
Abstract
In the United States, lumbar spinal stenosis (LSS) is the most common indication for lumbar spine surgery in those over 65 years of age [1]. The prevalence of LSS in the population is estimated at 8–11 % and disproportionately affects the elderly [2]. The rapidly expanding elderly population brought on by maturation of “baby boomers” (59 % increase expected from 2010 to 2025 to 64 million people) confluences with extended life expectancy to bring about cubic growth curve in the incidence of LSS when factoring in the increases in both the population rate (per 100,000 people) and absolute number of those afflicted [2, 3]. This results in a growing need to manage this disease with efficient, appropriate, and cost-effective treatment.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Intervertebral Disc
- Spinous Process
- Lumbar Spinal Stenosis
- Degenerative Spondylolisthesis
- Transforaminal Lumbar Interbody Fusion
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
In the United States, lumbar spinal stenosis (LSS) is the most common indication for lumbar spine surgery in those over 65 years of age [1]. The prevalence of LSS in the population is estimated at 8–11 % and disproportionately affects the elderly [2]. The rapidly expanding elderly population brought on by maturation of “baby boomers” (59 % increase expected from 2010 to 2025 to 64 million people) confluences with extended life expectancy to bring about cubic growth curve in the incidence of LSS when factoring in the increases in both the population rate (per 100,000 people) and absolute number of those afflicted [2, 3]. This results in a growing need to manage this disease with efficient, appropriate, and cost-effective treatment.
Medical management of LSS can, as can most spine-related diagnoses, be performed with a continuum of methodologies and interventions ranging from physical therapy to complex spinal fusion. Unfortunately, inconsistency within the literature detailing the best course of treatment for LSS complicates evidence-based practice. Nonoperative care in those with severe symptoms has been largely shown to be an ineffective permanent solution [4–8], while simple decompressions provide early (1 year) relief that is not always maintained in longer follow-up [9–11]. Arthrodesis in the treatment of LSS, while being a definitive and largely successful procedure with maintenance of outcome [4, 6, 7], is considered by some to be controversial in patients without concomitant instability or disc pathology. Additionally, and possibly more importantly, advanced age and the resultantly more frequent presence of medical comorbidities have led some surgeons to avoid surgical intervention [12], at least when using conventional open-exposure surgical approaches and procedures.
Modern, minimally disruptive surgical approaches have more recently been introduced into the surgical armamentarium that enable treatment in patients previously contraindicated or considered higher risk for surgery (i.e., those with advanced age or significant medical comorbidity), with significantly lower morbidity [13–15]. Interlaminar lumbar instrumented fusion (ILIF®, NuVasive, Inc., San Diego, CA), and a modification of the procedure to incorporate a specialized transforaminal lumbar interbody fusion (TLIF), is one such procedure that has been developed to treat the continuum of the disease LSS and which will be the subject of the following chapter.
Background/Etiology
Lumbar spinal stenosis is a condition of later life, typically presenting in the fifth or sixth decades. [16]. It can be a complex disease process and is often one part of a multifactorial degenerative cascade, though congenital factors (such as vertebral malformations) may also contribute to LSS [3, 9]. LSS is defined as a narrowing of the central spinal canal or neuroforamen [3, 6, 9]. LSS is most often the result of soft tissue or bony degeneration encroaching upon the neural elements. Intervertebral disc bulging herniation, facet arthropathy, ligamentum flavum hypertrophy or buckling, degenerative spondylolisthesis, and degenerative scoliosis is regularly associated with this condition [3, 9, 17]. As previously mentioned, prevalence of symptomatic stenosis in the general population is estimated to be between 8 % and 11 %, though as many as 20 % of the population may exhibit a radiographic diagnosis of stenosis asymptomatically [2, 12]. The most common level for LSS is L4–5, followed by L3–4, L2–3, and then L5–S1 [16, 18, 19].
Three main classifications of LSS exist: central stenosis, lateral or lateral recess stenosis, and neuroforaminal stenosis [9]. Central stenosis represents a decrease in the cross-sectional area of the spinal canal and is often associated with ligamentum flavum thickening, intervertebral disc bulging, or with bony abnormalities affecting the canal area (e.g., osteophytes, congenitally short pedicles). Congenital stenosis, however, is a relatively rare diagnosis, seen in only approximately 9 % of LSS patient population [16]. Lateral stenosis commonly accompanies central narrowing and is notably different from neuroforaminal stenosis, though both lateral and neuroforaminal stenosis affect existing nerve roots/spinal nerves rather than the cauda equina. Exiting lumbar nerve roots immediately travel through the lateral recess, a relatively small bony passageway bordered by the pedicle laterally, the superior articular facet posteriorly, and anteriorly by the posterior aspect of the vertebral body. Lateral recess stenosis is more common than neuroforaminal stenosis as this passageway is substantially smaller than the neuroforamen and is more sensitive to encroachment by intervertebral disc bulging and facet arthropathy. Foraminal stenosis is most commonly seen with degenerative spondylisthesis or an intervertebral disc herniations and is rarely seen outside of these diagnosis.
There are multiple mechanisms by which LSS can cause neural impairment and a variety of clinical presentations. LSS symptoms are most commonly caused by direct mechanical compression of the nerve roots or spinal nerves [16]. However, venous congestion and reduced arterial flow, resulting in increased epidural pressure, are commonly associated with multilevel LSS and is directly related to neurogenic claudication [6, 17]. Additionally, local inflammatory processes in LSS can result in nerve root or spinal nerve Irritation.
Presentation/Investigation/Treatment Options
Presentation/Evaluation
As LSS is often one part of a multifaceted disease complex, a single definitive differential diagnosis does not exist. Instead, a detailed patient history, physical examination, and variety of imaging studies are needed to determine the presence, location, and severity of LSS as well as any accompanying pathology such as degenerative spondylolisthesis or scoliosis [2, 3, 12]. Clinically, LSS often presents as low back pain and/or leg pain with or without neurogenic claudication [16]. Severe cases of LSS may exhibit myelopathic symptoms or cauda equina syndrome, including lower extremity motor deficits, sensory loss, and/or loss of bowel or bladder function [6, 9, 16]. In such extreme cases, immediate surgical intervention is normally indicated.
Physical evaluation should include a detailed review of both neurological and mechanical symptoms [16]. Patients with primarily neurological symptoms will generally exhibit characteristics of neurogenic claudication and radiculopathies. Mechanical symptoms, conversely, will present mainly as back pain.
Neurogenic claudication has been described as a “constellation of symptoms,” of which central stenosis may be only one contributing factor [17]. Neurogenic claudication secondary to stenosis more commonly affects women than men and generally presents as discomfort in the lower extremities, often brought on by walking or activity [17]. Symptoms of vascular claudication and neurogenic claudication are similar. Any evaluation of neurogenic claudication should begin with a detailed patient history to rule out peripheral vascular disease. Evaluation of symptoms should show a proximal to distal progression on onset during neurogenic claudication with distal to proximal progression in vascular claudication. A useful test to differentiate neurogenic claudication from peripheral vascular disease includes evaluating symptoms following a walk downhill as well as a bicycle ride. In neurogenic claudication, symptoms will often be exacerbated on the downhill walk and non-apparent in cycling [17]. Peripheral vascular disease symptoms are often exacerbated by cycling, while symptoms are attenuated on a treadmill [16].
Walking and stoop tests are common examination techniques for neurogenic claudication. A walking test includes a self-paced walk with recording of the distance walked prior to onset of symptoms, typically weakness, tiredness, or a heaviness of the lower extremities [20]. The threshold for walking is approximately twice the distance from when the patient first experiences discomfort [17]. A stoop test includes evaluation of symptom resolution following hitting the stop point on the walking test and instructing the patient to lean on a wall or stoop to tie a shoelace (flexion). In patients with neurogenic claudication, symptom resolution generally follows with this test or with lying supine or when sitting.
All history and physical evaluations for LSS should be accompanied by several modalities of imaging. Standing static and dynamic radiography should be obtained on all patients to evaluate any bony or gross abnormalities. Static films can be used to determine the presence of spondylolisthesis, deformity, or osteophytes, while dynamic films can be used to determine the presence of instability. Instability has been defined by Posner et al. [21] as horizontal translation on lateral dynamic films of at least 8 % anteriorly or 9 % posteriorly when evaluating single levels between L1–2 and L4–5 and of at least 6 and 9 % at L5–S1, respectively. Angular displacement is also defined as a measure of instability, with at least −9° displacement on flexion for levels L1–2 through L4–5 and of +1° at L5–S1 qualifying as instability.
Magnetic resonance imaging (MRI) is considered the “gold standard” imaging study for evaluating stenosis. On MRI, the intervertebral disc can be visualized to determine the extent and nature of any degenerative processes (e.g., bulging, prolapse, degeneration), and the quality of the disc can be evaluated on T2-weighted images, where healthy discs exhibit increased proton signal at the nucleus pulposus and a decreased signal in degenerative discs. Axial views are useful in determining the extent of central and lateral stenosis, while sagittal MRI reconstructions are the most useful imaging modality in evaluating neuroforaminal stenosis. A determining criterion in neuroforaminal stenosis is the absence of fat around the nerve roots in the foramen on MRI due to stenosis.
Myelography and CT myelography are also useful in determining the extent of central stenosis. In patients with stenosis, an “hourglass”-shaped dura at the level of the intervertebral disc is characteristic of central stenosis and is consistent in diagnosis of stenosis at multiple levels in a patient with neurogenic claudication symptoms. CT myelography provides additional detail, with an ability to evaluate stenosis in multiple planes as well as being able to evaluate the integrity of the nerve root sleeve.
As LSS impacts the elderly and females disproportionately, a dual-energy X-ray absorptiometry (DEXA) study can be performed to evaluate bone mineral density, especially in surgically indicated patients.
Treatment Options
Following a positive LSS diagnosis, a detailed medical treatment plan should be made with the patient. Considerations in determining a course of treatment should include the severity of symptoms and their effect on the patient, patient expectations from treatment, the ability for the patient to tolerate certain medical interventions, and the physician’s preference and ability with such interventions. Except in extreme cases or in those patients with cauda equina syndrome, medical management of LSS typically begins with a course of nonoperative care. Common nonoperative treatments for patients with LSS include orthotics, bed rest, nonsteroidal anti-inflammatory drugs (NSAIDs), narcotic medication, oral corticosteroids, physical and rehabilitation therapy, or epidural steroid injections.
NSAIDs and/or glucocorticosteroids can be used as part of a “first-line” anti-inflammatory therapy, though care must be taken with their long-term use as NSAIDs may cause cardiovascular or gastrointestinal side effects. In long-term use, liver and kidney function should be monitored by a primary care physician. In addition to nonsteroidal anti-inflammatory drugs, oral steroids (e.g., prednisolone, methylprednisolone) may also be effective. If prescribed, care should be taken in patients with diabetes as oral steroids may elevate blood glucose.
Lumbar flexion and isometric core strengthening exercises are appropriate rehabilitation exercises in addition to low-impact aerobic conditioning. In any rehabilitation or physical therapy, evaluation of patient tolerance for certain activities which may exacerbate stenotic symptoms (i.e., walking) may be replaced with aquatic therapy or recumbent bicycle riding.
Epidural steroid injection therapy is an additional means of nonsurgical intervention in the treatment of LSS, further along the invasiveness continuum of medical treatment than other forms of nonoperative care. The role and efficacy of injection therapy has been debated in the literature for some time, though more recent studies have suggested a positive dose effect exists in some patients. Manchikanti et al. [22], in a randomized, double-blind, controlled trial of 120 patients receiving lumbar facet injections with either a local anesthetic alone or local anesthetic with steroids, found that between 85 and 90 % of patients (depending on treatment group) with chronic function-limiting low back improved with the administration of analgesic injections with or without steroids.
Most patients with mild symptoms associated with LSS are adequately managed with nonoperative care, often indefinitely [1, 6, 23]. In a study of Medicare patients with a first-time diagnosis of LSS, Chen et al. [24] found that only 21 % of patients subsequently went on to have surgery within 3 years of diagnosis. However, in patients with multiple degenerative processes, instability, myelopathy, and/or other progressing or moderate to severe LSS symptoms, surgical intervention is generally warranted and shows significant clinical gains compared to nonoperative care [3–8]. In a study of 49 patients treated nonoperatively for LSS and followed for an average of 3 years after their first LSS diagnosis, Simotas et al. [8] found that 19 % of patients had undergone surgical intervention. Of those remaining who did not subsequently undergo surgical treatment in the study timeframe, 5 % experienced significant motor function deterioration, 13 % had symptom worsening, 30 % experienced no change in symptoms, and 28 % reported a mild improvement in symptoms, while only 30 % reported a sustained improvement in symptoms.
Simple Decompressions
Laminectomy is considered to be the “gold standard” treatment for lumbar spinal stenosis [11, 16]. Such pedicle-to-pedicle decompressions are useful in treating central and lateral stenosis as the canal is obviously decompressed with the removal of the laminas, but access is also gained to the subarticular and neuroforaminal space facilitating direct nerve root decompression. Laminectomy, however, has largely been replaced with alternative decompression techniques for a variety of reasons. First, the wide decompression afforded by laminectomy (in those cases with >50 % resection of the facet joints) [10, 25] results in iatrogenic destabilization of the spine. This, paired with bony regrowth and epidural fibrosis development, has been associated with progressively increasing postoperative symptoms in some patients, known as failed back/back surgery syndrome or post-laminectomy syndrome/instability [9, 26–28]. A study by Martin et al. [29] found that surgically indicated recurrent stenosis following laminectomy occurred in nearly 20 % of patients. In study by Postacchini et al. [28] in 40 patients treated with a decompression for LSS (32 patients received laminectomy, 8 laminotomy), the authors found that 88 % of patients had radiographic evidence of posterior vertebral arch regrowth, and in those with “marked regrowth,” only 40 % reported a satisfactory clinical results. This regrowth positively correlated with instability at the postoperative spinal level, due either to iatrogenic factors or to the presence of spondylolisthesis.
As a result of these challenges with laminectomy, bilateral laminotomy was increasingly adopted to provide a vehicle for similar, though slightly more limited, decompression while maintaining the central portion of the osteoligamentous arch and, thus, better preserving segmental stability. This largely remains a viable option for simple decompression in the treatment of LSS, though central stenosis has the potential to be inadequately addressed due to the maintenance of the central portion of the osteoligamentous arch.
Both laminectomy and laminotomy are primarily carried out using conventional surgical approaches and open exposures. This results in elevated associated surgical morbidity and has been described as a consideration against surgical intervention in medical decision making in elderly patients, potentially opting for less effective treatment protocols (nonoperative care) due to elevated risk of complication using conventional exposure procedures. Several examples of decompression morbidity include Deschuyffeler et al. [30] in 2012 reporting a 17.1 % complication rate in patients over 65 who underwent a unilateral laminotomy with bilateral decompression. A study by Kaymaz et al. [31] found similar results in laminectomy, with a complication rate of 19 % and incidence of failed back surgery syndrome of 8 % at between 6 and 12 months postoperatively.
Fusions
The addition of arthrodesis to decompressive procedures for LSS remains controversial, with a few exceptions. These exceptions include LSS accompanied by instability (iatrogenic or degenerative), degenerative spondylolisthesis, deformity (scoliosis or kyphosis), or cases of recurrent stenosis [10, 32]. Additionally, fusion is indicated in patients undergoing a decompression requiring removal of more than 50 % the facet, in those undergoing total laminectomy or laminotomy who are middle-aged and/or the intervertebral disc of the segment involved has normal or near-normal height (suggesting substantial anterior column mobility predisposing posterior decompressions to failed back syndrome), or in patients with segmental hypermobility, especially with back pain as the predominant symptom [9].
Despite the ongoing debate over fusion (and fusion type) for LSS alone, lumbar fusion has been found to be effective in more definitively treating LSS and has been shown to have incrementally superior outcomes than simple decompressions in some indications. Yone et al. [11] studied a series of patients treated with decompression with or without fusion for either LSS alone or LSS with instability. In the LSS with instability group, patients were treated with fusion procedures and realized an 80 % excellent or good clinical result. In those with LSS with instability who underwent a simple decompression, excellent or good outcomes were achieved in only 29 % of patients. Finally, in patients with LSS without instability who underwent simple decompression, patients fared similarly to fusion patients through 1 year postoperative, though their outcome precipitously deteriorated thereafter, settling on a 47 % excellent or good outcome rate at last follow-up. Many other high-quality studies have similarly found an incremental improvement in performing fusions for more advanced presentations of LSS (e.g., instability, spondylolisthesis, scoliosis) [4, 5, 7, 23]. In an analysis of fusion outcome by diagnosis, Glassman et al. [33] found that degenerative spondylolisthesis and scoliosis with concomitant LSS were two of the most responsive diagnoses to treatment with spinal fusion in terms of improvement in pain, disability, quality of life, and number of patients who met minimally clinically important difference.
Differences between uninstrumented and instrumented fusion mostly are related to patient and pathologic characteristics as well as surgeon preference. In patients with a likelihood for pseudoarthrosis (i.e., smoker, metabolic disease) or in spinal segments with normal anterior or hypermobile anterior segments or inherent instability (spondylolisthesis), instrumented fusions have been found to be superior to non-instrumented fusion [34–36]. In a comparative study of instrumented and non-instrumented fusion in the treatment of LSS with instability, Fischgrund et al. [34] found that 83 % of patients who underwent instrumented posterolateral fusion (PLF) went on to fuse, in contrast to fusion in only 45 % of those with uninstrumented fusions. Also, clinical outcomes were categorized as excellent or good in 86 % of those who were fused, while the same outcome was only achieved in 56 % of those who were not fused.
A Level I evidence literature review evaluating outcomes of LSS treatment with spinal fusion compared to nonoperative care found in all studies that operative care significantly improved pain, disability, and quality of life compared to nonoperative care. When taking into consideration the expanding elderly population and their extended life expectancy in connection to the relatively high incidence of subsequent reoperation in decompression, fusions may increasingly become more commonplace in order to treat LSS more definitively in an attempt to avoid reoperation when medical comorbidities are likely to be increased [3, 6].
One drawback to fusion is that conventional surgical approaches for fusion have been associated with higher complications rates when compared to those of simple decompressions [2, 33]. For example, single-level TLIF has been associated with complication rates as high as 46 % and early reoperation rates (many for infections) as high as 10 % [37]. The development of modern minimally disruptive approaches for fusion has led to the expanded availability of surgery to patients who were previously considered to be high-risk patients, namely, the elderly [15]. This host of newly developed approaches and instrumentation allow for more effective and expeditious treatment, minimizing the rate of complication and hastening postoperative recovery.
While several interspinous spacers are currently available for use in the USA, those which do not incorporate posterior fusion as part of their procedure have been challenged in adoption by elevated rates of complication, restenosis, and revision [38]. In a series of 13 patients treated with an interspinous, non-fusion device at the University of Utah, immediate postoperative clinical improvement deteriorated over the course of a 43-month follow-up, ultimately resulting in 77 % of patients experiencing return of preoperative symptoms, with a final “failure rate” of patients requiring reoperation of 85 %. A perioperative complication rate of 38 % was also realized.
Interspinous spacers paired with grafting and rigid fixation, making up a posterolateral fusion construct, have a long history in spinal surgery, and early results of newly designed procedures (ILIF) show promise in being able to provide adequate decompression with sufficient long-term segmental stability through a less invasive midline exposure in patients with LSS. In the early 1900s, Russell Hibbs and Fred Albee developed and published, independently of each other, procedures for fusion of the posterior lumbar spinal elements [39, 40]. These procedures were originally used primarily to treat Pott’s disease and required autogenous bone graft harvested from the spinous processes or tibia and then laid along the interlaminar space to stop motion between the segments by fusing together posterior elements of the vertebrae. Following treatment, even using these rudimentary techniques (by today’s standards), early positive clinical outcomes were reported. In most cases, disease progression was stopped following fusion and improvements in pain were realized. Further development of the procedure was outlined in a report by Howorth [41], in which he highlighted the advances made in spinal fusion procedures. These advancements include a more focused approach of harvesting autogenous graft material from other parts of the body (e.g., tibia) and stressing orientation of the graft material for solid fusion. More recently, focus has been to preserve as much of the posterior segment as possible while still decompressing the spinal canal in order to relieve pain [25].
ILIF uses some of the early principles of Hibbs’ fusion, though with a medialized and less invasive surgical exposure, implementation of decompression laminoplasty [25] to adequately decompress the segment while not compromising endogenous stability, and has an option to perform a specialized interlaminar grafting and interspinous plating to perform and maintain the posterior decompression with posterolateral fusion.
Interlaminar lumbar instrumented fusion is indicated for a variety of thoracolumbar pathologies. Primarily, ILIF is indicated for stenosis with or without mild to moderate instability. It is also indicated for the treatment of degenerative disc disease, trauma, spondylolisthesis, and tumors. Potential limitations to use of the ILIF procedure include patients with inadequate bone stock or quality.
Surgical Technique and Rehabilitation
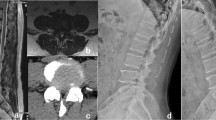
Standard preoperative planning should be conducted prior to surgery. Relevant imaging studies to review can include static and/or dynamic radiography, computed tomography (CT) scans, and magnetic resonance imaging (MRI), as available (Fig. 7.1). Confirmation of level being treated and presence of any anatomical variations should be noted and marked.

(a–c) Magnetic resonance imaging (MRI) showing lumbar spinal stenosis primarily at the L4–5 disc space on axial view and sagittal reconstruction
The ILIF procedure is performed under general endotracheal anesthesia, most commonly with the patient in the prone position with flexed hips. A Wilson frame or equivalent table will facilitate patient positioning (Figs. 7.2 and 7.3). Prior to incision, the surgical level is identified using guided fluoroscopy. Skin marking, preparation, and draping are performed using standard procedures. The spinous process and laminae of both adjacent vertebrae are exposed using a standard midline exposure, approximately 3–5 cm in length (Fig. 7.4). Self-retaining retractors are used to retract soft tissue and a Cobb elevator is used to elevate the paraspinal muscles and remove soft tissue on either side of the spinous processes. A scalpel or Leksell is used to remove the supraspinous ligament (Fig. 7.5). Distraction pins are placed into the spinous processes and a rack distractor is used to distract the spinous processes at the operative level. Bovie cautery is used to remove the interspinous ligament and expose the bony edges of the lamina. To open access to the spinal canal in preparation of the decompression procedure, a high-speed burr or Kerrison rongeur is used to remove portions of the inferior edge of the superior spinous process and lamina as well as the superior edge of the caudad spinous process that may limit access to the canal. To perform the decompression the ligamentum flavum is removed and the lamina may be thinned out or partially removed using the burr, with care to adequately decompress the space without compromising the integrity of the posterior bony arch. If necessary, rongeurs can be used to remove soft tissue from the medial aspect of the facet joints, taking only as much as it needed to adequately access and decompress the lateral space. This usually translates to between 10 and 20 %, though no more than 50 % of the facets should be taken in patients without plan for arthrodesis [25]. Partial facetectomy and proximal foraminotomies may be performed as needed. Throughout this section of the procedure, the rack distractor can be used to visualize all neural elements through targeted and, often temporary, changes in distraction amount.

Lateral view of a patient in the prone position in a Wilson frame, one possible patient positioning for the interlaminar lumbar instrumented fusion (ILIF®, NuVasive, Inc., San Diego, CA) procedure

Intraoperative photograph (a) and illustration (b) showing an alternative patient position, on a radiolucent Jackson table for interlaminar lumbar instrumented fusion (ILIF) with supplemental transforaminal interbody fusion (TLIF)

Posterior view illustrating the midline posterior incision used in the ILIF procedure

Posterior view showing dissection of the intraspinous ligament at the index level, with the ligamentum flavum visualization facilitated by the laminar spreader
After decompression, the interspinous space is carefully prepared using a rasp in a ventral/dorsal motion to lightly decorticate the inferior edge of the superior spinous process and the superior edge of the inferior spinous process. After measuring the interspinous space an ExtenSure® H2™ (NuVasive, Inc.) trial is placed in the interspinous space (Fig. 7.6). Sizing can be assessed by releasing distraction on the rack distractor and toggling the trial ventral/dorsal and superior/inferior to confirm that the trail is snugly secured between the laminae and spinous processes. To preserve sagittal balance, it is not advisable to oversize the trial but rather to use the smallest trial that fits snuggly within the anatomy. Once the appropriate allograft size has been identified, the ExtenSure H2 allograft can be inserted by attaching the allograft to the end of the inserter. The allograft is introduced into the interspinous space until it rests on the superior and inferior laminae (Fig. 7.7a, b). If necessary, the position of the allograft can be adjusted using a tamp. Once the allograft is in position the rack distractor is released and removed, and the rack and Caspar pins are removed.

Lateral illustration showing spinous process distraction and interlaminar graft sizing in the ILIF procedure

Lateral view (a) of interlaminar spacer insertion and posterior view (b) of final placement of the interlaminar spacer
The spinous process is prepared for plate insertion using a Cobb elevator and/or curette to remove any remaining soft tissue along both sides of the spinous processes. To identify the appropriate size for the spinous process plate, a sizing template is placed along the lateral aspect of the spinous processes and a lateral fluoroscopic image is taken. An appropriately sized plate should provide maximum surface area coverage of both spinous processes without extending beyond the cranial edge of the superior spinous process or beyond the caudal edge of the inferior spinous process (Fig. 7.8). Once the plate size has been selected, the corresponding plate can be attached to the inserter and positioned on the lateral aspects of the spinous processes. Once the plates are in position, they are compressed at the plate crossbar in the interspinous region to engage the teeth of the plate into the spinous process. Further compression may be applied directly over the spinous processes to contour the plate to the spinous process anatomy and further secure the teeth of the plate into the spinous processes. Using forceps or similar instrument, biologic materials are applied to the construct between the dorsal aspect of the allograft, spinous processes, and spinous process plates. Once biologic material(s) has been applied, retractor can be removed (Fig. 7.9a, b). The wound is closed in a standard fashion.

Lateral view of the sizing of the spinous process plate

Posterior (a) and lateral view (b) of the final ILIF construct consisting of ExtenSure® H2TM interlaminar spacer, biologic graft material, and Affix® (NuVasive, Inc.) spinous process plate
Patients are encouraged to limit back movement during the rehabilitation period to allow proper bone growth and fusion to occur. Participation in regular low-impact, limited range of motion, cardiovascular exercise (such as walking) may increase blood flow and nutrient delivery to the surgical site to encourage healing.
In summary, ILIF is a minimally disruptive approach to the lumbar spine to perform a distraction laminoplasty followed by interspinous grafting and interspinous fixation. The limited midline exposure avoids trauma to lateral musculature compared to wider exposures used in conventional decompressive or PLF procedures. As patients with LSS often have multiple simultaneous degenerative conditions, one drawback to ILIF is that it alone is not designed to access the intervertebral disc. In patients with discogenic pathology or in patients with hypermobile or normal disc height patients, this may increase the risk of long-term failure of the construct, as with all PLF constructs, where the intervertebral disc remains unaddressed and where continued motion is probable [9, 10, 32, 35, 36, 42]. In these and any other related indications requiring anterior column stability, ILIF can be supplemented with a specialized TLIF procedure through the same midline incision.
ILIF with Supplemental TLIF
As previously mentioned, some evidence has shown that non-pedicle screw and rod fixation for PLF may have an increased likelihood of long-term construct failure without interbody supplementation, especially when posterior to a highly mobile or less degenerative intervertebral disc [42, 43]. As such, a technique for supplementation of ILIF with a specialized TLIF technique has been developed to better treat both tight foraminal narrowing requiring facetectomy and the presence of instability (degenerative or iatrogenic) requiring interbody fusion. In cases of tight foraminal stenosis, distraction afforded by the ILIF procedure as well as the largely central decompression may not be sufficient alone to provide adequate foraminal decompression. In these cases a more robust decompression is warranted, though this compromises stability following facetectomy and requires supplementation to maintain segmental stability during healing [25].
The approach and initial technique for the TLIF-supplemented ILIF begin the same as for the standard ILIF technique, though the lead author (AT) places the patient in the prone position on a Jackson table, rather than a Wilson frame, to facilitate both compression on the interlaminar graft and segmental lordosis following release of interspinous distraction. The same less invasive (3–5 cm) posterior midline incision located at the junction of the spinous processes of the indicated level is used for the combined approach, following a distraction laminoplasty procedure for a standard central decompression. In the interbody fusion supplementation technique, two self-contained retractors can be overlapped to provide exposure for the ILIF procedure and also preferentially expose one side for the TLIF approach, to minimize contralateral morbidity by maintaining as small an incision as possible (Fig. 7.10a, b). These retractors should be placed in combination with the spinous process distractors to allow for the distraction laminoplasty exposure to be maintained during the TLIF procedure (Fig. 7.11a, b).

Photographs showing the retractors that can be used to exposure the site for incisional exposure for ILIF (a), with preferential unilateral exposure to facilitate the TLIF (ipsilateral) (b)

Intraoperative photographs showing surgical setup (a) and simultaneous incisional and interspinous distraction for ILIF and TLIF (b)
To begin, it should be stated that the approach for ILIF differs from a standard TLIF approach, so additional confirmation of the level being treated should be made. In ILIF, interspinous targeting is used to determine the index level and the incision point. A standard TLIF uses a pedicle- or facet-based approach trajectory, and thus, when performing a TLIF through an ILIF exposure, the appropriate facets should be identified on lateral fluoroscopy and marked with a K-wire. For instance, in an L4–5 TLIF through an ILIF exposure, the L5 facet would be marked for access (Fig. 7.12). The start of this technique begins with a partial contralateral facetectomy (approximately 10–15 %, never more than 50 %) of the medial facet aspect to allow for access to the contralateral foramen for decompression without destabilizing the segment [25]. The extent of decompression (out to the medial portions of the facets) can be used in standard ILIF to both adequately decompress the segment and maintain the integrity of the posterior elements, especially in axial rotation. A standard TLIF approach is then used on the ipsilateral side, with facetectomy facilitated by a high-speed burr to resect from the pars through to the lamina, taking the inferior articular facet which allows for access to and visualization of the nerve root (Figs. 7.13a, b). The traversing and existing nerve roots are then isolated retracted medially using a cottonoid and/or wide Penfield elevator for protection during access to the disc space (Fig. 7.14). TLIF annulotomy, discectomy, and endplate preparation are performed in the standard fashion. For the placement of bone graft material and the intervertebral spacer, the primary author (AT) packs the front of the extravasated disc space (posterior to the anterior longitudinal ligament [ALL]) with corticocancellous chips followed by an interdigitating layer of allograft cellular bone matrix (Osteocel® Plus, NuVasive, Inc.). Posterior to this graft material, a curved (banana) TLIF cage is placed in the anterior 1/3 of the disc space with the convexity facing posterior. Posterior to the first cage, a second layer of allograft cellular bone matrix is placed followed by a second curved TLIF cage with its concavity matching the convexity of the first TLIF cage. This graft material–cage–graft material–cage complex should occupy roughly the anterior two-thirds of the disc space, leaving the posterior third free of graft material of intervertebral spacer, to facilitate and maintain a sufficiently decompressed canal and nerve roots during healing (Figs. 7.15 and 7.16).

Lateral intraoperative fluororadiography depicting L5 facet localization in identifying and confirming level during the TLIF approach in the combined ILIF and TLIF procedure. A standard ILIF procedure uses the index level’s interspinous space as an approach landmark, and standard TLIF uses a facet-targeting approach, so by identifying the inferior articular facet (L5 for an L4–5 case), the disc space will be identified by a slight cranial trajectory following facetectomy

Intraoperative photograph (a) and oblique posterior illustration (b) showing facetectomy prior to TLIF in the combined ILIF and TLIF procedure

Posterior intraoperative photograph illustrating nerve root retraction prior to annulotomy and discectomy in TLIF through an ILIF exposure

Lateral intraoperative fluororadiography showing TLIF implant trialing (a) and the anterior column post-TLIF (b)

Lateral (a) and axial (b) illustrations showing TLIF cage and biologic material placement in the specialized TLIF approach to supplement ILIF
Following completion of the TLIF procedure, placement of the interspinous spacer, posterior graft material, and interspinous plate is performed to finalize the ILIF procedure. Closure of the surgical site is then performed in the standard fashion (Figs. 7.17, 7.18, and 7.19).

Intraoperative photographs showing placement of the ExtenSure H2 interlaminar graft (a) and the final ILIF construct (b) following TLIF

Lateral illustration (a) and fluororadiograph (b) showing the final ILIF construct supplemental with TLIF. Note that the interspinous plate can be placed in either vertical orientation

Intraoperative photograph showing the closed incision following a single-level ILIF with supplemental TLIF
Outcomes Including Literature Review
There are few literature results describing the characteristics of and outcomes following ILIF, as the procedure was only introduced in the past several years. However, several testing and early outcome references do exist, showing encouraging results for future evaluation.
A cadaveric study was undertaken by Pradhan et al. [44] to assess the biomechanical characteristics of ILIF (interspinous spacer with spinous process plate) and to compare those results to the results of alternative methods of PLF. In the study, 8 continuous L1–L5 spines underwent nondestructive multidirectional testing across a series of different conditions at L3–4. Test conditions included (1) the intact spine (control), (2) bilateral pedicle screws, (3) bilateral laminotomy, (4) ILIF, (5) partial laminectomy, (6) partial laminectomy plus unilateral pedicle screws, and (7) partial laminectomy plus bilateral pedicle screws. Three cycles of unconstrained, pure-moment flexion and extension, lateral bending, and axial rotation were carried out without compressive load. Data were evaluated from only the third cycle. The most rigid construct, intuitively, was the construct fixation with bilateral pedicle screws without destabilization. ILIF, however, was statistically similar to bilateral pedicle screw fixation with a destabilizing decompression in flexion/extension and axial rotation, though was superior in stiffness to ILIF in lateral bending. In lateral bending, ILIF was found to not differ statistically from unilateral pedicle screw fixation following laminectomy.
Several examples of clinical outcomes following ILIF have been reported or presented. In a retrospective, multicenter review, Bae [45] evaluated pain (visual analog score [VAS]), disability (Oswestry disability index [ODI]), and radiographic outcomes from a series of 52 patients who underwent single-level ILIF. Average operative time and length of hospital stay were 68.5 min and 1.7 days, respectively. Estimated blood loss was <100 mL 93.7 % of patients treated. Two wound complications occurred and three surgical-site reoperations were performed. Reoperations included two rhizotomies and 1 additional decompression for recurrent stenosis. Eighty percent of the patient reached the threshold for minimum clinically important difference (MCID) on VAS and ODI [33].
In a second study of a different patient series, Bae [46] reported interim 12-month clinical and radiographic results from an ongoing multicenter prospective study of ILIF. Evaluations included pain (VAS), disability (ODI), Zurich claudication scores (ZCQ), patient satisfaction, segmental and global lordosis measures, and fusion assessment. Of the 66 patients enrolled 21 were available for 12-month follow-up. Average operative time and length of stay were 71 min and 1.8 days, respectively. Estimated blood loss, similar to the previous study, was <100 mL in 86 % of patients. ODI improved, on average, 31 %, while ZCQ improved 23 %. VAS improved at least 20 mm in 90 % (19/21) of patients. 82 % (17/21) of patients were satisfied with their outcome. On average, global and segmental lordosis changed less than 2° from preoperative, and 71 % of patients exhibited radiographic evidence of interspinous bridging bone. Two instances of asymptomatic spinous process fractures were observed. No revision surgeries were performed.
A recent study by Berjano et al. [47] reported results of ILIF supplemented with interbody fusion as a small subset of a larger series of interbody fusions carried out using extreme lateral interbody fusion (XLIF®, NuVasive, Inc.). In the series, the authors treated 10 % (10/97) patients with ILIF following XLIF, though results were reported only as a whole, not by fixation types as subgroups. Regardless, in the series, low back pain, leg pain, and ODI improved 61, 64, and 55 % (28 point mean absolute ODI improvement), respectively. Clinical success was achieved in 92 % of patients. The authors noted two instances of implant subsidence, both in stand-alone interbody procedures, without any instances of subsidence in patients with supplemental internal fixation (including ILIF).
Complications of Treatment
For the ILIF procedure, standard surgical risks for PLF are a concern, though many are theoretically mitigated through the less invasive incision. The most common concerns for PLF and decompressive surgery, including in ILIF, are dural tears and any resultant sequelae and wound complications. Complications unique to the ILIF procedure, as evidenced in the literature [45], include spinous process fractures. However, all reported spinous process fractures in the literature were asymptomatic.
Conclusions/Personal View
ILIF in the treatment of many classifications of LSS appears to be a viable option based on testing, early literature results, and the outcomes of related techniques for decompression and PLF. The minimally invasive nature of the procedure is advantageous in that it is associated with low operative time and blood loss compared to conventional approaches, with less morbidity and hastened postoperative recovery. Flexibility in being able to deliver a supplemental TLIF through the same exposure provides a mechanism to better address a wider range of lumbar conditions while maintaining the benefits of ILIF alone.
References
Deyo RA, Gray DT, Kreuter W, Mirza S, Martin BI. United States trends in lumbar fusion surgery for degenerative conditions. Spine. 2005;30:1441–5.
Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010;303:1259–65.
Bae HW, Rajaee SS, Kanim LE. Nationwide trends in the surgical management of lumbar spinal stenosis. Spine (Phila Pa 1976). 2013;38(11):916–26.
Fischgrund JS. The argument for instrumented decompressive posterolateral fusion for patients with degenerative spondylolisthesis and spinal stenosis. Spine (Phila Pa 1976). 2004;29:173–4.
Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991;73:802–8.
Kovacs FM, Urrutia G, Alarcon JD. Surgery versus conservative treatment for symptomatic lumbar spinal stenosis: a systematic review of randomized controlled trials. Spine. 2011;36:E1335–51.
Mardjetko SM, Connolly PJ, Shott S. Degenerative lumbar spondylolisthesis. A meta-analysis of literature 1970–1993. Spine (Phila Pa 1976). 1994;19:2256S–65.
Simotas AC, Dorey FJ, Hansraj KK, Cammisa Jr F. Nonoperative treatment for lumbar spinal stenosis. Clinical and outcome results and a 3-year survivorship analysis. Spine. 2000;25:197–203.
Postacchini F. Surgical management of lumbar spinal stenosis. Spine. 1999;24:1043–7.
Sengupta DK, Herkowitz HN. Lumbar spinal stenosis. Treatment strategies and indications for surgery. Orthop Clin North Am. 2003;34:281–95.
Yone K, Sakou T, Kawauchi Y, Yamaguchi M, Yanase M. Indication of fusion for lumbar spinal stenosis in elderly patients and its significance. Spine (Phila Pa 1976). 1996;21:242–8.
Deyo RA. Treatment of lumbar spinal stenosis: a balancing act. Spine J. 2010;10:625–7.
Karikari IO, Grossi PM, Nimjee SM, et al. Minimally invasive lumbar interbody fusion in patients older than 70 years of age: analysis of peri- and postoperative complications. Neurosurgery. 2011;68:897–902.
Rodgers WB, Cox CS, Gerber EJ. Early complications of extreme lateral interbody fusion in the obese. J Spinal Disord Tech. 2010;23:393–7.
Rodgers WB, Gerber EJ, Rodgers JA. Lumbar fusion in octogenarians: the promise of minimally invasive surgery. Spine. 2010;35:S355.
Okubadejo GO, Buchowski JM. The textbook of spinal surgery. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2011. p. 394–401.
Porter RW. Spinal stenosis and neurogenic claudication. Spine. 1996;21:2046–52.
Guigui P, Barre E, Benoist M, Deburge A. Radiologic and computed tomography image evaluation of bone regrowth after wide surgical decompression for lumbar stenosis. Spine. 1999;24:281–8.
Johnsson KE, Rosen I, Uden A. The natural course of lumbar spinal stenosis. Clin Orthop Relat Res. 1992;279:82–6.
Tomkins-Lane CC, Battié MC. Validity and reproducibility of self-report measures of walking capacity in lumbar spinal stenosis. Spine. 2010;35:2097.
Posner I, White III AA, Edwards WT, Hayes WC. A biomechanical analysis of the clinical stability of the lumbar and lumbosacral spine. Spine (Phila Pa 1976). 1982;7:374–89.
Manchikanti L, Cash KA, McManus CD, Pampati V, Abdi S. Preliminary results of a randomized, equivalence trial of fluoroscopic caudal epidural injections in managing chronic low back pain: part 4 – spinal stenosis. Pain Physician. 2008;11:833–48.
Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med. 2008;358:794–810.
Chen E, Tong KB, Laouri M. Surgical treatment patterns among Medicare beneficiaries newly diagnosed with lumbar spinal stenosis. Spine J. 2010;10:588–94.
O’Leary PF, McCance SE. Distraction laminoplasty for decompression of lumbar spinal stenosis. Clin Orthop Relat Res. 2001;384:26–34.
Fritsch EW, Heisel J, Rupp S. The failed back surgery syndrome: reasons, intraoperative findings, and long-term results: a report of 182 operative treatments. Spine. 1996;21:626–33.
Long DM. Failed back surgery syndrome. Neurosurg Clin N Am. 1991;2:899.
Postacchini F, Cinotti G. Bone regrowth after surgical decompression for lumbar spinal stenosis. J Bone Joint Surg Br. 1992;74:862–9.
Martin G. Recurrent disc prolapse as a cause of recurrent pain after laminectomy for lumbar disc lesions. N Z Med J. 1980;91:206–8.
Deschuyffeleer S, Leijssen P, Bellemans J. Unilateral laminotomy with bilateral decompression for lumbar spinal stenosis: short-term risks in elderly individuals. Acta Orthop Belg. 2012;78:672–7.
Kaymaz M, Borcek AO, Emmez H, Durdag E, Pasaoglu A. Effectiveness of single posterior decompressive laminectomy in symptomatic lumbar spinal stenosis: a retrospective study. Turk Neurosurg. 2012;22:430–4.
Knaub MA, Won DS, McGuire R, Herkowitz HN. Lumbar spinal stenosis: indications for arthrodesis and spinal instrumentation. Instr Course Lect. 2005;54:313–9.
Glassman SD, Carreon LY, Djurasovic M, et al. Lumbar fusion outcomes stratified by specific diagnostic indication. Spine J. 2009;9:13–21.
Fischgrund JS, Mackay M, Herkowitz HN, Brower R, Montgomery DM, Kurz LT. 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine (Phila Pa 1976). 1997;22(24):2807–12.
Boden SD. The use of radiographic imaging studies in the evaluation of patients who have degenerative disorders of the lumbar spine. J Bone Joint Surg Am. 1996;78:114–24.
Boden SD, Wiesel SW. Lumbar spine imaging: role in clinical decision making. J Am Acad Orthop Surg. 1996;4:238–48.
Rihn JA, Patel R, Makda J, et al. Complications associated with single-level transforaminal lumbar interbody fusion. Spine J. 2009;9:623–9.
Bowers C, Amini A, Dailey AT, Schmidt MH. Dynamic interspinous process stabilization: review of complications associated with the X-stop device. Neurosurg Focus. 2010;28:E8.
Albee FH. The classic. Transplantation of a portion of the tibia into the spine for Pott’s disease. A preliminary report. Jama, 57: 885, 1911. Clin Orthop Relat Res. 1972;87:5–8.
Hibbs RA. An operation for progressive spinal deformities: a preliminary report of three cases from the service of the orthopaedic hospital. 1911. Clin Orthop Relat Res. 2007;460:17–20.
Howorth MB. Evolution of spinal fusion. Ann Surg. 1943;117:278–89.
Heggeness MH, Esses SI. Translaminar facet joint screw fixation for lumbar and lumbosacral fusion. A clinical and biomechanical study. Spine (Phila Pa 1976). 1991;16:S266–9.
Boden SD, Riew KD, Yamaguchi K, Branch TP, Schellinger D, Wiesel SW. Orientation of the lumbar facet joints: association with degenerative disc disease. J Bone Joint Surg Am. 1996;78:403–11.
Pradhan BB, Turner AW, Zatushevsky MA, Cornwall GB, Rajaee SS, Bae HW. Biomechanical analysis in a human cadaveric model of spinous process fixation with an interlaminar allograft spacer for lumbar spinal stenosis: laboratory investigation. J Neurosurg Spine. 2012;16:585–93.
Bae HW. A multi-center review of single-level interlaminar lumbar instrumented fusion (ILIF): early clinical and radiographic outcomes. Society For Minimally Invasive Spine Surgery (SMISS): 2012 annual meeting; Miami Beach, Sept 2012.
Bae HW. 12-month clinical and radiographic results from an ongoing prospective, multicenter evaluation of interlaminar lumbar instrumented fusion (ILIF). Society For Minimally Invasive Spine Surgery (SMISS): 2012 annual meeting, Miami Beach, Sept 2012.
Berjano P, Balsano M, Buric J, Petruzzi M, Lamartina C. Direct lateral access lumbar and thoracolumbar fusion: preliminary results. Eur Spine J. 2012;21 Suppl 1:S37–42.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
Thompkins, A.A. (2014). Less Invasive Decompression and Posterolateral Fusion Using Interlaminar Lumbar Instrumented Fusion (ILIF) with or Without Supplemental Transforaminal Lumbar Interbody Fusion (TLIF). In: Menchetti, P. (eds) Minimally Invasive Surgery of the Lumbar Spine. Springer, London. https://doi.org/10.1007/978-1-4471-5280-4_7
Download citation
DOI: https://doi.org/10.1007/978-1-4471-5280-4_7
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-5279-8
Online ISBN: 978-1-4471-5280-4
eBook Packages: MedicineMedicine (R0)