
Abstract
Background
Little is known about how the quality of decisions influences patient-reported outcomes (PROs). We hypothesized that higher decision quality for breast reconstruction would be independently associated with better PROs.
Methods
We conducted a prospective cohort study of patients undergoing mastectomy with or without reconstruction. Patients were enrolled before surgery and followed for 18 months. We used BREAST-Q scales to measure PROs and linear regression models to explore the relationship between decision quality (based on knowledge and preference concordance) and PROs. Final models were adjusted for baseline BREAST-Q score, radiation, chemotherapy, and major complications.
Results
The cohort included 101 patients who completed baseline and 18-month surveys. Breast reconstruction was independently associated with higher satisfaction with breasts (β = 20.2, p = 0.0002), psychosocial well-being (β = 14.4, p = 0.006), and sexual well-being (β = 15.7, p = 0.007), but not physical well-being. Patients who made a high-quality decision had similar PROs as patients who did not. Among patients undergoing mastectomy with reconstruction, higher decision quality was associated with lower psychosocial well-being (β = −14.2, p = 0.01).
Conclusions
Breast reconstruction was associated with better PROs in some but not all domains. Overall, making a high-quality decision was not associated with better PROs. However, patients who did not have reconstruction had a trend toward better well-being after making a high-quality decision, whereas patients who did have reconstruction had poorer well-being after making a high-quality decision. Additional research on the relationship between decision quality and PROs is needed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Greater patient engagement in medical treatments can improve clinical outcomes and satisfaction with care.1,2 Many patients, including those with breast cancer, prefer to be engaged in decisions about their care.3,4,5 In the case of breast reconstruction after mastectomy, making a good decision about whether to have the procedure can be challenging because of the decision’s unfamiliar, deeply personal, and high-stakes nature. Breast reconstruction has the potential to improve quality of life6 but is associated with a relatively high complication risk.7 Many patients have reported decisional regret after reconstruction,8 particularly if they had inadequate information9,10 or experienced a complication.10 Other patients have regretted not having reconstruction, with 67% reporting they were not informed of the option.11,12
The decision about breast reconstruction is considered ‘preference sensitive’, in that the right choice depends on the patient’s treatment goals or preferences. For preference-sensitive decisions, a high-quality decision has been defined as one that is (1) informed and (2) concordant with patient preferences.13 Unfortunately, many patients lack adequate knowledge about the pros and cons of breast reconstruction,14,15,16,17 and some receive treatment inconsistent with their preferences.18,19
Having surgery that is inconsistent with one’s preferences may have consequences for one’s satisfaction later. However, little is known about how decision making about reconstruction influences subsequent satisfaction and quality of life. Although studies have examined decision making or patient-reported outcomes (PROs) of breast reconstruction, few have assessed them together. Furthermore, few studies have compared outcomes with a control group (i.e., patients who had mastectomy alone), assessed baseline patient characteristics, and used validated measures.20
We sought to assess PROs in a prospective cohort of patients undergoing mastectomy with or without reconstruction, with particular interest in whether the quality of decisions was associated with PROs related to well-being. We hypothesized that higher decision quality would be independently associated with better PROs.
Methods
Study Design
We conducted a prospective cohort study of patients undergoing mastectomy with or without reconstruction at a single academic site. We enrolled patients before surgery and followed them for 18 months. The Institutional Review Board approved the study procedures. We have previously reported findings about knowledge, preferences, and accuracy of predictions.16,18,21
Study Population
Adult women planning to have mastectomy for the treatment of stage I–III breast cancer, ductal carcinoma in situ (DCIS), or for prophylaxis were enrolled. However, patients were excluded if they were younger than 21 years of age, planning breast-conserving surgery, had a history of mastectomy with reconstruction, had stage IV breast cancer, had tumors other than ductal or lobular carcinoma, or were not legally competent to make medical decisions due to psychiatric illness (confirmed in the medical record or with the surgical oncology team). Due to cost limitations, the questionnaire was not available in languages other than English; thus, patients who could not read and speak English were not included.
Enrollment
We screened clinic schedules and confirmed eligibility of patients with the surgical oncologist. If a patient was undecided about mastectomy, we followed her clinical course until she made a surgical decision and then approached her for enrollment. Most patients were approached in the clinic immediately after the surgical oncology visit. Some patients who left the clinic before we could approach them were contacted by conventional mail. The mailing included the study description, questionnaire, consent forms, self-addressed and stamped return envelope, and postcard to opt out of further contact. We sought to approach all eligible patients during the 20-month enrollment period. All participants provided written, informed consent.
Data Collection
Participants completed the baseline questionnaire after the surgical oncology visit but before surgery, while they were in clinic or at home. This timing was based on the fact that the study was focusing on the decision about whether or not to have reconstruction (as opposed to the type of reconstruction), which at the study site was generally made during the surgical oncology visit. The surgical oncologist would then refer patients who were interested in reconstruction to the reconstructive surgeon. If we did not receive a patient’s baseline questionnaire, we conducted a reminder call at 2 weeks and a reminder mailing at 4 weeks. Those who completed the baseline survey received a $50 gift card.22 Patients who did not complete the baseline survey before surgery were not included. We mailed follow-up questionnaires at 6, 12, and 18 months after surgery. We again conducted 2-week reminder calls and 4-week reminder mailings. For each completed follow-up survey, participants received a $25 gift card. The gift card amounts were designed to reimburse participants for their time, since the study questionnaires included multiple scales. We abstracted clinical data from medical records, including diagnosis, stage, comorbidities, cancer treatments, and major complications up to 18 months after surgery (defined as unplanned readmission, unplanned reoperation, surgical site infection treated with intravenous antibiotics, venous thromboembolic event, or death).7
Survey Measures
The baseline questionnaire included questions about race, ethnicity, income, education, health insurance status, marital status, personal preferences about reconstruction, knowledge about reconstruction, and PROs. The follow-up questionnaire consisted of only the PRO measures.
To elicit preferences about reconstruction, we asked participants to rate the importance of four treatment attributes, i.e. appearance, complication risk, recovery time, and length of surgery, on a scale from 0 (least important) to 5 (most important). They also ranked the attributes in order of importance. These scales were developed for this study and have been described previously.18,21 Knowledge about reconstruction was assessed using the Decision Quality Instrument–Breast Reconstruction (DQI-BR), a condition-specific, validated measure that contains nine knowledge items. Correctly answering at least half of the items is considered having adequate knowledge to make an informed decision.23,24,25 PROs were measured using BREAST-Q Version 1 scales for satisfaction with breasts, psychosocial well-being, sexual well-being, and physical well-being of the chest.26 Each scale results in a 0–100 score, with higher scores indicating better well-being.
Statistical Analyses
Decision quality was calculated as an index that included knowledge and preference concordance, using an approach that other studies have used.18,27 Specifically, a patient’s decision about breast reconstruction was considered high quality if it met two criteria: (1) the patient’s knowledge score was ≥50% (i.e., she answered at least half of the DQI knowledge questions correctly); and (2) her treatment preference (reconstruction or not) was the same as her treatment received.18,27 The patient’s treatment preference was calculated based on her ratings and rankings of importance, using the approach we have described in detail previously.18 Of note, when calculating preference concordance, we adjusted this analysis of treatment received, to account for radiation limiting some patients’ reconstruction options. At the study site, if postmastectomy radiation was planned, delayed reconstruction was performed. Thus, if a participant had mastectomy only and adjuvant radiation, and her stated treatment preference was mastectomy with reconstruction, we considered her ‘treatment received’ to be mastectomy with reconstruction, assuming she would eventually have delayed reconstruction (erring on the side of preference concordance). We performed this correction based on input from surgeon stakeholders. They did not recommend any other corrections. Otherwise, treatment received was actual treatment (mastectomy only versus mastectomy with reconstruction) within 18 months.
The demographic characteristics of patients having mastectomy only were compared with those of patients having mastectomy with reconstruction, using t-tests for continuous variables and Fisher’s exact tests for categorical variables. Treatment received was defined by whether or not the patient had reconstruction within 18 months of mastectomy. Patients who had reconstruction more than 18 months after mastectomy or who lacked BREAST-Q data at 18 months were excluded from the outcome analysis.
For each PRO, we calculated the mean BREAST-Q value at each time point (baseline and 6, 12, and 18 months) and plotted these to visualize overall treatment-specific trends.
The primary outcome variables were satisfaction with breasts, psychosocial well-being, sexual well-being, and physical well-being of the chest. The study was powered to detect a 10-point difference in BREAST-Q scores.18 To test for association between decision quality and each PRO domain, we performed a univariable model of the 18-month BREAST-Q score as a function of decision quality, adjusting for the baseline score. The baseline score was defined as the score on the baseline questionnaire before mastectomy since this was considered the time point for the decision about whether or not to have reconstruction.
We explored the possibility of a statistical interaction between treatment (mastectomy only versus mastectomy with reconstruction) and decision quality. These analyses were meant to be exploratory because the subgroups were limited in size. Statistical interaction occurs when the effect of one independent variable on the dependent variable depends on the value of a second independent variable. In this study, we were looking at the association between decision quality and PROs. We found that the association did in fact depend on treatment received (p-value for interaction: 0.13 for satisfaction with breasts, 0.01 for psychosocial well-being, 0.02 for sexual well-being, 0.93 for physical well-being of the chest). Because of this interaction, we proceeded with stratified analysis (by treatment received) for all outcomes using linear regression modeling.
For the multivariable model, we fit the same model as above and adjusted for factors known to be associated with PROs of breast reconstruction, including baseline PROs, adjuvant radiation, adjuvant chemotherapy, and major complications.6,28 We did not adjust for additional factors to avoid risk of overadjustment in a limited sample.
Results
Over a 20-month period, we approached 182 eligible women, of whom 145 enrolled. Of the 145, 14 did not complete the baseline survey before surgery and were therefore excluded. Among the patients who had a plastic surgery visit, most completed the survey after that visit. Those completing the survey after the plastic surgery visit had higher knowledge than those completing the survey before the plastic surgery visit, although the difference was not statistically significant.16 Of the 131 participants, 5 became ineligible, leaving a baseline study population of 126, of whom 17 were lost to follow up, 4 died, and 4 did not have complete survey data. This left a study sample of 101 participants who completed the baseline and 18-month surveys (Fig. 1). Those who did not complete the 18-month survey were more likely to have lower knowledge scores compared with the population retained.

Study selection process
The mean age was 52.7 years (Table 1). Around half were college graduates, most had private insurance, 23% were non-White, and 55.4% had immediate or delayed breast reconstruction within 18 months of mastectomy.12 Of patients who had mastectomy with reconstruction (n = 56), 14 had delayed reconstruction. Patients who had mastectomy with reconstruction were more likely to be partnered, have a high income, have private insurance, undergo bilateral mastectomy, have a major complication, or not have adjuvant radiation or chemotherapy. Of the patients who had reconstruction, 68% had alloplastic, 18% had autologous (abdominal), and 14% had combined alloplastic-autologous (latissimus) reconstruction. Fifteen patients who were anticipating delayed reconstruction did not proceed with reconstruction by 18 months. We kept these patients in the reconstruction group, since not all patients who have delayed reconstruction do so before 18 months after mastectomy.
Association Between Breast Reconstruction and Patient-Reported Outcomes (PROs)
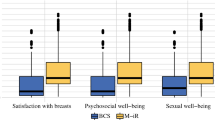
Having breast reconstruction was independently associated with higher satisfaction with breasts (β = 20.2, p = 0.0002), psychosocial well-being (β = 14.4, p = 0.006), and sexual well-being (β = 15.7, p = 0.007) at 18 months compared with mastectomy only. It was not associated with differences in physical well-being (β = 5.5, p = 0.1).
At all follow-up times (6, 12, and 18 months), participants who had reconstruction had higher satisfaction with breasts and sexual well-being compared with women who did not have breast reconstruction (Fig. 2).

(a–d) Patient-reported outcomes over 18 months, by treatment received. Error bars represent 95% confidence intervals
Association Between Decision Quality and PROs
Overall, patients who made a high-quality decision (informed and preference-concordant) had similar PROs as patients who did not make a high-quality decision (Tables 2 and 3). However, some interaction existed between the treatment received (mastectomy only versus mastectomy with reconstruction) and decision quality. Specifically, the association between decision quality and PROs depended somewhat on whether or not the patient had reconstruction. Stratified analysis was performed by treatment group (mastectomy only, Table 2; mastectomy with reconstruction, Table 3). For patients undergoing mastectomy only, there was a trend toward higher decision quality being associated with better PROs, although the results were not statistically significant. For patients undergoing mastectomy with reconstruction, higher decision quality was unrelated to satisfaction with breasts or physical well-being of the chest, showed a trend toward association with poorer sexual well-being, and was associated with poorer psychosocial well-being (β = −14.2, p = 0.01).
Discussion
In this prospective, longitudinal study of patients undergoing mastectomy, having breast reconstruction was associated with better PROs in some domains. The relationship between decision quality and PROs depended on whether the patient had breast reconstruction. Among patients who had mastectomy only, there was a trend toward association between making a high-quality decision and better PROs. Among patients who had mastectomy with reconstruction, making a high-quality decision was associated with poorer psychosocial well-being. This is one of the first longitudinal studies to evaluate the relationship between decision quality and PROs of breast reconstruction.
Breast reconstruction was associated with better satisfaction with breasts, psychosocial well-being, and sexual well-being, but not better physical well-being, a finding consistent with recent large studies of breast reconstruction outcomes. In a multisite cohort study of women undergoing mastectomy with reconstruction, physical well-being of the chest declined from baseline to 1 year after reconstruction, and pain interference and physical well-being of the abdomen worsened after autologous reconstruction.6 Satisfaction with breasts improved from baseline to 1 year after autologous reconstruction, but not after implant reconstruction. In a population-based, cross-sectional survey of women who had breast-conserving surgery or mastectomy, postmastectomy reconstruction was not associated with differences in well-being, but was associated with better cosmetic satisfaction, compared with mastectomy only.28 Other studies have reported mixed results.20,29,30,31,32,33 We interpret that breast reconstruction restores aspects of appearance and satisfaction with breasts but remains a physically challenging procedure with potential for lasting physical morbidity.
This study is unique because it examined whether decision quality about breast reconstruction was associated with better outcomes. We adhered to an international consensus definition of decision quality that emphasizes knowledge and preference concordance and posits that involvement alone is not sufficient.13 Other studies of decision making and outcomes have not assessed decision quality and have instead measured involvement.1,2 For example, one study of lung and colorectal cancer treatment decisions found that patients who reported physician-controlled (versus shared) decision making were less likely to report excellent quality of care.2 A study of primary care practices found that greater patient-centered culture was associated with less depression and better physical functioning.1 Thus, our study is one of the few that has examined decision quality and PROs. Overall, we did not find consistent evidence of an association. We recommend additional research on the relationship between decision quality and PROs.
We found that the relationship between decision quality and PROs depended on whether or not the patient had breast reconstruction. Among patients who had mastectomy only, there was a trend toward association between decision quality and better PROs. It is possible that the small sample (45 patients in this group) limited our ability to detect a significant difference. Among patients who had mastectomy with reconstruction, making a high-quality decision was associated with poorer psychosocial well-being and had a trend toward association with poorer sexual well-being. It is possible that women who chose reconstruction were more critical of their appearance in general, or that they had higher expectations than women who chose mastectomy without reconstruction, although we partly accounted for this by adjusting for baseline BREAST-Q scores. Future research using the BREAST-Q Expectations module, which was not available at the time our study, could examine this further. Another possibility is residual unmeasured confounding, i.e. that some other factor is associated with both decision quality and well-being. For example, some emotions and personality traits could be associated with greater knowledge or with making a preference-concordant decision (or both) if they motivate a person to seek more information or to assert their preferences more strongly. Future studies should examine the role of emotions and personality in decision making about surgical treatments. Finally, another possibility is that differences in PROs associated with decision quality were too small to be detected by the BREAST-Q, which was designed to detect differences and changes due to surgery.
We are uncertain why decision quality was more important, in terms of its association with well-being, for women undergoing mastectomy only than for women undergoing mastectomy with reconstruction. It is possible that some unmeasured confounding explains the difference. For example, strong social support, spiritual health, or having a highly supportive partner could be factors associated with both decision making and psychosocial well-being among women who have mastectomy without reconstruction, and we did not measure these. Type of reconstruction may play a role in how decision making affects PROs. We did not examine this possibility due to the limited sample size. We are also uncertain why making a high-quality decision was associated with lower psychosocial well-being among women who had reconstruction. Future studies could explore this in greater depth by interviewing these patients.
Our findings highlight the importance of two methodological characteristics that are often lacking—measuring preoperative PROs and assessing outcomes at consistent times for all patients. Preoperative satisfaction with breasts, psychosocial well-being, sexual well-being, and physical well-being were associated with 18-month satisfaction with breasts, psychosocial well-being, sexual well-being, and physical well-being, respectively. This will likely not surprise many reconstructive surgeons, who are accustomed to counseling patients that breast reconstruction does not ‘fix’ preoperative physical or psychological issues. Going forward, studies of PROs of breast reconstruction should measure and adjust for baseline characteristics.33 For both the mastectomy only and mastectomy with reconstruction groups, all PROs declined at 6 months and then increased. This finding illustrates the importance of measuring outcomes beyond 6 months, when patients may still be undergoing or recovering from adjuvant treatments and secondary reconstruction procedures. It also highlights the importance of measuring outcomes at the same time point in all study participants, rather than when they happen to return to clinic, for example.
Our findings should be considered in the context of the study’s limitations and strengths. It was conducted at a single, academic site, the rate of reconstruction was higher than the national average, and it only included patients who could read and speak English, therefore generalizability may be limited.12 The study population was similar to that of other studies, in terms of factors associated with reconstruction, namely income, insurance, stage, adjuvant therapy, and bilateral mastectomy.34,35,36 The multivariable models adjusted for baseline BREAST-Q scores, adjuvant chemotherapy, adjuvant radiation therapy, and major complications. However, the sample was relatively small, therefore the ability to detect small differences after multivariable adjustment was limited and some important variables such as type of reconstruction could not be included. Although the subgroup analyses (by reconstruction or not) were small, they were meant to be exploratory.
We did not measure the number of stages of reconstruction and may have underestimated the benefits of completing reconstruction. Since outcomes and complication events are less stable beyond 18 months for implant reconstruction than for autologous reconstruction, our findings may not be equally applicable to both reconstruction types. We did not account for wound complications managed in the outpatient setting, which may influence PROs. Some patients who had a reconstructive surgery visit completed the questionnaire before that visit, therefore their knowledge about reconstruction prior to surgery may have been higher than what we measured. However, we have previously reported that knowledge among patients who saw a plastic surgeon before completing the questionnaire was only slightly higher than knowledge among patients who had not seen a plastic surgeon, and the difference was not statistically significant.16 Finally, we included patients who were having mastectomy for prophylaxis only (12.9%). Their decision making about breast reconstruction may differ from patients with breast malignancy, who likely experience greater urgency and stress before surgery. Their outcomes are also likely different from patients receiving systemic and/or radiation therapy.
The study had several strengths, including adjustment for preoperative PROs, inclusion of a control group of patients who did not have reconstruction, use of validated measures, and longitudinal study design with minimal loss to follow up. We recommend future studies with a similar design but larger samples and multiple sites. A larger sample would have afforded higher-powered subgroup analyses and adjustment for more potential confounders, such as type of reconstruction. Future research examining the role of patient expectations in decision quality would also be valuable.
Our findings have implications for clinical care and future research. We recommend that surgeons counsel patients about the advantages and disadvantages of breast reconstruction so that patients can make an informed decision based on their personal preferences. The advantages include possible restoration of more psychological outcomes, such as satisfaction with breasts, psychosocial well-being, and sexual well-being; however, a disadvantage is that it may not restore physical well-being. They could also remind patients that their well-being before surgery is associated with their well-being after surgery, i.e. the procedure itself is not the only determinant of postoperative outcomes; and that well-being tends to decline from baseline over the first 6 months postoperatively before it improves. Future research should prioritize measurement of baseline PROs. Qualitative research could help clarify some of our surprising findings, especially why higher decision quality was associated with poorer psychosocial well-being among patients having reconstruction. The general question of how decision quality relates to well-being after surgery remains unclear and would benefit from larger, longitudinal studies.
Conclusion
Breast reconstruction after mastectomy was associated with higher satisfaction with breasts, psychosocial well-being, and sexual well-being, but not with differences in physical well-being. Making a high-quality decision was not associated with PROs, although the relationship depended on whether or not the patient had breast reconstruction. Patients who did not have reconstruction had a trend toward better well-being after making a high-quality decision. Patients who did have reconstruction had poorer well-being after making a high-quality decision. Future research employing qualitative methods and larger, longitudinal designs would be valuable to further understand how decision quality relates to PROs of surgery.
References
Shortell SM, Poon BY, Ramsay PP, et al. A multilevel analysis of patient engagement and patient-reported outcomes in primary care practices of accountable care organizations. J Gen Intern Med. 2017;32(6):640–7.
Kehl KL, Landrum MB, Arora NK, et al. Association of actual and preferred decision roles with patient-reported quality of care: shared decision making in cancer care. JAMA Oncol. 2015;1(1):50–8.
Degner LF, Sloan JA. Decision making during serious illness: what role do patients really want to play? J Clin Epidemiol. 1992;45(9):941–50.
Keating N, Guadagnoli E, Landrum M, Borbas C, Weeks J. Treatment decision making in early-stage breast cancer: should surgeons match patients’ desired level of involvement? J Clin Oncol. 2002;20(6):1473–9.
Hawley ST, Lantz PM, Janz NK, et al. Factors associated with patient involvement in surgical treatment decision making for breast cancer. Patient Educ Couns. 2007;65(3):387–95.
Pusic AL, Matros E, Fine N, et al. Patient-reported outcomes 1 year after immediate breast reconstruction: results of the mastectomy reconstruction outcomes consortium study. J Clin Oncol. 2017;35(22):2499–506.
Berlin NL, Tandon VJ, Qi J, et al. Hospital variations in clinical complications and patient-reported outcomes at 2 years after immediate breast reconstruction. Ann Surg. 2019;269(5):959–65.
Sheehan J, Sherman KA, Lam T, Boyages J. Regret associated with the decision for breast reconstruction: the association of negative body image, distress and surgery characteristics with decision regret. Psychol Health. 2008;23(2):207–19.
Sherman KA, Shaw LK, Winch CJ, et al. Reducing decisional conflict and enhancing satisfaction with information among women considering breast reconstruction following mastectomy: results from the BRECONDA randomized controlled trial. Plast Reconstr Surg. 2016;138(4):592e–602e.
Zhong T, Hu J, Bagher S, et al. Decision regret following breast reconstruction: the role of self-efficacy and satisfaction with information in the preoperative period. Plast Reconstr Surg. 2013;132(5):724e–34e.
Alderman AK, Hawley ST, Waljee J, Mujahid M, Morrow M, Katz SJ. Understanding the impact of breast reconstruction on the surgical decision-making process for breast cancer. Cancer. 2008;112(3):489–94.
Morrow M, Li Y, Alderman AK, et al. Access to breast reconstruction after mastectomy and patient perspectives on reconstruction decision making. JAMA Surg. 2014;149(10):1015–21.
Elwyn G, O’Connor A, Stacey D, et al. Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. BMJ. 2006;333(7565):417.
Sepucha K BJ, Chang Y, Cosenza C, Levin C, Moy B, Partridge A, Lee CN. Validation of knowledge measures for breast cancer treatment decisions [poster]. In: Presented at the 31st Annual Meeting of the Society for Medical Decision Making. (2009) Los Angeles, CA.
Lee CN, Belkora J, Chang Y, Moy B, Partridge A, Sepucha K. Are Patients making high-quality decisions about breast reconstruction after mastectomy? Plast Reconstr Surg. 2011;127(1):18–26.
Lee CN, Ubel PA, Deal AM, et al. How informed is the decision about breast reconstruction after mastectomy? A prospective. Cross-Sect Study Ann Surg. 2016;264(6):1103–9.
Sun CS, Reece GP, Crosby MA, et al. Plastic surgeon expertise in predicting breast reconstruction outcomes for patient decision analysis. Plast Reconstr Surg Glob Open. 2013;1(6):e78.
Lee CN, Deal AM, Huh R, et al. Quality of patient decisions about breast reconstruction after mastectomy. JAMA Surg. 2017;152(8):741–8.
Hasak JM, Myckatyn TM, Grabinski VF, Philpott SE, Parikh RP, Politi MC. Stakeholders’ perspectives on Postmastectomy breast reconstruction: recognizing ways to improve shared decision making. Plast Reconstr Surg Glob Open. 2017;5(11):e1569.
Lee CN, Chang Y, Adimorah N, et al. Decision making about surgery for early-stage breast cancer. J Am Coll Surg. 2012;214(1):1–10.
Lee CN, Pignone MP, Deal AM, et al. Accuracy of predictions of patients with breast cancer of future well-being after immediate breast reconstruction. JAMA Surg. 2018;153(4):e176112.
Dillman D. Mail and Telephone Surveys: The Tailored Design Method. 2nd edition: Wiley (1999)
Lee CN, Wetschler MH, Chang Y, et al. Measuring decision quality: psychometric evaluation of a new instrument for breast cancer chemotherapy. BMC Med Inform Decis Mak. 2014;14:73.
Lee CN, Dominik R, Levin CA, Barry MJ, Cosenza C, O’Connor AM, et al. Development of instruments to measure the quality of breast cancer treatment decisions. Health Expectations. 2010;13(3):258–72.
Sepucha KR, Belkora JK, Chang Y, et al. Measuring decision quality: psychometric evaluation of a new instrument for breast cancer surgery. BMC Med Inform Decis Mak. 2012;12:51.
Pusic AL, Klassen AF, Scott AM, Klok JA, Cordeiro PG, Cano SJ. Development of a new patient-reported outcome measure for breast surgery: the BREAST-Q. Plast Reconstr Surg. 2009;124(2):345–53.
McCaffery KJ, Smith SK, Wolf M. The challenge of shared decision making among patients with lower literacy: a framework for research and development. Medical Decision Making. 2010;30(1):35–44.
Jagsi R, Li Y, Morrow M, et al. Patient-reported quality of life and satisfaction with cosmetic outcomes after breast conservation and mastectomy with and without reconstruction: results of a survey of breast cancer survivors. Ann Surg. 2015;261(6):1198–206.
Metcalfe KA, Semple J, Quan ML, et al. Changes in psychosocial functioning 1 year after mastectomy alone, delayed breast reconstruction, or immediate breast reconstruction. Ann Surg Oncol. 2012;19(1):233–41.
Harcourt DM, Rumsey NJ, Ambler NR, et al. The psychological effect of mastectomy with or without breast reconstruction: a prospective, multicenter study. Plast Reconstr Surg. 2003;111(3):1060–8.
Chao LF, Patel KM, Chen SC, et al. Monitoring patient-centered outcomes through the progression of breast reconstruction: a multicentered prospective longitudinal evaluation. Breast Cancer Res Treat. 2014;146(2):299–308.
Pinell-White XA, Duggal C, Metcalfe D, Sackeyfio R, Hart AM, Losken A. Patient-reported quality of life after breast reconstruction: a one-year longitudinal study using the WHO-QOL survey. Ann Plast Surg. 2015;75(2):144–8.
Lee C, Sunu C, Pignone M. Patient-reported outcomes of breast reconstruction after mastectomy: a systematic review. J Am Coll Surg. 2009;209(1):123–33.
Morrow M, Mujahid M, Lantz PM, et al. Correlates of breast reconstruction: results from a population-based study. Cancer. 2005;104(11):2340–6.
Joslyn SA. Patterns of care for immediate and early delayed breast reconstruction following mastectomy. Plast Reconstr Surg. 2005;115(5):1289–96.
Greenberg CC, Schneider EC, Lipsitz SR, et al. Do variations in provider discussions explain socioeconomic disparities in postmastectomy breast reconstruction? J Am Coll Surg. 2008;206(4):605–15.
Funding
This work was supported by a National Institutes of Health 1K07CA154850-01A1 Cancer Prevention, Control, Behavioral, and Population Sciences Career Development Award (National Cancer Institute); Lineberger Comprehensive Cancer Center Population Sciences Cancer Research Award; and North Carolina Translational and Clinical Sciences Institute Pilot Award.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
DISCLOSURE
Shibani R. Chettri, Michael P. Pignone, Allison M. Deal, Karen R. Sepucha, Lillian B. Blizard, Ruth Huh, Yuen-Jong Liu, Peter A. Ubel, and Clara N. Lee declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chettri, S.R., Pignone, M.P., Deal, A.M. et al. Patient-Reported Outcomes of Breast Reconstruction: Does the Quality of Decisions Matter?. Ann Surg Oncol 30, 1891–1900 (2023). https://doi.org/10.1245/s10434-022-12785-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-12785-6