
Abstract
The aims of this survey are to document the current use of figures in epidemiological publications and to make proposals for future practice. To do this, the authors identified all 181 analytical epidemiology articles from 10 major medical journals in the period June to August 2008. For each article the number and type of figures were ascertained and each figure was studied for style and contents. The mean number of figures per article was 0.98. Eighty-four articles (46%) had no figures and most others had just one figure. The most common types of figures were plots of estimates, Kaplan–Meier plots, flow diagrams, smooth or model based curves and distributional plots. These 5 groups of plots accounted for 89% of the figures in the survey. For each of these 5 types of figures, examples of good practice were chosen and commented on. From this overview of current practice some general suggestions regarding the use of figures were given. Well-constructed figures greatly add value to the presentation of the study results. However, many authors choose not to include figures and there is room for improvement in the content and presentation of figures that are included.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Graphical data display is a valuable tool for presenting the results of an epidemiologic study. In general, figures have a major visual impact, and if employed properly they can catch the attention of the reader in illustrating and supporting the main results.
In principle, modern computing power makes the construction of figures straightforward, though not necessarily in a form suitable for journal publication. There is much guidance in the general use of graphics both as part of the dynamic process of data analysis and in formally presenting results (Cleveland 1994; Robbins 2004; Tufte 2001; Wilkinson 2005). Much of the focus in medical and epidemiology journals, however, is on specific types of figures, e.g., Kaplan–Meier plots (Pocock et al. 2002) or figures in meta-analyses (Bax et al. 2009). The STROBE initiative published guidelines with advice as to how to report observational studies in epidemiology (Vandenbroucke et al. 2007; von Elm et al. 2007) but these do not mention the use of figures in any detail.
A previous survey has explored the use of figures in clinical trials in major medical journals (Pocock et al. 2007, 2008). The current manuscript extends this work in considering the use of figures in observational studies in epidemiology. We reviewed epidemiologic studies published in 10 general medical and epidemiology journals from June to August 2008, with the goal of highlighting the types of figures in use, and making recommendations for improvements in practice.
2 Materials and Methods
The focus of this survey was analytical epidemiology, that is epidemiology relating health outcomes to exposures in individuals. The authors identified all 181 articles that could be termed analytical epidemiology, published in June to August 2008 in 10 journals. Five specialised epidemiological journals were chosen: American Journal of Epidemiology, Annals of Epidemiology, Epidemiology, International Journal of Epidemiology and Journal of Clinical Epidemiology as well as five major medical journals: Annals of Internal Medicine, British Medical Journal (BMJ), Journal of the American Medical Association (JAMA), Lancet and New England Journal of Medicine.
For each article we noted the number and types of figures used, concentrating on figures presenting data. Photographs and diagrams lacking data were not included in the survey nor were figures from meta-analyses or randomised trials. The first author went through the chosen volumes and identified all the articles that could be classified as analytical epidemiology and if any doubts arose over the classification of an article the remaining author was consulted. Key points for each study were noted such as type of study design (mainly cohort, case–control or cross-sectional) and number and types of figures.
Each figure was then considered carefully by the current authors to assess its content and appropriateness of appearance. To aide these considerations a list of desirable features was drawn up, partly based on the recommendations for the use of figures in clinical trials (Pocock et al. 2007, 2008). This list was concerned with general aspects of figures (e.g., including measures of uncertainty) but also with specific types of figures often included in epidemiological articles (e.g., Kaplan–Meier plots). Having gone through the sample of articles the classification of figures was simplified and common issues regarding each type of figure were identified using the list of desirable features leading to the recommendations at the end of this paper. Some figures were chosen as examples of good practice to illustrate the points the authors wish to make about the use of figures.
In this survey we have not dealt with genetic epidemiology. This field has its own set of figures, which would also merit investigation.
3 Results
3.1 Overall Survey Findings
Table 4.1 shows the main findings from our survey. In this 3-month period there were 181 analytical epidemiology papers identified, of which 62% appeared in the epidemiology journals and 38% in the general medical journals. The American Journal of Epidemiology had the largest number of such articles (53). Overall there were 97 articles (54%) with at least one figure. The mean number of figures per article was 0.98. Most articles had zero or one figure. As regards study design, cohort studies were most common (54%) and 97% of articles described cohort, cross-sectional, case–control or nested case–control studies. Whether or not figures were used did not appear to vary by study type. Twenty-five of the articles describe studies conducted in a clinical setting, such as hospitalised patients followed for recurrence of the disease of interest. The use of figures was more common in studies of this type: figures were used in 72% of these studies compared to 51% of the articles describing research done in a non-clinical setting (P = 0.047).
The most common types of figures were plots of estimates (39 articles) of outcome/risk factor association, which includes forest plots; Kaplan–Meier plots (23 articles) showing failure time outcomes; flow diagrams (20 articles) describing the flow of study subjects through the study; smooth or model based curves (20 articles) displaying the results of a statistical model fitted to the data; and distributional plots (14 articles) describing the study population. These five groups of plots accounted for 89% of the figures in the survey and they will be the ones we will focus on.
In addition, 6 articles had figures showing population incidence or mortality data, mainly as age-standardised rates. Four articles had individual data. This is not so common in analytical epidemiology as the studies often include a large number of subjects and plots showing individual data become very dense. Plots of repeated measures over time were only found in three articles, whereas this type of figure was one of the most common for clinical trials (10) where it is common to measure the treatment effect at certain fixed time points. This seldom occurs in analytical epidemiology.
Table 4.1 indicates that most figures published in epidemiological articles show associations between outcomes and risk factors. Apart from flow diagrams, purely descriptive figures are not that common. The style and content of the 5 most commonly used types of figures (from our survey) are now discussed with examples.
3.2 Plot of Estimates
The most common type of figure was a plot of point estimates of outcome/risk factor associations. These are typically from analyses of binary or time-to-event type outcomes showing odds ratios, relative risk or hazard-ratio estimates. Though they do not always do so, it is desirable that such figures include confidence intervals to display the statistical uncertainty in each point estimate (Frikke-Schmidt et al. 2008; Snape et al. 2008) and hence to avoid overinterpretation of the data. In some articles columns have been used to show the estimates, but since it is really each point estimate that needs to be shown a single symbol is preferred.
A good example of a plot of estimates with confidence intervals is seen Fig. 4.1 in (Frikke-Schmidt et al. 2008) which is a plot of hazard-ratios for ischemic heart disease as a function of high-density lipoprotein. The figure is clear, the axes are well chosen with good labeling and a caption that explains exactly what has been plotted. Another useful feature is that the number of events and total number in each group have been included in the figure making it easier for the reader to draw conclusions from the results: this was generally lacking in other articles. In general the combination of tabular and graphical presentation can add much-needed context to figures and is recommended. In this figure the hazard ratios are plotted on a log-scale allowing details to be seen more clearly and giving symmetric confidence intervals.

Odds ratios (ORs) for non-Hodgkin lymphoma (NHL) among women, by study center, in a pooled analysis of hair-dye use and NHL, 1988–2003. Boxes show results from individual studies; diamonds indicate pooled data. Bars, 95% confidence interval (CI) (Zhang et al. 2008)
Forest plots are included in this type of figure (8 of the 39 plots of estimates). What makes a forest plot slightly different from other figures containing point estimates with confidence intervals is that the forest plot usually shows estimates across different sub-groups or different studies, and sometimes also an overall estimated effect of the exposure of interest. An example of a forest plot is seen here in Fig. 4.1 (Zhang et al. 2008). This figure contains results from a pooled analysis of hair-dye use and non-Hodgkin lymphoma. It is helpful that the size of the square plotted for each estimate is proportional to the number of cases. Also it helps that the odds-ratios are plotted on a log-scale, so that the distance from 0.5 to 1 is the same as from 1 to 2 and each confidence interval is symmetric about the point estimate. It would, however, have been desirable if the numbers of cases and controls that led to each estimate had also been included in the figure. In general, the combination of graphical and tabular data can make a figure much more informative. The overall estimate has been plotted using a different symbol making it easy to distinguish from the individual estimates. It is not clear from the figure or the caption, however, how the overall estimate was calculated. In general it is recommended that the figure and caption stand on their own, providing context and support for the estimates displayed.
3.3 Kaplan–Meier Plot
Kaplan–Meier plots are used to show time-to-event data by groups of interest (e.g., with or without the exposure being studied). The event of interest can be death, but often it is disease incidence and sometimes a positive event such as recovery. Kaplan–Meier type plots can show either the probability of being event-free over time (the curves will go down) or the cumulative incidence (and the curves will go up). The plots of cumulative incidence are sometimes referred to as Nelson–Aalen plots.
A good example of a Kaplan–Meier type plot is found in the figure in (Wood et al. 2008) where the cumulative incidence of mortality has been plotted for injection drug users and non-injection drug users. The two groups are well identified and the axes are clearly labeled with the same axes used for the plots of all-cause mortality and non-accidental mortality allowing visual comparisons to be made (here only the all-cause mortality is shown). Under the horizontal axis the numbers at risk in the two groups are shown at appropriate intervals, another useful combination of graphical and tabular display. The uncertainty of the plots is shown by including confidence intervals at regular intervals (this is rarely done, but as above, acknowledging uncertainty is highly recommended), though it would have been clearer had the two groups’ confidence intervals been slightly staggered to avoid confusing overlap. Also an overall significance test comparing the two groups is included on the figure. If neither the confidence intervals nor a significance test was included in the Kaplan–Meier plot, it would be easy to over interpret any apparent differences in outcome between the exposure groups.
Sometimes the Kaplan–Meier plot is arguably extended for too long when there are very few subjects still at risk and the estimates become very uncertain (e.g., in Limaye et al. 2008). The Kaplan–Meier plot in (Williams et al. 2008) shows survival and the vertical axis is cut off at 0.5, which could make the differences between the groups seem deceptively larger than they really are. It may be better to plot the cumulative incidence (i.e., plot going up) in this type of situation when only a small part of the scale from 1 to 0 is used.
3.4 Flow Diagram
Flow diagrams are used to display the flow of the study subjects through a study. It is an essential part of study reporting for clinical trials (Begg et al. 1996) and can also be of value in many epidemiological studies (Vandenbroucke et al. 2007). In the article (Ix et al. 2008) a flow diagram is used to describe a case–cohort study of incident diabetes mellitus in older persons. The study uses a case–cohort design and the flow chart is effective in making the design clearer for the reader. The sub-cohort is clearly identified and the numbers of exclusions and numbers of incident cases of diabetes during follow-up are documented. In general a flow diagram can be very helpful in understanding the structure of an epidemiological study in both, describing the study subjects (e.g., responders and non-responders to questionnaires in a cross-sectional study), and in explaining more clearly any nuances of study design.
3.5 Smooth or Model Based Curve
A potentially useful way of summarising the results of a study is to show a fitted curve from the statistical model. This can be an eye-catching illustration, but there can be problems for the reader. There is often no information about the model’s goodness of fit and such figures seldom include any numbers, so it can be difficult to know how much to trust the results. Again, inclusion of parsimonious numerical information perhaps arranged in a table, can help matters here. It can also happen that the plotted curve covers a spread of the exposure variable’s distribution where there are few (or even no) data points, thus encouraging unjustified extrapolation. As noted previously, acknowledging the uncertainty in the data, either through the use of confidence regions or by displaying the raw data itself in addition to a smooth curve is critical. Despite these caveats, plotting smooth curves can be a creative way to explore variation in the conclusions of an analysis under different conditions. For instance, a figure showing a combination of a fitted curve from a statistical model with simple point estimates and confidence intervals (e.g., treating an exposure as continuous but also showing results from a categorical analysis) could add much value to both types of analyses.
Figure 4.2 (Lopez-Garcia et al. 2008) shows relative mortality risk by amount of coffee consumption compared to persons drinking no coffee. In this figure 95% confidence interval curves have been included to convey the extent of uncertainty in the estimates. From other results in the article it is seen there are very few individuals drinking more than four cups of coffee per day, so the figure’s extension out to six cups per day seems unwarranted. It is hard to know what to believe from such figures (e.g., how strong is the evidence of non-linearity in this case?), but as a supplement to the tables where the data are described and analysed in more detail (as in the tables in Lopez-Garcia et al. 2008) they can be useful illustrations.

Non-linear relationship between coffee consumption and cardiovascular mortality (Lopez-Garcia et al. 2008)
3.6 Distributional Plot
In this survey the authors found few purely descriptive figures (e.g., histograms, bar charts or box plots). This is probably due to the fact that in an article for a journal the number of tables and figures allowed can be limited, so often a figure showing the main results will be preferred. Nevertheless, some articles included descriptive plots to good effect.
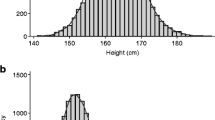
Figure 4.3 (Mikolajczyk et al. 2008) shows the distribution of interpregnancy intervals in the study population. This figure conveys the point clearly that the interpregnancy intervals were usually relatively short and the distribution is skewed to the right. The number of women in the study is usefully included in the caption.

Distribution of interpregnancy intervals in the study population (n = 533), Collaborative Perinatal Project, United States, 1959–1965 (Mikolajczyk et al. 2008)
4 Discussion
A good figure can be very effective in the presentation of results and is more likely to be noticed and remembered by the reader than a dense table full of results. As such it is therefore critical that the impressions conveyed in the graphical format are accurate and properly acknowledge the limits of the data in question. Analytical epidemiology articles can study several exposure/outcome associations, so it is up to the authors of an article to choose wisely which results should be presented as figures. In a study with many results choosing some key findings to present in a figure can help focus the reader’s attention on the main points the authors wish to make.
In this survey we were surprised to find that 46% articles did not include a figure even though it would often have been useful to do so. Given the speed of modern computing and availability of software, choosing not to present a graphical display may undersell a result, where for relatively little cost, a greater emphasis on the main finding could be obtained. For instance, a well-written article (Villamor et al. 2008) about the risk of oral clefts contains no figures. The results presented in the article (their tables 2–4) are odds ratios of cleft palate or cleft lip during second pregnancy by change in mother’s BMI since first pregnancy or by months since first pregnancy. We think the results would have been more readily appreciated by the reader if the odds ratios (with 95% confidence intervals) from the primary analyses were presented in a figure similar in style to the plot of estimates in (Frikke-Schmidt et al. 2008).
As in a prior survey of figures in the reporting of clinical trials (Pocock et al. 2007), the images examined here were of many different types and styles, but the vast majority could be classified into a small number of groups: These included plots of estimates, Kaplan–Meier plots, flow diagrams, smooth or model based curves and distributional plots. How best to present a figure is of course partly a matter of personal taste, but having done this survey we would like to make some general and some more specific points for the construction of figures in the future. Some of these recommendations seem like plain common sense, but it can still be useful to state them clearly.
5 Recommendations
Much has been written about presenting figures in general (Cleveland 1994; Robbins 2004; Tufte 2001; Wilkinson 2005) and such advice is also valid for analytical epidemiology. There are, however, a few points that could be emphasised in this particular setting:
-
It is important that each figure can largely stand alone. That is, key information needed to understand a figure should be included either on the figure itself, in the caption or as a footnote
-
Each exposure group should be clearly labeled within the figure itself, so groups are easily distinguishable. It is also important to choose any colours and symbols carefully as many readers will be seeing the article in black and white
-
Figures should include appropriate measures of uncertainty such as confidence intervals or standard errors. It may also be useful to include appropriate P-values on the figure to help the reader understand the extent to which any association could plausibly be due to chance
5.1 Plots of Estimates
-
Plots of estimates are best presented as points with 95% confidence intervals rather than as bar charts/columns
-
The scale used for the plot should be chosen to give enough detail. Consider using a log-scale especially for hazard-ratios, odds-ratios and risk-ratios, so that confidence intervals are symmetric around the point estimate
-
Any plot of estimates should also include some tabulations to give a better understanding of the data, e.g., number of events and number of subjects in each group. Far too many plots fail to provide such simple information
5.2 Kaplan–Meier Plots
-
Kaplan–Meier plots should include the numbers at risk at regular time points under the horizontal axis
-
When possible plots should include confidence limits at regular time points to give an impression of the uncertainty of the curves
-
The plots should not extend too far over time where there are few subjects left at risk and estimates become unreliable
-
If incidence rates are not high, a plot going up of the cumulative incidence is preferable as this allows differences between exposure groups to be seen more clearly
5.3 Flow Diagram
-
A flow diagram should include the number of subjects and their flow through the study
-
A flow diagram should help communicate the nature of the study design, e.g., number of cases and controls in a case–control study
-
It is important to include the numbers excluded from the analysis in each group and the reason for exclusion (e.g., ineligible prevalent cases in a study of incidence). If a questionnaire is used also include the number of non-responders in each group
5.4 Smooth or Model Based Curves
-
The caption or footnote should include key information about which model has been used to create the figure, and also about the goodness of fit of this model
-
Include confidence intervals to show the variability of the estimated curves
-
It is useful for the reader to know how the exposure data behind the curve are distributed, this could be indicated under the horizontal axis
-
If possible combine a figure of a fitted curve from a statistical model with simple point estimates and confidence intervals (e.g., treating an exposure as continuous but also showing results from a categorical analysis) as this would add much value to both types of analyses
5.5 Distributional Plots
Much is well known about how to present such descriptive plots (Robbins 2004; Tufte 2001). However, there are a couple of specific points arising from our survey.
-
Bar charts are sometimes used to show summary statistics, e.g., means or percentages, but it may be better to have such background data in a table
-
When using box plots it should be stated in the caption or footnote what the end of the whiskers represent. Having too many individual points outside the whiskers can be distracting
6 Conclusion
We would like to encourage a wider use of insightfully informative figures in articles on analytical epidemiology. We hope that our survey of current practice and consequent recommendations prove useful for the construction of such figures in future articles.
References
Bax L, Ikeda N, Fukui N et al (2009) More than numbers: the power of graphs in meta-analysis. Am J Epidemiol 169:249–255
Begg C, Cho M, Eastwood S et al (1996) Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA 276:637–639
Cleveland WS (1994) The elements of graphing data. Hobart Press, Summit, NJ
Frikke-Schmidt R, Nordestgaard BG, Stene MCA et al (2008) Association of loss-of-function mutations in the ABCA1 gene with high-density lipoprotein cholesterol levels and risk of ischemic heart disease. JAMA 299:2524–2532
Ix JH, Wassel CL, Kanaya AM et al (2008) Fetuin-A and incident diabetes mellitus in older persons. JAMA 300:182–188
Limaye A, Kirby KA, Rubenfeld GD et al (2008) Cytomegalovirus reactivation in critically ill immunocompetent patients. JAMA 300:413–422
Lopez-Garcia E, Van Dam RM, Li TY et al (2008) The relationship of coffee consumption with mortality. Ann Intern Med 148:904–914
Mikolajczyk RT, Zhang J, Ford J et al (2008) Effects of interpregnancy interval on blood pressure in consecutive pregnancies. Am J Epidemiol 168:422–426
Pocock SJ, Clayton TC, Altman DG (2002) Survival plots of time-to-event outcomes in clinical trials: good practice and pitfalls. Lancet 359:1686–1689
Pocock SJ, Travison TG, Wruck LM (2007) Figures in clinical trial reports: current practice and scope for improvement. Trials 8:36
Pocock SJ, Travison TG, Wruck LM (2008) How to interpret figures in reports of clinical trials. BMJ 336:1166–1169
Robbins NB (2004) Creating more effective graphs. Wiley-Interscience, Hoboken, NJ
Snape MD, Kelly DF, Lewis S et al (2008) Seroprotection against serogroup C meningococcal disease in adolescents in the United Kingdom: observational study. BMJ 336:1487–1491
Tufte ER (2001) The visual display of quantitative information. Graphics Press, Cheshire, CT
Vandenbroucke JP, von Elm E, Altman DG et al (2007) Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Epidemiology 18:805–835
Villamor E, Sparen P, Cnattingius S (2008) Risk of oral clefts in relation to prepregnancy weight change and interpregnancy interval. Am J Epidemiol 167:1305–1311
von Elm E, Altman DG, Egger M et al (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370:1453–1457
Wilkinson L (2005) The grammar of graphics. Springer, New York
Williams P, Van Dyke R, Eagle M et al (2008) Association of site-specific and participant-specific factors with retention of children in a long-term pediatric HIV cohort study. Am J Epidemiol 167:1375–1386
Wood E, Hogg RS, Lima VD et al (2008) Highly active antiretroviral therapy and survival in HIV-infected injection drug users. JAMA 300:550–554
Zhang Y, Sanjose SD, Bracci PM et al (2008) Personal use of hair dye and the risk of certain subtypes of non-hodgkin lymphoma. Am J Epidemiol 167:1321–1331
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer Science+Business Media, New York
About this chapter
Cite this chapter
Andersen, E.W., Pocock, S.J. (2012). The Use of Figures in Epidemiological Publications: A Survey of Current Practice and Consequent Recommendations. In: Krause, A., O'Connell, M. (eds) A Picture is Worth a Thousand Tables. Springer, Boston, MA. https://doi.org/10.1007/978-1-4614-5329-1_4
Download citation
DOI: https://doi.org/10.1007/978-1-4614-5329-1_4
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4614-5328-4
Online ISBN: 978-1-4614-5329-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)