
Abstract
Cytokines are major regulators of bone homeostasis and influence the function of both osteoblasts and osteoclasts. For instance, receptor activator of NF-kB ligand (RANKL) is a member of the tumor necrosis factor (TNF) family and an essential mediator of osteoclastogenesis. Apart from RANKL, proinflammatory cytokines modulate osteoclast differentiation, amongst them TNF-α is a potent stimulator of osteoclastogenesis. Other proinflammatory cytokines like IL-17 and IL-11 are also stimulators of bone resorption by inducing osteoclast differentiation, whereas others such as interferon-(IFN)-γ and IL-12 suppress osteoclastogenesis and balance enhanced bone resorption. In this chapter, we focus on the IL-1 of cytokine family and summarize their role on bone homeostasis. Members of the IL-1 cytokine family are involved in multiple cellular functions including the innate and adaptive immune system. They are key mediators of inflammation and govern the complex processes of cell trafficking, cytokine and matrix enzyme release, fever responses, and metabolic changes during inflammatory disease.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
- Osteoclast Differentiation
- Bone Homeostasis
- Fever Response
- Systemic Bone Loss
- Induce Osteoclast Differentiation
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Cytokines are major regulators of bone homeostasis and influence the function of both osteoblasts and osteoclasts. For instance, receptor activator of NF-kB ligand (RANKL) is a member of the tumor necrosis factor (TNF) family and an essential mediator of osteoclastogenesis. Apart from RANKL, proinflammatory cytokines modulate osteoclast differentiation, amongst them TNF-α is a potent stimulator of osteoclastogenesis. Other proinflammatory cytokines like IL-17 and IL-11 are also stimulators of bone resorption by inducing osteoclast differentiation, whereas others such as interferon-(IFN)-γ and IL-12 suppress osteoclastogenesis and balance enhanced bone resorption. In this chapter, we focus on the IL-1 of cytokine family and summarize their role on bone homeostasis. Members of the IL-1 cytokine family are involved in multiple cellular functions including the innate and adaptive immune system. They are key mediators of inflammation and govern the complex processes of cell trafficking, cytokine and matrix enzyme release, fever responses, and metabolic changes during inflammatory disease.
2 Interleukin-1
The pro-inflammatory cytokine IL-1 is induced by TNF-α and was first described as factor acting on T and B cells driving immune responses [1]. Since then, it became evident that IL-1 is one of the key players during acute inflammation and produced by multiple cell lineages including macrophages, lymphocytes as well as mesenchymal cells. There are two polypeptides, IL-1α and IL-1β. Both polypeptides bind to the same cell surface receptors and exert similar biological functions. IL-1α is predominantly expressed in the cytoplasm and already active as a pro-form (pro-IL-1α), whereas IL-1β is functionally inactive as a pro-form and only exerts its action after cleavage by the interkeukin-1 converting enzyme. IL-1 has multiple biological functions: it contributes the activation of several leukocyte lineages, endothelial cells, and synovial fibroblasts. In addition, IL-1 is a highly potent inducer of matrix enzyme production by chondrocytes. In addition, IL-1 is essentially involved in the fever response and also plays an important role in glucose metabolism by promoting the death of beta cells in the pancreas and impairing glucose tolerance and promoting diabetes.
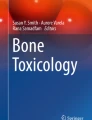
IL-1 was shown to exert potent effects on bone tissue by enhancing bone resorption activity in vitro and in vivo [2]. IL-1 has been shown to prolong the lifespan of osteoclasts [3] and thereby contributing to osteoclast survival and formation. Together with TNF-α, IL-1 appears to play a crucial role in recruiting osteoclasts together with inflammatory cells to inflammation sites and thereby induces local activation of joint destruction. Elegant studies by Wei et al. have shown that TNF induces expression of IL-1 and IL-1R in mesenchymal cells, which both support their osteoclastogenic effects on mononuclear cells [4]. Thus, IL-1 induces RANKL expression in mesenchymal cells and additionally acts directly on osteoclasts by enhancing expression of RANK [4–6] (Fig. 1). Blockade of IL-1 by its soluble receptor antagonist (IL-1ra) or by using mice deficient for the type I IL-1R receptor strongly reduced the potential of TNF to induce osteoclast formation, suggesting that IL-1 represents a major link between TNF and osteoclast formation in vitro and in vivo.

Interleukin-1 induces osteoclastogenesis. MC mesenchymal cell, OCP osteoclast precursor, RANKL receptor activator of nuclear factor kappa B ligand, RANK receptor activator of nuclear factor kappa B
The central role of IL-1 in inflammatory osteoclastogenesis is also supported by the destructive nature of arthritis models, which depend on IL-1, such as collagen-induced arthritis or serum transfer-induced arthritis [7]. Thus, for instance, deficiency of the type I IL-1R does not only achieve excellent protection from inflammatory signs of arthritis in the serum transfer model but also protection from local bone destruction. Even in arthritis, where inflammatory signs of disease are fully TNF-dependent (TNFtg mice) and which do not require IL-1, this cytokine is pivotal for local bone erosion and systemic bone loss [5, 6]. These previous data as well as the observation that over-expression of IL-1 causes osteopenia [8] suggested that IL-1 plays a central role in TNF-mediated systemic inflammatory bone loss as well.
3 Interleukin-18
IL-18 has been described as IFNg inducing factor in the mid-1990s [9]. IL-18 thereby acts in synergy with Il-12 to stimulate the release of IL-18 from TH1 cells. Moreover, IL-18 is involved in the regulation of energy intake and insulin sensitivity. IL-18, like IL-1 is widely expressed in the hematopoietic lineage and also found in mesenchymal cells. It is secreted from the cells and acts in an autocrine and paracrine fashion by engaging its receptor, which shares structural homologies to the IL-1 receptor. The b-subunit thereby forms high affinity complexes with IL-18/IL-18R alpha chain dimmers. IL-18 is expressed in mesenchymal cells such as osteoblasts and its expression is induced by parathyroid hormone [10] (Fig. 2). In fact, the anabolic effect of parathyroid hormone is at least in part mediated by the induction of IL-18 in the osteoblast lineage. Furthermore, binding of IL-18 to osteoblasts stimulates the expression of osteoprotegerin [11]. It is known as a potent suppressor of osteoclastogenesis [12]. Anti-osteoclastogenic activity of IL-18 is particularly strong during the early phase of the differentiation process. The fact that IL-18 induces several potent cytokine inhibitors of osteoclastogenesis such as IFNg and GM-CSF in T cells and explains its strong anti-osteoclastogenic activity, which is reflected by impaired bone resorption when IL-18 is administered. Thereby the induction of GMCSF appears to be essential in mediating the effects of IL-18 on the osteoclast and T cells have been identified as the primary source of GMCSF production elicited by IL-18 [13]. Thus IL-18 exerts profoundly different effects to the skeleton as compared to IL-1 by fostering osteoblast-mediated bone formation and inhibiting osteoclast-mediated bone erosion.

Interleukin-18 blocks osteoclastogenesis. OB osteoblast, OCP osteoclast precursor, PTH parathyroid hormone, OPG osteoprotegerin, GMCSF granulocyte/macrophage colony stimulating factor
4 Interleukin-33
Interleukin (IL)-33 is a recently described member of the IL-1 family [14, 15], constitutively expressed in various tissues, particularly in endothelial cells and epithelial cells exposed to the environment, such as skin, gastrointestinal tract, and the lungs. Similar to IL-1β, IL-33 may act as both a cytokine and a nuclear factor. As a cytokine, IL-33 signals through its interaction with a heterodimeric receptor consisting of membrane-bound ST2L (member of the IL-1 receptor family) and IL-1R accessory protein (IL-1RAcP), leading to NF-kB and MAPkinase activation. ST2L is expressed on monocytes, macrophages, neutrophils, T cells, particularly TH2 (but not TH1 cells), and mast cells. IL-33 is involved in the polarization of IL-5-producing T cells, migration of TH2 cells, activation of basophils, mast cells, eosinophils, and alternatively activated macrophages, contributing to allergic response and asthma. IL-33 also promotes chemo-attraction of neutrophils to inflammatory sites and attenuates poly-microbial sepsis and mediates mast cell-dependent arthritis.
IL-33 is expressed in the bone tissue and acts as a bone protective cytokine by effectively blocking osteoclastogenesis and local bone erosions [16]. Exogenously administered IL-33 also blocks TNF-α-mediated local and systemic bone loss in vivo. Conversely, deletion of the IL-33 receptor ST2 in bone marrow cells enhances bone loss [17]. The mechanism by which IL-33 exerts its inhibitory effect on osteoclast differentiation is not likely by the regulation of OPG or RANKL synthesis. Instead IL-33 directly acts on human and mouse bone marrow CD11b+ cells by inhibiting their development toward mature osteoclasts. IL-33 appears to shift the osteoclast precursor differentiation towards alternatively activated macrophages. IL-33-activated alternatively activated macrophages produce elevated levels of IL-4 and GM-CSF, which are known inhibitors of osteoclast differentiation [17] (Fig. 3). Interestingly, IL-33 is not able to affect osteoclast development when added to committed immature osteoclasts, suggesting that IL-33 acts on the very early step of cell commitment. This phenomenon may also explain the lack of an inhibitory effect of IL-33 on osteoclast development from human peripheral blood CD14+ cells [18, 19].

Interleukin-33 blocks osteoclastogenesis. OCP osteoclast precursor, RANKL receptor activator of nuclear factor kappa B ligand, MC mast cell, DC dendritic cell, GMCSF granulocyte/macrophage colony stimulating factor, IL-4 interleukin-4
5 Summary
IL-1 family members constitute a group of cytokines at the interphase between inflammation and the skeletal system. All three IL-1 family members have potent effects on bone and are particularly involved in the regulation of bone resorption by modulating osteoclast differentiation. Whereas IL-1 is a potent inducer of osteoclastogenesis and bone loss, IL-18 and IL-33 are strongly inhibitors of bone resorption. The pattern of IL-1 family member expression within inflammatory tissue is therefore of key importance for bone damage elicited by inflammation. Clinical relevance of this concept is strongly supported by the bone phenotype of gout, which is a highly IL-1-driven inflammatory process based on uric acid crystal deposition and inflammasome activation, which is accompanied by vast bone resorption induced by IL-1-driven osteoclastogenesis.
References
Gowen M et al (1983) An interleukin 1 like factor stimulates bone resorption in vitro. Nature 306(5941):378–380
Boyce BF et al (1989) Effects of interleukin-1 on bone turnover in normal mice. Endocrinology 125(3):1142–1150
Jimi E et al (1999) Interleukin 1 induces multinucleation and bone-resorbing activity of osteoclasts in the absence of osteoblasts/stromal cells. Exp Cell Res 247(1):84–93
Wei S, Kitaura H, Zhou P, Ross FP, Teitelbaum SL (2005) IL-1 mediates TNF-induced osteoclastogenesis. J Clin Invest 115:282–290
Zwerina J et al (2007) TNF-induced structural joint damage is mediated by IL-1. Proc Natl Acad Sci USA 104(28):11742–11747
Polzer K, Joosten L, Gasser J et al (2010) Interleukin-1 is essential for systemic inflammatory bone loss. Ann Rheum Dis 69(1):284–290
Ji H, Pettit A, Ohmura K, Ortiz-Lopez A, Duchatelle V, Degott C, Gravallese E, Mathis D, Benoist C (2002) Critical roles for interleukin 1 and tumor necrosis factor alpha in antibody-induced arthritis. J Exp Med 196(1):77–85
Aoki Y, Ichimura S, Kikuchi T, Yoshihara Y, Kogawa M, Tada N, Nemoto K et al (2005) Overexpression of the human Interleukin 1a gene causes osteopenia in mice. J Rheumatol 32:320–324
Okamura H et al (1995) Cloning of a new cyokine that induces IFN-g production by T cells. Nature 378:88–91
Ragatt LJ et al (2008) Interleukin-18 is regulated by parathyroid hormone and is required for its bone anabolic actions. J Biol Chem 283:6790–6798
Makiishi-Shimobayashi C, Tsujimura T, Iwasaki T, Yamada N, Sugihara A, Okamura H, Hayashi S, Terada N (2001) Interleukin-18 up-regulates osteoprotegerin expression in stromal/osteoblastic cells. Biochem Biophys Res Commun 281(2):361–366
Udagawa N et al (1997) Interleukin 18 (interferon-g-inducing factors) is produced by osteoblastst and acts via granulocyte/macrophage colony stimulating factor and not via interferon-g to inhibit osteoclast formation. J Exp Med 185:1005–1012
Horwood NJ et al (1998) Interleukin 18 inhibits osteoclast formation via T cell production of granulocyte macrophage colony-stimulating factor. J Clin Invest 101(3):595–603
Schmitz J et al (2005) IL-33, an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-associated cytokines. Immunity 23:479–490
Liew FY, Pitman NI, McInnes IB (2010) Disease-associated functions of IL-33: the new kid in the IL-1 family. Nat Rev Immunol 10:103–110
Schulze J, Bickert T, Beil FT et al (2011) Interleukin-33 is expressed in differentiated osteoblasts and blocks osteoclast formation from bone marrow precursor cells. J Bone Miner Res 26:704–717
Zaiss MM, Kurowska-Stolarska M, Böhm C et al (2011) Interleukin (IL)-33 shifts the balance from osteoclast to alternatively- activated macrophage differentiation and protects from TNFa-mediated bone loss. J Immunol 186(11):6097–6105
Mun SH et al (2010) Interleukin-33 stimulates formation of functional osteoclasts from human CD14(+) monocytes. Cell Mol Life Sci 67(22):3883–3892
Saidi S et al (2011) IL-33 is expressed in human osteoblasts, but has no direct effect on bone remodeling. Cytokine 53:347–354
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer New York
About this paper
Cite this paper
Schett, G. (2013). Effects of the Interleukin-1 Cytokine Family on Bone. In: Choi, Y. (eds) Osteoimmunology. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-5366-6_12
Download citation
DOI: https://doi.org/10.1007/978-1-4614-5366-6_12
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-5365-9
Online ISBN: 978-1-4614-5366-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)