
Abstract
While clinical guidelines clearly define mechanisms for asthma diagnosis based upon history, lung function testing, symptoms, and physical examination, surveillance for asthma is much less straightforward. Epidemiologists have long debated the best means of assessing the scope and burden of asthma, seeking to reduce the potential for confounding introduced by differential means of diagnosis and even slight differences in surveillance questions, both of which can bias surveillance results such that we over- or undercount cases. This chapter will provide an overview of asthma epidemiology in the USA and internationally, as well as review of the data and findings from the major surveillance systems, a discussion of a networked approach to the science and evaluation of therapeutic treatments using the exemplar of the Inner-City Asthma Network, and assessment of public health implications.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction to Asthma Epidemiology
While clinical guidelines clearly define mechanisms for asthma diagnosis based upon history, lung function testing, symptoms, and physical examination, surveillance for asthma is much less straightforward. Given that asthma is a non-reportable disease in the USA, we rely upon a surprisingly complex, multifaceted system that differs from agency to agency and often from state to state. This is even more problematic for global surveillance where diagnostic practices may differ even further among countries and cultures depending upon patients’ access to medical care and an adequate, well-trained health professions workforce. Epidemiologists have thus long debated the best means of assessing the scope and burden of asthma, seeking to reduce the potential for confounding introduced by differential means of diagnosis and even slight differences in surveillance questions, both of which can bias surveillance results such that we over- or undercount cases. Regardless, however, there is little disagreement that even with data from such a wide variety of different systems, asthma has increased markedly since the 1970s, despite a lack of consensus regarding causes for new onset disease. Virtually all surveillance systems and programs, both nationally and internationally, indicate an increasing burden of disease in terms of both prevalence (the proportion of existing cases in a population at a given time point) and incidence (onset of new cases within a specified period of time).
This chapter will provide an overview of asthma epidemiology in the USA and internationally. From a translational standpoint that finds the importance of the data in the use to which it is put, it includes a review of the data and findings from the major surveillance systems, a discussion of a networked approach to the science and evaluation of therapeutic treatments using the exemplar of the Inner-City Asthma Network, and assessment of public health implications. If one subscribes to the view that most cases of asthma are treatable and controllable, then it serves to follow that through an integrated approach to treatment and education, even greater reductions in morbidity and mortality can be achieved, especially in Emergency Department visits and unnecessary hospitalizations.
2 Sources of Data and Methods of Surveillance
2.1 USA
The United States Centers for Disease Control and Prevention carry out a wide variety of surveillance activities to determine the scope of asthma and the burden of disease, including prevalence of asthma, number of emergency department visits with a primary diagnosis of asthma, and both hospitalizations and deaths due to asthma. They also track other more indirect effects of asthma morbidity, including the limitations on activities of daily living, the number of days of work and/or school lost due to asthma, the use of medications including both rescue and control drugs, the proportion of patients who receive asthma self-management education, and the number of physician visits. Much data is collected through administration of the National Center for Health Statistics (NCHS) surveys and the Vital Statistics System. State-level data are provided from administration of the Behavioral Risk Factor Surveillance System (BRFSS) and its periodic Asthma Call-back Survey (ACBS). While many other sources of data are readily available, the following CDC surveys (CDC 2012) largely drive development of public health programs and development of policies and guidelines, including:
-
BRFSS: a random-digit-dialing telephone surveillance program designed to monitor the prevalence of adult asthma, morbidity, and mortality.
-
ACBS: a comprehensive asthma survey carried out with BRFSS survey respondents reporting a previous diagnosis of asthma.
-
National Health Interview Survey: a multistage probability sample survey carried out via interview with representative US households that includes questions related to both health and demographic information.
-
The National Ambulatory Medical Care Survey: a survey conducted with non-federally employed office-based physicians to provide information on provision and use of ambulatory medical care services.
-
The National Hospital Ambulatory Medical Care Survey: a survey conducted with Emergency Departments (ED) and outpatient departments of noninstitutional general and short-stay hospitals to provide information on utilization and provision of ambulatory care services in ED and outpatient clinics.
-
The National Hospital Discharge Survey (NHDS) and The National Hospital Care Survey (NHCS): The NHDS, a national probability survey, was carried out yearly from 1965 to 2010 to collect inpatient data related to hospitalization stays for patients who had been discharged from non-federal short-stay US hospitals. The NHCS integrated the NHDS surveillance methodology with new survey questions that expanded the study to include ED, outpatient clinic, and ambulatory surgery center data collected as a part of the National Hospital Ambulatory Medical Care Survey. Combining data from these two surveys, along with inclusion of personal identifiers, now makes it possible to link findings to both the National Death Index and Medicaid and Medicare data, an important step in allowing a more comprehensive analysis of patient morbidity and trends in patient outcomes related to provision of care in both inpatient and outpatient settings.
-
The National Environmental Public Health Tracking Network: a system of integrated health, exposure, and hazard information and data from a variety of national, state, and city sources.
2.2 Global Surveillance
Historically, the two largest global studies of asthma are the European Community Respiratory Health Survey (ECRHS), which involved surveillance of adults and the International Study of Asthma and Allergies in Children (ISAAC). Phase I of the ECRHS was initiated in the 1980s in response to the increasing concern related to a global increase in asthma prevalence. This was an important initiative, particularly since it was the first study of its kind to carry out a multi-country study of allergic disease and asthma using a standardized protocol. This two-stage study, carried out primarily in Europe, enrolled approximately 140,000 participants in a survey, with 26,000 enrolled in a clinical component. The purpose of the study was to investigate variation in the prevalence of asthma and asthma-like disorders, to better assess factors associated with risk for asthma, and describe variations in therapeutic asthma treatments in European countries. A follow-up study was carried out from 1998 to 2002, with a second follow-up now in the planning stages. The ECRHS was and continues to be important in providing data related to asthma causation. The first phase provided some of the first epidemiologic data identifying the importance of the effect of environmental exposures on asthma (ECRHS 2012).
Phase I of the ISAAC, rolled out in 1991, focused on investigating asthma, allergic rhinitis, and eczema. Like the ECRHS, a major emphasis was to carry out a large epidemiological investigation in multiple countries and study sites utilizing a uniform—and for the time period, unique—protocol. Phase I of the study utilized standard, age-appropriate questionnaires, combined with a videotape that provided children with illustrative examples of asthma signs and symptoms, in an effort to reduce confounding associated with lack of understanding of the disease and its manifestations. Phase II was built upon the knowledge gleaned in Phase I, including more in-depth studies in a smaller number of centers. Phase III was a follow-up of Phase I that investigated childhood asthma, rhino-conjunctivitis, and eczema worldwide. It also provided us with a world map of asthma prevalence. Phase IV, the current study, includes developing and expanding the ISAAC website, largely to provide resources for investigators and practitioners from low- and middle-income countries. An important addition is the inclusion of asthma management plans and other resources that have been documented as improving patient outcomes. Since initiation in 1991, the ISAAC has been carried out in 306 centers in 105 countries with nearly two million children (ISAAC 2012).
The 2004 publication of the Global Burden of Asthma (Masoli et al. 2004) combined data from the Phase I ISAAC and the ECRHS in an attempt to more comprehensively generate global estimates of asthma prevalence and disease burden. Prevalence varied tremendously from country to country, from as low as 0.7 % in children in Macau to 18.4 % in Scotland. Of real concern was the sheer number of cases at 300 million, with expected increases in developing countries undergoing rapid urbanization. This report, while important, was nonetheless a compendium of surveillance efforts that utilized different instruments and methodologies, thus limited (To et al. 2012).
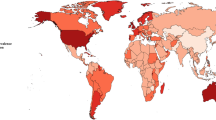
To deal with the inconsistencies, in 2002–2003, the World Health Organization (WHO) developed and conducted the World Health Survey (BedirhanÜstün et al. 2003), which used a standardized protocol that would enable collection of data that allowed both between and within country comparisons. As a cross-sectional survey, the WHS was conducted within 70 of the 192 WHO member states, thus comprising the largest multi-country asthma surveillance of adults ever conducted. To et al. utilized this data to estimate and compare both the worldwide and country-specific burden of asthma, utilizing a stratified probability sampling design, where the sampling frame covered 100 % of the country’s eligible adults ≥18 years of age in each of the countries. Of real importance was the effort to directly deal with issues of misdiagnosis and underdiagnosis by including questions related to previous diagnosis (doctor-diagnosed asthma), reported treatment for asthma either with or without a previous diagnosis (clinical asthma), and reported active wheezing/whistling breath in the past 12 months (symptoms of asthma) (To et al. 2012). Figure 2.1 depicts prevalence findings by region utilizing data from this report.

Global asthma prevalence. Data abstracted from Stanojevic S, Moores G, Gershon AS, Bateman ED, Cruz AA, Boulet L-P (2012) Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health 12:204
2.3 Limitations of Surveillance Methods
Although differences in surveillance methodology make it difficult to paint a comprehensive picture of the scope of asthma and the burden of disease, these fairly recent efforts to “marry” data sets and to launch new initiatives to standardize protocols have increased our understanding of national and global trends. Increasing interest is also focused on improving the evaluation of such surveillance systems, which are integral in driving many of our public health outreach efforts, interventions, and policies. In 2001, the CDC developed and published “Updated Guidelines for Evaluating Public Health Surveillance Systems” (CDC 2001), which provides six specific steps to evaluating surveillance programs:
-
1.
Engage stakeholders
-
2.
Describe system
-
3.
Focus evaluation design
-
4.
Gather evidence of system’s performance
-
5.
State conclusions and make recommendations
-
6.
Ensure use of findings and share lessons learned
Of particular importance in gathering evidence of the system’s performance is determining if the program was derived to include simplicity, flexibility, data quality, acceptability, sensitivity, positive predictive value, representativeness, timeliness, and stability. This is problematic for many of the surveillance systems in place, including several of the large-scale studies described. If criteria for a clinical diagnosis of asthma are based upon multiple factors including history, symptoms, genetic predisposition, etc., then asthma surveillance in the form of a cross-sectional questionnaire must be carefully derived to be both reliable and valid. Many use differing means of determining whether the patient has ever had asthma or has current asthma. Few studies include a potential or probable diagnosis of asthma. Thus in the absence of a uniform case definition for asthma, multiple surveillance systems developed to characterize asthma are not only not generalizable to one another but may actually provide conflicting data that cannot easily be interpreted (Petronella and Ellis 2003). This is clearly indicated in the 2002 report of the Global Initiative for Asthma,
Despite hundreds of reports on the prevalence and mortality of asthma in widely differing populations, the lack of precise definitions of asthma makes reliable comparison of reported prevalence from different parts of the world problematic. . . .because no epidemiological definition of asthma is emerging from current data, important components of epidemiological studies for asthma continue to include questionnaires, tests of airway hyper-responsiveness, and documentation of putative etiologic factors including atopic status. (GINA 2002, p. 13)
The NHIS survey, for example, assesses asthma prevalence by use of two questions: “Have you ever been told by a doctor or other health professional that you/your child had asthma?” and “Do you/your child still have asthma?” This was found to be a significant problem in school-based surveillance of childhood asthma which utilized these standard questions but also included diagnostic questions provided by physician asthma specialists. This particular study revealed that respondents who denied having received a previous diagnosis for asthma nonetheless reported morbidity due to asthma, including hospitalizations and ED visits. Among this group, Hispanics appeared to have been overrepresented, suggesting an underreporting of cases (Petronella et al. 2006). Still other surveillance questions for the purpose of identifying asthma cases are often based upon self-reported symptoms of wheezing and frequency of symptoms. Clearly, not all episodes of wheezing are due to asthma, and many patients may present with other symptoms such as a persistent cough in the absence of a cold. It is also well known that surveillance based upon personal recall that is not able to be validated by objective measure introduces the possibility for bias that in turn reduces our confidence in findings from surveillance studies. This potential for error is recognized, and as is demonstrated in the following sections, surveillance systems at the national and international levels are beginning to reassess the way we carry out and evaluate surveillance studies and systems.
3 Prevalence of Asthma: USA
In the past several decades, asthma prevalence has dramatically increased both nationwide and globally, sparking concern over what has been referred to as an “asthma epidemic.” According to a 2012 report published by the CDC utilizing data from the National Health Interview surveys, rates have continued to rise. In 2001, 7.3 % of Americans of all ages (20.3 million persons) had been diagnosed with asthma, compared to 8.2 % (24.6 million persons) in 2009, a 12.3 % increase (Schiller et al. 2012; Zahran et al. 2011). Of these, 17.5 million were over the age of 18, and 7.1 million children ages 0–17 (Akinbami et al. 2012a, b). Prevalence among children was 9.6 % and highest among low-SES (13.5 %) and non-Hispanic black children (17 %). Prevalence among adults (7.0 %) was revealed to be higher in women (9.7 %), and similar to children, among low-SES adults (10.6 %). As might be expected, those without health insurance reported not being able to purchase prescribed asthma medication (40.3 %), and only 58.6 % indicated they were able to afford to see a primary care physician about their asthma. This differs sharply from those with insurance, of whom only 11.5 % reported not being able to afford their medications and 85.6 % reported being able to afford to see a PCP (Zahran et al. 2011).
Significant disparities are observed among minority groups with asthma. More than one in four black adults and one in five Hispanic adults report not being able to afford their prescriptions, while one in four black adults and one in seven Hispanic adults report not being able to afford routine doctor’s visits (CDC, National Asthma Control 2012). In 2007–2009, black Americans were found to be far more likely to die of asthma than whites, and asthma death rates were found to increase with age for both blacks and whites (Gorina 2012). Poverty and race/ethnicity considered together reveal even sharper disparities. While among the poor, non-Hispanic whites (12.5 %) and blacks (12.2 %) have similar prevalence rates, Puerto Rican Hispanics and the multiracial were found to have significantly higher prevalence of disease at 22.4 % and 20.5 %, respectively. Similar trends were reported for the near poor and the nonpoor (Moorman et al. 2011).
Trends revealed increases in asthma across all demographic groups. From 2001 to 2009 childhood asthma increased from 8.7 to 9.6 %. Among adults, prevalence increased from 6.3 % to 7.1 % in males and from 8.3 % to 9.2 % in females. Increases were also found for each ethnic group: whites, up from 7.2 % to 7.8 %; blacks, up from 8.4 % to 10.8 %; and Hispanics, up from 5.8 % to 6.4 %. Significant differences were found for age, gender, and race/ethnicity across the time frame as well. Among non-Hispanic black children, the increase was pronounced, up from 11.4 % to 17.0 %. Increases were also found for non-Hispanic white women (up from 8.9 % to 10.1 %) and non-Hispanic black men (4.7 % vs. 6.4 %) (Zahran et al. 2011).
A separate study evaluating NHIS data from 2005 to 2009 revealed similar results, with significant health disparities among ethnic groups and socioeconomic classes. Adult females were found to have a higher prevalence rate of current asthma (9.3 %) than males (7.0 %); however, the reverse was true for children, with boys at significantly increased risk (11.3 %) compared to girls (7.9 %). Prevalence was found to be highest among the black population (11.1 %) and lowest in the Asian population (5.3 %). While Hispanics had lower prevalence (6.3 %) than other ethnic groups, prevalence was lower in those of Mexican heritage (4.9 %) and significantly higher among Puerto Ricans (16.6 %). A pronounced increase in prevalence was seen by socioeconomic group, with those at 200 % of the poverty rate and above at 7.3 %, those at 100 % but less than 200 % of the poverty rate at 8.5 %, and those below the poverty rate at 11.6 %. Little differences were found between metropolitan dwellers (8.1 %) and non-metropolitan (8.7 %) (Akinbami et al. 2012a, b). Asthma death rates per 1,000 persons revealed 30 % higher rates for females than males, with elevated rates for blacks as well (Akinbami et al. 2012a, b). Asthma was linked to 3,447 deaths (approximately 9/day) in 2007 alone (CDC 2011). It should be noted that ethnic differences in asthma morbidity and mortality have been found to be linked to conditions such as poverty, inner-city environments, poor air quality both indoors and outdoors, and lack of patient education and access to appropriate medical treatment (Asthma and Allergy Foundation of America 2012).
The burden of asthma is significant, both in terms of financial expenses and in lost productivity. Asthma costs increased from $53 billion in 2007 to approximately $56 billion in 2009 (CDC 2011).
According to the Asthma and Allergy Foundation of America (AAFA), every day in the USA, the burden of morbidity associated with asthma is monumental. Over 40,000 people will have an asthma exacerbation, while 36,000 children will miss school and 27,000 adults will miss work due to asthma. Almost 5,000 will visit the ED and 1,200 will be admitted to the hospital for treatment of asthma. Asthma is also the number one cause of school absenteeism in the USA, accounting for more than 13 million missed days of school annually (Asthma and Allergy Foundation of America 2012).
4 Prevalence of Asthma: Global
The prevalence of asthma in different countries throughout the world varies a great deal. Previously, the rates were higher in more developed countries, but the gaps are now closing, given the rise in prevalence in low- and middle-income countries and plateauing in high-income countries. Prevalence has been associated with adoption of a modern, urban lifestyle; however, it is unclear what specific factors are causal in nature. Increased prevalence of asthma is also strongly correlated with increases in allergy, a trend observed over the past 40 years. Globally, approximately 300 million people have asthma, with 250,000 annual deaths attributed to the disease—most of which are preventable. Mortality rates do not appear to be correlated with prevalence but rather are highest in countries where access to appropriate medications is lacking, specifically, controller meds (World Health Organization 2007). Worldwide, as in the USA, asthma accounts for many days of lost productivity in terms of missed school and work days. Disability-adjusted life years attributed to asthma are estimated at 15.3, ranking asthma at 22nd worldwide, similar in impact to other chronic diseases such as diabetes or Alzheimer disease (Masoli et al. 2004). An important risk factor in low- and middle-income countries is smoking and exposure to secondhand smoke. Prevalence of active smoking in adults with asthma in these countries is approximately 25 %, which places them at increased risk of more severe asthma symptoms, decline in lung function, and reduced response to corticosteroid therapy. Based upon existing data, the World Health Organization estimates that by 2025, the number of people with asthma will increase by 100 million, suggesting that marked increases in interventions be accelerated to minimize morbidity and its associated human and financial costs (World Health Organization 2007).
The World Health Survey described previously found great disparities between countries for doctor-diagnosed and clinical asthma as well as reported symptoms. Worldwide, the prevalence of doctor-diagnosed adult asthma in adults was reported as 4.3 % (95 % CI: 4.2; 4.4). Among the 70 countries included in the study, doctor-diagnosed asthma ranged from virtually no asthma in China (0.2 %) to a high of 21.0 % in Australia. Similar results were found for clinical asthma at a worldwide prevalence of 4.5 % (95 % CI: 4.4; 4.6), again with great disparities observed between and among countries, from a low of 1.0 % in Vietnam to 21.5 % in Australia. In rank order, the five participating countries with the highest prevalence of clinical asthma were Australia at 21.5 %, Sweden at 20.2 %, the UK at 18.2 %, the Netherlands at 15.3 %, and Brazil at 13.0 %. Reported asthma symptoms including wheezing or whistling in the chest in the past 12 months were reported as 8.6 % (95 % CI: 8.5; 8.7). The same five countries were found to have the highest prevalence of reported symptoms, albeit in slightly different rank order, with Australia topping the list at 27.4 %, the Netherlands at 22.7 %, the UK and Brazil tied at 22.6 %, and Sweden at 21.6 %. As observed in Fig. 2.1, which utilizes To and colleagues’ data, differences in doctor-diagnosed and clinical asthma are negligible within regions, but with marked differences in prevalence of reported symptoms. While in general the differences in doctor-diagnosed and clinical asthma are not remarkable, the Western Pacific region has the highest prevalence, driven primarily by the high prevalence of asthma in Australia. Similar observations are made for Europe. For those who reported clinical asthma, 49.7 % also reported current symptoms, the highest proportion of whom are from Southeast Asia at 57.9 %. It should be noted, however, that this may be a manifestation of lack of treatment since many indicated that they had never been professionally treated for asthma. This might also be driven by prevalence of smoking since in Europe and Southeast Asia, more than one third of participants indicated being current smokers (To et al. 2012).
5 From Bench to Bedside: Inner-City Asthma Consortium
For decades it has been known that childhood asthma in the inner-city population tends to be increased, if not complicated by a host of factors which range from exposure to environmental pollutants including poor indoor and outdoor air quality and allergens as well as social factors including socioeconomic level, access to health care and prescription medications, appropriate follow-up, and even stress. While it is not clearly understood if mechanisms of asthma in the inner-city population actually differ from asthma in those who do not reside in this environment, by the 1990s it was becoming increasingly clear that this was an important scientific issue, especially as it related to guiding development of evidence-based, effective medical and public health interventions to reduce morbidity and increase quality of life for inner-city children with asthma. To address this, the National Institute of Allergy and Infectious Diseases began what could now be described as one of the first comprehensive translational research programs by establishing the Inner-City Asthma Network Program in 1991, with a goal of improving outcomes for at-risk children in urban environments (Busse 2010).
The first of the networks established was to carry out the National Cooperative Inner-City Asthma Study over the period 1991–1997. This important study was focused on identifying environmental factors that might be causal factors in increased prevalence of childhood asthma and development of intervention strategies based upon these findings. While a number of key factors emerged indicating increased morbidity was associated with access to care and consistent treatment regimens, several environmental observations were made, namely, that sensitization to cockroach, house dust mite, and mouse was associated with increased hospitalizations, wheezing, and emergent medical visits. The second network, the Inner-City Asthma Study, was carried out from 1994 to 2001. This study was to design and conduct multicenter intervention trials to reduce asthma morbidity among inner-city children with asthma. This intervention study consisted of remediating exposure of enrolled children to cockroaches, dust mites, and rodents in addition to other environmental contaminants including pets, secondhand smoke, and molds. Those children in the intervention group were documented to have significant reductions in average maximal number of days with asthma symptoms and reduced number of emergent healthcare use for treatment of asthma; however, increases in lung function were not observed (Busse 2010).
The third NIAID-sponsored network, carried out from 2002 to 2009, was the Inner-City Asthma Consortium I. During this time, the Consortium focused on establishing a birth cohort, completing and publishing the results of the Asthma Control Evaluation trial, and beginning to investigate the use of immunotherapy treatment with cockroach antigen for children with asthma. A second phase of the Consortium work, scheduled to be conducted from 2009 to 2014, will involve investigating the birth cohort for immunologic causes of asthma, as well as designing, developing, and implementing clinical intervention protocols to evaluate immune-based therapies. Importantly, this phase will now be more team based than ever before. With a strong infrastructure for clinical trial management including a statistical and clinical coordinating center and the addition of two basic science projects focusing on epigenetics and microbiota, the networks have and continue to be strong examples of effective translational research (Busse 2010).
6 From Bench to Curbside: Public Health Implications
The experiences of the Inner-City Asthma Networks clearly demonstrate the potential for a translational approach to science to yield important findings that in turn are driving development of effective treatments and protocols for treatments for inner-city children with asthma. The next logical step is to expand efforts to adopt a T4 or public health approach to positively impact both children and adults with asthma.
With appropriate access to health care and medications and avoidance of asthma triggers, most people with asthma can control their disease, thus greatly reducing the number of asthma ED visits and hospitalizations and largely enjoying symptom-free lives. However, in 2008, less than half of people surveyed in the USA reported receiving education on how to avoid triggers. Of those who did report receiving patient education, only 48 % followed prescriptive advice in the absence of a personalized asthma care plan. Public health education programs, geared toward both providers and patients, are needed to increase appropriate patient training and the likelihood that each provider/patient pair collectively creates a personalized action plan. This is an important component of the National Asthma Education and Prevention Program guidelines, which call for assessing and monitoring, patient education, control of factors contributing to asthma severity, and appropriate medical treatment (NHLBI 2007; Zahran et al. 2011). Intervention programs, including patient education programs, have been demonstrated to be successful in reducing both hospitalizations and deaths from the disease (Szefler et al. 2010). One study of 3,748 low-income, primarily minority children in the USA revealed marked decreases in hospitalizations (35 %), a 27 % decrease in asthma-related visits to an ED (World Health Organization 2007; Cloutier et al. 2005). This can and should be an important initiative for public health practitioners and organizations as well as the asthma coalitions that have been formed at both state and national levels.
Additional public health measures should include a more integrated tracking infrastructure for asthma rates and the effectiveness of control measures. Doing so will enable improvement of prevention efforts and thus reduce both morbidity and costs of asthma care. Preventive measures can include improvement in influenza and pneumonia vaccine rates for patients with asthma and promotion of healthy indoor and outdoor air quality through policies geared toward smoke-free environments as well as healthy schools and workplaces (CDC 2011).
7 Summary
While asthma has no cure, with combined efforts in environmental controls to minimize exposure to allergens and irritants, appropriate pharmacologic therapy, and patient and healthcare provider education, the disease can be successfully managed to reduce morbidity, mortality, and financial costs. Efforts must also be increased to ensure access to appropriate health care and effective case management, which are essential to any comprehensive plan to address asthma as a public health problem. A multidisciplinary approach spanning T1 through T4 translational research coupled with such a public health plan is promising and has already demonstrated success in reducing the burden of disease.
References
Akinbami LJ, Moorman JE, Bailey C et al (2012a) Trends in asthma prevalence, health care use, and mortality in the United States, 2001–2010. NCHS data brief, no 94. National Center for Health Statistics, Hyattsville, MD
Akinbami LJ, Moorman JE, Liu, X (2012) Asthma prevalence, health care use, and mortality: United States, 2005–2009. National Health Statistics Reports, no 32. National Center for Health Statistics, Hyattsville, MD
Asthma and Allergy Foundation of America. Asthma facts and figures. Available at http://www.aafa.org/display.cfm?id=8&sub=42. Accessed 15 Sept 12
BedirhanÜstün T, Chatterji S, Mechbal A, Murray C, WHS Collaborating Groups (2003) Health systems performance assessment: debates, methods and empiricism. In: Murray C, Evans D (eds) The world health surveys. Health systems performance assessment: debates, methods and empiricism. World Health Organization, Geneva, pp 797–808
Busse WW (2010) The national institutes of allergy and infectious diseases networks on asthma in inner-city children: an approach to improved care. J Allergy Clin Immunol 125(3):529–537
CDC (2001) Updated guidelines for evaluating public health surveillance systems. http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5013a1.htm. Accessed 28 Aug 12
CDC (2011) Asthma in the US: growing every year. CDC vital signs
CDC (2012) Asthma Surveillance Data. Available at: http://www.cdc.gov/asthma/asthmadata.htm. Accessed 20 Sept 12
CDC, National Asthma Control Program (2012) Asthma’s Impact on the Nation. Available at: http://www.cdc.gov/asthma/impacts_nation/AsthmaFactSheet.pdf. Accessed 20 Sept 12
Cloutier MM et al (2005) Use of asthma guidelines by primary care providers to reduce hospitalizations and emergency department visits in poor, minority, urban children. J Pediatr 146:591–597
European Community Respiratory Health Survey (2012) http://www.ecrhs.org/home.htm. Accessed 20 Sept 2012
GINA (2002) Global strategy for asthma management and prevention. National Institutes of Health, National Heart, Lung, and Blood Institute, Washington, DC
Gorina Y (2012) QuickStats: asthma* death rates, by race and age group—United States, 2007–2009. MMWR 61(17):315
ISAAC (2012) http://isaac.auckland.ac.nz/story/index.html. Accessed 9 Sept 12
Masoli M, Fabian D, Holt S, Beasley R (2004) Global Initiative for Asthma (GINA) Program: The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy 59(5):469–478
Moorman JE, Zahran HS, Truman BI, Molla MT (2011) Division of environmental hazards and health effects, national center for environmental health, CDC. Current asthma prevalence—United States, 2006–2008. MMWR 60(Suppl):84–86
National Heart, Lung, and Blood Institute (2007) Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: US Department of Health and Human Services, National Institutes of Health, NHLBI, 2007. Available at http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf. Accessed 26 Sept 12
Petronella SA, Bricker S, Brown C, Perrotta D, Brooks EG (2006) Addressing asthma in Texas: development of a school-based asthma surveillance program for Texas elementary schools: report of findings. J Sch Health 76(6):227–234
Petronella SA, Ellis KC (2003) Asthma epidemiology, case finding and the role of asthma coalitions. Nurs Clin North Am 38:1–11
Schiller JS, Lucas JW, Ward BW, Peregoy JA (2012) Summary health statistics for U.S. adults: National Health Interview Survey, 2010. National Center for Health Statistics. Vital Health Stat 10(252)
Szefler SJ, Gergen PJ, Mitchell H, Morgan W (2010) Achieving asthma control in the inner city: do the National Institutes of Health Asthma Guidelines really work? J Allergy Clin Immunol 125:521–526
To T, Stanojevic S, Moores G, Gershon AS, Bateman ED, Cruz AA, Boulet L-P (2012) Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health 12:204
World Health Organization (2007) Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach
Zahran HS, Bailey C, Garbe P (2011) Division of environmental hazards and health effects, National Center for Environmental Health, CDC. Vital signs: asthma prevalence, disease characteristics, and self-management education—United States, 2001—2009. MMWR 60(17):547–552
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Croisant, S. (2014). Epidemiology of Asthma: Prevalence and Burden of Disease. In: Brasier, A. (eds) Heterogeneity in Asthma. Advances in Experimental Medicine and Biology, vol 795. Humana Press, Boston, MA. https://doi.org/10.1007/978-1-4614-8603-9_2
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8603-9_2
Published:
Publisher Name: Humana Press, Boston, MA
Print ISBN: 978-1-4614-8602-2
Online ISBN: 978-1-4614-8603-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)