
Abstract
Objective
To analyse the relationship between a series of estimated pharmaco-kinetic-pharmacodynamic parameters and the reported efficacy of ceftizoxime.
Design
Retrospective literature search and analysis using different correlation models.
Methods
The following parameters were calculated for each group of patients included in the study from the simulated plasma concentration curves corresponding to the dosage regimen administered: (i) peak concentration at steady state divided by the minimum inhibitory concentration (Cmax SS/MIC); (ii) the time that the plasma drug concentration exceeded the MIC scaled to 24 hours at steady state [(tss)24h > MIC]; (iii) the total area under the concentration-time curve over 24 hours at steady state divided by the MIC [(AUCss)24l/MIC]; and (iv) the AUC at steady state for the period of time that the concentration is above the MIC over a period of 24 hours divided by the MIC [(AUICss)24h]. A univariate correlation analysis was performed considering efficacy [rate (%) of clinical cure or bacterial eradication] as the dependent variable and the pharmacokinetic-pharmacodynamic parameter as the independent variable, using linear and nonlinear models.
Results
(tss)24h > MIC was the only parameter that was statistically correlated with efficacy, the linear model being the best choice among the 4 relationship approaches tested. A biased frequency distribution of reported efficacy data constricts the correlation analysis to a narrow range of efficacy and hinders interpretation of the results.
Conclusions
The reporting of cases with low efficacy rates as well as those with high efficacy rates, including information on patient idiosyncrasies and the infecting organisms, would be of great help in performing retrospective analyses of the use of antimicrobial agents, leading to the optimisation of therapy with this type of drug in clinical practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Antibacterial agents belong to a very heterogeneous group of drugs used in clinical practice with the common aim of preventing bacterial growth in human hosts. The outcomes of patients with infectious diseases receiving antibacterial treatment depend on the interactions among the 3 elements involved in the final response:[1] patient, drug and pathogen. The patient with the infection interacts with the drug, producing a plasma concentration profile dependent upon the absorption, distribution and elimination rates, and also interacts with the infecting bacterium, leading to a destruction rate that depends on the immune response. The antibacterial agent interacts with the pathogen to produce a growth inhibition rate that depends on its potency, its mechanism of action and the time or intensity of exposure (which is in turn determined by the plasma curve). The clinical outcome for infectious pathologies is conditioned by the pharmacokinetics and pharmacodynamics of the drug, as also happens for any other type of illness; nevertheless, in the latter case both depend only on the patient, while in the former case the pharmacokinetics are influenced by patient characteristics and the pharmacodynamics by the type of infecting bacterium.
This type of dual dependence hinders the establishment of the correct dosage pattern for antimicrobial agents. This was first considered by Schentag et al.[1,2] and later by many other authors.[3–5] In recent years, considerable efforts have been directed at finding a suitable methodology that considers both the pharmacokinetic and pharmacodynamic variability of drugs with a view to optimising antimicrobial treatment in clinical practice.[6,7] As a consequence, several so-called efficacy indices, pharmacokinetic-pharmacodynamic parameters, or surrogate markers, have been defined as indicators of the potential efficacy of antibacterial treatments. Such indicators consider a pharmacokinetic parameter together with the minimum inhibitory concentration (MIC) value.
Despite the limitations of the MIC as an indicator of the in vivo antibacterial activity of a drug, until now it has been the pharmacodynamic parameter universally considered for this purpose. Regarding pharmacokinetics, 3 different parameters have been involved in the definition of efficacy indices: the maximum drug plasma concentration (Cmax), the elimination half-life of the drug (t1/2β) and the area under the plasma concentration-time curve (AUC). The definitions of, and differences among, the several indices can be found in the literature.[2,7]
Antibacterial agents can be divided into different groups on the basis of their patterns of bactericidal activity.[8] One pattern is characterised by concentration-dependent killing over a wide range of concentrations, as happens with the aminoglycosides or fluoroquinolones and with metronidazole for anaerobic bacteria.[9] Another pattern is characterised by a limited killing rate when the concentration surpasses the MIC value by 3- to 4-fold, and this is observed with the β-lactam antibacterials, vancomycin, clindamycin and macrolides.[9] The peak value at steady state (Cmax ss)/MIC ratio seems to be the parameter best related to efficacy for drugs with concentration-dependent bactericidal activity, and the time that the plasma drug concentration exceeds the MIC scaled to 24 hours at steady state [(tss)24h > MIC] has been proposed as the best predictor for the other group. Despite this, the total AUC over 24 hours at steady state divided by the MIC [(AUCss)24h/MIC] and the AUC at steady state for the period of time that the concentration is above the MIC over a period of 24 hours divided by the MIC [(AUICss)24h] have been reported as good predictors of clinical outcomes for several drugs belonging to both groups, particularly the fluoroquinolones.[2] Moreover, recent publications[10,11] have pointed to (tss)24h > MIC as the pharmacokinetic-pharmacodynamic parameter best related to efficacy for any group of these drugs.
As previously reported,[2,10,12] there may not be any single efficacy index to predict patient outcome after treatment with a particular antimicrobial agent for all clinical situations, but the optimum pharmacokinetic-pharmacodynamic predictor might be dependent on clinical features.
Analysis of the correlation between the values taken by these parameters and the observed clinical efficacy of treatments may help to find the efficacy index to be considered for antimicrobial dosage optimisation. With this in mind, we were prompted to conduct a retrospective study to establish the relationship between the values achieved by different efficacy indices and the corresponding efficacy of treatment observed with the β-lactam drug ceftizoxime. The aim of this study was to evaluate the validity of the above-mentioned parameters in the prediction of clinical outcomes with this antibacterial administered under different dosage schedules for different clinical environments, using the data reported in the literature.
Patients and Methods
The methodology followed to carry out this work has been described previously in Clinical Pharmacokinetics[7] and was recently applied to ciprofloxacin.[10] Briefly, it consists of the following steps: acquisition of data, selection of data, estimation of efficacy indices and correlation analysis.
Data Acquisition
WINSPIRS (which includes MEDLINE, IPA and LIFE-SCIENCES) and Iowa Drug Information Service (IDIS) computer systems were used for the bibliographical search to collect information about the clinical efficacy of ceftizoxime, published within the period 1980 to 1997. Other biomedical journals not included in these databases were also reviewed.
Selection of Data
First, all publications including data about the clinical efficacy of treatments with ceftizoxime were collected. Following this, the following exclusion criteria were applied to the data thus acquired: (i) infectious processes caused by more than one pathogen; (ii) infections produced by an unidentified micro-organism; (iii) incomplete description of the treatment applied; (iv) paediatric patients; (v) renally impaired patients; (vi) multiple antibacterial treatments; and (vii) studies with less than 5 patients.
We define a ‘clinical case’ as a group of 5 or more patients infected at the same site with the same species of bacteria. After applying these criteria, the data were reduced to 60 different clinical cases[13–19] corresponding to infections caused by 24 different bacteria; these bacteria are shown in table I.[20–27]

90% minimum inhibitory concentration (MIC90) of ceftizoxime for the pathogens responsible for the infections in the clinical cases considered for correlation analysis
Estimation of Efficacy Indices
The following indices were calculated for each clinical case: Cmax ss/MIC, (tss)24h > MIC,[6] (AUCss)24h/MIC and (AUICss)24h.
A mean MIC value calculated from the data found in the literature was used to estimate the different indices. Table I shows the range of reported MIC values for the pathogens responsible for the infections in the clinical cases considered.
Cmax ss/MIC, (tss)24h > MIC, (AUCss)24h/MIC and (AUICss)24h were obtained from the simulated plasma concentration curves corresponding to the reported dosage regimens of ceftizoxime administered. As happens with other drugs, the administration route determines the optimum pharmacokinetic model to be used. The parameters defining the 1- and 2-compartment models were taken from the literature.[28–38] A 2-compartment model was used for the simulation of drug curves for intravenous administration with the following pharmacokinetic parameter values: distribution volume of the central compartment (Vc) = 0.27 L/kg; plasma clearance (CLp) = 0.15 L/h/kg; transfer rate constant from the central to the peripheral compartment (k12) = 3.17h-1 and transfer rate constant from the peripheral to the central compartment (k21) = 2.11h−1.
When ceftizoxime was administered intramuscularly, simulation of plasma curves was carried out using a 1-compartment model with the following parameters: volume of distribution (Vd) = 0.34 L/kg; CLp = 0.15 L/h/kg and absorption rate constant (Ka) = 1.87h−1.
Dosages, administration intervals and the total number of doses received by the patients described in the literature searched, and selected according to the above-mentioned exclusion criteria, were considered for curve simulation. Cmax ss and (tss)24h > MIC were obtained directly from simulated curves. Additionally, the simulated curves provide the time-concentration data necessary to calculate (AUCss)24h and (AUICss)24h by numerical integration,[39] as previously described.[7]
Simulation of the plasma concentration curves was carried out using the PKS Pharmacokinetic Computer System (Abbot Laboratories Diagnostic Division, Abbot Park, IL, USA).
Correlation Analysis
A univariate correlation analysis[40] was performed with the percentage of reported efficacy and the calculated indices as the dependent and independent variables, respectively. Linear and nonlinear conventional response models[41] were used for the correlation analysis. The equations defining these models are:
Linear models:
where a, a′ and b, b′ are the intercept and the slope values of the regression straight lines, respectively, I represents the calculated index [Cmaxss/MIC, (tss)24h > MIC, (AUCss)24h/MIC or (AUICss)24h] and E is the observed efficacy expressed as the percentage of either clinical cure or bacterial eradication. Emax model:
where Emax and E0 represent the maximum and intrinsic responses, respectively, I50 is the value of the index for a response of 50% of Emax, and n is the Hill coefficient related to the curve profile, leading to the asymptotic and sigmoid Emax models when n = 1 and n ≠1, respectively.
Model fitting was carried out using the PCNonlin 4.2 program (Scientific Consulting, Inc., Apex, NC, USA), which optimises the model parameters by nonlinear regression techniques according to statistical criteria such as the standard deviation of parameters and minimum Akaike’s information criterion (AIC).[42]
An analysis of variation (ANOVA) of the regression[40] was performed to establish the statistical significance of the slope for the linear models (p < 0.05).
Results
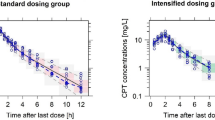
Table II shows the values of Cmax ss/MIC, (tss)24h > MIC, (AUCss)24h/MIC and (AUICss)24h calculated and their corresponding reported percentages of efficacy for ceftizoxime. Most data are for high efficacy rates, as shown by the biased frequency distribution histogram for reported efficacy in figure 1, which constrains the range to 71 to 100% efficacy and restricts the correlation analysis. A high dispersion of the index values for the same percentage of efficacy reported is observed, with mean values of 286.90 ± 505.22, 19.81 ± 7.39h, 1573.63 ± 2304.11h and 1811.21 ± 2656.43h for Cmax ss/MIC, (tss)24h > MIC, (AUCss)24h/MIC and (AUICss)24h, respectively, when 100% efficacy is recorded. The cases in table II with zero values for the calculated indices were not considered for the correlation analysis.


Values of estimated pharmacokinetic-pharmacodynamic indices and corresponding reported efficacy of ceftizoxime

Frequency distribution histogram of ceftizoxime efficacy data used to perform the pharmacokinetic-pharmacodynamic analysis. A ‘clinical case’ is a group of 5 or more patients infected at the same site with the same species of bacteria.
Tables III and IV show the parameters corresponding to the linear and the asymptotic Emax models respectively, together with the statistics of the correlation analysis. No correlation was found when the log-linear or the sigmoid Emax approaches were used.

Parameters defining the linear relationship between the reported efficacy and estimated indices of ceftizoxime

Parameters defining the asymptotic relationship between the reported efficacy and estimated indices of ceftizoxime
Discussion
As seen in table II, several cases of high efficacy with very low index values (even zero) were found. Scrutiny of these cases reveals that these correspond to infections caused by Pseudomonas aeruginosa, Staphylococcus aureus, Enterobacter spp. and Bacteroides for which MIC ranges of 6.3 to 100, 3.1 to 64, 0.12 to 100 and 4 to 128 mg/L, respectively, are reported for ceftizoxime. It should be noted that a mean MIC value was used to calculate the indices; the mean value is considered to be a good estimator of a particular value for normally distributed, low dispersed data, but it may differ strongly from any particular value for highly dispersed sample data.[10]
It is likely that the mean MIC literature values used to estimate these efficacy indices are not representative of the actual MIC value in such cases. This contradictory finding of some cases with maximum efficacy accompanied by low index values is not new for ceftizoxime, but rather had appeared previously when performing a similar study with ciprofloxacin,[10] although this happened in fewer cases for the quinolone. It is evident that the high variability in the literature MIC values seriously restricts the above-described methodology, since a true value of this parameter is essential for the correct calculation of the indices. This high variability in the reported MIC values also compromises the efficacy of antimicrobial treatments in such cases when the drug is empirically selected on the basis of the suspected pathogen and its reported MIC value, as for community-acquired infections or acute phases of hospital infections. Fortunately, growing concern about this problem has arisen among microbiologists and specialists in infectious disease and specific actions, such as the Alexander Project,[43,44] are being carried out to examine the antimicrobial susceptibilities of bacterial isolates from all over the world. There is a fair degree of consensus about the importance of greater surveillance of susceptibility and standardised test methods among laboratories, and recently very interesting results have been reported by Livermore et al.[45] highlighting the significance of these problems.
Despite the above limitations of using literature MIC values, the correlation analysis was performed by rejecting those cases with zero values for the indices. Although a poor correlation was found between the values of the estimated indices and the efficacy reported for ceftizoxime, a linear relationship between (tss)24h > MIC and efficacy was established (Pearson coefficient value of 0.402, and statistical significance of the slope of 1.9 × 10-3 [p = 0.0019]). For the rest of the indices, the slope did not show statistical significance (p > 0.05).
The asymptotic Emax model managed to fit the data for Cmaxss/MIC, (tss)24h > MIC and (AUCss)24h/MIC, but not for (AUICss)24h. According to the statistical criteria of model selection, this model is not a better choice since the AIC values do not decrease in comparison with the simplest linear model. Moreover, a lower degree of precision of the estimated parameters is observed with the asymptotic Emax model. Regarding the log-linear model and the sigmoid Emax model, both failed to fit the data. Accordingly, the time that the plasma concentrations are above the MIC value is the pharmacokinetic-pharmacodynamic parameter best related to efficacy for ceftizoxime under the conditions used in this study, which included a broad spectrum of infecting bacteria and a wide range of clinical circumstances.
In comparison with results recently obtained with ciprofloxacin in a very similar study,[10] these point to analogies and differences that merit comment. First, (tss)24h > MIC is the index best correlated with efficacy for both antibacterials, but in the case of ciprofloxacin not only this parameter but also the other 3 proved to have a statistical correlation, all of them being indicators of efficacy. Another difference is that the asymptotic Emax (n = 1) model constitutes a good alternative for correlation analysis with the quinolone, whereas it is not a good choice for ceftizoxime. The better goodness of data fitting observed for ciprofloxacin may be because of the wider efficacy range (100% to 24%) reported for this drug, since the remaining factors involved in the study were very similar for both cases.
Regarding the finding of (tss)24h > MIC as the best predictor of efficacy, according to previous information on the pharmacodynamics of β-lactam antibacterials this is in total agreement with the expectations for ceftizoxime; nevertheless, it is not expected for antibacterial agents that show concentration-dependent bactericidal activity, such as the fluoroquinolones, which should theoretically show the best correlation between the Cmax ss/MIC ratio and treatment efficacy. Despite the large body of information confirming higher bacterial killing rates with higher concentrations for fluoroquinolones or aminoglycosides, several studies carried out with this type of drug have disclosed that the Cmax ss/MIC ratio is not the pharmacokinetic-pharmacodynamic parameter best correlated to efficacy in clinical practice. Instead, other parameters depending on the AUC seem to be better predictors of efficacy for these antibacterials.[46,47] Since AUC is a pharmacokinetic parameter depending on t1/2β, there is covariance between both types of index and, therefore, if one is related to clinical response the other should also be related to it. This proves that the clinical efficacy of these drugs is also governed by the time that their concentrations remain above the MIC. This hypothesis is supported by the results from Bouvier et al.,[11] who integrated the kinetic behaviour of the drug and the fate of the bacterial population in a pharmacokinetic-pharmacodynamic model, and concluded that for concentration-independent as well as for concentration-dependent antimicrobial agents the longer the (tss)24h > MIC the higher the efficacy.
Additional studies of the correlation between pharmacokinetic-pharmacodynamic parameters and efficacy observed in clinical practice would be of great interest in clarifying the type of relationship between both variables and also in establishing the influence of certain clinical factors, such as the infecting organism or site of infection. In this context, it has recently been reported that the type of infecting bacteria is a relevant factor to be considered for the optimisation of administration of fluoroquinolones; an (AUCss)24h/MIC ratio of 125 to 250h has been reported to be related to clinical efficacy for Gram-negative infections, but values of 30 to 55h are sufficient for aerobic Gram-positive pathogens.[47] This is an interesting finding and should be taken into account when analysing the relationship between the efficacy of antibacterial agents and pharmacokinetic-pharmacodynamic indices. It is possible that the type of infecting bacteria could strongly determine the efficacy index to be considered as well as the type of antibacterial. The infection site may also be another factor. This might explain the lack of agreement in the data reported in the literature about the efficacy index that best predicts clinical outcome for a particular antibacterial. Further investigations in this field are necessary to confirm or reject such a hypothesis.
Conclusions
According to our results with ceftizoxime, the time that the plasma concentrations remain above the MIC is the only pharmacokinetic-pharmacodynamic index correlated with efficacy, although the biased efficacy range reported for this drug and used to perform the correlation analysis may influence this finding. If more information about the use of antimicrobial agents in clinical practice (including failures as well as successes) were available, a more accurate retrospective correlation analysis could be performed to determine the factors influencing clinical outcome. In this sense, maximum information about the patients’ idiosyncrasies and the infecting organism(s), together with the widest efficacy range observed, should be provided in the literature to facilitate the pharmacokinetic-pharmacodynamic interpretation of the results reported.
Prospective studies designed to provide all the necessary information (the aetiology of the infection with the actual MIC value, together with a complete description of patients, the treatment administered and the response obtained) would be the best alternative to investigate the pharmacokinetic-pharmacodynamic relationship for antimicrobial agents in order to optimise such type of pharmacotherapy in clinical practice.
References
Schentag JJ, Ballow CH, Paldino JA, et al. Dual individualization with antibiotics: integrated antibiotic management strategies for use in hospitals. In: Evans WE, Schentag JJ, Jusko WJ, editors. Applied pharmacokinetics. 3rd ed. Vancouver (WA): Applied Therapeutics, Inc., 1992; 17: 1–20
Schentag JJ, Nix DE, Adelman MH. Mathematical examination of dual individualization principles: I. Relationships between AUC above MIC and area under the inhibitory curve for cefmenoxime, Ciprofloxacin and tobramycin. Ann Pharmacother 1991; 25: 1050–7
Goss TF, Forrest A, Nix DE, et al. Mathematical examination of dual individualization principles: II. The rate of bacterial eradication at the same area under the inhibitory is more rapid for Ciprofloxacin than for cefmenoxime. Ann Pharmacother 1994; 28: 863–8
Luzier A, Goss TF, Cumbo TJ, et al. Mathematical examination of dual individualization principles: III. Development of a scoring system for pneumonia staging and quantitation of response to antibiotics: results in cefmenoxime treated patients. Ann Pharmacother 1992; 26: 1358–65
Hyatt JM, Mckinnon PS, Zimmer GS, et al. The importance of pharmacokinetic/pharmacodynamic surrogate markers to outcome. Clin Pharmacokinet 1995; 28: 143–60
Li RC, Zhu M, Schentag JJ. Achieving an optimal outcome in the treatment of infections: the role of clinical pharmacokinetics and pharmacodynamics of antimicrobials. Clin Pharmacokinet 1999; 37: 1–16
Sánchez-Navarro A, Sánchez Recio MM. Basis of anti-infective therapy: pharmacokinetic-pharmacodynamic criteria and methodology for dual dosage individualisation. Clin Pharmacokinet 1999; 37: 289–304
Shah PM, Junghanns W, Stille W. Bactericidal dose-activity relationships with E. coli, K. pneumoniae and Staphylococcus aureus [in German]. Dtsch Med Wochenschr 1976; 101: 325–8
Craig WA. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis 1998; 26: 1–10
Sanchez-Recio MM, Colino CI, Sanchez-Navarro A. A retrospective analysis of pharmacokinetic/pharmacodynamic indices as indicators of the clinical efficacy of Ciprofloxacin. J Antimicrob Chemother 2000; 45: 321–8
Bouvier D’Ivoire MIJ, Marie PH. Dosage regimens of antibacterials. Implications of a pharmacokinetic/pharmacodynamic model. Clin Drug Invest 1996; 11: 229–39
Dudley MN. Pharmacodynamics and pharmacokinetics of antibiotics with special reference to the fluoroquinolones. Am J Med 1991; 91 Suppl. 6A: 45–50S
Clini V, Clini E, Tana F, et al. Ceftizoxime in lower respiratory tract infection. Drug Invest 1992; 4 Suppl. 1: 38–9
Bechard DL. The efficacy of ceftizoxime in the therapy of bacteraemia. J Antimicrob Chemother 1982; 10 Suppl. C: 175–81
Montgomerie JZ, Morrow JW, Canawati HN, et al. Ceftizoxime in the treatment of urinary tract infection in spinal cord injury patients: comparison with tobramycin. J Antimicrob Chemother 1982; 10 Suppl. C: 247–52
Shimada J, Shimizu K. Experience with ceftizoxime: an overall summary of clinical trials in Japan. J Antimicrob Chemother 1982; 10 Suppl. C: 311–26
Parks D, Layne P, Uri J, et al. Ceftizoxime: clinical evaluation of efficacy and safety in the USA. J Antimicrob Chemother 1982; 10 Suppl. C: 327–38
Rimoldi R, Mandler F, Grasso S, et al. Clinical and bacteriological evaluation of ceftizoxime in lower respiratory tract infections. In: Spitzy KH, Karrer K, editors. Ceftizoxime. Proceedings of the Thirteenth International Congress of Chemotherapy; 1983 Aug 28–Sep 2; Vienna, Pt 32: 36–9
Fainstein V, Bolivar R, Elting L, et al. Ceftizoxime in the treatment of infections of patients with cancer. J Antimicrob Chemother 1982; 10 Suppl. C: 167–73
Richards DM, Heel RC. Ceftizoxime: a review of its antibacterial activity, pharmacokinetic properties and therapeutic use. Drugs 1985; 29: 281–329
Fu KP, Neu HC. Antibacterial activity of ceftizoxime, a β-lactamase-stable Cephalosporin. Antimicrob Agents Chemother 1980; 17: 583–90
Greenwood D, Pearson N, Eley A, et al. Comparative in vitro activities of cefotaxime and ceftizoxime (FK-749). New Cephalosporins with exceptional potency. Antimicrob Agents Chemother 1980; 17: 397–401
Muytjens H, van der Ros-van de Repe J. Comparative activities of 13 β-lactam antibiotics. Antimicrob Agents Chemother 1982; 21: 925–34
Bodey GP, Fainstein V, Hinkle AM. Comparative in vitro study of new Cephalosporins. Antimicrob Agents Chemother 1981; 20: 226–30
Yabuuchi E, Ito T, Tanimura N, et al. In vitro antimicrobial activity of ceftizoxime against glucose-nonfermentative gram-negative rods. Antimicrob Agents Chemother 1981; 20: 136–9
Drulak MW, Chow AW. Comparative in vitro activity of ceftizoxime, cefoperazone and cefoxitin against anaerobic bacteria. Antimicrob Agents Chemother 1981; 20: 683–5
Barry AL, Jones RN, Thornsberry C, et al. Ceftizoxime: collaborative multiphased in vitro evaluation including tentative interpretive standards for disc susceptibility test β-lactamase stability and inhibition. J Antimicrob Chemother 1982; 10 Suppl. C: 25–44
Cutler RE, Blair AD, Burgess ED, et al. Pharmacokinetics of ceftizoxime. J Antimicrob Chemother 1982; 10 Suppl. C: 91–7
Quintiliani R, Nightingale CH. Comparative pharmacokinetics of ceftizoxime and other third-generation Cephalosporins in humans. J Antimicrob Chemother 1982; 10 Suppl. C: 99–104
Shyu WC, Jordan NS, Quintiliani R, et al. Comparative pharmacokinetics of ceftizoxime (CZ) and cefotaxime (CT). In: Spitzy KH, Karrer K, editors. Ceftizoxime. Proceedings of the 13th International Congress of Chemotherapy; 1983 Aug 28–Sep 2; Vienna, Pt 32: 29–31
Kowalsky SF, Echols RM, Venezia AR, et al. Pharmacokinetics of ceftizoxime in subjects with various degrees of renal function. Antimicrob Agents Chemother 1983; 24: 151–5
Nakashima N, Suzuki K, Hashimoto H, et al. Phase I study of ceftizoxime, a new Cephalosporin: single-dose study. J Clin Pharmacol 1981; 21: 388–95
Peterson LR, Gerding DN, Van Etta LL, et al. Pharmacokinetics, protein binding and extravascular distribution of ceftizoxime in normal subjects. Antimicrob Agents Chemother 1982; 22: 878–81
Vallee F, LeBel M. Comparative study of pharmacokinetics and serum bactericidal activity of ceftizoxime and cefotaxime. Antimicrob Agents Chemother 1991; 35: 2057–64
Ohkawa M, Okasho A, Sugata T, et al. Elimination kinetics of ceftizoxime in humans with and without renal insufficiency. Antimicrob Agents Chemother 1982; 22: 308–11
Neu HC, Srinivasan S. Pharmacology of ceftizoxime compared with that of cefamandole. Antimicrob Agents Chemother 1981; 20: 366–9
Furlanut M, Montanari G, Padrini R, et al. Pharmacokinetics of ceftizoxime in healthy adult volunteers. Drug Exp Clin Res 1983; 9: 657–9
Neu HC. Ceftizoxime: a β-lactamase-stable, broad-spectrum Cephalosporin: pharmacokinetics, adverse effects and clinical use. Pharmacotherapy 1984; 4: 47–58
Yamaoka K, Nakagama T, Uno T. Statistical moments in pharmacokinetics. J Pharmacokinet Biopharm 1978; 6: 547–58
Sachs L. Measures of association: correlation and regression. In: Sachs L, editor. Applied statistics. New York: Springer-Verlag, 1982: 382–456
Ebert SC. Pharmacokinetic-pharmacodynamic modelling of irreversible drug effects. In: Derendorf H, Hochhaus G, editors. Handbook of pharmacokinetic/pharmacodynamic correlation. London: CRC Press, 1995: 35–6
Dunne AP, Stacker GE. PCNONLIN 4.2. Science software user’s guide. Lexington (KY): Statistical Consultants, 1992
Felmingham D, Grüneberg RN, Alexander Project Group. A multicentre collaborative study of the antimicrobial susceptibility of community-acquired, lower respiratory tract pathogens 1992–1993: the Alexander Project. J Antimicrob Chemother 1996; 38 Suppl. A: 1–57
Felmingham D, Grüneberg RN, Alexander Project Group. The Alexander Project 1996–1997: latest susceptibility data from this international study of bacterial pathogens from community-acquired lower respiratory infections. J Antimicrob Chemother 2000; 45: 191–203
Livermore DM, Threlfall EJ, Reacher MH, et al. Are routine sensitivity test data suitable for the surveillance of resistance? Resistance rates amongst Escherichia coli from blood and CSF from 1991–1997, as assessed by routine and centralized testing. J Antimicrob Chemother 2000; 45: 205–11
Ament PW. Predicting fluoroquinolone therapy outcomes: potential role of the AUC/MIC ratio. Formulary 1999; 34: 1033–40
Forrest A, Chodosh S, Amantea MA, et al. Pharmacokinetics and phannacodynamics of oral grepafloxacin in patients with acute bacterial exacerbations of chronic bronchitis. J Antimicrob Chemother 1997; 40 Suppl. A: 45–57
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sánchez-Navarro, A., Colino, CI. & Sánchez Recio, M.M. A Retrospective Analysis of Pharmacokinetic-Pharmacodynamic Parameters as Indicators of the Clinical Efficacy of Ceftizoxime. Clin Pharmacokinet 40, 125–134 (2001). https://doi.org/10.2165/00003088-200140020-00004
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003088-200140020-00004