
Abstract
Knee arthroscopy has evolved greatly from its inception in the twentieth century. Arthroscopic synovectomy is performed in the case of infection or significant synovitis. We continue to develop more minimally invasive procedures and the Nanoscope (Arthrex, Naples, FL) has provided a new generation of possibilities. The system does not require the use of a standard incision or portal and with the use of the Graftnet (Arthrex, Naples, FL) we can harvest tissue with a standard shaver for further evaluation. This technique provides an option to perform a synovectomy and biopsy without the use of a standard arthroscopy portals through an incisionless approach.
With permission from Arthroscopy Techniques: Lavender C, Patel T, Adil Syed, Blickenstaff B, Oliashirazi A. Incisionless Knee Synovectomy and Biopsy With Needle Arthroscope and Autologous Tissue Collector. Arthroscopy Techniques, Vol 9, No 9 (September), 2020; pp. e1259–1262.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Synovectomy of the knee is a procedure that has multiple indications of which the most common are septic arthritis, inflammatory arthritis, and synovial tumors. The procedure is done through either an open or an arthroscopic approach; however, an incisionless method using a Nanoscope (Arthrex, Naples, FL) can also be utilized. With the incisionless method, a Graftnet (Arthrex, Naples, FL) allows tissue from the synovium to be collected and evaluated which can aid in diagnosis and treatment. Septic arthritis of the knee is a surgical emergency and is one of the more common reasons to perform a synovectomy. Once septic arthritis is diagnosed, urgent surgical debridement along with antibiotic treatment is critical. Surgical decompression reduces the intra-articular burden of bacteria and removes harmful debris released from the host inflammatory response. Panjawani et al. conducted a systematic review and meta-analysis to compare reoperation rates, length of stay, and functional outcome between arthroscopy and open arthrotomy of septic native knees [1]. They found seven studies of which 723 patients underwent arthroscopic I&D and 366 patients underwent open I&D. The relative risk of reoperation and LOS of stay was lower in the arthroscopy group, and one study reported better functional outcomes with arthroscopy. The authors concluded arthroscopic debridement results in lower risk of re-operation than open arthrotomy. Furthermore, in a retrospective study of one institution, Johns et al. compared open to arthroscopic I&D of native knees [2]. They included 166 knees of which 123 knees were treated with arthroscopic I&D while 43 knees were treated with open I&D. They found 71% of open I&D and 50% of arthroscopic I&D required repeat irrigation. In addition, the arthroscopic groups had a lower total number of irrigation procedures, better mean post op ROM (p < 0.05). In regards to PVNS, arthroscopy has also been found to have similar recurrence and complication rates to open approaches [3, 4]. The following technique describes an incisionless approach for synovectomy and biopsy of the knee that can be used for the diagnosis and/or treatment of septic arthritis, inflammatory arthritis, and synovial tumors.
Indications
Patients with suspected septic knee, synovial tumors, or disease processes in which you would like a biopsy and synovectomy. Compromised patients at high risk and those in the intensive care setting.
Contraindications
Patients which require larger resections and those which have failed previous synovectomys.
Surgical Technique
Patient Setup
The patient is placed in the supine position with the operative extremity in a leg holder and a tourniquet applied to the operative thigh. The non-operative extremity is placed over a well-padded pillow in slight flexion. The operative extremity is exsanguinated, and the tourniquet is inflated.
Nanoscope Insertion
A spinal needle is inserted into anterolateral joint space while the knee is in full extension. The knee may need slight flexion to allow entry into the patellofemoral joint. A nitinol wire is inserted into the needle and the needle is removed. A small 2.7 mm cannula is then inserted over the wire and the wire is removed (Fig. 16.1). Care should be taken when inserting the 2.7 cannula as it can cause cartilage damage during insertion (Fig. 16.2). Inflow is then placed onto the cannula and the Nanoscope (Arthrex, Naples, FL) is inserted for visualization of the joint. A standard diagnostic arthroscopy is then performed in the patellofemoral joint. The Nanoscope is then redirected into the medial joint space. Rather than gliding into the medial joint as is done with standard arthroscopy, it can be helpful to come out slightly and redirect into the space.

View of a left knee from outside the knee. The spinal needle is seen inserted into the patellofemoral joint while the knee is in full extension

View of a left knee in the extended position from outside the knee. The cannula has been inserted into the knee with the Nanoscope inserted
Medial Portal
An 18-gauge spinal needle is then used to localize the medial portal location in an outside fashion. A nitinol wire is inserted into the needle and the needle is removed (Fig. 16.3). A small 2.7 mm cannula is then inserted over the wire and the wire is removed.

View of a left knee from outside the knee with the knee in full extension. The medial portal has been established with a nitinol wire inserted into a spinal needle while the Nanoscope is in the anterolateral portal and the knee is in full extension
Synovectomy
The Nanoscope is then redirected into the patellofemoral joint and a NanoShaver (Arthrex, Naples, FL) is used to perform the synovectomy through the medial portal. Alternatively, a 3 mm shaver can be used for a more aggressive option (Fig. 16.4). The Graftnet is then applied to the shaver to collect tissue for analysis (Figs. 16.5 and 16.6). The shaver is then brought to the medial compartment to then be used to debride the medial compartment. Next, the Nanoscope is switched to the medial compartment and the shaver can be brought in laterally to complete the synovectomy anteriorly, laterally, and in the patellofemoral joint. Finally, tissue obtained from the Graftnet is then placed into a sterile cup and sent to pathology for evaluation (Figs. 16.7 and 16.8).

View of a left knee in the extended position with the 0 degrees Nanoscope from the anterolateral portal. The shaver has been placed in the medial portal with the knee in full extension. The shaver is harvesting synovial tissue

View of a left knee in 90 degrees of flexion. The Graftnet has been attached to the shaver while the shaver is in the anterolateral portal

The synovial tissue has been removed from the Graftnet and is being placed into a sterile cup and submitted for pathologic evaluation

View of a left knee in full extension. The portal sites are seen on the front of the knee

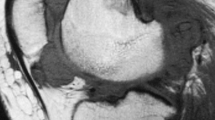
Final pathologic findings showing the synovium and the maintained cellular architecture after biopsy using the Graftnet. Hematoxylin and eosin stain with original magnification ×200
Discussion
Synovectomy can be done through an open incision or arthroscopically, and here we describe an incisionless arthroscopic technique using the Nanoscope. The Nanoscope needle arthroscopy system is both diagnostic and therapeutic. It allows direct visualization of intra-articular pathology and its use in combination with the Graftnet allows for recovery of tissue for histologic analysis. In addition, it eliminates the need for incisions, requiring only a spinal needle to establish access to the joint. The most common indications for synovectomy include septic arthritis, inflammatory arthritis, and synovial tumors. Traditional arthroscopy of knees offers several advantages including magnified view, better access to harder to reach areas of the knee and more visibility of gutters, as well as the high flow of normal saline in a closed cavity allowing for dislodgement of any necrotic material or pus [5]. There are limitations to the nanoscopic technique similar to those previously described for other nanoscopic techniques which include technical difficulty using the 0-degree lens, difficult visualization due to flow, and the need for the more precise location of portal sites [6]. Pearls of this technique include redirecting the Nanoscope when entering into different compartments, and using a 3 mm shaver for improved suction and debridement [7]. Risks of this technique include articular cartilage damage from the sharper trochar and missing joint pathology because of the decreased visualization due to flow and smaller size of the arthroscope. Finally, minimally invasive surgery results in reduced pain, swelling, complications, and a quicker recovery – therefore this technique should improve patient results and should especially be considered when the diagnosis is questioned or in critically ill patients where an incisionless approach is favored.
Editors View
This chapter describes another one of our incisionless techniques. This technique in particular is useful especially in a sick or compromised patient with a possible or probable knee infection to treat the infection in as minimally invasive fashion as possible. Also, it is very useful for diagnostic purposes that can easily be used in a setting of tumor pathology or other undiagnosed problems within the knee. I personally use the Nanoscope in many diagnostic cases at this point and feel that it is a very useful tool when combined with the Graftnet incisionless approach to correctly diagnose intra-articular pathologies of the knee. It is very exciting to see where we are with nano arthroscopy and combining that with some of the minimally invasive tools that we have to produce techniques such as this and improve patient outcomes.
References
Panjwani T, Wong KL, Tan SHS, Liau G, Vaidya N, Krishna L. Arthroscopic debridement has lower re-operation rates than arthrotomy in the treatment of acute septic arthritis of the knee: a meta-analysis. Journal of ISAKOS: Joint Disorders & Orthopaedic Sports Medicine 2019;(4):307–12.
Johns BP, Loewenthal MR, Dewar DC. Open compared with arthroscopic treatment of acute septic arthritis of the native knee. J Bone Joint Surg Am. 2017;99(6):499–505. https://doi.org/10.2106/JBJS.16.00110.
Rodriguez-Merchan EC. Review Article: Open versus arthroscopic synovectomy for pigmented villonodular synovitis of the knee. J Orthop Surg. 2014;22(3):406–8.
Pan X, Zhang X, Liu Z, Wen H, Mao X. Treatment for chronic synovitis of knee: arthroscopic or open synovectomy. Rheumatol Int. 2012;32:1733–6. https://doi.org/10.1007/s00296-011-1901-3.
Lui TH. Complete arthroscopic synovectomy in management of recalcitrant septic arthritis of the knee joint. Arthrosc Tech. 2017;6(2):e467–e475 137.
Lavender C, et al. Nanoscopic single-incision anterior labrum repair. Arthrosc Tech. 2020;9:e297.
Lavender C, Patel T, Syed A, Blickenstaff B, Oliashirazi A. Incisionless knee synovectomy and biopsy with needle arthroscope and autologous tissue collector. Arthrosc Tech. 2020;9(9):e1259–62.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Patel, T.K., Jasko, J. (2021). Incisionless Synovectomy of the Knee. In: Lavender, C. (eds) Biologic and Nanoarthroscopic Approaches in Sports Medicine. Springer, Cham. https://doi.org/10.1007/978-3-030-71323-2_16
Download citation
DOI: https://doi.org/10.1007/978-3-030-71323-2_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-71322-5
Online ISBN: 978-3-030-71323-2
eBook Packages: MedicineMedicine (R0)