
Abstract
Background and Objective: Rivaroxaban is an oral, direct Factor Xa inhibitor, which is at an advanced stage of clinical development for prevention and treatment of thromboembolic disorders. Two phase II studies, ODIXa-DVT and EINSTEIN DVT, assessed the efficacy and safety of oral rivaroxaban (once daily or twice daily) for treatment of acute deep-vein thrombosis (DVT). Population pharmacokinetic and pharmacodynamic analyses of rivaroxaban in patients in these two phase II studies were conducted to characterize the pharmacokinetics/pharmacodynamics of rivaroxaban and the relationship between important patient covariates and model parameters. Exposure simulations in patients with atrial fibrillation (AF) were also performed in order to predict the exposure of rivaroxaban, using modified demographic data reflecting the characteristics of a typical AF population.
Methods: A population pharmacokinetic model was developed using plasma samples from these patients. Various simulations were conducted to explore the pharmacokinetics of rivaroxaban in patients with DVT and to predict exposure in those with AF. Correlations between plasma rivaroxaban concentrations and the prothrombin time, Factor Xa activity, HepTest® and activated partial thromboplastin time were also described.
Results: The pharmacokinetics of rivaroxaban in patients with DVT were found to be consistent and predictable across all doses studied. The area under the plasma concentration-time curve (AUC) increased dose dependently. The same total daily doses given once daily achieved higher maximum plasma concentration (Cmax) values (∼20%) and lower trough (minimum) plasma concentration (Ctrough) values (∼60%) than when given twice daily; however, the 5th–95th percentile ranges for these parameters overlapped. Rivaroxaban clearance was moderately influenced by age and renal function, and the volume of distribution was influenced by age, body weight and sex; the effects were within the observed interindividual variability. Simulations in virtual patient populations with AF showed that a rivaroxaban dose of 15 mg once daily in patients with creatinine clearance of 30–49 mL/min would achieve AUC and Cmax values similar to those observed with 20 mg once daily in patients with normal renal function. The prothrombin time correlated almost linearly with plasma rivaroxaban concentrations (≤500 µg/L).
Conclusion: Population analyses of phase II clinical data indicated that the pharmacokinetics and pharmacodynamics of all rivaroxaban doses were predictable and were affected by expected demographic factors in patients with acute DVT.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Venous thromboembolism (VTE), manifesting as deep-vein thrombosis (DVT) and pulmonary embolism (PE), is a major cause of morbidity and mortality in the Western world.[1,2] In the US alone, there are at least 200 000 new cases of VTE each year.[3] Anticoagulant therapy is recommended for treatment of VTE, with the primary goal of stopping thrombus growth and preventing PE.[4,5]
Current VTE treatment guidelines recommend initial therapy with dose-adjusted intravenous unfractionated heparin, subcutaneous low-molecular-weight heparin (LMWH) adjusted to body weight, or fondaparinux sodium for at least 5 days, followed by long-term treatment with a laboratory-monitored vitamin K antagonist (VKA).[5] VKA therapy has drawbacks, including a slow onset/offset of action, a narrow therapeutic window, multiple food and drug interactions, and a need for dose adjustments according to laboratory monitoring.[6] An oral anticoagulant drug that does not require monitoring of its effect, with a rapid onset of action and a high benefit/risk ratio, is of considerable interest.
Rivaroxaban is an oral, direct Factor Xa inhibitor.[7] It has a dual mode of elimination, with two-thirds of the dose being metabolized in the liver (via cytochrome P450 [CYP] 3A4, CYP2J2 and CYP-independent biotransformation processes), half of which is excreted via the kidneys and half via the hepatobiliary route. One-third of the dose is directly excreted renally as the unchanged active compound.[8,9] Early clinical studies demonstrated that rivaroxaban has strong anticoagulant effects and predictable pharmacokinetic and pharmacodynamic profiles in healthy subjects.[10,11] These findings were confirmed in patients undergoing orthopaedic surgery.[12,13] Four large phase III clinical trials (the RECORD [Regulation of Coagulation in Orthopaedic Surgery to Prevent Deep Vein Thrombosis and Pulmonary Embolism] programme) showed that rivaroxaban is more effective than enoxaparin sodium and at least as safe as enoxaparin sodium for prevention of VTE after total hip- or knee-replacement surgery.[14–17]
Two large dose-ranging studies evaluated rivaroxaban for treatment of patients with acute symptomatic DVT.[18,19] Combined analysis of the two studies indicates that the optimal regimen consists of rivaroxaban 15 mg twice daily for 3 weeks, followed by once-daily administration of 20 mg for the subsequent treatment period. This regimen is associated with an efficacy and safety profile that is at least as good as that of conventional LMWH therapy, and this has been further confirmed by the recently completed EINSTEIN DVT phase III study.[20]
A population pharmacokinetic model that was generated using data from healthy subjects[21] has previously been extended to describe the pharmacokinetics and pharmacodynamics of rivaroxaban in patients receiving rivaroxaban for prevention of VTE after major orthopaedic surgery.[12,13] The aims of the present population analyses were to characterize the pharmacokinetics/pharmacodynamics of rivaroxaban in patients with acute DVT. Sparse pharmacokinetic/pharmacodynamic samples from the DVT dose-ranging studies were used to derive a population pharmacokinetic/pharmacodynamic model. This enabled evaluation of demographic factors (age, sex, body weight and renal function) that influence the pharmacokinetics of rivaroxaban when administered once daily or twice daily in this patient population. A further aim of this study was to simulate the pharmacokinetics of rivaroxaban in virtual patient populations with atrial fibrillation (AF). As patients with AF tend to be older, the pharmacokinetic model was adapted to represent a typical AF population in order to predict rivaroxaban exposure in virtual patient populations with AF.
Methods
Studies Included in the Analyses
The ODIXa-DVT (Oral Direct Factor Xa Inhibitor BAY 59–7939 in Patients with Acute Symptomatic Deep-Vein Thrombosis) study[18] and the EINSTEIN DVT study[19] were dose-ranging, randomized, comparator-controlled studies, which assessed the efficacy and safety of a variety of rivaroxaban regimens for treatment of acute DVT. A total of 1156 patients with confirmed acute, symptomatic, proximal DVT were enrolled. Key exclusion criteria were body weight ≤45 kg (ODIXa-DVT only[18]), severe renal impairment (calculated creatinine clearance [CLCR] <30 mL/min or a serum creatinine level [SCR] >1.5 × the upper limit of normal [ULN]), severe hepatic impairment (transaminases >2 × ULN) and systemic treatment with azole compounds or other strong CYP3A4 inhibitors. Patients were randomized to receive either double-blind rivaroxaban or open-label standard therapy. The studies evaluated different dosing regimens. Patients in ODIXa-DVT[18] received rivaroxaban 10, 20 or 30 mg twice daily; 40 mg once daily; or standard therapy. Patients in EINSTEIN DVT received rivaroxaban 20, 30 or 40 mg once daily; or standard therapy. The treatment duration was 12 weeks in both studies.
Sparse blood samples were taken from patients in both studies shortly after the start of treatment and at steady state. This technique was chosen because it was not considered realistic for outpatients to return to hospital at frequent intervals over the 3-month period. The sampling regimen for ODIXa-DVT[18] was as follows: on study day 1 or day 2, blood samples were taken 1, 3 and 6 hours after dosing and in the time interval between 8 hours after dosing and the second daily dose (i.e. 8–12 hours after the first dose) before the next dose was given. Samples were taken on day 2 only when patients had not started the study medication before 10:00 on day 1 and were only administered the evening dose. On study day 21, blood samples were taken 1 hour before morning dosing and 1, 3 and 6 hours after dosing. In EINSTEIN DVT, baseline samples were collected before randomization on study day 1 and then 2–6 hours after the first dose of rivaroxaban. In addition, on study day 43, a sample was taken immediately before the next dose, and on study day 84, a sample was taken 2–6 hours after the last rivaroxaban dose.
Pharmacokinetic and Pharmacodynamic Assays
The plasma rivaroxaban concentrations, Factor Xa activity, prothrombin time (PT), activated partial thromboplastin time (aPTT) and HepTest® (American Diagnostica, Stamford, CT, USA) were determined in the same laboratory, using methods described previously.[10] The PT was determined according to standard procedures at a central laboratory using STA® Neoplastine® (Diagnostica Stago, Asnières sur Seine, France) with an international sensitivity index of 1.82–1.85 and was used in the pharmacodynamic investigation.
Population Pharmacokinetic/Pharmacodynamic Modelling
Because of the lack of rich pharmacokinetic/pharmacodynamic data, a population-modelling approach, based on the data from the sparse sampling, was used. This analysis provides estimates of population mean values and descriptions of the variability inherent in a population. In addition, sources of variability, such as patient covariates, can be assessed, and post hoc empirical Bayes estimates allow for prediction of individual patient pharmacokinetic/pharmacodynamic parameters. All modelling was based on previously developed models derived from the population pharmacokinetic/pharmacodynamic analyses in healthy subjects[21] and the ones used to determine the population pharmacokinetics/pharmacodynamics in patients undergoing total hip replacement.[12,13]
Population pharmacokinetic/pharmacodynamic analyses were performed using non-linear mixed-effects modelling software (NONMEM® Version V Level 1.1; GloboMax LLC, Hanover, MD, USA) operated in a validated Linux server farm environment. The first-order conditional estimation with interaction method was used for all analyses. All statistics and graphs were generated using S-Plus Version 6 software (Insightful Corp., Seattle, WA, USA) or SAS Version 8.2 software (SAS Institute Inc., Cary, NC, USA).
NONMEM® is a mixed-effects modelling technique used to quantify random effects, such as unexplained interindividual variability (IIV) and residual variability, as well as the influence of measured patient characteristics or covariates (fixed effects) on basic (structural) model parameters (fixed effects).[22] Therefore, the developed population models can be viewed as consisting of three sub-models: a structural sub-model, a statistical sub-model and a covariate sub-model. The structural pharmacokinetic or pharmacokinetic/pharmacodynamic sub-model describes the structure, using fixed-effects parameters, and the statistical sub-model accounts for variability, using various levels of random effects, IIV and residual variability. Exponential models were used to account for IIV in the structural parameters. Residual variability was investigated as being additive, proportional or a combination of both. Local linear relationships were used to link pharmacokinetic/pharmacodynamic parameters with potential continuous covariates; the influence of categorical covariates was expressed as being present/absent.
The pharmacokinetic or pharmacokinetic/pharmacodynamic model structure was optimized; the goal was to reduce unexplained variability. Model components were incorporated into the model if the likelihood ratio test showed a p-value of ≤0.01 (a change in the objective function value [OFV] of >6.63). The model component remained in the model if, after backwards stripping from the full model, the likelihood ratio test showed a p-value of ≤0.001 (a change in the OFV of >10.8). In addition to goodness-of-fit statistics using the likelihood ratio test, goodness-of-fit graphs were used to evaluate the adequacy of the model.
An oral, one-compartment model was used as the starting point for the structural pharmacokinetic model, with the clearance (CL), volume of distribution (Vd) and first-order absorption rate constant (ka) as parameters. No data are currently available on the absolute bioavailability (F) of rivaroxaban; therefore, F was used to describe potential differences in the relative bioavailability between the different dosing regimens. As a result, CL and Vd were modelled as CL/F and Vd/F, respectively.
The predefined covariates that were evaluated for their influence on both the pharmacokinetic and pharmacokinetic/pharmacodynamic structural models were the effect of time (visit number); dosage; patient covariates (including age, body weight, height, body surface area, lean body mass [LBM], body fat, sex, SCR and CLCR calculated according to the Cockcroft-Gault formula);[23] and selected concomitant medications (including opioids, NSAIDs, diuretics and prespecified drugs that accelerate gastrointestinal passage).
Further selected co-medications, which were being taken by <10% of subjects — such as CYP3A4 inducers (rifampicin [rifampin], carbamazepine, phenobarbital [phenobarbitone], phenytoin), atorvastatin and aspirin (acetylsalicylic acid) — were evaluated for exposure differences between treatment groups in an exploratory, descriptive manner.
The pharmacokinetic/pharmacodynamic structural models for Factor Xa activity and for the PT, aPTT and HepTest® were developed from a conventional direct-effect linear model (linear intercept model) for the PT and a maximum effect (Emax) model, including a baseline effect for Factor Xa activity, aPTT and HepTest®.
Predictions of Exposure Parameters, Validation andSimulations
The pharmacokinetic data obtained from the blood samples taken from patients across both studies were pooled and used with the population model to estimate the pharmacokinetic profile of rivaroxaban in the VTE treatment population. Specific exposure parameters for rivaroxaban, such as the area under the plasma concentration-time curve (AUC) and maximum and trough (minimum) plasma concentrations (Cmax and Ctrough, respectively), were estimated for each individual in both studies for the dosing regimen that he or she received. Simulations were conducted to investigate the influence of once-daily or twice-daily dosing on rivaroxaban exposure.
Plasma rivaroxaban concentration-time profiles in elderly patients, patients with severe and moderate renal impairment (CLCR ≤30 mL/min and 30–50 mL/min, respectively) and patients with body weight at the upper and lower limits of the population were simulated for both once-daily and twice-daily doses. The predicted plasma concentrations of rivaroxaban once daily and twice daily for each typical patient were grouped demographically and plotted for comparison alongside the mean plasma concentration for the entire pooled population. Further simulations were conducted to predict the exposure of rivaroxaban for the dosing regimen that was selected for the phase III VTE treatment studies.
Non-parametric bootstraps (n = 1000) were performed on the original dataset. All pharmacokinetic/pharmacodynamic parameters were estimated using the respective final models and analysed via descriptive statistics (see figure S-1 in Supplemental Digital Content 1, available online at http://links.adisonline.com/CPZ/A20). Visual predictive checks were conducted to further investigate the validity of the established models. Individual empirical Bayesian estimates for pharmacokinetics and pharmacokinetics/pharmacodynamics were calculated (via the NONMEM® post hoc procedure) using population means, variation and individual patient information, by simulating sub-problems (n = 200). The 5th–95th percentile ranges were calculated and compared with the observations (see figure S-2a and S-2b in Supplemental Digital Content 1).
To predict the exposure of rivaroxaban in virtual patient populations with AF, the DVT treatment population data were modified to reflect the demographic characteristics of a patient population with AF. Demographic data from two clinical studies in AF[24,25] were used to represent a typical AF population. The VTE treatment population data were thus modified to reflect the mean age of the AF population (∼70 years), and SCR values were increased to reflect the decrease in renal function in this population.[26,27]
Results
Patients (n = 870) from both dose-ranging studies supplied 4634 rivaroxaban plasma samples. Overall, there were more males than females; however, there was a larger percentage of patients aged ≥75 years among the women than among the men (table I). The average female patient had an LBM approximately 25% lower than that of the average male patient (median LBM: 47 kg female, 63 kg male; table I). The average normal body weights were 73 kg and 85 kg for female and male patients, respectively (table I).

Pharmacokinetic Model
Using the pooled data, the pharmacokinetics of rivaroxaban were closely described by an oral, one-compartment model, with the CL, Vd and ka as parameters (table II). Rivaroxaban CL was estimated to be 5.67 L/h, with IIV of 39.9%. The Vd was estimated to be 54.4 L, with IIV of 28.8% — similar to that observed in healthy subjects (table II).[13,21] In the final population pharmacokinetic model, inclusion of the covariates age and SCR decreased the IIV in CL from 42% to 40%, and inclusion of the covariates LBM and age decreased the IIV in the Vd from 32% to 29%. No time-dependent effects on the pharmacokinetics of rivaroxaban were detected in patients over the 12-week course of the studies.

Oral, one-compartment population pharmacokinetic model for rivaroxaban in deep-vein thrombosis patients
The rivaroxaban AUC increased dose dependently with both once-daily and twice-daily dosing; similar AUCs were obtained for both once-daily and twice-daily dosing (figure 1a). When comparing the same total daily doses, the Cmax was higher (∼20%) and the Ctrough was lower (∼60%) with once-daily dosing than with twice-daily dosing; however, the 5th–95th percentile ranges for these parameters overlapped (figure 1b and 1c).

Box-and-whisker plots for rivaroxaban dosing in the ODIXa-DVT[18] and EINSTEIN DVT[19] studies: (a) the area under the plasma concentration-time curve from 0 to 24 hours (AUC24); (b) the maximum plasma concentration (Cmax); and (c) the trough (minimum) plasma concentration (Ctrough). All doses were once daily (od) and twice daily (bid) in patients receiving rivaroxaban for treatment of deep-vein thrombosis. The horizontal line within each box is the mean; the lower and upper limits of the box are the 25th and 75th percentiles, respectively; the whiskers are the 10th and 90th percentiles; and the circles are the 5th and 95th percentiles.
Demographic factors influencing the CL of rivaroxaban were age and renal function (expressed as CLCR); the Vd of rivaroxaban was influenced by age, body weight and, indirectly, by sex (table III). Variations in the rivaroxaban CL and Vd due to these demographic characteristics were moderate and within the IIV observed in patients enrolled in the two studies. Negative correlations were observed between age and both the CL and Vd of rivaroxaban, as well as the CLCR and CL of rivaroxaban, whereas a positive correlation was observed between the Vd and body weight (figure 2).

Effects of demographic factors on rivaroxaban clearance (CL) and volume of distribution (Vd)

Relationship between demographic factors and rivaroxaban clearance (CL) and volume of distribution (Vd) in male and female patients: (a) CL and age; (b) CL and creatinine clearance (CLCR); (c) Vd and age; and (d) Vd and body weight.
Effect of Demographic Factors on Rivaroxaban Exposure
In all once-daily and twice-daily simulations, plasma rivaroxaban concentrations reached the Cmax 2–4 hours after administration (figure 3). In all once-daily and twice-daily simulations, age and renal function had a moderate influence on rivaroxaban exposure; the influence of body weight was small. The Cmax for all simulations was within the 5th–95th percentile ranges of the population mean; this included a simulation of a typical patient aged 90 years with severe renal impairment (CLCR ≤30 mL/min).

Predicted plasma rivaroxaban concentration-time profiles for extremes in age, renal function and body weight for patients receiving (a) rivaroxaban 20 mg once daily or (b) rivaroxaban 10 mg twice daily. The simulated patients had typical mean characteristics (age 60 years, body weight 80 kg, creatinine clearance [CLCR] 90 mL/min) unless specified otherwise.
Simulations of the phase III VTE treatment dosing regimen (rivaroxaban 15 mg twice daily for 3 weeks followed by rivaroxaban 20 mg once daily) demonstrated that the transition from twice-daily to once-daily dosing should not expose patients to substantial fluctuations in the Cmax (figure 4).

Simulated venous thromboembolism treatment dosing regimen of rivaroxaban 15 mg twice daily (bid) for 3 weeks, followed by rivaroxaban 20 mg once daily (od) [N = 870].
Effect of Concomitant Medications on the Pharmacokinetics of Rivaroxaban
The absorption of rivaroxaban increased slightly with concomitant administration of drugs that accelerate passage through the gastrointestinal tract (e.g. laxatives, metoclopramide; n = 48) and decreased slightly when administered with opioids. Both of these influences resulted in a less than 15% change in the absorption rate and did not significantly affect overall exposure to rivaroxaban. Diuretics, NSAIDs and aspirin did not have any relevant effect on the pharmacokinetics of rivaroxaban. In a cohort of 28 patients, concomitant administration of drugs that are known for their potential to strongly induce CYP3A4, such as carbamazepine, phenobarbital and phenytoin, resulted in a reduction of up to 50% in rivaroxaban exposure, irrespective of the dose and dosing regimen.
Correlation between Plasma Rivaroxaban Concentrations and Pharmacodynamics
The concentration-effect relationships for all pharmacodynamic parameters (the PT, Factor Xa, HepTest® and aPTT) were broadly consistent with the previous findings[12] and showed rapid, direct responses to rivaroxaban treatment.
Plasma rivaroxaban concentrations of up to approximately 500 µg/L correlated with the PT in an almost linear fashion (figure 5). The slope of the correlation became non-linear at higher plasma rivaroxaban concentrations. At steady state, the baseline PT was estimated to be 12.5 seconds and the slope of the correlation was 3.3 seconds/100 µg/L. The residual variability was low (10.3%). Renal function had a small effect on the gradient of the slope (less than 23% maximum for the CLCR range in this study population). No other demographic factors or concomitant medications had a significant effect on the relationship between the plasma rivaroxaban concentration and PT.

Plasma rivaroxaban concentration-effect relationship for the prothrombin time (PT) analysis, showing the observed and population mean (model) values.
The plasma rivaroxaban concentration and inhibition of Factor Xa activity correlated following an inhibitory Emax model. Age had a small effect on baseline Factor Xa activity, although the clinical relevance of this is unknown. No covariates were found to exhibit significant effects on the Emax-type relationship between rivaroxaban concentrations and the HepTest® (data not shown). Because of the high variability in the aPTT response (which was consistent with previous findings), and the low sensitivity of the aPTT to rivaroxaban seen in this study, concentration-effect modelling for this pharmacodynamic parameter was limited, and thus no definitive Emax-type exposure relationship could be established.
Prediction of the Pharmacokinetics of Rivaroxaban in Patients with Atrial Fibrillation
Compared with patients with DVT, patients with AF tended to be older and to have decreased renal function. Thus, modified DVT population demographics (such as age and CLCR) were used to simulate a population of 1000 patients with AF (table I). Using this virtual AF population and the pharmacokinetic model that was established above, the average Cmax of rivaroxaban in AF patients was predicted to be 7.4% higher than that in DVT patients (290 µg/L vs 270 µg/L), albeit within the 5th–95th percentile ranges in the average DVT patient receiving the same dose. The difference in the Ctrough between the AF and DVT populations was more pronounced (32 µg/L vs 25.5 µg/L; a 25.5% increase), as was the difference in the AUC (3310 µg · h/L vs 2870 µg · h/L; a 15.3% increase).
Simulations were conducted to determine which demographic factors influenced the increase in rivaroxaban exposure that was observed in AF patients. These simulations demonstrated that moderate renal impairment (i.e. CLCR 30–49 mL/min) and, to a lesser extent, increased age (≥75 years) led to a slight increase in rivaroxaban exposure (figure 6) because of reduced clearance, a prolonged elimination half-life and increased Ctrough values. Body weight and sex did not influence rivaroxaban exposure.

Rivaroxaban exposure, expressed as the area under the plasma concentration-time curve from 0 to 24 hours (AUC24), for the total simulated virtual atrial fibrillation population compared with individual demographic extremes: age ≥75 years, lean body mass (LBM) ≤50 kg, serum creatinine level (SCR) ≥1.2 mg/dL and creatinine clearance (CLCR) ≤50 mL/min. For CLCR ≤50 mL/min, results from rivaroxaban 20 mg once daily (od) and 15 mg od are shown; for the other simulations, only results from rivaroxaban 20 mg od are shown. The horizontal line within each box is the mean; the lower and upper limits of the box are the 25th and 75th percentiles, respectively; the whiskers are the 10th and 90th percentiles; and the circles are the 5th and 95th percentiles.
The simulated plasma concentration-time profile for AF patients with normal renal function receiving 20 mg once daily was similar to the estimated plasma concentration-time profile for DVT patients receiving the same dose. In the AF and DVT populations, the Cmax values were 274 µg/L and 270 µg/L, respectively; the Ctrough values were 30 µg/L and 25.5 µg/L, respectively; and the AUC values were 3120 µg · h/L and 2870 µg · h/L, respectively. Simulations of AF patients with moderate renal impairment were compared for patients receiving rivaroxaban 15 mg once daily or 20 mg once daily. The increase in rivaroxaban exposure due to decreased renal function in this simulation was corrected by dose adjustment to 15 mg once daily (figure 7).

Plasma rivaroxaban concentration-time profiles for the simulated virtual atrial fibrillation population. For patients with creatinine clearance (CLCR) >50 mL/min, results from rivaroxaban 20 mg once daily (od) are shown; for patients with CLCR ≤50 mL/min, results from rivaroxaban 15 mg od are shown.
Discussion and Conclusion
These analyses of phase II DVT dose-ranging studies indicate that the pharmacokinetics and pharmacodynamics of rivaroxaban at all doses that were tested (20–60 mg total daily doses, administered either once daily or twice daily) were predictable and were affected by the expected demographic factors in DVT patients.
The pharmacokinetic/pharmacodynamic data from the two dose-ranging studies were used in these analyses.[18,19] In these studies, a sparse sampling technique was used. As a result of this sparse sampling approach, the pharmacokinetic/pharmacodynamic data over time were incomplete, and population modelling was used to derive the full pharmacokinetic and pharmacodynamic profiles of rivaroxaban.
The demographic factors that were identified as affecting the rivaroxaban CL and Vd were consistent with previous findings in healthy subjects and in patients receiving rivaroxaban for prevention of VTE after total hip- or knee-replacement surgery.[13,21] Approximately one-third of rivaroxaban is excreted unchanged by the kidneys;[8,9] therefore, it was anticipated that renal function, which decreases with age,[28] would affect the pharmacokinetics of rivaroxaban. In this analysis, both increased age and decreased renal function led to a decrease in rivaroxaban CL.
The Vd was moderately affected by age, body weight and, indirectly, by sex. As expected, body weight correlated directly with the Vd. The influence of sex is probably due to the difference in body weight between male and female patients; female patients had a lower average body weight than males and, therefore, a decreased Vd. The influence of age is also probably related to sex/body weight factors: in this study population, sex distribution was not constant across the age groups, with higher percentages of females in the older age groups. Therefore, the average body weight of older patients was lower than the average body weight of the whole population, leading to a decreased average Vd in elderly patients.
Rivaroxaban exposure was affected by changes in the CL and Vd. Elderly patients and those with a lower body weight had a slight decrease in the CL and Vd, leading to a slight increase in rivaroxaban exposure. Using this population model, it would theoretically be possible to predict the effects of rivaroxaban in patients with severe renal impairment; however, as with other drugs that have been evaluated in clinical trials, patients with severe renal impairment were excluded from these phase II studies. Patients with moderate-to-severe renal impairment (CLCR approximately 30 mL/min) had a moderate decrease in the CL and Vd, leading to a moderate increase in rivaroxaban exposure. However, the predicted Cmax of rivaroxaban for all patients was within the 5th–95th percentile ranges calculated for the average patient in the population.
Pharmacokinetics and pharmacokinetics/pharmacodynamics were consistent over the 12-week duration of the studies. The variability in the pharmacokinetics of rivaroxaban in this patient population was moderate and comparable with previous results.[12,13,21] The pharmacokinetics of rivaroxaban were similar when given once daily or twice daily. Dose-dependent increases in rivaroxaban exposure were observed with all once-daily and twice-daily doses, in line with findings in healthy subjects and in patients receiving rivaroxaban for prevention of VTE after total hip- or knee-replacement surgery.[13,21] As expected, when comparing the same total daily doses, rivaroxaban given once daily demonstrated a higher Cmax and a lower Ctrough than when given twice daily; however, the differences were within the 5th–95th percentile ranges for the population median. This suggests that once-daily dosing of rivaroxaban should not expose patients to a greater risk of bleeding (at the Cmax) or thrombus growth (at the Ctrough) than twice-daily dosing, as discussed when the two clinical trials were compared.[18,19]
Concomitant administration of long-term medications that are frequently prescribed to patients within this population, including diuretics, NSAIDs and aspirin, did not have any relevant effect on the pharmacokinetics of rivaroxaban, suggesting that it may be possible to co-administer rivaroxaban with these medications.
The slope of the plasma concentration-PT correlation graph reflected the sensitivity of the PT to increases in rivaroxaban exposure. The PT correlated in an almost linear fashion with rivaroxaban concentrations ≤500 µg/L, confirming that the PT could be used to assess exposure. The correlation became non-linear at higher plasma rivaroxaban concentrations; however, there were very few data points at such high concentrations, which in turn are unlikely to be observed in routine clinical practice. However, the commercially available PT tests, which provide results as percentages of normal and/or convert the results into international normalized ratio values, should not be used for assessing the anticoagulant effect of rivaroxaban. The pharmacodynamic effects of rivaroxaban as measured by the PT are strongly affected by the type of PT reagent used and, as a result, international normalized ratio values obtained with rivaroxaban do not correlate with the intensity of anticoagulation[12,29] and cannot be used to predict the efficacy and safety of the drug.
The prevalence of both AF and renal impairment increases with age;[28,30] therefore, patients with AF often have decreased renal function. This analysis suggests that increased rivaroxaban exposure in patients with AF may be caused by reduced rivaroxaban clearance due to reduced renal function. A dose of rivaroxaban 20 mg once daily was chosen for investigation in the phase III trial ROCKET AF (Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation).[31] However, a lower fixed dose of 15 mg once daily was chosen for patients with moderate renal impairment (CLCR 30–49 mL/min) in order to assess the effect of this reduced dose in this specific patient population. This analysis suggests that renally impaired patients receiving the lower dose should have similar exposure to that of patients with normal renal function receiving rivaroxaban 20 mg once daily.
In summary, the pharmacokinetics and pharmacodynamics of all rivaroxaban doses in the two DVT dose-ranging studies were found to be predictable and were affected by anticipated demographic factors, whether rivaroxaban was administered once daily or twice daily.
This analysis, combined with the efficacy and safety results from the DVT dose-ranging studies,[18,19] led to the selection of an intensified 15 mg twice-daily dose of rivaroxaban for 3 weeks, followed by a long-term 20 mg once-daily dose for evaluation in the phase III studies for treatment of VTE. The phase III rivaroxaban VTE treatment programme includes the following trials: EINSTEIN DVT,[20] EINSTEIN PE[32] and EINSTEIN Extension.[20]
EINSTEIN DVT[20] and EINSTEIN PE[32] are phase III clinical trials that utilize the same study protocol. In both trials, rivaroxaban is compared with therapeutic doses of enoxaparin sodium followed by a VKA. The studies are event-driven, non–inferiority programmes for efficacy with treatment durations of 3, 6 or 12 months. The EINSTEIN PE[32] trial, which is ongoing, is evaluating rivaroxaban in patients with acute symptomatic PE with or without symptomatic DVT. The EINSTEIN DVT trial[20] has been completed recently, and the results indicated that rivaroxaban was at least as effective as enoxaparin sodium/VKA therapy for prevention of recurrent VTE in patients with acute DVT without symptomatic PE.
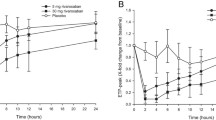
In the EINSTEIN Extension trial,[20] patients who had completed 6 or 12 months of treatment with rivaroxaban or a VKA for an acute episode of VTE were randomized to receive an additional 6 or 12 months of therapy with either rivaroxaban 20 mg once daily or placebo. The primary efficacy outcome was symptomatic recurrent VTE, whereas the principal safety outcome was major bleeding. The results showed that rivaroxaban was associated with a significantly lower rate of symptomatic recurrent venous thromboembolic events compared with the placebo, without a significant increase in major bleeding,[20] demonstrating promising efficacy and safety of rivaroxaban for long-term treatment of VTE.
Furthermore, the ROCKET AF study has also been completed recently.[31] The results showed that patients with AF who were receiving active treatment with rivaroxaban (20 mg once daily, or 15 mg once daily in patients with CLCR of 30–49 mL/min) had a significantly lower risk of stroke and non-central nervous system systemic embolism than those receiving warfarin, with similar rates of bleeding.[31]
References
White RH. The epidemiology of venous thromboembolism. Circulation 2003 Jun; 107(23 Suppl. 1): I4–I8
Heit JA. Venous thromboembolism: disease burden, outcomes and risk factors. J Thromb Haemost 2005 Aug; 3(8): 1611–7
Heit JA, Silverstein MD, Mohr DN, et al. The epidemiology of venous thromboembolism in the community. Thromb Haemost 2001 Jul; 86(1): 452–63
Snow V, Qaseem A, Barry P, et al. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med 2007 Feb; 146(3): 204–10
Kearon C, Kahn SR, Agnelli G, et al. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest 2008 Jun; 133(6 Suppl.): 454S–545S
Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest 2008 Jun; 133(6 Suppl.): 160S–198S
Perzborn E, Strassburger J, Wilmen A, et al. In vitro and in vivo studies of the novel antithrombotic agent BAY 59-7939 — an oral, direct Factor Xa inhibitor. J Thromb Haemost 2005 Mar; 3(3): 514–21
Lang D, Freudenberger C, Weinz C. In vitro metabolism of rivaroxaban — an oral, direct Factor Xa inhibitor — in liver microsomes and hepatocytes of rat, dog and man. Drug Metab Dispos 2009 May; 37(5): 1046–55
Weinz C, Schwarz T, Kubitza D, et al. Metabolism and excretion of rivaroxaban, an oral, direct Factor Xa inhibitor, in rats, dogs and humans. Drug Metab Dispos 2009 May; 37(5): 1056–64
Kubitza D, Becka M, Voith B, et al. Safety, pharmacodynamics, and pharmacokinetics of single doses of BAY 59-7939, an oral, direct factor Xa inhibitor. Clin Pharmacol Ther 2005 Oct; 78(4): 412–21
Kubitza D, Becka M, Wensing G, et al. Safety, pharmacodynamics, and pharmacokinetics of BAY 59-7939 — an oral, direct Factor Xa inhibitor — after multiple dosing in healthy male subjects. Eur J Clin Pharmacol 2005 Dec; 61(12): 873–80
Mueck W, Eriksson BI, Bauer KA, et al. Population pharmacokinetics and pharmacodynamics of rivaroxaban — an oral, direct factor Xa inhibitor — in patients undergoing major orthopaedic surgery. Clin Pharmacokinet 2008 Mar; 47(3): 203–16
Mueck W, Borris LC, Dahl OE, et al. Population pharmacokinetics and pharmacodynamics of once- and twice-daily rivaroxaban for the prevention of venous thromboembolism in patients undergoing total hip replacement. Thromb Haemost 2008 Sep; 100(3): 453–61
Eriksson BI, Borris LC, Friedman RJ, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med 2008 Jun; 358(26): 2765–75
Kakkar AK, Brenner B, Dahl OE, et al. Extended duration rivaroxaban versus short-term enoxaparin for the prevention of venous thromboembolism after total hip arthroplasty: a double-blind, randomised controlled trial. Lancet 2008 Jul; 372(9632): 31–9
Lassen MR, Ageno W, Borris LC, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty. N Engl J Med 2008 Jun; 358(26): 2776–86
Turpie AGG, Lassen MR, Davidson BL, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): a randomised trial. Lancet 2009 May; 373(9676): 1673–80
Agnelli G, Gallus A, Goldhaber SZ, et al. Treatment of proximal deep-vein thrombosis with the oral direct Factor Xa inhibitor rivaroxaban (BAY 59-7939): the ODIXa-DVT (Oral Direct Factor Xa Inhibitor BAY 59-7939 in Patients with Acute Symptomatic Deep-Vein Thrombosis) study. Circulation 2007 Jul; 116(2): 180–7
Buller HR, Lensing AW, Prins MH, et al. A dose-ranging study evaluating once-daily oral administration of the Factor Xa inhibitor rivaroxaban in the treatment of patients with acute symptomatic deep vein thrombosis: the EINSTEIN-DVT dose-ranging study. Blood 2008 Sep; 112(6): 2242–7
The EINSTEIN Investigators. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 2010 Dec; 363(26): 2499–510
Mueck W, Becka M, Kubitza D, et al. Population model of the pharmacokinetics and pharmacodynamics of rivaroxaban — an oral, direct Factor Xa inhibitor — in healthy subjects. Int J Clin Pharmacol Ther 2007 Jun; 45(6): 335–44
Beal SL, Sheiner LB. Estimating population kinetics. Crit Rev Biomed Eng 1982; 8(3): 195–222
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron 1976; 16(1): 31–41
Halperin JL; Executive Steering Committee, SPORTIF III and V Study Investigators. Ximelagatran compared with warfarin for prevention of thromboembolism in patients with nonvalvular atrial fibrillation: rationale, objectives, and design of a pair of clinical studies and baseline patient characteristics (SPORTIF III and V). Am Heart J 2003 Sep; 146(3): 431–8
Olsson SB; Executive Steering Committee of the SPORTIF III Investigators. Stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): randomised controlled trial. Lancet 2003 Nov; 362(9397): 1691–8
Jones CA, McQuillan GM, Kusek JW, et al. Serum creatinine levels in the US population: third National Health and Nutrition Examination Survey. Am J Kidney Dis 1998 Dec; 32(6): 992–9
Kubitza D, Becka M, Roth A, et al. Dose-escalation study of the pharmacokinetics and pharmacodynamics of rivaroxaban in healthy elderly subjects. Curr Med Res Opin 2008 Oct; 24(10): 2757–65
Clark B. Biology of renal aging in humans. Adv Ren Replace Ther 2000 Jan; 7(1): 11–21
Samama MM, Martinoli JL, Leflem L, et al. Assessment of laboratory assays to measure rivaroxaban — an oral, direct factor Xa inhibitor. Thromb Haemost 2010 Mar; 103(4): 815–25
Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA 2001 May; 285(18): 2370–5
Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. Epub 2011 Aug 10
Bayer. Oral direct Factor Xa inhibitor rivaroxaban in patients with acute symptomatic pulmonary embolism with or without symptomatic deep-vein thrombosis: EINSTEIN-PE evaluation [ClinicalTrials.gov identifier NCT00439777]. US National Institutes of Health, ClinicalTrials.gov [online]. Available from URL: http://www.clinicaltrials.gov/show/NCT00439777 [Accessed 2011 Jul 1]
Acknowledgements
This analysis was supported by Bayer HealthCare, who held the data from the original studies and performed the analyses. Wolfgang Mueck, Anthonie Lensing and Frank Misselwitz are employees of Bayer HealthCare. Both Wolfgang Mueck and Frank Misselwitz own limited stock in Bayer AG. Hervé Decousus is a member of the study management and coordination committee for the EINSTEIN Study Programme and has received grants from Bayer HealthCare. Giancarlo Agnelli and Paolo Prandoni have no conflicts of interest to declare.
The authors would like to thank Dagmar Klein, Ulrike Krueger and Matthias Frede for their excellent technical assistance, and to acknowledge Shahid Salaria, who provided editorial assistance with funding from Bayer HealthCare and Johnson & Johnson Pharmaceutical Research & Development, LLC.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Mueck, W., Lensing, A.W.A., Agnelli, G. et al. Rivaroxaban. Clin Pharmacokinet 50, 675–686 (2011). https://doi.org/10.2165/11595320-000000000-00000
Published:
Issue Date:
DOI: https://doi.org/10.2165/11595320-000000000-00000