
Abstract
Background
The prognostic factors for duodenal carcinoma (DC) remain unclear because of its rarity. This study aimed to investigate the prognostic impact of pancreatic invasion (PI) on postoperative survival for patients with DC.
Methods
This study retrospectively analyzed 86 patients with DC, including 18 patients with PI, who underwent surgical resection between October 2002 and March 2018. The clinicopathologic features and survival outcomes of these patients were investigated to identify the prognostic factors in DC. The long-term survival for the DC patients with PI was compared with that for the patients who underwent resection for resectable pancreatic head carcinoma (RPHC) during the same period.
Results
The median survival time (MST) for the DC patients with PI was 25.7 months, which was significantly worse than for the patients with T2 or deeper DC without PI (p = 0.010). The multivariate analysis showed that the independent prognostic factors were PI (hazard ratio [HR] 7.59; p = 0.019) and lymph node metastasis (LNM) (HR 5.01; p = 0.026). The MST for the DC patients with PI did not differ significantly from that for the RPHC patients treated without adjuvant chemotherapy (p = 0.135). Comparable rates of microscopic venous invasion and hematogenous metastasis were observed for the DC patients with PI and the RPHC patients.
Conclusions
Pancreatic invasion was an independent prognostic factor in DC. The survival outcomes for the DC patients with PI did not differ from those for the patients with RPHC, which was associated with a high rate of hematogenous recurrence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Duodenal carcinoma (DC), except for ampullary carcinoma, is the most common carcinoma originating from the small intestine and accounts for about 50% of the small intestinal carcinoma cases.1 Although the incidence of DC has been increasing in recent years,2 it remains an uncommon tumor, accounting for less than 1% of all gastrointestinal malignancies.3
Surgical resection is the only potentially curative treatment for DC,4 but the survival outcome has been undesirable.5,6 An association between various pathologic factors and survival has been unclarified,5,7,8 and strong evidence supporting the utility of adjuvant chemotherapy (ACT) remains elusive due to the rarity of DC.8,9
Some previous studies have investigated both the relative survival and histopathologic features of periampullary malignancies.10,11 Pancreatic carcinoma has the worst survival due to its higher incidences of lymphovascular and perineural invasion.12 In ampulla of Vater carcinoma and distal bile duct carcinoma, the association between pancreatic invasion (PI) and the poor survival outcome has been reported.13,14 The duodenum also anatomically contacts to the pancreas, and DC with PI classified as the T4 category according to the tumor-node metastasis (TNM) classification.15 However, few reports have described the influence of PI on survival in DC,16 and the prognostic impact of PI has not been fully investigated in DC patients.
In the current study, a retrospective evaluation of the clinicopathologic features and long-term outcomes of DC patients after resection was performed to investigate the prognostic impact of PI. In addition, the survival outcome for DC patients with PI were compared with those for patients with pancreatic carcinoma.
Methods
Patients
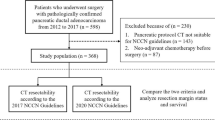
A retrospective review was performed using a prospectively collected database of 90 patients who underwent surgical resection for non-ampullary DC between October 2002 and March 2018 at the Shizuoka Cancer Center. The study excluded two of these patients with concomitant other advanced cancers (1 patient who underwent preoperative chemotherapy and 1 patient who underwent an emergency operation). The remaining 86 patients were selected for the analyses. The current study was approved by the institutional review board of the Shizuoka Cancer Center (no. 2312), and the need for patient consent was waived due to the retrospective nature of the study.
Preoperative Evaluation and Surgical Procedures
The preoperative assessment for DC to determine tumor status and resectability was performed via upper gastrointestinal endoscopy, endoscopic ultrasonography, and computed tomography (CT). The surgical procedures depended mainly on preoperative evaluation of the tumor depth. Partial resection (PR) of the duodenum (including wedge or segmental resection) or pancreas-sparing duodenectomy (PSD) without lymphadenectomy was performed for cases of cTis-cT1a DC, which were ineligible for endoscopic resection. Pancreaticoduodenectomy (PD) with regional lymphadenectomy was generally performed for cases of cT1b or deeper DC.17
Histopathologic Evaluation
All specimens were prepared in the usual manner for a microscopic examination with hematoxylin–eosin staining. The pathologic diagnosis was confirmed by an experienced pathologist (K.S) and classified according to the Union for International Cancer Control (UICC) TNM classification (8th ed).15 The tumor size, histologic grade, lymphovascular invasion, PI, and lymph node metastasis (LNM) were reported.
Follow-up and Definition of Recurrence
During the study period, ACT for DC after surgery generally was not performed because the role of adjuvant chemotherapy remains controversial due to conflicting results across a number of retrospective analyses, according to the National Comprehensive Cancer Network (NCCN) guidelines.18 Follow-up examinations, including laboratory tests, tumor markers, and CT, were performed at 3- to 6-month intervals. Tumor recurrence was confirmed based on the radiologic findings or histologic evidence, and the initial recurrence sites were recorded. Patients with recurrent disease underwent systemic chemotherapy if appropriate.
Comparisons of Survival Between DC and Resectable Pancreatic Head Carcinoma (RPHC)
The survival outcomes were compared between DC patients and RPHC patients managed without neoadjuvant chemotherapy who underwent PD during the same period at the Shizuoka Cancer Center. The resectability status for pancreatic carcinoma was defined by the criteria of the NCCN.19 Generally, ACT for RPHC was performed as described in our previous report.20
Statistical Analysis
All continuous variables were expressed as medians and ranges. Fisher’s exact test was used for comparisons between categorical variables. The Mann–Whitney U test was used for comparisons between continuous variables. The overall survival (OS) and relapse-free survival (RFS) rates were analyzed using the Kaplan–Meier method, and the log-rank test was used to evaluate statistical significance. The cutoff values for continuous variables, except for tumor markers, were determined based on the minimum p value approach. The cutoff values for carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19-9 levels were decided by the upper limit of the institutional standard levels (CEA > 5.0 ng/mL, CA19-9 > 37 U/mL). Variables with a p value lower than 0.05 in the univariate analysis were included in a multivariate Cox proportional hazards regression analysis to identify independent risk factors for OS. A p value lower than 0.05 was considered to be statistically significant. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan).21
Results
Clinicopathologic Features of the Patients
Table 1 shows the clinicopathologic characteristics of the 86 patients with DC. Regarding the surgical procedures, 46 patients (53%) underwent PD, 29 (34%) underwent PR, 10 (12%) underwent PSD, and 1 (1%) underwent distal gastrectomy. Of the 55 patients with pT1 disease, 7 had pT1b tumors. Three of these patients underwent PR or PSD without lymphadenectomy, and none experienced recurrence. All 31 patients with pT2 or deeper tumors underwent PD. Four of the five patients with M1 disease had distant LNM, and the remaining patient had localized peritoneal dissemination. All the patients with M1 disease except for peritoneal dissemination underwent macroscopic curative resection.
Survival Outcomes and Prognostic Factors
The median follow-up period was 58.7 months (range 1.1–156.3 months) for the censored cases. Figure 1 shows the OS and RFS rates for the DC patients according to their pT classification. The 5-year OS rate was 100% for the patients with pT1, 100% for those with pT2/3, and 26.1% for those with pT4. The 5-year RFS rate was 100% for the patients with pT1, 78.7% for those with pT2/3, and 28.0% for those with pT4.

a Overall survival curves for a 10-year period for 86 patients with duodenal carcinoma according to their pT classification. b Relapse-free survival curves for 85 patients, excluding 1 patient with peritoneal dissemination, according to their pT classification
In the RFS analysis, the one patient with peritoneal dissemination was excluded. Figure 2a shows the influence of PI on the OS rates among the 31 patients who underwent PD for pT2 or deeper DC (including 2 patients with pT2, 8 patients with pT3, and 21 patients with pT4 disease). Among the patients with pT4 DC, 18 had PI, 2 had invasion to the mesentery, and 1 had invasion to the transverse colon. Figure 2b shows the influence of PI on the RFS rates among 30 patients, excluding one with peritoneal dissemination. The median OS (25.7 months) and RFS (8.5 months) for the patients with PI were significantly worse than for the patients without PI (OS, p = 0.010; RFS, p = 0.005).

a Overall survival curves for a 5-year period for 31 patients who underwent pancreaticoduodenectomy for pT2 or deeper duodenal carcinoma (DC), according to pancreatic invasion (PI). b Relapse-free survival curves for 30 patients, excluding 1 patient with peritoneal dissemination, according to PI
Table 2 shows the results of uni- and multi-variate analyses to identify the prognostic factors for the OS for the 86 DC patients. The univariate analysis showed that the CEA level, CA19-9 level, tumor differentiation, tumor size, lymphovascular invasion, PI, and LNM were significantly associated with the OS. The multivariate analysis using these seven variables identified PI (hazard ratio [HR] 7.59; p = 0.019) and LNM (HR 5.01; p = 0.026) as independent prognostic factors.
Comparisons of Survival Outcomes Between the DC Patients with PI and the RPHC Patients
The survival outcomes for the 18 PI patients were compared with those for the 353 RPHC patients who underwent PD. The survival for the RPHC patients was subdivided according to the presence ACT. At our institution, ACT was started in 2006, and the rate for the patients who have undergone ACT since then is 67%. The median OS and RFS in the DC group with PI did not differ significantly from those in the RPHC group without ACT (median OS, 25.7 vs. 16.4 months, p = 0.135; median RFS, 8.5 vs. 7.1 months, p = 0.501) (Fig. 3). The median OS and RFS in the RPHC group with ACT were significantly better than those in the RPHC group without ACT (OS, p < 0.001; RFS, p < 0.001).

Kaplan–Meier survival curves for a 5-year period for duodenal carcinoma (DC) patients with pancreatic invasion (PI), and for resectable pancreatic head carcinoma (RPHC) patients who underwent pancreaticoduodenectomy, according to adjuvant chemotherapy (ACT). a Overall survival (OS) curves. b Relapse-free survival (RFS) curves. RPHC (A), RPHC with ACT; RPHC (N), RPHC without ACT
Table 3 compares the pathologic features and recurrence patterns between the 31 patients with pT2 or deeper DC (with or without PI) and the 141 RPHC patients without ACT. Chemotherapy for recurrent disease was performed for 10 of 16 patients with recurrent DC and 51 of 114 patients with recurrent RPHC. The rate of microscopic venous invasion (MVI) tended to be higher in the DC group with PI than in the DC group without PI (67% vs. 31%; p = 0.073). The frequency of hematogenous metastasis (including liver, lung, and uterus metastasis) was significantly higher in the DC group with PI than in the DC group without PI (56% vs. 15%; p = 0.025). These rates were comparable between the DC group with PI and the RPHC group.
Discussion
The current study aimed to investigate the prognostic factors of DC, with a focus on PI, which is caused by the anatomic features of the duodenum. The results showed that PI and LNM were independent prognostic factors for patients with DC after surgery. Reports show LNM to be an acceptable predictor of a poor survival,4,5,7 but the prognostic impact of PI on survival has not been fully investigated for DC patients. The OS and RFS in the DC group with PI were significantly worse than in the DC group without PI. In addition, the OS and RFS in the DC group with PI did not differ significantly from those in the RPHC group. The rates of MVI and hematogenous metastasis were comparable between the two groups. The current study reported a critical survival effect of PI for the patients with surgically resected DC, which may be associated with systemic recurrence of the disease.
Among periampullary malignancies, PI is reported to be a prognostic factor in ampulla of Vater carcinoma and distal bile duct carcinoma.13,14 In contrast, one previous report suggested a relationship between PI and survival in DC, but that study analyzed macroscopic PI, not pathologic PI, and a multivariate analysis for prognostic factors was not performed.16
In the current study, the DC group with PI showed high rates of hematogenous recurrence and MVI. Reports show MVI as a prognostic factor in other carcinomas including gastric, colorectal, and pancreatic carcinomas,22,23,24 and MVI as significantly associated with recurrence of hematogenous metastasis.24,25,26
The relationship between MVI and hematogenous metastasis may be due to the presence of circulating tumor cells (CTC). Recently, CTC was widely accepted as a prognostic factor in gastric, colorectal, and pancreatic carcinomas.27,28,29 The relationship between MVI and CTC was reported in colorectal carcinoma.28 The poor survival outcomes in the DC group with PI may have resulted in high rates of MVI and hematogenous metastasis, suggesting the possibility of coherence with CTC.
Among the common periampullary malignancies (pancreatic carcinoma, distal bile duct carcinoma, ampulla of Vater carcinoma, and DC), the OS in resected DC is reported to be better than in other resected carcinomas.6,30 In addition, the superior survivals in resected DC have been similar in all stages (stages 1–4).30 However, in the current study, the survival outcome in DC with PI was similar to that in RPHC, which was reported to have the worst survival outcome among periampullary carcinomas.6,30
Pancreatic carcinoma is one of the most lethal types of malignancy,31 and the rate of distant recurrence has been high even after curative resection.32 The prognosis of pancreatic carcinoma treated with surgical resection alone has been extremely poor, which prompted research into ACT and its introduction.33,34 Surgery alone seems to be an inadequate approach for achieving a long-term survival for DC patients with PI considering the poor survival outcomes, which may suggest the utility of ACT, as observed in pancreatic carcinoma. The indication for ACT has been established for other gastrointestinal tumors, such as gastric carcinoma and colorectal carcinoma.35,36 Although the efficacy of ACT to improve survival for DC patients has been controversial,8,9 its efficacy for small bowel carcinoma has been reported in a retrospective study using a large cohort from the cancer registry.37 An ongoing randomized phase 3 trial of ACT for patients with small bowel carcinoma may lead to the advancement of multidisciplinary treatment for DC patients.38
The limitations associated with the current study include its retrospective nature and single-institution setting with a limited number of patients, the latter of which was unavoidable because DC is a very rare disease. The survival impacts of T factors other than PI were not fully investigated because the T2 and T3 disease rates were low. The overall rate of LNM was low for the same reason. The depth of pancreatic DC invasion was not pathologically measured in the current study, which is included in pT classification of ampulla of Vater carcinoma.13 The DC and RPHC patients differed in extent of lymphadenectomy and dissection of retroperitoneal tissue. A large-scale multicenter investigation is required to prove the association between PI and survival.
In conclusion, PI was a critical prognostic factor for the patients with DC after surgery. The survival outcomes for the DC group with PI did not differ significantly from those for the patients with RPHC, which was associated with a high rate of hematogenous recurrence.
References
Overman MJ, Hu CY, Kopetz S, Abbruzzese JL, Wolff RA, Chang GJ. A population-based comparison of adenocarcinoma of the large and small intestine: insights into a rare disease. Ann Surg Oncol. 2012;19:1439–45.
Lu Y, Frobom R, Lagergren J. Incidence patterns of small bowel cancer in a population-based study in Sweden: increase in duodenal adenocarcinoma. Cancer Epidemiol. 2012;36:e158–63.
Cloyd JM, Norton JA, Visser BC, Poultsides GA. Does the extent of resection impact survival for duodenal adenocarcinoma? Analysis of 1611 cases. Ann Surg Oncol. 2015;22:573–80.
Kaklamanos IG, Bathe OF, Franceschi D, Camarda C, Levi J, Livingstone AS. Extent of resection in the management of duodenal adenocarcinoma. Am J Surg. 2000;179:37–41.
Poultsides GA, Huang LC, Cameron JL, et al. Duodenal adenocarcinoma: clinicopathologic analysis and implications for treatment. Ann Surg Oncol. 2012;19:1928–35.
He J, Ahuja N, Makary MA, et al. 2564 resected periampullary adenocarcinomas at a single institution: trends over three decades. HPB Oxford. 2014;16:83–90.
Solaini L, Jamieson NB, Metcalfe M, et al. Outcome after surgical resection for duodenal adenocarcinoma in the UK. Br J Surg. 2015;102:676–81.
Meijer LL, Alberga AJ, de Bakker JK, et al. Outcomes and treatment options for duodenal adenocarcinoma: a systematic review and meta-analysis. Ann Surg Oncol. 2018;25:2681–92.
Khan K, Peckitt C, Sclafani F, et al. Prognostic factors and treatment outcomes in patients with small bowel adenocarcinoma (SBA): the Royal Marsden Hospital (RMH) experience. BMC Cancer. 2015;15:15.
van Roest MH, Gouw AS, Peeters PM, et al. Results of pancreaticoduodenectomy in patients with periampullary adenocarcinoma: perineural growth more important prognostic factor than tumor localization. Ann Surg. 2008;248:97–103.
Chandrasegaram MD, Chiam SC, Chen JW, et al. Distribution and pathological features of pancreatic, ampullary, biliary, and duodenal cancers resected with pancreaticoduodenectomy. World J Surg Oncol. 2015;13:85.
Hatzaras I, George N, Muscarella P, Melvin WS, Ellison EC, Bloomston M. Predictors of survival in periampullary cancers following pancreaticoduodenectomy. Ann Surg Oncol. 2010;17:991–7.
Imamura T, Yamamoto Y, Sugiura T, et al. The prognostic relevance of the new 8th edition of the Union for International Cancer Control Classification of TNM Staging for Ampulla of Vater Carcinoma. Ann Surg Oncol. 2019;26:1639–48.
Ebata T, Nagino M, Nishio H, Igami T, Yokoyama Y, Nimura Y. Pancreatic and duodenal invasion in distal bile duct cancer: paradox in the tumor classification of the American Joint Committee on Cancer. World J Surg. 2007;31:2008–15.
Brierley JD, Gospodarowicz M, Wittekind C. UICC TNM classification of malignant tumours. 8th ed. New York: Wiley-Blackwell; 2016.
Ohigashi H, Ishikawa O, Tamura S, et al. Pancreatic invasion as the prognostic indicator of duodenal adenocarcinoma treated by pancreatoduodenectomy plus extended lymphadenectomy. Surgery. 1998;124:510–15.
Kohga A, Yamamoto Y, Sano S, et al. Surgical strategy for T1 duodenal or ampullary carcinoma according to the depth of tumor invasion. Anticancer Res. 2017;37:5277–83.
Benson AB, Venook AP, Al-Hawary MM, et al. Small bowel adenocarcinoma, version 1.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17:1109–33.
NCCN Clinical Practice Guidelines in Oncology. Pancreatic Adenocarcinoma, Version 2.2018, 10 July 2018. Retrieved 29 September 2019 at https://www2.tri-kobe.org/nccn/guideline/pancreas/english/pancreatic.pdf.
Ohgi K, Yamamoto Y, Sugiura T, et al. Is pancreatic head cancer with portal venous involvement really borderline resectable? Appraisal of an upfront surgery series. Ann Surg Oncol. 2017;24:2752–61.
Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013;48:452–8.
Araki I, Hosoda K, Yamashita K, et al. Prognostic impact of venous invasion in stage IB node-negative gastric cancer. Gastric Cancer. 2015;18:297–305.
Shinto E, Tsuda H, Ueno H, Shimazaki H, Yamamoto J, Hase K. Prognostic value of the number and size of venous invasions in pT3 colorectal cancer: a prospective observational study. World J Surg. 2014;38:3257–64.
Yamada M, Sugiura T, Okamura Y, et al. Microscopic venous invasion in pancreatic cancer. Ann Surg Oncol. 2018;25:1043–51.
Nishibeppu K, Komatsu S, Ichikawa D, et al. Venous invasion as a risk factor for recurrence after gastrectomy followed by chemotherapy for stage III gastric cancer. BMC Cancer. 2018;18:108.
Dirschmid K, Sterlacci W, Oellig F, et al. Absence of extramural venous invasion is an excellent predictor of metastasis-free survival in colorectal carcinoma stage II: a study using tangential tissue sectioning. J Clin Pathol. 2012;65:619–23.
Okabe H, Tsunoda S, Hosogi H, et al. Circulating tumor cells as an independent predictor of survival in advanced gastric cancer. Ann Surg Oncol. 2015;22:3954–61.
Iinuma H, Okinaga K, Egami H, et al. Usefulness and clinical significance of quantitative real-time RT-PCR to detect isolated tumor cells in the peripheral blood and tumor drainage blood of patients with colorectal cancer. Int J Oncol. 2006;28:297–306.
Pietrasz D, Pecuchet N, Garlan F, et al. Plasma circulating tumor DNA in pancreatic cancer patients is a prognostic marker. Clin Cancer Res. 2017;23:116–23.
Hester CA, Dogeas E, Augustine MM, et al. Incidence and comparative outcomes of periampullary cancer: a population-based analysis demonstrating improved outcomes and increased use of adjuvant therapy from 2004 to 2012. J Surg Oncol. 2019;119:303–17.
Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–49.
Groot VP, Rezaee N, Wu W, et al. Patterns, timing, and predictors of recurrence following pancreatectomy for pancreatic ductal adenocarcinoma. Ann Surg. 2018;267:936–45.
Uesaka K, Boku N, Fukutomi A, et al. Adjuvant chemotherapy of S-1 versus gemcitabine for resected pancreatic cancer: a phase 3, open-label, randomised, non-inferiority trial (JASPAC 01). Lancet. 2016;388:248–57.
Conroy T, Hammel P, Hebbar M, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med. 2018;379:2395–406.
Sasako M, Sakuramoto S, Katai H, et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol. 2011;29:4387–93.
Benson AB III, Schrag D, Somerfield MR, et al. American Society of Clinical Oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol. 2004;22:3408–19.
Ecker BL, McMillan MT, Datta J, et al. Efficacy of adjuvant chemotherapy for small bowel adenocarcinoma: a propensity score-matched analysis. Cancer. 2016;122:693–701.
Kitahara H, Honma Y, Ueno M, et al. Randomized phase III trial of postoperative chemotherapy for patients with stage I/II/III small bowel adenocarcinoma (JCOG1502C, J-BALLAD). Jpn J Clin Oncol. 2019;49:287–90.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
There are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nitta, N., Ohgi, K., Sugiura, T. et al. Prognostic Impact of Pancreatic Invasion in Duodenal Carcinoma: A Single-Center Experience. Ann Surg Oncol 27, 4553–4560 (2020). https://doi.org/10.1245/s10434-020-08512-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-08512-8