
Abstract
Purpose
Minimizing delays in delivering nursing care is paramount for enhancing the overall quality of care. Certain bottleneck variables restrict the workflow of nurses, resulting in extended shift times. This study is designed to pinpoint and analyze the principal factors contributing to bottleneck issues in nursing workflow, to direct improvement endeavors. This study seeks to provide insights into the key variables contributing to nurses’ extended shift times, with the ultimate goal of prioritizing efforts for improvement.
Methods
A descriptive multicenter cross-sectional study was conducted. A scale was developed for this study by the authors after conducting a literature review, subsequently validated, and its reliability was assessed.
Results
Among the 31 bottleneck variables, 29 were retained under three persistent bottleneck factors: (1) Nurse staffing— This pertains to the availability of sufficient nursing staff at all times across the continuum of care; (2) Working environment and quality of care—This refers to the availability of necessary skills and resources for nurses to perform their duties effectively and; (3) Medical devices— This factor concerns the availability of fully functional medical devices required for providing care.
Conclusion
Efforts aimed at enhancing the overall healthcare system should concentrate on addressing persistent bottleneck factors. This may involve the implementation of a healthcare workforce management system, the establishment of standards for a conducive and supportive working environment, and the utilization of a standardized system for the management of medical equipment. The outcomes of this study can be utilized by nurses and policymakers to devise comprehensive strategies for improvement.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In the Kingdom of Saudi Arabia (KSA), the nursing workforce is the largest population group in the healthcare system, with a total of 184,565 registered nurses currently working in Ministry of Health (MOH) institutions [1]. The nursing workforce plays a crucial role in nearly every aspect of health services and serves as a driver for care improvement [2]. However, the increasing demand for healthcare services has disrupted the efficiency of the healthcare system [3]. This disruption has visibly impacted the efficiency of nursing workflow, leading to delays in providing certain patient care activities [4]. Consequently, it has contributed to the development of critical but avoidable complications [5]. There are financial implications as well; taking care of critical patients requires more nursing resources, increasing costs to the healthcare system [6].
Workflow efficiency refers to the measurement of resources, especially time, spent by a nurse to complete a regularly recurring task during a shift [4]. Nurses are facing the challenge of efficiently delivering higher-quality care without delay and at stable cost [5]. However, current management approaches have often relied on increasing capacity without a thorough analysis of optimizing existing resources, which could potentially exacerbate the situation [7]. Healthcare researchers have advocated for the adoption of management philosophies in the nursing care context to enhance patient care delivery [5]. Of these management philosophies, “the Theory of Constraints (TOC)”. TOC was developed and introduced in 1984 by Dr. Eliyahu Goldratt [7] to address manufacturing and production performance and perceived organization as a system consisting of multiple interacting resources [7]. These interdependent resources collaborate to achieve the organization’s goal.
The TOC suggests that every system has at least one resource that restricts the capability of the entire system (known as the constraint), and managing this constraint will ultimately determine the performance of the entire system. In hospitals, nursing constraints that hinder the flow of nursing activities can be either physical or non-physical. Physical constraints include bottlenecks in care processes, such as a limited workload capacity for a nurse. Non-physical constraints refer to noncompliance with rules, regulations, or policies.
Bottlenecks in general refer to resources with insufficient capacity to meet demand [8]. In essence, they restrict or slow down the care process, causing inefficiency [9]. A typical example of a bottleneck is the referral requests. In a busy hospital ward, referral requests can become a bottleneck, if nurses receive more referral requests for patients than they can process within their maximum capacity, particularly during peak hours. Such bottlenecks are likely to cause delays across the entire activities. Other common bottlenecks include waiting for medication request approvals from physicians. These scenarios can disrupt the overall workflow efficiency of nurses. Since most healthcare policymakers may be unfamiliar with the TOC, the next section provides a brief description of the bottlenecks related to TOC.
Theory of constraints—TOC
The TOC focuses on delivering timely, excellent, and effective care. In the nursing work context, its primary goal is to increase the number of nursing activities completed on time while maintaining control over expenses. To gain a deeper understanding of bottlenecks related to TOC, let’s illustrate this with an example from Al-Moteri et al. [4]. In 2023, a multi-phase, multi-center quality improvement project was conducted in the Taif region of Saudi Arabia. The ultimate goal of the project was to enhance patient care outcomes from the perspective of nursing productivity. The first phase aimed at determining the time taken by nurses to complete various activities during their entire shifts [3]. This study is the second phase of this multi-phase, multi-center quality improvement project. The first phase study revealed that nurses were able to complete only 85% of all shift activities, leaving 15% unfinished (Fig. 1). On average, nurses stayed an additional 73 min beyond the end of their shift to complete the remaining necessary tasks. In Al-Moteri et al. [4] the nurses’ work was delayed and hampered by a buildup of tasks caused by new admissions, lengthy doctor rounds, etc. In their study [4], the new admissions were, as an example, the bottleneck in the nursing workflow. However, it could be argued the tasks that nurses are expected to complete can vary significantly every day based on patient needs and emerging activities during a shift. This unpredictability can create complexity in the flow of nursing activities, and finding a permanent resolution to bottlenecks is difficult, if not impossible.

Bottleneck in nursing workflow
According to the TOC, there are two main types of bottlenecks, temporary and persistent [10]. Short-term bottlenecks are usually unexpected and result from temporary factors. One common example is a sudden change in a patient’s medical condition. Coming across a sudden decline in a patient’s status is not an everyday event, and it can have varying effects on the nurse’s workflow. Meanwhile, persistent bottlenecks are ongoing issues that seriously affect the flow of nursing activities, causing dissatisfaction for both nurses and patients, as well as reduced process efficiency over time. Additionally, they can lead to more temporary bottlenecks and worsen their impact [4]. A typical example is the shortage of staff.
Since persistent bottlenecking leads to a decline in nurses’ capacity and more temporary bottlenecks, managing these bottlenecks is key to increasing nurses’ work efficiency. The best way to manage bottlenecks is first to conduct a thorough investigation to identify bottlenecks that may affect nurses’ work efficiency, particularly if the healthcare institution aims to provide efficient healthcare services. Given the complexity of identifying bottlenecks, this necessitates the utilization of the bottleneck detection analysis technique, as outlined by Bemthuis et al. [11]. This multi-center study aims to address the existing knowledge gap through the specific identification and analysis of bottlenecks within the nursing workflow. Through this approach, the study seeks to provide insights into the key variables contributing to nurses’ extended shift times, with the ultimate goal of prioritizing efforts for improvement.
Methods
Design
This descriptive multicenter cross-sectional study was conducted between October 2023 and November 2023 in the Taif region of Saudi Arabia. A bottleneck variable assessment method was used and included a combination of techniques to identify problems that occur and impact nursing workflow efficiency. The following includes a step-by-step procedure [6]:
Step 1 Obtain variables from the nursing literature.
Step 2 Design a structured questionnaire using variables obtained from Step 1.
Step 3 Determine sample size.
Step 4 Distribute the questionnaire online.
Step 5 Data analysis.
Step 6 Conduct PCA.
Step 7 Identify bottleneck variables to devise and prioritize improvement actions.
Setting
Every government hospital in the Taif region was invited to participate in the current study. Four large government hospitals agreed to participate, collectively having a total of 1,903 beds and serving around 709,000 people. Once the ethical approval was obtained, permission from the participating hospitals was requested.
Step 1 Obtain variables from the nursing literature
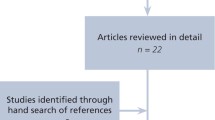
An initial literature review was conducted to identify bottleneck variables affecting nursing workflow by screening all empirical evidence published in peer-reviewed, scientific journals from 2000 to 2023. Forty bottleneck variables affecting nursing workflow were identified and statements of the data collection tool were constructed accordingly (see Fig. 2).

Search of literature for bottleneck variables
Step 2 design a structured questionnaire using variables obtained from step 1
First: The content validity index (CVI) of the current study data collection tool was evaluated by five subject matter experts (SMEs) possessing a minimum of 10 years of work experience in nursing administration. According to Shrotryia and Dhanda [12] assessing CVI requires assessing the relevancy of each item (I-CVI) and the overall scale (S-CVI). In this regard, SMEs were instructed to independently rate their opinion regarding the relevancy of the items by answering the following question: to what extent is item (X) perceived as a challenge that may restrict the workflow of nurses, resulting in extended shift times? SMEs were instructed to rate the 40 initial items using a 4-point Likert scale in which: 1 = not at all, 2 = slightly, 3 = moderately, and 4 = highly. A four-point scale was selected to avoid a neutral opinion. The I-CVI was then assessed by calculating the number of SMEs who rated the item as moderate = 3 or high = 4 and divided by the total number of SMEs [13]. The I-CVI for all the items on the scale ranged from 0.72 to 1. According to Lynn [14], any item scored below 0.78 can be eliminated. Nine items scored below 0.78 and were omitted. Thirty-one items were then tested for the S-CVI and were 0.85 [13], indicating high content validity for the overall instrument. Thirty-one items were included in the semi-final version.
Second: Before commencing the data collection process, a pilot study was carried out. Participants for the pilot study were recruited from the general medical and surgical units of one of the largest hospitals in the Taif region. The original plan was to recruit 40 participants. However, due to administrative issues, only 25 eligible participants were recruited. They were asked to evaluate the clarity of the scale items and the reliability of the entire scale using a 5-point Likert scale, ranging from “always” to “never.” These participants were informed to read the scale items loudly and briefly explain their understanding of each. Thus, the authors were able to determine if participants had difficulty understanding or if there were discrepancies in understanding and then modified the items accordingly. The pilot study was then conducted and the results showed a robust 𝛼 coefficient of 0.956 for the whole scale based on participants’ responses, indicating that the items effectively measure the underlying construct of bottleneck factors among respondents.
Third: The final questionnaire (31 items) was supplemented with additional items to assess the demographic data such as age, gender, qualifications, and work experience of the participants (Please see supplemented file).
Step 3 determine sample size
The representative sample size of the nursing population was determined using Thompson’s [15] formula:
Where:
N: Population size = 2460.
Z: Confidence level = 0.95.
d: Error proportion (0.05).
p: probability (50%).
n: sample size = 332.3884692.
Out of the 2460 nurses working in the four governmental hospitals, 334 nurses were considered appropriate for the study when population distributions were normal.
Step 4 distribute the questionnaire online
The final version of the scale was distributed to all nurses in the participating hospitals via an online Google Form, facilitated by their respective administration offices. Participants in the pilot study were excluded. Before accessing the Google Form, participants were required to review an explanatory statement and a consent statement. The online survey became accessible after participants confirmed that they had read and understood the consent statement:
“I certify that I did not participate in the pilot study. By clicking the “Next” button to enter the survey, I indicate my willingness to voluntarily participate in this study”.
Participants were assured that the online survey is anonymous, and no personally identifiable information is to be collected. The information they choose to provide in this study cannot be linked back to them.
A total of 570 nurses engaged in and completed the survey for the present study. To ensure diversity among participants, a follow-up email was sent to all department heads in the four hospitals, requesting them to encourage nurse participation. In the current study, the participants were distributed as follows: 38% (n = 216) were from general medical and surgical units, 5% (n = 28) were from the oncology units, 2% (n = 11) were from the hemodialysis departments, 2% (n = 11) were from diagnostic departments, 17% (n = 97) were from the emergency departments, 7% (n = 40) were from high dependency units, 22% (n = 126) were from intensive care units, and 5% (n = 30) were from the outpatient departments. Additionally, 2% (n = 11) were from other departments (e.g., Quality department, Training department, etc.).
Step 5 data analysis
Data were analyzed using the Statistical Package for the Social Sciences (IBM SPSS) version 26. A descriptive analysis was used for demographic data, and a Principal Component Analysis (PCA) was performed to identify how much each of the bottleneck variables impacts the nurses’ workflow.
Result
Participants’ characteristics
Table 1 shows that of the 570 participants in the survey, the age of 82% (n = 465) of the respondents ranged from 20 to 40 years and that 83% (n = 473) had 15 years or less of work experience. Such data on age and work experience indicate that the participants were young. Furthermore, the majority of the participants were women (n = 467) and 78% of the participants had a bachelor’s degree.
Factor analysis
The adequacy of the sample size was checked using Kaiser-Meyer-Olkin (KMO). Table 2 shows that the KMO value is 0.962 which is larger than 0.5, indicating that the Bartlett test has a high sampling adequacy to perform a factor analysis. Therefore, each of the 31 variables can be loaded heavily on only one of the principal components, while the absolute value of the loadings exceeds 0.50. Principal component analysis (PCA) was used to identify patterns in the correlations between the 31 bottleneck variables. These patterns are used to determine the presence of underlying factors, called components.
In the current study, factor aggregation was based on varimax rotation and this is indicated in Table 3. Using the varimax rotation has simplified the interpretation. Indeed, with varimax each variable is associated with one of the factors and each factor represents only a small number of variables. The three components are interpretable as follows: (1) Nurse staffing— This pertains to the availability of sufficient nursing staff at all times across the continuum of care (Aiken & Fagin, 2018); (2) Working environment and quality of care —This refers to the availability of necessary skills and resources for nurses to perform their duties effectively (Johansen et al.,2021) and; (3) Medical devices— This factor concerns the availability of fully functional medical devices required for providing care (Aronson et al., 2020).
Among the 31 bottleneck variables, 29 were retained in three components (Table 4). For example, the variable that measures the frequency of encountering an unbalanced nurse-patient ratio is relatively strongly correlated with the first component (0.83). Similarly, the variable that measures the frequency of encountering a lack of the skills and knowledge to provide high-quality care and malfunctioning medical equipment are relatively strongly correlated with the second (0.70) and the third (0.80) component, respectively.
Discussion
In this research, a bottleneck variable analysis using the PCA tool [16] was used to identify key variables that affect nurses’ workflow to prioritize improvement efforts. The analysis identified 29 bottleneck variables, each contributing to different levels of variance in nursing workflow. Recognizing bottlenecks has introduced a new approach to constraint management in nursing workflow. Instead of viewing any new improvement idea as beneficial for the entire nursing system, efforts should target the nurses’ workflow bottlenecks. If healthcare policymakers can identify and effectively manage nursing work bottlenecks, or allocate resources more efficiently towards the bottlenecks, it can result in significant improvements in the overall work productivity of the nurses and improve patient care outcomes [4, 16].
Applying TOC began in manufacturing and expanded to areas like logistics, project management, and sales [17]. Its significant impact on improving system performance while maintaining costs, suggests that TOC could be effective in the healthcare systems, but few studies have explored its application in this field [18]. While addressing short-term issues such as continuously monitoring patients to detect and prevent deterioration can help avoid complex events and any subsequent delay, it is not sufficient to address the persistent bottleneck. The lack of nursing capacity due to a shortage of nurses [19, 20], lack of skills [21], and medical device inefficiency [22] are the primary issues, and unless these are resolved, nursing overtime will continue to be necessary. TOC recommends investing in addressing persistent bottlenecks [7] to enhance resilience in nursing care processes. The following sections will outline the bottleneck factors that have been identified in the current study, along with some proposed solutions.
Bottleneck factor 1 (nursing staffing) is a principal factor that loaded 21% of the variables studied and contains nine variables. Of the nine variables, the ‘unbalanced nurse-patient ratio’, the ‘nursing shortage’, the ‘professional burnout’, and ‘nurse absenteeism’ received high loadings of 0.830, 0.829, 0.731, and 0.702, respectively. Meanwhile, ‘lack of actions to control absenteeism of nurses’, ‘insufficient rest breaks’, and ‘unbalanced nurses’ distribution across hospital wards’ received moderate loads of 0.672, 0.653, and 0.644. ‘Lack of support from your workplace colleagues and leaders’ received 0.556 and ‘inappropriate shift scheduling’ received 0.504.
In the initial phase of the quality improvement project, it was consistently necessary to allocate an additional 15% of time on top of the scheduled shift time. This strongly indicates that the staffing levels are insufficient to meet the demands of the workload. Many studies link nursing productivity to nurse staffing level [23,24,25]. Nurse staff levels are a determinant of care outcomes [26]. Just recently, nurse staffing level has become the focus of attention of healthcare setting managers and it is increasingly important that healthcare setting managers control costs without compromising the quality of the services [27]. Many techniques are available in the literature for planning nurse staffing levels; however, there is a lack of agreement on “what staffing levels are acceptable” and “how staffing levels should be planned” in different situations [27]. Achieving the goal of controlling costs without compromising quality outcomes requires replacing traditional techniques with reliable and integrated database-based staffing systems, systems that allow nursing managers to control who is doing what, where, and when. Studies that examine workforce management systems in healthcare settings remain limited [28, 29].
Bottleneck factor 2 (Working environment and quality of care) is a major factor that loaded 20% of the variables studied and contains 13 variables. Of the 13 variables, ‘lack of skills and knowledge needed to provide high-quality care’, ‘lack of research skills to apply evidence-based practice’, ‘high-acuity patients’, ‘lack of training to update their skills and knowledge’, ‘dealing with difficult patients/family members’, and ‘lack of professional development activities’ received high loadings of 0.708, 0.676, 0.654, 0.636, 0.616 and 0.600, respectively. Meanwhile, the loads received for ‘lack of communication with leaders’, ‘lack of recognition/ appreciation’, ‘lack of teamwork’, ‘lack of transparency in leadership’, ‘lack of educational activities outside the hospital’, ‘conflicts and disputes with healthcare team’, and ‘schedule inflexibility’ ranged from 0.590 to 0.503.
It is well-acknowledged that equipping nurses with the required skills and having good work environments are key factors in improving nurses’ work outcomes [30]. Creating a work environment that acts as a foundation for quality of care requires hospital managers’ support [31]. Some studies raise the potential importance of implementing the six essential standards of the American Association of Critical Care Nurses (AACN) of healthy work environment standards [32]. The six essential standards of the AACN are skilled communication, true collaboration, effective decision-making, appropriate staffing, meaningful recognition, and authentic leadership. Integrating the six essential standards of the AACN was found to help produce effective and sustainable outcomes for nurse work [33].
Bottleneck factor 3 (Medical devices) is a principal factor that loaded 18% of the variables studied and contains seven variables. Of the seven variables, ‘malfunctioning of medical equipment’, ‘lack of maintenance’, ‘low-quality’, ‘shortages of supplies’, and ‘medical equipment incompetency’ have received high loadings ranging from 0.809 to 0.732. Meanwhile, ‘unavailability’ and ‘loss of medical equipment’ received loading of 0.666 and 0.609 respectively.
Medical equipment and devices are an essential component of healthcare services. Indeed, medical devices are used by nurses daily and in almost every activity to prevent, diagnose, monitor, and treat diseases [34]. The shortage of medical devices was found to harm the ability of the healthcare system to provide quality healthcare [35]. Recently, there has been an ongoing increase in the quality control of medical equipment studies [36]. Having a ‘standardized management system’ for medical devices that is entirely based on a quality control system can significantly reduce the rate of maintenance and failure of equipment and establish a good basis for hospital development [36].
Study limitations
Although the results of the present study provide insight into the bottleneck variables that could impact nurses’ workflow and efficiency, the study results should be used with caution due to some limitations. First, study participants were from the same geographical locations which may interfere with the generalizability of the study results. Indeed, the geographical location may impact the perception of the variables, so larger geographical regions are highly recommended to provide additional insights. Second, although bottleneck variables were collected from the literature, a more systematic review of the literature is required to ensure a comprehensive set of bottleneck variables.
Conclusion
The results of the study contribute to the current literature by identifying key bottleneck factors that constrain nursing workflow efficiency which have not previously been captured by researchers. Three bottleneck factors, nurse staffing, work environment for quality of care, and medical devices, were identified as key bottleneck issues and may be considered by the leaders and managers to prioritize and deliver affordable and effective improvement efforts. Improvement plans involve the implementation of (1) a healthcare workforce management system, (2) healthy work environment standards and a supportive leadership system, and (3) a standardized management system of medical equipment based on the quality control process to provide quality care. Further research is needed to explore the implementation of systems and standards in hospitals, as this would be valuable to policymakers who are seeking to improve health services.
Data availability
The author confirms that all data generated or analysed during this study are included in this manuscript.
Abbreviations
- KSA:
-
Kingdom of Saudi Arabia
- AACN:
-
American Association of Critical Care Nurses
- CVI:
-
Content validity index
- SMEs:
-
Subject matter experts
- I-CVI:
-
Item content validity index
- S-CVI:
-
Scale- content validity index
- KMO:
-
Kaiser-Meyer-Olkin
- PCA:
-
Principal component analysis
References
Alsufyani AM, Alforihidi MA, Almalki KE, Aljuaid SM, Alamri AA, Alghamdi MS. Linking the Saudi Arabian 2030 vision with nursing transformation in Saudi Arabia: Roadmap for nursing policies and strategies. Int J Afr Nurs Sci. 2020;13:100256. https://doi.org/10.1016/j.ijans.2020.100256.
National Academies of Sciences, Engineering, and Medicine. The role of nurses in improving health care access and quality. The future of nursing 2020–2030: charting a path to achieve health equity. 2020:99–126. https://www.ncbi.nlm.nih.gov/books/NBK573898/
Alasiri AA, Mohammed V. Healthcare transformation in Saudi Arabia: an overview since the launch of vision 2030. Health Serv Insights. 2022;15:11786329221121214.
Al-Moteri M, Alzahrani AA, Althobiti ES, Plummer V, Sahrah AZ, Alkhaldi MJ, Rajab EF, Alsalmi AR, Abdullah ME, Abduelazeez AE, Caslangen MZ. The Road to Developing Standard Time for Efficient Nursing Care: A Time and Motion Analysis. InHealthcare 2023 Aug 6 (Vol. 11, No. 15, p. 2216). MDPI. https://doi.org/10.3390/healthcare11152216
Scott PA, Harvey C, Felzmann H, Suhonen R, Habermann M, Halvorsen K, Christiansen K, Toffoli L, Papastavrou E. Resource allocation and rationing in nursing care: A discussion paper. Nursing ethics. 2019;26(5):1528-39.
Zayas-Cabán T, Okubo TH, Posnack S. Priorities to accelerate workflow automation in health care. J Am Med Inform Assoc. 2023;30(1):195–201.
Bacelar-Silva GM, Cox JF III, Rodrigues PP. Outcomes of managing healthcare services using the theory of constraints: a systematic review. Health Syst. 2022;11(1):1.
Chen Y, Xie W, Gunter CA, Liebovitz D, Mehrotra S, Zhang H, Malin B. Inferring clinical workflow efficiency via electronic medical record utilization. InAMIA annual symposium proceedings 2015 (Vol. 2015, p. 416). American Medical Informatics Association. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4765602/
Mihalj M, Corona A, Andereggen L, Urman RD, Luedi MM, Bello C. Managing bottlenecks in the perioperative setting: optimizing patient care and reducing costs. Best Pract Res Clin Anaesthesiol. 2022;36(2):299–310. https://doi.org/10.1016/j.bpa.2022.05.005.
Subramaniyan M, Skoogh A, Bokrantz J, Sheikh MA, Thürer M, Chang Q. Artificial intelligence for throughput bottleneck analysis–state-of-the-art and future directions. J Manuf Syst. 2021;60:734–51.
Bemthuis RH, van Slooten N, Arachchige JJ, Piest JP, Bukhsh FA. A Classification of Process Mining Bottleneck Analysis Techniques for Operational Support. InICE-B 2021 (pp. 127–135). https://doi.org/10.5220/0010578601270135
Shrotryia VK, Dhanda U. Content validity of assessment instrument for employee engagement. Sage Open. 2019;9(1):2158244018821751. https://doi.org/10.1177/2158244018821751.
Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–97. https://doi.org/10.1002/nur.20147.
Lynn MR. Determination and quantification of content validity. Nurs Res. 1986;35(6):382–6. https://pubmed.ncbi.nlm.nih.gov/3640358/.
Thompson B. Effect sizes, confidence intervals, and confidence intervals for effect sizes. Psychol Sch. 2007;44(5):423–32. https://doi.org/10.1002/pits.20234.
Ongbali SO, Afolalu SA, Oyedepo SA, Aworinde AK, Fajobi MA. A study on the factors causing bottleneck problems in the manufacturing industry using principal component analysis. Heliyon. 2021;7(5). https://doi.org/10.1016/j.heliyon.2021.e07020.
Hajmirfattahtabrizi M, Song H. Investigation of bottlenecks in supply chain system for minimizing total cost by integrating manufacturing modelling based on MINLP approach. Appl Sci. 2019;9(6):1185.
Goldratt EM, Cox J. The goal: a process of Ongoing Improvement. Abingdon, UK: Routledge; 2016.
Alluhidan M, Tashkandi N, Alblowi F, Omer T, Alghaith T, Alghodaier H, Alazemi N, Tulenko K, Herbst CH, Hamza MM, Alghamdi MG. Challenges and policy opportunities in nursing in Saudi Arabia. Hum Resour Health. 2020;18:1–0.
Drennan VM, Ross F. Global nurse shortages—the facts, the impact and action for change. Br Med Bull. 2019;130(1):25–37.
Suprapto S. Capacity building for nurses in hospitals. Asia Pac J Manage Educ (APJME). 2022;5(1):11–21.
Akpor OA, Akingbade TO, Olorunfemi O. Lack of adequate equipment for healthcare–the agony of patients and nurses: a review. Indian J Continuing Nurs Educ. 2023;24(1):7–10.
Hockenberry JM, Becker ER. How do hospital nurse staffing strategies affect patient satisfaction? ILR Rev. 2016;69(4):890–910. https://doi.org/10.1177/0019793916642760.
Shimp KM. Systematic review of turnover/retention and staff perception of staffing and resource adequacy related to staffing. Nurs Econ. 2017;35(5):239–A66. https://www.proquest.com/scholarly-journals/systematic-review-turnover-retention-staff/docview/1954857855/se-2?accountid=15290.
Dall TM, Chen YJ, Seifert RF, Maddox PJ, Hogan PF. The economic value of professional nursing. Med Care. 2009;47(1):97–104. https://doi.org/10.1097/MLR.0b013e3181844da8.
Trepanier S, Yoder-Wise PS, Church CD, Africa L. Nurse leaders’ assumptions and attitudes toward residency programs for new graduate nurses. Nurs Adm Q. 2021;45(1):26–34. https://doi.org/10.1097/NAQ.0000000000000442.
Saville C, Dall’Ora C, Griffiths P. The association between 12-hour shifts and nurses-in-charge’s perceptions of missed care and staffing adequacy: a retrospective cross-sectional observational study. Int J Nurs Stud. 2020;112:103721. https://doi.org/10.1016/j.ijnurstu.2020.103721.
Griffiths P, Saville C, Ball JE, Jones J, Monks T. Safer Nursing Care Tool study team. Beyond ratios-flexible and resilient nurse staffing options to deliver cost-effective hospital care and address staff shortages: a simulation and economic modelling study. Int J Nurs Stud. 2021;117:103901. https://doi.org/10.1016/j.ijnurstu.2021.103901.
Wynne R, Davidson PM, Duffield C, Jackson D, Ferguson C. Workforce management and patient outcomes in the intensive care unit during the COVID-19 pandemic and beyond: a discursive paper. J Clin Nurs 2021 Apr. https://doi.org/10.1111/jocn.15916
Copanitsanou P, Fotos N, Brokalaki H. Effects of work environment on patient and nurse outcomes. Br J Nurs. 2017;26(3):172–6. https://doi.org/10.12968/bjon.2017.26.3.172.
Model AM. The Effect of Nurse Practice Environment on Retention and Quality of Care via Burnout, Work characteristics, and Resilience. J Nurs Adm. 2020;50(10):546–53. https://doi.org/10.1097/NNA.0000000000000932.
Kelly L, Todd M. Compassion fatigue and the healthy work environment. AACN Adv Crit Care. 2017;28(4):351–8. https://doi.org/10.4037/aacnacc2017283.
Ulrich B, Cassidy L, Barden C, Varn-Davis N, Delgado SA. National nurse work environments-October 2021: a status report. Crit Care Nurse. 2022;42(5):58–70. https://doi.org/10.4037/ccn2022798.
Iadanza E, Cerofolini S, Lombardo C, Satta F, Gherardelli M. Medical devices nomenclature systems: a scoping review. Health and Technology. 2021;11:681 – 92. https://springerlink.bibliotecabuap.elogim.com/article/10.1007/s12553-021-00567-1
Moyimane MB, Matlala SF, Kekana MP. Experiences of nurses on the critical shortage of medical equipment at a rural district hospital in South Africa: a qualitative study. Pan Afr Med J. 2017;28(1):157. https://www.ajol.info/index.php/pamj/article/view/167360.
Li J, Mao Y, Zhang J. Maintenance and quality control of medical equipment based on information fusion technology. Comput Intell Neurosci. 2022;2022(1):9333328. https://doi.org/10.1155/2022/9333328.
Acknowledgements
The authors extend their appreciation to Taif University, Saudi Arabia, for supporting this work through project number (TU-DSPP-2024-282). The authors wish also to express their gratitude to the nurses who participated in this study.
Funding
This research was funded by Taif University, Saudi Arabia, Project No. (TU-DSPP-2024-282).
Author information
Authors and Affiliations
Contributions
Conceptualization and design, M.A and J.A; Data curation, A.A.G, E.S.A, B.A, and A.A; Investigation, A.A.G, E.S.A, B.A, and A.A; Methodology, MA and JA; M.A; Writing—original draft, MA; Writing—review and editing, M.A and J.A; All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was reviewed and approved by the Scientific Research Ethics Committee in King Faisal Medical Complex (KFMC) (IRB number: 2023-B-40). A written informed consent was obtained from all the participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Al Moteri, M., Aljuaid, J., Alsufyani, B. et al. Bottleneck factors impacting nurses’ workflow and the opportunity to prioritize improvement efforts: factor analysis. BMC Nurs 23, 640 (2024). https://doi.org/10.1186/s12912-024-02311-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-024-02311-2