
Abstract
To investigate the effects of a 100-mg oral single-dose administration of sarpogrelate hydrochloride (SH) on saturation O2 (StO2) of calf muscle in healthy subjects experiencing simulated peripheral arterial disease (0.6 ankle brachial pressure index). Ten subjects performed three kinds of plantar flexion exercises at a work rate of 50% of maximal volunteer contraction for 4 min by using cuff occlusion ischemia,. Subjects performed a control test (C) without ischemia and SH, an ischemia test (I) without SH, and an I + SH test with ischemia. StO2, blood pressures (BP), and heart rate (HR) were measured through all experiments. At the end of the exercise, the decrease in StO2 from baseline in the C and I + SH tests was significantly less than that in the I test (p < 0.05, respectively). However, there were no significant differences in mean BP or HR in any of the exercise conditions. These results indicated that an oral single-dose administration of SH might improve peripheral circulation independent of any changes in BP and HR.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
- Peripheral Arterial Disease
- Calf Muscle
- Blood Flow Restriction
- Ankle Brachial Pressure Index
- Peripheral Arterial Disease Patient
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Sarpogrelate hydrochloride is an effective therapeutic drug that has been widely used for peripheral arterial disease (PAD) patients in Japan [6]. Although it has been reported that long-term oral administration of sarpogrlate hydrochloride improves vascular function in PAD patients [8], investigation of the effects of a single-dose administration of sarpogrelate hydrochloride on PAD patients has been insufficient. Knowledge of these effects is important for the noninvasive, continuous, and accurate evaluation of PAD patients.
Saturation O2 of muscle oxygenation (StO2) derived by near-infrared spectroscopy (NIRS) is represented by the ratio of HbO2 to total Hb. It is thought that StO2 would be a useful index of oxygen delivery and utilization. Therefore, this useful technique has been widely used to evaluate variation in the severity of PAD [5, 7]. However, it might be difficult to evaluate PAD patients accurately because of variation in disease severity and/or the effects and histories of administration of other medication.
The purpose of this study, therefore, was to investigate the effects of an oral single-dose administration of sarpogrelate hydrochloride on muscle oxygenation responses during plantar flexion exercise in healthy subjects who were simulated PAD patients using cuff occlusion ischemia.
2 Methods
Ten healthy male subjects with mean age 36 (5) years, height 174 (6) cm, body mass 65 (7) kg, participated in this study (values are means and standard deviation). All subjects were informed about this study and consent was obtained. This study was approved by an ethical committee of Hokusho University, Japan.
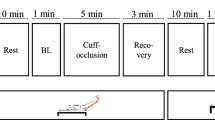
The subjects performed three kinds of unilateral planter flexion exercise with a long sitting position. The workload of all experimental exercises was set at 50% based on 1 repetition maximum. Subjects performed plantar flexion exercises for 4 min after 2 min of rest with 40 repetitions per 1 min, lifting the weight 5 cm above the ground. Exercise protocols were as follows: Control test (C) without ischemia and administration of sarpogrelate hydrochloride, Ischemia test (I) without administration of sarpogrelate hydrochloride, and ischemia test with administration of sarpogrelate hydrochloride (I + SH).
Subjects performing the I and I + SH tests had restricted blood flow caused by a pressure cuff in order to simulate PAD patients with 0.6 ankle brachial pressure index (ABI). To accomplish this, 40% pressure of systolic blood pressure (SBP) for an individual subject was carried out with a rapid inflator on the thigh muscle throughout the experiment. An oral single dose of sarpogrelate hydrochloride, 100 mg, was administered before 0.889 h of each test based on the Tmax [3].
During all tests, the responses of peripheral muscle oxygenation were measured using near-infrared spectroscopy (NIRS: BOM1-TRW, Omegawave, Japan). Optodes consisting of a transmitter and detector were placed on the right calf muscle, and the distance between the light source and the photo detector was 3 cm. This unit has continuous light source of triple wavelength (780, 810, and 830 nm) and calculates relative changes in tissue levels of muscle oxygenation (HbO2), deoxygenation, and total Hb, according to the Beer-Lambert law. The instrument can calculate tissue blood oxygen saturation in muscle (StO2, %) from the ratio of HbO2 to totalHb after assuming a certain density of the red cells in the blood; here we present our results as changes in StO2. The data were sampled by every second.
BP was monitored by the cuff occlusion method, and heart rate (HR) was monitored in synchronization with BP. Both parameters were measured at rest and 90 s after the onset of exercise at 1-min intervals. The mean BP (MBP) was calculated as diastolic pressure plus one-third of pulse pressure.
StO2 responses in the primary decreasing phase in the first 2 min minus the first 10 s were approximated by the following equation:
where t is a given length of time, b is a baseline value at the onset of exercise, Amp is an amplitude between baseline value and a value at 2 min of the exercise, TD is a time delay, and τ is a time constant.
StO2 of the calf muscle was represented as the values of a 30-s interval to minimize variability, and it represented the relative change from the value at baseline. MBP and HR were also represented as the relative change from the baseline value.
One-way ANOVA was used to compare the relative changes of StO2, BP, and HR among three experimental conditions. Significance level was accepted at p < 0.05.
3 Results
Mean values of systolic BP, ABI, skinfold thickness of calf muscle, 1 RM data, resistance load of 50% 1 RM, and applied cuff pressure to simulate PAD in all subjects were 123 (7) mmHg, 1.11 (0.06), 5.3(0.7) mm, 32 (6) kg, 15 (3) kg, and 51 (2) mmHg, respectively.
The time constant in the I and I + SH tests seemed to be slower than that in the C test. In fact, the time constant in the I (19.5 ± 3.6 s) and I + SH (16.8 ± 4.2 s) tests was significantly slower than that in the C (9.3 ± 2.8 s) test (p < 0.05, respectively).
StO2 changes by 30-s interval from a baseline value for all subjects are shown in Fig. 1. StO2 decreased with a short time delay in all conditions. In the C test, StO2 continued to decrease until about 120 s, and then it showed almost a plateau phase until the end of exercise. In the I test, it decreased rapidly until about 60 s, after which it continued to decrease gradually until the end of exercise. In the SH test, it decreased rapidly until about 60 s, after which it continued to decrease gradually until about 3 min of exercise, at which point it began to increase slightly until the end of exercise. During exercise, there were significant differences in the relative change from baseline of StO2 at 3.5 and 4 min of exercise between the C and I tests (at 3.5 and 4 min) and between the C and I, the I and SH tests (at 4 min), (p < 0.05, respectively). However, there were no significant differences in StO2 changes at 3.5 and 4 min between the C and SH tests.

Changes in StO2 from the baseline during all experimental conditions. □; control test, •; ischemia test, ○; sarpogrelate hydrochloride test. *; p < 0.05 between control and ischemia test, #; p < 0.05 between sarpogrelate hydrochloride and ischemia test
Figure 2 shows the changing rate of MBP and HR from baseline values in all conditions, respectively. Both MBP and HR showed almost the same kinetics. MBP and HR increased temporarily after the onset of exercise, then it showed stable values during exercise. After the end of exercise, each decreased slightly and recovered toward the baseline value. There were no significant differences in MBP and HR among the experimental conditions.

Changes in mean blood pressure (MBP; left panel) and heart rate (HR; right panel) from the baseline during all experimental conditions. □; control test, •; ischemia test, ○; sarpogrelate hydrochloride test
4 Discussion
It is reasonable that StO2 could change in either direction during exercise. That is, if StO2 increases during exercise, it may mean that O2 delivery to the active muscle exceeds O2 utilization in the muscle. If StO2 decreases during exercise, it may mean that StO2 utilization in the muscle exceeds O2 delivery to the active muscle. It has been reported that StO2 kinetics of calf muscle during plantar flexion exercise at a lower work rate [1] in PAD patients was slower compared with that of healthy subjects. This slower kinetics may be associated with skeletal muscle metabolism, including muscle oxygen consumption, because of the lack of any difference in blood flow between PAD patients and healthy subjects [1]. However, we simulated a situation of PAD patients with 0.6ABI using a cuff occlusion method by creating a relative lower pressure temporarily, and hence, muscle metabolism was not impaired. Thus, cuff occlusion ischemia might affect muscle blood flow rather than muscle metabolism. In this study, a slower time constant in the I and I + SH tests was observed compared with that in the C test. This slower response might have been caused by lower blood flow into the working muscle due to the ischemia by cuff occlusion. However, there were no differences in time constant between the I and I + SH tests.
In the decreasing phase of StO2 during exercise, O2 utilization was supposed to be greater than O2 delivery due to blood flow restriction by ischemia. After 120 s of the C test, the balance between O2 delivery and utilization may have remained constant, because StO2 showed almost no change until the end of exercise. On the contrary, it is reasonable that O2 utilization continued to exceed O2 delivery until the end of the I test. Interestingly, in the latter period of the SH test, StO2 increased slightly. As exercise continued at a same work rate in all experiments, it is unlikely that O2 utilization decreased only in the latter phase during the SH test. Moreover, we controlled the workload that subjects could perform when lifting the weight 5 cm above the ground accurately throughout all experiments. SH is an effective medication that inhibits platelet aggregation induced by collagen and secondary aggregation by ADP or epinephrine [2]. Moreover, SH inhibits 5HT2 receptor specifically [9] with result that it can be reasonably expected to improve blood flow in tissues, because 5HT2 receptor is related to vasoconstriction [10].
To our knowledge, there has been no previous study about the effects of single-dose administration of SH on the hemodynamics of calf muscle, in particular, in simulated PAD patients of the same ABI without any effects of other factors such as cardiovascular disease, diabetes, or the action of other medication. Although we cannot compare our results with those of previous studies, we tentatively conclude, based on our results, that local muscle O2 delivery might have increased in the latter phase of the SH test due to the effects of sarpogrelate hydrochloride.
Based on “Starling’s equation”, it is well known that stroke volume is affected not by arterial blood pressure but inflow in the vein. In the present study, as MBP and HR did not change during exercise in any of the test conditions, it was suggested that cardiac output did not increase during exercise. Therefore, it is unlikely that a single-dose administration of sarpogrelate hydrochloride affects the circulating blood volume from the heart.
5 Conclusion
Our results indicated that an oral single-dose administration of sarpogrelate hydrochloride improved peripheral hemodynamics in the latter period of exercise under greater demand of oxygen delivery and utilization during the exercise, independent of a lack of changes in blood pressure and heart rate.
References
Bauer TA, Brass EP, Barstow TJ, Hiatt WR (2007) Skeletal muscle StO2 kinetics are slowed during low work rate calf muscle in peripheral arterial disease. Eur J Appl Phyisol 100: 143–151.
Hara H, Osakabe M, Kitajima A, Tamamo Y, Kikumoto R (1991) MCI-9042, a new antiplatelet agent is a selective S2-serotonergic receptor antagonist. Thromb Haemost 65(4): 415–420.
Isogai Y, Yokose T, Ikemoto T, Maeda T, Akiyama M, Hara H, Kitajima A, Izawa O (1991) Phase- 1 Study of sarpogrelate hydrochloride (MCI-9042) – single and repeated oral administration study. J Clin Therap Med 7 (6): 1177–1192.
Kawaguchi K, Tabusadani M, Sekikawa K, Hayashi Y, Onari K (2001) Do the kinetics of peripheral muscle oxygenation reflect systemic oxygen intake? Eur J Appl Physiol 84: 158–161.
Komiyama T, Shigematus H, Yasuhara H, Muto T (2000) Near-infrared spectroscopy grades the severity of the intermittent claudication in diabetics more accurately than ankle pressure measurement. Br J Surg 87(4): 459–466.
Matsubara J, Shiiya N, Ishida A, Miyata T, Shigematsu H, Obitsu Y, Shindo T, Hida K, Ohta T, Ando M, Nishibe T, Kawasaki T, Yasugi T, Onohara T (2007) Current status of medication therapy for arteriosclerosis obliterans (ASO) in University Hospital in Japan. J Jpn Coll Angiol 47: 153–162.
McCully K, Landsberg L, Suarez M, Hofman M, Posner JD (1997) Identification of peripheral vascular disease in elderly subjects using optical spectroscopy. J Gerontology 52A: B15–B165.
Miyazaki M, Higashi Y, Goto C, Chayama K, Yoshizumi M, Sanada H, Orihashi K, Sueda T (2007) Sarpogrelate hydrochloride, a selective 5-HT2A antagonist, improves vascular function in patients with peripheral arterial disease. J Cardiovasc Pharamacol 49(4): 221–227.
Tsuchihashi H, Yagi N, Kimura M, Shirota K, Kinami J, Ngatomo T (1991) Binding characteristics of 3H ketanserin for serotonin-2 receptor in the rabbit platelet. J Pharmacobiodyn 14(8): 461–466.
Vanhoutte PM, Houston DS (1985) Platelets, endothelium, and vasospasm. Circulation 72(4): 728–734.
Acknowledgments
This study was supported by Tanabe-Mitsubishi Pharmaceutical Company.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer Science+Business Media, LLC
About this paper
Cite this paper
Horiuchi, M. et al. (2010). Effects of Oral Single-Dose Administration of Sarpogrelate Hydrochloride on Saturation O2 of Calf Muscle During Plantar Flexion Exercise. In: Takahashi, E., Bruley, D. (eds) Oxygen Transport to Tissue XXXI. Advances in Experimental Medicine and Biology, vol 662. Springer, Boston, MA. https://doi.org/10.1007/978-1-4419-1241-1_77
Download citation
DOI: https://doi.org/10.1007/978-1-4419-1241-1_77
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4419-1239-8
Online ISBN: 978-1-4419-1241-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)