
Abstract
Pulmonary hypertension (PH) is a disease with high pulmonary arterial pressure, pulmonary vasoconstriction, pulmonary vascular remodeling, and microthrombosis in complex plexiform lesions, but it has been unclear of the exact mechanism of PH. A new understanding of the pathogenesis of PH is occurred and focused on the role of crosstalk between the cells on pulmonary vessels and pulmonary alveoli. It was found that the crosstalks among the endothelial cells, smooth muscle cells, fibroblasts, pericytes, alveolar epithelial cells, and macrophages play important roles in cell proliferation, migration, inflammation, and so on. Therefore, the heterogeneity of multiple pulmonary blood vessels and alveolar cells and tracking the transmitters of cell communication could be conducive to the further insights into the pathogenesis of PH to discover the potential therapeutic targets for PH.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Alveolar epithelial cell
- Crosstalk
- Endothelial cells
- Fibroblasts
- Inflammation
- Macrophages
- Pericytes
- Pulmonary hypertension
- Remodeling
- Smooth muscle cells
1 Introduction
PH is defined as the mean pulmonary artery pressure (mPAP) is 20 mmHg or higher in the resting state. PH is an unwanted disease with the rising incidence rate and death rate, so the researchers pay more and more attention to explore the mechanism and effective treatment of PH (Hansmann 2017). The World Symposium on Pulmonary Hypertension (WSPH) divides PH into five groups according to its symptoms, pathological mechanisms, hemodynamic features, and treatment methods: Group 1: pulmonary arterial hypertension (PAH); Group 2: PH due to left heart disease; Group 3: PH due to lung diseases and/or hypoxia; Group 4: PH due to pulmonary artery obstructions and Group 5: PH with unclear and/or multifactorial mechanisms. The latest PH clinical classification and its causes are presented in Table 1 (Simonneau et al. 2019). The main pathological characteristics of PH include pulmonary vascular contraction and remodeling, inflammation, and microthrombosis. Specially, pulmonary vascular remodeling is becoming more and more important in PH, but there is still a lack of the effective therapy for pulmonary vascular remodeling (Zhao et al. 2021). Endothelin-1, prostacyclin, and nitric oxide are three pathological factors involved in PAH based on the dysfunction of endothelial cells and have been taken as the directions to PAH treatment (Pulido et al. 2016). However, these immediate treatments can’t markedly improve the morbidity and the mortality of PH, except lung transplantation (Evans et al. 2021). With the progression of cellular and molecular biology, it is believed that the therapeutic targets for alleviating vascular remodeling, pulmonary contraction, and pulmonary inflammation would be constantly discovered.
In addition, it is gradually recognized of the impacts of the changes on the pulmonary vascular microenvironment of PH, especially the role of the interactions between the cells of the pulmonary vascular wall in the development of PH (Pasha 2014). PH includes abnormalities of vascular cells (endothelial cells, smooth muscle cells, and fibroblasts) and inflammatory cells (Southgate et al. 2020). More and more reports are proved of the roles of endothelial cells (ECs), smooth muscle cells (SMCs), and fibroblasts, as well as platelets and inflammatory cells in PH (Stenmark et al. 2018). However, the role of the interaction between alveolar epithelial cells and other cells in PH is unclear. It should be furtherly explored whether alveolar epithelial cells are involved in pulmonary vascular remodeling, pulmonary vascular contraction, and pulmonary inflammation. The purpose of this review is focused on the roles of crosstalk between cells in the pathogenesis of PH and to explore the potential therapeutic targets to improve the survival rates.
2 Fundamental Pathogenesis in the Progression of PH
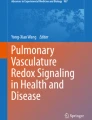
PH is a cardiopulmonary illness that can influence the pulmonary arterial and venous circulation and induce right ventricle hypertrophy (Hoeper et al. 2017; Kim and George 2019). The pathogenic factors of PH include pulmonary endothelial cell disorders, abnormal vascular wall cell proliferation, inflammation, and multiple gene mutations, which finally lead to right ventricular hypertrophy, cardio myocytes damage, and death (Makino et al. 2011; Tuder 2017; Montani et al. 2016) (Fig. 1). Despite different forms of PH exhibit diverse pathological mechanisms, the previous research results indicated that the crosstalks between the blood vessel wall cells (i.e., SMCs, fibroblasts, and Ecs) are the corporative features of the molecules and the cells involved in pulmonary vascular remodeling, pulmonary vascular contraction, and pulmonary inflammation (Pasha 2014). Therefore, exploring these molecular and cellular pathogenesis of PH will help to find more effective therapeutic targets to control the progression of PH.

Basic pathogenesis in the progression of PH. The basic pathogenesis of PH includes vasoconstriction, vascular remodeling, inflammation and gene mutation, which results in pulmonary arterial hypertension and right ventricular hypertrophy
3 Pulmonary ECs Crosstalk with SMCs
3.1 EC Regulation of SMC Proliferation
ECs can adjust and control the vascular function. EC dysfunction means the imbalance between vasoconstrictors and vasodilators produced by EC, between activators and inhibitors of SMC growth and migration, and between proinflammatory and anti-inflammatory signals in the PAH (Perros et al. 2015). Specifically, when EC dysfunction, PAH has the following characteristics: pulmonary inflammation, accumulation of inflammatory cells, oxidative/nitrifying stress, changes in vascular cell viability, and proliferation (Evans et al. 2021; Huertas et al. 2014). These characteristics of PAH support the key role of EC dysfunction in the pathogenesis of PAH. It is worth exploring whether the proliferation of SMC is an inherent sign or is caused by the dysfunction of ECs. In the homeostasis of the pulmonary circulation, the interaction between EC and SMC plays an important role (Gao et al. 2016). Under a pathological status, the interaction of the two cells leads to an increase in pulmonary blood vessel tension, which in turn results in a series of pathological manifestations such as increased pulmonary artery pressure, vascular remodeling, and right ventricular hypertrophy (Guignabert et al. 2015). Hypoxia-induced mitogenic factor (HIMF) plays an important role in EC-SMC crosstalk. HIMF stimulated pulmonary artery ECs (PAECs) to generate and release high mobility group box-1 (HMGB1) by the regulation of autophagy and bone morphogenic protein receptor 2 (BMPR2), and finally made pulmonary artery smooth muscle cells (PASMCs) proliferation (Gao et al. 2016). Dysfunctional PAECs deliver a variety of mediators, for instance, platelet-derived growth factor-BB (PDGF-B), endothelin-1 (ET-1), chemokine 12 (CXCL12), and macrophage migration inhibitory factor (MIF), which can induce forkhead box M1 (FoxM1) expression in PASMCs and activate FoxM1-related to PASMCs proliferation, resulting in pulmonary vascular remodeling and PH (Dai et al. 2018). There is an evidence that ECs can communicate with SMCs through micro-RNA195 to regulate serotonin transporter (5-HTT) to induce the proliferation of SMCs (Gu et al. 2017). Previous studies have shown that the proliferative endothelial cell phenotype is the prominent feature of PAH. The studies suggested that changes in EC phenotype contribute to the occurrence of PAH (Awad et al. 2016). For example, long-term smoking can change the phenotype of human lung microvascular EC. Thereby, inducing EC apoptosis or inherited epigenetic EC dysfunction is related to pulmonary artery remodeling and PH (Petrusca et al. 2014). This crosstalk between ECs and SMCs leads to SMC proliferation and an increase in the thickness of the inner wall of blood vessels.
3.2 SMC Regulation of EC Proliferation and Migration
Recent studies provide a few fascinating findings of SMC regulation of EC proliferation. In SMC-EC co-culture, it was found that BMPR2 activated notch receptor 1 (Notch1) to induce EC proliferation (Miyagawa et al. 2019). Both cells required BMPR2 to produce type IV collagen to activate integrin-linked kinase and result in stabilization of presenilin 1 (PS1) and activation of Notch1. And Notch1 kept the EC proliferative capacity by fortifying mitochondrial mass and tempting 6-phosphofructo-2-kinase/fructose-2, 6-biphosphatase 3 (PFKFB3). Loss of Notch1 aggravated hypoxia-induced PH, which was related to damaged EC proliferation and regeneration, leading to loss of anterior capillary arteries (Miyagawa et al. 2019). This research offered the direct evidence that SMC promoted EC proliferation and rebirth to keep monolayer integrity and vascular homeostasis. Some factors released by SMC entice EC migration. The important factors mediating cell–cell communication are cytokines, chemokines, and cell surface receptors (Hwang 2013). New research reports indicated that exosomes were also significant mediators of cell–cell interactions. A lot of diverse molecules existed in exosomes can be absorbed by recipient cells (Jiao et al. 2018). There is an evidence that microRNA-143 (miR-143) plays an important role in PAH patients and PAH animal models. The exosome miR-143 secreted from PASMCs facilitated the migration of PAECs (Deng et al. 2015). This shows that the exosome-mediated intercellular communication between PASMC and PAEC is of significance in PH.
4 Pulmonary ECs Crosstalk with Non-SMCs
4.1 Fibroblasts
The EC-fibroblast crosstalk acts a specific role in the pathogenesis of PAH as well. Endothelial to mesenchymal transition (EndoMT) is involved in the pathogenesis of many human illnesses such as PAH (Jimenez and Piera-Velazquez 2016). ECs can turn into fibroblast-like cells through EndoMT and have an effect on PAH. ECs polarized fibroblasts into myofibroblasts by releasing ET-1and interleukin 6 (IL-6) and then obtained collagen and extracellular matrix proteins to accelerate pulmonary vascular remodeling (Thenappan et al. 2018; Evans et al. 2021). Adventitia fibroblasts take a part in pulmonary vascular remodeling by means of multiple mechanisms. For instance, the augment of myofibroblasts increased the rigidity of the extracellular matrix, which directly caused the activation of PAEC proliferation (Thenappan et al. 2018). Fibroblast-originated matrix metalloproteinase-2 (MMP-2), matrix metalloproteinase-9 (MMP-9), and 15-hydroxyeicosatetraenoic acid (15-HETE) can regulate PAEC proliferation (Liu et al. 2018). The secreted protein thrombospondin-1 (TSP1) in lung fibroblasts disrupted EC–fibroblasts interactions to promote vascular remodeling in PAH (Labrousse-Arias et al. 2016).
4.2 Pericytes
In PAH, the number of pericytes is reduced and pericyte-EC crosstalk is also attributed to pulmonary vascular remodeling. Abnormal pericyte recruitment contributes to the pathogenesis of PAH (Ricard et al. 2014). Studies have shown that Wnt family member 5A (Wnt5a) plays a key role in the crosstalk between pulmonary microvascular endothelial cells (PMVECs) and pericytes, and also contributes to pulmonary vascular remodeling in PAH. The recruitment of pericytes in small blood vessels needed Wnt5a produced by healthy PMVECs. But defects of Wnt5a in PAH PMVECs can cause persistent pulmonary hypertension and right heart failure after hypoxia recovery (Yuan et al. 2019). As a result, PMVECs lack of Wnt5a had a decreasing capacity to recruit pericytes and resulted in a loss of small blood vessels in PAH (Yuan et al. 2019). In addition, Pyruvate Dehydrogenase Kinase 4 (PDK4), which is a gene encoding a mitochondrial enzyme responsible for inhibiting glucose oxidation, is related to the excessive proliferation of pericytes in PAH and improved EC-pericyte crosstalk. The decrease of PDK4 contributes to promote EC-pericyte crosstalk (Yuan et al. 2016). Therefore, genes that regulate and control pericyte-EC crosstalk may become a new therapeutic target to cure the loss of small blood vessels in PAH.
4.3 Inflammatory Cells
The main structural change of PAH is pulmonary vascular remodeling (Liang et al. 2020). And there have been definite reports showing that inflammation plays a major pathogenic factor in pulmonary vascular remodeling (Oliveira et al. 2017). At the same time, the recruitment of inflammatory cells and EC proliferation play an equally important effect in the pathogenesis of PAH (Mumby et al. 2017). It can be seen that inflammatory cells and ECs are inseparable from the development of PAH (Kuebler et al. 2018). Hence, the role of inflammation in PAH is getting more and more attention. Cytokines and chemokines are certain to be the driving factors and contributing factors of the perivascular inflammation in PAH (Le Hiress et al. 2015). Macrophages and lymphocytes may be referred to the course of pulmonary blood vessel remodeling. The recruitment and accumulation of leukocytes were facilitated by granulocyte macrophage colony-stimulating factor (GM-CSF) (Sawada et al. 2014), CXCL12 (Dai et al. 2016), connective tissue growth factor (CTGF) (Pi et al. 2018), IL-6 (Van Hung et al. 2014), and leptin (Xue et al. 2017) released by activated ECs. Other factors released from accumulated leukocytes such as leukotriene B4 (LTB4) derived from macrophages can cause EC apoptosis (Tian et al. 2013), and MIF derived from T cell lymphocytes can cause inflammation of the EC and recruit inflammatory cells (Le Hiress et al. 2015).
5 Alveolar Epithelial Cells Crosstalk with SMCs
5.1 Alveolar Epithelial Cell Regulation of SMC Proliferation
Apart from damage and dysfunction of EC in the pathogenesis of PH, more and more people realize that the alveolar epithelial cells (AECs) play an equally significant role in the development of PH. Some studies found that the activation of endoplasmic reticulum stress after long-term high-altitude exposure accelerates the apoptosis of AECs, which may induce the occurrence and development of high-altitude pulmonary hypertension (Pu et al. 2020). CTGF over-expressed in epithelial cells activates the integrin-linked kinase (ILK)/glucose synthesis kinase-3β (GSK-3β)/β-catenin pathway, resulting in dysfunction of epithelial cell and PASMC remodeling, which finally leads to the occurrence of PH (Chen et al. 2011). Recently, it has also been found that AECs take part in the pulmonary vascular contraction and remodeling of hypoxic pulmonary hypertension (Wang et al. 2021). The function of alveolar epithelial cells is not only a component of gas exchange but also a vital barrier to protect the human body from harm. AECs can quickly repair and regenerate cells to restore a complete alveolar epithelial barrier and then respond to acute lung injury (Zhang et al. 2019). Alveolar type I (AT1) and alveolar type II (AT2) cells are two types of AECs. The main function of AT2 cells is to synthesize and secrete pulmonary surfactants. Furthermore, AT2 cells can be differentiated into AT1 cells in the homeostasis of the alveoli and the repair process after injury. The AT1 cells constitute the thin air-blood barrier, which is the epithelial component, and the coverage rate reaches 95% of the alveolar surface area (Chen and Liu 2020). According to previous reports, in hypoxic pulmonary hypertension (HPH), the response of pulmonary blood vessels to hypoxia was not like the expansion of blood vessels in the systemic circulation but vasoconstriction (Böger and Hannemann 2020). The alveoli will not make a rise in systemic pressure after being hypoxic, but only made an increase in pulmonary artery pressure. After the alveoli sense hypoxia, it was primarily felt on the alveolar capillary membrane. The alveolar capillary membrane is composed of epithelial and endothelial membranes on the alveolar wall. The hypoxia signal propagated from the alveolar capillaries to the small arteries and then caused the contraction of PASMCs (Hough et al. 2018). Both AECs and ECs show tolerance to hypoxia, but AECs were more sensitive (Wang et al. 2021). It was reported that hypoxia increased the concentration of reactive oxygen species (ROS) in AECs (Grimmer and Kuebler 2017). Hydrogen peroxide (H2O2) from AECs dependent on the ROS/superoxide dismutase 2 (SOD2) pathway regulated pulmonary vascular remodeling and contraction. In vitro, it was manifested that AECs not only facilitated the proliferation of PASMCs but also facilitated the proliferation of aortic artery smooth cells (AASMCs) in hypoxia (Wang et al. 2021). Therefore, the pulmonary vascular microenvironment formed by AECs and SMCs was involved in the remodeling and contraction of pulmonary vessels.
5.2 SMC Regulation of AEC Proliferation
In acute lung inflammation, the spread of this inflammation relied on the immunologic function of lung interstitial cells, for example, SMCs (Udjus et al. 2019). SMC released a mass of proinflammatory factors, for instance, cytokines (Tumor Necrosis Factor-alpha [TNF-α], IL-6), chemokines (Chemokine 8 [CXCL8]/Interleukin 8 [IL-8]/murine Chemokine 1 [CXCL1]), and growth factors (neuregulins [NRGs] and transforming growth factor alpha [TGFα]) (Tliba and Panettieri 2009). These inflammatory responses need a disintegrin and metalloproteinase 17 (ADAM 17)-mediated transactivation of ErbB receptors after the application of exogenous TGFα or NRG1. Transactivation of cells mediated by ErbB via binding to epidermal growth factor receptor (EGFR)/ErbB1 or ErbB3 and ErbB4 receptors and shed TGFα or NRGs. Furthermore, ErbB4 has developmental functions and is involved in the synthesis and proliferation of surface active substances in AECs. Therefore, in the pulmonary inflammation, decreased ADAM 17-mediated growth factor in SMC accelerated the transactivation of ErbB4 by means of NRGs, for example, NRG1 activation facilitated the proliferation of AECs and keeps the homeostasis of the cellular environment (Dreymueller et al. 2014). It is worth attention of the crosstalk between AECs and SMCs in pulmonary inflammation of PH.
6 Alveolar Epithelial Cells Crosstalk with Non-SMCs
6.1 Fibroblast
Idiopathic pulmonary fibrosis (IPF), pathologically common interstitial pneumonia, is a long-term disease with unclear etiology (Larson-Casey et al. 2020). The pathogenesis of the disease includes alveolar epithelial injury, abnormal vascular repair, and pulmonary vascular remodeling. The main complications of IPF patient survival include lung cancer and pulmonary hypertension. There were a lot of evidence that one of the important factors leading to IPF is the dysfunction and continuous damage of AECs (Lee et al. 2018; Wang et al. 2020). The migration, proliferation, and activation of mesenchymal cells are caused by active AECs and are accompanied by the formation of fibroblasts/myofibroblasts foci and excessive accumulation of extracellular matrix. Just like that DNA harm in AEC II resulted in osteopontin (OPN) expression via activating extracellular signal-regulated kinase (ERK)-dependent signaling pathways. The induced OPN boosts the proliferation of AEC II and the migration of fibroblasts (Kato et al. 2014). Therefore, the integrity of the alveolar epithelial barrier was ultimately maintained due to the interaction between AECs and fibroblasts, which indicated that crosstalk between AECs and fibroblasts will be closely associated with the development of PH.
6.2 Macrophages
Similarly, the interactions between AECs and macrophages play an equally important regulatory role in the development of pulmonary diseases (Young et al. 2016; Byrne et al. 2016). Macrophages are one of the important regulators of pulmonary inflammatory disease. Macrophages plasticity, specificity, and ability to interact with other cells make them a pivotal factor in the pathogenesis of pulmonary inflammatory disease (Wang et al. 2019). In addition, the crosstalk between macrophages and AECs is a key factor in the pathological process of pulmonary inflammation and fibrosis, which is directly attributed to the contact between macrophages and AECs. AT2 cells can secrete sonic hedgehog (Shh), and its signal transduction facilitated the secretion of OPN in macrophages. OPN acted on macrophages through autocrine or paracrine mode. And OPN fortified the expression of arginase-1 by means of activating the Janus kinase-2/transcription 3 (JAK2/STAT3) signaling pathway, and caused pulmonary fibrosis to occur (Hou et al. 2021). Similarly, the interaction between AECs and macrophages also plays an important role in regulating the progression of lung injury, which is becoming a new research hotspot. Exosomes from AECs can cause pulmonary inflammation and enable the migration and activation of macrophages. MicroRNA-92a-3p (miR-92a-3p) in AECs-derived exosomes mediated cellular communication between AECs and macrophages and facilitated the activation of macrophages by means of controlling Phosphatase and tensin homolog (PTEN) expression and adjusting the activation of nuclear factor-κB (NF-κB) signaling pathways (Liu et al. 2021). Therefore, the crosstalks between AECs and macrophages probably take part in PH by regulating pulmonary inflammation.
7 Macrophages Crosstalk with SMCs
The accumulation of inflammatory cells is an important feature in vascular injury during PAH. Inflammatory cells (T, B lymphocytes, mast cells, monocytes, and macrophages) take a key part in the PAH process. Macrophages are innate immune cells, composed of recruited/infiltrated monocytes, which are essential for keeping homeostasis and repairing ability. Polarized macrophages may be generally classified into three genres: classically activated macrophages (M1), alternating activated macrophages (M2), and regulatory macrophages (M2b) (Huang et al. 2020). So it is worth noting that macrophages are involved in the pathogenesis of PAH (Bordenave et al. 2020). Early recruitment and replacement activation of macrophages are of great significance in the pathogenesis of PAH (Bai et al. 2019). Macrophage-mediated inflammation is intricate, and the interaction between macrophages and PASMCs can regulate the internal microenvironment of the lung. In the co-culture of m2-macrophages and PASMC in direct contact, we understand that it facilitates the proliferation and migration of PASMC by relying on C-C chemokine receptor types 2/C-C chemokine receptor types 5 (CCR2/CCR5) (Abid et al. 2019). Furthermore, we found that M2b macrophages can also adjust the proliferation, migration, and apoptosis of PASMC by adjusting and controlling the phosphatidylinositol-3-kinase/protein kinase B/forkhead box protein O3a (PI3K/Akt/FoxO3a) pathway (Huang et al. 2020). Six-transmembrane protein of prostate 2 (Stamp2) has been reported to be an important anti-inflammatory protein in macrophages. The lack of Stamp2 can directly affect the interaction between macrophages and SMCs, resulting in aggravation of pulmonary hypertension caused by hypoxia (Batool et al. 2020). And a recent study showed that LTB4 (5-lipoxygenase [5-LO] metabolite) derived from macrophages plays an important effect in causing pulmonary vascular remodeling in PAH (Tian et al. 2013; Peters-Golden and Henderson 2007). 5-LO and LTB4 are related to the evolution of PAH (Peters-Golden and Henderson 2007). In the lung lesions of hPAH patients with Bmpr2 mutations, 5-LO-mediated inflammation similarly converts PAEC into a diseased neointimal phenotype. In rats and patients with Bmpr2 mutations, 5-lo-expressing neointimal lesions might facilitate vascular inflammation and vascular remodeling (Tian et al. 2019). Pulmonary vascular remodeling is featured by the progress of distinct neointimal lesions, covering concentric laminar intima fibrosis and plexiform lesions (Dickinson et al. 2011). These neointimal lesions give rise to intraluminal obstruction due to EC and SMC proliferation, fibrosis, and inflammation, which ultimately leads to irreversible PAH (Steffes et al. 2020; Chan and Loscalzo 2008). Studies showed that activation of PI3K/Akt and extracellular signal-regulated kinase 1/2 (ERK1/2) pathways mediates LTB 4 through regulating the GSK-3β/β-catenin/cyclin D1 axis to induce PASMCs proliferation, and indicated that this pathway was involved in alleviating vascular remodeling and was beneficial to PAH treatment (Li et al. 2020). The above conclusions proved that the interactions between macrophages and SMCs played an equally significant effect in the pathogenesis and development of PAH.
8 Fibroblasts Crosstalk with Macrophages
Communication mediated by adventitia cells acts a potential role in vascular inflammation and pathogenesis. The adventitia contains many innate immune cells, especially macrophages, fibroblasts, and DCs. The number of fibroblasts accounts for the majority of adventitia cells. The interaction of fibroblasts and macrophages in the adventitia of blood vessels facilitates the transmission of inflammatory signals and the progression of PH (Li et al. 2021). Studies have reported that fibroblasts have the ability to recruit and activate macrophages, leading to vascular inflammation and vascular remodeling, in which lactate and IL-6 play a significant role. Fibroblasts in a large number of animal models and humans with PH regulate macrophage activation (El Kasmi et al. 2014). For example, previous studies have shown that fibroblast paracrine IL-6 and macrophage STAT3 united with hypoxia-inducible factor 1alpha (HIF1α) and CCAAT/enhancer-binding protein beta (C/EBPβ) caused the pathogenesis of PH, which directly led to the occurrence of vascular inflammation and remodeling (El Kasmi et al. 2014). At the same time, studies have found that macrophages can receive and combine the signals sent by fibroblasts and then carry out disparate transcriptomics and metabolomics programming to keep a more stable lung microenvironment during the pathogenesis of PH (Li et al. 2021). LTB4 derived from macrophages aggravated the proliferation, migration, and differentiation of human pulmonary artery adventitia fibroblasts in a dose-dependent manner via its homologous G protein-coupled receptor, BLT1. LTB4 stimulated human pulmonary artery adventitia fibroblasts by up-regulating p38 mitogen-activated protein kinase (MAPK) and NADPH oxidase 4 (Nox4) signaling pathway to promote PH development (Qian et al. 2015). The crosstalks between fibroblasts and macrophages in the microenvironment of the adventitia of blood vessels are expected to play a great therapeutic significance in improving the process of pulmonary vascular remodeling.
9 Concluding Remarks
PH is considered to be a cardiopulmonary disease with pulmonary vascular inflammation, vascular remodeling, and cardiac cell damage (Yeo et al. 2020; Hsu et al. 2020). Cell-to-Cell Crosstalk has been taken as a new and further understanding of the physiology and pathology of PH (Rafikova et al. 2019). Phenotypic changes resulted in pulmonary vascular remodeling, pulmonary vasoconstriction, and pulmonary inflammation contain: (a) the crosstalk between pulmonary ECs and SMCs that generate a lung microenvironment of proliferation, anti-apoptosis, and vasoconstriction (b) the crosstalk between pulmonary ECs and non-SMCs that generate a lung microenvironment of proliferation, anti-apoptosis, and vasoconstriction (c) the crosstalk between AECs and SMCs that cause a lung microenvironment of proliferation, anti-apoptosis, and vasoconstriction (d) the crosstalk between AECs and non-SMCs that create a lung microenvironment of proliferation, anti-apoptosis, and vasoconstriction (e) the crosstalk between macrophages and SMCs to promote a lung microenvironment of proliferation, anti-apoptosis, and vasoconstriction (f) the crosstalk between macrophages and fibroblasts to promote a lung microenvironment of proliferation, anti-apoptosis, and vasoconstriction. As a result, the imbalance between proliferation and apoptosis, between vasoconstriction and vasodilation, as well as proinflammatory and anti-inflammatory resulted in pathological changes in the inner, middle, and adventitia of the pulmonary blood vessels, narrowing of the vascular lumen, vascular remodeling, pulmonary inflammation, and finally increased pulmonary artery pressure.
The morbidity rate of PH is still very high. Some patients are asymptomatic during the onset of the disease, which is the disadvantage of the early diagnosis and treatment (Strauss et al. 2019). The damage and repair of cells and the complex crosstalk between multiple cells have been added to the pathogenesis of PH (Voelkel et al. 2012). If the intricate interactions between vascular cells and their regulatory signaling pathways are enough realized and are applied in clinic, the pathological state of PH can be changed to the greatest extent and the mortality can be reduced. Therefore, the signaling pathways emphasized in the crosstalk between multiple cells play an important role in many diseases, especially PH. It is summarized of the crosstalk between cells in the pathogenesis of PH (Fig. 2).

Cell-to-cell crosstalk in the pathogenesis of PH. The crosstalk between cells (Endothelial cell, Smooth muscle cell, Alveolar Epithelial cell, Fibroblast, Pericyte, and Macrophage) and the regulated signal pathways are involved in the pathogenesis of PH. NF-κB nuclear factor-κB, ET-1 Endothelin-1, BMPR bone morphogenic protein receptor, FoxM1 forkhead box M1, MIF macrophage migration inhibitory factor, BMPR2 bone morphogenic protein receptor 2, HIMF hypoxia-induced mitogenic factor, PDGF-B platelet-derived growth factor-BB, CXCL12 Chemokine 12, HMGB1 high mobility group box-1, 5-HTT Serotonin transporter, MMP-9 matrix metalloproteinase-9, TSP1 The secreted protein thrombospondin-1, IL-6 Interleukin 6, 15-HETE 15-hydroxyeicosatetraenoic acid, PDK4 Pyruvate Dehydrogenase Kinase 4, GM-CSF granulocyte macrophage colony-stimulating factor, CTGF Connective Tissue Growth Factor, LTB4 leukotriene B4, MMP-2 matrix metalloproteinase-2, PFKFB3 6-phosphofructo-2-kinase/fructose-2,6-biphosphatase3, H2O2 hydrogen peroxide, SOD2 superoxide dismutase 2, TNF-α Tumor Necrosis Factor alpha, CXCL8 Chemokine 8, IL-8 Interleukin 8, CXCL1 murine Chemokine 1, NRG1 neuregulin1, TGFα Transforming growth factor alpha, adam17 a disintegrin and metalloproteinase 17, Notch1 notch receptor 1, ERK extracellular signal-regulated kinase, OPN osteopontin, PTEN Phosphatase and tensin homolog, CCR2 C-C chemokine receptor types 2, CCR5 C-C chemokine receptor types 5, PI3K phosphatidylinositol-3-kinase, AKT protein kinase B, FoxO3a Forkhead box protein O3a, Stamp2 Six-transmembrane protein of prostate 2, HIF1α Hypoxia-inducible factor-1 alpha, C/EBPβ CCAAT/enhancer-binding protein beta, JAK2 Janus kinase-2, STAT3 transcription 3, Wnt5a Wnt family member 5A, PS1 presenilin 1, Shh Sonic hedgehog, MiR-143 microRNA-143, ROS reactive oxygen species, miR-92a-3p microRNA-92a-3p, ERK1/2 signal-regulated kinase 1/2, GSK-3β glycogen synthase kinase-3β, p38 MAPK p38 mitogen-activated protein kinases, Nox4 NADPH oxidase 4
In human and rodents PH, there exist the crosstalks between ECs and SMCs (Lin et al. 2019), ECs and pericytes (Yuan et al. 2019), ECs and Macrophages (Sawada et al. 2014), AECs and fibroblasts (Kato et al. 2014), AECs and macrophages (Hou et al. 2021), macrophages and SMCs (Abid et al. 2019), fibroblasts and macrophages (El Kasmi et al. 2014), ECs and fibroblasts (Labrousse-Arias et al. 2016). However, the crosstalk between AECs and SMCs has been studied only in rodent models until now (Wang et al. 2021). In comparison, the researches in rodent models of PH are more involved in cell-to-cell crosstalk than Human PH disease. And other studies found that in HIMF-induced PH, HMGB1-receptor for advanced glycation end products (RAGE) signal transduction is essential for mediating EC and SMC crosstalk, which was confirmed from idiopathic PH patients and rodent PH. However, data from humanized mice were found to further confirm the clinical significance of the HIMF/HMGB1 signal axis (Lin et al. 2019). Therefore, in future research, humanized mice should be more used in the crosstalk between cells for the development of biomedical research and clinical treatment of PH.
Nowadays, the research focused on network medicine can expand the opportunities for personalized treatment of PH (Wang and Loscalzo 2021). Network medicine is the use of effective genomic instruments as well as biostatistics, bioinformatics, and dynamic system analysis to find the way of the prevention and treatment of PH (Napoli et al. 2019; Fiscon et al. 2018). For instance, in future research, computational modeling techniques can be used to enhance the interpretation of the relationship between the cells on the pulmonary vessels and the pulmonary alveoli, and their interaction with neighboring cells. In conclusion, a full understanding of cell-to-cell crosstalk can bring more therapeutic options to the pathogenesis of PH. The important signals in cell-to-cell crosstalk will become the new targets for the prevention and treatment of PH.
Abbreviations
- 15-HETE:
-
15-Hydroxyeicosatetraenoic acid
- 5-HTT:
-
Serotonin transporter
- 5-LO:
-
5-Lipoxygenase
- AASMCs:
-
Aortic artery smooth cells
- ADAM17:
-
A disintegrin and metalloproteinase 17
- AECs:
-
Alveolar epithelial cells
- AKT:
-
Protein kinase B
- AT1:
-
Alveolar type I
- AT2:
-
Alveolar type II
- BMPR2:
-
Bone morphogenic protein receptor 2
- C/EBPβ:
-
CCAAT/enhancer-binding protein beta
- CCR2:
-
C-C chemokine receptor types 2
- CCR5:
-
C-C chemokine receptor types 5
- CTGF:
-
Connective tissue growth factor
- CXCL1:
-
Murine chemokine 1
- CXCL12:
-
Chemokine 12
- CXCL8:
-
Chemokine 8
- Ecs:
-
Endothelial cells
- EGFR:
-
Epidermal growth factor receptor
- EndoMT:
-
Endothelial-to mesenchymal transition
- ERK:
-
Extracellular signal-regulated kinase
- ERK1/2:
-
Signal-regulated kinase 1/2
- ET-1:
-
Endothelin-1
- FoxM1:
-
Forkhead box M1
- FOXO3a:
-
Forkhead box protein O3a
- GM-CSF:
-
Granulocyte macrophage colony-stimulating factor
- GSK-3β:
-
Glycogen synthase kinase-3β
- H2O2:
-
Hydrogen peroxide
- HIF1α:
-
Hypoxia-inducible factor-1alpha
- HIMF:
-
Hypoxia-induced mitogenic factor
- HIV:
-
Human immunodeficiency virus
- HMGB1:
-
High mobility group box 1
- hPAH:
-
Hereditary pulmonary arterial hypertension
- HPH:
-
Hypoxic pulmonary hypertension
- IL-6:
-
Interleukin 6
- IL-8:
-
Interleukin 8
- ILK:
-
Integrin-linked kinase
- IPF:
-
Idiopathic pulmonary fibrosis
- JAK2:
-
Janus kinase 2
- LTB4:
-
Leukotriene B4
- LVEF:
-
Left ventricular ejection fraction
- MIF:
-
Macrophage migration inhibitory factor
- MiR-143:
-
microRNA-143
- MiR-92a-3p:
-
microRNA-92a-3p
- MMP-2:
-
Matrix metalloproteinase-2
- MMP-9:
-
Matrix metalloproteinase-9
- mPAP:
-
Mean pulmonary artery pressure
- NF-κB:
-
Nuclear factor-Κb
- Notch1:
-
Notch receptor 1
- Nox4:
-
NADPH oxidase 4
- NRGs:
-
Neuregulins
- OPN:
-
Osteopontin
- p38MAPK:
-
p38 mitogen-activated protein kinases
- PAECs:
-
Pulmonary artery endothelial cells
- PAH:
-
Pulmonary arterial hypertension
- PASMCs:
-
Pulmonary artery smooth muscle cells
- PCH:
-
Pulmonary capillary hemangiomatosis
- PDGF-B:
-
Platelet-derived growth factor BB
- PDK4:
-
Pyruvate dehydrogenase kinase 4
- PFKFB3:
-
6-Phosphofructo-2-kinase/fructose-2,6-biphosphatase 3
- PI3K:
-
Phosphatidylinositol-3-kinase
- PMVECs:
-
Pulmonary microvascular endothelial cells
- PS1:
-
Presenilin 1
- PTEN:
-
Phosphatase and tensin homolog
- PVOD:
-
Pulmonary veno-occlusive disease
- RAGE:
-
Receptor for advanced glycation end products
- ROS:
-
Reactive oxygen species
- Shh:
-
Sonic hedgehog
- SMCs:
-
Smooth muscle cells
- SOD2:
-
Superoxide dismutase 2
- Stamp2:
-
Six-transmembrane protein of prostate 2
- STAT3:
-
Transcription 3
- TGFα:
-
Transforming growth factor-alpha
- TNF-α:
-
Tumor necrosis factor-alpha
- TSP1:
-
The secreted protein thrombospondin 1
- Wnt5a:
-
Wnt family member 5A
- WSPH:
-
World symposium on pulmonary hypertension
References
Abid S, Marcos E, Parpaleix A, Amsellem V, Breau M, Houssaini A, Vienney N, Lefevre M, Derumeaux G, Evans S, Hubeau C, Delcroix M, Quarck R, Adnot S, Lipskaia L (2019) CCR2/CCR5-mediated macrophage-smooth muscle cell crosstalk in pulmonary hypertension. Eur Respir J 54(4):1802308
Awad KS, Elinoff JM, Wang S, Gairhe S, Ferreyra GA, Cai R, Sun J, Solomon MA, Danner RL (2016) Raf/ERK drives the proliferative and invasive phenotype of BMPR2-silenced pulmonary artery endothelial cells. Am J Physiol Lung Cell Mol Physiol 310(2):L187–L201
Bai P, Lyu L, Yu T, Zuo C, Fu J, He Y, Wan Q, Wan N, Jia D, Lyu A (2019) Macrophage-derived legumain promotes pulmonary hypertension by activating the MMP (matrix metalloproteinase)-2/TGF (transforming growth factor)-β1 signaling. Arterioscler Thromb Vasc Biol 39(4):e130–e145
Batool M, Berghausen EM, Zierden M, Vantler M, Schermuly RT, Baldus S, Rosenkranz S, Ten Freyhaus H (2020) The six-transmembrane protein Stamp2 ameliorates pulmonary vascular remodeling and pulmonary hypertension in mice. Basic Res Cardiol 115(6):68
Böger R, Hannemann J (2020) Dual role of the L-arginine-ADMA-NO pathway in systemic hypoxic vasodilation and pulmonary hypoxic vasoconstriction. Pulm Circ 10(2):2045894020918850
Bordenave J, Thuillet R, Tu L, Phan C, Cumont A, Marsol C, Huertas A, Savale L, Hibert M, Galzi J-L, Bonnet D, Humbert M, Frossard N, Guignabert C (2020) Neutralization of CXCL12 attenuates established pulmonary hypertension in rats. Cardiovasc Res 116(3):686–697
Byrne AJ, Maher TM, Lloyd CM (2016) Pulmonary macrophages: a new therapeutic pathway in fibrosing lung disease? Trends Mol Med 22(4):303–316
Chan SY, Loscalzo J (2008) Pathogenic mechanisms of pulmonary arterial hypertension. J Mol Cell Cardiol 44(1):14–30
Chen Q, Liu Y (2020) Heterogeneous groups of alveolar type II cells in lung homeostasis and repair. Am J Physiol Cell Physiol 319(6):C991–C996
Chen S, Rong M, Platteau A, Hehre D, Smith H, Ruiz P, Whitsett J, Bancalari E, Wu S (2011) CTGF disrupts alveolarization and induces pulmonary hypertension in neonatal mice: implication in the pathogenesis of severe bronchopulmonary dysplasia. Am J Physiol Lung Cell Mol Physiol 300(3):L330–L340
Dai Z, Li M, Wharton J, Zhu MM, Zhao Y-Y (2016) Prolyl-4 hydroxylase 2 (PHD2) deficiency in endothelial cells and hematopoietic cells induces obliterative vascular remodeling and severe pulmonary arterial hypertension in mice and humans through hypoxia-inducible factor-2α. Circulation 133(24):2447–2458
Dai Z, Zhu MM, Peng Y, Jin H, Machireddy N, Qian Z, Zhang X, Zhao Y-Y (2018) Endothelial and smooth muscle cell interaction via FoxM1 signaling mediates vascular remodeling and pulmonary hypertension. Am J Respir Crit Care Med 198(6):788–802
Deng L, Blanco FJ, Stevens H, Lu R, Caudrillier A, McBride M, McClure JD, Grant J, Thomas M, Frid M, Stenmark K, White K, Seto AG, Morrell NW, Bradshaw AC, MacLean MR, Baker AH (2015) MicroRNA-143 activation regulates smooth muscle and endothelial cell crosstalk in pulmonary arterial hypertension. Circ Res 117(10):870–883
Dickinson MG, Bartelds B, Molema G, Borgdorff MA, Boersma B, Takens J, Weij M, Wichers P, Sietsma H, Berger RMF (2011) Egr-1 expression during neointimal development in flow-associated pulmonary hypertension. Am J Pathol 179(5):2199–2209
Dreymueller D, Martin C, Schumacher J, Groth E, Boehm JK, Reiss LK, Uhlig S, Ludwig A (2014) Smooth muscle cells relay acute pulmonary inflammation via distinct ADAM17/ErbB axes. J Immunol 192(2):722–731
El Kasmi KC, Pugliese SC, Riddle SR, Poth JM, Anderson AL, Frid MG, Li M, Pullamsetti SS, Savai R, Nagel MA, Fini MA, Graham BB, Tuder RM, Friedman JE, Eltzschig HK, Sokol RJ, Stenmark KR (2014) Adventitial fibroblasts induce a distinct proinflammatory/profibrotic macrophage phenotype in pulmonary hypertension. J Immunol 193(2):597–609
Evans CE, Cober ND, Dai Z, Stewart DJ, Zhao Y-Y (2021) Endothelial cells in the pathogenesis of pulmonary arterial hypertension. Eur Respir J 58(3):2003957
Fiscon G, Conte F, Farina L, Paci P (2018) Network-based approaches to explore complex biological systems towards network medicine. Genes 9(9):437
Gao Y, Chen T, Raj JU (2016) Endothelial and smooth muscle cell interactions in the pathobiology of pulmonary hypertension. Am J Respir Cell Mol Biol 54(4):451–460
Grimmer B, Kuebler WM (2017) The endothelium in hypoxic pulmonary vasoconstriction. J Appl Physiol (1985) 123(6):1635–1646
Gu J, Zhang H, Ji B, Jiang H, Zhao T, Jiang R, Zhang Z, Tan S, Ahmed A, Gu Y (2017) Vesicle miR-195 derived from endothelial cells inhibits expression of serotonin transporter in vessel smooth muscle cells. Sci Rep 7:43546
Guignabert C, Tu L, Girerd B, Ricard N, Huertas A, Montani D, Humbert M (2015) New molecular targets of pulmonary vascular remodeling in pulmonary arterial hypertension: importance of endothelial communication. Chest 147(2):529–537
Hansmann G (2017) Pulmonary hypertension in infants, children, and young adults. J Am Coll Cardiol 69(20):2551–2569
Hoeper MM, Ghofrani H-A, Grünig E, Klose H, Olschewski H, Rosenkranz S (2017) Pulmonary hypertension. Dtsch Arzteblatt Int 114(5):73–84
Hou J, Ji J, Chen X, Cao H, Tan Y, Cui Y, Xiang Z, Han X (2021) Alveolar epithelial cell-derived sonic hedgehog promotes pulmonary fibrosis through OPN-dependent alternative macrophage activation. FEBS J 288(11):3530–3546
Hough RF, Bhattacharya S, Bhattacharya J (2018) Crosstalk signaling between alveoli and capillaries. Pulm Circ 8(3):2045894018783735
Hsu JY, Major JL, Riching AS, Sen R, Pires da Silva J, Bagchi RA (2020) Beyond the genome: challenges and potential for epigenetics-driven therapeutic approaches in pulmonary arterial hypertension. Biochem Cell Biol = Biochim Biol Cell 98(6):631–646
Huang S, Yue Y, Feng K, Huang X, Li H, Hou J, Yang S, Huang S, Liang M, Chen G, Wu Z (2020) Conditioned medium from M2b macrophages modulates the proliferation, migration, and apoptosis of pulmonary artery smooth muscle cells by deregulating the PI3K/Akt/FoxO3a pathway. PeerJ 8:e9110
Huertas A, Perros F, Tu L, Cohen-Kaminsky S, Montani D, Dorfmüller P, Guignabert C, Humbert M (2014) Immune dysregulation and endothelial dysfunction in pulmonary arterial hypertension: a complex interplay. Circulation 129(12):1332–1340
Hwang I (2013) Cell-cell communication via extracellular membrane vesicles and its role in the immune response. Mol Cells 36(2):105–111
Jiao Y, Li Z, Loughran PA, Fan EK, Scott MJ, Li Y, Billiar TR, Wilson MA, Shi X, Fan J (2018) Frontline science: macrophage-derived exosomes promote neutrophil necroptosis following hemorrhagic shock. J Leukoc Biol 103(2):175–183
Jimenez SA, Piera-Velazquez S (2016) Endothelial to mesenchymal transition (EndoMT) in the pathogenesis of systemic sclerosis-associated pulmonary fibrosis and pulmonary arterial hypertension. Myth or reality? Matrix Biol 51:26–36
Kato A, Okura T, Hamada C, Miyoshi S, Katayama H, Higaki J, Ito R (2014) Cell stress induces upregulation of osteopontin via the ERK pathway in type II alveolar epithelial cells. PLoS One 9(6):e100106
Kim D, George MP (2019) Pulmonary hypertension. Med Clin North Am 103(3):413–423
Kuebler WM, Bonnet S, Tabuchi A (2018) Inflammation and autoimmunity in pulmonary hypertension: is there a role for endothelial adhesion molecules? (2017 Grover conference series). Pulm Circ 8(2):2045893218757596
Labrousse-Arias D, Castillo-González R, Rogers NM, Torres-Capelli M, Barreira B, Aragonés J, Cogolludo Á, Isenberg JS, Calzada MJ (2016) HIF-2α-mediated induction of pulmonary thrombospondin-1 contributes to hypoxia-driven vascular remodelling and vasoconstriction. Cardiovasc Res 109(1):115–130
Larson-Casey JL, He C, Carter AB (2020) Mitochondrial quality control in pulmonary fibrosis. Redox Biol 33:101426
Le Hiress M, Tu L, Ricard N, Phan C, Thuillet R, Fadel E, Dorfmüller P, Montani D, de Man F, Humbert M, Huertas A, Guignabert C (2015) Proinflammatory signature of the dysfunctional endothelium in pulmonary hypertension. Role of the macrophage migration inhibitory factor/CD74 complex. Am J Respir Crit Care Med 192(8):983–997
Lee J, Arisi I, Puxeddu E, Mramba LK, Amicosante M, Swaisgood CM, Pallante M, Brantly ML, Sköld CM, Saltini C (2018) Bronchoalveolar lavage (BAL) cells in idiopathic pulmonary fibrosis express a complex pro-inflammatory, pro-repair, angiogenic activation pattern, likely associated with macrophage iron accumulation. PLoS One 13(4):e0194803
Li S, Zhai C, Shi W, Feng W, Xie X, Pan Y, Wang J, Yan X, Chai L, Wang Q, Zhang Q, Liu P, Li M (2020) Leukotriene B induces proliferation of rat pulmonary arterial smooth muscle cells via modulating GSK-3β/β-catenin pathway. Eur J Pharmacol 867:172823
Li M, Riddle S, Kumar S, Poczobutt J, McKeon BA, Frid MG, Ostaff M, Reisz JA, Nemkov T, Fini MA, Laux A, Hu C-J, El Kasmi KC, D'Alessandro A, Brown RD, Zhang H, Stenmark KR (2021) Microenvironmental regulation of macrophage transcriptomic and metabolomic profiles in pulmonary hypertension. Front Immunol 12:640718
Liang L-Y, Wang M-M, Liu M, Zhao W, Wang X, Shi L, Zhu M-J, Zhao Y-L, Liu L, Maurya P, Wang Y (2020) Chronic toxicity of methamphetamine: oxidative remodeling of pulmonary arteries. Toxicol In Vitro 62:104668
Lin Q, Fan C, Gomez-Arroyo J, Van Raemdonck K, Meuchel LW, Skinner JT, Everett AD, Fang X, Macdonald AA, Yamaji-Kegan K, Johns RA (2019) HIMF (hypoxia-induced mitogenic factor) signaling mediates the HMGB1 (high mobility group box 1)-dependent endothelial and smooth muscle cell crosstalk in pulmonary hypertension. Arterioscler Thromb Vasc Biol 39(12):2505–2519
Liu Y, Zhang H, Yan L, Du W, Zhang M, Chen H, Zhang L, Li G, Li J, Dong Y, Zhu D (2018) MMP-2 and MMP-9 contribute to the angiogenic effect produced by hypoxia/15-HETE in pulmonary endothelial cells. J Mol Cell Cardiol 121:36–50
Liu F, Peng W, Chen J, Xu Z, Jiang R, Shao Q, Zhao N, Qian K (2021) Exosomes derived from alveolar epithelial cells promote alveolar macrophage activation mediated by miR-92a-3p in sepsis-induced acute lung injury. Front Cell Infect Microbiol 11:646546
Makino A, Firth AL, Yuan JXJ (2011) Endothelial and smooth muscle cell ion channels in pulmonary vasoconstriction and vascular remodeling. Compr Physiol 1(3):1555–1602
Miyagawa K, Shi M, Chen P-I, Hennigs JK, Zhao Z, Wang M, Li CG, Saito T, Taylor S, Sa S, Cao A, Wang L, Snyder MP, Rabinovitch M (2019) Smooth muscle contact drives endothelial regeneration by BMPR2-Notch1-mediated metabolic and epigenetic changes. Circ Res 124(2):211–224
Montani D, Lau EM, Dorfmüller P, Girerd B, Jaïs X, Savale L, Perros F, Nossent E, Garcia G, Parent F, Fadel E, Soubrier F, Sitbon O, Simonneau G, Humbert M (2016) Pulmonary veno-occlusive disease. Eur Respir J 47(5):1518–1534
Mumby S, Gambaryan N, Meng C, Perros F, Humbert M, Wort SJ, Adcock IM (2017) Bromodomain and extra-terminal protein mimic JQ1 decreases inflammation in human vascular endothelial cells: implications for pulmonary arterial hypertension. Respirology 22(1):157–164
Napoli C, Benincasa G, Loscalzo J (2019) Epigenetic inheritance underlying pulmonary arterial hypertension. Arterioscler Thromb Vasc Biol 39(4):653–664
Oliveira SDS, Castellon M, Chen J, Bonini MG, Gu X, Elliott MH, Machado RF, Minshall RD (2017) Inflammation-induced caveolin-1 and BMPRII depletion promotes endothelial dysfunction and TGF-β-driven pulmonary vascular remodeling. Am J Physiol Lung Cell Mol Physiol 312(5):L760–L771
Pasha Q (2014) Saudi guidelines on the diagnosis and treatment of pulmonary hypertension: genetics of pulmonary hypertension. Ann Thorac Med 9(Suppl 1):S16–S20
Perros F, Ranchoux B, Izikki M, Bentebbal S, Happé C, Antigny F, Jourdon P, Dorfmüller P, Lecerf F, Fadel E, Simonneau G, Humbert M, Bogaard HJ, Eddahibi S (2015) Nebivolol for improving endothelial dysfunction, pulmonary vascular remodeling, and right heart function in pulmonary hypertension. J Am Coll Cardiol 65(7):668–680
Peters-Golden M, Henderson WR (2007) Leukotrienes. N Engl J Med 357(18):1841–1854
Petrusca DN, Van Demark M, Gu Y, Justice MJ, Rogozea A, Hubbard WC, Petrache I (2014) Smoking exposure induces human lung endothelial cell adaptation to apoptotic stress. Am J Respir Cell Mol Biol 50(3):513–525
Pi L, Fu C, Lu Y, Zhou J, Jorgensen M, Shenoy V, Lipson KE, Scott EW, Bryant AJ (2018) Vascular endothelial cell-specific connective tissue growth factor (CTGF) is necessary for development of chronic hypoxia-induced pulmonary hypertension. Front Physiol 9:138
Pu X, Lin X, Duan X, Wang J, Shang J, Yun H, Chen Z (2020) Oxidative and endoplasmic reticulum stress responses to chronic high-altitude exposure during the development of high-altitude pulmonary hypertension. High Alt Med Biol 21(4):378–387
Pulido T, Zayas N, de Mendieta MA, Plascencia K, Escobar J (2016) Medical therapies for pulmonary arterial hypertension. Heart Fail Rev 21(3):273–283
Qian J, Tian W, Jiang X, Tamosiuniene R, Sung YK, Shuffle EM, Tu AB, Valenzuela A, Jiang S, Zamanian RT, Fiorentino DF, Voelkel NF, Peters-Golden M, Stenmark KR, Chung L, Rabinovitch M, Nicolls MR (2015) Leukotriene B4 activates pulmonary artery adventitial fibroblasts in pulmonary hypertension. Hypertension 66(6):1227–1239
Rafikova O, Al Ghouleh I, Rafikov R (2019) Focus on early events: pathogenesis of pulmonary arterial hypertension development. Antioxid Redox Signal 31(13):933–953
Ricard N, Tu L, Le Hiress M, Huertas A, Phan C, Thuillet R, Sattler C, Fadel E, Seferian A, Montani D, Dorfmüller P, Humbert M, Guignabert C (2014) Increased pericyte coverage mediated by endothelial-derived fibroblast growth factor-2 and interleukin-6 is a source of smooth muscle-like cells in pulmonary hypertension. Circulation 129(15):1586–1597
Sawada H, Saito T, Nickel NP, Alastalo T-P, Glotzbach JP, Chan R, Haghighat L, Fuchs G, Januszyk M, Cao A, Lai Y-J, Perez VJ, Kim Y-M, Wang L, Chen P-I, Spiekerkoetter E, Mitani Y, Gurtner GC, Sarnow P, Rabinovitch M (2014) Reduced BMPR2 expression induces GM-CSF translation and macrophage recruitment in humans and mice to exacerbate pulmonary hypertension. J Exp Med 211(2):263–280
Simonneau G, Montani D, Celermajer DS, Denton CP, Gatzoulis MA, Krowka M, Williams PG, Souza R (2019) Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J 53(1):1801913
Southgate L, Machado RD, Gräf S, Morrell NW (2020) Molecular genetic framework underlying pulmonary arterial hypertension. Nat Rev Cardiol 17(2):85–95
Steffes LC, Froistad AA, Andruska A, Boehm M, McGlynn M, Zhang F, Zhang W, Hou D, Tian X, Miquerol L, Nadeau K, Metzger RJ, Spiekerkoetter E, Kumar ME (2020) A Notch3-marked subpopulation of vascular smooth muscle cells is the cell of origin for occlusive pulmonary vascular lesions. Circulation 142(16):1545–1561
Stenmark KR, Frid MG, Graham BB, Tuder RM (2018) Dynamic and diverse changes in the functional properties of vascular smooth muscle cells in pulmonary hypertension. Cardiovasc Res 114(4):551–564
Strauss B, Sassi Y, Bueno-Beti C, Ilkan Z, Raad N, Cacheux M, Bisserier M, Turnbull IC, Kohlbrenner E, Hajjar RJ, Hadri L, Akar FG (2019) Intra-tracheal gene delivery of aerosolized SERCA2a to the lung suppresses ventricular arrhythmias in a model of pulmonary arterial hypertension. J Mol Cell Cardiol 127:20–30
Thenappan T, Chan SY, Weir EK (2018) Role of extracellular matrix in the pathogenesis of pulmonary arterial hypertension. Am J Physiol Heart Circ Physiol 315(5):H1322–H1331
Tian W, Jiang X, Tamosiuniene R, Sung YK, Qian J, Dhillon G, Gera L, Farkas L, Rabinovitch M, Zamanian RT, Inayathullah M, Fridlib M, Rajadas J, Peters-Golden M, Voelkel NF, Nicolls MR (2013) Blocking macrophage leukotriene b4 prevents endothelial injury and reverses pulmonary hypertension. Sci Transl Med 5(200):200ra117
Tian W, Jiang X, Sung YK, Shuffle E, Wu T-H, Kao PN, Tu AB, Dorfmüller P, Cao A, Wang L, Peng G, Kim Y, Zhang P, Chappell J, Pasupneti S, Dahms P, Maguire P, Chaib H, Zamanian R, Peters-Golden M, Snyder MP, Voelkel NF, Humbert M, Rabinovitch M, Nicolls MR (2019) Phenotypically silent bone morphogenetic protein receptor 2 mutations predispose rats to inflammation-induced pulmonary arterial hypertension by enhancing the risk for neointimal transformation. Circulation 140(17):1409–1425
Tliba O, Panettieri RA (2009) Noncontractile functions of airway smooth muscle cells in asthma. Annu Rev Physiol 71:509–535
Tuder RM (2017) Pulmonary vascular remodeling in pulmonary hypertension. Cell Tissue Res 367(3):643–649
Udjus C, Cero FT, Halvorsen B, Behmen D, Carlson CR, Bendiksen BA, Espe EKS, Sjaastad I, Løberg EM, Yndestad A, Aukrust P, Christensen G, Skjønsberg OH, Larsen K-O (2019) Caspase-1 induces smooth muscle cell growth in hypoxia-induced pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 316(6):L999–L1012
Van Hung T, Emoto N, Vignon-Zellweger N, Nakayama K, Yagi K, Suzuki Y, Hirata K-i (2014) Inhibition of vascular endothelial growth factor receptor under hypoxia causes severe, human-like pulmonary arterial hypertension in mice: potential roles of interleukin-6 and endothelin. Life Sci 118(2):313–328
Voelkel NF, Gomez-Arroyo J, Abbate A, Bogaard HJ, Nicolls MR (2012) Pathobiology of pulmonary arterial hypertension and right ventricular failure. Eur Respir J 40(6):1555–1565
Wang R-S, Loscalzo J (2021) Network module-based drug repositioning for pulmonary arterial hypertension. CPT Pharmacometrics Syst Pharmacol 10(9):994–1005
Wang Y, Kuai Q, Gao F, Wang Y, He M, Zhou H, Han G, Jiang X, Ren S, Yu Q (2019) Overexpression of TIM-3 in macrophages aggravates pathogenesis of pulmonary fibrosis in mice. Am J Respir Cell Mol Biol 61(6):727–736
Wang X, Liu M, Zhu M-J, Shi L, Liu L, Zhao Y-L, Cheng L, Gu Y-J, Zhou M-Y, Chen L, Kumar A, Wang Y (2020) Resveratrol protects the integrity of alveolar epithelial barrier via SIRT1/PTEN/p-Akt pathway in methamphetamine-induced chronic lung injury. Cell Prolif 53(3):e12773
Wang Y, Li X, Niu W, Chen J, Zhang B, Zhang X, Wang Y, Dang S, Li Z (2021) The alveolar epithelial cells are involved in pulmonary vascular remodeling and constriction of hypoxic pulmonary hypertension. Respir Res 22(1):134
Xue C, Sowden M, Berk BC (2017) Extracellular cyclophilin A, especially acetylated, causes pulmonary hypertension by stimulating endothelial apoptosis, redox stress, and inflammation. Arterioscler Thromb Vasc Biol 37(6):1138–1146
Yeo Y, Yi ES, Kim J-M, Jo E-K, Seo S, Kim R-I, Kim KL, Sung J-H, Park SG, Suh W (2020) FGF12 (fibroblast growth factor 12) inhibits vascular smooth muscle cell remodeling in pulmonary arterial hypertension. Hypertension 76(6):1778–1786
Young LR, Gulleman PM, Short CW, Tanjore H, Sherrill T, Qi A, McBride AP, Zaynagetdinov R, Benjamin JT, Lawson WE, Novitskiy SV, Blackwell TS (2016) Epithelial-macrophage interactions determine pulmonary fibrosis susceptibility in Hermansky-Pudlak syndrome. JCI Insight 1(17):e88947
Yuan K, Shao N-Y, Hennigs JK, Discipulo M, Orcholski ME, Shamskhou E, Richter A, Hu X, Wu JC, de Jesus Perez VA (2016) Increased pyruvate dehydrogenase kinase 4 expression in lung pericytes is associated with reduced endothelial-pericyte interactions and small vessel loss in pulmonary arterial hypertension. Am J Pathol 186(9):2500–2514
Yuan K, Shamskhou EA, Orcholski ME, Nathan A, Reddy S, Honda H, Mani V, Zeng Y, Ozen MO, Wang L, Demirci U, Tian W, Nicolls MR, de Jesus Perez VA (2019) Loss of endothelium-derived Wnt5a is associated with reduced pericyte recruitment and small vessel loss in pulmonary arterial hypertension. Circulation 139(14):1710–1724
Zhang C, Zhu X, Hua Y, Zhao Q, Wang K, Zhen L, Wang G, Lü J, Luo A, Cho WC, Lin X, Yu Z (2019) YY1 mediates TGF-β1-induced EMT and pro-fibrogenesis in alveolar epithelial cells. Respir Res 20(1):249
Zhao Q, Song P, Zou M-H (2021) AMPK and pulmonary hypertension: crossroads between vasoconstriction and vascular remodeling. Front Cell Dev Biol 9:691585
Acknowledgments
This work was supported by National Natural Science Foundation of China (No. 81973404, 81503058), Department of Education of Liaoning Province (No. JC2019034).
Declaration of Competing Interest: The authors declare that there are no competing interests.
Author Contributions: All authors contributed to the study conception and design. The first draft of the manuscript was written by Yan Zhang, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Zhang, Y., Wang, Y. (2022). Cell-to-Cell Crosstalk: A New Insight into Pulmonary Hypertension. In: Pedersen, S.H.F. (eds) Reviews of Physiology, Biochemistry and Pharmacology. Reviews of Physiology, Biochemistry and Pharmacology, vol 184. Springer, Cham. https://doi.org/10.1007/112_2022_70
Download citation
DOI: https://doi.org/10.1007/112_2022_70
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-24203-8
Online ISBN: 978-3-031-24204-5
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)