
Abstract
Endometrioid adenocarcinoma is the most common type of endometrial carcinoma (approximately 85 %). By definition, it should resemble, at least focally, proliferative-type endometrium with tubular glands lined by mitotically active columnar cells. Common problems in diagnosis involve its distinction from complex atypical hyperplasia, endocervical adenocarcinoma, serous carcinoma, clear cell carcinoma, and carcinosarcoma. Pure serous carcinomas comprise about 10 % of endometrial cancers. The term “serous” refers to shared characteristics with cells lining the fallopian tube, particularly the tumor cells’ columnar shape, eosinophilic cytoplasm, and tendency to form papillae. However, some serous carcinomas are not papillary but glandular. Importantly, all serous carcinomas exhibit marked nuclear pleomorphism and most demonstrate discrepancies between architectural differentiation and cytologic features. Clear cell carcinoma is the third most common endometrial carcinoma subtype, even though it represents <5 % of all endometrial cancers. Epidemiologic characteristics of patients with clear cell carcinoma are obscure because of this tumor’s rarity, difficulties in diagnostic reproducibility, and accumulating evidence that there are perhaps several subtypes of clear cell carcinoma. Most clear cell carcinomas are composed of cells with clear cytoplasm, but this feature is not restricted to clear cell carcinoma and some clear cell carcinomas contain cells with eosinophilic cytoplasm. Other subtypes of endometrial carcinoma are rare and include squamous, transitional, small cell, undifferentiated/dedifferentiated, and mixed cell types. Among pure mesenchymal tumors of the uterus, leiomyosarcoma is the most common. Microscopic criteria to establish the diagnosis of leiomyosarcoma include the combination of two of the following: cytologic atypia, mitotic activity, and tumor cell necrosis. The threshold for mitotic activity varies for spindled, epithelioid, and myxoid subtypes and a variety of uterine tumors enter in the differential diagnosis, including several variants of leiomyoma (mitotically active, apoplectic, with bizarre nuclei, highly cellular, and hydropic). Low-grade endometrial stromal sarcomas are composed of a homogenous population of small cells with scant cytoplasm resembling proliferative-type endometrial stroma. They show a diffuse growth and infiltrate the uterine wall in a permeative (not destructive) fashion and may have prominent intravascular growth. High-grade endometrial stromal sarcomas do not resemble proliferative stroma, are composed of small rounds cells with brisk mitotic activity and are more aggressive than low-grade tumors. Undifferentiated uterine sarcoma is a very poorly differentiated sarcoma and a diagnosis of exclusion. Carcinosarcomas (malignant mixed müllerian tumors) are biphasic tumors typically composed of highly malignant epithelial and stromal/mesenchymal elements. The histogenesis of these tumors has evolved in recent years and it is now accepted that they either arise from a common pluripotential cell with divergent differentiation or that the sarcomatous component develops from the carcinomatous component by a metaplastic process. Other rare low-grade or clinically aggressive mesenchymal tumors include: (1) low-grade müllerian adenosarcoma (composed of benign-appearing glands and malignant stroma); (2) PEComa, which is composed of epithelioid cells that are typically positive for HMB-45 and may be associated with tuberous sclerosis; and (3) intravenous leiomyomatosis which shows a proliferation of smooth muscle cells within vascular spaces. Even though the latter smooth muscle proliferation is considered benign it can behave aggressively from the clinical point of view.
The original version of this chapter was revised. An erratum to this chapter can be found at DOI 10.1007/7631_2018_4
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
- Endometrioid
- Serous
- Clear cell
- Mixed carcinomas
- Leiomyosarcoma
- Endometrial stromal sarcoma
- Carcinosarcoma
- Low-grade müllerian adenosarcoma
- PEComa
- Intravenous leiomyomatosis
Endometrial Carcinoma and Precursor Lesions
Endometrioid Carcinoma
Endometrioid adenocarcinoma is the most common type of endometrial carcinoma (~85 %). They are considered type I endometrial cancers according to the Bokhman classification [1] because of their epidemiologic association with estrogen excess. Recent work indicates that low-grade endometrioid carcinomas segregate into three subcategories, defined by the number of mutations [2]. Slightly more than one-half of these tumors have low numbers of mutations, mostly restricted to the PTEN/PI3K pathway. These are probably the prototypical type I carcinomas. The remaining low-grade tumors are either microsatellite instability-high, with high numbers of additional mutations, or have mutations in the hotspot region of POLE, leading to enormous numbers of additional mutations. High-grade endometrioid carcinomas segregate not only into these groups, but also into a serous-like group, characterized by extensive DNA insertions and deletions and TP53 mutations. This signifies that some high-grade endometrioid carcinomas are more akin to Bokhman type II than to type I tumors [3]. The current model of estrogen-dependent endometrial carcinogenesis involves progression from hyperplasia with increasing degrees of architectural and cytologic atypia (complex atypical hyperplasia). The development of an invasive neoplasm heralds the emergence of “adenocarcinoma” in this context.
Gross Features
The typical endometrioid adenocarcinoma forms a grossly visible mass that protrudes into the endometrial cavity or causes a diffuse thickening of the endometrial stripe, making it difficult to appreciate a dominant mass. Most tumors arise in the fundus; less commonly, they are found in one of the cornua or in the lower uterine segment, and in some cases, the lesion is centered in an endometrial polyp. Endometrioid adenocarcinomas are usually tan in color and soft in consistency. A good gross description will include an estimate of the depth of invasion into the myometrium as well as involvement of the cervix, uterine serosa, fallopian tubes, or ovaries. The latter three tissues may be involved by direct extension or metastasis.
Histologic Features
Endometrioid adenocarcinomas by definition should resemble, at least focally, proliferative-type endometrium showing tubular glands with smooth luminal surfaces, lined by mitotically active columnar cells (Fig. 1). Based on the degree of glandular differentiation, these tumors are divided into three Federation International Gynecologic Oncologists (FIGO) categories: grade 1 shows ≤5 % of solid non-glandular growth (Figs. 1, 2, 3, and 4), grade 2 is defined by finding between 6 and 50 % of solid non-glandular growth, and grade 3 contains >50 % of solid growth (Fig. 5). The presence of marked cytologic atypia increases the grade by one. Solid components showing overt squamous differentiation are not counted as “solid” for the purposes of tumor grading. Several binary grading schemes have been proposed in an effort to improve interobserver variability in grade assignment, but none is currently in routine use [4,5,6]. Histologic features considered typical of endometrioid carcinoma include keratinizing squamous metaplasia or morular metaplasia (nonkeratinizing). Additional features commonly encountered in both nonneoplastic and neoplastic endometrium include tubal and/or mucinous metaplasia, and secretory/clear cell change (with subnuclear or supranuclear cytoplasmic vacuoles) (Fig. 4).


Endometrioid adenocarcinoma. This typical well-differentiated adenocarcinoma (FIGO grade 1) is composed of well-formed endometrioid glands


Endometrioid adenocarcinoma. This well-differentiated adenocarcinoma (FIGO grade 1) features a highly complex proliferation of fused and branched glands that excludes endometrial stroma


Endometrioid adenocarcinoma, well differentiated (FIGO grade 1), displaying papillary architecture. Note the smooth luminal contours and low-grade cytologic appearance of the tumor cells


Endometrioid adenocarcinoma, well differentiated (FIGO grade 1), displaying secretory changes (cytoplasmic clearing). Note the absence of hobnail change and the low-grade cytologic appearance of the tumor cells


Endometrioid adenocarcinoma, poorly differentiated (FIGO grade 3). In contrast to FIGO grade 1 tumors, these neoplasms are predominantly solid
There are three typical endometrioid growth patterns that on occasion elicit concern for serous carcinoma or carcinosarcoma. Villoglandular architecture is typified by long and thin, finger-like papillae lined by cells with cytologically low-grade nuclei. Endometrioid carcinomas with “small non-villous” papillae demonstrate typical endometrioid cytomorphology along with small papillae [7]. Last, the corded and hyalinized variant of endometrioid carcinoma “CHEC pattern” [8] displays corded growth and hyalinized stroma at a minimum, but many examples also show cytologically bland spindle cell proliferations, sex cord-like growth, and chondroid or osseous metaplasia lacking atypia.
Endometrioid adenocarcinomas display different patterns of myometrial invasion, some of which appear to have prognostic significance. Standard myometrial invasion is manifested by irregular infiltration of myometrium with a surrounding desmoplastic response. Less commonly encountered patterns include “pushing” [9], “adenoma malignum” [10], and “microcystic elongated and fragmented” (MELF) [11]. The pushing pattern demonstrates extension into myometrium over a broad front without irregular infiltration. The pattern is recognized as invasive only when a stromal reaction is found at the advancing invasive edge. The adenoma malignum pattern shows myometrial infiltration by well-formed glands lacking a stromal response. It is distinguished from adenomyosis by its diffuse infiltration and lack of endometrial stroma. MELF pattern of invasion is characterized by microcystic and elongate invasive glands, frequently showing squamous metaplasia with attenuation of epithelium lining the microcysts. Single neoplastic cells can be found adjacent to these foci, leading to the impression of gland fragmentation. Single and clustered neoplastic cells may be found in the microcysts’ lumens, leading to the erroneous impression of lymphovascular invasion. Probably most striking about MELF invasion is the almost invariable presence of an exaggerated fibromyxoid and fibroinflammatory stromal reaction surrounding the invasive foci. MELF invasion is treacherous because it may be discontinuous with the endomyometrial junction and present deep in myometrium. MELF pattern invasion is statistically associated with the presence of lymphovascular invasion (Fig. 6).


Endometrioid carcinoma with MELF pattern of invasion with elongated and fragmented glands associated with fibromyxoid stromal response and abundant acute inflammatory infiltrate
Differential Diagnosis
The differential diagnosis of uterine endometrioid adenocarcinoma includes other uterine carcinomas such as serous and clear cell carcinomas. Strategies for distinguishing between these entities are summarized in Table 1. Other common problems in diagnosis involve the distinction of complex atypical hyperplasia from endometrioid adenocarcinoma (Table 2), endocervical from endometrial adenocarcinoma (Table 3), and carcinosarcoma from endometrioid adenocarcinoma, which will be discussed subsequently in this chapter.
Since complex atypical hyperplasia and well-differentiated (FIGO grade 1) endometrial endometrioid carcinoma are both differentiated neoplasms, endometrioid tubular glands generally predominate in both. Conceptually, hyperplasia is separated from adenocarcinoma by the absence of endometrial stromal invasion (Fig. 7) [12,13,14]. Squamous metaplasia may be seen in both (Fig. 8). In practice, the presence of extensive confluent papillary growth, macroglands, and cribriform architecture is sufficient to categorize a lesion as adenocarcinoma [12,13,14]. Marked cytologic atypia also disqualifies the diagnosis of hyperplasia [13]. Another challenge concerns the differential diagnosis with endocervical adenocarcinoma. The latter may demonstrate features that resemble those of endometrial endometrioid adenocarcinoma, but there are usually subtle histologic differences. Clinical presentation, precursor lesions (endocervical adenocarcinoma in situ versus endometrial hyperplasia), and immunophenotype differ and can be used to establish the correct diagnosis (Table 3).


Complex atypical hyperplasia. Note the preserved endometrial stroma between abnormal endometrioid glands


Complex atypical hyperplasia exhibiting squamous metaplasia. Squamous metaplasia is typical of neoplastic endometrioid proliferations, either hyperplasia or carcinoma
Related Carcinomas
As mentioned earlier, endometrioid adenocarcinomas can demonstrate mucinous differentiation and can contain ciliated cells and cells with secretory features. When mucinous differentiation predominates (intracytoplasmic but not luminal mucin; present in >50 % of cells), the tumor is referred to as “mucinous carcinoma” [15, 16]. Likewise, “ciliated carcinoma” [17] and “secretory carcinoma” [18] have been described but are rare. Endometrioid adenocarcinomas may also feature papillary architecture. The tumor is referred to as “villoglandular carcinoma” [19] when the papillae are long, slender with delicate fibrovascular cores, and lined by pseudostratified columnar cells perpendicular to the basement membrane. Other findings that can be seen in endometrioid adenocarcinomas include psammomatous calcifications [20], cells with clear cytoplasm, spindled cells, trabeculae resembling sex cord ovarian tumors, hyalinized and myxoid stroma, and, exceptionally, heterologous elements [8] such as osteoid and lobules of cartilage.
Immunophenotype
The immunophenotype of endometrioid carcinoma tends to vary with degrees and types of differentiation. In general, endometrioid adenocarcinomas coexpress pan-cytokeratin and vimentin [21, 22] and they rarely show diffuse cytoplasmic staining with carcinoembryonic antigen (CEA) [23,24,25]. Almost all endometrioid neoplasms express CK7 and are largely negative for CK20 [26, 27]. Other commonly expressed antigens include CA125 [28], BerEP4 [29], and B72.3 [30]. The expression of estrogen and progesterone receptors (ER, PR) is ubiquitous among FIGO grade 1 adenocarcinomas, but this feature is present in <50 % of FIGO grade 3 tumors [31, 32]. Overexpression of p53 (expression in >50–75 % of nuclei) is seen in about one-third of FIGO grade 3 adenocarcinomas, but almost never in FIGO grade 1 tumors [33, 34]. The expression of p16 also tends to accumulate with increasing histological grade [31]. High-molecular-weight cytokeratins, p63, and nuclear β-catenin are preferentially expressed in areas demonstrating squamous differentiation [35, 36].
Serous Carcinoma
Pure serous carcinomas comprise about 10 % of endometrial cancers. They are epidemiologically, biologically, histologically, and clinically distinct. The mean age of women with serous carcinoma is approximately one decade older than those with endometrioid adenocarcinoma. Instead of being related to hyperestrinism, serous carcinomas arise in the setting of atrophy and, as such, correspond to Bokhman’s type II endometrial cancers [1]. Other associations with serous carcinoma include a personal history of breast cancer [37, 38], treatment with tamoxifen [39, 40], and pelvic radiation therapy [41, 42]. Serous carcinomas are aggressive neoplasms that have a tendency to present at high stage [43, 44].
Gross Features
Uteri harboring serous carcinomas tend to be small and lack the endometrial thickening that is more characteristic of endometrioid adenocarcinomas. Instead, many serous carcinoma uteri contain endometrial polyps. When carcinomas are confined to the polyp, the tumor itself may not be grossly apparent. More advanced tumors frequently demonstrate obvious myometrial permeation and either extension or metastasis to tissues included in the resection. Uterine serous carcinomas have a predilection for peritoneal dissemination as seen in their ovarian counterpart.
Histologic Features
The term “serous” refers to shared characteristics with cells lining the fallopian tube, particularly the tumor cells’ columnar shape, eosinophilic cytoplasm, and tendency to form papillae (Fig. 9). However, not all serous carcinomas are papillary and not all papillary carcinomas are serous. Essentially, all serous carcinomas exhibit marked nuclear pleomorphism and most demonstrate discrepancies between architectural differentiation and cytologic features. Serous carcinoma cells have high nuclear to cytoplasmic ratio with enlarged nuclei that tend to be irregularly shaped. They may be hyperchromatic or contain large, red macronucleoli (Fig. 10). Brisk mitotic activity and atypical mitoses are common. In contrast to endometrioid carcinoma, the luminal surfaces are irregular and jagged (Fig. 9), and the cells are less cohesive with frequent cellular tufting, and detached small cell aggregates. Unlike endometrioid adenocarcinomas, serous carcinomas do not show squamous or mucinous metaplasia, or ciliated cells.


Serous carcinoma. Typical low-power appearance demonstrating papillary architecture and slit-like spaces


Serous carcinoma. This high power shows the ragged luminal profiles and highly atypical nuclei
The earliest serous carcinoma may consist solely of neoplastic epithelium colonizing preexisting atrophic endometrium, particularly on the surface of endometrial polyps [45, 46]. This has been referred to as intraepithelial serous carcinoma or endometrial intraepithelial carcinoma [45, 46]. Importantly, intraepithelial serous carcinoma can metastasize despite the absence of myometrial invasion. At low power, these minimal carcinomas appear hyperchromatic and display abrupt transition with the nonneoplastic epithelium. Serous carcinomas may be difficult to diagnose when they replace preexisting atrophic endometrial glands and papillary architecture is not apparent [47]. Correct classification as serous carcinoma centers on appreciation of the cytologic features, jagged luminal profiles, absence of confirmatory endometrioid characteristics (including squamous and mucinous metaplasia), and background atrophy. Architectural patterns encountered in established serous carcinomas include papillae, tubular glands, slit-like glands, and solid nests and sheets. Since these patterns are not specific for serous carcinoma, attention directed to the cytologic characteristics is essential to make the correct diagnosis.
Immunophenotype
Like endometrioid adenocarcinomas, serous carcinomas coexpress pan-cytokeratins and vimentin and rarely express diffuse cytoplasmic CEA. They also are positive for CK7, CA125, BerEP4, and B72.3 and are largely negative for CK20. The expression of ER and PR is less common than in endometrioid adenocarcinomas and is found in <50 % of tumors [31, 32, 48]. Overexpression of p53 (>50–75 % of nuclei) is seen in nearly 90 % of serous carcinomas and is related to the near-universal presence of p53 mutations [34, 49], while p16 expression is also very common [31].
Clear Cell Carcinoma
This subtype of endometrial carcinoma is the third most common, even though it represents <5 % of all carcinomas at this site. The epidemiologic characteristics of patients with clear cell carcinoma are obscure because of this tumor’s rarity, difficulties in diagnostic reproducibility, and accumulating evidence that there are perhaps several subtypes of clear cell carcinoma. The subtypes include (1) tumors admixed with endometrioid adenocarcinoma; (2) those mixed with or histologically resembling serous carcinoma; and (3) pure clear cell carcinoma [50, 51]. There are emerging data that suggest that clear cell carcinomas might be overrepresented in patients with Lynch syndrome [52].
Gross Features
Clear cell carcinoma has no distinctive gross features. Tumors combined with endometrioid adenocarcinomas may be associated with a thickened endometrium. Pure clear cell carcinomas as well as those mixed with serous carcinomas are often associated with endometrial polyps and deep myometrial invasion.
Histologic Features
Most clear cell carcinomas are composed of cells with clear cytoplasm, but this feature is not restricted to this subtype of endometrial cancer (see “Discussion” of endometrioid adenocarcinomas). Furthermore, some clear cell carcinomas may contain cells with eosinophilic cytoplasm. As with other endometrial carcinoma subtypes, the combination of low-power architectural features and cytologic characteristics permits its diagnosis. These tumors classically demonstrate varied architectural patterns that include papillary, tubular, tubulocystic, solid, and mixtures thereof. The papillae of clear cell carcinoma are small and round in comparison to those of either serous carcinoma or villoglandular endometrioid adenocarcinomas. Characteristically, the stroma of the papillae is densely hyalinized (Fig. 11). The lining epithelium is only one or two cells thick, without prominent tufting. The cells are large, generally contain ample clear cytoplasm filled with glycogen, and show sharply defined cytoplasmic boundaries. Hobnail cells may be seen lining papillae or glands. The nuclei are cytologically malignant, sometimes containing macronucleoli, although overt pleomorphism is found only infrequently (Fig. 11). Like serous carcinoma, clear cell carcinoma usually arises in the setting of atrophic endometrium and in endometrial polyps [45].


Clear cell carcinoma. The tumor cells have cytoplasmic clearing, hobnail features, and striking cytologic atypia, and hyalinized stroma is seen
Immunophenotype
Most clear cell carcinomas coexpress pan-cytokeratins and vimentin and rarely show diffuse cytoplasmic CEA positivity. They also express CK7 and are largely negative for CK20. Data regarding expression of ER, PR, and p53 are contradictory, while results of p16 expression are now just emerging. ER and PR expression is uncommon and, when present, is weak and focal [31, 51, 53]. p53 overexpression can be seen, but with a rate (approximately at the 50 % level) significantly lower than in serous carcinoma [50, 51, 53]. The degree of ER, PR, and p53 expression might be related to an individual tumor’s pathogenesis [50, 51, 53]. For example, clear cell carcinomas associated with endometrioid adenocarcinomas might preferentially express ER and PR, while those resembling or associated with serous carcinomas might overexpress p53. p16, expression of which may also be found in pure clear cell carcinomas, is more common than in endometrioid adenocarcinomas but less frequent than in serous carcinomas [31]. Expression of napsin A [54] and hepatocyte nuclear factor 1 beta [55] has been reported in both ovarian and endometrial clear cell carcinomas, but the sensitivity and specificity of these markers tend to be stronger in ovarian tumors with clear cytoplasm than in endometrial tumors.
Mixed (Mixed Epithelial) Carcinomas
With only one exception (mucinous carcinoma), mixed epithelial carcinomas are diagnosed when at least two endometrial carcinoma subtypes are present and the minor component(s) constitute 5 % of the tumor. Because mucinous differentiation is so commonly encountered in endometrioid adenocarcinomas, there is less enthusiasm now than in the past to diagnose “mixed endometrioid and mucinous carcinoma.” The 2014 World Health Organization classification of gynecologic tumors [56] now specifies that mixed epithelial tumors must contain one component that is high grade or “type II.” The term “mixed carcinoma” should not be used for tumors that contain areas with subtle differences. For example, a serous carcinoma with glandular architecture should not be considered a mixed serous and endometrioid adenocarcinoma unless two distinctive morphologies are present. Emerging data suggest that most carcinomas historically interpreted as "mixed epithelial" are instead monoclonal tumors with intratumoral heterogeneity, with one possible exception being those tumors that arise in the setting of Lynch Syndrome.
Squamous Cell Carcinoma
Primary squamous cell carcinoma of the endometrium is very rare and should only be diagnosed in the absence of hyperplasia or any endometrioid glandular differentiation [57]. They are histologically similar to squamous cell carcinomas of the cervix and most are cytologically high grade. Extension from a cervical squamous carcinoma or a history of a previous cervical squamous cell carcinoma excludes a diagnosis of primary squamous carcinoma of the endometrium.
Transitional Cell Carcinoma
This extraordinarily rare tumor is by definition composed of cells resembling those of urothelial transitional cell carcinoma [58, 59]. The architecture is papillary or trabecular, just like the urothelial counterparts. Extension and metastasis from a urothelial primary carcinoma should always be excluded. These tumors can occur in pure form or be mixed with other carcinoma subtypes. Many cases may, indeed, represent morphological variants of endometrioid carcinoma.
Small Cell Carcinoma
The histologic appearance of this tumor is essentially identical to that of small-cell neuroendocrine carcinomas of other organs [60]. These tumors can occur in pure form or be mixed with other carcinoma subtypes.
Undifferentiated Carcinoma
Undifferentiated carcinomas by definition lack any evidence of differentiation. As such, their appearance may simulate high-grade sarcoma, lymphoma, melanoma, and metastases to the uterus. Universal but frequently only focal expression of cytokeratins and epithelial membrane antigen (EMA) is seen [60, 61]. Many examples coexist with differentiated endometrioid carcinoma, in which case the tumors may be diagnosed as “dedifferentiated endometrial carcinoma” or “mixed undifferentiated and endometrioid carcinoma.” (Fig. 12).


Dedifferentiated carcinoma. A well-differentiated endometrioid carcinoma is juxtaposed to an undifferentiated carcinoma (a), which is composed of non-cohesive poorly differentiated epithelial cells without gland formation (b)
Uterine Sarcomas and Mixed Müllerian Tumors
Leiomyosarcoma
Uterine leiomyosarcoma constitutes 1 % of all uterine malignancies; it is the most common uterine sarcoma, and represents approximately 40 % of all sarcomas at this site, and 40 % of leiomyosarcomas among women at all sites [62] (Table 4). The incidence of uterine leiomyosarcoma is approximately 0.67/100,000 women per year [63]. Even though uterine leiomyomas are the most common tumor of the female genital tract, the incidence of leiomyosarcoma originating from leiomyoma is very low, ranging between 0.13 and 0.80 [64], but some authors believe that leiomyosarcoma may have areas closely resembling classic leiomyoma or its variants but do not really arise from leiomyoma as when evaluating both leiomyoma-like areas and leiomyosarcoma areas both have nearly the same genetic aberrations by CGH array [65]. As occurs with leiomyomas, uterine leiomyosarcomas are more frequent among black women [62]. There is at least one familial cancer syndrome characterized by retinoblastoma, hereditary leiomyomatosis, and renal cell cancer which has an increased incidence of uterine leiomyosarcoma [66].
Gross Features
Leiomyosarcoma occurs most commonly as a single nodule in almost 90 % of cases and if multiple nodules are present in the uterus, it is usually the largest [67, 68]. Leiomyosarcoma typically forms an intramyometrial mass with either well-circumscribed or irregular infiltrative growth into the surrounding myometrium. On sectioning, the tumors appear fleshy, gray to pink, and are frequently associated with areas of hemorrhage and necrosis [67, 69]. If the tumor has a prominent gelatinous cut surface, it should raise suspicion for a myxoid leiomyosarcoma [69].
Histologic Features
The diagnosis of malignancy in a smooth muscle tumor is based on three histologic features: (1) tumor cell necrosis; (2) moderate-to-severe cytologic atypia; and (3) mitotic activity [70]. Tumor cell necrosis is defined by the finding of an abrupt transition between the nonviable and viable tumor. The viable tumor frequently grows around vessels (perivascular distribution) and pleomorphic cells may still be identified in the devitalized areas. However, it is often difficult to distinguish tumor cell necrosis from infarct-type necrosis [71] and interobserver agreement amongst gynecologic pathologists is only fair in making a diagnosis of tumor cell necrosis [72]. In most cases, tumor cell necrosis is accompanied by tumor cells showing increased mitotic activity and marked cellular atypia. The latter is defined by cellular pleomorphism, nuclear enlargement and/or irregular outlines, hyperchromatism, as well as prominent nucleolus. Cytologic atypia should be identified at medium power (10×) and typically is diffuse in leiomyosarcomas. Finally, it may be difficult to count mitotic activity in smooth muscle tumors as not infrequently apoptotic cells are misinterpreted as mitoses. Apoptotic cells are typically characterized by refractile dense eosinophilic cytoplasm and coarse clumped chromatin, which contrasts with the hairy chromatin extending from a central dense mass of chromosomes with discernible cytoplasm and absent nuclear membrane in a true mitoses. Immunohistochemical markers including PHH3 and MPM-2 have been used to increase interobserver reproducibility in the assessment of mitotic activity and appear helpful in this distinction although they are not used universally [73, 74]. Even though mitotic activity had been considered the most important criterion to establish a diagnosis of malignancy in a smooth muscle tumor in the past, it has been demonstrated that mitotic activity in the absence of one of the other two histologic features previously described is insufficient to establish the diagnosis of leiomyosarcoma. Furthermore, it is important to keep in mind that the threshold for mitotic activity is higher in smooth muscle tumors of the uterus than that used in soft tissue tumors [75]. This is due to the mitogenic effect of estrogen and progesterone on gynecologic tumors and in particular on spindle cell smooth muscle tumors of the uterus. It is also important to be aware that the diagnostic mitotic threshold varies among the different subtypes of leiomyosarcoma, being ≥10 in spindle, ≥5 in epithelioid, and ≥2 in myxoid leiomyosarcomas [71].
Leiomyosarcomas can be classified into grades 1, 2, and 3 or low and high grade based on the degree of cellular differentiation, mitotic activity, and tumor cell necrosis, but these classifications are subjective. A tumor showing marked cytologic atypia associated with brisk mitotic activity and tumor cell necrosis is classified as high grade while a tumor that at low power displays mild cytologic atypia but has brisk mitotic activity and focal tumor necrosis can be classified as low-grade leiomyosarcoma. However, based on the available diagnostic criteria, most malignant smooth muscle tumors are high grade while the majority of leiomyosarcomas diagnosed as low grade in the past can be reclassified as leiomyoma variants or other low-grade mesenchymal tumors of the uterus [76].
Leiomyosarcomas are divided into three main categories depending on their morphologic appearance: (a) spindled, (b) epithelioid, and (c) myxoid; and not infrequently, they show more than one component. Rarely, leiomyosarcomas can contain xanthomatous or giant cells.
-
1.
Spindle cell leiomyosarcoma is composed of fusiform cells showing central elongated nuclei with blunted ends occasionally indented by a clear vacuole (Fig. 13). The cytoplasm is deeply eosinophilic due to the presence of myofilaments that are disposed parallel to the cell axis (best seen in a Masson trichrome stain). The cells form long well-oriented intersecting fascicles [77]. The combination of any two of the following three features establishes the diagnosis of spindled leiomyosarcoma: diffuse moderate-to-severe cytologic atypia, ≥10 mitoses/10 high-power fields (HPFs), and tumor cell necrosis (Fig. 14; Table 5) [75]. Vascular invasion is detected in approximately 20 % of leiomyosarcomas and some tumors may have a prominent intravascular growth (“intravenous leiomyosarcomatosis”) [78, 79].
Fig. 13 
Spindle cell leiomyosarcoma. The neoplastic cells form intersecting fascicles and display pleomorphic and hyperchromatic nuclei
Fig. 14 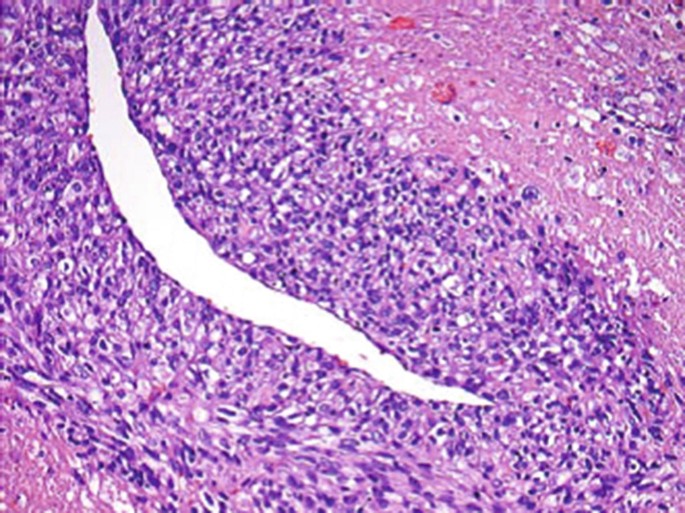
Spindle cell leiomyosarcoma. There is an abrupt transition from viable to nonviable tumor (tumor cell necrosis) and the tumor cells typically grow around vessels. Notice that scattered atypical cells are seen in the necrotic foci
Table 5 Diagnostic criteria for the different subtypes of leiomyosarcoma -
2.
Epithelioid leiomyosarcoma is composed of sheets, nests, or cords of cells with abundant cytoplasm. To establish the diagnosis of epithelioid leiomyosarcoma, at least 50 % of the cells should display epithelioid features. The cells show a centrally located round nucleus and eosinophilic cytoplasm (Fig. 15) but in up to 25 % of the tumors, the cytoplasm is clear. Variable amounts of collagen deposition may be seen. The criteria to establish the diagnosis of malignancy in epithelioid smooth muscle tumors are not well established. However, as a general rule, the diagnosis of epithelioid leiomyosarcoma is warranted when there are ≥5 mitoses/10 HPFs and diffuse moderate-to-severe cytologic atypia or tumor cell necrosis (Table 5) [80,81,82].
-
3.
Myxoid leiomyosarcoma is rare and it is characterized by the presence of abundant myxoid matrix that is positive for Alcian Blue or colloidal iron histochemical stains. The tumors are often hypocellular in contrast to most spindled and epithelioid leiomyosarcomas. Most tumors show an infiltrative growth into the surrounding myometrium (Fig. 16a). At higher magnification, the degree of cytologic atypia and mitotic activity is quite variable [83,84,85,86,87,88]. The diagnosis of myxoid leiomyosarcoma is made when either marked cytologic atypia or tumor cell necrosis is identified. In their absence, the finding of ≥2 mitoses/10 HPFs separates myxoid leiomyosarcoma from myxoid leiomyoma (Fig. 16b; Table 5) [83].
Fig. 15 
Epithelioid leiomyosarcoma. The tumor cells grow in sheets. They have abundant eosinophilic cytoplasm and focal moderate nuclear atypia and mitoses are easy to identify (arrows)
Fig. 16 
Myxoid leiomyosarcoma. The tumor has an infiltrative margin into surrounding myometrium. It is hypocellular with a prominent myxoid background 9 (a) and the tumor cells show nuclear pleomorphism and mitotic activity (arrow) (b)








Immunophenotype
Leiomyosarcomas are typically positive for actin, desmin, and h-caldesmon. They also frequently express CD10 [89], oxytocin [90], ER, PR, and androgen receptor [91]. Epithelioid leiomyosarcomas frequently express keratin and EMA [92], and both epithelioid and myxoid leiomyosarcomas are less frequently positive for smooth muscle markers. Leiomyosarcomas display p53 and c-kit positivity; however, no associated c-kit mutations have been reported [93,94,95]. They also express strongly and diffusely p16 [96] while they show variable expression of bcl-2 [97] and rare-to-absent Med12 mutations [98,99,100].
Differential Diagnosis
Spindle cell leiomyosarcoma should be distinguished from leiomyoma variants including mitotically active leiomyoma, apoplectic leiomyoma, and leiomyoma with bizarre nuclei. Mitotically active leiomyoma displays brisk mitotic activity; however, it lacks cytologic atypia and tumor cell necrosis [101, 102]. Leiomyoma with apoplectic change may show areas of hypercellularity associated with slight cytologic atypia and brisk mitotic activity surrounding the areas of hemorrhage, thus causing concern for malignancy. However, away from these areas, the tumor has the appearance of a conventional leiomyoma [103, 104]. It is important to keep in mind that areas close to the apoplectic change frequently show an increased ki-67 index as well as p16 positivity increasing the concern for malignancy. Positivity becomes imperceptible away from these areas which is helpful in establishing the diagnosis of leiomyoma with apoplectic change [105]. Finally, worrisome features associated with leiomyoma with bizarre nuclei include the presence of mono- or multinucleated cells which may show prominent nuclei, nuclear pseudoinclusions, karyorrhectic nuclei (that may mimic atypical mitotic figures), and some degree of mitotic activity. It is important to notice that in most cases, the bizarre cells have a patchy distribution in the tumor, mitotic activity is low, and there is no tumor cell necrosis [106, 107]. This leiomyoma variant is frequently p16 and p53 strongly and diffusely positive and shows variable ki67 expression, an immunoprofile that overlaps with that observed in leiomyosarcoma. Other rare malignant tumors in the differential diagnosis include spindle cell rhabdomyosarcoma [108] and undifferentiated uterine sarcoma [109]. The former may be very difficult to distinguish from a spindle cell leiomyosarcoma. The finding of cytoplasmic cross striations and positivity for skeletal muscle markers (myoglobin, myoD1, and myogenin) are helpful in this differential diagnosis. Undifferentiated uterine sarcoma is a diagnosis of exclusion based on histologic and immunohistochemical findings [77].
Epithelioid leiomyosarcoma should be distinguished from a poorly differentiated carcinoma, trophoblastic tumors (placental site trophoblastic tumor and epithelioid trophoblastic tumor) [110], PEComa (discussed below) [111,112,113], uterine tumor resembling an ovarian sex cord stromal tumor [114,115,116], the rare alveolar soft part sarcoma [117, 118], and metastatic melanoma [119]. In order to establish the correct diagnosis, it is important to consider the patient’s clinical history and to sample the tumor extensively. In difficult cases, the use of a battery of immunohistochemical markers including those for epithelial, smooth muscle, sex cord, and intermediate trophoblast differentiation may be helpful.
Myxoid leiomyosarcoma must be distinguished from its benign counterpart, the myxoid leiomyoma. The latter is an extremely rare tumor that typically is small (<5 cm), shows well-circumscribed margins, no cytologic atypia, absent tumor cell necrosis, and mitotic count <2/10 HPFs [80]. Leiomyoma with hydropic change may also be considered in the differential diagnosis of a myxoid leiomyosarcoma; however, the background matrix is composed of edema fluid which is Alcian Blue and colloidal iron negative [120a]. Rarely an inflammatory myofibroblastic tumor may mimic a myxoid leiomyosarcoma. It is frequently associated with a lymphoplasmatic unfiltrate and it is ALK positive, showing ALK rearrangement by FISH [120b]
Low-Grade Endometrial Stromal Sarcoma
Endometrial stromal neoplasms are divided into three main groups based on the latest WHO classification: (a) endometrial stromal nodule, (b) low-grade endometrial stromal sarcoma, and (c) high-grade endometrial stromal sarcoma. Low-grade endometrial stromal sarcoma accounts for approximately 80 % of all stromal neoplasms and it represents the second most common pure uterine sarcoma of the homologous type following leiomyosarcoma. A new category of high-grade endometrial stromal sarcoma has been established as it is associated with an intermediate prognosis between low-grade endometrial stromal sarcoma and undifferentiated endometrial/uterine sarcoma and it is characterized by distinctive morphology, immunophenotype, and chromosomal translocation [121]. The term undifferentiated uterine sarcoma includes tumors of stromal derivation but these tumors (either arising from the endometrial stroma or the myometrium) are very aggressive with a behavior similar to that of any high-grade sarcomas in the soft tissues [121].
Gross Features
Low-grade endometrial stromal sarcomas commonly appear as multiple coalescent tan to yellow soft nodules involving the endometrium and myometrium. The tumors typically show a permeative growth into the myometrial wall and myometrial veins and, not infrequently, may be identified grossly, outside the uterus in parametrial veins. They may show areas of necrosis and hemorrhage [122].
Histologic Features
These tumors infiltrate the myometrium as irregular islands without any associated stromal response (Fig. 17). The tumor cells are small, uniform with scant cytoplasm and round-to-oval nuclei with indistinct nucleoli. The tumor cells may whorl around the vessels, which are small and reminiscent of endometrial-type arterioles (Fig. 18). Histiocytes, single or in groups, collagen plaques, and cholesterol clefts are common associated findings [123]. Low-grade endometrial stromal sarcomas may show morphologic variations or unusual features including smooth muscle [124], skeletal muscle [125] or adipose differentiation [125], fibrous and/or myxoid background [126, 127], endometrioid glandular [128, 129] and sex cord-like differentiation [130], cells with granular eosinophilic or clear cytoplasm [131, 132], cells with a rhabdoid phenotype [133], cells with bizarre nuclei [125] or osteoclast-like cells [134], and finally pseudopapillary architecture [135].


Low-grade endometrial stromal sarcoma. The tumor is hypercellular and infiltrates the myometrium as irregular tongues


Low-grade endometrial stromal sarcoma. The tumor cells are small and uniform and focally whorl around arterioles
To establish the diagnosis of low-grade endometrial stromal sarcoma, the tumor must resemble proliferative-type endometrial stroma regardless of the mitotic index. A diagnosis of high-grade endometrial stromal sarcoma could be made when a tumor with high-grade cytologic atypia (undifferentiated) arises in the context of a low-grade endometrial stromal sarcoma [77].
Immunophenotype
The neoplastic endometrial stromal cells are typically immunoreactive for vimentin, muscle-specific and smooth muscle actin, keratin, and CD10 [136,137,138]. However, it is important to note that CD10 staining can be seen in other uterine tumors. They typically express ER and PR [139] and may express androgen receptors [140]. Some degree of positivity for desmin and caldesmon may be seen particularly if the tumor shows smooth muscle differentiation [89, 137, 138, 141,142,143]. Areas of sex cord-like differentiation may be positive for inhibin, calretinin, CD99, WT1, and melan A as well as demonstrate positivity for epithelial and smooth muscle markers [115, 144, 145]. Areas of rhabdomyoblastic differentiation are positive for myoD1, myoglobin, and myogenin [125]. C-kit has been reported to be positive in low-grade endometrial stromal sarcomas; however, no associated mutations have been noted [146]. Some low-grade endometrial stromal sarcomas express β-catenin [109, 147] and some may show aromatase expression which may be used for therapeutic purposes [148].
Molecular Genetics
Low-grade endometrial stromal sarcomas are genetically heterogeneous and often harbor recurrent chromosomal translocations resulting in specific gene rearrangements. The most common genetic alteration is the t(7;17)(p15;q21) translocation resulting in JAZF1–SUZ12 gene fusion. However, other chromosomal translocations and their corresponding gene fusions have been identified: t(7;17)(p15;q21), t(6;7)(p21;p15), t(6;10;10)(p21;q22;p11), and t(1;6)(p34;p21), resulting in JAZF1–SUZ12, PHF1–JAZF1, EPC1–PHF1, and MEAF6–PHF1 rearrangements, respectively [149, 150].
Differential Diagnosis
The main entities in the differential diagnosis of low-grade endometrial stromal sarcoma include endometrial stromal nodule and highly cellular leiomyoma. An endometrial stromal nodule shares the same cytologic features described in low-grade endometrial stromal sarcoma. The main difference is the finding of a well-defined tumor-myometrium interface. Focal irregularities in the form of small finger-like projections or small islands not exceeding 3 mm are allowed; however, no vascular invasion should be seen [151]. It is important to extensively sample the tumor–myometrium interface in order to identify subtle permeation into the myometrium that may escape the naked eye [151]. Clinicians should be made aware that the pathologist cannot distinguish between an endometrial stromal nodule and a low-grade endometrial stromal sarcoma in a curettage specimen in most instances, as it is not possible to assess the entire margin, which is the most important feature in this differential diagnosis. The other important differential diagnosis is with a highly cellular leiomyoma. This benign smooth muscle tumor is characterized by dense uniform cellularity, prominent vascularity, and sometimes a pseudoinfiltrative growth into the surrounding myometrium, features that overlap with those described in endometrial stromal tumors. However, the tumor cells frequently form fascicles, the vessels are typically large with thick walls, and there is transition from the tumor to the myometrium, features that are lacking in a low-grade endometrial stromal sarcoma. The distinction is important, as it has prognostic implications, especially in a curettage specimen from a young woman. If the diagnosis is that of highly cellular leiomyoma, the patient may retain her uterus, whereas if the diagnosis is that of endometrial stromal neoplasm, the patient requires a hysterectomy in most cases [152, 153]. Other neoplastic and nonneoplastic processes that rarely enter into the differential diagnosis include gland poor adenomyosis [154] and cellular intravenous leiomyomatosis [155]. When low-grade endometrial stromal sarcomas show unusual features, the differential diagnosis is broader including endometrioid adenomyoma (if there is prominent smooth muscle differentiation) [156], myxoid smooth muscle tumor (if there is prominent myxoid change) [123], uterine tumor resembling an ovarian sex cord tumor (if there is prominent sex cord-like differentiation) [114], and finally adenomyosis and low-grade müllerian adenosarcoma (if there is glandular differentiation) [157].
High-Grade Endometrial Stromal Sarcoma
These are tumors that often show a pattern of myometrial infiltration similar to that seen in low-grade endometrial stromal sarcomas. They are composed of small round cells that either grow in diffuse or vaguely nested patterns. In the latter, the nests are separated by a delicate capillary network. Cells have a high nuclear to cytoplasmic ratio and the cytoplasm is scant to moderate at most and faintly eosinophilic. Mitotic activity is typically high (>10/10 HPFs), and tumor cell necrosis and vascular invasion are often present (Fig. 19a). In approximately 50 % of the tumors, a component of low-grade endometrial stromal sarcoma is present, typically the fibromyxoid variant where monomorphic, fusiform to spindled cells are set in a fibrocollagenous or fibromyxoid background [158].


High-grade endometrial stromal sarcoma. Small epithelioid cells with brisk mitotic activity grow in sheets (a). The tumor cells are strongly and diffusely cyclin D1 positive (b)
Patients with these tumors typically present with advance stage and have a prognosis that is intermediate between low-grade endometrial stromal sarcoma and undifferentiated endometrial/uterine sarcoma [158].
A diagnosis of high-grade endometrial stromal sarcoma can also be made when a high-grade sarcoma is associated with a second component that can be diagnosed as a low-grade endometrial stromal sarcoma. The prognosis of these tumors is similar to that reported for undifferentiated endometrial/uterine sarcomas [121].
Immunophenotype and Molecular Genetics
These tumors, in contrast to low-grade endometrial stromal sarcomas, are typically negative for CD10, ER, and PR but strongly and diffusely positive for CyclinD1 (Fig. 19b) and show a characteristic t(10,17) with YWHAE–FAM22 rearrangement [158].
Undifferentiated Uterine Sarcoma
This is a high-grade sarcoma without specific histologic features. In the 2014 WHO classification, the term undifferentiated uterine sarcoma replaces undifferentiated endometrial sarcoma as not all these tumors have an endometrial stromal origin [121]. This diagnosis should only be made after poorly differentiated carcinoma, leiomyosarcoma, rhabdomyosarcoma, adenosarcoma with sarcomatous overgrowth, and malignant mixed müllerian tumor have been excluded by extensive sampling, careful histologic examination, and use of immunohistochemical stains if needed [77].
As mentioned earlier, a diagnosis of high-grade endometrial stromal sarcoma can be applied only in cases in which a component of low-grade endometrial stromal sarcoma is identified. Otherwise, the diagnosis is that of undifferentiated uterine sarcoma. This nomenclature conveys the highly aggressive nature of the tumor which contrasts with the much better prognosis associated with a low-grade endometrial stromal sarcoma [77].
Low-Grade Müllerian Adenosarcoma
This tumor belongs to the biphasic müllerian category of tumors (Table 6). It is typically composed of benign-appearing glands and a low-grade malignant mesenchymal component. It has been reported to represent approximately 7 % of all uterine sarcomas in a large series [159]. It most commonly affects perimenopausal women and has a similar incidence in white and black women. These tumors have been reported in women receiving tamoxifen therapy or after pelvic radiation therapy [160].
Gross Features
Most low-grade müllerian adenosarcomas appear as large polypoid masses filling the endometrial cavity, but rarely arise in the myometrium, within adenomyosis [161]. On sectioning, they may be predominantly solid or have a spongy appearance with cysts of different sizes. The cysts are filled with clear fluid or hemorrhage and are separated by variable amounts of tan to brown tissue [157].
Histologic Features
On low-power examination, the key histologic features include the finding of marked condensation of the low-grade malignant stromal component around glands that may be cystically dilated (Fig. 20a) or a phyllodes-type morphology. In the latter, the finding of intraluminal protrusions of the neoplastic stroma is also characteristic. The malignant mesenchymal component is commonly a low-grade homologous sarcoma reminiscent of low-grade endometrial stromal sarcoma or fibrosarcoma. The greatest degree of cytologic atypia (at most moderate) and mitotic activity is seen in the areas of stromal condensation. The glandular component is commonly of endometrioid-type although mucinous or tubal-type epithelium and squamous differentiation may be found. The epithelium is typically benign, but it may on occasion appear atypical. The diagnosis of adenosarcoma is generally established by the finding of the typical architectural and cytologic features accompanied by any degree of mitotic activity in the hypercellular stromal component surrounding the glands. Even though in the past a threshold of 4 mitoses/10 HPFs was used for the diagnosis of adenosarcoma, it has been shown that tumors showing prominent periglandular condensation, stromal atypia, and < 4 mitoses/10 HPFs frequently recur and, thus, should be diagnosed as adenosarcoma [157]. It is important to keep in mind that endometrial polyps may sometimes show focal architectural and/or cytologic features that overlap with that described in adenosarcoma including phyllodes-like architecture, intraglandular polypoid projections, altered periglandular stroma, and stromal cytologic atypia [162]. However, as mentioned earlier, these findings are focal and these polyps appear to be associated with a benign outcome [162]. It is also important to be aware that the diagnosis of müllerian adenofibroma should be only rendered with extreme caution. Adenofibroma is the benign counterpart of adenosarcoma, and although it is common in the ovary it is exceedingly rare in the uterus. It has been shown that tumors diagnosed as uterine adenofibromas may in fact represent very low-grade adenosarcomas as they have recurred multiple times and have been associated with an adverse outcome [163]. The mesenchymal component of an adenosarcoma may show bizarre nuclei, foamy histiocytes, smooth muscle, and sex cord-like differentiation [157, 160, 164]. Rhabdomyoblastic, cartilaginous, or fatty differentiation is more commonly seen outside the uterine corpus and is present in 10–15 % of cases [157, 165]. Finally, 10 % of these tumors show sarcomatous overgrowth, defined by the presence of pure sarcoma involving approximately 25 % of the tumor (Fig. 20b) [166]. In most cases, the sarcomatous overgrowth is composed of a high-grade sarcoma but it has also been reported as a low-grade sarcoma [167]. Sarcomatous overgrowth is associated with destructive invasion of the myometrium by sarcoma not accompanied by glands. This is in contrast to typical low-grade müllerian adenosarcomas which show a low incidence of myometrial invasion with both epithelial and stromal components forming part of the invasive tumor [157].


Low-grade müllerian adenosarcoma. The neoplastic stromal cells condensate around the müllerian-type glands (“collaring”) (a). Sarcomatous overgrowth. A high-grade sarcoma is associated with focal necrosis and has overgrown areas of conventional low-grade müllerian adenosarcoma (b)
Immunophenotype and Molecular Genetics
The low-grade malignant stromal component is typically positive for vimentin, WT1, CD10, ER, and PR with variable expression of cytokeratin, muscle actin, and androgen receptor. This immunohistochemical profile overlaps with that reported in low-grade endometrial stromal sarcomas. Areas of sarcomatous overgrowth show decreased or absent CD10, ER, and PR expression [168]. The most frequent abnormalities in low-grade müllerian adenosarcomas include MDM2 and CDK4 amplifications but alterations in PIK3CA/AKT/PTEN pathway members are also common while MYBL1 amplification and p53 mutations are uncommon and typically seen in areas of sarcomatous overgrowth [169].
Malignant Mixed Müllerian Tumor (Carcinosarcoma)
Even though it represents <5 % of all malignant uterine tumors, this highly malignant mixed tumor was previously considered the most common uterine sarcoma [170]. The histogenesis of these tumors has evolved in recent years. It is now widely accepted that carcinosarcomas either arise from a common pluripotential cell with divergent differentiation or that the sarcomatous component develops from the carcinomatous component by a metaplastic process or dedifferentiation [171, 172]. These tumors occur typically in postmenopausal women and have a higher incidence in black women [170].
Gross Features
These are typically large, bulky polypoid tumors filling and distending the endometrial cavity. On sectioning, they show a fleshy heterogeneous cut surface with extensive areas of hemorrhage and necrosis. Deep and destructive infiltration of the myometrium is easily identified in most cases. While most tumors originate in the uterine corpus, approximately 5 % arise in the cervix [173,174,175].
Histologic Features
These tumors are characterized by an intimate admixture of high-grade malignant epithelial and mesenchymal elements. However, in some cases, the two elements do not appear admixed but they are juxtaposed. The high-grade carcinoma is more frequently either of serous or endometrioid type (with or without squamous differentiation) (Fig. 21), although any type of endometrial carcinoma can be seen. If the tumor arises in the cervix, the epithelial component is typically squamous and can be found adjacent to high-grade squamous dysplasia. The high-grade sarcoma is often of the homologous type, resembling high-grade leiomyosarcoma, malignant fibrous histiocytoma, or undifferentiated endometrial sarcoma. Heterologous differentiation [including in order of frequency rhabdomyosarcoma (Fig. 21), chondrosarcoma, liposarcoma, and rarely osteosarcoma and neuroectodermal differentiation] is seen in approximately 50 % of cases [173, 176,177,178].


Malignant mixed müllerian tumor. The epithelial and sarcomatous components of the tumor are intimately admixed. The sarcomatous component shows rhabdomyoblastic differentiation (arrows)
Immunophenotype
The high-grade carcinoma typically coexpresses epithelial markers (keratin and EMA) and vimentin. The high-grade sarcoma is positive for vimentin and frequently for smooth muscle actin and epithelial markers. This overlapping profile of epithelial and mesenchymal components supports a common histogenesis. Synaptophysin, neuron-specific enolase, Leu-7, and CD10 may be expressed in the mesenchymal as well as in the epithelial component. The rhabdomyosarcomatous component is positive for myoglobin, myogenin, and MyoD1. p53 is frequently positive in both components [173, 179, 180]. These tumors are an excellent example of the epithelial-mesenchymal transition with loss of epithelial characteristics, including cadherin switching and acquisition of a mesenchymal phenotype. Typically E-cadherin is drastically diminished in the mesenchymal component while CDH11, SPARC, TGFβ1, and TGFβ2 are augmented in the mesenchymal areas [181].
Perivascular Epithelioid Cell Tumor (PEComa)
These are rare uterine tumors that belong to the family of neoplasms thought to originate from the perivascular epithelioid cell (PEC). The latter cell type is defined by the presence of abundant clear to eosinophilic granular cytoplasm, positive staining for HMB-45 or other melanocytic markers including melan A, microphthalmia transcription factor, cathepsinK, or TFE3, as well as frequent expression of muscle markers [182, 183]. Other tumors that belong to this family include clear cell “sugar” tumors of the lung and pancreas, some forms of angiomyolipoma, and the clear cell myelomelanocytic tumor of ligamentum teres/falciform ligament [184,185,186,187]. These tumors show a particular association with lymphangiomyomatosis as well as tuberous sclerosis [113, 185]. PEComa (sporadic or syndromic) frequently harbors mutation and loss of heterozygosity (LOH) of TSC2 and much more rarely TSC1 [188].
Gross Features
Most tumors are solitary and can be well circumscribed with a white and whorled cut surface or show poorly defined margins, often with a fleshy and soft, gray-white to tan or yellow cut surface [111,112,113, 189].
Histologic Features
On low-power examination, some tumors have a tongue-like infiltrative growth similar to that seen in a low-grade endometrial stromal sarcoma, while in others, the interface between the tumor and the surrounding tissue is smooth [111, 112]. The tumor cells grow in sheets or small nests with scant intervening stroma but prominent sinusoidal vasculature. The cells have abundant clear or eosinophilic cytoplasm and oval-to-round nuclei (Fig. 22a). Tumors with pure clear cell morphology are much less frequently associated with TSC mutations [188]. PEComas not infrequently show, at least focally, a fascicular growth and in these areas, the cells have elongated nuclei with an appearance similar to that described in smooth muscle tumors. The degree of nuclear atypia is variable and the mitotic rates are low in most cases [111,112,113, 189, 190]. Tumors with ≥2 of the following criteria are typically associated with a malignant behavior including gross size >5 cm, infiltrative growth, high-grade nuclear features, necrosis, vascular invasion, or a mitotic index ≥1/50 HPFs [188]. Unusual forms of PEComa have been reported including PEComatosis (multiple PEComas) [191,192,193] sclerosing PEComa (striking hyalinizing background stroma) [194] and TFE-3 mutated PEComas characterized by prominence of clear cells [188].


PEComa. The tumor cells have abundant pale cytoplasm and grow in sheets and cords (a) and are diffusely positive for HMB-45 (b)
Immunophenotype
The tumors are characteristically positive for HMB-45 (Fig. 22b), melanA, microphthalmia transcription factor (MiTF), cathepsinK, and TFE3 although the degree of positivity is variable and may be minimal for HMB45 and melan A [188] and are typically negative for S-100. They frequently express muscle markers, more often smooth muscle actin and desmin and much less commonly h-caldesmon, and may be positive for CD10, but they are negative for inhibin and keratin. In contrast to most PEComas, tumors composed predominantly of clear cells show diffuse TFE3, HMB45, and cathepsinK positivity with either focal or no melan A expression [188]. The coexpression of two melanocytic markers (HMB-45, melan A, microphthalmia transcription factor, cathepsinK, or TFE3) +/− muscle markers is diagnostic of this tumor [111, 113, 183, 189].
Intravenous Leiomyomatosis
Although this is a rare, histologically benign condition, characterized by a predominant intravascular proliferation of smooth muscle cells, it is included in this chapter because it may pursue an aggressive behavior, growing along the inferior vena cava into the right heart [195,196,197,198,199]. As intravenous leiomyomatosis is frequently associated with uterine leiomyomas, a diagnosis of intravenous leiomyomatosis should only be made when the intravascular growth is present beyond the confines or in the absence of a leiomyoma [155]. Extrauterine extension is most common within the broad ligament veins (up to 80 % of cases) and into the right heart (up to 40 % of cases) [155, 197]. This condition may occur at any age, but it is more common in middle-aged women.
Gross Features
In some occasions, the gross appearance is similar to that seen in a leiomyoma being more often multinodular [200]. White to yellow and firm to soft worm-like plugs of tumor may be seen filling and distending the myometrial veins, sometimes with extrauterine extension; however, not infrequently, it is not appreciated on initial gross examination of the uterus [155, 200, 201].
Histologic Features
On low-power examination, intravenous leiomyomatosis shows a prominent growth into vascular spaces. On high power, its appearance closely overlaps with that seen in typical leiomyomas [155]. The bland tumor cells form intersecting fascicles and display elongated nuclei with “blunt ends,” eosinophilic cytoplasm, and rare-to-absent mitotic activity [155, 200,201,202]. Leiomyoma variants have also been described including hydropic change, myxoid, epithelioid, highly cellular, lipoleiomyoma, and with bizarre nuclei [203,204,205].
Cytogenetics
It has been recently shown that recurrent loss of 22q12.3-q13.1 is common in intravenous leiomyomatosis, followed by losses of 22q11.23-q13.31, 1p36.13-p33, 2p25.3-p23.3, and 2q24.2-q32.2 and gains of 6p22.2, 2q37.3 and 10q22.2-q22.3, in decreasing order of frequency [206].
Conclusions
-
Endometrioid adenocarcinomas resemble, at least focally, proliferative-type endometrium showing tubular glands with smooth luminal surfaces, lined by mitotically active columnar cells
-
Based on the degree of glandular differentiation, endometrioid carcinomas are divided into three FIGO categories: grade 1: ≤5 % of solid non-glandular growth; grade 2: 6–50 % of solid non-glandular growth; and grade 3: >50 % of solid growth. The presence of marked cytologic atypia increases the grade by one.
-
The presence of extensive confluent papillary growth, macroglands, or cribriform architecture as well as marked cytologic atypia is diagnostic of adenocarcinoma and excludes endometrial hyperplasia.
-
The distinction between endometrial carcinoma and endocervical carcinoma or between high-grade endometrioid- carcinoma and serous carcinoma may be very difficult on a curettage specimen.
-
Mucinous, ciliated, secretory, and villoglandular carcinomas are related to endometrioid carcinomas.
-
Serous carcinomas may be very small or even confined to a polyp or the endometrium but they are always of high grade and frequently have extrauterine spread. They typically show p53 overexpression and they are ER and PR positive in <50 % of cases.
-
Clear cell carcinoma is uncommonly ER and PR positive and p53 overexpression is significantly less frequent than in serous carcinoma.
-
The specific diagnostic criteria for the different subtypes of leiomyosarcomas differ.
-
A combination of any two of the following three features establishes the diagnosis of spindled leiomyosarcoma: diffuse moderate-to-severe atypia, ≥10 mitoses/10 HPFs, and tumor cell necrosis.
-
The criteria to establish the diagnosis of malignancy are not well established in epithelioid smooth muscle tumors. As a general rule, this diagnosis is warranted when there are ≥5 mitoses/10 HPFs and diffuse moderate-to-severe cytologic atypia or tumor cell necrosis.
-
The diagnosis of myxoid leiomyosarcoma is warranted when either marked cytologic atypia or tumor cell necrosis is identified. In their absence, the finding of ≥2 mitoses/10 HPFs separates myxoid leiomyosarcoma from myxoid leiomyoma.
-
Clinicians should be made aware that pathologists cannot distinguish between endometrial stromal nodule and low-grade endometrial stromal sarcoma in a curettage specimen in most instances; the most important feature in this differential diagnosis, the status of the tumor myometrial interface, cannot be assessed in this setting.
-
A new category of high-grade endometrial stromal sarcoma has been included in the latest WHO classification which is defined by relatively small epithelioid cells growing in sheets or nests associated with cytologic atypia and brisk mitotic activity. The tumor is typically CD10, ER, and PR negative and CyclinD1 positive and shows a t(10,17) in contrast to the t(7,17) observed in >50 % of low-grade endometrial stromal sarcomas.
-
A diagnosis of high-grade endometrial stromal sarcoma can also be applied when the tumor has arisen in the context of a low-grade endometrial stromal sarcoma. However, it is important to be aware that these tumors behave in a very aggressive fashion.
-
The diagnosis of undifferentiated uterine sarcoma is a diagnosis of exclusion as this is a high-grade sarcoma without specific histologic features.
-
The most important histologic parameters in the prognosis of low-grade müllerian adenosarcoma are myometrial invasion and sarcomatous overgrowth.
-
Malignant mixed müllerian tumors arise either from a common pluripotential cell with divergent differentiation or by progression from the carcinomatous component by a metaplastic process or dedifferentiation, coexpressing epithelial and mesenchymal markers.
-
PEComas are rare uterine tumors that belong to the family of neoplasms thought to originate from the perivascular epithelioid cell (PEC), which is defined by the presence of abundant clear to eosinophilic granular cytoplasm, positivity for melanocytic markers (HMB-45, melan A, microphthalmia transcription factor, cathepsinK, and TFE3) with or without expression of muscle markers.
-
Intravenous leiomyomatosis is a proliferation of histologically benign smooth muscle growing in vascular spaces. It may be seen in the absence of leiomyomas or outside the confines of leiomyomas. It has commonly extrauterine extension which may be responsible of an aggressive behavior.
References
Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. 1983;15(1):10–7.
Kandoth C, Schultz N, Cherniack AD, et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73.
Alvarez T, Miller E, Duska L, Oliva E. Molecular profile of grade 3 endometrioid endometrial carcinoma: is it a type I or type II endometrial carcinoma? Am J Surg Pathol. 2012;36(5):753–61.
Alkushi A, Abdul-Rahman ZH, Lim P, et al. Description of a novel system for grading of endometrial carcinoma and comparison with existing grading systems. Am J Surg Pathol. 2005;29(3):295–304.
Conlon N, Leitao Jr MM, Abu-Rustum NR, Soslow RA. Grading uterine endometrioid carcinoma: a proposal that binary is best. Am J Surg Pathol. 2014;38(12):1583–7.
Lax SF, Kurman RJ, Pizer ES, Wu L, Ronnett BM. A binary architectural grading system for uterine endometrial endometrioid carcinoma has superior reproducibility compared with FIGO grading and identifies subsets of advance-stage tumors with favorable and unfavorable prognosis. Am J Surg Pathol. 2000;24(9):1201–8.
Murray SK, Young RH, Scully RE. Uterine endometrioid carcinoma with small nonvillous papillae: an analysis of 26 Cases of a favorable-prognosis tumor to be distinguished from serous carcinoma. Int J Surg Pathol. 2000;8(4):279–89.
Murray SK, Clement PB, Young RH. Endometrioid carcinomas of the uterine corpus with sex cord-like formations, hyalinization, and other unusual morphologic features: a report of 31 cases of a neoplasm that may be confused with carcinosarcoma and other uterine neoplasms. Am J Surg Pathol. 2005;29(2):157–66.
Quick CM, May T, Horowitz NS, Nucci MR. Low-grade, low-stage endometrioid endometrial adenocarcinoma: a clinicopathologic analysis of 324 cases focusing on frequency and pattern of myoinvasion. Int J Gynecol Pathol. 2012;31(4):337–43.
Longacre TA, Hendrickson MR. Diffusely infiltrative endometrial adenocarcinoma: an adenoma malignum pattern of myoinvasion. Am J Surg Pathol. 1999;23(1):69–78.
Murray SK, Young RH, Scully RE. Unusual epithelial and stromal changes in myoinvasive endometrioid adenocarcinoma: a study of their frequency, associated diagnostic problems, and prognostic significance. Int J Gynecol Pathol. 2003;22(4):324–33.
Kurman RJ, Norris HJ. Evaluation of criteria for distinguishing atypical endometrial hyperplasia from well-differentiated carcinoma. Cancer. 1982;49(12):2547–59.
Longacre TA, Chung MH, Jensen DN, Hendrickson MR. Proposed criteria for the diagnosis of well-differentiated endometrial carcinoma. A diagnostic test for myoinvasion. Am J Surg Pathol. 1995;19(4):371–406.
Norris HJ, Tavassoli FA, Kurman RJ. Endometrial hyperplasia and carcinoma. Diagnostic considerations. Am J Surg Pathol. 1983;7(8):839–47.
Melhem MF, Tobon H. Mucinous adenocarcinoma of the endometrium: a clinico-pathological review of 18 cases. Int J Gynecol Pathol. 1987;6(4):347–55.
Ross JC, Eifel PJ, Cox RS, Kempson RL, Hendrickson MR. Primary mucinous adenocarcinoma of the endometrium. A clinicopathologic and histochemical study. Am J Surg Pathol. 1983;7(8):715–29.
Hendrickson MR, Kempson RL. Ciliated carcinoma--a variant of endometrial adenocarcinoma: a report of 10 cases. Int J Gynecol Pathol. 1983;2(1):1–12.
Tobon H, Watkins GJ. Secretory adenocarcinoma of the endometrium. Int J Gynecol Pathol. 1985;4(4):328–35.
Chen JL, Trost DC, Wilkinson EJ. Endometrial papillary adenocarcinomas: two clinicopathological types. Int J Gynecol Pathol. 1985;4(4):279–88.
Parkash V, Carcangiu ML. Endometrioid endometrial adenocarcinoma with psammoma bodies. Am J Surg Pathol. 1997;21(4):399–406.
Hedrick Ellenson L, Ronnett BM, Soslow RA, Zaino RJ, Kurman RJ. Endometrial carcinoma. In: Kurman RJ, Hedrick Ellenson L, Ronnett BM, editors. Blaustein’s Pathology of the Female Genital Tract. New York:Springer; 2011. p. 407–8.
Dabbs DJ, Geisinger KR, Norris HT. Intermediate filaments in endometrial and endocervical carcinomas. The diagnostic utility of vimentin patterns. Am J Surg Pathol. 1986;10(8):568–76.
Dabbs DJ, Sturtz K, Zaino RJ. The immunohistochemical discrimination of endometrioid adenocarcinomas. Hum Pathol. 1996;27(2):172–7.
Dallenbach-Hellweg G, Lang-Averous G, Hahn U. The value of immunohistochemistry in the differential diagnosis of endometrial carcinomas. APMIS Suppl. 1991;23:91–9.
McCluggage WG, Sumathi VP, McBride HA, Patterson A. A panel of immunohistochemical stains, including carcinoembryonic antigen, vimentin, and estrogen receptor, aids the distinction between primary endometrial and endocervical adenocarcinomas. Int J Gynecol Pathol. 2002;21(1):11–5.
Castrillon DH, Lee KR, Nucci MR. Distinction between endometrial and endocervical adenocarcinoma: an immunohistochemical study. Int J Gynecol Pathol. 2002;21(1):4–10.
Wang NP, Zee S, Zarbo RJ, Bacchi CE, Gown AM. Coordinate expression of cytokeratins 7 and 20 defines unique subsets of carcinomas. Appl Immunohistochem. 1995;3(2):99–107.
Ginath S, Menczer J, Fintsi Y, Ben-Shem E, Glezerman M, Avinoach I. Tissue and serum CA125 expression in endometrial cancer. Int J Gynecol Cancer. 2002;12(4):372–5.
Cherchi PL, Bosincu L, Dessole S, et al. Immunohistochemical expression of BerEP4, a new epithelial antigen, in endometrial carcinoma: correlation with clinical parameters. Eur J Gynaecol Oncol. 1999;20(5–6):393–5.
Katari RS, Fernsten PD, Schlom J. Characterization of the shed form of the human tumor-associated glycoprotein (TAG-72) from serous effusions of patients with different types of carcinomas. Cancer Res. 1990;50(16):4885–90.
Reid-Nicholson M, Iyengar P, Hummer AJ, Linkov I, Asher M, Soslow RA. Immunophenotypic diversity of endometrial adenocarcinomas: implications for differential diagnosis. Mod Pathol. 2006;19(8):1091–100.
Soslow RA, Shen PU, Chung MH, Isacson C, Baergen RN. Cyclin D1 expression in high-grade endometrial carcinomas--association with histologic subtype. Int J Gynecol Pathol. 2000;19(4):329–34.
Lax SF, Kendall B, Tashiro H, Slebos RJ, Hedrick L. The frequency of p53, K-ras mutations, and microsatellite instability differs in uterine endometrioid and serous carcinoma: evidence of distinct molecular genetic pathways. Cancer. 2000;88(4):814–24.
Sherman ME, Bur ME, Kurman RJ. p53 in endometrial cancer and its putative precursors: evidence for diverse pathways of tumorigenesis. Hum Pathol. 1995;26(11):1268–74.
Brachtel EF, Sanchez-Estevez C, Moreno-Bueno G, Prat J, Palacios J, Oliva E. Distinct molecular alterations in complex endometrial hyperplasia (CEH) with and without immature squamous metaplasia (squamous morules). Am J Surg Pathol. 2005;29(10):1322–9.
Schlosshauer PW, Ellenson LH, Soslow RA. Beta-catenin and E-cadherin expression patterns in high-grade endometrial carcinoma are associated with histological subtype. Mod Pathol. 2002;15(10):1032–7.
Gehrig PA, Bae-Jump VL, Boggess JF, Groben PA, Fowler Jr WC, Van Le L. Association between uterine serous carcinoma and breast cancer. Gynecol Oncol. 2004;94(1):208–11.
Geisler JP, Sorosky JI, Duong HL, et al. Papillary serous carcinoma of the uterus: increased risk of subsequent or concurrent development of breast carcinoma. Gynecol Oncol. 2001;83(3):501–3.
Magriples U, Naftolin F, Schwartz PE, Carcangiu ML. High-grade endometrial carcinoma in tamoxifen-treated breast cancer patients. J Clin Oncol. 1993;11(3):485–90.
Olson SH, Finstad CL, Harlap S, Kurian L, Saigo PE, Barakat RR. A case-case analysis of factors related to overexpression of p53 in endometrial cancer following breast cancer. Cancer Epidemiol Biomarkers Prev. 1997;6(10):815–7.
Parkash V, Carcangiu ML. Uterine papillary serous carcinoma after radiation therapy for carcinoma of the cervix. Cancer. 1992;69(2):496–501.
Pothuri B, Ramondetta L, Martino M, et al. Development of endometrial cancer after radiation treatment for cervical carcinoma. Obstet Gynecol. 2003;101(5 Pt 1):941–5.
Carcangiu ML, Chambers JT. Uterine papillary serous carcinoma: a study on 108 cases with emphasis on the prognostic significance of associated endometrioid carcinoma, absence of invasion, and concomitant ovarian carcinoma. Gynecol Oncol. 1992;47(3):298–305.
Hendrickson M, Ross J, Eifel P, Martinez A, Kempson R. Uterine papillary serous carcinoma: a highly malignant form of endometrial adenocarcinoma. Am J Surg Pathol. 1982;6(2):93–108.
Ambros RA, Sherman ME, Zahn CM, Bitterman P, Kurman RJ. Endometrial intraepithelial carcinoma: a distinctive lesion specifically associated with tumors displaying serous differentiation. Hum Pathol. 1995;26(11):1260–7.
Spiegel GW. Endometrial carcinoma in situ in postmenopausal women. Am J Surg Pathol. 1995;19(4):417–32.
Darvishian F, Hummer AJ, Thaler HT, et al. Serous endometrial cancers that mimic endometrioid adenocarcinomas: a clinicopathologic and immunohistochemical study of a group of problematic cases. Am J Surg Pathol. 2004;28(12):1568–78.
Demopoulos RI, Mesia AF, Mittal K, Vamvakas E. Immunohistochemical comparison of uterine papillary serous and papillary endometrioid carcinoma: clues to pathogenesis. Int J Gynecol Pathol. 1999;18(3):233–7.
Tashiro H, Isacson C, Levine R, Kurman RJ, Cho KR, Hedrick L. p53 gene mutations are common in uterine serous carcinoma and occur early in their pathogenesis. Am J Pathol. 1997;150(1):177–85.
An HJ, Logani S, Isacson C, Ellenson LH. Molecular characterization of uterine clear cell carcinoma. Mod Pathol. 2004;17(5):530–7.
Lax SF, Pizer ES, Ronnett BM, Kurman RJ. Clear cell carcinoma of the endometrium is characterized by a distinctive profile of p53, Ki-67, estrogen, and progesterone receptor expression. Hum Pathol. 1998;29(6):551–8.
Carcangiu ML, Dorji T, Radice P, Bertario L, Sala P. HNPCC-related endometrial carcinomas show a high frequency of non-endometrioid types and of high FIGO grade endometrioid carcinomas. Mod Pathol. 2006;19(1S):173A.
Vang R, Whitaker BP, Farhood AI, Silva EG, Ro JY, Deavers MT. Immunohistochemical analysis of clear cell carcinoma of the gynecologic tract. Int J Gynecol Pathol. 2001;20(3):252–9.
Fadare O, Desouki MM, Gwin K, et al. Frequent expression of napsin A in clear cell carcinoma of the endometrium: potential diagnostic utility. Am J Surg Pathol. 2014;38(2):189–96.
Fadare O, Liang SX. Diagnostic utility of hepatocyte nuclear factor 1-beta immunoreactivity in endometrial carcinomas: lack of specificity for endometrial clear cell carcinoma. Appl Immunohistochem Mol Morphol. 2012;20(6):580–7.
Zaino R, Carinelli SG, Ellenson LH, et al. Epithelial tumours and precursors. Chapter 5, Tumours of the uterine corpus. In: Kurman R, Carcangiu ML, Herrington CS, Young RH, editors. WHO classification of tumours of female reproductive organs. Lyon: IARC Press; 2014. p. 125–35.
Goodman A, Zukerberg LR, Rice LW, Fuller AF, Young RH, Scully RE. Squamous cell carcinoma of the endometrium: a report of eight cases and a review of the literature. Gynecol Oncol. 1996;61(1):54–60.
Lininger RA, Ashfaq R, Albores-Saavedra J, Tavassoli FA. Transitional cell carcinoma of the endometrium and endometrial carcinoma with transitional cell differentiation. Cancer. 1997;79(10):1933–43.
Spiegel GW, Austin RM, Gelven PL. Transitional cell carcinoma of the endometrium. Gynecol Oncol. 1996;60(2):325–30.
Abeler VM, Kjorstad KE, Nesland JM. Undifferentiated carcinoma of the endometrium. A histopathologic and clinical study of 31 cases. Cancer. 1991;68(1):98–105.
Altrabulsi B, Malpica A, Deavers MT, Bodurka DC, Broaddus R, Silva EG. Undifferentiated carcinoma of the endometrium. Am J Surg Pathol. 2005;29(10):1316–21.
Toro JR, Travis LB, Wu HJ, Zhu K, Fletcher CD, Devesa SS. Incidence patterns of soft tissue sarcomas, regardless of primary site, in the surveillance, epidemiology and end results program, 1978-2001: an analysis of 26,758 cases. Int J Cancer. 2006;119(12):2922–30.
Harlow BL, Weiss NS, Lofton S. The epidemiology of sarcomas of the uterus. J Natl Cancer Inst. 1986;76(3):399–402.
Schwartz PE, Kelly MG. Malignant transformation of myomas: myth or reality? Obstet Gynecol Clin North Am. 2006;33(1):183–98. xii.
Mittal KR, Chen F, Wei JJ, et al. Molecular and immunohistochemical evidence for the origin of uterine leiomyosarcomas from associated leiomyoma and symplastic leiomyoma-like areas. Mod Pathol. 2009;22(10):1303–11.
Launonen V, Vierimaa O, Kiuru M, et al. Inherited susceptibility to uterine leiomyomas and renal cell cancer. Proc Natl Acad Sci U S A. 2001;98(6):3387–92.
Rammeh-Rommani S, Mokni M, Stita W, et al. [Uterine smooth muscle tumors: retrospective epidemiological and pathological study of 2760 cases]. J Gynecol Obstet Biol Reprod (Paris). 2005;34(6):568–71.
Schwartz LB, Diamond MP, Schwartz PE. Leiomyosarcomas: clinical presentation. Am J Obstet Gynecol. 1993;168(1 Pt 1):180–3.
Oliva ECP, Young RH. Mesenchymal tumors of the uterus: selected topics emphasizing potential pitfalls. Curr Diagn Pathol. 2002;8:268–82.
Bell SW, Kempson RL, Hendrickson MR. Problematic uterine smooth muscle neoplasms. A clinicopathologic study of 213 cases. Am J Surg Pathol. 1994;18(6):535–58.
Chiang S, Oliva E. Recent developments in uterine mesenchymal neoplasms. Histopathology. 2013;62(1):124–37.
Lim D, Alvarez T, Nucci MR, et al. Interobserver variability in the interpretation of tumor cell necrosis in uterine leiomyosarcoma. Am J Surg Pathol. 2013;37(5):650–8.
Tapia C, Kutzner H, Mentzel T, Savic S, Baumhoer D, Glatz K. Two mitosis-specific antibodies, MPM-2 and phospho-histone H3 (Ser28), allow rapid and precise determination of mitotic activity. Am J Surg Pathol. 2006;30(1):83–9.
Veras E, Malpica A, Deavers MT, Silva EG. Mitosis-specific marker phospho-histone H3 in the assessment of mitotic index in uterine smooth muscle tumors: a pilot study. Int J Gynecol Pathol. 2009;28(4):316–21.
Hornick JL, Fletcher CD. Criteria for malignancy in nonvisceral smooth muscle tumors. Ann Diagn Pathol. 2003;7(1):60–6.
Veras E, Zivanovic O, Jacks L, Chiappetta D, Hensley M, Soslow R. “Low-grade leiomyosarcoma” and late-recurring smooth muscle tumors of the uterus: a heterogenous collection of frequently misdiagnosed tumors associated with an overall favorable prognosis relative to conventional uterine leiomyosarcomas. Am J Surg Pathol. 2011;35(11):1626–37.
Tavassoli F. World Health Organization classification of tumours. In: Tavassoli F, Devilee P, editors. Pathology and genetics of tumors of breast and female genital organs. Lyon: IARC Press; 2003.
Burns B, Curry RH, Bell ME. Morphologic features of prognostic significance in uterine smooth muscle tumors: a review of eighty-four cases. Am J Obstet Gynecol. 1979;135(1):109–14.
Coard KC, Fletcher HM. Leiomyosarcoma of the uterus with a florid intravascular component (“intravenous leiomyosarcomatosis”). Int J Gynecol Pathol. 2002;21(2):182–5.
Kurman RJ, Norris HJ. Mesenchymal tumors of the uterus. VI. Epithelioid smooth muscle tumors including leiomyoblastoma and clear-cell leiomyoma: a clinical and pathologic analysis of 26 cases. Cancer. 1976;37(4):1853–65.
Prayson RA, Goldblum JR, Hart WR. Epithelioid smooth-muscle tumors of the uterus: a clinicopathologic study of 18 patients. Am J Surg Pathol. 1997;21(4):383–91.
Oliva E, Nielsen GP, Clement PB, et al. Epithelioid smooth muscle tumors of the uterus: a clinicopathologic analysis of 80 cases. Mod Pathol. 1997;10:107A.
Atkins K, Bell SW, Kempson RL. Myxoid smooth muscle tumors of the uterus. Mod Pathol. 2001;14:132A.
Burch DM, Tavassoli FA. Myxoid leiomyosarcoma of the uterus. Histopathology. 2011;59(6):1144–55.
Chen KT. Myxoid leiomyosarcoma of the uterus. Int J Gynecol Pathol. 1984;3(4):389–92.
King ME, Dickersin GR, Scully RE. Myxoid leiomyosarcoma of the uterus. A report of six cases. Am J Surg Pathol. 1982;6(7):589–98.
Pounder DJ, Iyer PV. Uterine leiomyosarcoma with myxoid stroma. Arch Pathol Lab Med. 1985;109(8):762–4.
Salm R, Evans DJ. Myxoid leiomyosarcoma. Histopathology. 1985;9(2):159–69.
Oliva E, Young RH, Amin MB, Clement PB. An immunohistochemical analysis of endometrial stromal and smooth muscle tumors of the uterus: a study of 54 cases emphasizing the importance of using a panel because of overlap in immunoreactivity for individual antibodies. Am J Surg Pathol. 2002;26(4):403–12.
Loddenkemper C, Mechsner S, Foss HD, et al. Use of oxytocin receptor expression in distinguishing between uterine smooth muscle tumors and endometrial stromal sarcoma. Am J Surg Pathol. 2003;27(11):1458–62.
Leitao MM, Soslow RA, Nonaka D, et al. Tissue microarray immunohistochemical expression of estrogen, progesterone, and androgen receptors in uterine leiomyomata and leiomyosarcoma. Cancer. 2004;101(6):1455–62.
Iwata J, Fletcher CD. Immunohistochemical detection of cytokeratin and epithelial membrane antigen in leiomyosarcoma: a systematic study of 100 cases. Pathol Int. 2000;50(1):7–14.
Anderson SE, Nonaka D, Chuai S, et al. p53, epidermal growth factor, and platelet-derived growth factor in uterine leiomyosarcoma and leiomyomas. Int J Gynecol Cancer. 2006;16(2):849–53.
Leath 3rd CA, Straughn Jr JM, Conner MG, et al. Immunohistochemical evaluation of the c-kit proto-oncogene in sarcomas of the uterus: a case series. J Reprod Med. 2004;49(2):71–5.
Raspollini MR, Pinzani P, Simi L, et al. Uterine leiomyosarcomas express KIT protein but lack mutation(s) in exon 9 of c-KIT. Gynecol Oncol. 2005;98(2):334–5.
Mills AM, Ly A, Balzer BL, et al. Cell cycle regulatory markers in uterine atypical leiomyoma and leiomyosarcoma: immunohistochemical study of 68 cases with clinical follow-up. Am J Surg Pathol. 2013;37(5):634–42.
D'Angelo E, Espinosa I, Ali R, et al. Uterine leiomyosarcomas: tumor size, mitotic index, and biomarkers Ki67, and Bcl-2 identify two groups with different prognosis. Gynecol Oncol. 2011;121(2):328–33.
Bertsch E, Qiang W, Zhang Q, et al. MED12 and HMGA2 mutations: two independent genetic events in uterine leiomyoma and leiomyosarcoma. Mod Pathol. 2014;27(8):1144–53.
Matsubara A, Sekine S, Yoshida M, et al. Prevalence of MED12 mutations in uterine and extrauterine smooth muscle tumours. Histopathology. 2013;62(4):657–61.
Schwetye KE, Pfeifer JD, Duncavage EJ. MED12 exon 2 mutations in uterine and extrauterine smooth muscle tumors. Hum Pathol. 2014;45(1):65–70.
Perrone T, Dehner LP. Prognostically favorable “mitotically active” smooth-muscle tumors of the uterus. A clinicopathologic study of ten cases. Am J Surg Pathol. 1988;12(1):1–8.
Prayson RA, Hart WR. Mitotically active leiomyomas of the uterus. Am J Clin Pathol. 1992;97(1):14–20.
Myles JL, Hart WR. Apoplectic leiomyomas of the uterus. A clinicopathologic study of five distinctive hemorrhagic leiomyomas associated with oral contraceptive usage. Am J Surg Pathol. 1985;9(11):798–805.
Norris HJ, Hilliard GD, Irey NS. Hemorrhagic cellular leiomyomas (“apoplectic leiomyoma”) of the uterus associated with pregnancy and oral contraceptives. Int J Gynecol Pathol. 1988;7(3):212–24.
Lim D, Ip PP, Cheung AN, Kiyokawa T, Oliva E. Immunohistochemical comparison of ovarian and uterine endometrioid carcinoma, endometrioid carcinoma with clear cell change and clear cell carcinoma. Am J Surg Pathol. 2015;39:1061–9.
Croce S, Young RH, Oliva E. Uterine leiomyomas with bizarre nuclei: a clinicopathologic study of 59 cases. Am J Surg Pathol. 2014;38(10):1330–9.
Downes KA, Hart WR. Bizarre leiomyomas of the uterus: a comprehensive pathologic study of 24 cases with long-term follow-up. Am J Surg Pathol. 1997;21(11):1261–70.
McCluggage WG, Lioe TF, McClelland HR, Lamki H. Rhabdomyosarcoma of the uterus: report of two cases, including one of the spindle cell variant. Int J Gynecol Cancer. 2002;12(1):128–32.
Kurihara S, Oda Y, Ohishi Y, et al. Endometrial stromal sarcomas and related high-grade sarcomas: immunohistochemical and molecular genetic study of 31 cases. Am J Surg Pathol. 2008;32(8):1228–38.
Baergen RN, Rutgers JL, Young RH, Osann K, Scully RE. Placental site trophoblastic tumor: a study of 55 cases and review of the literature emphasizing factors of prognostic significance. Gynecol Oncol. 2006;100(3):511–20.
Folpe AL, Mentzel T, Lehr HA, Fisher C, Balzer BL, Weiss SW. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature. Am J Surg Pathol. 2005;29(12):1558–75.
Schoolmeester JK, Howitt BE, Hirsch MS, Dal Cin P, Quade BJ, Nucci MR. Perivascular epithelioid cell neoplasm (PEComa) of the gynecologic tract: clinicopathologic and immunohistochemical characterization of 16 cases. Am J Surg Pathol. 2014;38(2):176–88.
Vang R, Kempson RL. Perivascular epithelioid cell tumor (‘PEComa’) of the uterus: a subset of HMB-45-positive epithelioid mesenchymal neoplasms with an uncertain relationship to pure smooth muscle tumors. Am J Surg Pathol. 2002;26(1):1–13.
Clement PB, Scully RE. Uterine tumors resembling ovarian sex-cord tumors. A clinicopathologic analysis of fourteen cases. Am J Clin Pathol. 1976;66(3):512–25.
Irving JA, Carinelli S, Prat J. Uterine tumors resembling ovarian sex cord tumors are polyphenotypic neoplasms with true sex cord differentiation. Mod Pathol. 2006;19(1):17–24.
Krishnamurthy S, Jungbluth AA, Busam KJ, Rosai J. Uterine tumors resembling ovarian sex-cord tumors have an immunophenotype consistent with true sex-cord differentiation. Am J Surg Pathol. 1998;22(9):1078–82.
Nielsen GP, Oliva E, Young RH, Rosenberg AE, Dickersin GR, Scully RE. Alveolar soft-part sarcoma of the female genital tract: a report of nine cases and review of the literature. Int J Gynecol Pathol. 1995;14(4):283–92.
Roma AA, Yang B, Senior ME, Goldblum JR. TFE3 immunoreactivity in alveolar soft part sarcoma of the uterine cervix: case report. Int J Gynecol Pathol. 2005;24(2):131–5.
Giordano G, Gnetti L, Ricci R, Merisio C, Melpignano M. Metastatic extragenital neoplasms to the uterus: a clinicopathologic study of four cases. Int J Gynecol Cancer. 2006;16 Suppl 1:433–8.
Clement PB, Young RH, Scully RE. Diffuse, perinodular, and other patterns of hydropic degeneration within and adjacent to uterine leiomyomas. Problems in differential diagnosis. Am J Surg Pathol. 1992;16(1):26–32.
Parra-Herran C et al. Am J Surg Pathol 2015; 39:157–68
Oliva E, Carcangiu ML, Carinelli S, et al. Mesenchymal tumours. In: Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. WHO classification of tumours of female reproductive organs. Lyon: IARC Press; 2014. p. 135–47.
Chang KL, Crabtree GS, Lim-Tan SK, Kempson RL, Hendrickson MR. Primary uterine endometrial stromal neoplasms. A clinicopathologic study of 117 cases. Am J Surg Pathol. 1990;14(5):415–38.
Oliva E, Clement PB, Young RH. Endometrial stromal tumors: an update on a group of tumors with a protean phenotype. Adv Anat Pathol. 2000;7(5):257–81.
Oliva E, Clement PB, Young RH, Scully RE. Mixed endometrial stromal and smooth muscle tumors of the uterus: a clinicopathologic study of 15 cases. Am J Surg Pathol. 1998;22(8):997–1005.
Baker PM, Moch H, Oliva E. Unusual morphologic features of endometrial stromal tumors: a report of 2 cases. Am J Surg Pathol. 2005;29(10):1394–8.
Oliva E, Young RH, Clement PB, Scully RE. Myxoid and fibrous endometrial stromal tumors of the uterus: a report of 10 cases. Int J Gynecol Pathol. 1999;18(4):310–9.
Yilmaz A, Rush DS, Soslow RA. Endometrial stromal sarcomas with unusual histologic features: a report of 24 primary and metastatic tumors emphasizing fibroblastic and smooth muscle differentiation. Am J Surg Pathol. 2002;26(9):1142–50.
Clement PB, Scully RE. Endometrial stromal sarcomas of the uterus with extensive endometrioid glandular differentiation: a report of three cases that caused problems in differential diagnosis. Int J Gynecol Pathol. 1992;11(3):163–73.
Levine PH, Abou-Nassar S, Mittal K. Extrauterine low-grade endometrial stromal sarcoma with florid endometrioid glandular differentiation. Int J Gynecol Pathol. 2001;20(4):395–8.
McCluggage WG, Date A, Bharucha H, Toner PG. Endometrial stromal sarcoma with sex cord-like areas and focal rhabdoid differentiation. Histopathology. 1996;29(4):369–74.
Lifschitz-Mercer B, Czernobilsky B, Dgani R, Dallenbach-Hellweg G, Moll R, Franke WW. Immunocytochemical study of an endometrial diffuse clear cell stromal sarcoma and other endometrial stromal sarcomas. Cancer. 1987;59(8):1494–9.
Oliva E, Clement PB, Young RH. Epithelioid endometrial and endometrioid stromal tumors: a report of four cases emphasizing their distinction from epithelioid smooth muscle tumors and other oxyphilic uterine and extrauterine tumors. Int J Gynecol Pathol. 2002;21(1):48–55.
Kim YH, Cho H, Kyeom-Kim H, Kim I. Uterine endometrial stromal sarcoma with rhabdoid and smooth muscle differentiation. J Korean Med Sci. 1996;11(1):88–93.
Fadare O, McCalip B, Mariappan MR, Hileeto D, Parkash V. An endometrial stromal tumor with osteoclast-like giant cells. Ann Diagn Pathol. 2005;9(3):160–5.
McCluggage WG, Young RH. Endometrial stromal sarcomas with true papillae and pseudopapillae. Int J Gynecol Pathol. 2008;27(4):555–61.
Chu P, Arber DA. Paraffin-section detection of CD10 in 505 nonhematopoietic neoplasms. Frequent expression in renal cell carcinoma and endometrial stromal sarcoma. Am J Clin Pathol. 2000;113(3):374–82.
Farhood AI, Abrams J. Immunohistochemistry of endometrial stromal sarcoma. Hum Pathol. 1991;22(3):224–30.
Lillemoe TJ, Perrone T, Norris HJ, Dehner LP. Myogenous phenotype of epithelial-like areas in endometrial stromal sarcomas. Arch Pathol Lab Med. 1991;115(3):215–9.
Wu TI, Chou HH, Yeh CJ, et al. Clinicopathologic parameters and immunohistochemical study of endometrial stromal sarcomas. Int J Gynecol Pathol. 2013;32(5):482–92.
Moinfar F, Regitnig P, Tabrizi AD, Denk H, Tavassoli FA. Expression of androgen receptors in benign and malignant endometrial stromal neoplasms. Virchows Arch. 2004;444(5):410–4.
de Leval L, Waltregny D, Boniver J, Young RH, Castronovo V, Oliva E. Use of histone deacetylase 8 (HDAC8), a new marker of smooth muscle differentiation, in the classification of mesenchymal tumors of the uterus. Am J Surg Pathol. 2006;30(3):319–27.
Franquemont DW, Frierson Jr HF, Mills SE. An immunohistochemical study of normal endometrial stroma and endometrial stromal neoplasms. Evidence for smooth muscle differentiation. Am J Surg Pathol. 1991;15(9):861–70.
Rush DS, Tan J, Baergen RN, Soslow RA. h-Caldesmon, a novel smooth muscle-specific antibody, distinguishes between cellular leiomyoma and endometrial stromal sarcoma. Am J Surg Pathol. 2001;25(2):253–8.
Baker RJ, Hildebrandt RH, Rouse RV, Hendrickson MR, Longacre TA. Inhibin and CD99 (MIC2) expression in uterine stromal neoplasms with sex-cord-like elements. Hum Pathol. 1999;30(6):671–9.
Sumathi VP, Al-Hussaini M, Connolly LE, Fullerton L, McCluggage WG. Endometrial stromal neoplasms are immunoreactive with WT-1 antibody. Int J Gynecol Pathol. 2004;23(3):241–7.
Geller MA, Argenta P, Bradley W, et al. Treatment and recurrence patterns in endometrial stromal sarcomas and the relation to c-kit expression. Gynecol Oncol. 2004;95(3):632–6.
Hrzenjak A, Tippl M, Kremser ML, et al. Inverse correlation of secreted frizzled-related protein 4 and beta-catenin expression in endometrial stromal sarcomas. J Pathol. 2004;204(1):19–27.
Reich O, Regauer S. Aromatase expression in low-grade endometrial stromal sarcomas: an immunohistochemical study. Mod Pathol. 2004;17(1):104–8.
Chiang S, Oliva E. Cytogenetic and molecular aberrations in endometrial stromal tumors. Hum Pathol. 2011;42(5):609–17.
Sandberg AA. The cytogenetics and molecular biology of endometrial stromal sarcoma. Cytogenet Genome Res. 2007;118(2–4):182–9.
Dionigi A, Oliva E, Clement PB, Young RH. Endometrial stromal nodules and endometrial stromal tumors with limited infiltration: a clinicopathologic study of 50 cases. Am J Surg Pathol. 2002;26(5):567–81.
Oliva E. Cellular mesenchymal tumors of the uterus: a review emphasizing recent observations. Int J Gynecol Pathol. 2014;33(4):374–84.
Oliva E, Young RH, Clement PB, Bhan AK, Scully RE. Cellular benign mesenchymal tumors of the uterus. A comparative morphologic and immunohistochemical analysis of 33 highly cellular leiomyomas and six endometrial stromal nodules, two frequently confused tumors. Am J Surg Pathol. 1995;19(7):757–68.
Goldblum JR, Clement PB, Hart WR. Adenomyosis with sparse glands. A potential mimic of low-grade endometrial stromal sarcoma. Am J Clin Pathol. 1995;103(2):218–23.
Clement PB. Intravenous leiomyomatosis of the uterus. Pathol Annu. 1988;23(Pt 2):153–83.
Gilks CB, Clement PB, Hart WR, Young RH. Uterine adenomyomas excluding atypical polypoid adenomyomas and adenomyomas of endocervical type: a clinicopathologic study of 30 cases of an underemphasized lesion that may cause diagnostic problems with brief consideration of adenomyomas of other female genital tract sites. Int J Gynecol Pathol. 2000;19(3):195–205.
Clement PB, Scully RE. Mullerian adenosarcoma of the uterus: a clinicopathologic analysis of 100 cases with a review of the literature. Hum Pathol. 1990;21(4):363–81.
Lee CH, Marino-Enriquez A, Ou W, et al. The clinicopathologic features of YWHAE-FAM22 endometrial stromal sarcomas: a histologically high-grade and clinically aggressive tumor. Am J Surg Pathol. 2012;36(5):641–53.
Major FJ, Blessing JA, Silverberg SG, et al. Prognostic factors in early-stage uterine sarcoma. A Gynecologic Oncology Group study. Cancer. 1993;71(4 Suppl):1702–9.
Clement PB, Oliva E, Young RH. Mullerian adenosarcoma of the uterine corpus associated with tamoxifen therapy: a report of six cases and a review of tamoxifen-associated endometrial lesions. Int J Gynecol Pathol. 1996;15(3):222–9.
Clarke BA, Mulligan AM, Irving JA, McCluggage WG, Oliva E. Mullerian adenosarcomas with unusual growth patterns: staging issues. Int J Gynecol Pathol. 2011;30(4):340–7.
Howitt BE, Quade BJ, Nucci MR. Uterine polyps with features overlapping with those of Mullerian adenosarcoma: a clinicopathologic analysis of 29 cases emphasizing their likely benign nature. Am J Surg Pathol. 2015;39(1):116–26.
Gallardo A, Prat J. Mullerian adenosarcoma: a clinicopathologic and immunohistochemical study of 55 cases challenging the existence of adenofibroma. Am J Surg Pathol. 2009;33(2):278–88.
Clement PB, Scully RE. Mullerian adenosarcomas of the uterus with sex cord-like elements. A clinicopathologic analysis of eight cases. Am J Clin Pathol. 1989;91(6):664–72.
Ramos P, Ruiz A, Carabias E, Pinero I, Garzon A, Alvarez I. Mullerian adenosarcoma of the cervix with heterologous elements: report of a case and review of the literature. Gynecol Oncol. 2002;84(1):161–6.
Clement PB. Mullerian adenosarcomas of the uterus with sarcomatous overgrowth. A clinicopathological analysis of 10 cases. Am J Surg Pathol. 1989;13(1):28–38.
Wu RI, Schorge JO, Dal Cin P, Young RH, Oliva E. Mullerian adenosarcoma of the uterus with low-grade sarcomatous overgrowth characterized by prominent hydropic change resulting in mimicry of a smooth muscle tumor. Int J Gynecol Pathol. 2014;33(6):573–80.
Soslow RA, Ali A, Oliva E. Mullerian adenosarcomas: an immunophenotypic analysis of 35 cases. Am J Surg Pathol. 2008;32(7):1013–21.
Howitt BE, Sholl LM, Dal Cin P, et al. Targeted genomic analysis of Mullerian adenosarcoma. J Pathol. 2015;235(1):37–49.
Brooks SE, Zhan M, Cote T, Baquet CR. Surveillance, epidemiology, and end results analysis of 2677 cases of uterine sarcoma 1989-1999. Gynecol Oncol. 2004;93(1):204–8.
McCluggage WG. Malignant biphasic uterine tumours: carcinosarcomas or metaplastic carcinomas? J Clin Pathol. 2002;55(5):321–5.
Zelmanowicz A, Hildesheim A, Sherman ME, et al. Evidence for a common etiology for endometrial carcinomas and malignant mixed mullerian tumors. Gynecol Oncol. 1998;69(3):253–7.
Costa MJ, Khan R, Judd R. Carcinoma (malignant mixed mullerian [mesodermal] tumor) of the uterus and ovary. Correlation of clinical, pathologic, and immunohistochemical features in 29 cases. Arch Pathol Lab Med. 1991;115(6):583–90.
Grayson W, Taylor LF, Cooper K. Carcinosarcoma of the uterine cervix: a report of eight cases with immunohistochemical analysis and evaluation of human papillomavirus status. Am J Surg Pathol. 2001;25(3):338–47.
Clement PB, Zubovits JT, Young RH, Scully RE. Malignant mullerian mixed tumors of the uterine cervix: a report of nine cases of a neoplasm with morphology often different from its counterpart in the corpus. Int J Gynecol Pathol. 1998;17(3):211–22.
Ferguson SE, Tornos C, Hummer A, Barakat RR, Soslow RA. Prognostic features of surgical stage I uterine carcinosarcoma. Am J Surg Pathol. 2007;31(11):1653–61.
Fukunaga M, Nomura K, Endo Y, Ushigome S, Aizawa S. Carcinosarcoma of the uterus with extensive neuroectodermal differentiation. Histopathology. 1996;29(6):565–70.
Kempson RL, Hendrickson MR. Smooth muscle, endometrial stromal, and mixed Mullerian tumors of the uterus. Mod Pathol. 2000;13(3):328–42.
George E, Manivel JC, Dehner LP, Wick MR. Malignant mixed mullerian tumors: an immunohistochemical study of 47 cases, with histogenetic considerations and clinical correlation. Hum Pathol. 1991;22(3):215–23.
Meis JM, Lawrence WD. The immunohistochemical profile of malignant mixed mullerian tumor. Overlap with endometrial adenocarcinoma. Am J Clin Pathol. 1990;94(1):1–7.
Castilla MA, Moreno-Bueno G, Romero-Perez L, et al. Micro-RNA signature of the epithelial-mesenchymal transition in endometrial carcinosarcoma. J Pathol. 2011;223(1):72–80.
Pea M, Martignoni G, Zamboni G, Bonetti F. Perivascular epithelioid cell. Am J Surg Pathol. 1996;20(9):1149–53.
Conlon N, Soslow RA, Murali R. Perivascular epithelioid tumours (PEComas) of the gynaecological tract. J Clin Pathol. 2015;68(6):418–26.
Bonetti F, Pea M, Martignoni G, et al. Clear cell (“sugar”) tumor of the lung is a lesion strictly related to angiomyolipoma--the concept of a family of lesions characterized by the presence of the perivascular epithelioid cells (PEC). Pathology. 1994;26(3):230–6.
Folpe AL, Goodman ZD, Ishak KG, et al. Clear cell myomelanocytic tumor of the falciform ligament/ligamentum teres: a novel member of the perivascular epithelioid clear cell family of tumors with a predilection for children and young adults. Am J Surg Pathol. 2000;24(9):1239–46.
Pea M, Bonetti F, Zamboni G, et al. Melanocyte-marker-HMB-45 is regularly expressed in angiomyolipoma of the kidney. Pathology. 1991;23(3):185–8.
Zamboni G, Pea M, Martignoni G, et al. Clear cell “sugar” tumor of the pancreas. A novel member of the family of lesions characterized by the presence of perivascular epithelioid cells. Am J Surg Pathol. 1996;20(6):722–30.
Schoolmeester JK, Dao LN, Sukov WR, et al. TFE3 translocation-associated perivascular epithelioid cell neoplasm (PEComa) of the gynecologic tract: morphology, immunophenotype, differential diagnosis. Am J Surg Pathol. 2015;39(3):394–404.
Fukunaga M. Perivascular epithelioid cell tumor of the uterus: report of four cases. Int J Gynecol Pathol. 2005;24(4):341–6.
Bosincu L, Rocca PC, Martignoni G, et al. Perivascular epithelioid cell (PEC) tumors of the uterus: a clinicopathologic study of two cases with aggressive features. Mod Pathol. 2005;18(10):1336–42.
Fang CL, Lin YH, Chen WY. Microscopic endometrial perivascular epithelioid cell nodules: a case report with the earliest presentation of a uterine perivascular epithelioid cell tumor. Diagn Pathol. 2012;7:117.
Froio E, Piana S, Cavazza A, Valli R, Abrate M, Gardini G. Multifocal PEComa (PEComatosis) of the female genital tract associated with endometriosis, diffuse adenomyosis, and endometrial atypical hyperplasia. Int J Surg Pathol. 2008;16(4):443–6.
Liang SX, Pearl M, Liu J, Hwang S, Tornos C. “Malignant” uterine perivascular epithelioid cell tumor, pelvic lymph node lymphangioleiomyomatosis, and gynecological pecomatosis in a patient with tuberous sclerosis: a case report and review of the literature. Int J Gynecol Pathol. 2008;27(1):86–90.
Lim GS, Oliva E. The morphologic spectrum of uterine PEC-cell associated tumors in a patient with tuberous sclerosis. Int J Gynecol Pathol. 2011;30(2):121–8.
Burke M, Opeskin K. Death due to intravenous leiomyomatosis extending to the right pulmonary artery. Pathology. 2004;36(2):202–3.
Carr RJ, Hui P, Buza N. Intravenous leiomyomatosis revisited: an experience of 14 cases at a single medical center. Int J Gynecol Pathol. 2015;34(2):169–76.
To WW, Ngan HY, Collins RJ. Intravenous leiomyomatosis with intracardiac involvement. Int J Gynaecol Obstet. 1993;42(1):37–40.
Topcuoglu MS, Yaliniz H, Poyrazoglu H, et al. Intravenous leiomyomatosis extending into the right ventricle after subtotal hysterectomy. Ann Thorac Surg. 2004;78(1):330–2.
Virzi G, Ragazzi S, Bussichella F, et al. Intravenous leiomyomatosis extending from the inferior caval vein to the pulmonary artery. J Thorac Cardiovasc Surg. 2007;133(3):831–2.
Mulvany NJ, Slavin JL, Ostor AG, Fortune DW. Intravenous leiomyomatosis of the uterus: a clinicopathologic study of 22 cases. Int J Gynecol Pathol. 1994;13(1):1–9.
Nogales FF, Navarro N, Martinez de Victoria JM, et al. Uterine intravascular leiomyomatosis: an update and report of seven cases. Int J Gynecol Pathol. 1987;6(4):331–9.
Norris HJ, Parmley T. Mesenchymal tumors of the uterus. V. Intravenous leiomyomatosis. A clinical and pathologic study of 14 cases. Cancer. 1975;36(6):2164–78.
Clement PB, Young RH, Scully RE. Intravenous leiomyomatosis of the uterus. A clinicopathological analysis of 16 cases with unusual histologic features. Am J Surg Pathol. 1988;12(12):932–45.
Han HS, Park IA, Kim SH, Lee HP. The clear cell variant of epithelioid intravenous leiomyomatosis of the uterus: report of a case. Pathol Int. 1998;48(11):892–6.
Jordan LB, Al-Nafussi A, Beattie G. Cotyledonoid hydropic intravenous leiomyomatosis: a new variant leiomyoma. Histopathology. 2002;40(3):245–52.
Buza N, Xu F, Wu W, Carr RJ, Li P, Hui P. Recurrent chromosomal aberrations in intravenous leiomyomatosis of the uterus: high-resolution array comparative genomic hybridization study. Hum Pathol. 2014;45(9):1885–92.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Soslow, R.A., Oliva, E. (2015). Uterine Cancer: Pathology. In: Muggia, F., Santin, A.D., Oliva, E. (eds) Uterine Cancer. Current Clinical Oncology. Springer, Cham. https://doi.org/10.1007/7631_2015_7
Download citation
DOI: https://doi.org/10.1007/7631_2015_7
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-47267-6
Online ISBN: 978-3-319-47269-0
eBook Packages: MedicineMedicine (R0)