
Abstract
Purpose
The objective of this systematic review and metaanalysis is to compare the efficacy and safety of decompression alone versus decompression plus fusion in single-level lumbar spinal stenosis with spondylolisthesis.
Methods
A comprehensive search of the PubMed, Embase, Cochrane Library, and Ovid Medline databases was conducted to find randomized control trials (RCTs) or cohort studies that compared decompression alone and decompression plus fusion in single-level lumbar spinal stenosis with spondylolisthesis. Operation time; reoperation; postoperative complications; postoperative Oswestry disability index(ODI) scores and scores related to back and leg pain were collected from eligible studies for meta-analysis.
Results
We included 3 randomized controlled trials and 9 cohort studies with 6182 patients. The decompression alone group showed less operative time(P < 0.001) and intraoperative blood loss(p = 0.000), and no significant difference in postoperative complications was observed in randomized controlled trials(p = 0.428) or cohort studies(p = 0.731). There was no significant difference between the other two groups in reoperation(P = 0.071), postoperative ODI scores and scores related to back and leg pain.
Conclusions
In this study, we found that the decompression alone group performed better in terms of operation time and intraoperative blood loss, and there was no significant difference between the two surgical methods in rate of reoperation and postoperative complications, ODI, low back pain and leg pain. Therefore, we come to the conclusion that decompression alone is not inferior to decompression and fusion in patients with single-level lumbar spinal stenosis with spondylolisthesis.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Lumbar spinal stenosis refers to a series of clinical symptoms caused by nerve root compression in the lumbar spinal canal due to various reasons [1, 2]. Lumbar spondylolisthesis refers to the mutual displacement between adjacent vertebral bodies, generally defined as the anterior displacement of the upper vertebral body relative to the lower vertebral body [3]. Lumbar spinal stenosis with spondylolisthesis is a common disease in spine surgery. The main clinical symptoms of this disease are low back pain, hip pain, lower limb pain and numbness, and neurogenic claudication, which affects the daily life of patients [4]. Non-surgical treatment including physical therapy, drug therapy or acupuncture can help patients relieve symptoms to a certain extent, but when the condition is serious and conservative treatment is ineffective, doctors will consider surgical treatment for patients [5, 6]. Previous studies have confirmed that surgical treatment has a better prognosis and significantly improved quality of life compared with conservative treatment [7, 8]. With the development of implants, interbody fusion through a variety of approaches has gradually been favored by clinicians. In some regions, spinal canal decompression combined with instrument fusion has accounted for more than 90% of the treatment of lumbar spondylolisthesis [9, 10]. However, with the increasing use of decompression and fusion surgery in the case of lumbar spinal stenosis with spondylolisthesis, more and more problems have begun to appear, such as prolonged operation and hospitalization time, increased treatment costs, increased postoperative complications and reoperation rate, and other adverse consequences [11,12,13]. Therefore, the surgical treatment of lumbar spinal stenosis with spondylolisthesis is controversial [6]. The most controversial were three randomized controlled trials on the selection of surgical procedure for single-level lumbar spinal stenosis with spondylolisthesis. Inose concluded that f decompression plus fusion was not superior to decompression alone [14], and the RCT conducted by Austevoll reported that decompression alone was not inferior to decompression plus fusion [15]. However, Ghogawala suggested that decompression plus fusion should be chosen over decompression alone in the surgical treatment of single-level lumbar spinal stenosis with spondylolisthesis [16]. Two systematic reviews [17, 18] did not recommend decompression plus fusion in patients with lumbar spinal stenosis and spondylolisthesis. However, there is no systematic review or meta analysis on the advantages and disadvantages of decompression alone or decompression plus fusion in the surgical treatment of single-level lumbar spinal stenosis with spondylolisthesis. Therefore, this article mainly aimed at the patients with single-level lumbar spinal stenosis with spondylolisthesis, whether fusion surgery is necessary after decompression surgery.
Materials and methods
This review protocol was registered with PROSPERO(CRD42023399298) and followed the Preferred Reporting Items of Systematic Reviews and Meta-analysis guidelines [19].
Search strategy
Two investigators independently searched the following databases (inception to Dec 2022): PubMed, Embase, Cochrane Library, Web of Science, and Ovid Medline databases. The search strategy follows PICOS principles: (1) Participants: Patients with single-level lumbar spinal stenosis with spondylolisthesis. (2) Intervention(D group): All decompression procedures for spinal stenosis, including minimally invasive or open laminectomy, unilateral laminectomy and bilateral decompression, etc. (3) Comparison(F group): Additional arthrodesis is performed on the basis of the above decompression procedures, including Interbody fusion or/and posterolateral fusion et al. (4) Outcomes: The study should include at least one of the following data: Operation time, intraoperative blood loss, reoperation, complications, Oswestry disability index(ODI) socres, and scores related to back or leg pain (5) Study design: Observational studies and randomized control trials were eligible.
The electronic search strategy used the following keywords: “spinal stenosis”, spondylolisthesis”, “decompression”, “fusion”. The search terms were adjusted according to the characteristics of each database, and we also examined the reference lists of the screened full-text studies to identify additional trials that might be eligible. And a third reviewer was consulted when the two reviewers could not reach a consensus.
Eligibility criteria
Inclusion criteria were randomized clinical trials and cohort studies written in English that compared the decompression alone versus decompression plus fusion in patients with single-level lumbar spinal stenosis with spondylolisthesis. We excluded reports surgery with more than one level, case reports, case series, commentaries, practice guidelines, systematic reviews and meta-analysis. In addition, duplicate studies with the same cohort or studies considered by consensus to be of low quality were excluded.
Data collection
Data were extracted from the included studies as follows: (1)study design: first author, publication region, publication time, and study type; (2) sample demographics: number of patients, age, sex, and disease diagnosis; (3) surgery details: methods of decompression alone and decompression plus fusion, operation time, intraoperative blood loss; (4) analysis variables: reoperation and postoperative complications, postoperative Oswestry disability index(ODI) scores and scores related to back or leg pain. In case of absence of data, variances were transformed or estimated using the recommendations in Sect. 6.5.2 in the Cochrane Handbook for Systematic Reviews of Interventions [20]. We resolved disagreements for data extraction through discussion, or with arbitration by a third reviewer if necessary.
Assessment of risk of bias
The Cochrane Collaboration’s tool was used by two reviewers to independently evaluate the included RCTs for potential bias. And the bias risk of cohort studies was evaluated by the Newcastle-Ottawa scales, The quality of cohort studies was evaluated according to the Newcastle-Ottawa scale, with scores above 7 (including 7) of high quality.
Statistical analysis
The continuous variables were estimated by weighted mean difference (WMD), and for dichotomous variables, odds ratios (ORs) with a 95% confdence interval (CI) were calculated. The statistical heterogeneity of the pooled results was determined using the I² statistic. For this meta-analysis, we used the fixed-effect model when I² was greater than 50%, and if I² was less than 50%, a random-effect model was applied. The meta-analysis results were considered statistically significant when the p value < 0.05. And the magnitude of publication bias was estimated by Begg’ and Egger’ test. The meta-analysis was performed using STATA 16.0 (StataCorp, College Station, TX, USA).
Results
Search results
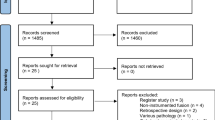
A total of 131 articles from PubMed, Embase, Cochrane Library, and Ovid Medline databases were initially identified. The exact number of articles identified in each database is as follows: PubMed (n = 601), Embase (n = 599), the Cochrane library (n = 78), Ovid Meline(n = 589). 872 articles were excluded because of duplication, and 960 studies were excluded by screening the titles and abstracts for: irrelevant studies, case reports, non-comparative studies and review articles. Leaving 35 articles that underwent a comprehensive full-text analysis. Finally, 3 randomized controlled trials [15, 16, 21] and 9 cohort studies [22,23,24,25,26,27,28,29] were included studies in the final meta-analysis. The flow chart used for the new systematic review according to PRISMA 2020 is shown in Fig. 1.

Flow diagram for the selection of studies (PRISMA)
Study characteristics and quality assessment
A total of 6182 patients were enrolled in the 3 randomized controlled trials and 8 cohort studies. The decompression alone group(D group) included 2339 participants, and the decompression plus fusion group(F group) included 3783 patients. The characteristics of the included studies are presented in Table 1. A summary of the risk of bias assessment of the RCTs is displayed in Fig.S1 and the risks of bias of the included cohort studies are displayed in Table S1.
Meta-analysis results
Operation time
Seven studies (n = 2936 patients; 1344 in the D group and 1592 in the F group) provided operation time, and there was statistically significant difference between the two groups regarding Operation time(WMD − 67.71; 95% CI − 92.12 to − 43.30, P = 0.000; I²=98.1%, p = 0.000)(Fig. 2). The heterogeneity was not reduced after subgroup analysis and and included studies (Except chen reported that the same operation time in both groups) reported that the operation time in the decompression alone group was shorter than that in the decompression plus fusion group.

Forest plot of operation time; CI: Confidence Internal
Intraoperative blood loss
A total of 4 studies reported the intraoperative blood loss (n = 447 patients; 220 in the D group and 247 in the F group). Statistically significant difference was observed in D group and F group (WMD − 260.95; 95% CI − 396.48 to − 125.42, P = 0.000; I² =95.3%, p = 0.000)(Fig. 3). Since Kimura(2019) [26] did not provide standard deviation, this part of the combined effect value was not calculated. However, the intraoperative blood loss reported by Kimura(2019) was also less in the decompression alone group than in the decompression plus fusion group. Subgroup analysis was based on surgical procedures (open or minimally invasive), and the heterogeneity decreased after excluding Hua (2021) [23](WMD − 310.04; 95% CI − 389.53 to − 230.54 P = 0.000; I² =67%, p = 0.048)(Fig. S2).

Forest plot of intraoperative blood loss
Reoperation
A total of 10 articles reported the occurrence of reoperation after surgery, but no reoperation was observed in the two groups by hua2021 during the two-year follow-up period, so a total of 9 articles (n = 4773 patients; 1953 in the D group and 2820 in the F group) were used for Meta-analysis. There was no statistically significant difference in reoperation between the D group and F group (OR 0.87; 95% CI 0.58 to 1.30, P = 0.493; I² =44.5%, p = 0.071) (Fig. 4), Subgroup analysis by article type (cohort study or RCT) and duration of follow-up (2 years or more) reduced heterogeneity, but no between-group differences in reoperation were observed (Fig. S3/Fig. S4).

Forest plot of reoperation
Postoperative complications
Eight articles(n = 2746 patients; 1275 in the D group and 1741 in the F group) reported postoperative complications, which did not include changes in neurological function, only included infection, hematoma, or other systemic complications such as pneumonia, urine retention, etc. The results showed that the incidence of postoperative complications in D group was lower than that in F group (OR 0.89; 95% CI 0.56 to 1.41, P = 0.612; I² = 26.2%, p = 0.220) (Fig. 5). Subgroup analysis by article type showed no significant statistical differences between the two groups in the cohort studies (OR 0.89; 95% CI 0.56 to 1.41, P = 0.731; I² = 53.2%, p = 0.074), or the randomized controlled trials(OR 0.77; 95% CI 0.39 to 1.49, P = 0.433; I² = 0.0%, p = 0.738)(Fig. S5).

Forest plot of postoperative complications
Oswestry disability index (ODI) scores
Seven articles(n = 2268 patients; 925 in the D group and 1343 in the F group) provided baseline Oswestry disability index scores. Sigmundsson(2015) [28] grouped participants according to preoperative low back pain and back pain, so to avoid the bias caused by grouping within the study, the articles were divided into two groups(BP < LP for Sigmundsson1 and BP > LP for Sigmundsson2) for analysis. There was no statistically significant difference in ODI scores between decompression alone group and decompression plus fusion group at the follow-up time of 3 months(WMD − 0.92; 95% CI -2.48 to 0.64, p = 0.246; I² =11%, p = 0.338), 1 year(WMD 0.44; 95% CI -0.71 to 1.60, p = 0.453; I² =11.3%, p = 0.343), and 2 years(WMD 0.67; 95% CI -1.14 to -0.69, p = 0.908; I² =54.4%, p = 0.052)(Fig. 6).

Forest plot of postoperative oswestry disability index (ODI) scores
Back pain and leg pain
A total of five included articles(n = 2103 patients; 915 in the D group and 1188 in the F group) reported scores related to back pain and leg pain, including Numeric Rating Scale(NRS) and visual analogue scale(VAS)scores. As with ODI scores, Sigmundsson2015 was divided into two groups for analysis. The results of the meta-analysis showed that there were no statistically significant differences in back pian at 3 months(WMD − 0.03; 95% CI -0.26 to 0.21, p = 0.821; I² =0.0%, p = 0.771), 1 year(WMD − 0.44; 95% CI -1.08 to 0.21, p = 0.186; I² =86.5%, p = 0.000) and 2 years(WMD − 0.53; 95% CI -1.06 to 0.00, p = 0.05; I² =69.8%, p = 0.019)( Fig. 7) after surgery. And for leg pain, no statistically significant differences were observed at 3 months (WMD 0.35; 95% CI -0.03 to 0.68, p = 0.034; I² =41%, p = 0.184), 1 year (WMD − 0.06; 95% CI -0.52 to 0.65, p = 0.831; I² =82.1%, p = 0.000) and 2 years (WMD − 0.10; 95% CI -0.32 to 0.13, p = 0.410; I² =0.0%, p = 0.441) postoperatively (Fig. 8).

Forest plot of scores related to back pain

Forest plot of scores related to leg pain
Publication bias
The potential publication bias was evaluated by Begg’ and Egger’ test, and the results showed that there was no obvious publication bias in all indicators. The results are shown in the table S2.
Discussion
A total of 6182 patients were included in this study, including 2339 patients in the decompression alone group and 3783 patients in the decompression plus fusion group. The operation time, intraoperative blood loss, postoperative complications, Oswestry disability index (ODI) scores and scores related to back and leg pain were analyzed. We found that decompression alone was superior to decompression plus fusion with respect to operative time and intraoperative blood loss, and there were no other differences between the two groups.
In terms of operation time and intraoperative blood loss, the conclusions were consistent with the results of all the included studies with relevant indexes: the operation time and intraoperative blood loss of the decompression group alone were less, and the reason for the higher heterogeneity was considered to be related to the different decompression and fusion methods, as well as the understanding of the standard operation procedures and the surgeons in various regions. In addition to decompression, the surgeon needs to perform cage or screw implantation, as well as intraoperative X-ray projection and other operations, which will prolong the operation time and intraoperative bleeding, which is consistent with various studies and systematic reviews [11, 17, 18].
No significant heterogeneity was observed in the reoperation either in the overall effect size or in the subgroup analysis. There were no significant differences in reoperation rates and postoperative complications between the decompression alone group and the decompression plus fusion group. Sato [30] found that among patients with lumbar spondylolisthesis, decompression alone was awssociated with more reoperation rates after at least 5 years of follow-up. But other studies [31, 32] found no gap between the two groups in degenerative spondylolisthesis patients. Wei [33] showed in a meta-analysis that no significant difference was found in reoperation between the two groups in short-term (< 4 years) or long-term (> 4 years). We did not find a difference in the randomized controlled trials or in the cohort studies, which is consistent with our finding that there was no difference between two groups in postoperative complications [34]. In addition to further progression of spondylolisthesis, facet joint invasion and degeneration of adjacent joints are important causes of reoperation [35]. Therefore, to reduce the reoperation rate of instrumental fusion surgery, attention should be paid to the accuracy of intraoperative pedicle screw implantation, and Robot-Assisted pedicle screw implantation is an effective way.
In terms of postoperative scores related to back and leg pain, we found no significant difference between the two groups at 3 months, 1 year, and 2 years after surgery. Similarly, Försth [11] found no significant difference between the two groups at 12 months in patients with degenerative spondylolisthesis patients. Similar findings have been confirmed by multiple studies [31, 36]. However, Chan [37, 38] found in two studies that patients with lumbar spondylolisthesis had better improvement in ODI scores in the fusion group than in the decompression alone group. Among the included studies in this paper, one RCT [36] and four cohort studies [15, 23, 24, 29, 36] showed no significant difference in ODI scores between the two groups. while Sigmundsson’s [28] study found that fusion surgery could bring better improvement in ODI scores, but also proposed that the statistical difference may not reach the minimum clinically significant difference. Similarly, Ghogawala [16] reported that the fusion group showed a higher ODI score improvement, but there was no statistical difference.
Previous studies [31, 38] have found that in patients with lumbar spondylolisthesis, there was no significant difference in back pain or leg pain between the two groups with or without fusion. Although the methods used to evaluate back pain and leg pain were slightly different in this study, the basic principles were the same and were analyzed as in other studies [33]. In patients with lumbar degenerative spondylolisthesis or spinal stenosis, Försth [11] found no difference between the two groups after surgery, while the multi-center cohort study conducted by Austevoll [36] et al. found that for patients with lumbar degenerative spondylolisthesis, the fusion group showed a higher improvement in low back pain at 12 months, and Chan [37] also found that the fusion group was associated with better improvement in back pain at 24 months. However, there was no significant difference in leg pain between the two groups. All the articles included in this study reported no significant difference in scores related to back and leg pain in patients with single-level lumbar spinal stenosis with spondylolisthesis [15, 23, 24, 28].
Since Briggs [39] first described lumbar fusion in 1944, lumbar interbody fusion has been widely used to treat a range of spinal diseases. It can stabilize the vertebral body in cases of instability caused by trauma, infection, degeneration, deformities, or iatrogenic factors [40]. As mentioned above, spinal fusion surgery has become the preferred surgical method for clinical surgeons as an auxiliary means of decompression. Although some scholars have always questioned the necessity of adding spinal fusion surgery after decompression, it has not attracted attention. However, in 2016, Ghogawala and Försth presented different research conclusions in their articles respectively, this necessity became the focus of debate. The relevant guidelines recommend the use of fusion surgery in patients with lumbar spinal stenosis and degenerative spondylolisthesis [41], while it is not recommended for patients with spinal stenosis without spondylolisthesis [42]. However, in this paper, we believe that fusion surgery should not be used routinely in the case of single-level lumbar spinal stenosis with degenerative spondylolisthesis, but research should seek to improve knowledge about individualized surgical treatment. One can not rule out that subgroups of patients can benefit from fusion surgery.
Limitations of the study
This study has some limitations. First of all, there is great heterogeneity in the evaluation indicators such as operation time and intraoperative loss, which is considered to be due to the differences between the operations and the differences between the operators, so it may be necessary to consider the consistency of surgical procedures in more studies. Secondly, for postoperative Scores related to back and leg pain, the pain assessment methods were different among different studies, including Numeric Rating Scale(NRS) and visual analogue scale(VAS)scores. Although the basic principles were consistent, there were confounding factors when analyzing the combined effect size in the analysis of low back pain and leg pain. Thirdly, most of the articles included in this study were cohort studies, and only three randomized controlled trials were included. The level of evidence was low, and there may be many potential confounding factors affecting the results, so a large number of randomized controlled trials are needed to obtain the results. Fourth, this study only focused on the most common type of lumbar spondylolisthesis, single-level spondylolisthesis with spinal stenosis, without exploring multi-level spondylolisthesis or multi-level spinal stenosis. More complex types of spondylolisthesis should be paid attention to in the later stage.
Conclusion
The results of this study showed that in the patients with single-level lumbar spinal stenosis and degenerative spondylolisthesis, the operation time and intraoperative blood loss of decompression alone were significantly better than those of decompression plus fusion. In terms of postoperative complications, there was no significant difference between decompression alone group and decompression plus fusion group in general, the subgroup analysis of the article type suggests that the incidence of postoperative complications in the cohort study is lower in the decompression alone group than in the decompression plus fusion group. There was no significant difference in reoperation, postoperative ODI scores and scores related to back and leg pain between decompression alone group and decompression plus fusion group. Therefore, this study concluded that decompression alone was superior to decompression plus fusion with respect to operative time and intraoperative blood loss, and there were no other differences between the two groups in patients with single-level lumbar spinal stenosis and degenerative spondylolisthesis. In addition, considering the longer operation cost and more intraoperative blood loss for decompression plus fusion, we recommend that decompression alone be preferred in patients with single-level lumbar spinal stenosis with degenerative spondylolisthesis.
Data availability
The data of this study are included in the manuscript and supplementary materials.
Abbreviations
- CI:
-
Confdence interval
- NRS:
-
Numeric Rating Scale
- ODI:
-
Oswestry disability index
- ORs:
-
Odds ratios
- PRISMA:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses
- RCTs:
-
Randomized control trials
- VAS:
-
Visual analogue scale
- WMD:
-
Weighted mean difference
References
Walter KL, O’Toole JE. Lumbar spinal stenosis. JAMA. 2022;328:310.
Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst Rev 2016, 2016:Cd010264.
Matz PG, Meagher RJ, Lamer T, Tontz WL Jr., Annaswamy TM, Cassidy RC, Cho CH, Dougherty P, Easa JE, Enix DE, et al. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2016;16:439–48.
Alvarez JA, Hardy RH Jr. Lumbar spine stenosis: a common cause of back and leg pain. Am Fam Physician. 1998;57:1825–34.
Bydon M, Alvi MA, Goyal A. Degenerative lumbar spondylolisthesis: definition, natural history, Conservative Management, and Surgical Treatment. Neurosurg Clin N Am. 2019;30:299–304.
Katz JN, Zimmerman ZE, Mass H, Makhni MC. Diagnosis and management of lumbar spinal stenosis: a review. JAMA. 2022;327:1688–99.
Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Blood E, Hanscom B, Herkowitz H, Cammisa F, Albert T, Boden SD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med. 2008;358:794–810.
Malmivaara A, Slätis P, Heliövaara M, Sainio P, Kinnunen H, Kankare J, Dalin-Hirvonen N, Seitsalo S, Herno A, Kortekangas P, et al. Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial. Spine (Phila Pa 1976). 2007;32:1–8.
Kepler CK, Vaccaro AR, Hilibrand AS, Anderson DG, Rihn JA, Albert TJ, Radcliff KE. National trends in the use of fusion techniques to treat degenerative spondylolisthesis. Spine (Phila Pa 1976). 2014;39:1584–9.
Kim CH, Chung CK, Choi Y, Kim MJ, Kim MJ, Shin S, Yang SH, Hwang SH, Kim DH, Park SB, Lee JH. Increased proportion of Fusion surgery for degenerative lumbar spondylolisthesis and changes in Reoperation Rate: a Nationwide Cohort Study with a minimum 5-Year follow-up. Spine (Phila Pa 1976). 2019;44:346–54.
Försth P, Ólafsson G, Carlsson T, Frost A, Borgström F, Fritzell P, Öhagen P, Michaëlsson K, Sandén B. A Randomized, Controlled Trial of Fusion surgery for lumbar spinal stenosis. N Engl J Med. 2016;374:1413–23.
Tosteson AN, Lurie JD, Tosteson TD, Skinner JS, Herkowitz H, Albert T, Boden SD, Bridwell K, Longley M, Andersson GB, et al. Surgical treatment of spinal stenosis with and without degenerative spondylolisthesis: cost-effectiveness after 2 years. Ann Intern Med. 2008;149:845–53.
Kim S, Mortaz Hedjri S, Coyte PC, Rampersaud YR. Cost-utility of lumbar decompression with or without fusion for patients with symptomatic degenerative lumbar spondylolisthesis. Spine J. 2012;12:44–54.
Inose H, Kato T, Yuasa M, Yamada T, Maehara H, Hirai T, Yoshii T, Kawabata S, Okawa A. Comparison of decompression, Decompression Plus Fusion, and Decompression Plus stabilization for degenerative spondylolisthesis: a prospective, randomized study. Clin Spine Surg. 2018;31:E347–52.
Austevoll IM, Hermansen E, Fagerland MW, Storheim K, Brox JI, Solberg T, Rekeland F, Franssen E, Weber C, Brisby H, et al. Decompression with or without Fusion in degenerative lumbar spondylolisthesis. N Engl J Med. 2021;385:526–38.
Ghogawala Z, Dziura J, Butler WE, Dai F, Terrin N, Magge SN, Coumans JV, Harrington JF, Amin-Hanjani S, Schwartz JS, et al. Laminectomy plus Fusion versus Laminectomy alone for lumbar spondylolisthesis. N Engl J Med. 2016;374:1424–34.
Abdel-Fattah AR, Bell F, Boden L, Ferry J, McCormick C, Ross M, Cameron I, Smith T, Baliga S, Myint PK. To fuse or not to fuse: the elderly patient with lumbar stenosis and low-grade spondylolisthesis. Systematic review and meta-analysis of randomised controlled trials. Surgeon. 2023;21:e23–31.
Shen Z, Guan X, Wang R, Xue Q, Zhang D, Zong Y, Ma W, Zhuge R, Liu Z, He C, et al. Effectiveness and safety of decompression alone versus decompression plus fusion for lumbar spinal stenosis with degenerative spondylolisthesis: a systematic review and meta-analysis. Ann Transl Med. 2022;10:664.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Higgins J, Thompson SG, Deeks JJ, Altman DGJN. -SAfePuP: cochrane handbook for systematic reviews of interventions version 5.1.0. the cochrane collaboration. 2008, 5:S38.
Inose H, Kato T, Sasaki M, Matsukura Y, Hirai T, Yoshii T, Kawabata S, Hirakawa A, Okawa A. Comparison of decompression, decompression plus fusion, and decompression plus stabilization: a long-term follow-up of a prospective, randomized study. Spine J. 2022;22:747–55.
Badhiwala JH, Leung SN, Jiang F, Wilson JRF, Akbar MA, Nassiri F, Witiw CD, Wilson JR, Fehlings MG. In-hospital course and complications of laminectomy alone Versus Laminectomy Plus Instrumented Posterolateral Fusion for lumbar degenerative spondylolisthesis: a retrospective analysis of 1804 patients from the NSQIP database. Spine (Phila Pa 1976). 2021;46:617–23.
Hua W, Wang B, Ke W, Xiang Q, Wu X, Zhang Y, Li S, Yang S, Wu Q, Yang C. Comparison of clinical outcomes following lumbar endoscopic unilateral laminotomy bilateral decompression and minimally invasive transforaminal lumbar Interbody Fusion for one-level lumbar spinal stenosis with degenerative spondylolisthesis. Front Surg. 2020;7:596327.
Joelson A, Nerelius F, Holy M, Sigmundsson FG. Reoperations after decompression with or without Fusion for L3-4 spinal stenosis with degenerative spondylolisthesis: a study of 372 patients in Swespine, the National Swedish Spine Register. Clin Spine Surg. 2022;35:E389–93.
Joelson A, Nerelius F, Holy M, Sigmundsson FG. Reoperations after decompression with or without fusion for L4-5 spinal stenosis with or without degenerative spondylolisthesis: a study of 6,532 patients in Swespine, the national Swedish spine register. Acta Orthop. 2021;92:264–8.
Kimura R, Yoshimoto M, Miyakoshi N, Hongo M, Kasukawa Y, Kobayashi T, Kikuchi K, Okuyama K, Kido T, Hirota R, et al. Comparison of posterior lumbar Interbody Fusion and Microendoscopic muscle-preserving Interlaminar Decompression for degenerative lumbar spondylolisthesis with > 5-Year follow-up. Clin Spine Surg. 2019;32:E380–5.
Matsudaira K, Yamazaki T, Seichi A, Takeshita K, Hoshi K, Kishimoto J, Nakamura K. Spinal stenosis in grade I degenerative lumbar spondylolisthesis: a comparative study of outcomes following laminoplasty and laminectomy with instrumented spinal fusion. J Orthop Sci. 2005;10:270–6.
Sigmundsson FG, Jönsson B, Strömqvist B. Outcome of decompression with and without fusion in spinal stenosis with degenerative spondylolisthesis in relation to preoperative pain pattern: a register study of 1,624 patients. Spine J. 2015;15:638–46.
Yagi M, Fujita N, Okada E, Tsuji O, Nagoshi N, Tsuji T, Nakamura M, Matsumoto M, Watanabe K. Comparisons of direct costs, outcomes, and cost-utility of decompression surgery with fusion versus decompression alone for degenerative lumbar spondylolisthesis. J Orthop Sci. 2018;23:653–7.
Sato S, Yagi M, Machida M, Yasuda A, Konomi T, Miyake A, Fujiyoshi K, Kaneko S, Takemitsu M, Machida M, et al. Reoperation rate and risk factors of elective spinal surgery for degenerative spondylolisthesis: minimum 5-year follow-up. Spine J. 2015;15:1536–44.
Staartjes VE, Schröder ML. Effectiveness of a decision-making protocol for the Surgical treatment of lumbar stenosis with Grade 1 degenerative spondylolisthesis. World Neurosurg. 2018;110:e355–61.
Vorhies JS, Hernandez-Boussard T, Alamin T. Treatment of degenerative lumbar Spondylolisthesis with Fusion or Decompression alone results in similar rates of reoperation at 5 years. Clin Spine Surg. 2018;31:E74–9.
Wei FL, Zhou CP, Gao QY, Du MR, Gao HR, Zhu KL, Li T, Qian JX, Yan XD. Decompression alone or decompression and fusion in degenerative lumbar spondylolisthesis. EClinicalMedicine. 2022;51:101559.
Kuo CC, Merchant M, Kardile MP, Yacob A, Majid K, Bains RS. In degenerative spondylolisthesis, unilateral laminotomy for bilateral decompression leads to less reoperations at 5 years when compared to posterior decompression with Instrumented Fusion: a propensity-matched retrospective analysis. Spine (Phila Pa 1976). 2019;44:1530–7.
Perna A, Velluto C, Smakaj A, Tamburrelli F, Borruto MI, Santagada DA, Gorgoglione FL, Liuzza F, Proietti L. Positioning accuracy and facet joints violation after percutaneous pedicle screws placement with robot-assisted versus fluoroscopy-guided technique: systematic review and meta-analysis. J Neurosci Rural Pract. 2023;14:406–12.
Austevoll IM, Gjestad R, Solberg T, Storheim K, Brox JI, Hermansen E, Rekeland F, Indrekvam K, Hellum C. Comparative effectiveness of Microdecompression alone vs Decompression Plus Instrumented Fusion in lumbar degenerative spondylolisthesis. JAMA Netw Open. 2020;3:e2015015.
Chan AK, Bisson EF, Bydon M, Glassman SD, Foley KT, Potts EA, Shaffrey CI, Shaffrey ME, Coric D, Knightly JJ, et al. A comparison of minimally invasive transforaminal lumbar interbody fusion and decompression alone for degenerative lumbar spondylolisthesis. Neurosurg Focus. 2019;46:E13.
Chan AK, Bisson EF, Bydon M, Glassman SD, Foley KT, Potts EA, Shaffrey CI, Shaffrey ME, Coric D, Knightly JJ, et al. Laminectomy alone versus fusion for grade 1 lumbar spondylolisthesis in 426 patients from the prospective quality outcomes database. J Neurosurg Spine. 2018;30:234–41.
Briggs H, Milligan PRJJ. CHIP FUSION OF THE LOW BACK FOLLOWING EXPLORATION OF THE SPINAL CANAL. 1944, 26.
Resnick DK, Schmidt BT. Update on spinal Fusion. Neurol Clin. 2022;40:261–8.
Resnick DK, Watters WC 3rd, Sharan A, Mummaneni PV, Dailey AT, Wang JC, Choudhri TF, Eck J, Ghogawala Z, Groff MW, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 9: lumbar fusion for stenosis with spondylolisthesis. J Neurosurg Spine. 2014;21:54–61.
Resnick DK, Watters WC 3rd, Mummaneni PV, Dailey AT, Choudhri TF, Eck JC, Sharan A, Groff MW, Wang JC, Ghogawala Z, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 10: lumbar fusion for stenosis without spondylolisthesis. J Neurosurg Spine. 2014;21:62–6.
Acknowledgements
Not applicable.
Funding
This work was funded by Tianjin Key Project of Applied Basic Research (22JCZDJC00250), Tianjin Health Science and Technology Key Discipline Special Project (TJWJ2022XK016), and Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-064B).
Author information
Authors and Affiliations
Contributions
The study’s concept and design were contributed to by STW and CHY. Material preparation, data collection and analysis were performed by CHY, LG, XD, LYQ and YHZ. CS and CHY assessed the bias in articles, and disagreements were settled by CHY. All the authors contributed to the draft of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cheng, H., Luo, G., Xu, D. et al. Decompression alone or fusion in single-level lumbar spinal stenosis with spondylolisthesis? A systematic review and meta analysis. BMC Musculoskelet Disord 25, 726 (2024). https://doi.org/10.1186/s12891-024-07641-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07641-5