
Abstract
Background
Dietary cholesterol has been confirmed to be associated with high risks of diabetes, hypertension, and stroke, but whether it is detrimental to cognitive health is highly debated. This study aimed to investigate the associations between dietary cholesterol and all-cause dementia and AD dementia.
Methods
This prospective study analyzed Framingham Offspring Study cohort (FOS) participants who were dementiafree at baseline and had detailed information on daily diet (measured by food frequency questionnaires) and demographic characteristics. Surveillance for incident dementia commenced at examination 5 (1991–1995) through 2018 and continued for approximately 30 years.
Results
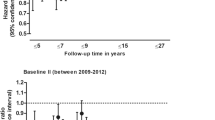
A total of 3249 subjects were included with a mean age of 54.7 years (SD: 9.8). During a median follow-up of 20.2 years (interquartile range: 14.2–24.8), a total of 312 incident dementia events occurred, including 211 (67.7%) cases of AD dementia. After multivariate adjustments for established dementia risk factors, participants with the highest intake of dietary cholesterol had a lower risk of all-cause dementia (HR: 0.70; 95% CI: 0.57–0.93) and AD dementia (HR: 0.68; 95% CI: 0.60–0.88) relative to individuals with the lowest intake. However, the associations were not significant for the group with a medium intake of dietary cholesterol.
Conclusion
High intake of dietary cholesterol was associated with a decreased risk of all-cause dementia and AD dementia. The findings of this observational study need to be confirmed by other studies to highlight the role of dietary cholesterol in the development of neurodegenerative diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dementia is a group of cognitive dysfunctions, including thinking, memory, and reasoning. Furthermore, as one of the most prevalent neurodegenerative diseases, dementia, whose main subtype is Alzheimer’s disease (AD), has caused a heavy disease burden and posed a great public health challenge worldwide (1, 2). However, the pathophysiological processes leading to dementia have not been fully elucidated, and there are no effective strategies to treat dementia or to delay cognitive decline (3). Therefore, it is necessary to target risk factors to prevent dementia in the elderly and delay the onset of the disease. Diet and other lifestyle factors have been identified as important and promising modifiable risk factors for dementia (4–7).
High intake of dietary cholesterol, such as eggs, red meat, poultry, and full-fat dairy products, has traditionally been stigmatized with warnings since it was associated with high risks of hypercholesterolemia, diabetes, hypertension, and stroke (8, 9). However, associations between dietary cholesterol and dementia have not been fully investigated, and the results of previous studies have been inconsistent. Meta-regression analyses indicated a positive, nonlinear relation between dietary cholesterol and LDL-C, a known risk factor for dementia, and dietary cholesterol intake was significantly higher in subjects with altered cognitive performance (10–12). In contrast, inverse associations between dietary cholesterol and mild cognitive impairment (MCI), which is a precursory stage of dementia, were shown in a cross-sectional study (13). There have also been reports of no significant dietary cholesterol-dementia associations (14). In summary, the conclusion of these studies has been limited by the presence of high variability in study design, including heterogeneous patient populations, incomprehensive diet assessment, and varied prevalence of dementia risk factors in the population studied. Regarding outcomes, the existing studies have also been limited by inaccurate and nonstandard surveillance, diagnosis, and subtype of dementia.
Hence, we examined the long-term associations between dietary cholesterol and risks of all-cause dementia and AD dementia in the Framingham Offspring Study cohort, a large prospective study of the US community population with detailed demographic characteristics, medical history, and lifestyle factors and over decades of follow-up.
Methods
Study Design and Population
The Framingham Heart Study (FHS) involves a series of ongoing, prospective, population-based cohorts from the town of Framingham, MA, USA. The Original cohort was established in 1948, and the Framingham Offspring Study cohort (FOS, ClinicalTrials.gov: NCT00005121) was established in 1971, including children of the Original cohort and their spouses. The Offspring cohort recruited 5,124 participants who were studied over nine examination cycles at approximately four-year intervals, with the latest one concluding in 2018. At each exam, each subject underwent standardized interviews, physician examinations, laboratory tests, lifestyle habit assessments, and continuous surveillance for various incident outcomes, including dementia. Details of the Framingham Offspring Cohort have been described previously (15). All participants provided written informed consent. The original study protocol was approved by the institutional review board and Boston University Medical Center, and the present secondary study was approved by the institutional review board for human research at the First People’s Hospital of Chongqing Liang Jiang New Area.
Dietary assessment
The Harvard semiquantitative Food Frequency Questionnaire (FFQ) was used to assess dietary cholesterol intake. The FFQ consists of a list of foods with standard serving size, with the selection of 9 frequency categories for each food ranging from never or < 1 serving/month to ≥6 servings/day. Participants were asked to report their frequency of intake of each food item during the year prior and the frequencies and doses of vitamin and mineral supplements used. We considered individual FFQs to be valid if there were <13 blank items and the estimated daily caloric intake was ≥600 kcal/d and <4000 kcal/d for women or <4200 kcal/d for men (16).
For the present study, examination cycle 5 was defined as the baseline, since it was the first and only thorough and intact evaluation of dietary cholesterol intake, and confounders were obtained at this time point. Nutrients and energy intake were derived by multiplying the nutrients and energy content of each food of the specific portion size by the frequency of consumption as stated on the FFQ and then summed over all food items. Consumption frequencies of food items were converted into estimated numbers per day using the median. Estimated daily cholesterol (mg/d), total energy (Cal/d), alcohol (g/d), carbohydrate (g/d), protein (g/d) and fat (g/d) intakes were derived.
Outcome ascertainment
Methods used for dementia screening and follow-up have been previously described (17, 18). Our primary outcomes of interest included the incidence of all-cause dementia and AD dementia, both of which were determined a priori and assessed through 2018. A diagnosis of dementia was made in accordance with the Diagnostic and Statistical Manual of Mental Disorders, 4th edition. Alzheimer’s disease was based on the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) for definite, probable, or possible AD (19, 20). Full methods for dementia surveillance and confirmation are described in the eMethods in the Supplement.
Covariates
In these analyses, those factors that have been demonstrably considered risk factors for dementia were found to be confounders. The clinical covariates were drawn from the most recent examination cycle during the period of dietary cholesterol intake assessment (5th exam cycle).
Body mass index (BMI) was defined as the ratio of weight to squared height. Waist circumstance (WC) was measured by a trained professional by applying anthropometric tape at the level of the umbilicus. Physical activity was self-reported using the physical activity index (PAI). Smoking was categorized into two groups (current smokers and not current smokers). We classified participants as having diabetes mellitus if they had fasting blood glucose concentrations >7 mmol/L or used hypoglycemic medications and as having hypertension if systolic blood pressure (SBP) >140 mmHg, diastolic blood pressure (DBP)>90 mmHg, or use of antihypertensive medications. Mini-mental score examination (MMSE), employment status (working, retired or unemployed), personal income (>25,000 dollar/year or not), marital status (single, married, no longer married, unknown) and educational level (no high school degree, high school degree, some college, college degree) were assessed by medical interviews. Fasting (≥8 h or overnight) blood samples were drawn to assess the concentrations of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C) and glucose.
Statistical Analysis
Baseline characteristics of participants were described by equal tertiles of dietary cholesterol intake. Means and standard deviations are presented for continuous variables and were tested by variance (ANOVA). Frequency and percentage are presented for categorical variables and tested by chi-square test. Follow-up time was calculated as the time from the date of the baseline FFQ through date of diagnosis of dementia, date of death, date of not consenting to follow-up, or date of the end of the latest survey, whichever came first. We used Cox proportional hazards models to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of all-cause dementia or AD dementia associated with dietary cholesterol intake. The lowest tertile of intake formed the reference category, and the continuous variable for each exposure was used to calculate the P value for trend. In multivariable adjustment, potential confounder selection was based on literature and deferring to statistical criteria. Model 1 was adjusted for sex, age, MMSE at baseline, and education level. Model 2 was further adjusted for SBP, prevalent hypertension, LDL-C, prevalent diabetes mellitus, current smoking, alcohol consumption, employment status, dietary fiber intake, total energy intake, personal income, marital status, PAI, and BMI. Schoenfeld residuals were used to check proportionality assumptions. Kaplan-Meier curves were used with adjustment for age and sex to describe all-cause dementia and AD dementia risk according to dietary cholesterol intake. To assess how robust our results were to the potential unmeasured confounding, we calculated the E-value through an online calculator (https://www.evalue-calculator.com/) (21, 22), with an assumption of outcome prevalence less than 15%. The E-value represents what the minimum HR would have to be for an unmeasured confounder, conditional on the measured covariates, to negate the observed association of diet cholesterol consumption with all-cause dementia and AD dementia. A competing risk regression analysis was conducted to avoid risk overestimation where death was set as a competing risk event for dementia. Analyses were performed using SPSS version 23 (SPSS Inc., Chicago, IL, USA) and Stata statistical software, version 15 (Stata Corporation, College Station, Texas, USA). A 2-sided P<0.05 was considered statistically significant. All analyses were performed based on a predefined statistical analysis plan (available on request).).
Results
Participant characteristics
Among the 5,124 participants in the FHS-OS, 3341 had a valid FFQ at the baseline examination (5th cycle) and over a median of 20.2 years (interquartile range: 14.2–24.8) of follow-up, 54 subjects lacked information on dementia, 14 subjects were diagnosed with dementia at baseline, and 24 subjects were lost to follow-up. Therefore, 3249 subjects could be included in the final analyses with a mean age of 54.7 years (SD: 9.8) (see Figure 1).

Selection of Study Participants in the Framingham Heart Study
Compared with those with a lower cholesterol intake, participants with a higher cholesterol intake were more likely to be male, current smokers, married, and working at that time and to have a higher BMI, WC, PAI, SBP, DBP, LDL-C, TC, and income. They also tended to have a higher intake of total calories, alcohol consumption, carbohydrates, protein, animal fat, vegetable fat, and dietary fiber (see Table 1). These excluded persons were comparable to the subjects in the final analysis (eTable 1 in the Supplement).
Dementia events
The absolute number of dementia events over the follow-up period was 312, including 121 (38.8%) dementia events in the low intake group, 108 (34.6%) in the medium intake group and 83 (26.6%) in the high intake group, with an overall incidence rate of 5.1 per 1000 person-years. Regarding dementia events with respect to subtypes and status, see Table 2.
Dietary cholesterol consumption and risk for dementia
After full adjustment for potential confounders, including demographic and lifestyle factors and key dietary nutrients, the highest dietary cholesterol intake was associated with modestly decreased risks of all-cause dementia (HR: 0.70; 95% CI: 0.57–0.93; P-trend < 0.001; E-value=2.21) and AD dementia (HR: 0.68; 95% CI: 0.60–0.88; P-trend < 0.001; E-value= 2.30) compared with the lowest tertile of intake. However, the medium tertile of dietary cholesterol intake tended to increase the risks of all-cause dementia and AD dementia but lacked statistical significance (see Table 3). Figure 2 shows the cumulative incidence curves for all-cause dementia and AD dementia according to the tertiles of dietary cholesterol intake after adjustment for age and sex. In the competing risk regression analysis where death was set as a competing event, the association between dietary cholesterol intake and all-cause dementia and AD dementia did not significantly differ in the Cox proportional hazards model. In detail, comparing the lowest categories for total WG intake, a 27% (SHR 0.73, 95% CI 0.56–0.92, P=0.001) lower rate of all dementia and a 30% (SHR 0.70, 95% CI 0.51–0.89, P=0.001) lower rate of AD dementia in the highest category of dietary cholesterol consumption were found.

Adjusted cumulative incidence of all-cause dementia and AD dementia based on dietary cholesterol intake
Data are for the cumulative incidence of (A) all dementia, and (B) AD dementia among participants based on dietary cholesterol intake in the Framingham Offspring Study. Adjustments were made for age and sex; Abbreviations: AD, Alzheimer’s disease; DC, dietary cholesterol.
Discussion
Using data from a large population-based cohort, we found that a high intake of dietary cholesterol (over 255 mg/d) was associated with a decreased risk of all-cause dementia and AD dementia after carefully adjusting for other dementia risk factors and demographic covariates. However, a medium intake is not; consequently, a nonlinear pattern of dietary cholesterol is related to risks of all-cause dementia or AD dementia.
Recently, the association between diet and dementia has been a research focus for dementia prevention. For instance, the Mediterranean-Dietary Approaches to Stop Hypertension Intervention for Neurodegenerative Delay (MIND) diet has been proven to be a brain-healthy diet (23). However, the evidence about the association between dietary cholesterol intake and risks of dementia is controversial in either animal or clinical research. For human-based research, a cross-sectional study recruiting 2,892 elderly subjects in China showed that adequate dietary intake of monounsaturated fatty acids and cholesterol was significantly associated with a decreased risk of MCI, a preclinical stage of AD dementia (13). However, the Effects and Mechanism Investigation of Cholesterol and Oxysterol on Alzheimer’s disease (EMCOA) study included 2514 participants who completed a selection of comprehensive cognitive tests and were followed for an average of 2.3 years. Neither cholesterol nor egg intake was associated with a higher risk of accelerated global cognitive decline, but in mixed-effect linear models, quadratic and longitudinal inverse relations of dietary cholesterol and egg intake to global cognition, processing speed, and executive function were observed (24). Furthermore, a prospective population-based cohort study including 2497 dementiafree men (aged 42–60 years) with a 21.9-year follow-up concluded that neither cholesterol nor egg intake is associated with an increased risk of incident dementia or AD in Eastern Finnish men. Instead, moderate egg intake may have a beneficial association with certain areas of cognitive performance (14). In contrast, dietary cholesterol and sodium intake was linked to cognitive impairment in a small sample (12). For basic research, the association between high cholesterol intake and AD-type pathologies has been shown comprehensively. In detail, hypercholesterolemia accelerates amyloid beta-induced cognitive deficits, and a high-cholesterol diet given to Apo lipoprotein E-knockout mice has a differential effect on the various neurotropic systems in the hippocampus (25). The inconsistency of clinical research could also be due to the differences in study design, sociodemographic characteristics of the study population, nonstandard diagnosis, subtype for dementia or only assessment for cognition function, and a lack of enough control for the covariates. The different lipoprotein metabolism of rats, mice, rabbits, and humans could be the explanation for the distinction between animal and human studies for dietary cholesterol and dementia. Against these shortages, our study found that dietary cholesterol was inversely associated with risks of all-cause dementia and AD dementia at a community population level with detailed information about dietary intakes, previously affirmed dementia risk factors and standard surveillance and diagnosis of dementia. Interestingly, this association occurred in the high-intake subgroup but not the medium-intake subgroup, suggesting a nonlinear relationship that deserves further investigation.
Several hypotheses could explain our findings. First, dietary cholesterol has been shown to suppress appetite and decrease plasma ghrelin levels (26). In the healthy hippocampus, the ghrelin/GHSR1α signal affects the learning, motivational, and hedonic components of eating (27). Emerging evidence suggests that the loss of GHSR1α induces AD-like hippocampal synaptic stress and memory deficits, where hippocampal lesions are one of the earliest lesions to appear in AD and affect cognitive function (28). Second, eggs (the main source of dietary cholesterol) were enriched with ovotransferrin, a glycoprotein associated with a category of transferrin iron-binding glycoproteins, which is a risk factor for dementia (29). More specifically, two tripe tides, IRW and IQW, both derived from ovotransferrin hydrolysis, were found to attenuate TNF-α-induced inflammatory responses and oxidative stress in vascular endothelial cells (30). It has been confirmed that oxidative stress and neuroinflammation share molecular mechanisms among all dementia types (31). Finally, the protective effect on neurodegenerative diseases is potentially related to the content of zeaxanthin and lutein, which may be beneficial to cognitive performance across the lifespan. The Third National Health and Nutrition Examination Survey (NHANES III) showed that incident all-cause dementia was inversely associated with serum lutein zeaxanthin and β-cryptoxanthin levels (32). Correspondingly, experimental research indicated that rats with oral zeaxanthin supplementation showed a reduction in the brain levels of inflammatory indicators, viz. interleukin-1β and inducible nitric oxide synthetase as well as brain contents of Aβ protein and myelin base protein (33).
The strengths of our study include its well-characterized community-based large sample size, prospective design, long-term follow-up, detailed information about dietary intakes, accurate diagnosis and subtype of clinical outcomes, and carefully comprehensive adjustment for multiple potential confounders. Of course, our study also has some limitations. First, although we adjusted for several confounders, our results may still be subject to residual confounding due to unrecognized or unmeasured confounders in the public dataset, such as the Apo-E4 phenotype for all participants. Second, our dietary and nutrient intake assessments were based on FFQ data that tend to contain recall biases and are subject to measurement error; hence, future research based on better diet evaluation tools is also warranted. Third, there were small numbers of incident events, raising concerns about selection bias and a lack of statistical power. Fourth, our study cannot establish causal links between dietary intake and all-cause dementia and AD dementia because our analyses were observational. Finally, our results lacked generalizability because essentially all participants of the FOS cohort were white and of European descent. Future studies are necessary to replicate our findings in a more diverse larger-scale prospective study.
Conclusions
High intake of dietary cholesterol was associated with a decreased risk of all-cause dementia and AD dementia. The findings of this observational study need to be confirmed by other studies to highlight the role of dietary cholesterol in the development of neurodegenerative diseases. Our findings support that enough cholesterol intake may be beneficial in reducing dementia burden, which is in accordance with the recommendation of the 2015–2020 US dietary guidelines that eggs are an important part of a healthy diet. However, nonlinear associations were also shown in our study, where the medium intake of dietary cholesterol was not significantly associated with decreased risks for dementia, and the upper limit of dietary cholesterol should be clarified in future studies. Finally, the results of our observational study are prone to residual confounding and require confirmation as well.
Data Sharing Statement: Data described in the manuscript, code book, and analytic code will not be made available because the authors are prohibited from distributing or transferring the data and codebooks on which their research was based to any other individual or entity under the terms of an approved NHLBI Framingham Heart Study Research Proposal and Data and Materials Distribution Agreement through which the authors obtained these data.
References
Collaborators GBDDF (2022) Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health 7, e105–e125. doi: https://doi.org/10.1016/S2468-2667(21)00249-8.
Wu YT, Beiser AS, Breteler MMB, Fratiglioni L, Helmer C, Hendrie HC, Honda H, Ikram MA, Langa KM, Lobo A, Matthews FE, Ohara T, Peres K, Qiu C, Seshadri S, Sjolund BM, Skoog I, Brayne C (2017) The changing prevalence and incidence of dementia over time - current evidence. Nat Rev Neurol 13, 327–339. doi: https://doi.org/10.1038/nrneurol.2017.63.
Silva MVF, Loures CMG, Alves LCV, de Souza LC, Borges KBG, Carvalho MDG (2019) Alzheimer’s disease: risk factors and potentially protective measures. J Biomed Sci 26, 33. doi: https://doi.org/10.1186/s12929-019-0524-y.
Wang K, Liu H (2021) Association between widespread pain and dementia, Alzheimer’s disease and stroke: a cohort study from the Framingham Heart Study. Reg Anesth Pain Med 46, 879–885. doi: https://doi.org/10.1136/rapm-2021-102733.
Zhou S, Wang K (2021) Childhood Secondhand Smoke Exposure and Risk of Dementia, Alzheimer’s Disease and Stroke in Adulthood: A Prospective Cohort Study. J Prev Alzheimers Dis 8, 345–350. doi: https://doi.org/10.14283/jpad.2021.10.
Wang Z, Yang Z, Liu J, Hao Y, Sun B, Wang J (2021) Potential Health Benefits of Whole Grains: Modulation of Mitochondrial Biogenesis and Energy Metabolism. J Agric Food Chem 69, 14065–14074. doi: https://doi.org/10.1021/acs.jafc.1c05527.
Wang K, Liu H (2022) Response to the letter from Barash et al. Reg Anesth Pain Med 47, 270. doi: https://doi.org/10.1136/rapm-2021-103244.
Cha D, Park Y (2019) Association between Dietary Cholesterol and Their Food Sources and Risk for Hypercholesterolemia: The 2012(-)2016 Korea National Health and Nutrition Examination Survey. Nutrients 11. doi: https://doi.org/10.3390/nu11040846.
Greenberg JA, Jiang X, Tinker LF, Snetselaar LG, Saquib N, Shadyab AH (2021) Eggs, dietary cholesterol, choline, betaine, and diabetes risk in the Women’s Health Initiative: a prospective analysis. Am J Clin Nutr 114, 368–377. doi: https://doi.org/10.1093/ajcn/nqab036.
Vincent MJ, Allen B, Palacios OM, Haber LT, Maki KC (2019) Meta-regression analysis of the effects of dietary cholesterol intake on LDL and HDL cholesterol. Am J Clin Nutr 109, 7–16. doi: https://doi.org/10.1093/ajcn/nqy273.
Zingel R, Bohlken J, Riedel-Heller S, Barth S, Kostev K (2021) Association Between Low-Density Lipoprotein Cholesterol Levels, Statin Use, and Dementia in Patients followed in German General Practices. J Alzheimers Dis 79, 37–46. doi: https://doi.org/10.3233/JAD-201176.
Salerno-Kennedy R, Cashman KD (2007) The relationship between nutrient intake and cognitive performance in people at risk of dementia. Ir J Med Sci 176, 193–198. doi: https://doi.org/10.1007/s11845-007-0036-8.
Lu Y, An Y, Guo J, Zhang X, Wang H, Rong H, Xiao R (2016) Dietary Intake of Nutrients and Lifestyle Affect the Risk of Mild Cognitive Impairment in the Chinese Elderly Population: A Cross-Sectional Study. Front Behav Neurosci 10, 229. doi: https://doi.org/10.3389/fnbeh.2016.00229.
Ylilauri MP, Voutilainen S, Lonnroos E, Mursu J, Virtanen HE, Koskinen TT, Salonen JT, Tuomainen TP, Virtanen JK (2017) Association of dietary cholesterol and egg intakes with the risk of incident dementia or Alzheimer disease: the Kuopio Ischaemic Heart Disease Risk Factor Study. Am J Clin Nutr 105, 476–484. doi: https://doi.org/10.3945/ajcn.116.146753.
Shishtar E, Rogers GT, Blumberg JB, Au R, Jacques PF (2020) Long-term dietary flavonoid intake and risk of Alzheimer disease and related dementias in the Framingham Offspring Cohort. Am J Clin Nutr 112, 343–353. doi: https://doi.org/10.1093/ajcn/nqaa079.
Juul F, Vaidean G, Lin Y, Deierlein AL, Parekh N (2021) Ultra-Processed Foods and Incident Cardiovascular Disease in the Framingham Offspring Study. J Am Coll Cardiol 77, 1520–1531. doi: https://doi.org/10.1016/j.jacc.2021.01.047.
Westwood AJ, Beiser A, Jain N, Himali JJ, DeCarli C, Auerbach SH, Pase MP, Seshadri S (2017) Prolonged sleep duration as a marker of early neurodegeneration predicting incident dementia. Neurology 88, 1172–1179. doi: https://doi.org/10.1212/WNL.0000000000003732.
Wang K, Tang W, Hao X, Liu H (2022) High consumption of whole grain foods decreases the risk of dementia and Alzheimer’s disease: Framingham Offspring Cohort. Psychiatry Clin Neurosci. doi: https://doi.org/10.1111/pcn.13509.
McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM (1984) Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 34, 939–944. doi: https://doi.org/10.1212/wnl.34.7.939.
American Psychatric Association.Arlington V (2000) Diagnostic and Statistical Manual of Mental Disorders.4th ed, American Psychiatric Publishing
Mathur MB, Ding P, Riddell CA, VanderWeele TJ (2018) Web Site and R Package for Computing E-values. Epidemiology 29, e45–e47. doi: https://doi.org/10.1097/EDE.0000000000000864.
VanderWeele TJ, Ding P (2017) Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann Intern Med 167, 268–274. doi: https://doi.org/10.7326/M16-2607.
Vu THT, Beck T, Bennett DA, Schneider JA, Hayden KM, Shadyab AH, Rajan KB, Morris MC, Cornelis MC (2022) Adherence to MIND Diet, Genetic Susceptibility, and Incident Dementia in Three US Cohorts. Nutrients 14. doi: https://doi.org/10.3390/nu14132759.
An Y, Zhang X, Wang Y, Wang Y, Liu W, Wang T, Qin Z, Xiao R (2019) Longitudinal and nonlinear relations of dietary and Serum cholesterol in midlife with cognitive decline: results from EMCOA study. Mol Neurodegener 14, 51. doi: https://doi.org/10.1186/s13024-019-0353-1.
Park SH, Kim JH, Choi KH, Jang YJ, Bae SS, Choi BT, Shin HK (2013) Hypercholesterolemia accelerates amyloid beta-induced cognitive deficits. Int J Mol Med 31, 577–582. doi: https://doi.org/10.3892/ijmm.2013.1233.
Ratliff J, Leite JO, de Ogburn R, Puglisi MJ, VanHeest J, Fernandez ML (2010) Consuming eggs for breakfast influences plasma glucose and ghrelin, while reducing energy intake during the next 24 hours in adult men. Nutr Res 30, 96–103. doi: https://doi.org/10.1016/j.nutres.2010.01.002.
Hsu TM, Noble EE, Reiner DJ, Liu CM, Suarez AN, Konanur VR, Hayes MR, Kanoski SE (2018) Hippocampus ghrelin receptor signaling promotes socially-mediated learned food preference. Neuropharmacology 131, 487–496. doi: https://doi.org/10.1016/j.neuropharm.2017.11.039.
Tian J, Guo L, Sui S, Driskill C, Phensy A, Wang Q, Gauba E, Zigman JM, Swerdlow RH, Kroener S, Du H (2019) Disrupted hippocampal growth hormone secretagogue receptor 1alpha interaction with dopamine receptor D1 plays a role in Alzheimer’s disease. Sci Transl Med 11. doi: https://doi.org/10.1126/sdtranslmed.aav6278.
Giansanti F, Leboffe L, Angelucci F, Antonini G (2015) The Nutraceutical Properties of Ovotransferrin and Its Potential Utilization as a Functional Food. Nutrients 7, 9105–9115. doi: https://doi.org/10.3390/nu7115453.
Majumder K, Chakrabarti S, Davidge ST, Wu J (2013) Structure and activity study of egg protein ovotransferrin derived peptides (IRW and IQW) on endothelial inflammatory response and oxidative stress. J Agric Food Chem 61, 2120–2129. doi: https://doi.org/10.1021/jf3046076.
Raz L, Knoefel J, Bhaskar K (2016) The neuropathology and cerebrovascular mechanisms of dementia. J Cereb Blood Flow Metab 36, 172–186. doi: https://doi.org/10.1038/jcbfm.2015.164.
Beydoun MA, Beydoun HA, Fanelli-Kuczmarski MT, Weiss J, Hossain S, Canas JA, Evans MK, Zonderman AB (2022) Association of Serum Antioxidant Vitamins and Carotenoids With Incident Alzheimer Disease and All-Cause Dementia Among US Adults. Neurology 98, e2150–e2162. doi: https://doi.org/10.1212/WNL.0000000000200289.
El-Baz FK, Abdel Jaleel GA, Hussein RA, Saleh DO (2021) Dunalialla salina microalgea and its isolated zeaxanthin mitigate age-related dementia in rats: Modulation of neurotransmission and amyloid-beta protein. Toxicol Rep 8, 1899–1908. doi: https://doi.org/10.1016/j.toxrep.2021.11.021.
Acknowledgments
We want to express our thanks to the FHS participants for their decades of dedication and to the FHS staff for their hard work in collecting and preparing the data. We also thank The People’s Hospital of Chongqing Liang Jiang New Area, Chongqing, China.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures: The authors declare that they have no conflicts of interest.
Ethical Standards: The study procedures followed were in accordance with the ethical standards of the Institutional Review Board and the Principles of the Declaration of Helsinki.
Additional information
Financial Support: None.
Electronic Supplementary Material
42414_2023_225_MOESM1_ESM.docx
High intake of dietary cholesterol decreases the risk of All-cause dementia and Alzheimer’s disease: A results from Framingham Offspring Cohort
Rights and permissions
About this article

Cite this article
Wang, M., Wang, Y., Zhang, Y. et al. High Intake of Dietary Cholesterol Decreases the Risk of All-Cause Dementia and AD Dementia: A Results from Framingham Offspring Cohort. J Prev Alzheimers Dis 10, 748–755 (2023). https://doi.org/10.14283/jpad.2023.59
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.14283/jpad.2023.59