
Abstract
Asthma is one of America’s most perplexing public health problems. It is a ubiquitous and costly disease of society, as well as individuals. This chapter examines asthma in the larger context of public health by discussing different but related aspects of disease management and control. We will consider the way the characteristics of the society affect the extent and severity of the disease, and how asthma affects important public health indicators of well-being. We will review examples of interventions, some that have focused on clinical settings and some that have ventured into the community to relieve the burden of asthma more broadly. We will suggest how these efforts can be directed to generate a wider change. We will discuss ways to modify the impact of the condition through policy. Finally, we will consider the problems in our current approaches to asthma control and suggest alternative directions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Asthma is one of America’s most perplexing public health problems. It is a ubiquitous and costly disease of society, as well as individuals. This chapter examines asthma in the larger context of public health by discussing different but related aspects of disease management and control. We will consider the way the characteristics of the society affect the extent and severity of the disease, and how asthma affects important public health indicators of well-being. We will review examples of interventions, some that have focused on clinical settings and some that have ventured into the community to relieve the burden of asthma more broadly. We will suggest how these efforts can be directed to generate a wider change. We will discuss ways to modify the impact of the condition through policy. Finally, we will consider the problems in our current approaches to asthma control and suggest alternative directions.
The Public Health Burden of Asthma
Asthma exacts a toll not only for the person with the disease, but those closest to him or her. In addition, extant evidence suggests that the public health impact of asthma is substantial and that characteristics of the society themselves conspire to create a disease that is more prevalent and more serious than an alternative set of conditions .
Asthma costs the society greatly. Over 15 million people suffer from asthma, and it affects children and adolescents more than any other illness (Sondik 2008). Each year in the U.S., there are 5,000 deaths, 500,000 hospitalizations, and 2 million ED visits for asthma. In 1998, health care costs were approximately $12.7 billion. Just over 58% of asthma-related health care costs were direct medical care costs of which 45% comprised hospitalizations, outpatient hospital visits, and ED visits. Over 40% were the costs indirectly associated with the illness (Sondik 2008). Adults with asthma have more days of poor health, as well as more days with limited activity than adults who do not have asthma. Adults who have children with asthma accrue more work absence days and restricted days than parents of children where asthma is not present (Goldfarb et al. 2004). Asthma annually accounts for 14 million school absence days and 14.5 million work absence days.
Societal Influences on Asthma
Perhaps, the most well-documented society-wide features associated with more severe asthma are the economic, social, and demographic factors reflected in a community and seen specifically in income, education, age, race/ethnicity, sex, physical environment, stress, and obesity.
Income
Income disparities among populations have long been shown to produce a negative picture of health status in public health data in general (Kaplan et al. 1996) and in asthma specifically (Weiss et al. 1992). The extent to which income is a proxy for other related characteristics of a population such as education and race/ethnicity has been discussed. One or two studies have indicated that the contribution of race, specifically the African American, to asthma prevalence, morbidity and mortality is independent of income (Grant et al. 2000). Others contend that the two are so interrelated as to confound efforts to consider them separately (Weiss et al. 1992). Regardless, being poor is hazardous to one’s health and results in severity and premature mortality for people with asthma which is more than twice as common than in those of higher income (Volmer 2001).
The way in which low income leads to more burdensome asthma frequently has been discussed. Access to a requisite level of quality of clinical care has been identified (National Asthma Education and Prevention Program, 2007). For example, children in a community where the average family income is less than $20,000 per annum have been shown to be on clinical regimens for asthma that fall far below the National Asthma Education and Prevention Program (NAEPP) standard of care (Cabana et al. 2004; Clark et al. 2002). Emergency department data (Radeos et al. 2001) illustrate that income is closely associated with the lack of follow-up care subsequent to an urgent asthma ED visit.
Interestingly, studies have suggested that the majority of poor asthma patients, especially children, have some form of insurance coverage that would give them access to a health care provider (Clark et al. 2004). However, two glaring problems greatly reduce one’s optimism about this apparent fact. First is the previously mentioned questionable quality of care that may be provided. Second is the well-documented fact that 20 million Americans (conservatively speaking, 10% of whom have a respiratory condition) have no health insurance and, frequently, avoid seeking health care even in urgent situations (Ayanian et al. 2000; Becker 2001; Sudano and Baker 2003). African American and Latino/Hispanic people are more likely not to have health insurance [American Diabetes Association (ADA) 2008]. Effective clinical care is the frontline of defense for managing asthma. The presence of large numbers of citizens who have no care or receive inadequate care guarantees the failure of public health disease control efforts.
The cost of asthma drugs is another route for producing ill effects for the poor. For example, Ungar et al. (2005) showed that at a cost of $300–$3,000 a year, paying for asthma medicine reduces the ability of families to pay for other essentials, e.g. food and housing, as well as “nonessentials” such as recreation. These costs were also shown to detract from vital long-term family investments; for example, the child’s future education, home mortgages, etc. Stealing from the future helps perpetuate poverty and ill health for asthma sufferers.
Race/Ethnicity
Despite the discussion of race/ethnicity as a confounder with income, one’s racial and ethnic identification has frequently been associated with asthma (Gupta et al. 2006) and the asthma disparities observed between minority and nonminority groups. For example, mortality data indicate that young, African American men are particularly susceptible to death from asthma (McFadden and Warren 1997; Weitzman et al. 1998). Krishnan et al. (2006) subsequent to a study of patients hospitalized for asthma concluded that the overall higher risk of death from asthma in black patients compared with white patients is not explained by race differences in hospital deaths and is attributable to factors preceding hospitalization. Research has also found that young children of African American and Latino/Hispanic families admitted to the hospital for asthma were less likely to have received optimum preventive therapy and experienced lower quality discharge planning compared to white patients (Finkelstein et al. 1995). Epidemiologic data suggest that asthma prevalence in predominantly Latino/Hispanic areas such as Puerto Rico are far above national averages (Lara et al. 2006; Sondik 2008). Data also indicate that asthma in pregnancy worsens most significantly for African American women (Carroll et al. 2005).
An interesting study by Cunningham et al (1996) suggests another way that race may play out in asthma. They found that minority patients were more likely than others to receive a diagnosis of asthma. On the other hand, race did not influence the higher presence of asthma symptoms. No definitive explanation is available for this contradiction, although one speculation is that clinicians may be responding to the epidemiological data suggesting that minorities are more susceptible to the disease.
The glaring reality in such studies is that whether there is some unexplained causative factor in race/ethnicity or whether these variables actually represent lower income in the populations studied, minority people with asthma have been shown to be more vulnerable as far as prevalence, incidence, and burden of the diseaseare concerned.
Education, Age, and Sex
Education too has predicted asthma outcomes. Educational background has been shown to enable (when at a higher level) or detract (when lower) from an asthma patient’s ability to access specialized asthma care (Finnvold 2006). Education, defined as a low level of health literacy, has been shown to predict poor longitudinal asthma outcomes (Mancuso and Rincon 2006). It has also been shown to be independent of income in predicting negative consequences of asthma for African Americans (Grant et al. 2000).
Age and sex are influential in asthma. Most Americans are aware that the general population is aging. By 2030, it is estimated that about 20% of the U.S. population will be 65 years of age or older (Centers for Disease Control 2003). Currently, older individuals comprise 10% of the population of asthma sufferers, and this growing population of individuals over time is likely to require more hospitalizations and longer stays for asthma (Cortes et al. 2004). As noted earlier, adolescent age puts some individuals with asthma at greater mortality risk. Further, young children have consistently accounted for the highest number of emergency department visits for asthma in the U.S. (Centers for Disease Control 2002).
Sex, too, plays a role. Asthma clearly predominates in boys in childhood and in women in adulthood (Mannino et al. 2002; Schatz et al. 2006). Somewhere around puberty, asthma makes the epidemiological transition from favoring males to favoring females. Quite likely, hormonal factors play an important role in this shift, but the particular mechanisms are not well understood. Nonetheless, in childhood, more boys than girls have a diagnosis and symptoms and are taken for health care services although the proportionate differences are not always great (Schatz et al. 2006). In adulthood, however, significantly more women are burdened with asthma. They have 30% higher prevalence, 50% higher outpatient care use, a 35% higher hospitalization rate, a 6% higher ED use rate, and a 40% higher death rate than men (Sondik 2008)
Stress, Depression, and Violence
There are a range of other complex societal features that have been explored as influences on the prevalence of asthma and public health efforts to control the disease. These include the levels of stress, depression, and violence in a community.
Some of the most interesting works regarding these aspects of asthma have been done by Wright and colleagues. For example, their group has provided persuasive evidence that psychological stress is associated with atopy in predisposed children (Wright et al. 2005; Wright et al. 2004a) and that higher parental levels of stress predict wheezing in infants (Wright et al. 2002). As one might expect, stress has been identified at particularly high levels in low income communities (Ampon et al. 2005). Depression (some say the major chronic condition of the 21st century) has been shown to be associated with lower levels of asthma-related quality of life (Kullowatz et al. 2006), and one study has indicated that its effects may be additive in producing an adverse quality of life (Opolski and Wilson 2005). Likely of little surprise to any reader are the data that illustrate low income mothers of children with asthma report more symptoms of depression and the presence of more life stressors than those of higher income (Shalowitz et al. 2006) and that mental health is a significant factor in predicting asthma morbidity (Weil et al. 1999).
Wright et al. (2004b) and Wright and Steinbach (2001) have also shown the complex picture that exposure to violence draws for children with asthma. Their study illustrated that the higher the level of exposure to violence, the greater the number of days with asthma symptom for the child and the more nights the child’s caretaker lost sleep. When stress levels were controlled in the analyses, the gradient of increase in the outcomes was somewhat attenuated. In short, however, one can say that neither stress nor exposure to violence is good for any child, and this fact is especially clear for a child with asthma.
On the other hand, those with circumstance, reason, or predisposition to be optimistic appear to have a different disease trajectory. Kubzansky et al. (2002) in a longitudinal study of older men with asthma illustrated that their level of optimism about their life and health was significantly associated with better FEV1 (forced expiratory volume) and forced vital capacity.
Obesity and Asthma
As public health data and public attention have increasingly concerned the rising levels of obesity and overweight in the U.S., their associations with asthma have been discussed (Chinn et al. 2006; Flaherman and Rutherford 2006; Hendler et al. 2006). Cogent arguments for the role of leptin in obesity and asthma have been made (Mancuso et al. 2004; Shore et al. 2005). One review (Ford 2005) suggested that in adults obesity was higher in those with asthma. Among children and adolescents, study results were less consistent. Prospective studies have found a link between higher BMI (body mass index) at baseline and an increased risk for asthma in adults; however, again, data were inconclusive regarding children. Reports show particularly high levels of overweight and obesity among female patients with asthma (Clark et al. 2003) and illustrate increased symptoms in these women compared to those of normal weight (Clark et al. 2003). Two or three studies suggest that weight loss reduces asthma symptoms (see in: (Ford 2005)). However, the chicken or egg question about asthma and overweight has not been answered. Are overweight people more susceptible to asthma or does being overweight exacerbate a problem that was already there? Regardless of the answer, it would appear that being overweight or obese gives rise to problems with managing asthma. These problems are on the rise, and, in part, are viewed as a social-cultural phenomenon. Our current understanding of day to day management of asthma does not stretch to the special problems of the overweight.
Physical Environment
Yet another set of public health concerns is the physical environment of a community. At least two aspects of the environment, indoor and outdoor conditions, have been discussed as essential to asthma control. Further, the interaction of the physical and social environments as a predictor of more asthma symptoms has been considered (Levy et al. 2006). In two reports, the Institute of Medicine (IOM) (Institute of Medicine 2000, 2004) has described factors in the indoor physical environment associated with asthma. In “Clearing the Air,” the IOM provides evidence to support the presence of cat dander, cockroach antigen, house dust mites, and environmental tobacco smoke (ETS) as causally related to the development of asthma. In “Damp Indoor Spaces,” dampness, usually a function of inadequate building construction, is viewed as precipitating respiratory symptoms in sensitized persons and people with asthma. All these factors (except ETS) have been associated with low income.
A number of studies have connected air pollution, i.e. particulate matter in the air, to asthma symptoms. For example, levels of air pollutants above the National Ambient Air Quality standards have been shown to adversely affect lung function of susceptible children with asthma (Lewis et al. 2005). However, the data are not definitive regarding the aspects of air of matter that are most troublesome in asthma, nor the underlying mechanisms that produce ill effects. As a result, policy action is made more difficult. Further, the standards that may apply to adults may be different for children, and the policy actions to control pediatric asthma deserve more concerted attention (Goldman et al. 2004).
In summary, asthma is a significant public health problem. In reciprocal fashion, the nature of the society regarding its economic, social, and psychosocial features exerts influence on asthma prevalence and burden, and asthma detracts significantly from the public’s health. One can argue that to realize a dramatic downturn in negative asthma outcomes, for example, reduction in asthma disparities evident across populations in the U.S., fundamental economic changes are needed to eliminate the pockets of poverty associated with these disparities. This position has been well formed by a number of observers (Kaplan et al. 1996). Another part of the problem may be the ways in which we conceive of helping those with asthma control the effects of the disease. Control, that is, full functioning with no (or rare) symptoms, is the benchmark of success as long as we are unable to cure or prevent asthma.
Interventions for Asthma Control
Public health efforts to achieve control over asthma have tended to be directed toward therapies (see, for example, (Paltiel et al. 2001)) and more effective organization and delivery of health services (Weiss et al. 1992). There is little doubt in the mind of an informed observer that these are needed fixes. However, in our vision of intervention, we have usually ignored or avoided a locus of power for real change in asthma outcomes: effective management by the person himself or herself who has the disease. Further, we have failed to recognize that the major task of everyone else in the circles of influence of such an individual is assisting the person to manage optimally. Excellent therapies are a needed element of control. Members of the health system must be the guides and advisors of patients and families. But, the power is in the hands of the individual and the resources available to that person, as well as the efforts of those surrounding him or her, who enable or deter effective management.
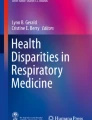
Figure 20.1 presents the concentric circles of influence in asthma control. It shows that at the center of all efforts is the patient whose capacity for day to day management must be at an optimum level to enable full functioning and quality of life. Families must positively support the one managing the disease. The responsible clinician must guide and recommend appropriate actions for the person and family, and do so within a health system that is effectively and efficiently organized to enable the clinician to help the patient. The neighborhood or community must be aware of the problem and nurture and sustain the person and family in their efforts. The physical environment must be one that fosters health. Policies must be conducive to effective asthma management and control.


Concentric circles of influence in asthma control
If our collective efforts focus on this vision of capacity, they are likely to be more successful in reaching the goals of fewer symptoms, more appropriate health care use, full functioning of patients, and families that reach their optimum level of asthma-related quality of life.
Management by People with Asthma and their Families
Indeed, we have examples of a number of types of interventions that appear to have built capacity for effective asthma management. A fair number of clinical trials have been directed at the center of the circles of influence: management by individual patients. Many have shown positive results. For example, Gibson et al. (2000) in a systematic Cochrane review showed that self-management interventions for adult patients resulted in changes in symptoms, health care use, and quality of life. Wolf and colleagues in another Cochrane review (Wolf et al. 2003) showed similar results for interventions directed at children with asthma. This form of capacity building is widely accepted as important (National Asthma Education and Prevention Program, 2007) to asthma control. Yet, the quality and quantity of programs that are actually available and accessible for individual patients have been called into question. Proven models have not been replicated, modes of wide spread distribution have not been found, and financial support for interventions to enhance patient self-management is not widely available.
There are far fewer studies that show us how to build capacity in the other circles of influence, that is, beyond the individual’s management abilities. Some, however, hold promise, for example, capacity building programs for families (Hindi-Alexander and Cropp 1984; Melnyk et al. 2004; Wilson et al. 1996). Family involvement is crucial when the patient is a child, and these caretakers have been the target of effective interventions to enhance their capacity to support and, as needed, undertake management on behalf of the child (Wilson et al. 1996). For example, studies illustrate that parents can be directly helped through an educational intervention to manage a child’s asthma better (Clark et al. 2004) and a program for children that indirectly involves parents also can enhance their management (Evans et al. 1987).
Management by Clinicians and the Health System
A small but important body of work has concerned the capacity of clinicians and of the health care system to organize and deliver effective support to the person managing asthma. For example, brief interventions to build the capacity of physicians to provide guideline-recommended therapies, communicate with, and educate their patients have been shown to significantly improve physician performance, patients’ health care use, and family ratings of the care they received (Cabana et al. 2006; Clark et al. 1998, 2000). Nurses deployed to provide follow-up care to asthma patients have been shown to be effective and comprise the equivalent of physician follow up care (Nathan et al. 2006). Community health workers have been successfully utilized to extend asthma clinical care to high risk individuals (Perez et al. 2006). Emphasizing, as part of emergency department services, the need for continuity of asthma care has been shown to increase subsequent visits by patients to a primary care physician (Sockrider et al. 2006; Zorc et al. 2003), and ED information systems have been used to track action plan use and use of controller medicine (Boychuck et al. 2006). System-wide interventions to improve disease management for asthma within a facility have been shown to increase physician adherence to asthma guidelines for diagnosis and treatment and to reduce health care use (Cloutier et al. 2005). Physician information systems, case management, and quality improvement activities have been associated with positive outcomes (Sullivan et al. 2005). Nonetheless, these interventions have rarely been replicated, tested for generalizability, or disseminated beyond the initial research site.
Communities and Coalitions
The same might be said for community-based efforts: reaching those with asthma through schools, work sites, and in other community settings. However, a number of excellent prototypes do exist (Clark et al. in press). For example, a number of investigators have examined models for school-based programs to build the capacity of children, their parents, and those in the school system to manage asthma. These efforts have been undertaken in elementary schools (Clark et al. 2004; Levy et al. 2006; Splett et al. 2006) and in high schools (Shah et al. 2001) with positive results related to the child’s asthma symptoms, activity levels, and academic performance. At least one study has shown that hospitals are willing and effective partners in school based programs (Byrne et al. 2006) and that school-based programs can be disseminated to additional school sites (Johnstone et al. 2006).
Community coalitions for asthma control (there are more than 200 asthma coalitions in the U.S. alone) have proven effective in mobilizing important organizations and constituencies to work collaboratively. The means by which they organize and carry out their work has been closely examined (Clark et al. 2006). The contribution of asthma coalitions to community organization, development of leadership, and creation of new collaborations has been documented (Butterfoss et al. 2006; Clark et al. 2006; Krieger et al. 2006; Nicholas et al. 2006; Wandersman 2003; Wandersman et al. 1996). The promise of the community coalitions is great, currently there is limited information about their ultimate impact on the health status of individual asthma patients or benefits for their families. Although the available data are promising suggesting that both policy change and improved asthma status for children can result from the work of coalitions (Clark et al. 2009). Work sites, churches, recreational facilities, and other community venues have not been examined regarding their effectiveness and efficacy for supporting management by asthma patients, but they may well hold potential.
Interventions designed to enable people with asthma to control indoor environments have been shown to reduce the presence of dust mites, dander, and cockroach antigen; however, subsequent changes in asthma symptoms or exacerbations have not been well documented (Institute of Medicine 2000), and/or studies have not separated environmental changes from other social and behavioral efforts (Kercsmar et al. 2006). Careful examination of changes in health associated with remediation of building dampness has not been undertaken, although there is consensus that constructing buildings to resist dampness should be the standard of practice (Institute of Medicine 2004).
Changing standards for clean air (U.S. Clean Air Act Amendments 1990) have been examined for their impact on the health of children. Prospective analyses suggest that the benefits of such change would greatly outweigh the costs (Wong et al. 2004), although data regarding specific asthma outcomes are scarce.
The utility and impact of interventions across the circles of influence on asthma management, such as the ones described here, ultimately depend on the extent to which they (and other successful innovations for asthma control) become regular practice as usual in families, health systems, and communities in the country. No doubt, sustaining and disseminating effective asthma programs and services are do-able; however, this result is likely possible only with organizational, institutional, community, and public policies that specifically support capacity building and effective practice.
National Public Health Effort
The control of asthma requires a national response, and the efforts of a number of agencies have been important to local through nation-wide public health. The Centers for Disease Control and Prevention (CDC) has instituted surveillance in most US states and maintains a database of prevalence and incidence statistics and associated demographic factors. The Behavioral Risk Factors Survey of the CDC includes a number of asthma-related items, and data are compiled periodically to describe behaviors associated with prevention and management of the disease.
Most state health authorities have risen to the asthma challenge. Many have initiated surveillance in addition to those they conduct in concert with the CDC. Further, many state health departments have engaged in efforts to coordinate and assist asthma awareness and intervention programs, as well as to enhance service delivery. In many states, these efforts have been carried out in collaboration with asthma coalitions.
The National Heart, Lung and Blood Institute has been at the forefront for national asthma control activities. It not only sponsors research into respiratory disease, but is responsible for the National Asthma Education and Prevention Program (NAEPP). NAEPP comprises all the major national organizations with interest in asthma (see Table 20.1 for a list). These organizations through the NAEPP undertake information and education activities targeted at people with asthma and their families, as well as clinicians and other health care providers. The Science Base Committee of NAEPP has generated the National Guidelines for Diagnosis and Treatment of Asthma (NAEPP 2007), the gold standard for clinical care. The NAEPP has also promulgated a Guidelines Implementation Plan (NAEPP 2008) describing strategies to ensure adherence to NAEPP clinical recommendations. The NAEPP has also issued other important guidelines: for example, concerning asthma in pregnancy (NAEPP 2004) and, in concert with the American Academy of Pediatrics, asthma in childhood (NAEPP 2007).
National voluntary organizations also work toward asthma control through providing information, education, and supporting research. The American Lung Association is perhaps the most well known and works through approximately 50 local and state affiliates and chapters. The Asthma and Allergy Foundation is another major provider of asthma information and services.
The Role of Policy in Asthma Control
A number of conferences, workshops, and studies have delved into the question of needed public health-related policies. One fairly comprehensive report is an investigation using a nominal group process involving asthma experts conducted by the Rand corporation (Lara et al. 2002) and resulting in a policy action blueprint. This report posited that national public health efforts are essential to turning around the discouraging data regarding asthma morbidity, mortality, and disparities across population groups. The study advisors conceived of “Asthma Friendly Communities” where proven services and programs were evident and available for all those needing assistance. A number of blueprint recommendations attempted to get at the underlying causes of negative asthma outcomes for the poor or otherwise disadvantaged. Advisors called for financing for universally available primary care, self management education and case management in childhood asthma. They believed expanded coverage and improved benefits were vital to reach and help the underserved. They posited that a strengthened public health infrastructure is necessary to achieve asthma friendly communities, that is, a system that provides resources for schools, public education campaigns, and a fully national surveillance system. They included a call for a national agenda for asthma prevention research.
The specific elements of the Blueprint for Policy Action paper are presented in Table 20.1. Although these recommendations focus on pediatric asthma, the proposals are generalizable to asthma in all age groups. That being said, other areas, e.g. policy related to environmental conditions, work settings, research regarding asthma’s interaction with obesity, sex and gender role, race and ethnicity, and the implications for management deserve policy attention.
These important observations notwithstanding, a number of problems and issues precede the formulation of sound asthma-related local, state, and national public health policy. One is the lack of standardization of approaches to asthma therapy and service delivery obvious across the country, as well as a lack of conclusive evidence about the effectiveness of many of the clinical approaches utilized (Buxton et al. 2004; Paltiel et al. 2001; Silber et al. 2003). One of the most influential efforts to address this problem is the Guidelines for the Diagnosis and Treatment of Asthma of the National Asthma Education and Prevention Programs of the National Heart, Lung, and Blood Institute. These guidelines draw on the best evidence and collective judgment in the asthma field. The newest guidelines [2007] incorporate evidence and expert opinion to recommend clinical practice to enhance disease control. Nonetheless, studies have shown that in general and specifically in asthma, use of guidelines is not as robust as we might wish. Particularly in low-income communities, care has been shown to fall below NAEPP standards (Clark et al. 2002; Halm et al. 2005) In considering the problem of use of guidelines for respiratory disease, a distinguished group of experts called for exploration of more effective ways to communicate key asthma information both to clinicians and patients and promote appropriate management of the disease (Boulet et al. 2006).
Another challenge for policy making is the ongoing debate about the role of nonclinical factors in asthma exacerbations e.g. social factors, income (Brown et al. 2004; Kramer et al. 2006; Rogge and Combs-Orme 2003), the rights of asthma sufferers etc. (Jones and Wheeler 2004; Joseph et al. 2006).
Further, there are looming questions regarding conventional wisdom in asthma, that is, assumptions that guide policy and practice that have not been proven. For example, as noted previously, a number of environmental studies show it is possible to reduce environmental triggers to asthma in the home (Martin et al. 2006), however, rarely have changes in health status been clearly documented from such modifications (Kattan et al. 1997; Kercsmar et al. 2006). Although a number of interventions have attempted to ensure that high risk children see a primary care physician after an asthma emergency, subsequent change in the child’s health status has not been examined and at least one study says that such follow-up does not change outcomes for patients (likely because the PCP continues to do the same thing that did not work in the first place) (Cabana et al. 2003). A number of studies have shown that community health workers can be trained and deployed to extend clinical care to the disadvantaged asthma patients, but changes in health status for individuals reached by these workers have not been extensively documented (Krieger et al. 2006). As discussed earlier, we do not know if more severe asthma is a result of obesity and requires special therapies, although we do know that overweight individuals have more asthma-related management problems than those of normal weight (Clark et al. 2003). Further, we are still in the dark regarding the onset of asthma and, therefore, its prevention or cure. For example, Marks et al. (2006) tried allergen avoidance and diet modification in newborns over five years to see if these interventions eliminated or reduced the effects of asthma, wheeze, eczema, or atopy. No differences were observed. The gaps in our conventional wisdom about asthma are many and wide. Some actually may be deterring control and are not wise choices at all. Some may be worthy of continuing. Only data can tell.
Conclusion
Reflecting on the example problems and solutions described in this chapter leads one to a few conclusions. If we are serious about controlling asthma as a public health problem, the effects of asthma on the society and the effects of the society on asthma, we need to think differently about our fundamental approach. Several things come to mind: (1) One is to recognize that in asthma there are interactions among environmental, social, behavioral, neural, endocrine, and immune processes that produce disease and affect interventions (Wright et al. 2004a). This suggests that new models for research are needed that can describe and explicate these interactions. (2) Another is to advocate for intervention research that illuminates how to build capacity across the circles of influence of the individual managing the condition. We need to keep that person in the center of our efforts and emphasize that he or she is the primary manager (not act as if clinicians or health faculties are). We must see health professionals and health systems as crucial advisors and facilitators who direct all their actions to one end: enabling effective management efforts of the patient. Similarly, families, communities, and policy makers – all must be recognized as enablers of good management and encouraged to do their part. (3) We need to explore conventional wisdom in asthma to discover if our assumptions about how to control it are sound ones. In short, we need to explore not only what we do not know but also what we think we know but have not examined closely. (4) The means to widely apply what we do know about asthma control and effective interventions must be found. In other words, replication of promising models and dissemination research are requisite for positive change. (5) The societal attention span (reflected in media, policy, practice) is short and many health problems vie for the spotlight. Although currently we know more about treating asthma than we have ever known, we are not seeing dramatic downward changes in data that indicate the high level of burden of the disease. A concerted voice and continuous effort are needed to remind patients, the clinical community, politicians, and policymakers how serious and costly asthma is and what they can do to help.
References
American Diabetes Association (2008) Economic costs of diabetes in the U.S. in 2007. Diabetes Care 31:1–20
Ampon RD, Williamson M, Correll PK, Marks GB (2005) Impact of asthma on self-reported health status and quality of life: a population based study of Australians aged 18–64. Thorax 60:735–739
Ayanian JZ, Weissman JS, Schneider EC, Ginsburg JA, Zaslavsky AM (2000) Unmet health needs of uninsured adults in the United States. J Am Med Assoc 284(16):2061–2069
Becker G (2001) Effects of being uninsured on ethnic minorities’ management of illness. West J Med 175(1):19–23
Boulet L, Becker A, Bowie D, McIvor A, Hernandez P, Rouleau M et al (2006) Implementing practice guidelines: a workshop on guidelines dissemination and implementation with a focus on asthma and COPD. Can Respir J 13(Suppl A):5–47
Boychuck RB, DeMesa CJ, Kiyabu KM, Yamamoto F, Yamamoto LG, Sanderson R et al (2006) Change in approach and delivery of medical care in children with asthma: results from a multicenter emergency department educational asthma management program. Pediatrics 117(4):S145–S151
Brown P, Mayer M, Zavestoski S, Luebke T, Mandelbaum J, McCormick S (2004) Clearing the air and breathing freely: the health politics of air pollution and asthma. Int J Health Serv 34(1):39–63
Butterfoss FD, Gilmore LA, Krieger JW, Lachance LL, Lara M, Meurer JR et al (2006) From formation to action: how allies against asthma coalitions are getting the job done. Health Promot Pract 7(2 Suppl):34s–43s
Buxton MJ, Sullivan SD, Andersson LF, Lamm CJ, Liljas B, Busse WW et al (2004) Country-specific cost-effectiveness of early intervention with budesonide in mild asthma. Eur Respir J 24(4):568–574
Byrne J, Schreiber ME, Nguyen TQ (2006) Community hospital-school partnership to treat asthma episodes at school and improve management. J Sch Health 76(6):336–339
Cabana MD, Bruckman D, Bratton SL, Kemper AR, Clark NM (2003) Association between outpatient follow-up and pediatric emergency department asthma visits. J Asthma 40(7):741–749
Cabana MD, Slish KK, Evans D, Mellins RB, Brown R, Lin X et al (2006) Impact of physician asthma care education on patient outcomes. Pediatrics 117(6):2149–2157
Cabana MD, Slish KK, Lewis TC, Brown R, Nan B, Lin X et al (2004) Parental management of asthma triggers within a child’s environment. J Allergy Clin Immunol 114:352–357
Carroll KN, Griffin MR, Gebretsadik T, Shintani A, Mitchel E, Hatert TV (2005) Racial differences in asthma morbidity during pregnancy. Obstet Gynecol 106:66–72
Centers for Disease Control (2002) Surveillance for asthma – United States, 1980–1999. MMWR Surveill Summ 51:1–13
Centers for Disease Control (2003) Public Health and Aging: Trends in Aging -- United States and Worldwide. In: MMWR (ed) MMWR Weekly (February 14, 2003 edn, Vol. 52). CDC, Atlanta, pp 101–106
Chinn S, Downs SH, Anto JM, Gerbase MW, Leynaert B, deMarco R et al (2006) Incidence of asthma and net change in symptoms in relation to changes in obesity. Eur Respir J 28:763–771
Clark NM, Brown R, Joseph CL, Anderson EW, Liu M, Valerio M (2004) Effects of a comprehensive school-based asthma program on symptoms, parent management, grades, and absenteeism. Chest 125(5):1674–1679
Clark NM, Brown R, Joseph CL, Anderson EW, Liu M, Valerio M et al (2002) Issues in identifying asthma and estimating prevalence in an urban school population. J Clin Epidemiol 55(9):870–881
Clark NM, Doctor LJ, Friedman AR, Lachance LL, Houle CR, Geng X et al (2006) Community Coalitions to Control Chronic Disease: Allies Against Asthma as a Model and Case Study. Health Promot Pract 7(Suppl):44s–55s
Clark NM, Doctor LJ, Gilmore L, Kelly C, Krieger J et al (2009) Policy and system change and community coalitions outcomes from allies against asthma. Manuscript submitted for publication
Clark NM, Gong M, Schork MA, Evans D, Roloff D, Hurwitz M et al (1998) Impact of education for physicians on patient outcomes. Pediatrics 101(5):831–836
Clark NM, Gong M, Schork MA, Kaciroti N, Evans D, Roloff D et al (2000) Long-term effects of asthma education for physicians on patient satisfaction and use of health services. Eur Respir J 16:15–21
Clark NM, Gong M, Yu J, Lin X, Valerio M, Bria W et al (2003) Impact of overweight in women with asthma. European Respiratory Society Annual Congress, Vienna
Clark NM, Lachance LL, Friedman, AR, Stoll SC, Awad DA (in press) Characteristics of successful asthma programs. Public Health Rep
Cloutier MM, Hall CB, Wakefield DB, Bailit H (2005) Use of asthma guidelines by primary care providers to reduce hospitalizations and emergency department visits in poor, minority, urban children. J Pediatr 146(5):591–597
Cortes T, Lee A, Boal J, Mion L, Butler A (2004) Using focus groups to identify asthma care and education issues for elderly urban-dwelling minority individuals. Appl Nurs Res 17(3):207–212
Cunningham J, Dockery DW, Speizer FE (1996) Race, asthma, and persistent wheeze in Philadelphia schoolchildren. Am J Public Health 86(10):1406–1409
Evans D, Clark NM, Feldman CH, Rips J, Kaplan D, Levison MJ et al (1987) A school health education program for children with asthma aged 8–11 years. Health Educ Q 14(3):267–279
Finkelstein JA, Brown RW, Schneider LC, Weiss ST, Quintana JM, Goldmann DA et al (1995) Quality of care for preschool children with asthma: the role of social factors and practice setting. Pediatrics 95(3):389–394
Finnvold JE (2006) Access to specialized health care for asthmatic children in Norway: the significance of parents’ educational background and social network. Soc Sci Med 63(5):1316–1327
Flaherman V, Rutherford GW (2006) A meta-analysis of the effect of high weight on asthma. Arch Dis Child 91:334–339
Ford E (2005) The epidemiology of obesity and asthma. J Allergy Clin Immunol 115(5):897–909
Gibson P, Coughlan J, Wilson A, Abramson M, Bauman A, Hensley M et al (2000) Self-management education and regular practitioner review for adults with asthma . Cochrane Database Syst Rev. 2000;(2):CD001117
Goldfarb N, Weston C, Hartmann C, Sikirica M, Crawford A, He H et al (2004) Impact of appropriate pharmaceutical therapy for chronic conditions on direct medical costs and workplace productivity: a review of the literature. Dis Manag 7(1):61–75
Goldman L, Falk H, Landrigan PJ, Balk SJ, Reigart JR, Etzel RA (2004) Environmental pediatrics and its impact on government health policy. Pediatrics 113(4):1146–1157
Grant EN, Lyttle CS, Weiss KB (2000) The relation of socioeconomic factors and racial/ethnic differences in US asthma mortality. Am J Public Health 90(12):1923–1925
Gupta RS, Carriòn-Carire V, Weisse KB (2006) The widening black/white gap in asthma hospitalizations and mortality. J Allergy Clin Immunol 117(2):351–358
Halm EA, Wisnivesky JP, Leventhal H (2005) Quality and access to care among a cohort of inner city adults with asthma. Chest 128:1943–1950
Hendler I, Schatz M, Momirova V, Wise R, Landon M, Mabie W et al (2006) Association of obesity with pulmonary and nonpulmonary complications of pregancy in asthmatic women. Obstet Gynecol 108(1):77–82
Hindi-Alexander MC, Cropp GJ (1984) Evaluation of a family asthma program. J Allergy Clin Immunol 74(4 pt 1):505–510
Institute of Medicine (2000) Clearing the air: asthma and indoor air exposures. Institute of Medicine, Washington, DC
Institute of Medicine (2004) Damp indoor spaces and health. Washington, DC, National Academies Press
Johnstone E, Knight J, Gilham K, Campbell E, Nicholas C, Wiggers J (2006) System-wide adoption of health promotion practices by schools: evaluation of a telephone and mail-based dissemination strategy in Australia. Health Promot Int 21(3):209–218
Jones SE, Wheeler L (2004) Asthma inhalers in schools: rights of students with asthma to a free appropriate education. Am J Public Health 94(7):1102–1108
Joseph CL, Williams LK, Ownby DR, Saltzgaber J, Johnson CC (2006) Applying epidemiological concepts of primary, secondary, and tertiary prevention to the elimination of racial disparities in asthma. J Allergy Clin Immunol 117(2):233–240
Kaplan G, Pamuk ER, Lynch JW, Cohen RD, Balfour JL (1996) Inequality in income and mortality in the United States: analysis of mortality and potential pathways. Br Med J 312:999–1003
Kattan M, Mitchell H, Eggleston P, Gergen PJ, Crain E, Redline S et al (1997) Characteristics of inner-city children with asthma: the National Cooperative Inner-City Asthma Study. Pediatr Pulmonol 24(4):253–262
Kercsmar CM, Dearborn DG, Schluchter M, Xue L, Kirchner HL, Sobolewski J et al (2006) Reduction in asthma morbidity in children as a result of home remediation aimed at moisture sources. Environ Health Perspect 114(8):1564–1580
Kramer CB, Cullen AC, Faustman EM (2006) Policy implications of genetic information on regulation under the Clean Air Act: the case of particulate matter and asthmatics. Environ Health Perspect 114(3):313–319
Krieger JW, Bourcie E, Lara M, Peterson JW, Ronsenthal MP, Taylor-Fishwick JC et al (2006) Integrating asthma prevention and control: the roles of the coalition. Health Promot Pract 7(2 Suppl):127S–138S
Krishnan V, Diette GB, Rand CS, Bilderback AL, Merriman B, Hansel NN et al (2006) Mortality in patients hospitalized for asthma exacerbations in the United States. Am J Respir Crit Care Med 174:633–638
Kubzansky LD, Wright RJ, Cohen S, Weiss ST, Rosner B, Sparrow D (2002) Breathing easy: a prospective study of optimism and pulmonary function in the normative aging study. Ann Behav Med 24(4):345–353
Kullowatz A, Kanniess F, Dahme B, Magnussen H, Ritz T (2006) Association of depression and anxiety with health care use and quality of life in asthma patients. Respir Med 2007 Mar:101(3):638–44. Epub 2006 Aug 7.
Lara M, Akinbami L, Flores G, Morgenstern H (2006) Heterogeneity of childhood asthma among Hispanic children: Puerto Rican children bear a disproportionate burden. Pediatrics 117(1):43–53
Lara M, Rosenbaum S, Rachelefsky G, Nicholas W, Morton SC, Emont S et al (2002) Improving childhood asthma outcomes in the United States: a blueprint for policy action. Pediatrics 109(5):919–930
Levy JI, Brugge D, Peters JL, Clougherty JE, Saddler SS (2006) A community-based participatory research study of multifaceted in-home environmental interventions for pediatric asthmatics in public housing. Soc Sci Med 63:2191–2203
Lewis T, Robins TG, Dvonch JT, Keeler GJ, Yip FY, Mentz GB et al (2005) Air pollution-associated changes in lung function among asthmatic children in Detroit. Environ Health Perspect 113(8):1068–1075
Mancuso CA, Rincon M (2006) Impact of health literacy on longitudinal asthma outcomes. J Gen Intern Med 21(8):813
Mancuso P, Canetti CA, Gottschalk A, Tithof PK, Peters-Golden M (2004) Leptin enhances macrophage leukotriene synthesis by augmenting arachidonic acid release and cPLA2 v protein expression. Am J Physiol Lung Cell Mol Physiol 287:L497–L502
Mannino DM, Homa DM, Akinbami L, Moorman JE, Gwynn C, Redd SC (2002) Surveillance for asthma – United States, 1980–1999. MMWR 51:1–13
Marks GB, Mihrshahi S, Kemp AS, Tovey ER, Webb K, Almqvist C et al (2006) Prevention of asthma during the first 5 years of life: a randomized controlled trial. J Allergy Clin Immunol 118(1):53–60
Martin MA, Hernandez O, Naureckas E, Lantos J (2006) Reducing home triggers for asthma: the Latino community health worker approach. J Asthma 43(5):369–374
McFadden ER, Warren EL (1997) Observations on asthma mortality. Ann Intern Med 127(2):142–147
Melnyk BM, Alpert-Gillis L, Feinstein NF, Crean HF, Johnson J, Fairbanks E et al (2004) Creating opportunities for parent empowerment: program effects on the mental health/coping outcomes of critically ill young children and their mothers. Pediatrics 113(6):e597–607
Nathan JA, Pearce L, Field C, Dotesio-Eyres N, Sharples LD, Cafferty F et al (2006) A randomized controlled trial of follow-up of patients discharged from the hospital following acute asthma. Chest 130:51–57
National Asthma Education and Prevention Program (2004) Managing asthma during pregnancy: recommendations for pharmacologic treatment. Retrieved October, 2006, from www.nhlbi.nih.gov/health/prof/lung/asthma/astpreg/astpreg_full.pdf
National Asthma Education and Prevention Program (2007) Guidelines for the diagnosis and management of asthma (No. 07-4051). National Heart, Lung and Blood Institute, Bethesda, Maryland
National Asthma Education and Prevention Program (2008) Expert panel report 3 – guidelines for the diagnosis and management of asthma: partners putting guidelines into action (No. 09-6147). National Heart, Lung and Blood Institute
Nicholas EA, Dwyer M, Murphy A, Taylor-Fishwick JC, Cohn JH, Kelly CS et al (2006) Coalition-based approaches for addressing environmental issues in childhood asthma. Health Promot Pract 7(2 Suppl):108S–116S
Opolski M, Wilson I (2005) Asthma and depression: a pragmatic review of the literature and recommendations for future research. Clin Pract Epidemol Ment Health 1:18
Paltiel AD, Fuhlbrigge AL, Kitch BT, Liljas B, Weiss ST, Neumann PJ et al (2001) Cost-effectiveness of inhaled corticosteroids in adults with mild-to-moderate asthma; results from the asthma policy model. J Allergy Clin Immunol 108(1):39–46
Perez M, Findley SE, Mejia M, Martinez J (2006) The impact of community health worker training and programs in New York City. J Health Care Poor Underserved 17(1 Suppl):26–43
Radeos MS, Leak LV, Lugo BP, Hanrahan JP, Clark S, Camargo CA (2001) Risk factors for lack of asthma self management knowledge among ED patients not on inhaled steroids. Am J Emerg Med 19(4):253–259
Rogge ME, Combs-Orme T (2003) Protecting children from chemical exposure: social work and US social welfare policy. Soc Work 48(4):439–450
Schatz M, Clark S, Camargo CA (2006) Sex differences in the presentation and course of asthma hospitalizations. Chest 129(1):50–55
Shah S, Peat JK, Mazurski EJ, Wang H, Sindhusake D, Bruce C et al (2001) Effect of peer led programme for asthma education in adolescents: cluster randomised controlled trial. Br Med J 322:583–585
Shalowitz MU, Mijanovich T, Berry CA, Cark-Kauffman E, Quinn KA, Perez EL (2006) Context matters: a community-based study of maternal mental health, life stressors, social support, and children’s asthma. Pediatrics 117(5):e940–e948
Shore SA, Schwartzman IN, Mellema MS, Flynt L, Imrich A, Johnston RA (2005) Effect of leptin on allergic airway responses in mice. J Allergy Clin Immunol 115(1):103–109
Silber JH, Rosenbaum PR, Even-Shoshan O, Shabbout M, Zhang X, Bradlow ET et al (2003) Length of stay, conditional length of stay, and prolonged stay in pediatric asthma. Health Serv Res 38(3):867–886
Sockrider MM, Abramson S, Brooks E, Caviness AC, Pilney S, Koerner C et al (2006) Delivering tailored asthma family education in a pediatric emergency department setting: a pilot study. Pediatrics 117(4):S135–S144
Sondik EJ (2008, May) Focus area 24 respiratory diseases progress review. Presented at the National Center for Health Statistics, Hyattsville, MD
Splett PL, Erickson CD, Belseth SB, Jensen C (2006) Evaluation and sustainability of the healthy learners asthma initiative. J Sch Health 76(6):276–282
Sudano JJ, Baker DW (2003) Intermittent lack of health insurance coverage and use of preventive services. Am J Public Health 93(1):130–137
Sullivan SD, Lee TA, Blough DK, Finkelstein JA, Lozano P, Inui TS et al (2005) A multisite randomized trial of the effects of physician education and organizational change in chronic asthma care: cost-effectiveness analysis of the Pediatric Asthma Care Patient Outcomes Research Team II (PAC-PORT II). Arch Pediatr Adolesc Med 159(5):428–434
Ungar WJ, Macdonald T, Cousins M (2005) Better breathing or better living? A qualitative analysis of the impact of asthma medication acquisition on standard of living in low-income families of children with asthma. J Pediatr Health Care 19(6):354–362
Volmer T (2001) The socio-economics of asthma. Pulm Pharmacol Ther 14(1):55–60
Wandersman A (2003) Community science: bridging the gap between science and practice with community-centered models. Am J Community Psychol 31(3–4):227–242
Wandersman A, Valois R, Ochs L, Cruz DSdl, Adkins E, Goodman RM (1996) Toward a social ecology of community coalitions. Am J Health Promot 10(4):299–307
Weil CM, Wade SL, Bauman LJ, Lynn H, Mitchell H, Lavigne J (1999) The relationship between pyschosocial factors and asthma morbidity in inner-city children with asthma. Pediatrics 104(6):1274–1280
Weiss KB, Gergen PJ, Hodgson TA (1992) An economic evaluation of asthma in the United States. N Eng J Med 326(13):862–866
Weitzman JB, Kanarek NF, Smialek JE (1998) Medical examiner asthma death autopsies: a distinct subgroup of asthma deaths with implications for public health preventive strategies. Arch Pathol Lab Med 122(8):691–699
Wilson SR, Latini D, Starr NJ, Fish L, Loes LM, Page A et al (1996) Education of parents of infants and very young children with asthma: a developmental evaluation of the Wee Wheezers Program. J Asthma 33(4):239–254
Wolf FM, Guevara JP, Grum CM, Clark NM (2003) Educational interventions for asthma in children. Cochrane Database Syst Rev 2003;(1): CD000326.
Wong EY, Gohlke J, Griffith WC, Farrow S, Faustman EM (2004) Assessing the health benefits of air pollution reduction for children. Environ Health Perspect 112(2):226–232
Wright RJ, Cohen RT, Cohen S (2005) The impact of stress on the development and expression of atopy. Curr Opin Allergy Clin Immunol 2005 Feb; 5(1):23–29
Wright RJ, Cohen S, Carey V, Weiss ST, Gold DR (2002) Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Respir Crit Care Med 165(3):358–365
Wright RJ, Finn P, Contreras JP, Cohen S, Wright RO, Staudenmayer J et al (2004a) Chronic caregiver stress and IgE expression, allergen induced proliferation, and cytokine profiles in a birth cohort predisposed to atopy. J Allergy Clin Immunol 113(6):1051–1057
Wright RJ, Mitchell H, Visness CM, Cohen S, Stout J, Evans R et al (2004b) Community violence and asthma morbidity: the inner-city asthma study. Am J Public Health 94(4):625–632
Wright RJ, Steinbach SF (2001) Violence: an unrecognized environmental exposure that may contribute to greater asthma morbidity in high risk inner city populations. Environ Health Perspect 109(10):1085–1089
Zorc JJ, Scarfone RJ, Li Y, Hong T, Harmelin M, Grunstein L et al (2003) Scheduled follow-up after a pediatric emergency department visit for asthma: a randomized trial. Pediatrics 111(3):495–502
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Clark, N.M. (2010). Asthma, Public Health, and Policy. In: Harver, A., Kotses, H. (eds) Asthma, Health and Society. Springer, Boston, MA. https://doi.org/10.1007/978-0-387-78285-0_20
Download citation
DOI: https://doi.org/10.1007/978-0-387-78285-0_20
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-0-387-78284-3
Online ISBN: 978-0-387-78285-0
eBook Packages: MedicineMedicine (R0)