
Abstract
Genomic-based methodologies are increasingly used at all stages of drug development. The most extensive applications have occurred in early drug discovery stages due to advances in technologies that allow for automated synthesis and characterization of organic compounds, and for high-throughput screening of these molecules against known drug targets. The adaptation of genomic-based methodologies in later stages of drug development presents a more difficult task.
In this review we describe how genomics can be used to identify previously uncharacterized pharmacologic actions that provide a basis for the development of new classes of antimycotic agents or for adverse event aversion. Clinically, novel antimycotics are gravely needed. This review provides a perspective on new technologies that will bridge the gap between drug discovery and development that may enable more rapid access to new antimycotic agents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Advances in genomics and the sequencing of organisms’ genomes (human, yeast, and molds) have spawned the subspecialty fields of pharmacogenomics and toxicogenomics. From a pharmacological perspective, these subspecialties provide useful principles for solving a multitude of hypotheses in antifungal drug discovery and therapeutics, along with providing structure and defined tools for assessing genomic or genetic outcomes associated with eukaryote exposure to pharmaceuticals.
Ribonucleic acids obtained from eukaryotic cells (host/pathogens) exposed to pharmaceuticals, referred to as a ‘eukaryotic transcriptome’, can provide insight into biochemical processes associated with pharmaceutical efficacy or toxicity. Our purpose is to review the state of the art and science related to transcriptome screening in the discovery of new antifungals for human pathogens.
1. Antimycotic Pharmacotherapy
Pharmacotherapy of mycotic infections is plagued by a lack of new drug development and diminishing therapeutic responses. Large pharmaceutical companies are abandoning anti-infective discovery and development; Bristol-Myers Squibb, Lilly, and Wyeth discontinued all anti-infective discovery in 2003, while GlaxoSmithKline, Abbott, and Aventis are in the process of downsizing their programs. Only a handful of companies (e.g. Astella Pharma US, Inc. [formally Fujisawa Healthcare], Pfizer, and Diversa Corporation) are continuing antimycotic drug discovery.
The prevailing opinions on drug discovery and development suggest that in order to get one marketed product, a company must start with 25 candidate agents and dedicate 9 years of research. Most candidates are lost due to chemical instability, animal toxicity, poor human pharmacokinetics, poor human tolerance, and unacceptable formulation characteristics of the product. The average industry cost for this scenario was $US600 million in 2004. In one economic model, increasing the yield of marketed agents from the current 5% of candidate agents to 10% or 20% could decrease development cost to $US300 or $US100 million, respectively.[1]
The decreases in antimicrobial development would not be as profound if it were not for the limited number of therapeutic options. Our current armamentarium against disseminated fungal infections involves only four unique drug classes: the polyenes (amphotericin B), azoles (ketoconazole, fluconazole, itraconazole, and voriconazole), echinocandins (caspofungin and micafungin), flourocytosine, and allylamines (terbinafine). Since allylamines inhibit the same pathway as the azole antifungals, allylamines do not provide a unique therapeutic tool.[2] The need for additional ’novel compounds’ or creative means to utilize our current agents is illustrated by the poor clinical outcomes in patients.
Prior to these developmental cutbacks, antifungal therapies were already associated with suboptimal responses. High mortality is common with Candida albicansblood infections (∼42% attributable mortality) and invasive Aspergillus fumagatus(∼85% attributable) diagnosed in immunocompetent individuals. These already high rates of mortality are increasing yearly.[3] Yeast Candidaand Cryptococcusresistance to the mainstay medications (polyenes, echinocandins, and azoles) has now been identified. Yeast (C. albicansappear to have acquired resistance mechanisms that involve changing biochemical pathways associated with manufacturing essential cell structure proteins and altering receptor sites.[4] In addition, resistance has been identified in one of our newest antimycotic agents, caspofungin, less than 1 year after its approval for disseminated fungal infections.[5] Finally, suboptimal responses are complimented by the inability of the medications to discriminate eukaryotic host from eukaryotic pathogen, leading to toxicity in patients.
2. Drug Discovery: Novel Products with Antimycotic Activity
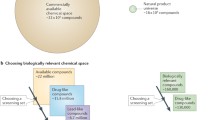
There are essentially two approaches that can be taken to identify new compounds with direct antifungal activity: (a) undirected screening, evaluating libraries of synthetic and natural products for either whole cell inhibitory activity or activity against a specific molecular target; or (b) directed screening, identifying the biochemical processes of the pathogen, and designing synthetic compounds that specifically and selectively interact with a target. Recent development of synthetic antifungal drugs has centered on the synthesis of new analogs of the existing synthetic azole and echinocandin antifungal agents. Limited resources have been directed toward denovodesign and synthesis of novel compounds using the known molecular targets of the opportunistic fungal pathogens. Thus, the discovery of novel antifungal lead compounds that can be used as probes for new molecular targets should facilitate rational drug design efforts in the future.
Natural products provide a rich source of novel prototypes, particularly as previously unexplored biosphere niches are investigated, new molecular targets are discovered, more sensitive and robust assay methods are developed, and technological advances in de-replication, isolation, and structure elucidation are achieved. A number of natural antifungal products with diverse structures have been isolated in recent years from plants, microbes, and marine sources (see table I and figure 1). The biological diversity displayed in the natural world reflects a rich underlying chemical diversity and a vast source of novel structures with biological activities such as chemical defense. These natural products have been used directly as drugs, or have provided leads for the synthetic preparation of pharmaceutical products. Secondary metabolites of compounds isolated from natural sources, predominantly plants,[6] microorganisms, insects, animals and, more recently, from aquatic and marine organisms[7,8] have provided many of the therapeutic agents currently on the market. Approximately 60% of those compounds commercially available or in the late stages of clinical trials for the treatment of infectious diseases or cancer are of natural product origin.[9,10]

Sample antifungal natural products/analogs with unknown mechanisms of actiona

Structures of sample antifungal natural products/analogs. These lead compounds were isolated at the National Center for Natural Products Research and Department of Pharmacognosy, University of Mississippi. The mechanisms of action of these products are still under investigation. See table I for further information.
Amphotericin B, derived from an actinomycete, has been a mainstay of systemic antifungal therapy and remains the most broadly efficacious agent for serious infections, in spite of its considerable toxicity. A selected listing of microbially derived antifungal agents in early pharmaceutical development classifies these compounds into three putative ‘mode-of-action’ classes: those that inhibit cell wall synthesis (e.g. the phellinsin and pradimicin/benanomycin class), sphingolipid synthesis (e.g. sphingofungins, australifungins, and aureobasidins), or protein synthesis (e.g. sordarins).[11]
New targets and prototype agents have the most pivotal role in the future of drug discovery. This is particularly true for the discovery of drugs used in infectious diseases and cancer, where the development of resistance is a significant problem. Antifungal compounds appear to be widely distributed, not only in higher plants[12,13] but are also produced by many microbes. New antifungal leads have been discovered from these sources in the past decade. Some of these are being developed as new drug candidates, while others have provided useful new insights into the cellular and molecular processes of fungal pathogens.
For example, among the most important antifungal compounds to be discovered through the screening of pathogenic yeast are the lipopeptides, echinocandins, and pneumocandins.[14,15] The prototype lipopeptide antifungal antibiotic echinocandin B was isolated from a soil micro-organism and ultimately found to inhibit (1,3)β-D-glucan synthase from C. albicans.[16]}The discovery of the echinocandins as novel prototype antifungal antibiotics, followed by the determination of their mechanism of action, led to a new class of antifungals and the recognition of (1,3)β-D-glucan synthase as a potential molecular target for the discovery and development of other novel antifungal antibiotics.
Other recent reports have identified novel classes of natural products with antifungal activity. The alkylcitrates citrafungin A and B were discovered by Merck scientists[17] to be inhibitors of geranylgeranyltransferase. Laakso et al.[18] reported the isolation of two azaphilones with potent antifungal activity from a Penicillium species. These agents appear to act by inhibiting the fungal fatty acid synthase. Japanese investigators have also reported antifungal metabolites of the fischerin and fusapyrone classes from the Phomaspecies of fungi.[19] Finally, the National Center for Natural Product Development reported the antifungal activity of hypocrellins A and B, photoreactive pigments isolated from the fungal genus Hypocrella in China.[20]
Plant-derived compounds include chalcones,[21] flavonoids,[22] alkaloids,[23–25] napthopyrones,[26] steroidal glycosides,[27] and sesquiterpenoids.[28] Many of these compounds are fungicidal and appear to act by novel mechanisms. They have been the subject of extensive investigations, these include the sampangines,[29–32] eupolauridines,[33–35] and pseudolaric acid B (see table I).[36]
The availability of antifungal agents with novel chemistry, reasonable selectivity for fungi, and unknown mechanisms of action, affords a set of valuable tools that can be used as probes for identifying new antifungal target pathways. To illustrate the feasibility of this approach, several specific examples can be cited where natural products have been successfully used in this fashion.
Investigators have exploited the glucan synthase pathway to identify acidic terpenoids as potent inhibitors.[37] The natural immunosuppressant product tacrolimus (FK506) was used to demonstrate Candidadependence on calcineurin B during membrane stress by azoles,[38] suggesting the viability of this enzyme as an antifungal target. There are also cited examples of antineoplastic agents,[39] mostly natural products, that demonstrate antifungal activity. But more importantly, these compounds are useful as probes of potential new target pathways in Saccharomycesand, conversely, the yeast could be used to gain insights into target and the ‘off-target’ effects of the drugs.
2.1 Genomic Screening Methods
Identification of novel natural products with antifungal activity typically begins with a screening system that can identify compounds with selective and fungicidal effects on the pathogen. Typically, a tier of assays may be established, beginning with a primary assay that has a relatively high throughput capacity, and is designed to detect samples with the most promise for yielding interesting compounds. This process screens out the vast majority of samples with low to moderate activity or with nonselective activity. Prior to major advances in molecular biology and genomics, most assays for the discovery of new antibiotics were based on identifying compounds that inhibited the growth of the target pathogens. This remains an important component in many natural product-based programs, because of the desire to identify leads that provide novel chemistry, novel mechanisms of action, or both. In this way, agents acting by a novel mechanism are less likely to be missed in the primary screening. Secondary assays (pharmacogenomic, toxicogenomic) are usually designed to corroborate and quantitate the activity observed in the primary assay, to establish the spectrum of activity, or to provide insight into the mode of action.
An important criterion for determining the relative importance of a lead compound is evidence to suggest it acts by a novel mechanism of action. For antifungal agents, this may be accomplished initially by relatively simple methods such as determining if the compound is active against strains resistant to other known agents, if the compound inhibits known antifungal targets (e.g. ergosterol biosynthesis), or how it effects unique biochemical pathways (e.g. protein or nucleic acid synthesis). Results that suggest a novel mechanism of action are followed up with more extensive studies to determine the molecular site of action. Additional studies determining where the compound is localized subcellularly, which usually requires the availability of labeled compound, and comparative protein analysis of treated versus untreated cells may also be useful.
Once novel antifungal compounds have been identified, characterization of their activity profiles and mechanisms of action is planned. Precise estimation of their minimum growth inhibitory and fungicidal concentrations provide quantitative comparators versus other antifungal agents. Mode of action studies (versus mechanism of action studies in which an isolated target is assayed) can suggest the general biological process perturbed by an antifungal agent and whether that action is fungicidal or fungistatic. It may also be of interest to assess whether the novel agent acts via known mechanisms for existing classes of antifungals. The pharmacogenomic screening of yeast is an innovative directed screening method for testing or predicting mechanisms of action and toxicity.
2.1.1 Candidate Gene Approach
In converse to traditional pharmaceutical screening, a research strategy using the candidate gene approach to medication discovery identifies uniquely transcribed genes in pathogens and host. Transcriptional changes in pathogens associated with altered susceptibility or resistance may relate to changes in biochemical processes that can be used as screening targets for new drugs. Optimal targets in the host are gene transcripts directly associated with serious diseases (disseminated mycoses), outcomes, or medication responses (adverse reactions).
The candidate gene approach has been expanded to include the identification of single nucleotide polymorphism (SNP) marker sets associated with specific disease processes. GlaxoSmithKline was one of the first to develop a collaboration with three biotechnology companies to expedite this process.[39] In April 1999, the Wellcome Trust and ten pharmaceutical companies formed a nonprofit foundation, the SNP Consortium Ltd,[40] to contract with academic sequencing laboratories to identify/map up to 300 000 SNPs. A total of 1.5 million SNPs were ultimately discovered. The goal was to use genetic profiling to target effective medicines to specific responder patients and avoid treating patients who may carry genetic risk factors for adverse events.[41] However, the pharmacological effects will vary in each patient according to their specific ‘susceptibility’ gene signature or SNP profile associated with either a desired or adverse therapeutic response. Given the complexity of these methodologies and the volume of quantitative endpoints, new bioinformatic tools are being developed to aid in the identification of candidate SNPs associated with disease. These bioinformatic s tools should be freely accessible to the research community in order to spur the rapid integration of these platforms into clinical drug development.
2.1.2 Transcriptome Profiling
Use of gene expression profiling for candidate/gene identification, also called transcriptome profiling, is still in its infancy with regards to antifungal drug discovery. Transcriptome profiling has been the basis for drug discovery research, most notably at companies like Johnson & Johnson or at smaller companies (e.g. Millennium Pharmaceuticals) working in conjunction with a larger pharmaceutical company (e.g. Pfizer Pharmaceuticals). Using transcribed genes provides assurance that the gene activity change is associated with the disease process or adverse event. Unfortunately, many of the business relationships in this arena have not been successful secondary to the difficulties of finding pharmacological agents that target and alter either the expression of the identified transcript or the secondary proteins (biochemical pathways). The discovery process will be advanced by the establishment of a database of human transcriptomes and genetic markers of each disease with elucidation of the associated biochemical pathways.
2.1.3 Data Mining
Investigators use multiple search strategies to mine data from their measured transcriptomes, striving to identify patterns or ‘signatures’ associated with pharmacological effects in pathogens and host. These techniques include visual inspection, cluster analysis,[42] self-organizing maps,[43] class discovery,[44] and support vector machines.[45] The class discovery and support vector machine techniques are supervised and, therefore, dependent on the existence of a set of labeled training data. Currently, there are insufficient published human or yeast pathway (i.e. biochemical) data in human mycology, forcing most investigators to focus instead on unsupervised techniques.
Two promising variations on the clustering theme include hierarchical cluster analysis and self-organizing maps. Eisen et al. [42] employ hierarchical clustering based on the average-linkage method of Sokal and Michener.[46] In this method, a hierarchy of nested sets is constructed by repeatedly selecting the closest pair of genes from all genes (or gene groups) based on a similarity measure. A node in the hierarchy is created to contain an ‘averaged’ gene expression profile (transcriptome) for the two selected genes/gene groups, and the average for the group is used in place of the two individual gene expression profiles. A relationship ’tree’ is generated and the branch length between two gene sets indicates the degree of similarity between the sets. Hierarchical clustering has several shortfalls, however, the leading issue is lack of versatility.[43] As an alternative, self-organizing maps allow the possibility of establishing partial structure on the clusters, improving robustness and accuracy of the method. Both of these methods are being used to identify the pathway and dissect the biochemical processes described below.
2.1.4 Evolving Technologies
Historically, identification of transcriptomes was performed using subtractive hybridizations or differential display reverse transcription-PCR evaluated by polyacryamide gel electrophoresis. These methods were front-end labor intensive, requiring days or weeks to identify and, ultimately, clone a few genes that were uniquely expressed. Subsequent to searching GenBank, one often learned there were only a handful of genes of interest. PCR-based gene disruption methods,[47] alternative dominant selectable marker[48] and related Tet promoter systems[49] have each previously been applied to C. albicansas methods to identify uniquely expressed genes associated with the organism’s behavior or susceptibility.
Innovative genome-wide transcription profiling with complementary DNA (cDNA) or oligonucleotide arrays (e.g. GeneArray™) has now largely replaced these older methods. Using these arrays, one can complete a transcription profile in days, leading to identification of hundreds of genes with significantly altered expression. Review of the microarray technology is outside the scope of this presentation, however, outstanding research using silicon, glass or nylon based platforms for high density human arrays (19 400 cDNA printed) to complete genome arrays (C. albicans and S. cerevisiae)are abundant.[42–45,47,50]
Transcriptome profiling can be utilized to assess the impact of a pharmacological agent on a host, pathogen, or the interaction of a pharmacologic agent in an infected host. Human trial designs are frequently unable to identify explanations for therapeutic failure and mechanism of pharmacological adverse events, especially for antifungal agents. We could assume that our inability to capture and delineate many mechanisms is directly attributed to complex, multifactorial interplay between host responses and external environment influencing a combination with individual variances in pharmacodynamics. Garrod[51] were first to propose that variable responses to pharmacological agents could be attributed to familial components. His observations with a monogenetic disease, alkaptonuria, was the basis of his supposition. The lack of an apparent familial aggregation in patients who develop invasive yeast infection (candidiasis) suggests that the alteration in defense is an acquired or temporary event (alteration in transcriptome) induced by host immunosuppression (trauma, pharmaceutical) leading to a clinically important variation in gene expression. Identification of patient-specific transcriptomes should provide insight into this milieu.
2.2 Application of Genomics in Clinical Drug Development
There is uncertainty in both industry and the regulatory agencies about how the drug approval process should evolve as molecular biological measurements of drug efficacy and toxicity become available. The integration of genomics-based methodologies into clinical drug development is likely to continue lagging behind drug discovery until industry and government adopt a plan that will provide incentives to the private sector yet adhere to historical regulatory behaviors.
To encourage pharmaceutical companies to incorporate pharmacogenomic testing during drug development, the US Food and Drug Administration (FDA) has recently updated regulatory guidance for the industry - the Guidance For Industry: Pharmacogenomic Data Submissions. [52]This guidance provides nonbinding recommendations for voluntary submission of pharmacogenomic data in order to help the FDA gain ‘experience’ as this field evolves. These recommendations do not provide guidance on data obtained from analysis of differential protein expression (proteomic data) or analysis of differential metabolism techniques (metabolomic data).
Previously the scientific community had established a consortium of experts from various European research centers in order to enhance the field of pharmacogenomics. A prime goal was to integrate patient and laboratory genomic data with patient epidemiology (genomic epidemiology).[53] In the US, the National Institutes of Health (NIH) established the Pharmacogenomics Research Network (PGRN) and funded the development of the Pharmacogenetics and Pharmacogenomics Knowledge Base (PharmGKB) in an attempt to enhance development of strategies that identify ‘signatures’ (pharmacogenetic mapping) of specific diseases. PharmGKB specifically focuses on the variation in medication responses related to genetics. Similarly, the need for international collaboration between regulatory agencies results from a general lack of sufficient expertise for reviewing pharmacogenomic information included in new drug applications. For example, in 2003 an agreement for “parallel scientific advice” was signed between the European Medicines Agency (EMEA) and the FDA.
The clinical development of new classes of anti-infectives may, to some extent, be easier than for other therapeutic categories. New antimycotics only need to demonstrate fungicidal activity at concentrations that avoid toxicity in humans. Therefore, pharmacogenomic screening should focus mainly on those genes that (i) control the disposition and level of exposure of these antifungal agents and (ii) determine susceptibility to drug toxicity, especially if homology with yeast genes is the source of the unwanted human toxicity. Drug toxicity is dependent on a three-way interaction between: (i) the host genes that confer susceptibility or risk for adverse effects; (ii) the level of drug exposure; and (iii) the host environment that includes disease, other chemical exposures, and dietary and social factors.
Animal and human testing can reveal those genes that confer susceptibility to toxicity for a ‘lead compound’ at a particular level of exposure, while clinical trials are still required to identify the impact of co-morbidities and specific environments on response to therapy. Technological advances are needed to enable the multiplexing of pharmacogenomic platforms with proteomics or metabolomics so that we can reliably quantitate interspecies relationships between levels of exposure and measures of efficacy and toxicity. Such methods will also allow more precise diagnosis of disease and provide quantitative measures of the effects of pharmacotherapy.[54]
3. Host Genomics
3.1 Genes Influencing Drug Absorption, Distribution, Metabolism, and Elimination
Pharmacogenetics, a term first coined around 1959,[55] has its origin in the key discoveries of the 1950s. More recently, it has been defined as “the study of variability in drug response due to heredity”.[56] Genetically determined enzyme variation havepharmacogenomicsintodrugdeve been identified as a basis for many untoward drug reactions, for example glucose-6-phosphate dehydrogenase deficiency, pseudocholinesterase, and acetyltransferase activity.[51] The seminal twin studies in the 1960s and 1970s extended these observations to include genetic variation in the elimination half-life of many drugs and properly established the field of pharmacogenetics.[57] Today, the broader field of pharmacogenomic s is entrenched in transcriptomes and the elucidation of polymorphisms of the major biological determinants that influence the absorption, disposition, metabolism and elimination (ADME) of antifungals. These determinants include the major phase I drug metabolizing enzymes of the cytochrome P450 (CYP) superfamily, the P-glycoprotein family of major drug transporters belonging to the ATP-binding cassette (ABC) transporter superfamily, and enzymes involved in phase II metabolism.
Deficiencies in the ADME and safety characteristics, and in the potential of new drug candidates for drug-drug interactions, are the major causes for failures during the drug development process. Research efforts focused on the elucidation of the pharmacogenomic basis for variation in ADME characteristics have resulted in the development of several CYP SNP bioarray platforms that are now commercially available for broad-based toxicogenetic screening of CYP1A1/2, CYP1B1, CYP2C9/19, CYP2D6, CYP2E1, and CYP3A4/5allelic polymorphism in clinical trial populations (e.g. CodeLink™ P450 Bioarrays [GE Healthcare] and AmpliChip™ CYP450 Test [Roche Diagnostics]). In addition, gene ‘transcriptome’ arrays are now available for expression profiling of CYP genes, P-glycoprotein family genes, along with phase II metabolism genes such as epoxide hydrolases and acetyl-, sulfo-,methyl-, glutathione-S-glycosyltransferase, and uridine diphosphate (UDP)-glycosyltransferase genes (e.g. GEArray™, Super-Array Bioscience).
Submissions to the FDA must now include preclinical characterization of drug disposition pathways and the identification of major metabolites and their responsible enzymes, as well as preclinical and clinical assessment of toxicity risks for both the parent compound and metabolites. However, the use of current ‘state-of-the-art’ technologies for SNP and RNA expression profiling of drug disposition genes in preclinical and clinical development is still investigational and conducted for internal research purposes only, and as noted in section 2.2, there are no specific FDA requirements at this time.
The establishment of a genetic basis for variability in drug response is most advanced in the area of drug metabolism, and the integration of pharmacogenomic s into drug development is most likely to occur within drug metabolism research first. While the industry and FDA would like to move toward integrating pharmacogenomics into drug development, first they must agree on minimal assessment criteria for establishing the drug interaction potential of novel compounds, since drug interactions cannot be predicted on the basis of variation in metabolism genes alone. Workshops attended by representatives from the European Federation of Pharmaceutical Sciences, the US FDA, and the American Association of Pharmaceutical Sciences have taken place since 1997 to provide guidance on the conduct of in vitroand in vivo investigations of pharmaceutical interactions resulting in abnormal drug metabolism and transport.[58] Recently, a consensus opinion for minimal best practice for in vitroand in vivodrug-drug interaction studies targeted to drug development (not discovery support) was developed that defines a data package that can be expected by regulatory agencies.[59]
3.1.1 Polymorphisms in Cytochrome P450 (CYP) Genes
The identification of ADME genes that determine exposure levels for the current classes of antimycotic agents provides an essential baseline for the development of newer agents that may differ either in structure or in mechanism of action. Depicted in table II are the genetic polymorphisms reported to date for the major CYP subfamilies involved in the metabolism of antimycotic agents, along with the relative importance of each subfamily to the metabolism of most therapeutic agents. Polymorphisms in the CYP subfamilies 2C, 2D, and 3A are likely to have the greatest impact on either the disposition of antimycotic agents or on their potential for drug interactions, since these three subfamilies:

Substrate and inhibitor specificities of the major cytochrome P450 (CYP) subfamilies for current classes of antifungal agents
-
1.
are involved in the metabolism of antimycotic agents or in the metabolism of a large proportion of known drugs;
-
2.
are among the most highly polymorphic of the CYP subfamilies;
-
3.
can be inhibited to variable degrees by antimycotic agents currently available.
As a comprehensive review of the substrate and inhibitor specificities of the approximately 19 CYP isozymes and the genetic variants that are known to participate in the metabolism of drugs is beyond the scope of this review, readers are referred to recent reviews by Donato and Castell[60] and Daly[61] which focus on the genetic diversity of the CYP superfamily. For the purpose of this review, polymorphisms in the CYP2D6 and CYP3A subfamilies are discussed since they predispose antifungal agents to important drug interactions and toxicities.
CYP2D6
A large number of polymorphisms in the CYP2D6gene are highly prevalent in certain populations and can result in >1000-fold variation in phenotypic activity towards some substrates.[62] Since many of the important therapeutic agents used to control heart rate or rhythm are CYP2D6 substrates, the FDA has encouraged the pharmaceutical industry to move away from the development of new drug candidates that are substrates for this CYP isozyme. Appropriately, none of the current antimycotics are CYP2D6 substrates, and new antimycotic agents should be screened as either potential substrates or potential inhibitors of CYP2D6 because of the risk for serious drug interactions with other CYP2D6 substrate drugs.
It is difficult to assess the potential of a new drug candidate for serious drug interactions, since such interactions are dependent on specific combinations of therapeutic agents. Terbinafine, which was introduced into the market in 1996, is an example of how screening strategies and the use of pharmacokinetics analysis can fail to detect potential drug toxicity during drug development. Until recently, terbinafine was thought to have only limited potential for drug-drug interactions because multiple CYPs contribute to its metabolism (table II) and because it is not a CYP2D6 substrate.[63] However, a possible interaction with CYP2D6 substrates was suggested from case reports and from CYP2D6genotype association studies that prompted a re-examination of the potential for drug interactions with terbinafine. Subsequently, terbinafine was found to be a potent inhibitor of CYP2D6 in vitro[64] and in vivoin individuals who were extensive CYP2D6 metabolizers.[65] In 2001 the FDA revised the labeling for terbinafine to reflect post-marketing data on its potential for hepatotoxicity[66] and it is likely that the FDA will re-examine terbinafine’s potential for CYP2D6-dependent drug interactions. It is possible that antifungal agents, including terbinafine, may greatly increase the risk for developing torsade de pointes when coadministered with drugs known to prolong the QT interval.[67] The observation that a proposed molecular structure-based pharmacophore model to predict CYP2D6 inhibition failed to identify terbinafine as a potent CYP2D6 inhibitor, and that the potential for CYP2D6 drug interactions in vivomay be dependent on the CYP2D6genotype of an individual,[64] emphasizes the difficulty in predicting drug interactions in early stages of drug development.
CYP3A
Most of the antimycotics currently available are either substrates or inhibitors of CYP3A isozymes (table II). There is a potential for serious drug-drug interactions since more than 40% of all known drugs are metabolized by CYP3A isozymes.[68] The levels of CYP3A activity in the liver and gut vary greatly in humans primarily because of differences in the relative expression of three CYP3A family members (i.e. CYP3A4, CYP3A5, and CYP3A7), which are co-expressed but independently regulated and share to a large extent similar substrate specificities.
The genetic basis for the wide interindividual variation in our ability to metabolize CYP3A substrates has not been completely established. Polymorphisms in the CYP3A4gene are not likely to contribute significantly to the variability in CYP3A activity since most of the nonsynonymous variants occur at very low frequencies.[69] CYP3A7 is normally expressed in fetal liver; however, low frequency polymorphisms in the promoter region of the CYP3A7 gene may account for the expression of CYP3A7 in some adult livers.[70] In contrast, several recently identified intronic and exonic polymorphisms in the CYP3A5gene, which result in the expression of a truncated protein and loss of activity,[71] are found in high frequency in certain populations such as African Americans. Currently, it is not possible to prospectively identify individuals who might be at risk of toxicities associated with high serum concentrations of drugs that undergo CYP3A-dependent elimination.
3.1.2 Polymorphisms in Hepatic Drug Transporter Genes
The importance of hepatic drug transport processes in the disposition of drugs has only recently been recognized. In this regard, hepatic influx and efflux transport proteins can control drug access to the intracellular phase I and II drug metabolism processes and, therefore, influence the overall bioavailability of drugs to the systemic circulation.[67] The gatekeeper role of hepatic drug transporters, which is depicted in figure 2,[72] results from their location on the basolateral membrane of hepatocytes. During the past decade there has been a surge in research interest on drug transport processes due to efforts to enhance rational drug design. Increased knowledge of the structure-transport relationship would allow better prediction of optimal disposition properties of new drug candidates.

Absorption, distribution, metabolism and excretion (ADME) genes involved in drug disposition. The ADME of drugs is influenced by three major cellular processes: (i) active and passive drug transport processes located on cell surfaces; (ii) phase I processes primarily catalyzed by members of the cytochrome P450 (CYP) superfamily of drug metabolism enzymes; and (iii) phase II processes that involve the conjugation of lipophilic drug molecules or their metabolites to highly polar functional groups that allow their rapid elimination by biliary and urinary routes. These three processes are variably expressed in most tissues (figure depicts those found in hepatocytes) and represent the ‘barriers’ that new antimycotic agents must overcome in order to achieve serum concentrations that are needed for antimycotic activity (reproduced from Chandra and Brouwer,[72] with permission from Springer Science and Business Media). Bi-directional and co-transport processes are indicated by arrows and active transport processes are indicated by solid circles. The SLC22Agene family consists of many organic anion transporter (the OATs) and organic cation transporter (OCTs) family members that are expressed in the liver. The organic anion transporting polypeptides (OATPs) represent a family of proteins that transport both organic anions and cations. ATP= adenosine triphosphate; cAMP= adenosine 3t?,5t?-cyclic monophosphate; ER = endoplasmic reticulum; MDR1= multidrug resistance 1; MRP= multidrug resistance-associated protein; NTCP= sodium/taurocholate cotransporting polypeptide; OA- = organic anions; OC+= organic cations; TC= taurocholate.
The majority of hepatic drug transport proteins belong to either the ‘solute carriers’ superfamily (root gene designation is SLC), or to the ATP-binding cassette superfamily (root gene designation is ABC). The substrate specificity and regulation of the transport proteins depicted in figure 2 has recently been reviewed in detail.[72,73] Although genetic polymorphisms have been noted for several genes in the SLC superfamily, their functional effects have not been established in most instances and few have been shown to result in significant effects on transport kinetics in humans.[74] Similarly, other than specific rare ABCC1, ABCC2, and ABCC6 mutations that are associated with genetic diseases, common genetic variants in the ABC superfamily have not been associated with conclusive physiological significance. Although genetic polymorphism in major hepatic drug transporter genes such as ABCB1(multidrug resistance-1 [MDR1] or P-glycoprotein) do not appear to affect the disposition of drugs to any great extent, it is important to understand that in vivostudies are difficult to interpret because of the hepatic compartmentalization of transport proteins and the difficulty in measuring biliary elimination.
3.1.3 Polymorphisms in Phase II Genes
There is less understanding of the role of genetic polymorphisms in phase II metabolizing enzymes as predictors of drug safety and efficacy in humans since many of these enzymes have very narrow substrate specificities, and the extent of the molecular diversity of each superfamily of phase II enzymes has not been completely characterized. For example, important polymorphisms in the glutathione-S-tranferase (GST) genes GSTM1and GSTT1 have been detected (in 40–50% of individuals from various ethnic backgrounds, and in 20% of Europeans) that result in loss of catalytic activity due to gene deletions.[75,76] However, the limited substrate specificity of GSTM1 and GSTT1 towards drugs (i.e. cytotoxic agents such as carmustine [BCNU] and nitrogen mustard) and environmental toxicants (i.e. dichloromethane), respectively, make it unlikely that these polymorphisms play a significant role in drug metabolism.
Nonsynonymous polymorphisms in other GST gene family members such as GSTM3and GSTP1have been described, but do not appear to have significant effects on activity. A single promoter polymorphism that affects the expression levels of GSTA1 and GSTA2 has been described.[77]
Polymorphisms in the genes encoding two N-acetyltransferase isoforms, NAT1and NAT2, which acetylate amino, hydroxyl, and sulfhydryl moieties, have been extensively characterized.[78] However, the limited substrate specificity of NAT2 (i.e. isoniazid, sulphamethoxazole, and caffeine) and the low frequency of NAT1 polymorphisms suggest that these polymorphisms do not play a significant role in drug outcomes. Similarly, polymorphisms in the thiopurine-S-methytransferase gene TMPT have been extensively characterized with respect to the myelosuppression and toxicity associated with mercaptopurine.[79] However, as with the GST and NAT enzymes, TMPT is associated with a narrow substrate specificity. In contrast, recent studies suggest that polymorphisms in the sulfotransferase (SULT) superfamily have substantial functional significance and are likely to play a role in drug outcomes.[80–82]
Glucuronidation represents an important phase II pathway of metabolism for a variety of hydrophobic drugs and their metabolites, and ranks third behind CYPs and drug transporters as important modifiers of drug disposition. To date, 17 functional UDP-glucuronosyltransferases (UGT) have been identified as members of the UGT gene superfamily.[83] Coding and noncoding polymorphisms have been identified for several UGT genes and, due to the broad and overlapping substrate specificities of UGT isoforms, polymorphism in this gene family are likely to have significant pharmacological consequences. Given the diversity of the UGT superfamily, an assessment of the impact of UGT polymorphisms on drug metabolism and therapeutic outcomes is beyond the scope of this review (but has been discussed with respect to cancer therapeutics elsewhere[84]).
3.1.4 Other Genes that Influence Drug Disposition
The use of cDNA expression systems that provide specific assays for key phase I and II drug metabolism enzymes has provided valuable quantitative structure-activity information for developing predictive computational models to optimize the ADME properties of drug candidates. However, in addition to the phase I and II enzymes that are directly involved in drug metabolism, there are many other genes and proteins that regulate cellular functions and metabolic pathways that can indirectly influence the disposition and exposure of drugs in various organs. For example, the proteins comprising the gap junctions and tight junctions between cells form the barriers and aqueous pores, respectively, which restrict the distribution of hydrophobic and hydrophilic molecules to certain in vivocompartments.
Active- and passive-transporter processes can similarly affect the disposition of drugs without participating directly in their phase I and II metabolism. The genes involved in the metabolic pathways that provide the substrates and cofactors for phase I and II metabolism, such as reduced nicotinamide adenine dinucleotide phosphate (NADPH), glutathione, coenzyme A, etc., are as important as modifier genes that may regulate these pathways or regulate the level of expression of phase I and II enzymes. Therefore, the ability to develop more complex cell-based models that reflect the ‘net’ effects of all tandem processes affecting drug disposition is essential for in vivoprediction.
The development of new molecular tools for immortalizing primary cells will provide novel cellular models that closely reflect the terminal differentiation properties of human tissues. These cellular models will provide key platforms for studying the complex interplay between the processes that influence drug disposition in different tissues and will allow for more accurate prediction of desirable ADME properties for the selection of drug candidates.[85]
3.2 Host Genes that Confer Disease Susceptibility/Drug Toxicity in Mammals
A considerable fraction of the human genome, approximately 5% of all genes, is involved in the immune response.[86] Some of these genes are among the most highly polymorphic of the human genome. An example of this extreme genetic diversity is seen in the major histocompatibility complex (major histocompatibility complex [MHC] or human leukocyte antigen [HLA]) class I and II genes, where up to 500 alleles per locus have been reported.[87] This is probably a result of natural selection for resistance during periodic infection. The role of MHC polymorphism in antimicrobial resistance has recently been extensively reviewed.[88] Circumstantial evidence suggests that this diversity is driven by pathogen exposures, although few MHC associations with infectious diseases have been identified.[89] Importantly, it has been suggested that while pathogen exposure may drive MHC diversity, MHC-associated resistance to infection may also exert a selection pressure on pathogens. Since the generation times of pathogens are considerably shorter than host cells, they can respond relatively quickly to these selection pressures from their host.[90] Both class I and II MHC molecules are involved in the presentation of peptide fragments that are derived from microbial proteins to activate T-cell response against infection. It is reasonable to hypothesize that individuals who differ in a particular combination of MHC alleles may demonstrate different degrees of resistance or immune response to certain pathogens.
For most novel compounds that possess antimycotic activity, any demonstration of pharmacological effects on mammalian physiology could be regarded as toxicity. The exceptions to this rule are antimycotic effects that lead to enhanced activity (e.g. stimulation of immune response against the infectious agent). The prototype of this ‘indirect’ reaction is the immunostimulatory actions of the polyene antifungals. Genomic screening strategies should prove useful in the identification of highly penetrant candidate genes that are markers of, or predispose to, a specific indirect effect or end-organ toxicity. Some polymorphisms might result in toxicities in a large proportion of the population carrying the trait. However, in most instances, these polymorphisms are only carried by a small percentage of the population and, therefore, do not represent frequently identified mechanisms for drug toxicity. A classic example is the increased susceptibilities to ototoxicity caused by certain ribosomal gene traits in patients receiving aminoglycosides.[91]
Interactions between less penetrant ‘susceptibility’ genes and certain environmental factors frquently lead to common drug toxicities. However, these are more difficult to detect with genomic methods during the early stages of drug development. A primary reason for this difficulty is the lack of suitable animal models that reflect the genetic diversity of human populations. Polymorphisms that are associated with alterations in expression or activity of less penetrant genes cause toxicity in susceptible individuals due to drug exposure levels or other host susceptibility factors (disease or concomitant medications). These less penetrant susceptibility genes are often highly prevalent in the population. Unfortunately, related drug toxicities are usually detected only during phase IV post-marketing surveillance. Therefore, such subtle interactions have a profound effect on the health of a population and should concern agencies like the FDA.
Traditionally, toxicology screening strategies utilizing various animal species, including dog and mouse, have assisted companies and the FDA in their interpretation of safety assessments and in their projections of risk for early human efficacy studies. However, such strategies are ultimately inadequate because of their inability to assess the impact of human polymorphisms on potential mechanisms of drug toxicity. The current practice of employing single animal strains for toxicology screening is akin to using a single family to conduct a clinical trial. No single strain-specific genotype is representative of the variance that is present in human populations. In support of this concept, recent analyses have suggested that the individual variation between mouse strains is as great as the variation observed across human populations. The International Mouse Phenome Project coordinated by The Jackson Laboratory (Bar Harbor, Maine, USA) aims to exploit this genetic variation for experimental purposes by constructing a database encompassing the genotype and physiological profile (phenotype) for each major inbred mouse strain.[92] In addition, nearly complete genomic sequences are already available for four of these strains through Celera Genomics and public databases.[93] These databases provide approximately 100 000 SNPs that can be used for modeling genetic variation.
Inclusion of an assessment of genetic variation in toxicological screening of new drug candidates would allow the detection of unique genotype-specific toxicities that would otherwise go undetected until discovered in later stages of drug development or during post-marketing evaluation. To illustrate this last point, it has been suggested that an allylic metabolite may play a causal role in the pathogenesis of the hepatotoxicity associated with terbinafine.[94] This is regarded as a previously undetected toxicity rather than just an idiosyncratic reaction.[94] Genetic variation in metabolism has been hypothesized as the source of increased concentrations of this metabolite in some individuals and increased incidence of this toxicity.
3.2.1 Antifungal Induced Mammalian Toxicity
Many of the reported transcriptomes resulting from exposure of human cells to novel or FDA approved antimycotics have utilized immortal hematopoetic cell lines (monocytic like [THP-1; ATCC TIB 202], histiocytic like [U937; ATCC CRL 1593], and liver epithelial cells [THLE-1; ATCC CRL 11233]). It was recognized very early that antimycotic agents impact host-related transcriptomes as well as those of the pathogen. Polyenes were first reported to downregulate elongation factor 1?, fatty acid synthase, and dynein, while interleukin (IL)-2 receptor and inflammatory cytokines (IL-1β, tumor necrosis factor-?, and prostaglandin E2) were upregulated in response to exposure to amphotericin B formulations.[95] Changes in biochemical enzymes secondary to exposure to other antifungals include histamine metabolism changes by caspofungin, and cyanide metabolism changes by 5-flurocytosine (flucytosine). However, the most exciting has been the discoveries related to changes in receptor density and immune-mediated responses discussed in the subsections below. Several of these discoveries have progressed to clinical trials.
3.2.2 Interleukin -2 Receptor
The discovery that IL-2 receptors were significantly upregulated in response to amphotericin B (lipid and nonlipid formulation) exposure did not lead to the development of a novel antifungal agent. However, these data led investigators to hypothesize a mechanism for drug toxicity. The known pharmacologic toxicities (flu-like symptoms [fever, chills, myalgias], capillary leak syndrome [hypotension, decreased organ perfusion], pulmonary congestion, changes in mental status [lethargy, confusion, agitation], renal dysfunction with secondary hypokalemia, hypomagnesemia, and anemia, and liver dysfunction) associated with the administration of therapeutic doses of IL-2 were similar to those observed with amphotericin B formulations.
Monoclonal antibodies targeting the IL-2 receptor (basiliximab and daclizumab) interfere with IL-2 activity by blocking the IL-2 receptor (CD25). The humanized antibody daclizumab is commercially marketed and FDA approved for the treatment of transplant rejection in renal transplant recipients. Unfortunately, the humanized antibody would not be effective in murine models and, therefore, human phase II clinical trials were initiated with daclizumab in 2002 without preclinical animal studies.[96] Preliminary data on renal dysfunction and secondary infections support the safety of administering an IL-2 receptor antagonist in a patient with a mycotic infection. Roche Pharmaceuticals and the FDA are currently reviewing these data and considering a request for a phase III clinical trial assessing the efficacy of an IL-2 receptor antagonist, as a single prophylactic dose, in the prevention of amphotericin B-associated adverse reactions.
3.2.3 Hdistamine Metabolism
Transcriptome signatures representing known or suspected histamine-related toxicities have been identified through the exposure of human cell lines to caspofungin, azoles, amphotericin B formulations, and flucytosine. Critical enzymes in the biochemical pathway associated with histamine metabolism were downregulated in monocytic (THP-1) and histiocytic (U937) cells or mast cells exposed to caspofungin. At antifungal concentrations achieved during therapy, the predominant histamine degradation enzyme, histamine N-methyltransferase (HNMT), was downregulated within minutes of caspofungin exposure and remained depressed for up to 24 hours. In addition, a minor enzyme, monoamine (diamine) oxidase A (MAOA), was also transcriptionally impacted. Interestingly, amphotericin B formulations upregulated HNMT in the same model.[97] Studies of enzyme activity (HNMT) in an in vitromast cell or an ex vivohematogenous cell model demonstrated that HNMT activity is attenuated minutes after exposure to caspofungin. At 1 hour, caspofungin induced a 33% decrease in HNMT activity, in a dose-dependent manner, compared with media alone. The relative decrease in activity for caspofungin was maintained for the entire 24 hours. An in vitro affect on histamine could also be detected, with peak concentrations measured at 2 hours after exposure to caspofungin (19.7 ± 0.9 ng/mL) compared with unexposed cells (14.7 ± 1.7 ng/mL).[97]
Clinical trials demonstrated that histamine release reactions occur in <10% of caspofungin-treated patients.[98] Anecdotal experience suggests that these reactions are infusion rate (dose) dependent. It is intuitive to conclude that certain populations may exhibit a phenotypic underexpression of HNMT, leading to a pronounced effect when caspofungin is administered. It is not clear if the attenuation of HNMT expression is a class affect for echinocandins (i.e. includes anidulafungin and micafungin).
3.2.4 Cyanide Metabolism
Identification of potential drug interactions or toxicologic effects using pharmacogenomics could become a powerful screening tool for the clinical pharmacologist. One report of drug interaction ‘signatures’ was identified from the screens of novel and FDA approved antifungal agents.[99] Transcription of rhodanese (thiosulfate sulfurtransferase; TST, which is involved in cyanide detoxification, in an in vitrohuman cell line was significantly decreased in response to flucytosine, increased >2 fold in response to amphotericin B, potassium iodide, aframodial (pseudolauric acid B), pentagonia, sam-allyloxime B, and eupoloridine, and was unchanged in response to caspofungin and the azoles.
In biochemical validation assays, thiocyanate, a less toxic metabolite of cyanide metabolism produced by the action of rhodanese, was markedly decreased with increasing flucytosine concentrations. At a flucytosine concentration of 200 μg/mL, there was no measurable conversion of nitroprusside-associated cyanide to thiocyanate. At concentrations achieved during therapy, amphotericin B was associated with increased thiocyanate concentrations. Caspofungin did not affect cyanide metabolism. These studies have biochemically validated the pharmacogenomic signature suggesting altered rhodanese activity in response to at least one antimycotic agent.[99] Further clinical investigations are needed to elucidate if alternate, cyanide metabolic pathways prevent human toxicity. Until clarified, the combination of nitroprusside or natural sources of cyanide (i.e. smoking) and flucytosine should be used with caution.
4. Pathogen Genomics
The Fungal Genome Initiative at the Massachusetts Institute of Technology (MIT) Center for Genome Research was developed to sequence and annotate key human and agriculture fungal organisms.[100] Thus far, C. albicans(diploid: Strain WO-1), C. tropicalis (diploid), C. guilliermondii(haploid), and C. lusitaniae(diploid) have been sequenced. A database[101] of the most current annotation of the C. albicans genome is maintained with the support of the Wellcome Trust, National Research Council (NRC) Genome-Health Initiative, Burroughs Wellcome Fund and Pfizer (Pharmacia) Corporation. Assembly 6, performed by the Galar Fungal Consortium and Stanford Genome Technology Center, utilized the C. albicans SC5314 genome.[102] Unfortunately, the majority of gene functions are not reported in this annotation.
The sequenced C. albicans genome contains ∼15.5Mb, an estimated 6200 individual genes predicted to encode proteins of at least 100 amino acids or larger. Complete annotation of the genome, currently 7680 open reading frames (ORFs), should be complete within the year and provide a foundation from which systematic functional genomic strategies may be based. In addition, C. parapsilosis has had a genomic library sequenced containing approximately 2500 genes (33% of the genes for the 26Mb diploid genome).
Novel methodologies for screening yeast expression patterns include gene insertion with regulated expression or genome-wide transcription profiling. One noteworthy functional genomics approach, termed GRACE™ (gene replacement and conditional expression), involves the mutation of yeast by deleting one allele of a gene and leaving the remaining allele under a tightly regulatable tetracycline promoter.[103] Using this method, Roemer et al.[103] generated 1152 mutants and determined that nearly 49% (567) of the genes tested were essential for growth. Of these, 33 were absent from both Saccharomyces cerevisiae and human genomes, suggesting Candida-specific candidate genes that could be targeted. The investigators suggested that their mutants could be used to prioritize sites of action as potential antifungal drug targets. Specifically, the selection of genes essential for yeast survival which do not have human homology would make a good pathogen target that may not be toxic to the host. Transcriptome screening should allow for the analysis of expressed genes (assuming all essential genes are expressed), especially those associated with drug therapy that could lead to resistance.
4.1 Genes Conferring Pathogen Susceptibility/ Pathogenicity in Yeast
Pharmacogenomic screening of pathogenic yeast exposed to an antifungal agent permits identification of transcriptomes related to the antifungal killing and pathogen defense mechanisms. S.cerevisiae has been the ‘organism’ of choice for in vitro susceptibility, animal infection models and genomic studies, due to the preponderance of published data. Screening S.cerevisiae transcriptomes has been used as a technique to identify mechanisms of drug action, however, due to the relative lack of pathogenicity and limited drug resistance, this model is less than ideal.[50] In addition, the ability to extrapolate observations in S.cerevisiae to common clinical pathogens (C. albicans or Histoplasma capsulatum) appears limited. Bender et al.[104] observed significant (∼5%) and rapid (≺2 hours) transcriptome changes in Candida in response to phagocytosis. These changes were not observed in S. cerevisiae, suggesting that Candida has the ability to recognize innate human immunity and protect itself. These authors identified a Candida genomic ‘signature’ specifically associated with contact with the human immune system.
Genomics studies in S.cerevisiae have identified a complete set of genes essential for survival by systematic deletion of functional genes.[105] These ‘essential’ genes define a novel group of antifungal targets. Laboratory-induced lethal phenotypes, associated with deletion of essential genes, should mimic the pharmacologic effects of a drug-induced gene inactivation or poisoning of a biochemical pathway. Transcriptome studies and gene deletion analysis will hopefully lead to discoveries of novel lead compounds.
Transcriptome analysis of C. albicans has been the focus of recent yeast trials; however, Histoplasma and Aspergillus species have also been tested. Traditional biochemical screens of C. albicans and other pathogenic yeast used in antifungal drug discovery have been restricted to a select set of validated targets. An advantageous target characteristic would be a transcript for a protein that lacked human homology. A limited number of yeast genes with this characteristic have been identified and published, including MDR1,EFT2 (elongation factor 2), ERG11 (ergosterol biosynthesis-11), ERG1 (ergosterol biosynthesis-1), FKS1 (FK506 sensitivity), CDR1Candida drug resistance-1), and CDR2Candida drug resistance-2).[106–109] An orthological relationship between MDR1in yeast and ABCB1 in humans has been identified recently, and follow-up evaluation of any MDR1 inhibitor will be required. Overexpression of drug efflux pumps (CDR, CDR2, and MDR1, the azole target gene (ERG11),or mutational alteration of ERG11 is most commonly associated with antimycotic resistance.
Some yeast genes with complimentary biochemical pathways in humans have been successfully targeted by the current antifungal drugs. These include PDR16 (phosphatidylinositol transfer protein; increased expression of PDR16 has been observed during azole resistance),[106] REP2 (regulator of efflux pump),[107] NOT5(CCR4-NOT transcription complex, subunit 5 [CNOT5]-required for morphogenesis), IPF8663 (insulin promoter factor, homeodomain transcription factor-required for morphogenesis), LPD1(virulance factor-dihydrolipoamide dehydrogenase), and IPF15632 (insulin promoter factor, homeodomain transcription factor-cell integrity).[108,109] EPA6 and EPA6P (erythroid-potentiating activity-tissue inhibitor of metalloproteinases) have been associated with biofilm formation.[110] CKA2 (protein kinase CK2α subunit), a gene specific to the catalytic subunit of the protein kinase CK2, is a negative feedback protein on CDR1 expression, and downregulation has been measured in antifungal-resistant yeasts.[111]
Transcriptome analysis has revealed an association of EFG1and EFH1 with hyphal development.[112] Hyphal development can be essential for host tissue invasion. If these altered transcripts can be utilized as pharmacologic targets for novel antifungals, there is potential to attenuate the pathogenicity of the Candida or to kill the organism. Another essential process in pathogenicity appears to be biofilm formation. This ‘slime’ appears to be the result of the interaction of a spectrum of proteins. C. albicans strains (GDH12346 and SC5314) exposed for 6, 12, and 24 hours to human dental surfaces and venous access devices, revealed variable gene expression dependent on the species and dental or catheter surface used. Although specific signatures were associated with the length of incubation time, variation in surface exposure and yeast strain make interpretation difficult.[113] EPA6 and EPA6Pwere implicated in slime production in this trial.
The use of resistant C. albicans has been instrumental in finding promising drug targets. A standard methodology has been used, where both azole-susceptible and -resistant C. albicans are grown in secreted aspartyl-proteinase inducing media. In these in vitro trials, yeast is exposed to antifungals that inhibit growth to 40–80% of control yeast. Expression of Candida genes from susceptible and resistant yeast is compared in this model in order to isolate essential gene transcripts. Researchers aspire to identify gene transcripts associated not only with putative virulence mechanisms for yeast resistance to given antifungals, but also transcripts related to unrecognized resistance mechanisms. Differential display experiments have been performed in vitro comparing azole-susceptible versus azole-resistant Candida species in response to antimycotics (amphotericin B, caspofugin, flucytosine, fluconazole, and itraconazole) at concentrations achievable during human therapy but which are sublethal to yeast.[114
Confirmatory reports of known upregulated transcripts associated with the development of resistance (ERG2,CDR1,and CDR2) have been reported in matched sets of organisms that were initially susceptible, yet acquired resistance during human therapy.[5,10,115–117] ERG2 transcribes a protein of ergosterol biosynthesis in which mutations can lead to altered antifungal susceptibility, and CDR gene transcripts are multidrug transporters that are overexpressed in azole-resistant yeast. In addition, some identified transcripts are suspected of having a role in resistance pathways, including RTA1 (resistance to aminocholesterol; conferring strong and specific resistance to 7-aminocholesterol) and YHB1 (yeast flavohemoglobin gene).[118] S. cerevisiae contains a gene (RTA1p, similar to RTA1 of Candida) that is upregulated during resistance associated with exposure to 7-aminocholesterol. YHB1 appears necessary for virulence by encoding a nitric oxide dioxygenase that scavenges and detoxifies nitric oxide. Some studies identified altered expression of putative virulence transcripts, including FRP1-3 (ferric reductase gene) and GPX1 (glutathione peroxidase 1). [114] However, many of the novel transcripts identified during these early unpublished trials are not available in the most recent annotations of the Candida genome. Validation of these observations and peer review will be required.
An N-myristoyl transferase inhibitor was pursued as an antifungal agent directed against C. albicans N-myristoyl transferase activity. The gene transcript for N-myristoyl transferase (NMT) has low homology with known human genes. However, the product was discontinued after the identification of resistant Candidamutants following limited product exposure.[119]
Inhibitors of yeast FAS1 (fatty acid synthase) represent another class of agent being evaluated as a candidate drugs. FAS1 translates to an integral membrane enzyme involved in fatty acid synthesis that is essential for yeast survival. Cerulenin and tetracycline shut down fatty acid synthesis at concentrations that are tolerated in humans. These agents probably work by affecting the yeast FAS 1 enzyme. Further work is underway evaluating the role of these and many proprietary compounds as novel or ‘lead’ antifungals.
5. Dynamic Models of Yeast Infection
Translational research relating in vitro and in vivo observations are a desirable goal in combating fungal infections in humans. Independent observations exists on SNPs, gene expression profiles, pharmacologic, and toxicologic data in multiple frameworks (human, animal, in vitro).However, in order to relate this information to outcomes in humans, specific molecular biological information corroborated with clinical observations is required. Large scale clinical (patient care) trials incorporating these molecular biologic tools will partially address this problem. Databases that compile smaller controlled and uncontrolled observations will also be beneficial. Such databases are now being compiled, for example the National Institute of Environmental Health Sciences (NIEHS) initiative for acetaminophen hepatotoxicity.[120] In addition, clinically correlated in vitro models testing variables, some unethical to evaluate in humans, should be effective in resolving why yeast respond poorly to therapy and survive intracellularly.
Ultimately proteomics and metabolomics may provide useful data for predicting antifungal drug toxicity. In humans, protein diversity results from alternative splicing of RNA. The relative number of proteins (∼60 000–70 000) compared with gene transcripts (∼30 000) and redundancy in protein activities make comparison more difficult. The multiplexing methods in development will link these various informatic (gene, protein, etc.) platforms together (e.g. Gene to Cell to System™, Icoria, Inc., Research Triangle Park, NC, USA) for determining associations of these changes with specific SNP profiles in humans.
One key to the development of novel antifungals will be to understand how yeast survives in the host, even when treated with antifungal therapy that resolves acute signs and symptoms. The current antifungals, like the antituberculosis drugs, do not always eradicate the pathogen, leaving no other option but to administer life-long maintenance therapy. Evaluation of the human and yeast transcriptomes during infection appear optimal for identifying biochemical processes that are activated by yeast or missing in the host, allowing yeast survival. Isolation of enough invading (cell adhered or phagocitized) yeast from an infected patient for pharmacogenomic studies has been thus far unsuccessful. In vitrostudies will most likely be required to fully understand alterations in yeast behavior and host response.
Clinical (nv ivo or ex vivo) investigations of transcriptomes reflecting the impact of yeast on mammalian physiology are limited. Studies of transcriptomes from patients infected with C. albicans have reported several unique transcripts presumably associated with the dynamics of infection and its treatment.[121–125] In one clinical trial, investigators included any consenting patient with a positive blood culture for yeast unless there was a contraindication to phlebotomy (hematocrit <20%, severe hypotension).[122,123] Venous blood was collected on four separate days, the day yeast cultures were positive, prior to therapy (T1), day 2 of therapy (T2), the end of therapy (T3), and 2 weeks post-therapy (T4). Each time a blood samples was taken, a transcriptome was determined. By comparison with the final sample (T4, host baseline) the investigators represented the impact of Candida on the host (T1 vs T4), the dynamic of drug and infection (T2 vs T4), and the impact of drug on the host (T3 vs T4). These patients with disseminated candidiasis were treated with a broad range of antifungals.[121,122] During infection (T1), the host cellular defenses appeared enhanced based on significant increases in colony stimulating factors and receptors, chemo-attractants (i.e. IL-16), and adhesion molecules in addition to several T-cell receptors (table III).[123]

Gene transcripts altered in yeast infection and its treatment
In the clinical trial,[123] antifungals did not affect expression of the previously reported, pathogen associated downregulated receptors,[122–127,130,131] interferon-related proteins,[122,128] or ATPase-dependent transporting activity and cytokines.[122] Several previously reported regulatory pathways in infected mammals showed increased expression associated with antifungal therapy, including signal recognition particles, most specifically, the endocyte receptors (MRC2,SRPR), sterol isomerase, vesicle-associated kinases, and lymphocyte function-associated antigens (CD58).[122] Expression of TLR4 was higher in the dynamic of treated infection than for infected patients prior to treatment. Of note, several transcripts reported from animal studies were unaffected in the human clinical trials (table III).[122–132,134,135] These transcriptional changes could represent a combined affect of host response to an invading pathogen and antifungal treatment, or a specific reaction to the antifungal alone. Antifungal-specific changes (those occurring at end-of-therapy) included multiple altered transcripts. Universally altered transcripts included the downregulation of apoptosis related genes (e.g. API5 [apoptosis inhibitor 5]). Increased transcription of immune activators (i.e. C6 [complement component 6], UBD [ubiquitin D], LIF [leukemia inhibitory factor]) and immune-related receptors (i.e. TLR4 [toll-like receptor 4], AP4S1 [adapter-related protein complex 4 sigma 1 subunit], SSR3 [signal sequence receptor, γ/translocon-associated protein γ], CDH3 [cadherin 3, type 1/P-cadherin, placental], and PFP4 [perforin 4/ pore forming protein]) and enzymes such as citrate synthase (CS) and mannosidase (MAN2A2) were also observed regardless of the agent used.[123] These altered transcripts may represent the effects of antifungal treatment or the residual effects of a serious infection. Further investigation using an in vitro pharmacogenetic/ genomic model will be necessary to elucidate these observations
6. Challenges, Strategies, and Virtual Phenotypes
Traditionally, the FDA has required extensive toxicokinetic studies in multiple species to obtain interspecies comparisons on drug safety. The need to evaluate multiple species to determine exposure/safety information for novel compounds reflects the long recognized problem that no one animal species exhibits the genetic diversity that is encountered in human populations. The absence of genetic diversity in animal models, used for analyzing interactions between genetic polymorphisms and the environment that affect drug disposition and susceptibility to drug toxicity, makes it difficult to develop predictive statistical models on drug safety in humans. Recently the Complex Trait Consortium (CTC) has proposed the development of a new resource called the Collaborative Cross,[136] which will encompass the development of a large panel of recombinant inbred (RI) mouse strains from a set of genetically diverse inbred founder strains. The Collaborative Cross will require approximately 1000 RI strains to achieve 135 000 recombination events and retain segregating polymorphisms every 100–200 bp, and the CTC estimates that this level of genetic diversity will be sufficient to observe phenotypic variation in almost any quantitative trait of interest.[136]
Construction of statistical models or ‘virtual phenotypes’ to select novel compounds with desirable properties will require an assessment of the effects of polymorphism for genes involved in drug disposition and toxicity. While the use of RI mouse strains represents one approach for the assessment of genetic diversity, such information may also be derived from the huge, untapped database on drug exposures and toxicities found in the investigational phase I/II safety studies that are on file with the FDA. In this regard, the NIH has launched its Molecular Libraries Roadmap initiative that aims to assimilate these data for use by both public and private sectors (avaliable at http://nihroadmap.nih.gov/index.asp). The construction of ‘virtual phenotypes’ to predict genetic diversity, safety, and efficacy in humans from data extrapolated from animal models will require the resolution of high quality transcriptomic, proteomic, and metabolomic data with discrete quantitative phenotypic measures of drug disposition and toxicity for every organ system. Therefore, new informatics-based technologies that can translate important qualitative measures of safety and efficacy into discrete quantitative data will be needed.
During the toxicologic evaluation of novel compounds, adverse effects are customarily characterized by histological examination of drug-induced changes in the organization of subcellular organelles, proteins, and cellular products that comprise the specific tissues involved. These drug-induced histological changes reflect changes in RNA and protein expression, and in protein activity and the level of critical intermediary metabolites. Therefore, technologies that can reduce the measurement of such complex interactions down to quantifiable pathologic changes in the affected organ or tissue would also be able to take advantage of the vast amount of histologic information already obtained. Advancements in machine vision technology and computer-linked intelligent image processing systems that can quantitate histologic changes in tissues with high resolution and precision, may allow the objective classification of human diseases through histopathologic imaging.[137–141]
The utility of quantitative histopathologic imaging analysis in drug development will depend on its reproducibility and predictive accuracy in toxicology screening. Because machine vision histopathologic screening allows quantitative comparisons of thousands of tissue samples through differential display, this methodology will enable the reduction of data obtained from various informatics platforms into a format that allows for unsupervised and objective preclinical safety determination.
In the future, genomic-based methodologies in combination with automated quantitative analytical systems will enable the rapid preclinical screening and selection of drugs with potent antimycotic activity and desireable ADME and safety properties. This integrative predictive systems approach will greatly decrease the number of costly failures that are encountered in early clinical development of investigational drugs and will rapidly increase the number of agents available for treatment of mycotic diseases.
References
Shlaes DM, Progan SJ, Edwards JE. Antibiotic discovery: state of the state. Am Soc Microbiol News 2004; 70: 275–81
Andriole VT. Current and future antifungal therapy: new targets for antifungal agents. J Antimicrob Chemother 1999; 44: 151–62
Pfaller M, Wenzel R. Impact of the changing epidemiology of fungal infections in the 1990s. Eur J Clin Microbiol Infect Dis 1992; 11: 287
Lupetti A, Danesi R, Campa M, et al. Molecular basis of resistance to azole antifungals. Trends Mol Med 2002; 8(2): 76–81
Pacetti SA, Gelone SP. Caspofungin acetate for treatment of invasive fungal infections. Ann Pharmacother 2003; 37(1): 90–8
Schultes R, Raffauf R. The healing forest: medicinal and toxic plants of the Northwest Amazonia. Portland (OR): Discorides Press, 1990
Faulkner DJ. Marine natural products. Nat Prod Reps 2001; 18: 1–49
Urban S, Hickford SJH, Blunt JW, et al. Bioactive marine alkaloids. Current Org Chem 2000; 4: 765–807
Newman DJ, Cragg GM, Snader KM. Natural products as sources of new drugs over the period 1981–2002. J Nat Prod 2003; 66: 1022–37
Cragg GM, Newman DJ, Snader KM. Natural products in drug discovery and development. J Nat Prod 1997; 60: 52–60
Vicente MF, Basilio A, Cabello A, et al. Microbial natural products as a source of antifungals. Clin Microbiol Infect 2003; 9: 15
Kinghorn AD, Balandrin MF, editors. Human medicinal agents from plants. ACS Symposium Series 534. Washington, DC: American Chemical Society, 1993: 2–12
Cowan MM. Plant products as antimicrobial agents. Clin Microbiol Rev 1999; 12: 564–82
Graybill JR. The future of antifungal therapy. Clin Infect Dis 1996; 22Suppl. 2: S166–78
Denning DW. Echinocandins and pneumocandins: a new antifungal class with a novel mode of action. J Antimicrob Chemother 1997; 40: 611–4
Sawistowska-Schroder ET, Kerridge D, Perry H. Echinocandin inhibition of 1,3-beta-D-glucan synthase from Candida albicans. FEBS Lett 1984; 173: 134
Singh SB, Zink DL, Doss GA, et al. Citrafungins A and B, two new fungal metabolite inhibitors of GGTase I with antifungal activity. Org Lett 2004; 6: 337–40
Laakso JA, Raulli R, McElhaney-Feser GE, et al. CT2108A and B: new fatty acid synthase inhibitors as antifungal agents. J Nat Prod 2003; 66(8): 1041–6
Shibazaki M, Taniguchi M, Yokoi T, et al. YM-215343, a novel antifungal compound from Phoma sp. QN04621. J Antibiotics (Tokyo) 2004; (6): 379–82
Ma G, Khan SI, Jacob MR, et al. Antimicrobial and antileishmanial activities of hypocrellins A and B. Antimicrob Agents Chemother 2004; 48(11): 4450–2
El Sohly HN, Joshi AS, Nimrod AC, et al. Antifungal chalcones from Maclura tinctoria. Planta Med 2001; 67: 87–9
Li XC, Joshi AS, El Sohly HN, et al. Fatty acid synthase inhibitors from plants: isolation, structure elucidation, and SAR studies. J Nat Prod 2002; 65: 1909–14
Muhammad I, Dunbar DC, Takamatsu S, et al. Antimalarial, cytotoxic and antifungal alkaloids from Duguetia hadrantha. J Nat Prod 2001; 64: 559–62
El Sayed KA, Kelly M, Kara UAK, et al. New manzamine alkaloids with potent activity against infectious disease. J Am Chem Soc 2001; 123: 1804–8
Dunbar DC, Rimoldi JM, Clark AM, et al. Anti-cryptococcal and nitric oxide synthase inhibitory imidazole alkaloids from the calcareous sponge Leucetta cf chagosensis. Tetrahedron 2000; 56: 8795–8
Li XC, Dunbar DC, El Sohly HN, et al. A new naphthopyrone derivative from Cassia quinquangulata and structure revision of quinquangulin and its glycosides. J Nat Prod 2001; 64: 1153–6
Bedir E, Khan IA, Walker LA. Biologically active steroidal glycosides from Tribulus terrestris. Pharmazie 2002; 57: 491–4933
Zhang Z, ElSohly HN, Jacob MR, et al. New sesquiterpenoids from the root of Guatteria multivenia. J Nat Prod 2002; 65: 856–9
Liu S-C, Oguntimein BO, Hufford CD, et al. 3-methoxysampangine, a novel antifungal copyrine akaloid from Cleistopholis patens. Antimicrob Agents Chemother 1990; 34: 529–34
Clark AM. Sampangine and derivatives useful as an antifungal agent. Unversity of MIssissippi. US Patent 5,128,344.1992 July 7
Peterson JR, Zjawiony JK, Liu S-C, et al. Copyrine alkaloids: synthesis, spectroscopic characterization and antifungal/antimycobacterial activity of A- and B-ring functionalized sampangines. J Med Chem 1992; 35: 4069–77
Orabi KY, Li E, Clark AM, et al. Microbial transformation of sampangine. J Nat Prod 1999; 62: 988–92
Khan SI, Nimrod AC, Nitiss JL, et al. Antifungal activity of eupolauridine and its action on DNA topoisomerases. Antimicrob Agents Chemother 2002; 46: 1785–92
Hufford CD, Liu S-C, Clark AM, et al. Anticandidal activity of eupolauridine and onychine, alkaloids from Clesitopholis patens. J Nat Prod 1987; 50: 961
Clark AM. Antimicrobial compound [Eupolauridine] and compositions particularly effective against Candida albicans. US Patient 07/218,986. 1990 Oct
Li E, Clark AM, Hufford CD. Fungal evaluation of pseudolaric acid B, a major constituent of Pseudolarix kaempferi. J Nat Prod 1995; 58: 57–67
Onishi J, Meinz M, Thompson J, et al. Discovery of novel antifungal (1,3)-beta-D-glucan synthase inhibitors. Antimicrob Agents Chemother 2000; 44(2): 368–77
Cruz MC, Goldstein AL, Blankenship JR, et al. Calcineurin is essential for survival during membrane stress in Candida albicans. EMBO J 2002; 21(4): 546–59
Cruz MC, Goldstein AL, Blankenship J, et al. Rapamycin and less immunosuppressive analogs are toxic to Candida albicans and Cryptococcus neoformans via FKBP12-dependent inhibition of TOR. Antimicrob Agents Chemother 2001; 45(11): 3162–70
The SNP Consortium Ltd. Single nucleotide polymorphisms for biomedical research [online]. Available from URL: http://snp.cshl.org [Accessed 2005 Oct 10]
The Wellcome Trust. The human genome [online]. Available from URL: http://www.wellcome.ac.uk/en/genome/index.html [Accessed 2005 Oct 10]
Eisen MB, Spellman PT, Brown PO, et al. Cluster analysis and display of genome-wide expression patterns. Proc Nat Acad Sci 1998; 95: 14863–8
Tamayo P, Slonim D, Mesirov J, et al. Interpreting patterns of gene expression with self-organizing maps: methods and applications to hematopoietic differentiation. Proc Nat Acad Sci 1999; 96: 2907–12
Slonim DK, Tamayo P, Nesirov JP, et al. Class prediction and discovery using gene expression data. Information Systems 2003; 28(4): 243–268 [online]. Available from URL: http://www.broad.mit.edu/mpr/publications/projects/Leukemia/Slonim_et_al_2000.pdf [Accessed 2005 Oct 6]
Brown MPS, Grundy WN, Lin D, et al. Knowledge-based analysis of microarray gene expression data by using support vector machines. Proc Nat Acad Sci 2000; 97: 262–7
Sokal RR, Michener CD. A statistical method for evaluating systematic relationships. Univ Kans Sci Bull 1958; 38: 1409–38
Prigneau O, Porta A, Maresca B. Candida albicans CTN gene family is induced during macrophage infection: homology, disruption and phenotypic analysis of CTN3 gene. Fungal Genet Biol 2004; 41(8): 783–93
Beckerman J, Chibana H, Turner J, et al. Single-copy IMH3 allele is sufficient to confer resistance to mycophenolic acid in Candida albicans and to mediate transformation of clinical Candida species. Infect Immun 2001; 69(1): 108–14
Nakayama H, Mio T, Nagahashi S, et al. Tetracycline-regulatable system to tightly control gene expression in the pathogenic fungus Candida albicans. Infect Immun 2000; 68(12): 6712–9
Agarwal AK, Rogers PD, Baerson SR, et al. Genome-wide expression profiling of the response to polyene, pryimidine, azole and echinocandin anti-fungal agents in Saccharomyces cerevisiae. J Biol Chem 2003; 278: 34998–5015
Garrod AE. The incidence of alkaptonuria: a study in chemical individuality. 1902. Mol Med 1996; 2(3): 274–82
US Department of Health and Human Services. Guidance for industry: pharmacogenomic data submissions. March 2005 [online]. Available from URL: http://www.fda.gov/cder/guidance/6400fnl.pdf [Accessed 2005 Oct 10]
Butler D. Epidemiology set to get fast-track treatment. Nature 2001; 414: 38–43
Clifford RJ, Edmonson MN, Nguyen C, et al. Bioinformatics tools for single nucleotide polymorphism discovery and analysis. Ann N Y Acad Sci 2004; 1020: 101–9
Vogel F. Moderne probleme de humangenetik. Ergeb Inn Med Kinderheilkd 1959; 12: 52–125
Nebert DW. Extreme discordant phenotype methodology: an intuitive approach to clinical pharmacogenetics. Eur J Pharmacol 2000; 410: 107–20
Vesell ES. Pharmacogenetic perspectives gained from twin and family studies. Pharmacol Ther 1989; 41(3): 535–52
Tucker GT, Houston JB, Huang S-M. Optimizing drug development: strategies to assess drug metabolism/transporter interaction potential: toward a consensus. Clin Pharmacol Ther 2001; 70(2): 103–14
Bjornsson TD, Callaghan JT, Einolf HJ, et al. Pharmaceutical Research and Manufacturers of America (PhRMA) Drug Metabolism/Clinical Pharmacology Technical Working Group; FDA Center for Drug Evaluation and Research (CDER). The conduct of in vitro and in vivo drug-drug interaction studies: a Pharmaceutical Research and Manufacturers of America (PhRMA) perspective. Drug Metab Dispos 2003; 31(7): 815–32
Donato MT, Castell JV. Strategies and molecular probes to investigate the role of cytochrome P450 in drug metabolism. Clin Pharmacokinet 2003; 42(2): 153–78
Daly AK. Pharmacogenetics of the major polymorphic metabolizing enzymes. Fund Clin Pharmacol 2003; 17: 27–41
Sachse C, Brockmoller J, Bauer S, et al. Cytochrome P450 2D6 variants in a Caucasian population: allele frequencies and phenotypic consequences. Am J Hum Genet 1997; 60: 284–95
Vickers AEM, Sinclair JR, Zollinger M, et al. Multiple cytochrome P-450s involved in the metabolism of terbinafine suggest a limited potential for drug-drug interactions. Drug Metab Disp 1999; 27(9): 1029–38
Abdel-Rahman SM, Marcucci K, Boge T, et al. Potent inhibition of cytochrome P-450 2D6-mediated dextromethorphan O-demethylation by terbinafine. Drug Metab Dispos 1999; 27(7): 770–5
Madani S, Barilla D, Cramer J, et al. Effect of terbinafine on the pharmacokinetics and pharmacodynamics of desipramine in healthy volunteers identified as cytochrome P450 2D6 (CYP2D6) extensive metabolizers. J Clin Pharmacol 2002; 42(11): 1211–8
FDA Public Health Advisory. The safety of Sporanox® capsules and Lamisil® tablets for the treatment of onychomycosis [online]. Available from URL: http://www.fda.gov/cder/drug/advisory/sporanox-lamisil/advisory.htm [Accessed 2005 Oct 10]
Liu L, Pang KS. The roles of transporters and enzymes in hepatic drug processing. Drug Met Disp 2005; 33(1): 1–9
Venkatakrishnan K, von Moltke LL, Greenblatt DJ. Effects of the antifungal agents on oxidative drug metabolism. Clin Pharmacokinet 2000; 38(2): 111–80
Lamba JK, Lin YS, Thummel K, et al. Common allelic variants of cytochrome P4503A4 and their prevalence in different populations. Pharmacogenet 2002; 12: 121–32
Burk DL, Berghuis AM. Protein kinase inhibitors and antibiotic resistance. Pharmacol Ther 2002; 93(2-3): 283–92
Kuehl P, Zhang J, Lin Y, et al. Sequence diversity in CYP3A5 promoters and characterization of the genetic basis of polymorphic CYP3A5 expression. Nature Genet 2001; 27: 383–91
Chandra P, Brouwer KLR. The complexities of hepatic drug transport: current knowledge and emerging concepts. Pharm Res 2004; 21(5): 719–35
Faber KN, Muller M, Jansen PLM. Drug transport proteins in the liver. Adv Drug Del Rev 2003; 55: 107–24
Nishizato Y, Ieiri I, Suzuki H, et al. Polymorphisms of OATP-C (SLC21A6) and OAT3 (SLC22A8) genes: consequences for pravastatin pharmacokinetics. Clin Pharmacol Ther 2003; 73: 554–65
Seidegard J, Vorachek WR, Pero RW, et al. Hereditary differences in the expression of the human glutathione S-transferase active on trans-stillbene oxide are due to a gene deletion. Proc Natl Acad Sci U S A 1988; 85: 7293–7
Pemble S, Schroeder KR, Spencer SR, et al. Human glutathione S-transferase theta (GSTT1): cDNA cloning and the characterization of a genetic polymorphism. Biochem J 1994; 300: 271–6
Coles BF, Morel F, Rauch C, et al. Effect of polymorphism in the human glutathione S-transferase A1 promoteron hepatic GSTAi and GSTA2 expression. Pharmacogenetics 2001; 11: 663–9
Arylamine N-acetyltransferase (NAT) nomenclature [online]. Available from URL: http://www.louisville.edu/medschool/pharmacology/NAT.html [Accessed 2005 Oct 10]
Relling MV, Rubnitz JE, Rivera GK, et al. Mercaptopurine therapy intolerance and heterozygosity at the thiopurine S-methyltransferase locus. J Natl Cancer Inst 1999; 91: 2001–8
Nagata K, Yamazoe Y. Pharmacogenetics of sulfotransferase. Annu Rev Pharmacol Toxicol 2000; 40: 159–76
Freimuth RR, Eckloff B, Wieben ED, et al. Human sulfotransferase SULT1C1 pharmacogenetics: gene resequencing and functional genomic studies. Pharmacogenetics 2001; 11: 747–56
Nowell S, Sweeney C, Winters M, et al. Association between sulfotransferase 1A1 genotype and survival of breast cancer patients receiving tamoxifen therapy. J Natl Cancer Inst 2002; 94(21): 1635–40
Tukey RH, Strassburg CP. Human UDP-glucuronosyltransferases: metabolism, expression, and disease. Annu Rev Pharmacol Toxicol 2000; 40: 581–616
Desai AA, Innocenti F, Ratain MJ. UGT pharmacogenetics: implications for cancer risk and cancer therapeutics. Pharmacogenetics 2003; 13: 517–23
Riley RJ, Kenna JG. Cellular models for ADMET predictions and evaluation of drug-drug interactions. Curr Opin Drug Discov Devel 2004; 7(1): 86–99
Trowsdale J, Parham P. Defense strategies and immunity-related genes. Eur J Immunol 2004; 34: 7–17
Marsh SGE, Parham P, Barber LD. The HLA factsbook. San Diego (CA): Academic Press, 2000
Nikolich-Zugich J, Fremont DH, Miley MJ, et al. The role of MHC polymorphism in anti-microbial resistance. Microbes Infect 2004; 6: 501–12
Jeffery KJM, Bangham CRM. Do infectious diseases drive MHC diversity? Microbes Infect 2000; 2: 1335–41
Brodsky FM. Stealth, sabotage and exploitation. Immunol Rev 1999; 168: 5–11
DiMauro S, Schon E. Mechanisms of Disease: Mitochondrial respiratory-chain diseases. New Engl J Med 2003; 348(26): 2656–68
The Jackson Laboratory. JAX® mice literature [online]. Available from URL: http://jaxmice.jax.org/library/notes/498l.html [Accessed 2005 Oct 10]
The Jackson Laboratory. Mouse genome informatics [online]. Available from URL: http://www.informatics.jax.org/ [Accessed 2005 Oct 10]
Ajit C, Suvannasankha A, Zaeri N, et al. Terbinafine-associated hepatotoxicity. Am J Med Sci 2003; 325(5): 292–5
Cleary JD, Chapman SW. Altered gene expression in amphotericin B therapy [abstract 139]. 19th Annual American College of Clinical Pharmacy Meeting; 1996 Aug 4–7; Nashville (TN). 139
Cleary JD, Gordon R, Chapman SW. Phase II clinical trial of daclizumab/amphotericin B combination [abstract M-967]. 43rd Interscience Conference on Antimicrobial Agents and Chemotherapy; 2003 Sep 14–17; Chicago (IL). 447
Cleary JD, Schwartz M, Rogers PD, et al. Effects of amphotericin B and caspofungin on histamine expression. Pharmacotherapy 2003; 23(8): 966–73
Caspofungin package insert. Liberty Corner (NJ): Merck Pharmaceuticals, 2005
Cleary JD, Kelley KL, Chapman BA, et al. Differential transcriptome expression: rhodanase and cyanide clearance. 45th Interscience Conference on Antimicrobial Agents and Chemotherapy; 2005 Dec 16–19; Washington, DC
Broad Institute. Fungal genome initiative [online]. Available from URL: http://www.broad.mit.edu/annotation/fungi/fgi/ [Accessed 2005 Oct 10]
National Research Council Canada. Candida albicans Research Lab [online]. Available from URL: http://Candida.bri.nrc.ca/candida/index.cfm?.%20page%20=%20CaAnno,%20assembly%2019 [Accessed 2005 Oct 10]
Sequencing of Candida albicans at the Stanford Genome Technology Center [online]. Available from URL: http://www-sequence.stanford.edu/group/candida/ [Accessed 2005 Oct 10]
Roemer T, Jiang B, Davison J, et al. Large-scale essential gene identification in Candida albicans and applications to antifungal drug discovery. Mol Microbiol 2003; 50(1): 167–81
Bender JA, Fink GR, Lorenz MC. How C. albicans survivies in vivo: a genomic view [abstract]. Seventh American Society of Microbiology Candida and Candidiasis Conference; 2004 Mar 18–22; Austin (TX).
Giaever G, Chu AM, Ni L, et al. Functional profiling of the Saccharomyces cerevisiae genome. Nature 2002; 418(6896): 387–91
De Deken X, Raymond M. Constitutive activation of the PDR16 promoter in a Candida albicans azole-resistant clinical isolate overexpressing CDR1 and CDR2. Antimicrob Agents Chemother 2004; 48(7): 2700–3
Chen CG, Yang YL, Shih HI, et al. CaNdt80 is involved in drug resistance in Candida albicans by regulating CDR1. Antimicrob Agents Chemother 2004; 48(12): 4505–12
Clancy CJ, Cheng S, Checkley M, et al. Antibody screening identifes Candida albicans genes expressed during human oropharyngeal candidiasis that contribue to virulence at mucosal and/or deep tissue sites [abstract]. Seventh American Society of Microbiology Candida and Candidiasis Conference; 2004 Mar 18–22; Austin (TX).
DiDomenico B. Novel antifungal drugs. Curr Opin Microbiol 1999; 2: 509–15
Iraqui I, Aubert S, Cormack B, et al. EPA6P is a major adhesion responsible for biofilm formation by Candida glabrata [abstract]. Seventh American Society of Microbiology Candida and Candidiasis Conference; 2004 Mar 18–22; Austin (TX).
Bruno VM, Lopez LA, Nobile CJ, et al. Analysis of candidate azole resistance genes in C. albicans [abstract]. Seventh American Society of Microbiology Candida and Candidiasis Conference; 2004 Mar 18–22; Austin (TX).
Doedt T, Krishnamurthy S, Bockmuhl DP, et al. APSES proteins regulate morphogenesis and metabolism in Candida albicans. Mol Biol Cell 2004; 15(7): 3167–80
Yeater KM, Chandra J, Cheng G, et al. Microarray analysis of Candida glabrata gene expression during biofilm formation [abstract]. Seventh American Society of Microbiology Candida and Candidiasis Conference; 2004 Mar 18–22; Austin (TX).
Coping VM, Brown AJ, Gow NA, et al. Expression of Candida albicans genes in cells treated with antifungal agents [abstract]. Seventh American Society of Microbiology Candida and Candidiasis Conference; 2004 Mar 18–22; Austin (TX).
White TC, Holleman S, Dy F, et al. Resistance mechanisms in clinical isolates of Candida albicans. Antimicrob Agents Chemother 2002; 46(6): 1704–13
Karababa M, Coste AT, Rognon B, et al. Comparison of gene expression profiles of Candida albicans azole-resistant clinical isolates and laboratory strains exposed to drugs inducing multidrug transporters. Antimicrob Agents Chemother 2004; 48(8): 3064–79
Rogers PD, Kramer RE, Chapman SW, et al. Amphotericin B induces expression of genes encoding chemokines and cell adhesion molecules in the human monocytic cell line THP-1. J Inf Dis 2000; 180: 1259–66
Ullmann BD, Myers H, Chiranand W, et al. Inducible defense mechanism against nitric oxide in Candida albicans. Eukaryot Cell 2004; 3(3): 715–23
Cardenas ME, Cruz MC, Del Poeta M. Antifungal activities of anti-neoplastic agents: saccharomyces cerevisiae as a model system to study drug action. Clin Microbiol Rev 1999; 12: 583–611
Cunningham ML, Irwin R, Boorman G. Tox/Path team takes on differential gene expression. Environ Health Perspect 2003; 111(15): A814–5 [online]. Available from URL: http://ehp.niehs.nih.gov/txg/docs/2003/111-15/nct/nct.html [Accessed 2005 Oct 13]
Cleary JD, Sullivan D, Wilkins D, et al. Pharmacogenomics of disseminated Candidemia [abstract]. Seventh American Society of Microbiology Candida and Candidiasis Conference; 2004 Mar 18–22; Austin (TX).
Cleary JD, Chapman JW. Pharmacogenomic responses in patients with disseminated candidiasis [abstract]. International Society for Human and Animal Mycology Meeting; 2003 May 26; San Antonio (TX).
Cleary JD, Sullivan D, Fang M, et al. Anti-mycotic pharmacogenomics in candidemia [abstract M-1971]. 44th Interscience Conference on Antimicrobial Agents and Chemotherapy; 2004 Oct 30-Nov 2, Washington, DC, 440
Tang YQ, Yeaman MR, Selsted ME. Antimicrobial peptides from human platelets. Infect Immun 2002; 70(12): 6524–33
Gustafson KS, Vercellotti GM, Bendel CM, et al. Molecular mimicry in Candida albicans: role of an integrin analogue in adhesion of the yeast to human endothelium. J Clin Invest 1991; 87(6): 1896–902
Kim HS, Choi EH, Khan J, et al. Expression of genes encoding innate host defense molecules in normal human monocytes in response to Candida albicans. Infect Immun 2005; 73(6): 3714–24
Suzuki H, Kurihara Y, Takeya M, et al. A role for macrophage scavenger receptors in atherosclerosis and susceptibility to infection. Nature 1997; 386(6622): 292–6
Lilic D, Gravenor I, Robson N, et al. Deregulated production of protective cytokines in response to Candida albicans infection in patients with chronic mucocutaneous candidiasis. Infect Immun 2003; 71(10): 5690–9
Babula O, Lazdane G, Kroica J, et al. Relation between recurrent vulvovaginal candidiasis, vaginal concentrations of mannose-binding lectin, and a mannose-binding lectin gene polymorphism in Latvian women. Clin Infect Dis 2003; 37(5): 733–7
Netea MG, van Der Meer JW, Meis JF, et al. Fas-FasL interactions modulate host defense against systemic Candida albicans infection. J Infect Dis 1999; 180(5): 1648–55
Ohman SC, Jontell M, Jonsson R. Phenotypic characterization of mononuclear cells and class II antigen expression in angular cheilitis infected by Candida albicans or Staphylococcus aureus. Scand J Dent Res 1989; 97(2): 178–85
Scaringi L, Cornacchione P, Rosati E, et al. Induction and persistence in vivo of NK/LAK activity by a mannoprotein component of Candida albicans cell wall. Cell Immunol 1994; 155(2): 265–82
Mukhopadhyay K, Prasad T, Saini P, et al. Membrane sphingolipid-ergosterol interactions are important determinants of multidrug resistance in Candida albicans. Antimicrob Agents Chemother 2004; 48(5): 1778–87
Alonso R, Llopis I, Flores C, et al. Different adhesins for type IV collagen on Candida albicans: identification of a lectin-like adhesin recognizing the 7S(IV) domain. Microbiology 2000; 1147 (Pt 7): 1971–81
Netea MG, Van der Graaf C, Van der Meer JW, et al. Recognition of fungal pathogens by Toll-like receptors. Eur J Clin Microbiol Infect Dis 2004; 23(9): 672–6
Churchill GA, Airey DC, Allayee H, et al. The Collaborative Cross, a community resource for the genetic analysis of complex traits. Nat Genet 2004; 36(11): 1133–7
Hamilton PW, Thompson D, Sloan J, et al. Knowledge-guided segmentation and morphometric analysis of colorectal dysplasia. Anal Quant Cytol Histol 1995; 17: 172–82
Bartels PH, Thompson D, Bartels H, et al. Machine vision-based histometry of premalignant and malignant prostatic lesions. Pathol Res Pract 1995; 191: 935–44
Anderson NH, Hamilton PW, Bartels PH, et al. Computerized scene segmentation for the discrimination of architectural features in proliferative lesions of the breast. J Pathol 1997; 181: 374–80
Keenean S, Diamond J, McCluggage WG, et al. An automated machine vision system for the histological grading of cervical intra-epithelial neoplasia (CIN). J Pathol 2000; 192: 351–62
Diamond J, Anderson NH, Bartels PH, et al. The use of morphological characteristics and texture analysis in the identification of tissue composition in prostatic neoplasia. Hum Pathol 2004; 95: 1121–31
Acknowledgments
The authors wish to thank Drs Alice Clark, XingCong Li, Hala ElSohly, Mohammed Ilias, Erdal Bedir, Ikhlas Khan, and their colleagues at the NCNPR; Drs Mark Hamann and Jordan Zjawiony, at the Department of Pharmacognosy, for their work in isolation of the antifungal actives; Drs Li and Zjawiony for preparation of analogs; Dr Chuck Dunbar (NCNPR) for structural elucidations; Drs Melissa Jacob and Shabana Khan of the NCNPR for most of the antifungal screening. All their hard work made evaluation and illustrations of many novel compounds possible.
This paper was funded by a grant from the National Institutes of Health (NIH grant no. AI49770-01A2) entitled, “Pharmacogenomics of natural products with antifungal activity”.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cleary, J.D., Walker, L.A. & Hawke, R.L. Antimycotic Drug Discovery in the Age of Genomics. Am J Pharmacogenomics 5, 365–386 (2005). https://doi.org/10.2165/00129785-200505060-00004
Published:
Issue Date:
DOI: https://doi.org/10.2165/00129785-200505060-00004