
Abstract
Background
We developed a procedure for laparoscopic infrapyloric area lymph node (LN) dissection with No. 14v enlargement, which is complicated for patients with advanced lower gastric cancer (GC) (Xu et al., World J Gastroenterol 13:5133–5138,2007; Masuda et al., Dig Surg 25:351–358,2008; An et al., Br J Surg 98:667–672,2011].
Methods
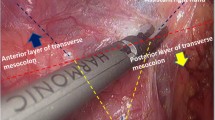
From April 2008 to December 2014, 1096 patients with GC underwent laparoscopy-assisted radical distal gastrectomy in our department. According to the Japanese GC treatment guidelines, D2 (+No. 14v) may be beneficial in tumors with apparent metastasis to the No. 6 nodes (Japanese Gastric Cancer Association, Gastric Cancer 14:113–123,2010). Thus, 151 advanced lower GC patients with apparent metastasis to the No. 6 nodes underwent additional No. 14v LN dissection.␣We dissected infrapyloric area LNs with No. 14v dissection from the left to the right side (i.e., middle colic vein approach).
Results
Mean operation time was 22.8 ± 10.0 min, mean blood loss was 17.1 ± 14.6 ml, and mean times to first flatus, fluid diet, and soft diet were 3.7 ± 1.2 days, 5.0 ± 1.7 days, and 8.4 ± 1.6 days, respectively. A mean of 33.7 ± 11.2 LNs were retrieved, including 3.9 ± 2.7 No. 6 LNs and 2.0 ± 1.6 No. 14v LNs. Of 151 patients, 26 had No. 14v metastasis (17.2 %), and 43 (28.5 %) were accompanied by an extensive infrapyloric area nodal involvement. The overall postoperative morbidity rate was 10.6 % (16 of 151). At a median follow-up of 56 months (range 5–84 months), cumulative 3-year overall survival was 56.0 %.
Conclusions
Although it remains controversial whether prophylactic No. 14v dissection improves survival, laparoscopic infrapyloric area LN dissection using a middle colic vein approach may be safely achieved and is more convenient for advanced lower GC.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Xu YY, Huang BJ, Sun Z, et al. Risk factors for lymph node metastasis and evaluation of reasonable surgery for early gastric cancer. World J Gastroenterol. 2007;13:5133–8.
Masuda TA, Sakaguchi Y, Toh Y, et al. Clinical characteristics of gastric cancer with metastasis to the lymph node along the superior mesenteric vein (14v). Dig Surg. 2008;25:351–8.
An JY, Pak KH, Inaba K, et al. Relevance of lymph node metastasis along the superior mesenteric vein in gastric cancer. Br J Surg. 2011;98:667–72.
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines, 2010 (ver. 3). Gastric Cancer. 2011;14:113–23.
Acknowledgments
Sponsored by National Key Clinical Specialty Discipline Construction program of China (grant [2012]649) and the Key Project of Science and Technology Plan of Fujian Province, China (Grant 2014Y0025).
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Chen, QY., Huang, CM., Lin, JX. et al. Laparoscopic Infrapyloric Area Lymph Node Dissection with No. 14v Enlargement for Advanced Lower Gastric Cancer in Middle Colic Vein Approach. Ann Surg Oncol 23, 951 (2016). https://doi.org/10.1245/s10434-015-4992-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4992-3