
Abstract
In this chapter, the technical principles and in particular the surgical approaches required to perform a synovectomy will be discussed (septic arthritis and tumor pathology and synovectomy after TKA are excluded). A synovectomy may be indicated in:
-
Pigmented villonodular synovitis
-
Inflammatory diseases
-
Rare pathologies: chondromatosis, osteochondromatosis, hemangiosclerosis, desmoid tumors
-
More specific synovitis
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Total Knee Arthroplasty
- Skin Incision
- Posterior Cruciate Ligament
- Medial Collateral Ligament
- Lateral Meniscus
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Indications
In this chapter, the technical principles and in particular the surgical approaches required to perform a synovectomy will be discussed (septic arthritis and tumor pathology and synovectomy after TKA are excluded). A synovectomy may be indicated in:
-
Pigmented villonodular synovitis
-
Inflammatory diseases
-
Rare pathologies: chondromatosis, osteochondromatosis, hemangiosclerosis, desmoid tumors
-
More specific synovitis
It must be stressed that a synovectomy is particularly indicated in the young patient with no cartilage loss. For this reason, it is rare for a patient with advanced arthritis secondary to an inflammatory arthropathy to require a synovectomy. A “total” synovectomy in the strictest sense is an overstatement since the configuration of the knee joint is very complex and renders a “total” synovectomy virtually impossible. It would be more appropriate to speak in terms of a “reduction” synovectomy.
The lesions that have not been eradicated during the total synovectomy are better treated with adjuvant chemotherapy or radioactive isotopes. The surgeon must therefore balance the advantages of a total synovectomy with respect to the surgical “goal.” In order to make decisions, some objective parameters have to be taken into account. To do so, the surgeon has to know each of the different surgical approaches to the knee. He can then select one or more approaches dependant on the particular situation. This heterogeneity of treatment options makes analysis of the results even more difficult; however, they also make this type of surgery more interesting.
Preoperative Planning
A diagnostic MRI (with gadolinium injection) is useful in locating the lesions. These images help the surgeon’s decision-making process in planning how to address each of the individual lesions. Perhaps most importantly, they help evaluate whether there is extra-articular extension of the disease in the soft tissues posteriorly. The size and the location of the lesions will define the surgical technique chosen (arthroscopy or open surgery) and the surgical approaches needed.
Plain radiographies of the knee (anteroposterior (AP) view, single-leg weight-bearing view (AP and lateral), schuss (flexed PA) view, and a skyline view of the patella at 45° of flexion) are mandatory. They help to assess any joint space narrowing and identify any bone lesions.
Others imaging techniques have little importance in the detection of lesions except for maybe the arthroCT, which has the advantage of showing the articular cartilage in great detail. If extension in the proximity of vascular structures is suspected, a MRI angiogram can be of great help. In those specific situations, the availability of a vascular surgeon at the time of the intervention is required.
Surgical Techniques
Arthroscopic Synovectomy
Limited Synovectomy
This intervention is indicated in focal PVNS. For the arthroscopy, the patient is placed supine with a vertical lateral post at the level of the proximal femur (to resist the knee during valgus strain) and a horizontal distal post (to hold the knee in the 90° flexed position).
A tourniquet is positioned high on the thigh and inflated to 300 Hg. Its use is helpful for visualization during the arthroscopy since resection of synovitis is typically associated with significant intra-articular bleeding.
The arthroscopic portals are chosen depending on the location of the lesions. The frequently used portals are described in detail in the chapters on arthroscopy and meniscectomy.
For lesions in the suprapatellar pouch or in the notch, the anterolateral and anteromedial portals are frequently sufficient. In order access lesions situated in the femoral gutters, a superolateral or superomedial portal is necessary. For lesions situated more posteriorly in the knee, i.e., behind the PCL or behind the femoral condyles, a posterolateral or posteromedial portals can be necessary as described by Philippe Beaufils.
A posteromedial portal is made with a knee in 90° of flexion. The entry point of this portal is made at the edge of the posteromedial border of the condyle, 1 cm above the joint line. This portal allows visualization of the posterior aspect of the medial condyle and the medial portion of the distal PCL. The round-tipped obturator is then reintroduced into the sleeve, gently perforating the synovial tent covering the PCL while staying in contact with the posterior condyles. The arthroscope is reintroduced into the sleeve and the posterior part of the lateral condyle can be visualized. Transillumination of the posterolateral region is of major importance: the portal has to be ventral to the biceps tendon to eliminate the risk for nerve damage. The posterolateral entry portal can be made with an 11 blade in 90° of flexion following spinal needle localization (Fig. 10.1). The posterolateral portal allows the use of a shaver (Fig. 10.2). Shaving of the lesions in this region can thus be done under arthroscopic control (Fig. 10.3).

Posterolateral entry portal with an 11 blade

Shaver used through the posteromedial portal (posterolateral portal view)

Shaving of the posterior compartment synovial
The instruments used in this technique include a 30° arthroscope, a biopsy grasper and a 5.5 shaver blade. A 70° arthroscope can be of help in the case of a posterior synovectomy. The use of an arthroscopic pump (pressure set at 40 mmHg) helps in visualization due to the possibility of excessive intra-articular bleeding.
When localized PVNS is suspected, we recommend performance of several synovial biopsies in order to confirm that the PVNS is not diffuse.
Total Synovectomy
This surgical approach can be used for diffuse forms of PVNS and for nonspecific synovitis without extra-articular involvement. The volume of the lesions must be fairly limited.
The setup and instrumentation are identical to that required for a “limited” synovectomy. Four portals are used, anterolateral, anteromedial, superolateral, and superomedial, which allow for a total synovectomy in the anterior compartment of the knee using a shaver (Fig. 10.4).

Synovectomy of the anterior compartment
In PVNS, the technique introduced by P. Beaufils is of particular interest when the lesions are situated just posteriorly to the PCL without extra-articular involvement into the popliteal fossa (Fig. 10.5).

Synovectomy of the posterior compartment using P. Beaufils technique
Open Synovectomy (with Arthrotomy)
Limited Synovectomy
This technique can be used for focal PVNS. The arthrotomy allows for a complete “en bloc” resection of the lesions. Many of these lesions could also be addressed arthroscopically. Nevertheless, some areas in the knee are more difficult to access arthroscopically, and in some cases the surgeon could be uncertain about the completeness of the excision (because of the limited accessibility by instruments but also because of the difficulty in interpreting the arthroscopic images). Furthermore, the arthroscopy does not allow an “en bloc” resection of the lesions. Yet, an arthroscopic approach has the advantage to allow a complete exploration of the joint cavity and to perform multiple biopsies. These considerations frequently justify a combination of both techniques. The surgical approach largely depends on the location of the lesion(s) (Figs. 10.6 and 10.7). Each common approach to the knee can thus be used, always taking into account the existence of previous skin incisions.

Cutaneous incision after open limited synovectomy

Resection of localized pigmented villonodular synovitis
Total Synovectomy
The patient is placed in a supine position with a vertical lateral and a horizontal distal post. A tourniquet is inflated high on the thigh. This technique is used for diffuse PVNS and nonspecific synovitis without involvement of the popliteal fossa. We typically use an anteromedial and an anterolateral skin incision (Fig. 10.8). This method avoids one single large midline incision that would require significant subcutaneous dissection resulting in an increased risk for skin necrosis. Arthrotomies posterior to the medial and lateral collateral ligaments allow for intra-articular access posterior to the PCL. Posteromedial lesions situated between the medial head of the gastrocnemius muscle (MGM) and the semimembranosus are accessible by the medial approach. The posteromedial and posterolateral approaches not only give intra-articular access but also allow extra-articular lesions to be addressed.

Cutaneous incision after open total synovectomy
-
(a)
The anteromedial approach
An anteromedial vertical skin incision is made with a knee in 90° of flexion starting 1 cm proximal to the patella and extending distally to a point just medial to the tibial tuberosity.
The length of incision is about 8–10 cm. An extended resection of the supra patellar pouch can thus be done using a scalpel with the knee in extension and the extensor apparatus retracted with a Farabeuf retractor. (For a complete resection of this area, it is advised to combine this approach with an anterolateral approach.) A Volkman retractor is used to retract the anteromedial capsule. A synovectomy of the medial gutter can also be performed with the help of a large grasper (Fig. 10.9). At first sight, this technique could seem rather imprecise and less elegant, but in our hands it is considered very efficient and reproducible. Synovial tissue is easily caught without any resistance between the teeth of the instruments, while ligamentous and capsular tissues are much tougher. The scalpel has to be carefully manipulated in the presence of the cruciate ligaments and collateral ligaments but allows easy identification of the different planes of dissection and allows one to quickly proceed with a “en bloc” resection. The synovectomy underneath and above the meniscus can be performed using the same approach and the same instruments but care has to be taken not to damage the cartilage. The intercondylar notch is easily accessible using this approach. A specific patellar retractor can reflect the patellar tendon and the extensor mechanism laterally (Fig. 10.10). The same instruments can be used to perform a synovectomy of the Hoffa fat pad and the cruciate region (arthroscopic grasper).
Fig. 10.9 
Synovectomy of the medial gutter performed with a large grasper
Fig. 10.10 
Medial parapatellar arthrotomy and intercondylar notch view
-
(b)
The posteromedial approach
-
Direct
The skin incision is vertical with the knee in 90° of flexion and centered on the posterior border of the medial condyle (Fig. 10.11). The anteromedial arthrotomy can be used to palpate the posterior border of the medial collateral ligament and thus the exact location of the posteromedial skin incision can be determined. The skin incision extends from the superior and posterior borders of the medial condyle to the tibial insertion of the semimembranosus approximately 8–10 mm distally to the joint line. The anatomic advantages of this skin incision are disputable. Moreover, lesions of the saphenous nerve and its branches are frequently noted.
Fig. 10.11 
Posteromedial approach and anatomy
-
Approach with subcutaneous undermining (preferred technique)
This approach requires an extended skin incision 3 cm proximal to the superior edge of the patella to 2 cm distal to the regular medial approach. This skin and the subcutaneous fat are elevated using a Farabeuf retractor. The knee is now placed in a 90° flexed position in the figure-of-four position. The posterior border of the medial collateral ligament serves as a landmark as does the posterior edge of the tibial plateau and the medial femoral condyle. The vertical arthrotomy is performed just posteriorly to the medial collateral ligament and stops just superior to the medial meniscus. One has to take care not to cut the posterior corner of the medial meniscus. For an extended exposure, it is sometimes necessary to release the posterior capsule for a couple of millimeters from the femoral condyle. By doing this, it is possible to obtain a good view in the posteromedial compartment. At the end of the procedure, the released capsule can be reattached using an anchor or suture. The synovectomy in the posteromedial compartment and posterior to the posterior cruciate ligament is performed with the use of a large grasper. The knee is always kept in a flexed position and in varus in order to maximally relax the posterior capsule (Fig. 10.12).
Fig. 10.12 
The synovectomy in the posteromedial compartment and posterior to the posterior cruciate ligament is performed with the use of a large grasper
-
-
(c)
Anterolateral approach
With the knee in a 90° flexed position, a second anterolateral skin incision is performed starting from the mid part of the patella and extending 10 cm proximally in the direction of the upper border of the iliotibial band (ITB) (Fig. 10.13). In order to avoid skin necrosis, the anterolateral and anteromedial skin incision should be at least 4 finger widths apart. It is also advisable to place the anterolateral (superolateral) skin incision proximally and the anteromedial (inferomedial) skin incision more distally to avoid skin necrosis. If a posterolateral arthrotomy is planned and the skin is to be undermined, the anterolateral skin incision should be made somewhat more laterally, i.e., on the middle part of the ITB. An extended lateral approach necessitates longer skin incisions notably at the height of Gerdy’s tubercle distally that could compromise the cutaneous vascularization in the prepatellar and infrapatellar region. The lateral parapatellar arthrotomy starts distally at the inferior pole of the patella and goes up 3 cm in a vertical direction always staying lateral to the midline. The lateral condyle, the superior border of the lateral meniscus, and the lateral portion of the infrapatellar fat pad can thus be visualized.
Fig. 10.13 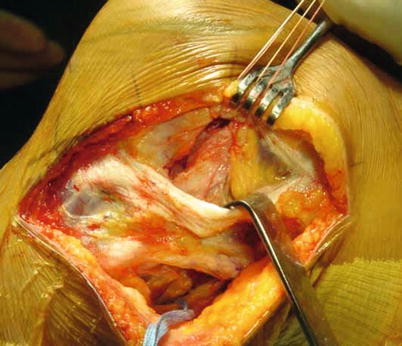
Anterolateral approach and ITB exposure
With the knee in full extension, an incision in the quadriceps tendon allows for visualization of the suprapatellar pouch. The complete extensor mechanism can now be lifted with a “Farabeuf” retractor (Fig. 10.14) or a specific patellar retractor. A synovectomy can now be performed in the same way as with a medial parapatellar arthrotomy. In order to have access below the meniscus, the skin incision has to be extended distally (always keeping attention to the minimum required distance between both skin incisions) and then a small horizontal arthrotomy is performed underneath the meniscus. This synovectomy on the undersurface of the meniscal body and on its posterior part is more difficult with this open approach than with an arthroscopy.
Fig. 10.14 
Suprapatellar pouch exposure through a lateral parapatellar approach
-
(d)
Posterolateral approach
-
Direct
In combination with an anterolateral approach, a direct vertical arthrotomy just posterior to the lateral collateral ligament and superior to the lateral meniscus can be performed. The exact location of the lateral collateral ligament can be found with the knee in the “figure-of-four” position. The skin incision is now performed with the knee in 90° of flexion and neutral rotation. Additional transillumination with the arthroscope can provide some additional help. A skin incision is made from the posterosuperior border of the lateral condyle vertically down to tibial plateau always staying just posterior to the lateral collateral ligament (Figs. 10.15).
Fig. 10.15 
Posterolateral approach and anatomy
-
Approach with subcutaneous undermining (preferred technique)
With the ITB as landmark, the posterolateral compartment can be accessed above, through, or under the ITB.
Access to the posterolateral capsule
The posterolateral knee capsule can be accessed through the ITB (incising it in the direction of the fibers) or just anterior to it. The lateral collateral ligament and the anterior border of the lateral head of the gastrocnemius muscle can be palpated with the Metzenbaum scissors (Fig. 10.16). The knee should always be flexed. Thus, a vertical arthrotomy can be performed just posterior to the lateral collateral ligament (Fig. 10.17). A small artery is frequently present and care should be taken to achieve hemostasis. Attention should be paid not to cut the posterior corner of the lateral meniscus or the popliteus tendon. The latter blocks access to the tibial plateau, especially to its posterior part and to the posterior recess. The posterior border of the lateral tibial plateau and femoral condyle can now be palpated. The synovectomy of the posterolateral supra-meniscal recess and the posterior cruciate ligament can be performed using a large grasper (Fig. 10.18). As for the medial side, the approach can be extended by dissecting the posterior capsule from the femoral condyle; this provides access to the posterior part of the lateral tibial plateau. The exposure of this zone is very difficult through the previously described approach. It can be necessary to go posterior to the distal ITB. This allows visualization of the popliteal hiatus and the posterior border of the lateral tibial plateau. If increased exposure is required, incision of the lateral meniscus in the red-red zone is necessary.
Fig. 10.16 
Dissection of the lateral collateral ligament
Fig. 10.17 
Vertical arthrotomy posteriorly to the lateral collateral ligament
Fig. 10.18 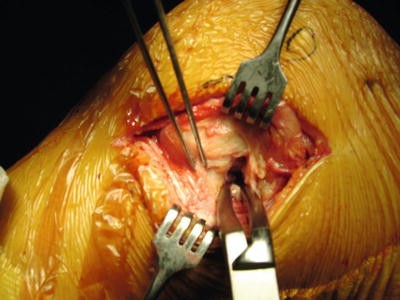
Posterolateral synovectomy using a large grasper
-
-
(e)
Posterior approach
This approach is needed in diffuse PVNS with lesions posterior to the PCL or extra-articular lesions in the popliteal fossa. In some rare cases, one can encounter localized PVNS or a benign tumor located posterior to the PCL that must also be addressed via this approach. The first surgical step is always the anterior synovectomy, either arthroscopically or using arthrotomies. After skin closure, the patient is placed in the prone position. The surgical field is left in place. The surgical team turns the lower limbs of the patient, while the anesthesia team turns the thorax and head of the patient. Rotation of the patient is performed clockwise for a right knee and counterclockwise for a left knee when viewed from the patient’s feet.
A new stocking and extremity sheet are applied, and the flexion crease of the knee is marked by placing a skin marker in the flexion crease and flexing the knee. The marker is then slowly retracted while exactly marking the flexion crease. A sterile opsite is then applied.
The posterior approach is performed according to Trickey. A lateral vertical skin incision of approximately 5 cm is performed just medially to the biceps tendon. It is continued horizontally in the flexion crease from lateral to medial to the insertion of the medial gastrocnemius muscle. The incision is then extended distally in a vertical direction, for about 7 cm. An angled skin incision is to be avoided. The skin incision is performed with a knee in extension (Fig. 10.19). With the support under the foot and the knee in slight flexion, the subsequent surgical steps are performed. First, one identifies the small saphenous vein, which is never easy. The head of the medial gastrocnemius muscle is retracted medially and its fascia is incised vertically. This exposes the hamstring tendons superficially and the deeper semimembranosus tendon. These tendons guide the surgeon to the posterior area of the tibia and thus to the “safe zone” avoiding potential damage to the neurovascular structures in cases where the posterior border of the posterior cruciate ligament needs to be exposed. The posterior tibia is covered with the popliteus muscle. The neurovascular elements can be retracted carefully by placing a Homan retractor in contact with the tibia. Finally a capsulotomy is performed. The arthrotomy is vertical and extending towards the posteromedial border of the lateral condyle. In specific cases, it can be necessary to perform a partial section of the head of the medial gastrocnemius muscle in its tendinous part for approximately 15 mm. This allows an improved view of the posterior capsule. The posterior synovectomy in the zone behind the posterior cruciate ligament can now be performed using the large grasper.
Fig. 10.19 
Posterior midline skin incision (prone position)
Some extensive lesions in the popliteal fossa are situated more superficially. The popliteal neurovascular structures should be identified and carefully retracted using a Farabeuf retractor (Fig. 10.20). The posterior extra-articular lesions are carefully dissected (Fig. 10.21). When in close contact with the vascular structures, the assistance of a vascular surgeon is sometimes advisable, especially in revision operations with adhesions that require exploration both medial and lateral to the neurovascular structures.
Fig. 10.20 
Dissection of tibial nerve and popliteal blood vessels
Fig. 10.21 
Resection of a large posterior lesion (posterior approach, prone position)













Combined Synovectomies
The indication for this surgery is typically a revision operation for diffuse PVNS with limited lesions in the anterior compartment but extensive posterior lesions or lesions not accessible by arthroscopy. The first surgical step is an arthroscopy of the anterior compartment as described previously. It allows for arthroscopic evaluation and multiple biopsies. After closure of the arthroscopic skin portals, the patient is turned in a prone position as described previously and a Trickey approach to the posterior compartment is performed.
Total Knee Arthroplasty
Placement of a total knee arthroplasty offers the opportunity to perform an extensive synovectomy.
This surgical intervention is performed using a single classic approach to the knee. The bony cuts allow a more extended exposure to the different compartments. Only in cases of extensive extra-articular lesions, an additional approach may be necessary. A primary total knee arthroplasty can be justified in the elderly with articular destruction but is less frequently performed in PVNS of the knee compared to that of the hip. Nevertheless, the exposure during the TKA does not allow removal of extra-articular pathology.
Postoperative Care
Because of the risk of extensive intra-articular bleeding after a synovectomy and hence increased risk of skin necrosis, anticoagulants are avoided in our department. To prevent DVT, weight bearing, mobilization of the ankle and foot, and early ROM exercises are encouraged. Postoperative stiffness is a well-known complication in this type of surgery. In order to limit the risk after a total synovectomy, the position of the knee is frequently changed from extension to flexion using a specifically designed flexion brace. The knee is held in this flexed position during 1 or 2 h every 6 h.
Continuous passive motion is allowed from the first postoperative day on. Time should always be taken to look for any signs of skin problems.
Specific Cases
Pigmented Villonodular Synovitis
The aim in the treatment of this type of pathology should be a single procedure involving a total synovectomy with multiple biopsies (Fig. 10.22). Limited PVNS does not need specific postoperative surveillance. In diffuse PVNS, we prefer a total synovectomy with an arthrotomy. In case of surgical failure, a chemical synovectomy can be performed 4–6 weeks after the surgical intervention. Recurrence should be looked for during follow-up (clinical examination and MR imaging every year during the first 3 years following surgery and following this if there is any clinical suspicion of recurrence). One must remember that findings at pathology (clean margins) do not predict recurrence. Recurrence rates decreased with the passage of time, but the surgeon must carefully follow these patients for many years.

Pigmented villonodular synovitis (resected lesions)
Primary (Osteo) Chondromatosis
Arthroscopic treatment of this pathology is in most cases effective. In contrast with our aggressive treatment for PVNS, we believe that the symptomatic, limited treatment of primary osteochondromatosis is appropriate. Of course, one should take into account the extent of the pathology in every patient. The typical grains of rice can be attached to the synovial tissue (early stage of primary osteochondromatosis) necessitating a debridement of the synovial tissue using the shaver. In a later stage, joint lavage and a limited synovectomy in those regions of synovial hypertrophy can suffice. This type of surgery can be repeated if needed, and in many cases the extent of the patient’s symptoms diminishes over time. Malignant transformation is rarely described in the literature. It is very important to identify and debride the regions underneath the lateral and medial meniscus. In order to remove the grains of rice that are located in the popliteal hiatus, manual pressure in the posterolateral region of the knee and the popliteal fossa is applied while repeatedly flexing and extending the knee. This forces the grains of rice into the knee joint from which they can be removed easily.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
Archbold, P., Pinaroli, A. (2014). Synovectomies of the Knee. In: Neyret, P., Demey, G. (eds) Surgery of the Knee. Springer, London. https://doi.org/10.1007/978-1-4471-5631-4_10
Download citation
DOI: https://doi.org/10.1007/978-1-4471-5631-4_10
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-5630-7
Online ISBN: 978-1-4471-5631-4
eBook Packages: MedicineMedicine (R0)