
Abstract
Background
Nephrotic syndrome is characterized by proteinuria, hyperlipidemia, and edema. The annual incidence of nephrotic syndrome is 2–7 cases/100,000 children.
Methods and results
The present study included 32 control, 32 steroid-sensitive nephrotic syndrome cases, and 32 steroid-resistant nephrotic syndrome cases aged ≤ 17 years. Serum samples were handled to check serum albumin, creatinine, calcium, and total cholesterol in SSNS and SRNS. Pearson’s correlation test was performed to investigate the relationship between the parameters. The independent sample t-test was done to compare the mean differences between two parameters by SPSS (Statistical Package for the Social Sciences). We found a significant positive correlation in SSNS in serum albumin, creatinine, calcium, and total cholesterol. In SRNS, we did not find a correlation between serum calcium and total cholesterol.
Conclusions
The combination of serum albumin, creatinine, and total cholesterol with serum calcium improves the diagnostic sensitivity of SSNS and SRNS. Thus, serum calcium may be used as an equivalent marker in the early diagnosis and treatment of nephrotic syndrome in children.
Similar content being viewed by others

Background
Nephrotic syndrome (NS) is a clinical triad of proteinuria, hyperlipidemia, and edema. The clinical manifestation of NS is characterized by the alteration in the permeability of the glomerular capillary wall, which causes extensive loss of plasma proteins and leads to proteinuria [1]. The loss of glomerular membrane permeability is might be primary with no visible cause, i.e., idiopathic or secondary with various causes like infections, medications, systemic lupus erythematosus, and diabetes mellitus [2]. The annual incidence of nephrotic syndrome is 2–7 cases/100,000 children and the total prevalence of 16/100,000 [3]. Based on patient response to steroid therapy, NS is classified as steroid-sensitive nephrotic syndrome (SSNS) and steroid-resistant nephrotic syndrome (SRNS) [4]. NS diagnosis depends on proteinuria > 1000 mg/M2/day, hypoalbuminemia, hypocalcemia, and hypercholesterolemia. The increased loss of protein in urine is exhibited by urinary loss of protein and increased release of protein by the liver [5]. Proteinuria leads to hypoalbuminemia (serum albumin < 2.5 gm/dl). Hypoalbuminemia causes an increase in the synthesis of lipoproteins in the hepatic cells. The exact mechanism of hyperlipidemia is not known, but it may be because of the elevation in lipoprotein synthesis. Hyperlipidemia is a clinical presentation found majorly in all nephrotic syndrome patients. It affects the overall composition and consistency of the lipoproteins and leads to different lipid abnormalities [6, 7]. There was no definite guideline and treatment for this condition. The data for hypercholesterolemia in patients with steroid-sensitive and steroid-resistant nephrotic syndrome is unavailable, making this condition under-treated [8]. Hypocalcemic condition observed due to severity of proteinuria, which affects calcium metabolism [9]. Patients suffering from nephrotic syndrome lose 25-hydroxyvitamin D3 (25OHD3) in urine, so the blood 25OHD3 level decreases simultaneously, which leads to hypocalcemia [10]. The loss of 25-hydroxyvitamin D3 (25OHD3) in urine with the steroid treatment contributes to disturbances in calcium (Ca) and vitamin D metabolism in nephrotic children [11]. Vitamin supplementation does not affect this abnormality [12]. The SSNS patients achieved partial or complete remission associated with steroid treatment, while SRNS patients do not respond to steroids, and survival of these patients is based on dialysis or renal transplant. Therefore, research has been focused on determining the disease severity and treatment [13]. Many researchers investigated the metabolic disturbances to find out their use as indicators of response to treatment. This study aimed to determine the correlation between different biochemical parameters like serum albumin, creatinine, total cholesterol, and calcium, and their significant difference in steroid-sensitive and steroid-resistant nephrotic syndrome patients.
Methods
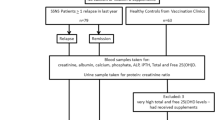
The present study included 32 control, 32 SSNS, and 32 SRNS cases aged ≤ 17 years. All study procedure was sanctioned by the Institutional Ethical Committee of Muljibhai Patel Urological hospital (MPUH) Nadiad, Gujarat, India [EC/395/2017].
Inclusion criteria
Children (age ≤ 17 years) with glomerular filtration rate (GFR) was less than 82 ml/min per 1.73 m2, and renal histology of FSGS (focal segmental glomerulosclerosis) and MCD (minimal change disease) on biopsy were recruited for this study.
Exclusion criteria
After clinical testing, patients who had other systemic diseases and nephrotic patients on vitamin D therapy were excluded from the study.
All the patients were clinically examined, and the following tests were performed:
-
1.
Serum albumin: BCG (bromocresol green) method [14]
-
2.
Serum total cholesterol: CHOD/PAP (cholesterol oxidase/peroxidase aminophenazone) method [15]
-
3.
Serum total calcium: OCPC (o-cresolphthalein complexone) method [16]
-
4.
Serum creatinine: Jaffe’s method [17]
Statistical data analysis
The statistical data were analyzed by SPSS (Statistical Package for the Social Sciences) version 28. The relationship between the two parameters was done by Pearson’s correlation test. The independent sample t-test was done to compare the mean differences between two parameters.
Results
There were 96 patients enrolled in this study in which there are 32 in the control group, 32 in the SSNS group, and 32 in the SRNS group of patients. The mean value of serum albumin was 4.19 gm/dl in the control group, 2.59 gm/dl in the SSNS group, and 2.33 gm/dl in the SRNS group of patients. There was 61% lower serum albumin observed in the SSNS group, while in SRNS, it was 55% lower compared to the control. Decreased serum albumin levels indicate hypoalbuminemia. Significant values were found between the SSNS vs. control and SRNS vs. control in serum albumin concentration (Table 1). The serum albumin was significantly decreasing in the SSNS and SRNS patients in comparison to the control. There was no significant difference found in the SSNS and SRNS group of patients in serum albumin.
The serum calcium concentration decreased to the same extent (29% lower) in both the SSNS and SRNS group of patients compared to the control. Hypocalcemic condition observed in the SSNS and SRNS patient group. The serum calcium was lower in SRNS compared to SSNS. The p-value of serum calcium in both patients’ groups was significant compared to the control. In contrast, the comparison of SSNS and SRNS was found to be non-significant. The mean total cholesterol concentration of control was 185.11 gm/dl. SSNS patients had a 223% significance increase in the total cholesterol, while SRNS patients had 234% compared to control. As shown in Table 1, the mean serum creatinine concentration was 0.649 mg/dl, 1.606 mg/dl, and 1.727 mg/dl for control, SSNS, and SRNS, respectively. Patients with SSNS showed a 247 % increase in serum total cholesterol, while SRNS had 226 %. The p-value of serum creatinine for control vs. SSNS and SRNS was 1.54E−15 and 3.84E−14, respectively.
Pearson’s correlation test was performed to evaluate the correlation between serum albumin, calcium, cholesterol, and creatinine. There was no correlation found in control patients between any of the studied parameters (Table 2). In the SSNS group, we got a significant positive correlation for all the performed estimations. The serum albumin was found to be positively correlated with serum calcium with R2 = 0.4634. The R2 value represents that serum albumin concentration is closely related to serum calcium concentration (Table 3). The correlation in the SRNS found that there was no significant correlation observed between serum total cholesterol and calcium. As shown in Table 4, the correlation between all the other parameters was significantly correlated.
Discussion
The preliminary characteristic of nephrotic syndrome is the disturbance in the permselectivity of the filtration membrane, which leads to leaking out the macromolecules into the urine. As a result, the most prevalent clinical presentation found in NS is hypoalbuminemia. The concentration of different biochemical parameters is also affected because of this. To determine the relationship, if any, it is necessary to investigate the correlation between other biochemical parameters and albumin. A total of 90 (32 control, 32 SSNS, and 32 SRNS) patients were recruited in this study. This study investigates the correlation between different parameters like serum albumin, total cholesterol, calcium, and creatinine.
In the present study, in comparison to control, we found a decrease in the albumin concentration in the SSNS (61%) and SRNS (55%). In addition, we found a significant difference in serum albumin in SSNS (p=1.01E−13) and SRNS (p=2.12E−15) compared to a healthy individual. However, we did not find a significant difference between SSNS and SRNS in serum albumin. One study by Krishanamurthy et al. found nearly the equivalent serum albumin concentration of 2.21 gm/dl in the NS patients [18]. A study on the Bangladesh population found decreased albumin levels in these populations. They also found a negative correlation between serum albumin and cholesterol [11].
Hypercholesterolemia observed in steroid-sensitive and steroid-resistant nephrotic syndrome patients. The SRNS patients had higher mean cholesterol concentrations than SSNS. Still, there was no significant difference found in serum total cholesterol between them. The correlation study found that serum cholesterol significantly correlated with serum albumin, creatinine, and calcium in SSNS. In SRNS, there was no correlation found between serum total cholesterol and calcium, but cholesterol was significantly correlated with serum albumin and creatinine. These suggest that cholesterol is also associated with serum creatinine. Hashim et al. found the most significant negative correlation between serum albumin and serum cholesterol which was p=0.001. There was severe hypercholesterolemia observed with the mean serum cholesterol of 11.29 mmol/L [19]. A study held in India found hypoalbuminemia with hypercholesterolemia. And the albumin was inversely proportional to cholesterol. They also discovered that cholesterol and triglycerides, LDL, and VLDL were also higher in nephrotic syndrome patients [20]. According to Biswas et al. and Agrawal et al., the significant increase in the cholesterol concentration in the NS patients is because of elevated apoB levels. The apoB is responsible for hypercholesterolemia with the impaired removal of lipoproteins from the blood of NS patients [21, 22].
Hypocalcemic condition observed in the SSNS and SRNS. There was a minute difference in the mean serum concentration between SSNS and SRNS, which showed no significant difference in serum calcium between the patients who responded and non-respond to steroids. According to Goldstein et al., steroids may also contribute to causing hypocalcemia with the loss of albumin and vitamin D metabolites [23]. The positive correlation between serum albumin and calcium in the current study suggests that serum calcium may use as an equivalent marker for the nephrotic syndrome as serum albumin and creatinine. The study on 60 NS patients found hypoalbuminemia as well as a significant positive correlation between serum albumin and calcium (p-value< 0.01) [9]. The study by Hashim et al. found hypocalcemic conditions in their studied population with hypoalbuminemia [19].
The serum creatinine had a significant positive correlation with all the studied parameters in both groups. A study on the Nepal population discovered almost similar findings to the current research in serum creatinine concentration (1.58 mg/dL) in idiopathic primary NS patients [24]. The Pearson’s correlation study was performed to find a correlation between different parameters in all the studied groups. There was no correlation found in the control group. In SSNS patients, we found a significant positive correlation between all the studied parameters. But in SRNS, we did not find a significant correlation between serum calcium and total cholesterol. The serum albumin and creatinine have already been used as biomarkers for SSNS and SRNS. This study found that serum calcium and total cholesterol had a significant positive correlation with serum albumin and creatinine. So, the present study results suggest that serum calcium may also be used as a biomarker for SSNS and SRNS patients.
Conclusion
The present study found that the patients had low albumin levels, leading to hyperlipidemia and hypocalcemia. Concentrations of these parameters were significantly correlated with each other in SSNS and SRNS. The combination of serum albumin, creatinine, and total cholesterol with serum calcium improves the diagnostic sensitivity of SSNS and SRNS. The study did not find a significant difference between SSNS and SRNS, and it may be due to the delayed response of steroid treatment. However, the study population was small still a larger population would be needed to strengthen the study.
Availability of data and materials
All data generated or analyzed during this study are included in this article.
Abbreviations
- NS:
-
Nephrotic syndrome
- SSNS:
-
Steroid-sensitive nephrotic syndrome
- SRNS:
-
Steroid-resistant nephrotic syndrome
- 25OHD3:
-
25-Hydroxyvitamin D3
- Ca:
-
Calcium
- BCG:
-
Bromocresol green
- CHOD/PAP:
-
Cholesterol oxidase/peroxidase aminophenazone
- OCPC:
-
o-Cresolphthalein complexone
- FSGS:
-
Focal segmental glomerulosclerosis
- MCD:
-
Minimal change disease
References
Hossain MA, Deb KP, Mannan KA, Mostafa G (2016) Correlation between serum cholesterol and serum albumin level in childhood nephrotic syndrome. Urol Nephrol Open Access J 4:86–90
Kodner C (2016) Diagnosis and management of nephrotic syndrome in adults. Am Fam Physician 93(6):479–485
Eddy AA, Symons JM (2003) Nephrotic syndrome in childhood. Lancet 362(9384): 629-639.
Nourbakhsh N, Mak RH (2017) Steroid-resistant nephrotic syndrome: past and current perspectives. Pediatr Health Med Therapeutics 8:29–37
Shearer GC, Kaysen GA (2001) Proteinuria and plasma compositional changes contribute to defective lipoprotein catabolism in the nephrotic syndrome by separate mechanisms. Am J Kidney Dis 37(1):S119–S122
Hu P, Lu L, Hu B, Du PF (2009) Characteristics of lipid metabolism under different urinary protein excretion in children with primary nephrotic syndrome. Scand J Clin Lab Investigation 69(6):680–686
Biswas A, Basu R (2018) Derangement in lipid profile in nephrotic syndrome in children. Int J Res Med Sci 6(4):1269–1272
Muso E, Mune M, Hirano T, Hattori M, Kimura K, Watanabe T et al (2015) A prospective observational survey on the long-term effect of LDL apheresis on drug-resistant nephrotic syndrome. Nephron Extra 5(2):58–66
Hossain A, Mostafa G, Mannan KA, Prosad Deb K, Hossain MM (2015) Correlation between serum albumin level and ionized calcium in idiopathic nephrotic syndrome in children. Urol Nephrol Open Access J 3:70–71
El Kersh MM, Sharaki OA, Omar OM, Galal YA (2018) Ionized calcium, 25-hydroxyvitamin D, and parathyroid hormone in children with steroid-sensitive nephrotic syndrome. Alexandria J Pediatr 31(3):132–140
Sinha N, Wade P, Ghildiyal RG, Maniar H (2018) Biochemical bone markers in children with steroid sensitive nephrotic syndrome in remission. Int J Contemp Pediatr 5(4):1588–1593
Banerjee S, Basu S, Sen A, Sengupta J (2017) The effect of vitamin D and calcium supplementation in pediatric steroid-sensitive nephrotic syndrome. Pediatr Nephrol 32(11):2063–2070
Bierzynska A, Soderquest K, Koziell A (2015) Genes and podocytes–new insights into mechanisms of podocytopathy. Front Endocrinol 5:1–7
Cosgrove D, Meehan DT, Pozzi A, Chen X, Rodgers KD, Tempero RM et al (2008) Integrin α1β1 regulates MMPs via p38 MAPkinase in mesangial cells: implications for Alport syndrome. Am J Pathol 172:761–773
Allain CC, Poon LS, Chan CS, Richmond WFPC, Fu PC (1974) Enzymatic determination of total serum cholesterol. Clin Chem 20(4):470–475
Baginski ES, Marie SS, Clark WL, Zak B (1973) Direct microdetermination of serum calcium. Clinica Chimica Acta 46(1):46–54
Toora BD, Rajagopal G (2002) Measurement of creatinine by Jaffe’s reaction-determination of concentration of sodium hydroxide required for maximum color development in standard, urine and protein free filtrate of serum. Indian J Experimental Biol 40(3):352–354
Krishanamurthy C, Rukmani J, Clarin D (2018) Evaluation of serum lipid profile in children with nephrotic syndrome admitted in emergency ward of Government Tirunelveli Medical College and Hospita India. Int J Contemp Pediatr 5(6):2244–2248
Hashim RD, Nathir I, Khalil NM (2020) The response of hypoalbuminemia, hypocalcemia and hypercholesterolemia to regular treatment in a group of pediatric patients with nephrotic syndrome. Int J Pharmaceut Res 12(4):2513–2517
Kusuma SK, Surath PD, Prabha I (2018) A clinical study of nephrotic syndrome with special reference to serum lipid profile. Int J Sci Res 8(11):1441–1444
Biswas A, Basu R, Basu K (2017) Nephrotic syndrome induced dyslipidemia in children and need for early assessment. J Med Dental Sci Res 3(12):35–38
Agrawal S, Zaritsky JJ, Fornoni A, Smoyer WE (2018) Dyslipidaemia in nephrotic syndrome: mechanisms and treatment. Nat Rev Nephrol 14(1):57–70
Goldstein DA, Haldimann B, Sherman D, Norman AW, Massry SG (1981) Vitamin D metabolites and calcium metabolism in patients with nephrotic syndrome and normal renal function. J Clin Endocrinol Metabol 52(1):116–121
Baral S, Baral BK, Joshi K, Shrestha S, Raut KB, Jha B (2018) Prevalence and study of lipid abnormalities in nephrotic syndrome attending a tertiary hospital Nepal. Int J Res Med Sci 6(11):3576–3581
Acknowledgments
The authors are grateful to Charutar Vidya Mandal Vallabh Vidyanagar and Muljibhai Patel Urological Hospital Nadiad, Gujarat, India, for providing a platform for this research work. We want to thank the SHODH- ScHeme Of Developing High quality research, Government of Gujarat, for providing fellowship to Jinal Thakor for the research work.
Funding
The research was supported by the SHODH- ScHeme Of Developing High quality research, Government of Gujarat.
Author information
Authors and Affiliations
Contributions
Ms. Jinal Thakor performed the statistical analysis and wrote the manuscript. Kinnari Mistry and Sishir Gang are responsible for study design and study conduct, made suggestions in the statistical analysis and interpretation, and critically reviewed the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Ethical Committee of Muljibhai Patel Urological hospital (MPUH) Nadiad, Gujarat, India [EC/395/2017].
Written informed consent was obtained from all of the participants in the study.
Consent for publication
Not applicable
Competing interests
The author declares that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thakor, J.M., Mistry, K.N. & Gang, S. Association between serum calcium and biochemical parameters among nephrotic syndrome patients: a case-control study. Egypt Pediatric Association Gaz 70, 18 (2022). https://doi.org/10.1186/s43054-022-00110-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-022-00110-5