis. His wife had mild diarrhea and was treated (ciprofloxacin and rehydration) as an outpatient. V. cholerae O1, serotype Inaba, biotype El Tor was isolated from both patients [15].
The main virulence factor associated with cholera is an exotoxin known as the cholera toxin (CTX). CTX is not produced by all strains of V. cholerae, and it is a protein that is composed of two subunits – one A subunit and five B subunits. The ctx genes that encode for these two subunits, ctxA and ctxB, are actually genes in a virus (a bacteriophage or phage) that infects V. cholerae and establishes a lysogenic relationship with its host [148]. The CTX phage that infects V. cholerae is a lambdaphage; and instead of producing more phage when it infects its host, this phage inserts its DNA into the chromosome (Ch1) of the host which then allows the host to produce CTX – a process called lysogenic conversion.
V. cholerae produces other virulence factors, including the toxin-coregulated pilus (TCP) produced by the tcpA gene, repeat-in-toxins (RTXs), and a heat-stable enterotoxin (NAG-ST) that is related to the heat-stable enterotoxin produced by E. coli [135]. The TCP is thought to be necessary for intestinal colonization by V. cholerae and may also serve as an attachment site for CTX phage [148]. Type 2 secretion systems are present in V. cholerae, and these systems provide a physical conduit for the bacteria to secrete toxins into their host cells (see secretion system discussion in “ Vibrio parahaemolyticus ” section).
In closing, prevention and treatment of cholera deserves mention. Cholera has a very low incidence in developed countries, primarily because of good sanitation, but this is not the case in developing countries [68]. In both developed and developing countries, cholera is usually a self-limiting disease requiring minimal treatment other than rehydration and electrolyte replacement; antibiotics are not usually administered. In developing countries where safe drinking water is not readily available, filtration of drinking water is very effective in preventing cholera. A very simple but highly effective filtration procedure was pioneered in Bangladesh [26]. The procedure involves using folded sari cloth (eight layers of old sari) to filter the drinking water; this procedure removes zooplankton to which the cholera bacilli are attached [26].
Vibrio fluvialis
The incidence of disease caused by V. fluvialis is thought to be very low, both in the USA (Table 4.1) and worldwide. This Vibrio primarily causes enteric disease but can cause wound infections and, rarely, other extraintestinal infections.
Vibrio mimicus
This Vibrio is similar to V. cholerae in many ways and early on was thought to be an atypical V. cholerae – hence the species name “mimicus.” The primary disease caused by V. mimicus is gastroenteritis and some strains carry ctx genes as well as other virulence factors found in V. cholerae and other Vibrios.
Vibrio parahaemolyticus
First isolated in Japan from a gastroenteritis outbreak traced to the consumption of shirasu, a popular fish product (272 cases and 20 deaths; [54]), V. parahaemolyticus is the most common cause of foodborne disease in countries that consume high quantities of seafood [61]; in the USA, it is the most common cause of seafood-borne disease (see Table 4.1). As is the case with all the Vibrios that cause human disease, V. parahaemolyticus causes gastroenteritis and wound infections, and it is the most common cause of Vibrio disease in the USA (Table 4.1). V. parahaemolyticus can be isolated from most forms of seafood but is most commonly associated with shellfish [12].
The first V. parahaemolyticus pandemic began in 1996, and it continues to involve three major serotypes – O3:K6, O4:K68, and O1:K untypable [23]. Recent outbreaks are described in Table 4.3.
All V. parahaemolyticus strains possess the tlh (thermolabile hemolysin) gene, and this gene is frequently used to rapidly detect and confirm identification of the species. However, tlh is not unique to V. parahaemolyticus; V. harveyi, V. alginolyticus, and V. fischeri have also been shown to contain a tlh homologue or a related hemolysin gene [72, 134, 149].
When first discovered, it was shown that V. parahaemolyticus had the ability to hemolyze red blood cells in a special culture medium called Watsumaga agar; it was later shown that this hemolysis, called the Kanagawa reaction, was mediated by a hemolysin called thermostable direct hemolysin TDH [67]. Most pathogenic V. parahaemolyticus strains possess the tdh gene and/or the trh (thermostable related hemolysin) gene [73], although some pathogenic strains contain neither tdh nor trh [98]. The tdh genes are located in a pathogenicity island on Ch2 [91]. In general, environmental and food isolates do not contain tdh and trh ([73] and [74]).
Gram-negative bacteria possess a fascinating injection apparatus called secretion systems. These allow bacteria to inject various substances into the cells of Eukarya . As is the case for many bacterial virulence factors, especially those associated autochthonous pathogens, such as the Vibrios; microbiologists understand how these factors function in human pathogenesis but do not know the function of these factors in the environment. To date, six secretion systems (T1SS, T2SS, T3SS, T4SS, T5SS and T6SS) have been described. In 2003, the sequenced genome of V. parahaemolyticus RIMD2210633 was shown to contain two different T3SS genes – T3SS1 and T3SS2 [91]. T3SS1 is located in a pathogenicity island on Ch1, T3SS2 is in a Ch2 pathogenicity island, and it is now known that there are two different T3SS2 – T3SS2α and T3SS2β [103].
Makino et al. [91] identified at least 50 other genes in V. parahaemolyticus that may be involved with pathogenesis. Some of these additional virulence factors include urease [112], attachment mechanisms [60, 130], ToxR [30], and RTX toxin [91].
Vibrio vulnificus
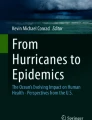
One of the more recently discovered pathogenic Vibrios [46, 123], V. vulnificus,causes serious diseases in humans and is thought by some Vibrio biologists to be the most virulent bacterium now known (death rate >50% in patients at risk [104]; the overall case fatality rate reported by CDC [97] for 1992–1997 was 39%). V. vulnificus is thought to cause three human diseases: primary septicemia (caused by the ingestion of raw or undercooked shellfish – especially oysters), gastroenteritis (caused by the ingestion of raw or undercooked shellfish), and wound infections (caused by contact with water, barnacles, fish barbs, and other marine objects). The literature documenting simple gastroenteritis is scant and, accordingly, some experts question this disease having a V. vulnificus etiology (J.D. Oliver, personal communication). Primary septicemia is a rapidly developing disease that can result in death in less than 48 h after consuming seafood containing the bacteria. The bacteria move from the intestinal tract into the blood stream and, from there, set up serious infections in tissues, especially the extremities. Wound infections also most frequently involve extremities and will cause bullas (Fig. 4.1). When the infection progresses into deep tissue and begins to cause death of that tissue, the disease is called necrotizing fasciitis. The infection shown in Fig. 4.1 did not develop into necrotizing fasciitis but is a good example of what often happens when patients are placed on aggressive antibiotic therapy to prevent progression of the infection. In this case, the patient was given three different antibiotics (clindamycin, levafloxacin, and doxycycline) prior to culture of the lesion, and these antibiotics probably caused the etiological agent to become nonculturable, a phenomenon observed and discussed by others [55, 126].

Wound infection of unknown etiology, caused by a minor scratch from a barnacle. Within 36 h the scratch had developed into a bula (a). The bula was debrided (b) and did not progress into necrotizing fasciitis (Grimes DJ, Ekenna O unpublished data)
In general, V. vulnificus infections in healthy individuals are often not serious, but this is not always the case. Serious and fatal infections can occur in all patients and especially in those at risk; risk factors include: preexisting liver dysfunction or disease, diabetes, alcoholism, poor circulation, and immunosuppressive drug therapy. It is imperative that such individuals at risk are properly counseled about contact with seafood and seawater, so that they do not become infected with any Vibrio capable of causing disease in humans.
The virulence factors associated with V. vulnificus are not well understood. Known factors include V. vulnificus hemolysin (VVH) and RT [104]. There are two genotypes of V. vulnificus – clinical (C) and environmental (E) – and only C causes disease in humans. All strains of V. vulnificus have powerful iron sequestration ability (siderophores) which allows them to out-compete other species (including humans and fish) for essential iron. Capsular polysaccharide (CPS) formation is important and only encapsulated strains are virulent [104]. In addition, endotoxin (the lipoidal moiety of LPS) is very important and may be the most important cause of shock and death from V. vulnificus infections [104]. The complete genomic analysis of V. vulnificus YJ016 revealed the presence of RTX genes and they along with siderophore genes are located on Ch2 [21]. Type IV pilins, used as adherence mechanisms by many Gammaproteobacteria including V. cholerae, are a consistent feature of V. vulnificus and function in biofilm formation, attachment to epithelial cells, and possibly in the colonization of oysters [109, 110]. Other putative virulence factors have been described but their role in pathogenesis is unclear.
Aeromonas
Members of the genus Aeromonas are primarily freshwater bacteria that cause disease in both humans and aquatic animals. The most common isolates from human clinical specimens are A. hydrophila, A. caviae, and A. sobria, with A. hydrophila being the most common. Although Aeromonas spp. are frequently isolated from estuaries and the coastal ocean, they may not be truly autochthonous, and human disease from Aeromonas does not normally result from seawater or seafood. In fact, there is controversy about the ability of Aeromonas, a well-known pathogen of fish and amphibians, to cause disease in humans [48]. If one accepts the literature in support of human disease, it is believed that most human disease occurs in the form of gastroenteritis resulting from the ingestion of fish, shellfish, red meats, and contaminated water [48]. Aeromonas gastroenteritis presents either as a cholera-like disease with watery stools or a dysenteric-like illness that can include bloody stools [48]. Wound infections can also result from contact with contaminated water, either freshwater, seawater or brackish water [14, 75, 144].
Three recent reports of Aeromonas infections are illustrative of this seafood-borne and waterborne pathogen. In the aftermath of the 2004 tsunami that devastated eight countries and caused an estimated 225,000 deaths, the Thai Ministry of Public Health quickly began meeting health care needs in Thailand. From December 26, 2004 (the day of impact) to January 11, 2005, 1,237 cases of acute diarrhea, 356 wound infections, 177 febrile illnesses, and 156 respiratory illnesses were reported to the MOPH; only two deaths (both from aspiration pneumonia) resulted [14]. The most common isolates from the wound infections were Proteus spp., Klebsiella spp., Pseudomonas spp., Enterobacter spp. E. coli, and A. hydrophila (two isolates); surprisingly, no Vibrios were isolated, as was the case with Hurricanes Katrina and Rita.
Eighty-two strains of presumptive Aeromonas spp. were isolated from 250 frozen freshwater fish (Tilapia, Oreochromis niloticus niloticus) intended for human consumption and purchased in local markets in Mexico City. The isolates were identified with standard molecular techniques (16 S rRNA) and 88.3% were placed in two species – A. salmonicida (67.5%) and A. bestiarum (20.9%). The remaining isolates were identified as A. veronii (5.2%), A. encheleia (3.9%), and A. hydrophila (2.6%). The authors noted that this was one of the first major Aeromonas studies conducted in Mexico, and further noted that their results demonstrated the need for concern over putative pathogens with antimicrobial resistance and known virulence factors being present in food meant for human consumption [9].
Finally, a study of the prevalence of A. hydrophila in marketed seafood (fish and prawns) was conducted in land-locked city in South India by Vivekanandhana et al. [145]. Random samples of seafood (536 fish and 278 prawns) were collected from several vendors in a popular seafood market, and fish showing visible spoilage, injury or disease were avoided. Overall, 180 fish samples (33.6%) and 49 prawn samples (17.6%) contained A. hydrophila. The authors attributed the incidence to temperature abuse, fly contamination from a nearby sewage treatment plant, and the ability of A. hydrophila to grow at refrigerator temperatures (4–7°C); and they further noted that A. hydrophila is a pathogen of emerging importance [145].
Edwardsiella
There are three species of Edwardsiella, and the one that causes human disease is the opportunistic pathogen E. tarda. E. tarda causes a Salmonellosis-type enteritis in humans and typically derives from freshwater and freshwater animals (e.g., pet turtles). Infections from marine sources are unknown. E. ictaluria is a serious fish pathogen, often associated with septicemia in catfish (especially in aquaculture of catfish), but it is not known to cause disease in humans or marine fishes.
Yersinia
Several Yersinia spp. cause diseases in humans (Bubonic plague or Black Death, pseudotuberculosis, enteritis, extraintestinal complications) and in fish, including marine fish (salmonids). However, none of the marine fish pathogens are known to cause human disease and will therefore not be discussed here.
Brucella
Long known to cause disease in terrestrial animals and humans, these zoonotic bacteria are now known to exist in the ocean. The classic Brucella spp., B. abortus, B. melitensis and B. suis, cause brucellosis or undulant fever in humans and domestic animals. In domestic animals, the disease outcome is often abortion because the bacteria prefer to metabolize mesoerythritol which is found in the uterus and fetus of animals but not in humans. In humans, symptoms are general and include fever, chills, malaise, with heavy sweating, and high fever at night.
The three classic Brucella species have not been reported in marine mammals. Instead, it appears that marine mammals carry their own Brucella spp. [71], and they have caused three naturally acquired cases of human disease. Two cases were reported in Peru in 2003 (Sohn et al. 2003) and one in New Zealand [95]. The three Brucella human isolates were characterized with several molecular methods, and all three were found to share a common genotype with previously reported marine mammal Brucella spp. [152]. Representing 173 animals and one human patient were analyzed using a molecular method called multiple loci VNTR (variable number of tandem repeats), and the authors targeted 16 genetic loci (MLVA-16) that had been shown to be highly descriptive for Brucella spp. [93]. The study included two new species isolated from marine mammals, B. ceti and B. pinnipedialis, and concluded that these two species cluster into three distinct clades. Interestingly, the three isolates described by Whatmore et al. [152] did not cluster within the three clades but were, however, closely linked to the three marine mammal groups [93].
Enterococcus
Members of the genus Enterococcus are largely commensal colonizing organisms of the gastrointestinal tract of humans and warm-blooded animals and are commonly recovered in their feces [49]. These organisms are gram-positive facultative anaerobes that do not form spores but are capable of survival and growth in a wide variety of environmental conditions. These include tolerance of temperatures ranging from 10°C to 45°C, pH from 4.5 to 9.0 and high sodium chloride concentrations [63]. Although Enterococcus species have been found in many different marine and freshwater environments [85, 92, 124, 143, 158] as well as being associated with processed and fresh fish and seafood [31, 70, 99, 116, 154], these organisms are not usual pathogens for fish or marine mammals. Enterococci are known to be introduced into these environments by sewage contamination from known point sources, such as sewage treatment plants, and are used as indicator organisms for the probable presence of disease-producing pathogens in marine waters [147]. It is unlikely that point sources are the sole contributor of these organisms to an aquatic environment. Domestic and wild animals, water runoff from storms or agricultural sources, wind-driven sediment resuspension events, and humans utilizing the waters have all been shown to contribute to the presence of Enterococcus species in aquatic environments. ([1, 33, 42, 43, 107]; Rebarchik DM, Grimes DJ unpublished data).
The principal pathogenic Enterococcus in humans, Enterococcus feacalis and E faecium, are among the Enterococcus species isolated from aquatic environments; however, Enterococci found in marine settings have not been linked directly to the onset of human enterococcal infections. In general, these organisms are primarily associated with serious, often fatal, nosocomial infections, including postsurgical wound infections, endocarditis, urinary tract infections, and sepsis; and they are currently emerging common pathogens [49]. Enterococci lack significant virulence factors associated with disease but are intrinsically resistant to many antibiotics currently in use. These bacteria, especially E. fecium, are known to easily acquire antibiotic resistance genes from other microorganisms encountered in their environment. In addition to its importance as an indicator organism, the significance of Enterococcus in a marine-water setting is the increased likelihood that the organisms will be exposed to other microorganisms from which they might acquire antibiotic resistance genes, thus adding to the difficulty of treating an already challenging infection.
Streptococcus
Numerous species of fish are susceptible to infection by members of the genus Streptococcus. Although these infections are not common, when they do occur, it is often in an aquaculture setting and can be responsible for significant mortality and large economic costs. One species that is responsible for such infections, Streptococcus iniae,is a primary pathogen for fish that can also infect humans. This organism was first isolated from infected freshwater dolphins in 1996 [113] and has subsequently been associated with sporadic infections in multiple fish species [41, 77, 80, 115]. It was recognized as a human pathogen in the mid-1990s with several documented infections in North America [11, 150], and later in Japan [84]. S. iniae infections in humans present as fever and cellulitis, often with bacterimia, and can be treated with intravenous penicillin and gentamicin [84].
S. agalactiae (Lancefield group B) is a significant human pathogen especially in newborn infants where it can cause sepsis, pneumonia, and meningitis; and in pregnant women where it is associated with urinary tract infections. This organism has been linked to disease outbreaks and some massive kills in several fish species [121]. Investigations performed to type the bacteria isolated from infected fish and environmental samples indicated that sewage contamination was a likely source for the infections in fish [121, 125]. There is no evidence linking fish or a marine environment with human disease.
Listeria
The genus Listeria consists of six species including two that are recognized as pathogens. L. monocytogenes is an important human pathogen, and L. ivanovii is an animal pathogen that may very rarely infect humans but is not associated with marine related infections. L. monocytogenes are short, motile, gram-positive rods that may appear as coccobaccili. They are hardy organisms that grow as facultative anaerobes in a wide range of temperatures (from 1°C to 45°C), pH (pH 4.3 to pH 9), and they tolerate high salt concentrations. They are ubiquitous organisms that are commonly found in soil and water, on vegetation, and decaying matter and excreted in feces of humans and animals [89]. L. monocytogenes is the causative agent of listeriosis, a serious but rare infection caused by eating food contaminated with the bacteria. Multiple types of food have been associated with Listeria infections, classically soft cheeses made from unpasteurized milk, meat and processed meat products, and fish and shell fish [87]. Food may become contaminated before, during, or after preparation; and the usual measures for prevention of growth of contaminating organisms, low temperatures, extremes of pH, and high salt, are ineffective against Listeria. Included among the marine sources implicated in food contamination are crab meats and dips, lobster and shell fish, and many varieties of fish, especially those smoked or processed [6, 36, 81–83]. In a recent report from the CDC addressing the incidence of infection with pathogens that are commonly transmitted via a food borne route, of the greater than that 17,000 culture-proven infections, Listeria accounted for less than 1% of cases with an incidence of 0.34 per 100,000 [18].
Listeriosis occurs primarily in pregnant women, newborn infants, elderly patients, and patients who are immunocompromised, and in all but the newborns; the infections result in an initial mild influenza-like illness that may progress to sepsis and meningitis. In pregnant women, there is an increased risk of miscarriage, and in newborns the infection is associated with a high mortality, up to 40%, and long-term side effects [7, 120]. Adults and children acquire the disease after ingestion of contaminated foods, whereas newborns acquire infecting organisms either transplacentally or via an ascending route during labor and delivery. Onset of the disease varies with population and exposure routes, and it may be from days to weeks. The mortality rates for infections in these populations are high, up to 25%. Listeria are facultative intracellular pathogens, a characteristic that contributes to the severity of listeriosis. After being phagocytosed, the bacterium utilizes unique virulence factors to spread from cell to cell without an extracellular state, thus evading the humoral immune response. Included among these factors are internalins (inlA, inlB, inlC) that facilitate attachment to the cells. Once inside the cell, listerolysin O and phospholipase C enzymes act to release the bacteria to the cytosol where the bacteria utilizes a protein, ActA, to coordinate the assembly of actin into a “tail” that propels the bacterium across one cell and into the next. Listeria infections can be treated with common antibiotics, such as ampicillin, ciprofloxacin, linezolid and azithromicin.
Mycobacterium
The genus Mycobacterium consists of numerous aerobic, nonmotile, non-spore-forming, acid-fast rods that occur widely in nature. These bacteria range from soil-dwelling saprophytes to pathogens of humans and animals. Of the greater than 20 human pathogenic Mycobacterium species, few have been associated with infections from or in a marine environment [155]. Mycobacterium marinum (synonym M balnei) is the primary aquatic pathogen and is a free living organism found throughout the world in both fresh and marine water environments. It was first discovered as a pathogen for fish, causing skin nodules and ulcers, in the mid-1920s and has since been recognized as a natural pathogen for other ectotherms,such as frogs. Since the early 1950s [88] it has been recognized as a cause of human infections first described as causing superficial skin lesions, nodules referred to as “swimming pool granulomas,” in children who swam in contaminated pools. Like most other human pathogenic Mycobacteria, M marinum grows slowly, having a typical incubation period of 2–4 weeks before cutaneous lesions appear, but occasionally may progress rapidly. Unlike other human pathogenic Mycobacteria, it optimally grows at lower temperatures, 30–33°C, and is usually inhibited at 37°C, helping to explain the typical location of the lesions on the extremities and the usual lack of systemic involvement.
Currently M marinum is the most common cause of atypical Mycobacterium infection in humans with a reported incidence of 0.27 cases per 100,000 adults [128] Infection with these organisms can occur at any age, but it usually occurs in adults who handle fresh- or saltwater fish or fish tanks, and is now rarely associated with swimming pools, as proper construction and chlorination has eliminated this source [40]. Human exposure now primarily comes through inoculation of existing skin abrasions while handling fish or their tanks, or directly through fish bites or puncture wounds from fins. Local trauma is an important factor in establishing M marinum infections and their sequelea. Infections obtained after inoculation of an existing abrasion or a direct puncture manifests as a localized nodule or granuloma at the site of bacterial entry that may develop into an ulcer or progress to involve nearby lymph nodes, sporotrichotic lymphangitis. In healthy individuals it rarely progresses to involve bones, joints, or other systemic sites. Immunocompromised states increase the risk for becoming infected and can be associated with more aggressive systemic disease [111, 151]. Diagnosis and treatment are often delayed because of a lack of suspicion for mycobacterial involvement versus more common bacterial pathogens and are contributed to by the long incubation period.
Treatment for M marinum is driven by the severity of the infection [122] and ranges from oral monotherapy with minocycline, clarithromycin, doxycycline, ciprofloxacin, and trimethoprim-sulfamethoxazole for superficial cutaneous infections with susceptible organisms to combination therapies for drug resistant strains. Severe infections, including those with a sporotrichoid distribution pattern, generally require combination therapy with rifampicin and ethambutol. Surgical debridement is not usually recommended, however, other alternative topical therapies, such as cryotherapy, X-ray therapy, electrodesiccation, photodynamic therapy, and local hyperthermic therapy can be effective.
Allochthonous Pathogens
Escherichia
The first species of this genus, Bacterium coli,was first isolated in the late 1800s and it was proposed as an indicator of fecal contamination of water. The isolate was renamed Escherichia coli in 1919 and today remains in use as the fecal indicator recommended by the USEPA for freshwater [142]. Unfortunately, E.coli and the enterococci do not correlate with indigenous pathogens such as the vibrios [29] and enteric viruses (see s.no. 12, J. Woods, Waterborne Disease of the Ocean, Enteric Viruses, this volume). In addition to its worldwide use as a fecal indicator, E. coli is the most common cause of urinary tract disease in humans (ca. 90% of human UTIs): certain strains cause gastroenteritis of various degrees of severity (e.g., STEC or the Shiga toxin-producing E. coli O157 usually derived from meats and produce) and nonpathogenic strains such as E. coli K12 that laid the early foundation for much of what is known about metabolism and enzymology.
Despite extensive documentation of E. coli causing human disease from the consumption of contaminated raw and undercooked foods, oral–fecal transmission in public facilities such as nurseries and day care centers and contaminated drinking water, transmission from seafood and seawater is rare and does not occur in the USA with great frequency. The overall foodborne STEC O157 incidence in the USA for 2009 was 0.99 per 100,000 population, and the STEC non-O157 incidence was 0.57 [18] for many years. This disease agent will not be further discussed in this chapter, and readers interested in this important pathogen are encouraged to peruse other literature.
Shigella
Shigella spp. cause a significant incidence of foodborne disease worldwide, but they are not often acquired from the ocean. Some strains produce the powerful Shiga toxin which, like CTX, is a lysogenic conversion product. In the USA, shigellosis (bacillary dysentery) has a fairly high incidence (3.99 per 100,000) as a foodborne agent of disease [18].
Salmonella
The Salmonellae are important pathogens but are much like E. coli and P. aeruginosa, with regard to their importance as marine pathogens. There are two species of Salmonella, S. enterica and S. bongori, and these two species are comprised of many serovars and subspecies. Both Salmonella enterica serotype Typhi (formerly S. typhi) and the other gastroenteritis-causing Salmonella spp. are human pathogens that historically were frequently acquired from the ingestion of contaminated seafood (especially filter-feeding bivalves, such as raw or undercooked oysters) and seawater. With the advent of fecal indicator monitoring of seafood and seawater, refrigeration of seafood, sanitary surveys (especially surveys of molluscan shellfish beds), and sewage treatment in developed nations, the origin of these diseases from the ocean declined significantly. Today, diseases caused by Salmonellae are still frequent worldwide, most commonly caused by S. enterica subspp. enterica, and they are almost always foodborne in both developed and developing countries (see http://www.who.int/mediacentre/factsheets/fs139/en/; [97]). In the USA, CDC reported a Salmonella foodborne disease incidence of 15.9 per 100,000 population; this is the highest incidence of any foodborne disease, but there was no breakdown on food type, i.e., seafood incidence was not given [18].
Non-typhoid salmonellosis in humans is most commonly gastroenteritis although complications, such as septicemia, can occur; deaths are rare if the patients are kept hydrated and placed on appropriate antibiotic treatment. Virulence is largely determined by pathogenicity islands, and the non-typhoid Salmonellae contain at least 12 of these genetically mobile elements [65]. Human salmonellosis is usually acquired from food, although contaminated water can also serve as a vehicle for transmission. The Food and Agriculture Organization (FAO) of the United Nations recently published a report on the control of Salmonella in sustainable aquaculture, and it contains a very nice review of occurrence and survival in the aquatic environment [44].
The incidence of salmonellosis deriving from seafood in the USA is low but is probably far underreported. DePaola et al. [34] recently provided evidence that, even though the reported incidence is low, the potential for acquisition in the USA certainly exists. They conducted a 2-year study of market oysters collected twice each month from retail establishments (restaurants and raw bars, seafood markets, wholesale dealers) in nine states. In all, FDA collected 397 samples representing 258 establishments. Salmonella was detected in 8.6% of the market oysters, a rate only exceeded by V. parahaemolyticus and V. vulnificus [34].
In the FAO report [44], it was noted that many studies have shown Salmonella serotype Sneftenberg to be the major serotype in marine environments and raw seafood worldwide. The report further noted that Salmonella spp. have been isolated from many marine mammals.
Morganella
Human disease from Morganella morganii is common (postoperative and other nosocomial) but these infections rarely emanate from the ocean. However, M. morganii is often associated with the decomposition of seafood; and if such seafood is consumed, scombroid fish poisoning can result. Scombroid results from histamine build up (and possibly buildup of other vasoactive amines) in the seafood as a result of histidine decarboxylation during the seafood spoilage process. This disease is a true food poisoning or intoxication, as opposed to a food infection, e.g., Salmonellosis and Vibrio gastroenteritis. Scombroid is probably caused by several enteric bacteria, including Proteus, spp. Klebsiella pneumoniae, Hafnia alvei, Enterobacter spp., Serratia spp., and Citrobacter freundii; in addition, V. alginolyticus, Aeromonas spp., and Photobacterium spp. are also histamine formers; and all have been isolated from spoiled fish [139]. The incidence of scombroid in the USA is thought to be common (http://www.fda.gov/Food/FoodSafety/FoodborneIllness/FoodborneIllnessFoodbornePathogensNaturalToxins/BadBugBook/ucm070823.htm), and worldwide incidence is also common. However, because scombroid is not a reportable disease, documented cases are very low, e.g., only 103 incidents involving 4 people were reported from 1968 to 1980 (see above FDA URL). The most common fish involved with this intoxication are tuna, bonito, mackerel, and mahi mahi, and once the amines are formed in the meat, neither cooking, canning, or freezing lowers toxicity. Onset of this intoxication is rapid (often 30 min) and symptoms include a tingling or burning sensation in the mouth, rash on the upper body, and a drop in blood pressure; nausea, vomiting, and diarrhea may also present, and hospitalization may be required.
Pseudomonas
The most common human pathogen in this genus is Pseudomonas aeruginosa,and, like the Vibrios, this species is metabolically very diverse. P. aeruginosa is a very common cause of death in third-degree burn patients, it is a common nosocomial agent of disease, is frequently resistant to most clinically useful antibiotics, it is a cause of urinary tract infections, and it is a common (and often lethal) complication of cystic fibrosis. There have been numerous reports of human P. aeruginosa infections occurring from various types of freshwater contact (e.g., swimming pools, whirlpools, hot tubs, atomizers), but this literature is far too extensive to be summarized here. Although P. aeruginosa is frequently isolated from the coastal ocean [58], the authors are not aware of any literature documenting that disease caused by P. aeruginosa came from the ocean. It is primarily a freshwater bacterium [114].
Campylobacter
Campylobacter spp. are frequently isolated from healthy cattle, chickens, and birds [48], and they are also associated with several foods (unpasteurized milk, poultry, shellfish, fruits, and vegetables), freshwater ponds, and streams contaminated with fecal material [69]; Campylobacters are not normally isolated from seawater. While a few reports of seawater isolations exist [3, 58], most marine isolates come from shellfish [69]. The association with shellfish is similar to that of Salmonella, in that shellfish acquire Campylobacter spp., and usually C. jejuni, from filter-feeding in water contaminated with fecal material [2]. The incidence of foodborne Campylobacter disease in the USA is 13.02 per 100,000, second only to Salmonella [18]. However, seafood-borne disease is rare [2, 69].
Staphylococcus
The genus Staphylococcus is made up of at least 40 species of gram-positive, facultative anaerobic organisms that are found throughout the world. Most of these organisms exist as commensal colonizing organisms of animals and humans, but may also be found in soil, on surfaces and in untreated water. They are hardy organisms that grow in the presence of bile salts and NaCl (up to 6.5%), and they can survive on many types of surfaces for extended periods of time making them a challenge to eliminate in public environments, such as gyms, prisons and hospitals. Staphylococcal species are differentiated from other important gram-positive organisms by the presence of the enzyme catalase, and they are differentiated amongst themselves by the presence of the enzyme coagulase which is present in the more clinically relevant organisms.
Among the organisms that make up this genus are a large variety of coagulase-negative staphylococci (CoNS) that are the primary commensal colonizers of humans. CoNS are pathogenic primarily for compromised populations only, such as preterm infants or persons with implanted prosthetic devices. Staphylococcus aureus is coagulase positive, and this species is the principle pathogen associated with human infection. In humans, S. aureus strains are opportunistic pathogens that may colonize, without infecting, up to 40% of the population [24, 79, 146], but may occasionally gain access to the host, evade the immune response, and causes disease [52, 53]. In addition, these organisms have acquired resistance to most of the antibiotics used against them making treatment of infections challenging.
Most infections caused by S. aureus are limited to the cutaneous tissues and are caused by a person’s own colonizing organisms. However, these bacteria are also capable of causing serious, life threatening systemic disease. In fact, S. aureus including the methicillin resistant S. aureus, MRSA, are among the leading causes of nosocomial infections [10, 78]. Furthermore, MRSA have emerged as significant causes of community as well as hospital-associated infections [38, 78].
The diseases caused by S. aureus in humans and animals are often produced through the action of specific toxins or virulence factors that different bacterial isolates can produce. Specific toxins are associated with particular syndromes, such as toxic shock syndrome toxin and scalded skin syndrome. Many S. aureus are also capable of producing and secreting toxins responsible for staphylococcal food poisoning, termed enterotoxins, that only need to be ingested to cause intoxication and do not require the continued presence of the bacteria for disease. Consumption of seafood contaminated with S. aureus producing enterotoxins leads to staphylococcal food poisoning. Contamination of the food products often comes during processing as is seen in Listeriosis; however, organisms in the water and associated with marine life as seen in Peter the Great Bay, Japan, and Nha Trang Bay, South China, seas may also contribute to human disease [5].
S. aureus including drug resistant MRSA and CoNS have been isolated at recreational beaches, from marine ccc and temperate environments [5, 19, 50, 57, 133]. Adults and toddlers in diapers have been shown to shed S. aureus and the indicator organism Enterococcus into recreational marine waters and sand [118]. Persons using these recreational beaches may transmit and receive these organisms from the environment [42, 51, 131]. A retrospective epidemiological/microbiological monitoring study performed in Hawaii in subtropical marine waters and beaches found that persons were four times more likely to have staphylococcal skin infections if they had a history of seawater contact [20]. Whether there is a correlation of the microbial load in these environments and increased infections is yet to be verified; however, a recent study performed at a South Florida recreational beach did show a correlation between the average number of bathers in the water and the presence of S. aureus [119].
S. aureus and MRSA have also been isolated from marine mammals, including bottlenose dolphins (Tursiops truncates), seals, and walruses (blowholes, gastric fluids, fecal and anal cultures), both in captivity and in the wild, and have been associated with both colonization and disease [45, 105, 129]. In marine mammals in captivity, it is likely that the source of S. aureus and MRSA are colonized human handlers. The source of these organisms for the non-captive animals is not clear; however, colonized wild mammals were primarily identified in locations associated with human recreational use in the estuarine waters of Charleston, SC and Indian River Lagoon, FL [100, 129]. It has been suggested that some of the marine mammals, such as bottlenose dolphins, might serve as sentinels for transfer of resistant organisms from humans and animals into this environment, or simply indicate that the antibiotics are reaching this environment. To date, there are no confirmed cases of human infection from colonized or infected marine mammals.
General Treatment Principles
Many of the marine or ocean-dwelling microorganisms important in human disease are gram-negative bacteria. The diseases caused by these microorganisms run the spectrum, from septicemia (e.g., V. vulnificus), to gastroenteritis, wound infections, ear infections, and eye infections. It is not surprising that treatment is also varied from syndrome to syndrome.
Cholera (V. cholera) is the classic example of a cause of noninflammatory severe gastroenteritis (rice water stools). In cholera, the diarrhea is toxin induced. The pathogenesis of diarrhea in other organisms may be inflammatory (e.g., Salmonella, Campylobacter or Shigella). The nature or mechanism of the diarrhea may affect the primary choice of, or decision regarding, treatment.
As a general rule, severe diarrheal diseases require fluid replacement, given either by mouth (oral rehydration) or by intravenous means as the primary mode of treatment, while inflammatory diarrheas require, in addition to fluids, also antimicrobial therapy. The mode of fluid delivery will depend on how sick the patient is, the availability of which treatment, and the capacity or resources available to deliver the fluid replacement to the patient.
Sometimes, antimicrobial treatment may be detrimental in severe diarrhea. A good example is the bloody diarrhea caused by E. coli 0157:H7, which may lead to hemolytic-uremic syndrome, especially in children exposed to both the toxin-producing E. coli, as well as antibiotic therapy [156]. In such cases, withdrawal of antimicrobial therapy may sometimes help prevent further complications of renal failure [108]. Treatment in this circumstance is entirely supportive.
For toxin-producing diarrheas, antibody binding in situ presents an attractive and elegant option, but this type of therapy has not yet been developed (for all practical purposes) for most diarrheal diseases seen in the clinical setting [101].
Septicemia (e.g., due to V. vulnificus) requires aggressive management in the intensive care unit (ICU) setting, surgical debridement where necessary, as well as antimicrobial therapy. Severe wound infections like necrotizing fasciitis require primary surgical debridement, antimicrobial treatment, and sometimes hyperbaric oxygen therapy.
Most patients with severe wound infections or septicemia do not typically die or have other adverse outcomes due to or as a consequence of antimicrobial resistance, but complications result because they present too late to the hospital, have devitalized tissues that were not promptly debrided, or for other host factor reasons.
In our experience, most Vibrio organisms seen in clinical practice on the Gulf Coast are sensitive to the third-generation cephalosporins (sometimes also to second generation cephalosporins), quinolones, tetracyclines, and aminoglycosides. The same goes for Aeromonas hydrophila, with similar susceptibilities as above, in addition to usual sensitivity to trimethorprim/sulfamethoxazole.
Acute diarrheal illnesses require antimicrobial therapy usually only for a short period (5 days is typically enough); while septicemia (e.g., typhoid fever and Vibrio sepsis) would require longer therapy (2 weeks or longer), depending on the complications.
Severe wound infections of the necrotizing fasciitis type often require multiple surgical debridements, in addition to antimicrobial therapy and local wound care. In addition, skin grafting or plastic surgery is often required to cover defective skin or tissue.
The key to successful treatment of all of these disease entities is timeliness in starting treatment. The earlier appropriate therapy is started, the better the clinical outcome. The later treatment is started, the more complications one can expect. Adjustments in antimicrobial therapy can and should be made after in vitro antimicrobial susceptibility studies are available. However, prompt treatment must be started very early, empirically (best guess or educated guess), before the laboratory susceptibility reports are available.
The Vibrios have predictable antimicrobial susceptibilities, more so than Salmonella, E. coli, or Shigella. Antimicrobial resistance to enteric pathogens reflects the pattern of use of antibiotics in a given environment, as well as the ease of antimicrobial drug availability and abuse in the area or locale where the infection was acquired. Typically for Aeromonas,resistance to ampicillin-like agents and first-generation cephalosporins is common; these agents should therefore not be used to treat infections due to Aeromonas.
In general, a gram-negative bacillus found in coastal or ocean water (outside and far away from a sewage drainage site) is likely to be free-living and, therefore, is more likely to be sensitive to multiple antimicrobial agents. Organisms causing disease acquired through human-to-human or foodborne transmission (e.g., Salmonella), on the other hand, are more likely to have been previously exposed to antibiotics (e.g., in animals or food products). Infections acquired through such contacts may therefore be more resistant to antimicrobials than free-living ocean, river, or brackish water bacteria [4].
The sensitivity of human-to-human or animal-to-human transmitted gram-negative bacteria (E. coli, Salmonella, Shigella, Pseudomonas, etc.) will usually reflect the pattern of local prevailing antimicrobial use in that community. The local hospital’s antibiogram should provide the initial guide in the choice of empiric therapy, with necessary adjustments made after in vitro susceptibility studies are available.
Antimicrobial therapy for Brucellosis is often prolonged (up to 6 weeks) in order to prevent relapse. Often, combination therapy that includes a tetracycline plus rifampin, or an aminoglycoside, is required and recommended for complete cure of this debilitating disease [127, 132].
Acute gastroenteritis caused by food poisoning (e.g., staphylococcal preformed heat-stable enterotoxin) is often rapid in onset (within 1–6 h of food ingestion) and is also self-limited. The symptoms of severe nausea and vomiting occur usually within 1–6 h, and are usually over in less than 24 h [13]. Antimicrobial therapy is usually not required.
Treatment Considerations for Gram-Positive Organisms
Enterococci lack significant virulence factors associated with disease but are intrinsically resistant to many antibiotics currently in use. These bacteria are known to easily acquire antibiotic resistance genes from other microorganisms encountered in their environment. Treatment is guided by the determined antibiotic sensitivities of the infecting organisms and may be prolonged.
Streptococcus iniae infections usually present after exposure to fish with fever and cellulitis, often with bacterimia, and can be treated with intravenous penicillin and gentamicin [84]. S. agalactiae (Lancefield group B) remains sensitive to penicillin.
Listeria infections can be treated with common antibiotics, such as ampicillin, ciprofloxacin, linezolid and azithromicin. The delivery method of antibiotic is determined by the severity of diease.
Treatment for Mycobacterium marinum is driven by the severity of the infection [122] and ranges from oral monotherapy with minocycline, clarithromycin, doxycycline, ciprofloxacin, and trimethoprim-sulfamethoxazole for superficial cutaneous infections with susceptible organisms to combination therapies for drug-resistant strains. Severe infections, including those with a sporotrichoid distribution pattern, generally require combination therapy with rifampicin and ethambutol. Surgical debridement is not usually recommended however other alternative topical therapies such as cryotherapy, X-ray therapy, electrodesiccation, photodynamic therapy, and local hyperthermic therapy can be effective.
The majority of infections by Staphylococcus aureus are cutaneous infections limited to skin and soft tissues. Minor skin infections are usually treated with topical antibiotics, such as a nonprescription triple-antibiotic mixture or mupirocin. In some cases, oral antibiotics may be given for more severe skin infections. If abscesses are present, surgical drainage may be required and for smaller abscesses may be curative. More serious and life-threatening systemic infections are treated with intravenous antibiotics. The choice of antibiotic depends on the susceptibility of the particular staphylococcal strains, as determined by culture results in the laboratory. MRSA from the community may be sensitive to several antibiotics effective against MSSA; however, hospital-associated MRSA are usually resistant multiple antibiotics and may be challenging to treat. Vancomycin remains the drug of choice for multidrug resistant MRSA.
Future Directions
Clearly, most of what is known about waterborne human pathogens is based on laboratory and clinical observations, and this is especially true for autochothonous bacteria. The diseases and metabolic capabilities of these pathogens can be described in great detail, and in many cases the genomes of these bacteria have been completely sequenced. However, until their role or niche in the ocean and in freshwater habitats is fully investigated, it will not be possible to fully understand their ability to cause disease in humans. Accordingly, scientists need to continue asking the question, “how does this microorganism live in the ocean and yet invade humans to cause disease?”
Abbreviations
- Allochthonous:
-
Exogenous, alien or nonindigenous; arising from another source or medium.
- Ambient:
-
Being of the surrounding area or environment.
- Archaea:
-
One of three domains on Earth, including the Bacteria and Eukarya. Archaea are prokaryotes that do not have peptidoglycan cell walls; they lack membrane-bound organelles (e.g., nucleus, mitochondria, endoplasmic reticulum, chloroplasts), possess 70 S ribosomes and have ether-linked lipids in their membranes.
- Autochthonous:
-
Indigenous, native, arising from within.
- Bacteria:
-
One of three domains on Earth, including the Archaea and Eukarya. Bacteria are prokaryotes that possess peptidoglycan cell walls; they lack membrane-bound organelles (e.g., nucleus, mitochondria, endoplasmic reticulum, chloroplasts), possess 70 S ribosomes and have ester-linked lipids in their membranes.
- Biodiversity:
-
The richness or complexity of life forms in an ecosystem, biome or on Earth itself.
- Commensal organism:
-
An organism participating in a symbiotic relationship in which one species derives some benefit while the other is unaffected.
- Ectotherm:
-
An organism that controls body temperature through external means.
- Endotoxin:
-
The lipid component (lipid A) of the outer membrane lipopolysaccharide (LPS) of all gram-negative bacteria. Endotoxin is released into a host or the environment when the cell lyses and its outer membrane breaks up.
- Epidemic:
-
The incidence of disease above the normal or endemic incidence.
- Eukarya:
-
One of three domains on Earth, including the Bacteria and Archaea. Eukarya possess membrane-bound organelles (e.g., nuclei, mitochondria, chloroplasts), histones associated with their DNA and 80 S ribosomes in their cytoplasm. Plants and animals are eukaryotic.
- Exotoxin:
-
Any toxin that is secreted into the cell’s immediate environment. Most exotoxins are proteins, and they are made by both gram-negative and gram-positive bacteria.
- Facultative organism:
-
An organism that is capable of growth both in the presence and absence of oxygen.
- Foodborne disease:
-
A disease that is caused by the ingestion of pathogens conveyed by food.
- Food intoxication:
-
Illness caused by the ingestion of food that contains a toxic substance.
- Hemolysin:
-
A proteolytic enzyme that lyses red blood cells.
- Lysogenic conversion:
-
Insertion of bacterial virus (bacteriophage) DNA into the chromosomal DNA of its bacterial host thereby conferring one or more new traits on the host.
- Nosocomial:
-
Infections (and disease) that are acquired in clinical settings (e.g., hospitals, outpatient clinics, emergency rooms, physician offices).
- Opportunistic pathogen:
-
Any pathogen that accidently acquires entrance to a host and then only causes disease if one or more risk factors are present in the host.
- Pandemic:
-
An epidemic of world-wide proportions.
- Pathogenesis:
-
The production or development of a disease, specifically the cellular reactions and other pathologic mechanisms occurring in the progression of the disease.
- Pathogenic:
-
The ability of a species to cause disease. However, because pathogenesis is typically caused by one or more than one virulence factors produced by one or more genes, any given pathogenic species will often display different degrees of pathogenesis.
- Pathogenicity island:
-
A cluster of virulence genes (and sometimes cryptic genes and other small genetic elements) flanked by direct repeats, insertion sequences or tRNA genes such that the clusters are easily transmitted to other bacteria via a process called horizontal gene transfer.
- Plasmid:
-
A circular, double-stranded DNA molecule containing specialty genes that, in general, are not essential for survival of the host bacterium or genes that are cryptic (unknown). Plasmids can replicate autonomously or integrate into and replicate with the chromosome. Plasmids are smaller than the chromosome, on average 5% the size of the chromosome.
- Point source:
-
A single, identifiable localized source of something.
- Quorum sensing:
-
A chemical mechanism used by bacteria to measure their population density. When the chemical signals reach a certain level, special genes are expressed.
- Sentinel:
-
An indicator whose presence is directly related to a particular quality in its environment at a given location.
- Sequences:
-
The order of nucleotides in a specific length of DNA or RNA.
- Virulence:
-
The degree of pathogenicity. Virulence is a compilation of toxins, hemolysins, proteases and lipases that may not be possessed by all strains of a pathogenic species.
- Waterborne disease:
-
A disease that is transmitted by water.
- Zoonosis:
-
An animal disease transmissible to humans under natural conditions or a human disease transmissible to animals.
Bibliography
Primary Literature
Abdelzaher AM, Wright ME, Ortega C, Solo-Gabriele HM, Miller G, Elmir S, Newman X, Shih P, Bonilla JA, Bonilla TD, Palmer CJ, Scott T, Lukasik J, Harwood VJ, McQuaig S, Sinigalliano C, Gidley M, Plano LR, Zhu X, Wang JD, Fleming LE (2010) Presence of pathogens and indicator microbes at a non-point source subtropical recreational marine beach. Appl Environ Microbiol 76:724–732
Abeyta C, Deeter FG, Kaysner CA, Stott RF, Wekell MM (1993) Campylobacter jejuni in a Washington state shellfish growing bed associated with illness. J Food Prot 56:323–325
Alonso JL, Alonso MA (1993) Presence of Campylobacter in marine waters of Valencia, Spain. Water Res 27:1559–1562
Baya AM, Brayton PR, Brown VL, Grimes DJ, Russek-Cohen E, Colwell RR (1986) Coincident plasmids and antimicrobial resistance in marine bacteria isolated from polluted and unpolluted Atlantic Ocean samples. Appl Environ Microbiol 51:1285–1292
Beleneva IA (2011) Incidence and characteristics of Staphylococcus aureus and Listeria monocytogenes from the Japan and South China seas. Mar Pollut Bull 62(2):382–387
Boerlin P, Boerlin-Petzold F et al (1997) Typing Listeria monocytogenes isolates from fish products and human listeriosis cases. Appl Environ Microbiol 63(4):1338–1343
Bortolussi R (2008) Listeriosis: a primer. CMAJ 179(8):795–797
Brock TD (1999) Robert Koch, a life in medicine and bacteriology. ASM Press, Washington, DC
Castro-Escarpulli G, Figuerasb MJ, Aguilera-Arreolaa G, Solerb L, Ferna´ndez-Rendo´na E, Aparicioa GO, Guarrob J, Chaco´n MR (2003) Characterisation of Aeromonas spp. isolated from frozen fish intended for human consumption in Mexico. Int J Food Microbiol 84:41–49
Centers for Disease Control and Prevention (1999) National Nosocomial Infections Surveillance system report: data from 1997–1999, Atlanta, GA
CDC (1996) Invasive infection due to Streptococcus iniae – Ontario, 1995–1996. Morb Mortal Wkly Rep 45:650–653
CDC (1998) Outbreak of Vibrio parahaemolyticus infections associated with eating raw oysters – Pacific Northwest, 1997. MMWR 47:457–462
CDC (2001) Diagnosis and management of foodborne illnesses: a primer for physicians. MMWR 50(RR02):1–69
CDC (2005) Rapid health response, assessment, and surveillance after a tsunami – Thailand, 2004–2005. MMWR 54:61–64
CDCb (2006) Vibrio parahaemolyticus infections associated with consumption of raw shellfish – three states, 2006. MMWR 55:1–2
CDCa (2006) Two cases of toxigentic Vibrio cholerage O1 infection after Hurricanes Katrina and Rita – Louisiana, October 2005. MMWR 55(02):31–32
CDC (2009) Preliminary FoodNet data on the incidence of infection with pathogens transmitted commonly through food – 10 states, 2008. MMWR 58:333–337
CDC (2010) Preliminary foodnet data on the incidence of infection with pathogens transmitted commonly through food – 10 states, 2009. MMWR 59:418–422
Charoenca N, Fujioka R (1993) Assessment of staphylococcus bacteria in Hawaii marine recreational waters. Water Sci Technol 27:283–289
Charoenca N, Fujioka RS (1995) Association of staphylococcal skin infections and swimming. Water Sci Technol 31:11–17
Chen C-Y, Wu K-M, Chang Y-C, Chang C-H, Tsai H-C, Liao T-L, Liu Y-M, Chen H-J, Shen AB-T, Li J-C et al (2003) Comparative genome analysis of Vibrio vulnificus, a marine pathogen. Cold Spring Harbor Laboratory Press, pp 2577–2587
Colwell RR, West PA, Maneval D, Remmers EF, Elliot EL, Carlson NE (1984) Ecology of the pathogenic vibrios in Chesapeake Bay. In: Colwell RR (ed) Vibrios in the environment. Wiley, New York
Chowdhury NR, Chakraborty S, Ramamurthy T, Nishibuchi M, Yamasaki S, Takeda Y, Nair GB (2000) Molecular evidence of clonal Vibrio parahaemolyticus pandemic strains. Emerg Infect Dis 6:631–636
Cole AM, Tahk S, Oren A, Yoshioka D, Kim YH, Park A, Ganz T (2001) Determinants of Staphylococcus aureus nasal carriage. Clin Diagn Lab Immunol 8:1064–1069
Colwell RR (1996) Global climate and infectious disease: the cholera paradigm. Science 274:2025–2031
Colwell RR, Huq A, Islam MS, Aziz KMA, Yunus M, Khan NH, Mahmud A, Sack RB, Nair GB, Chakraborty J, Sack DA, Russek-Cohen E (2003) Reduction of cholera in Bangladeshi villages by simple filtration. Proc Natl Acad Sci 100:1051–1055
Colwell RR (2006) A global and historical perspective of the genus Vibrio. In: Thompson FL, Austin B, Swings J (eds) The biology of Vibrios. ASM Press, Washington, DC, pp 3–11
Constantin de Magny G, Murtugudde R, Sapiano MRP, Nizam A, Brown CW, Busalacchi AJ, Yunus M, Nair GB, Gil AI, Lanata CF, Calkins J, Manna B, Rajendran K, Bhattacharya MK, Huq A, Sack RB, Colwell RR (2008) Environmental signatures associated with cholera epidemics. Proc Natl Acad Sci 105:17676–17681
Cook DW, Ruple AD (1989) Indicator bacteria and Vibrionaceae multiplication in post-harvest shellstock oysters. J Food Prot 52:343–349
Croci L, Suffredini E, Cozzi L, Paniconi M, Ciccaglioni G, Colombo MM (2007) Evaluation of different polymerase chain reaction methods for the identification of Vibrio parahaemolyticus strains isolated by cultural methods. J AOAC Int 90:1588–1597
Dalgaard P, Vancanneyt M et al (2003) Identification of lactic acid bacteria from spoilage associations of cooked and brined shrimps stored under modified atmosphere between 0 degrees C and 25 degrees C. J Appl Microbiol 94(1):80–89
DePaola A, Kaysner CA, Bowers J, Cook DW (2000) Environmental investigations of Vibrio parahaemolyticus in oysters after outbreaks in Washington, Texas, and New York (1997 and 1998). Appl Environ Microbiol 66:4649–4654
DePaola A, Nordstrom JL, Bowers JC, Wells JG, Cook DW (2003) Seasonal abundance of total and pathogenic Vibrio parahaemolyticus in Alabama oysters. Appl Environ Microbiol 69:1521–1526
DePaola A, Jones JL, Woods J, Burkhardt W III, Calci KR, Krantz JA, Bowers JC, Kasturi K, Byars RH, Jacobs E, Williams-Hill D, Nabe K (2010) Bacterial and viral pathogens in live oysters: 2007 United States survey. Appl Environ Microbiol 76:2754–2768
DeLong EF, Pace NR (2000) Environmental diversity of bacteria and archaea. Syst Biol 50:470–478
Destro MT (2000) Incidence and significance of Listeria in fish and fish products from Latin America. Int J Food Microbiol 62(3):191–196
Dibrov P (2005) The sodium cycle in Vibrio cholerae: riddles in the dark. Biochemistry (Mosc) 70:150–153
Diep BA, Carleton HA et al (2006) Roles of 34 virulence genes in the evolution of hospital- and community-associated strains of methicillin-resistant Staphylococcus aureus. J Infect Dis 193(11):1495–1503
Eckburg PB, Lepp PW, Relman DA (2003) Archaea and their potential role in human disease. Infect Immun 71:591–596
Edelstein H (1994) Mycobacterium marinum skin infections. Report of 31 cases and review of the literature. Arch Intern Med 154(12):1359–1364
Eldar A, Bejerano Y, Bercovier H (1994) Streptococcus shiloi and Streptococcus difficile: two new streptococcal species causing a meningoencephalitis in fish. Curr Microbiol 28:139–143
Elmir SM, Wright ME, Abdelzaher A, Solo-Gabriele HM, Fleming LE, Miller G, Rybolowik M, Peter Shih MT, Pillai SP, Cooper JA, Quaye EA (2007) Quantitative evaluation of bacteria released by bathers in a marine water. Water Res 41:3–10
Elmir SM, Shibata T, Solo-Gabriele HM, Sinigalliano CD, Gidley ML, Miller G, Plano LR, Kish J, Withum K, Fleming LE (2009) Quantitative evaluation of enterococci and Bacteroidales released by adults and toddlers in marine water. Water Res 43:4610–4616
FAO (2010) FAO expert workshop on the application of biosecurity measures to control Salmonella contamination in sustainable aquaculture. Food and Agriculture Organization of the United Nations, Rome (ISBN 978-92-5-106553-2)
Faires MC, Gehring E et al (2009) Methicillin-resistant Staphylococcus aureus in marine mammals. Emerg Infect Dis 15(12):2071–2072
Farmer JJ (1980) Revival of the name Vibrio vulnificus. Int J Syst Bacteriol 30:656
Farmer JJI, Janda M, Brenner FW, Cameron DN, Birkhead KM (2005) Genus 1. Vibrio. In: Brenner DJ, Krieg NR, Staley JT, Garrity GM (eds) Bergey’s manual of systematic bacteriology, vol 2, The proteobacteria, Part B. The gammaproteobacteria. Springer, New York, pp 494–546
FDA (2009) Bad bugs book: foodborne pathogenic microorganisms and natural toxins handbook. http://www.fda.gov/Food/FoodSafety/FoodborneIllness/FoodborneIllnessFoodbornePathogensNaturalToxins/BadBugBook/ucm070523.htm
Fisher K, Phillips C (2009) The ecology, epidemiology and virulence of Enterococcus. Microbiology 155(Pt 6):1749–1757
Fleisher JM, Fleming LE et al (2010) The BEACHES Study: health effects and exposures from non-point source microbial contaminants in subtropical recreational marine waters. Int J Epidemiol 39(5):1291–1298
Fleming L, Solo Gabriel H et al (2008) Final report on the pilot epidemiologic assessment of microbial indicators for monitoring recreational water quality in marine sub/tropical environments. The NSF NIEHS OHH Center, Rosenstiel School of Marine and Atmospheric Sciences, University of Miami, Miami
Foster TJ (2004) The Staphylococcus aureus “superbug”. J Clin Invest 114(12):1693–1696
Foster TJ (2005) Immune evasion by staphylococci. Nat Rev Microbiol 3(12):948–958
Fujino T, Okuno Y, Nakada D, Aoyama A, Fukai K, Mukai T, Ueho T (1953) On the bacteriological examination of shirasu-food poisoning. Med J Osaka Univ 4:299–304
Gefen O, Mumcuoglu M, Engel G, Balaban NQ (2008) Single-cell protein induction dynamics reveals a period of vulnerability to antibiotics in persister bacteria. Proc Natl Acad Sci 105:6145–6149
Gil AL, Louis VR, Rivera ING, Lipp E, Huq A, Lanata CF, Taylor DN, Russek-Cohen E. Choopun N, Sack RB, Colwell RR (2004) Occurance and distribution of Vibrio cholerae in the coastal environment of Peru. Environ Microbiol 6:699–706
Goodwin KD, Pobuda M (2009) Performance of CHROMagar Staph aureus and CHROMagar MRSA for detection of Staphylococcus aureus in seawater and beach sand–comparison of culture, agglutination, and molecular analyses. Water Res 43:4802–4811
Grimes DJ, Singleton FL, Stemmler J, Palmer LM, Brayton P, Colwell RR (1984) Microbiological effects of wastewater effluent discharge into coastal waters of Puerto Rico. Water Res 18:613–619
Grimes DJ, Mills AL, Nealson KH (2000) The importance of viable but nonculturable bacteria in biogeochemistry. In: Colwell RR, Grimes DJ (eds) Nonculturable microorganisms in the environment. ASM Press, Washington, DC, pp 209–227
Guvener ZT, McCarter LL (2003) Multiple regulators control capsular polysaccharide production in Vibrio parahaemolyticus. J Bacteriol 185:5431–5441
Hara-Kudo Y, Saito S, Ohtsuka K, Yamasaki S, Yahiro S, Nishio T, Iwade Y, Otomo T, Konuma H, Tanaka H, Nakagawa H, Sugiyama K, Sugita-Konishi Y, Kumagai S (2010) Decreasing Vibrio parahaemolyticus infections and analysis of seafood contamination in Japan. Vibrios in the Environment-2010, Biloxi, MS (Abstracts)
Harth E, Matsuda L, Hernández C, Rioseco ML, Romero J, González-Escalona N, Martínez-Urtaza J, Espejo RT (2009) Epidemiology of Vibrio parahaemolyticus outbreaks, southern Chile. Emerg Infect Dis 15:163–168
Harwood VJ, Whitlock J, Withington V (2000) Classification of antibiotic resistance patterns of indicator bacteria by discriminant analysis: use in predicting the source of fecal contamination in subtropical waters. Appl Environ Microbiol 66:3698–3704
He H, Wang Q, Sheng L, Liu Q, Zhang Y (2010) Functional characterization of Vibrio alginolyticus twin-arginine translocation system: Its roles in biofilm formation, extracellular protease activity, and virulence towards fish. Curr Microbiol. doi:10.1007/s00284-010-9844-6
Hensel M (2004) Evolution of pathogenicity islands of Salmonella enterica. Int J Med Microbiol 294:95–102
Ho PL, Tang WM, Lo KS, Yuen KY (1998) Necrotizing fasciitis due to Vibrio alginolyticus following an injury inflicted by a stingray. Scand J Infect Dis 30:192–193
Honda T, Iida T (1993) The pathogenicity of Vibrio parahaemolyticus and the role of thermostable direct haemolysin and related haemolysins. Rev Med Microbiol 4:106–113
Huq A, Sack RB, Nizam A, Longini IM, Balakrish Nair G, Ali A, Morris JG Jr, Khan MNH, Siddique AK, Yunus M, Albert MJ, Sack DA, Colwell RR (2005) Critical factors influencing the occurrence of Vibrio cholerae in the environment of Bangladesh. Appl Environ Microbiol 71:4645–4654
Jacobs-Reitsma W (2000) Campylobacter in the food supply. In: Nachamkin I, Blaser MJ (eds) Campylobacter, 2nd edn. ASM Press, Washington, DC, pp 467–480
Jaffres E, Sohier D et al (2009) Study of the bacterial ecosystem in tropical cooked and peeled shrimps using a polyphasic approach. Int J Food Microbiol 131(1):20–29
Jensen AE, Cheville NF, Thoen CO, MacMillan AP, Miller WG (1999) Genomic fingerprinting and development of a dendrogram for Brucella spp. isolated from seals, porpoises, and dolphins. J Vet Diagn Invest 11:152–157
Jia A, Woo NY, Zhang XH (2010) Expression, purification, and characterization of thermolabile hemolysin (TLH) from Vibrio alginolyticus. Dis Aquat Organ 90:121–127
Johnson CN, Flowers AR, Young VC, Gonzalez-Escalona N, DePaola A, Grimes DJ (2009) Genetic relatedness among tdh + and trh + Vibrio parahaemolyticus cultured from Gulf of Mexico oysters (Crassostrea virginica) and surrounding water and sediment. Microb Ecol 57:437–443
Johnson CN, Flowers AR, Noriea NF III, Zimmerman AM, Bowers J, DePaola A, Grimes DJ (2010) Relationships between environmental factors and pathogenic vibrios in the northern Gulf of Mexico. Appl Environ Microbiol 76:7076–7084
Joseph SW, Daily OP, Hunt WS, Seidler RJ, Allen DA, Colwell RR (1979) Aeromonas primary wound infection of a diver in polluted waters. J Clin Microbiol 10:46–49
Kaper JB, Morris JG, Levine MM (1995) Cholera. Clin Microbiol Rev 8:48–86
Kitao T, Aoki T, Sakoh R (1981) Epizootic caused by beta-hemolytic Streptococcus species in cultured freshwater fish. Fish Pathol 19:173–180
Klevens RM, Morrison MA, Nadle J, Petit S, Gershman K, Ray S, Harrison LH, Lynfield R, Dumyati G, Townes JM, Craig AS, Zell ER, Fosheim GE, McDougal LK, Carey RB, Fridkin SK (2007) Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA 298:1763–1771
Kluytmans J, van Belkum A, Verbrugh H (1997) Nasal carriage of Staphylococcus aureus: epidemiology, underlying mechanisms, and associated risks. Clin Microbiol Rev 10:505–520
Kusuda R (1992) Bacterial fish diseases in marineculture in Japan with special emphasis on streptococcosis. Isr J Aquacult 44:140
Lappi VR, Ho A et al (2004) Prevalence and growth of Listeria on naturally contaminated smoked salmon over 28 days of storage at 4 degrees C. J Food Prot 67(5):1022–1026
Lappi VR, Thimothe J et al (2004) Longitudinal studies on Listeria in smoked fish plants: impact of intervention strategies on contamination patterns. J Food Prot 67(11):2500–2514
Lappi VR, Thimothe J et al (2004) Impact of intervention strategies on Listeria contamination patterns in crawfish processing plants: a longitudinal study. J Food Prot 67(6):1163–1169
Lau SK, Woo PC et al (2003) Invasive Streptococcus iniae infections outside North America. J Clin Microbiol 41(3):1004–1009
Lauková A, Juris P (1997) Distribution and characterization of Enterococcus species in municipal sewages. Microbios 89:73–80
Li XC, Xiang ZY, Xu XM, Yan WH, Ma JM (2009) Endophthalmitis Caused by Vibrio alginolyticus. J Clin Microbiol 47:3379–3381
Lianou A, Sofos JN (2007) A review of the incidence and transmission of Listeria monocytogenes in ready-to-eat products in retail and food service environments. J Food Prot 70(9):2172–2198
Linell F, Norden A (1954) Mycobacterium balnei, a new acid-fast bacillus occurring in swimming pools and capable of producing skin lesions in humans. Acta Tuberc Scand Suppl 33:1–84
Liu D (ed) (2008) Handbook of Listeria monocytogenes. CRC Press, Boca Raton
Louis VR, Russek-Cohen E, Choopun N, Rivera ING, Gangle B, Jiang SC, Rubin A, Patz JA, Huq A, Colwell RR (2003) Predictability of Vibrio cholerae in Chesapeake Bay. Appl Environ Microbiol 69:2773–2785
Makino K, Oshima K, Kurokawa K, Yokoyama K, Uda T, Tagomori K, Iijima Y, Najima M, Nakano M, Yamashita A, Kubota Y, Kimura S, Yasunaga T, Honda T, Shinagawa H, Hattori M, Iida T (2003) Genome sequence of Vibrio parahaemolyticus a pathogenic mechanism distinct from that of V. cholerae. Lancet 361:743–749
Manero A, Blanch AR (1999) Identification of Enterococcus spp. with a biochemical key. Appl Environ Microbiol 65:4425–4430
Maquart M, LeFleche P, Foster G, Tryland M, Ramisse F, Djønne B, Al Dahouk S, Jacques I, Neubauer H, Walravens K, Godfroid J, Cloeckaert A, Vergnaud G (2009) MLVA-16 typing of 295 marine mammal Brucella isolates from different animal and geographic origins identifies 7 major groups within Brucella ceti and Brucella pinnipedialis. BMC Microbiol 9:145. doi:10.1186/1471-2180-9-145
McCarter LL (2006) Motility and chemotaxis. In: Thompson FL, Austin B, Swings J (eds) The biology of Vibrios. ASM Press, Washington, DC, pp 115–132
McDonald WL, Jamaludin R, Mackereth G, Hansen M, Humphrey S, Short P, Taylor T, Swingler J, Dawson CE, Whatmore AM, Stubberfield E, Perrett LL, Simmons G (2006) Characterisation of a Brucella sp. strain as a marine-mammal type despite isolation from a patient with spinal osteomyelitis in New Zealand. J Clin Microbiol 44:4363–4370
McLaughlin JB, DePaola A, Bopp CA, Martinek KA, Napolilli NP, Allison CG, Murray SL, Thompson EC, Bird MM, Middaugh JP (2005) Outbreak of Vibrio parahaemolyticus gastroenteritis associated with Alaskan oysters. N Engl J Med 353:1463–1470
Mead PS, Slutsker L, Dietz V, McCaig LF, Bresee JS, Shapiro C, Griffin PM, Tauxe RV (1999) Food-related illness and death in the United States. Emerg Infect Dis 5:607–625
Meador CE, Parsons MM, Bopp CA, Gerner-Smidt P, Painter JA, Vora GJ (2007) Virulence gene- and pandemic group-specific marker profiling of clinical Vibrio parahaemolyticus isolates. J Clin Microbiol 45:1133–1139
Mejlholm O, Kjeldgaard J et al (2008) Microbial changes and growth of Listeria monocytogenes during chilled storage of brined shrimp (Pandalus borealis). Int J Food Microbiol 124(3):250–259
Morris PJ, Johnson WR et al (2011) Isolation of culturable microorganisms from free-ranging bottlenose dolphins (Tursiops truncatus) from the southeastern United States. Vet Microbiol 148(2–4):440–447
Mukherjee J, Chios K, Fishwild D, Hudson D, O’Donnell S, Rich SM, Donohue-Rolf A, Tzipori S (2002) Human Stx2-specific monoclonal antibodies prevent systemic complications of Escherichia coli O157:H7 infection. Infect Immun 70(2):612–619
Nishibuchi M (2006) Miscellaneous human pathogens. In: Thompson FL, Austin B, Swings J (eds) The biology of Vibrios. ASM Press, Washington, DC, pp 367–381
Noriea NF III, Johnson CN, Griffitt KJ, Grimes DJ (2010) Distribution of type III secretion systems in Vibrio parahaemolyticus from the Northern Gulf of Mexico. J Appl Microbiol 109:953–962
Oliver JD (2006) Vibrio vulnificus. In: Thompson FL, Austin B, Swings J (eds) The biology of Vibrios. ASM Press, Washington, DC, pp 349–366
O’Mahony R, Abbott Y et al (2005) Methicillin-resistant Staphylococcus aureus (MRSA) isolated from animals and veterinary personnel in Ireland. Vet Microbiol 109(3–4):285–296
O’Neill KR, Jones SH, Grimes DJ (1992) Seasonal incidence of Vibrio vulnificus in the Great Bay Estuary of New Hampshire and Maine. Appl Environ Microbiol 58:3257–3262
Oshiro R, Fujioka R (1995) Sand, soil, and pigeon droppings – sources of indicator bacteria in the waters of Hanauma Bay, Oahu, Hawaii. Water Sci Technol 31:251–254
Panos GZ, Betsi GI, Falagas ME (2006) Systematic review: are antibiotics detrimental or beneficial for the treatment of patients with Escherichia coli O157:H7 infection? Aliment Pharmacol Ther 24(5):731–742
Paranjpye RN, Strom MS (2005) A Vibrio vulnificus Type IV pilin contributes to biofilm formation, adherence to epithelial cells, and virulence. Infect Immun 73:1411–1422
Paranjpye RN, Johnson AB, Baxter AE, Strom MS (2007) Role of Type IV pilins in persistence of Vibrio vulnificus in Crassostrea virginica oysters. Appl Environ Microbiol 73:5041–5044
Parenti DM, Symington JS et al (1995) Mycobacterium kansasii bacteremia in patients infected with human immunodeficiency virus. Clin Infect Dis 21(4):1001–1003
Park K-S, Iida T, Yamaichi Y, Oyagi T, Yamamoto K, Honda T (2000) Genetic characterization of DNA region containing the trh and ure genes of Vibrio parahaemolyticus. Infect Immun 68:5742–5748
Peir GB, Madin SH (1976) Streptococcus iniae sp. nov., a beta-hemolytic streptococcus isolated from an Amazon freshwater dolphin, Inia geoffrensis. Int J Syst Bacteriol 26:545–553
Pellett S, Bigley DV, Grimes DJ (1983) Distribution of Pseudomonas aeruginosa in a riverine ecosystem. Appl Environ Microbiol 45:328–332
Perera RP, Johnson SK, Collins MD, Lewis DH (1994) Streptococcus iniae associated with mortality of Tilapia nilotica and T. aurea hybrids. J Aquat Anim Health 6:335–340
Petersen A, Dalsgaard A (2003) Species composition and antimicrobial resistance genes of Enterococcus spp, isolated from integrated and traditional fish farms in Thailand. Environ Microbiol 5(5):395–402
Phillips AMB, DePaolo A, Bowers J, Ladner S, Grimes DJ (2007) An evaluation of the use of remotely sensed parameters for prediction of incidence and risk associated with Vibrio parahaemolyticus in Gulf Coast oysters (Crassostrea virginica). J Food Prot 70:879–884
Plano LR, Garza AC et al (2011) Shedding of Staphylococcus aureus and methicillin-resistant Staphylococcus aureus from adult and pediatric bathers in marine waters. BMC Microbiol 11(1):5
Plano LRW, Shibata T et al (2011) Characterization of Staphylococcus aureus and community associated MRSA at a recreational marine beach in South Florida. J Antimicrob Chemother (in review)
Posfay-Barbe KM, Wald ER (2009) Listeriosis. Semin Fetal Neonatal Med 14(4):228–233
Qasem JA, Sameer A-Z, Salwa A-M, Samee A-A, Ahmed A-M, Al-Sharifi Faisal A-S (2008) Molecular investigation of Streptococcus agalactiae isolates from environmental samples and fish specimens during a massive fish kill in Kuwait Bay. Pakistan J Biol Sci 11:2500–2504
Rallis E, Koumantaki–Mathioudaki E (2007) Treatment of Mycobacterium marinum cutaneous infections. Expert Opin Pharmacother 8(17):2965–2978
Reichelt JL, Bauman P, Bauman L (1979) Study of genetic relationships among marine species Beneckea and Photobacterium by means of DNA/DNA hybridization. Arch Microbiol 1110:101–120
Rice EW, Messer JW et al (1995) Occurrence of high-level aminoglycoside resistance in environmental isolates of enterococci. Appl Environ Microbiol 61(1):374–376
Rivas AL, Gonzalez RN, Wiedmann M, Bruce JL, Cole EM et al (1997) Diversity of Streptococcus agalactiae and Staphylococcus aureus ribotypes recovered from New York dairy herds. Amer J Vet Res 58:482–487
Rivers B, Steck TR (2001) Viable but nonculturable uropathogenic bacteria are present in the mouse urinary tract following urinary tract infection and antibiotic therapy. Urol Res 29:60–66
Roushan MRH, Mohraz M, Hajiahmadi M, Ramzani A, Valayati AA (2006) Efficacy of Gentamicin plus Doxycycline versus Streptomycin plus Doxycycline in the treatment of Brucellosis in humans. Clin Infect Dis 42:1075–1080
Saubolle M (1989) Nontuberculous mycobacteria as agents in human disease in the United States. Clin Microbiol Newslett 11:113–117
Schaefer AM, Goldstein JD et al (2009) Antibiotic-resistant organisms cultured from Atlantic bottlenose dolphins (Tursiops truncatus) inhabiting estuarine waters of Charleston, SC and Indian River Lagoon, FL. Ecohealth 6(1):33–41
Shime-Hattori A et al (2006) Two type IV pili of Vibrio parahaemolyticus play different roles in biofilm formation. FEMS Microbiol Lett 264:89–97
Sinigalliano CD, Fleisher JM et al (2010) Traditional and molecular analyses for fecal indicator bacteria in non-point source subtropical recreational marine waters. Water Res 44(13):3763–3772
Skalsky K, Yahav D, Bishara J, Pitlik S, Leibovici L, Paul M (2008) Treatment of human brucellosis: systematic review and meta-analysis of randomized trials. BMJ 336(7646):701–704
Soge OO, Meschke JS, No DB, Roberts MC (2009) Characterization of methicillin resistant Staphylococcus aureus and methicillin-resistant coagulase negative Staphylococcus spp isolated from US West coast public marine beaches. J Antimicrob Chemother 64:1148–1155
Sun B, Zhang XH, Tang X, Wang S, Zhong Y, Chen J, Austin B (2007) A single residue change in Vibrio harveyi hemolysin results in the loss of phospholipase and hemolytic activities and pathogenicity for turbot (Scophthalmus maximus). J Bacteriol 189:2575–2579
Takeda T, Peina Y, Ogawa A, Dohi S, Abe H, Nair GB, Pal SC (1991) Detection of heat-stable enterotoxin in a cholera toxin gene-positive strain of Vibrio cholerae O1. FEMS Microbiol Lett 64:23–27
Tauxe R, Seminario L, Tapia R, Libel M (1994) The Latin American epidemic. In: Wachsmuth IK, Blake PA, Olsvik O (eds) Vibrio cholerae and cholera: molecular to global perspectives. American Society for Microbiology, Washington, DC
Thompson FL, Hoste B, Vandemeulebroecke K, Swings J (2003) Reclassification of Vibrio hollisae as Grimontia hollisae gen. nov., comb. Nov. Int J Syst Evol Microbiol 53:1615–1617
Tokuda H, Unemoto T (1982) Characterization of the respiration-dependant Na+ pump in the marine bacterium Vibrio alginolyticus. J Biol Chem 257:10007–10014
Tsai YH, Kung H-F, Lee T-M, Lin G-T, Hwang D-F (2004) Histamine-related hygienic quantities and bacteria found in popular commercial scombroid fish fillets in Taiwan. J Food Prot 67:407–412
Uh Y, Park JS, Hwang GY, Jang IH, Yoon KJ, Park HC, Hwang SO (2001) Vibrio alginolyticus acute gastroenteritis: a report of two cases. Clin Microbiol Infect 7:104–106
Ulitzer S (1975) The mechanism of swarming of Vibrio alginolyticus. Arch Microbiol 104:67–71
USEPA (2000) Improved enumeration methods for the recreational water quality indicators: Enterococci and Escherichia coli. EPA/821/R-97/004, Washington, DC
Valdivia E, Martin-Sanchez I et al (1996) Incidence of antibiotic resistance and sex pheromone response among enterococci isolated from clinical human samples and from municipal waste water. J Appl Bacteriol 81(5):538–544
Vally H, Whittle A, Cameron S, Dowse GK, Watson T (2004) Outbreak of Aeromonas hydrophila wound infections associated with mud football. Clin Infect Dis 38:1084–1089
Vivekanandhana G, Hathab AAM, Lakshmanaperumalsamy P (2005) Prevalence of Aeromonas hydrophila in fish and prawns from the seafood market of Coimbatore, South India. Food Microbiol 22:133–137
Von Eiff C, Becker K, Machka K, Stammer H, Peters G (2001) Nasal carriage as a source of Staphylococcus aureus bacteremia. Study Group. N Engl J Med 344:11–16
Wade TJ, Pai N et al (2003) Do U.S. Environmental Protection Agency water quality guidelines for recreational waters prevent gastrointestinal illness? A systematic review and meta-analysis. Environ Health Perspect 111(8):1102–1109
Waldor MK, Mekalanos JJ (1996) Lysogenic conversion by a filamentous phage encoding cholera toxin. Science 272:1910–1914
Wang SX, Zhang XH, Zhong YB, Sun BG, Chen JX (2007) Genes encoding the Vibrio harveyi haemolysin (VHH)/thermolabile haemolysin (TLH) are widespread in vibrios. Wei Sheng Wu Xue Bao 47:874–881
Weinstein MR, Litt M, Kertesz DA, Wyper P, Rose D, Coulter M, McGeer A, Facklam R, Ostach C, Willey BM, Borczyk A, Low DE et al (1997) Invasive infections due to a fish pathogen, Streptococcus iniae. N Engl J Med 337:589–594
Wendt JR, Lamm RC et al (1986) An unusually aggressive Mycobacterium marinum hand infection. J Hand Surg Am 11(5):753–755
Whatmore AM, Dawson CE, Groussaud P, Koylass MS, King AC, Shankster SJ, Sohn AH, Probert WS, McDonald WL (2008) Marine mammal Brucella genotype associated with zoonotic infection. Emerg Infect Dis 14:517–518
WHO (World Health Organization) (2010) Cholera, 2009. Wkly Epidemiol Rec 85:293–308
Wilson IG, McAfee GG (2002) Vancomycin-resistant enterococci in shellfish, unchlorinated waters, and chicken. Int J Food Microbiol 79(3):143–151
Wolinsky E (1992) Mycobacterial diseases other than tuberculosis. Clin Infect Dis 15(1):1–10
Wong CS, Jelacic S, Habeeb RL, Watkins SL, Tarr PI (2000) The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med 342(26):1930–1936
Yakushi T, Maki S, Homma M (2004) Interaction of PomB with the third transmembrane segment of PomA in the Na+-driven polar flagellum of Vibrio alginolyticus. J Bacteriol 186:5281–5291
Yamahara KM, Walters SP et al (2009) Growth of enterococci in unaltered, unseeded beach sands subjected to tidal wetting. Appl Environ Microbiol 75(6):1517–1524
Zimmerman AM, Rebarchik DM, Flowers AR, Williams JL, Grimes DJ (2009) Escherichia coli detection using mTEC agar and fluorescent antibody direct viable counting on coastal recreational water samples. Lett Appl Microbiol 49:478–483
Books and Reviews
Belkin S, Colwell RR (eds) (2005) Pathogenic microorganisms in the sea. Kluwer/Plenum, New York
Colwell RR, Grimes DJ (eds) (2000) Nonculturable microorganisms in the environment. ASM Press, Washington, DC
Walsh PJ, Smith SL, Fleming LE, Solo-Gabriele HM, Gerwick WH (eds) (2008) Oceans and human health: risk and remedies from the sea. Elsevier, St. Louis
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Grimes, D.J., Plano, L.W., Ekenna, O. (2013). Human Bacterial Diseases from Ocean. In: Kanki, P., Grimes, D. (eds) Infectious Diseases. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-5719-0_4
Download citation
DOI: https://doi.org/10.1007/978-1-4614-5719-0_4
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-5718-3
Online ISBN: 978-1-4614-5719-0
eBook Packages: MedicineMedicine (R0)