
Abstract
Background
There is limited evidence of the associations between postural-derived sitting time, waist-worn derived sedentary time and children’s health and the moderation effect of physical activity (PA). This study examined associations of children’s device-measured sitting time with cardiometabolic health risk factors, including moderation by physical activity.
Methods
Cross-sectional baseline data from children (mean-age 8.2 ± 0.5 years) in Melbourne, Australia (2010) participating in the TransformUs program were used. Children simultaneously wore an activPAL to assess sitting time and an ActiGraph GT3X to assess sedentary time and physical activity intensity. Cardiometabolic health risk factors included: adiposity (body mass index [BMI], waist circumference [WC]), systolic and diastolic blood pressure (SBP, DBP), high-density lipoprotein (HDL), low-density lipoprotein (LDL), cholesterol, triglycerides, fasting plasma glucose (FPG), serum insulin, and 25-hydroxyvitaminD (25[OH]D). Linear regression models (n = 71–113) assessed associations between sitting time with each health risk factor, adjusted for different PA intensities (i.e. light [LIPA], moderate-vigorous intensities [MVPA], separately on each model), age, sex, adiposity, and clustering by school. Interaction terms examined moderation. The analyses were repeated using device-measured sedentary time (i.e. ActiGraph GT3X) for comparison.
Results
Sitting time was positively associated with SBP (b = 0.015; 95%CI: 0.004, 0.026), DBP (b = 0.012; 95%CI:0.004, 0.020), and FPG (b = 0.001; 95%CI: 0.000, 0.000), after adjusting for higher PA intensities. The association between sitting time and insulin (b = 0.003; 95%CI: 0.000, 0.006) was attenuated after adjusting for higher PA intensities. When the models were adjusted for LIPA and MVPA, there was a negative association with LDL (b=-0.001; 95%CI: -0.002, -0.000 and b=-0.001; 95%CI: -0.003, -0.000, respectively). There was a negative association of sedentary time with WCz (b=-0.003; 95%CI: -0.005, 0.000) and BMIz (b=-0.003; 95%CI: -0.006, -0.000) when the models were adjusted by MVPA. Sedentary time was positively associated with triglycerides (b = 0.001; 95%CI: 0.000, 0.001) but attenuated after adjusting for MVPA. No evidence of moderation effects was found.
Conclusions
Higher volumes of sitting and sedentary time were associated with some adverse associations on some cardiometabolic health risk factors in children. These associations were more evident when sitting time was the predictor. This suggests that reducing time spent sitting may benefit some cardiometabolic health outcomes, but future experimental research is needed to confirm causal relationships and identify the biological mechanisms that might be involved.
Trial registration
Australian New Zealand Clinical Trials Registry: ACTRN12609000715279.
Similar content being viewed by others

Background
Sedentary behaviours, characterised as waking behaviours with an energy expenditure ≤ 1.5 metabolic equivalents (METs) while in a sitting or reclining posture [1], have been associated with unhealthy cardiometabolic profiles in adults [2]. There has been significant interest in examining both cross-sectional and longitudinal associations between sedentary time volumes and patterns typically assessed using hip-worn devices, with a range of children’s health outcomes including adiposity markers [3,4,5], cardiorespiratory fitness [3], cardiometabolic risk [6] among children and adolescents. However, these associations have been mixed [4, 7,8,9,10,11,12]. Some studies amongst youth have reported positive associations between sedentary time and cardiometabolic risk factors, which attenuate when adjusted for moderate- to vigorous-intensity physical activity (MVPA) [13, 14]. In contrast, some studies have shown associations remain unchanged after adjustment for MVPA [15, 16]. This may partly relate to the assessment used, which traditionally relies on accelerometer cut-points to estimate periods of ‘little too low movement’ and does not differentiate between postures when sitting or standing still [17, 18].
While a novel computational method has been developed that classifies sitting posture from hip-mounted accelerometers among children [19], postural-detection devices (e.g. activPAL) can differentiate between sitting and standing but have rarely been used to explore associations between sitting time and cardiometabolic risk factors among youth [20, 21]. In the studies that have assessed sitting using postural devices, Contardo Ayala et al. [21] found no cross-sectional associations between activPAL-measured sitting time and adiposity markers (body mass index [BMI] or waist circumference [WC] z-scores) among 219 adolescents (age = 14.9 ± 1.6 years). While some evidence of associations has been observed for components of sitting patterns (i.e., breaks, prolonged sitting) with adiposity and high-density lipoprotein cholesterol (HDL) among 118 children (aged 11–12 years) [20], total sitting volume was not reported due to collinearity in the model. Further research using postural devices is needed to better understand associations between sitting time and cardiometabolic risk factors in children.
Different analytical methods have been used to examine associations between movement behaviours and cardiometabolic health [14]. Historically, the focus has been on MVPA and sedentary time, often with adjustments for other intensities and assessed using one device [12]. However, little research has examined the potential health benefit of light-intensity physical activity (LIPA), and the use of different devices to capture sitting and physical activity of different intensities on these associations. It is important to understand the potential health benefits of LIPA, as it represents a substantial portion of daily physical activity in adolescents [22]. In addition, examining whether physical activity moderates associations between sitting and health, and which intensity of activity moderates the associations to a greater extent, has rarely been explored despite this potentially providing insights into how much physical activity is needed to counteract the detrimental effects of too much sitting. However, to our knowledge, the moderation effect of different physical activity intensities on the association between sitting time and health markers has only been reported in one study [21]. That study found that LIPA and not MVPA moderated the relationship between sitting and adiposity markers (i.e. BMI and WC) in adolescents [21], with negative associations between sitting and adiposity markers in those who engaged in greater amounts of LIPA. These findings suggest that increasing time spent in LIPA may attenuate the potential deleterious association of high levels of sitting on health. However, whether different PA intensities moderate relationships between sitting and other cardiometabolic risk factors among children has yet to be examined in this way.
The aim of this study was to examine the cross-sectional associations between children’s device-measured sitting time (i.e. activPAL3) and cardiometabolic risk factors and to determine whether physical activity of varying intensities moderated associations between sitting time and cardiometabolic risk factors. We also repeated the analyses using device-measured sedentary time (i.e. ActiGraph GT3X) for comparison.
Methods
Study population
Baseline data from the TransformUs randomised controlled trial [23] were analysed. TransformUs was an 18-month, four-arm cluster-randomized controlled trial within primary schools in Melbourne, Australia (2010-12), aiming to increase children’s physical activity, decrease sedentary behaviour, and optimize health outcomes [23, 24]. TransformUs was approved by the Deakin University Human Research Ethics Committee Group (141–2009), Victorian Department of Education and Early Childhood Development (2009_000344) and Catholic Education Office (1545).
Recruitment details have been published previously [24]. In brief, schools within a 50 km radius from the Melbourne Central Business District were identified. The school selection criteria included: enrolment greater than 300 students, having at least two grade three classes, being co-educational (i.e. no single-sex schools) and being located in the first, third or fifth quintile of the Socio-economic Index for Areas (SEIFA; for socio-economic diversity) [25]. In total, 20 schools were recruited. All grade three students were invited to consent to the opt-in evaluation assessments (n = 1606). In total, 599 parents provided written informed consent for their child to participate in evaluation assessments (37%), and of these, 532 consented to wear an activPAL. Due to equipment availability, a random sample of 216 children wore an activPAL at baseline. Parental consent to collect children’s blood pressure and blood samples was obtained for 477 and 219 children, respectively. Baseline data collection occurred between February to June 2010.
Measures
Demographics
Children self-reported their sex and age in a survey completed during class time.
Physical activity, sitting and sedentary time
Participants were asked to concurrently wear two devices during waking hours (except for water-based activities) for eight days. Children wore an activPAL3 inclinometer (PAL Technologies Ltd, Glasgow, UK) on the front of their right thigh (at the mid-point), attached via an elastic belt. The activPAL3 is considered a valid measure of sitting [26]. Children also wore an ActiGraph GT3X (ActiGraph LLC, Pensacola, FL., USA) on an elastic belt on their right hip. The ActiGraph is commonly used to quantify physical activity in children [27]. All data were extracted using manufacturer software (activPAL Professional v7.2.29 and Actilife v6.11.18) and processed using a customised Microsoft Excel macro in 15-second periods. Consecutive zero counts for 20 min were used as non-wear time for both devices [28, 29]. For each device, data were included in the analysis if participants had at least four valid days (including a weekend day), which was defined as ≥ 8 h/day of wear time for weekdays and ≥ 7 h/day for weekend days [30, 31].
From the activPAL data, the total volume of sitting was computed as the average duration per valid day (mins/day). From the ActiGraph data, Freedson age-adjusted cut-points [32] were used to obtain average time spent in sedentary time (< 100 counts/minutes), LIPA (i.e. 101 counts/minute to 3.99 METs) and MVPA (≥ 4 METS for those < 18years, based on age-specific thresholds [e.g. for a 8 year old is 802 counts/minute]) per valid day. LIPA was further dichotomised into low light-intensity physical activity (low-LIPA) (i.e. 101–799 counts/minute) and high light-intensity physical activity (high-LIPA) (i.e. 800 counts/minute to 3.99 METs). The cut-point of > 800 counts/min was based on previous research as it captures static LIPA, such as standing as high-LIPA [17, 33]. Prior to the analysis, all activPAL and ActiGraph-derived outcome variables were standardised (to account for variations in the amount of time individuals wear the device) according to total wear time during the period of interest as follows: (duration of ‘X’ within waking hours/wear time within waking hours) multiplied by 960 min, where ‘X’ is the activity (e.g., sitting, LIPA, low-LIPA, high-LIPA and MVPA) and waking hours are equivalent to 960 min–16 h.
Anthropometric measures
Measurements were taken at the schools by trained researchers using standardised protocols. Stature was measured to the nearest 0.1 cm using portable stadiometers (SECA 0123, SECA, Hamburg, Germany) and body mass to the nearest 0.1 kg using portable electronic scales (InnerScan 50; TANITA, Illinois, USA). WC was assessed using a flexible measuring tape at the narrowest, or middle, point between the bottom rib and the iliac crest. Two measurements were taken, with a third measure taken when a difference of over 0.5 cm (stature), 0.5 kg (body mass) and 1 cm (WC) was noted. BMI (kg/m2) was calculated from body mass and stature, and participants were categorised according to the International Obesity Task Force definitions of healthy weight or overweight/obese [34]. BMI z-scores (BMIz) were calculated and converted to z-values, standardized for age and sex, using the World Health Organization Child Growth Standards [35]. WC z-scores (WCz) were calculated from raw anthropometric data using Stata function with UK growth chart (zanthro) [36]. Australian percentile curves for WC were utilised to determine age- and sex-specific waist circumference percentiles, where a WC ≥ 90th percentile was used to classify obesity and overweight was defined as a WC ≥ 75th percentile but less than the 90th percentile [37].
Blood pressure
Participants were asked to sit quietly for two minutes, then blood pressure (BP) was measured from the right arm using a paediatric cuff (OMRON HEM-907, Kyoto, Japan). Three measures were taken one-minute apart, on two different occasions one week apart. Average systolic and diastolic BP were calculated from four measures after removing the first measurement from weeks one and two [38].
Blood biomarkers
Following an overnight fast, a morning blood sample was collected from each child with parental consent by a trained phlebotomist at a local commercial pathology clinic (the same pathology company was used for all blood samples). All children were provided with a dermal anaesthetic topical cream (EMLA®) to apply 1 h before the blood collection. The following biomarkers were assessed by the pathology laboratory using standard laboratory techniques: HDL-cholesterol, LDL- cholesterol, total cholesterol, triglycerides, fasting plasma glucose (FPG), serum insulin, and serum 25-hydroxyvitamin D (25[OH]D). All assays were performed according to manufacturer’s instructions, and all samples were run in duplicate. Biomarker ranges considered as acceptable are presented in the Additional file 1.
Statistical analysis
Statistical analyses were conducted using Stata 18.0 (Stata-Corp LPD46XX). Statistical significance was set at p < 0.05. Shapiro–Wilk test were used to check the normality of the data. Pearson’s correlations were used to test for multicollinearity, confirming the absence of collinearity between the variables studied (i.e. the correlation between sitting [from activPAL] and each physical activity intensity variable [from ActiGraph] ranged between − 0.06 and 0.05). Collinearity was confirmed between sedentary time [from ActiGraph] and LIPA [from ActiGraph].
The main association of sitting (minutes/day) with cardiometabolic risk factors was examined using separate regression models (Model A) for each cardiometabolic health marker (11 models in total). The associations with cardiometabolic risk factors were further explored by adjusting for each PA intensity (LIPA and MVPA) separately, age, sex, adiposity (BMIz), season in which the assessment was conducted, and clustering by school (Models B to E). Moderation by LIPA, low-LIPA, high-LIPA, and MVPA were also examined by adding interaction terms to the respective main regression models and checking p values. The main association of sedentary time (minutes/day) with cardiometabolic risk factors was examined using separate regression models (Model A) for each cardiometabolic health marker (11 models in total). The associations with cardiometabolic risk factors were further explored by adjusting for MVPA, age, sex, adiposity (BMIz), season in which the assessment was conducted, and clustering by school (Model B). Moderation by MVPA was also examined. All moderator variables were centered around the individual variable mean.
Results
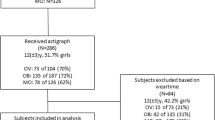
activPAL data: In total, 113 children provided valid activPAL data, of whom 103 had valid ActiGraph data. For the analyses, 113 children had anthropometric measures, 111 had BP measures, and 71 had blood biomarkers. For the analysis of the ActiGraph data, 334-335 children had anthropometric measures, 323 had BP measures, and 159 had blood biomarkers.
Children (mean ± SD, age 8.1 ± 0.4 years, 58% girls) spent an average of 59% of their waking hours sitting, 41% in LIPA (33% and 8% in low and high LIPA, respectively), and 4% in MVPA (Table 1). All participants had their biomarkers in the acceptable range.
Associations of sitting time with health risk biomarkers
Table 2 reveals a positive association between sitting time and SBP, DBP, and FPG, persisting even after adjustments for age, sex, adiposity, season in which the assessment was conducted, and various physical activity intensity variables in the model. Similarly, sitting time was positively associated with insulin, but this association was attenuated after adjusting for the physical activity intensity variables. There was a negative association with LDL in the LIPA (i.e. total LIPA and low-LIPA) and MVPA adjusted models.
Associations of sedentary time with health risk biomarkers
There was a negative association with WCz and BMIz only when the models were adjusted by MVPA. Sedentary time was positively associated with triglycerides but attenuated after adjusting for MVPA (Table 3).
Moderation analysis
No significant interactions between sitting (i.e. SBP, p = 0.446; DBP, p = 0.958; LDL, p = 0.768; FPG, p = 0.160; and insulin, p = 0.117) and sedentary time (i.e. WCz, p = 0.569; BMIz, p = 0.599; and triglycerides, p = 0.388) and any of the physical activity intensity variables were found for the significant models (prior and after the adjustment for physical activity intensity).
Discussion
This cross-sectional study aimed to examine associations between activPAL-measured sitting time and cardiometabolic risk factors and to determine whether ActiGraph-measured LIPA and MVPA moderated the relationship between sitting and cardiometabolic risk factors among children. Sitting time was unfavourably associated with SBP, DBP, and FPG and these associations persisted after adjusting for each PA intensity separately. There was a trend for sitting time to be detrimentally associated with insulin, however, this association was attenuated after adjusting for the physical activity intensity variables. Also, there was a negative association with LDL, in the unexpected direction, in the LIPA (i.e. total LIPA and low-LIPA) and MVPA adjusted models. When sedentary time was the predictor, an unfavourably association was observed between WCz and BMIz, but only in models adjusted for MVPA. Sedentary time was positively associated with triglycerides; however, this association weakened after adjusting for MVPA. There was, however, no significant moderation effects of LIPA (total, low-LIPA, high-LIPA) nor MVPA on associations between children’s sitting and sedentary time and cardiometabolic risk factors, which was inconsistent with previous research in adolescents.
While the sample size was small, to our knowledge, this is the first study to show a significant, detrimental association between device-based measures of sitting time and BP and FPG, among children aged 7–10 years. A previous study that measured sitting time using activPALs in older children (11–12 years) found no association with cardiometabolic risk outcomes after adjusting for MVPA [20]. Although demographically comparable, the total volume of MVPA by Stockwell (2019) was double that recorded in the current study (90 vs. 38.2 min/day). The amount of time spent on MVPA in the current study is consistent with the amount of MVPA that has previously been reported for this age group [39]. The total amount of MVPA that might be needed to attenuate the association of sitting on FPG (e.g. 60 min for adults [40]) is arguably unrealistic based on population prevalence data; therefore, it is necessary to further explore if engaging in more LIPA and/or MVPA could benefit health among young people. For example, studies using isotemporal substitution to explore the effects of replacing sedentary time with PA of different intensities have found that replacing sedentary time with MVPA, but not LIPA, was favourably associated with body fat percentage [41]. Longitudinal and experimental research with larger sample sizes and similar methods to measure sitting time (activPAL) are needed to determine if the findings of this study are spurious or reflect the actual associations of sitting time and cardiometabolic health makers among children.
The current study found an unfavourable association between sitting time and SBP and DBP, which also contrasts previous research [20]. The mechanisms responsible for the potential impact of excessive sitting and BP are unclear (e.g. sitting-induced reductions in blood flow and an increase in the accumulation of extravascular fluid in the legs [42] and reductions in conduit vessel flow and elevations in vasoactive mediators [42]), and there is limited evidence of this relationship among children. Previous studies, indicate a positive association between sedentary time [20, 43], using hip-mounted devices, and higher levels of SBP/DBP in children and adolescents. However, contrasting findings exist, with some studies reporting null associations [44,45,46], highlighting the complex relationship between sitting/sedentary time and blood pressure in youth. Longer-term BP monitoring and experimental research are needed to explore the association between sitting time and BP. A weak unfavourable association between sitting time and insulin have been found in this study and similar to the finding among adults [47], however this association has not been found among adolescents [48]. The unexpected association with LDL observed in our study warrants careful consideration. While the explanation remains unclear, several factors could contribute to this unexpected finding. For example, the relationship between sitting time and LDL may be influenced by a complex interplay of factors, such as dietary habits, genetic predispositions, and overall lifestyle. In addition, the inclusion of LIPA in the model may have affected the results due to sitting time and LIPA often being highly inversely correlated. It may be that children who engage in higher levels of LIPA accumulate different patterns of sitting, which are known to have varied relationships with health outcomes. Further exploration of these factors may provide further insights.
This study found no associations between sitting and the remaining cardiometabolic risk factors (i.e. WCz, BMIz, Cholesterol, HDL, Triglycerides and serum 25[OH]D), which is consistent with previous literature [12]. Only one previous study showed that prolonged sitting (bouts ≥ 30 min) was negatively associated with adiposity markers and positively associated with HDL cholesterol [20]. However, participants in the study by Stockwell et al. were several years older (aged 11–12 years) than those participants in our study. Therefore, the younger children in the present study may have had less exposure to higher volumes of sitting to impact cardiometabolic risk factors, although studies have shown an impact at early ages [29]. Importantly, children in the current study were generally healthy (normal BP, blood biomarkers and only n = 28 overweight/obese), therefore, finding associations between total volume sitting and health can be more challenging, and sitting patterns might play an important role in these associations. The adverse relationship between total volume of sedentary time and WC and BMI aligns, which was non-significant when sitting time was the predictor, with findings from prior cross-sectional and longitudinal studies [49]. However, while evidence suggests a connection between sedentary time and adiposity markers, it remains inconclusive and lacks evidence of causation [7]. Nonetheless, the evidence supporting the relationship between sedentary time and adiposity markers appears to be increasing over time [49]. The adverse association with triglycerides aligns with previous research [43]. For instance, Strizich et al. [44] demonstrated an association between sedentary time and triglycerides, which aligns with the findings of this study. However, unlike our study, they did not observe a similar relationship with HDL.
In the current study, children spent 59% of their day sitting, which is consistent with previous studies that have reported between 57 and 78% of waking time spent sitting, measured with activPALs [31, 50, 51]. Children in this study also spent 40% of their waking hours in LIPA and only 4% in MVPA; however, neither LIPA nor MVPA moderated the relationship between sitting and cardiometabolic risk factors. In a previous study, sitting time was not associated with adiposity markers (BMIz and WCz), but LIPA and low-LIPA showed to moderate the detrimental association between sitting and BMIz and WCz in adolescents [21]. The inconsistent findings between this study in children and adolescents could be partly because adolescents had a higher volume of sitting (i.e., 59% vs. 68% of the day, respectively) and less volume of LIPA (27% vs. 39%, respectively). It is also possible that the very low percentage of waking hours spent in MVPA (∼4%) is not enough to overcome the effects of two-thirds of the day spent sitting by the children. Experimental research is needed to understand if, for example, replacing sitting time with LIPA is beneficial for children and adolescents in the long term.
This study found no associations between sitting and sedentary time and serum 25[OH]D when the models were adjusted for the season in which the assessment was conducted. To our knowledge, no previous studies have examined the relationship between device-assessed sitting time and circulating vitamin D in children. However, a previous study suggested that higher self-reported screen time was related to reduced serum concentrations of 25[OH]D in 8–9 year olds (n = 1464, not adjusted for MVPA) [52], but not 12–17 year olds (n = 1152, adjusted for MVPA) [53]. It could be that the deleterious impacts of sitting, which might be attributed to lower sun exposure due to sitting indoors, is counterbalanced with higher intensity physical activities (e.g. outdoor play/MVPA), which is likely to be performed outdoors (Cleland et al., 2010). Furthermore, considering that 72% of the data was collected during summer and autumn, significant sun exposure likely occurred during this study. Participation in outdoor play and MVPA is typically greater amongst children than adolescents, which may also partly explain the findings in the current study. Further research focusing on associations between sitting and vitamin D is needed to clarify the role of PA (i.e. indoors v outdoors). In contrast to previous cross sectional and longitudinal research (e.g. increase in sedentary time was unfavourably associated with changes in cardiometabolic score, triglycerides and DBP) [6], this study did not find any associations with other cardiometabolic makers (i.e. BP, Cholesterol, HDL, LDL, FPG, serum 25[OH]D and insulin). This divergence underscores the complexity of the relationship between sedentary behaviour and cardiometabolic health, potentially influenced by various factors such as sample characteristics, measurement techniques, and confounding variables.
Strengths of this study included the use of device-based assessments of sitting time (i.e. postural detection device) and PA of different intensities (i.e. actigraphy), the inclusion of a range of cardiometabolic risk factors among children, as well as the use of WC as a measure of central adiposity, given that BMI, while widely used, does not distinguish lean and fat mass. The limitations of this study include the use of cross-sectional data collected in 2010 and the small sample size, which may limit statistical power and the generalisability of the findings to the wider population. Nonetheless, this study contributes uniquely to the literature by employing both activPAL and ActiGraph devices in children to explore their associations with health markers and the moderation effects of physical activity. However, while the data were collected in 2010 and patterns of sitting (and activities undertaken while sitting) may have changed, the device used to capture sitting time has undergone minor changes and relationships between volumes of sitting time and health outcomes are likely to be constant [54]. The study included a generally healthy sample, which may limit the ability to find associations with health outcomes. A further limitation is that participants had to remove the monitors for water-based activities. It is possible that physical activity levels were underestimated as water activities were not included. Use of waterproof wearable monitors may overcome this limitation in future studies. Given the study’s limitations and the scarcity of literature with which to compare our findings, the results should be considered cautiously.
Conclusions
Our findings indicate that excessive sitting time is associated with some negative associations on cardiometabolic risk factors in children, suggesting that reducing the amount of time spent sitting could be a potential intervention to improve cardiometabolic health outcomes in children. However, further longitudinal and experimental studies are required to elucidate the relationship between sitting time and cardiometabolic health outcomes in children, and to inform targeted interventions to mitigate the adverse effects of sitting and sedentary time on health outcomes in children. Also, to examine the interplay between sitting time and different intensities of physical activity in relation to cardiometabolic risk factors also warranted.
Data availability
The dataset used for the current study could be made available on reasonable request, as the datasets are not publicly available due to ethical restrictions (participants have not consented to the use of their data for purposes other than those of which they originally consented)
Abbreviations
- BMI:
-
body mass index
- BP:
-
blood pressure
- DART:
-
Diabetes Australia Research Trust
- DBP:
-
diastolic blood pressure
- FPG:
-
fasting plasma glucose
- HDL:
-
high-density lipoprotein
- High-LIPA:
-
high light-intensity physical activity
- LDL:
-
low-density lipoprotein
- LIPA:
-
light-intensity physical activity
- Low-LIPA:
-
low light-intensity physical activity
- METs:
-
metabolic equivalents
- MVPA:
-
moderate- to vigorous-intensity physical activity
- NHMRC:
-
National Health and Medical Research Council
- PA:
-
physical activity
- SBP:
-
systolic blood pressure
- SEIFA:
-
Socio-economic Index for Areas
- WC:
-
waist circumference
- 25[OH]D:
-
25-hydroxyvitaminD
References
Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary Behavior Research Network (SBRN) - terminology Consensus Project process and outcome. Int J Behav Nutr Phys Act. 2017;14(1):75.
Young DR, Hivert MF, Alhassan S, Camhi SM, Ferguson JF, Katzmarzyk PT, et al. Sedentary Behavior and Cardiovascular Morbidity and Mortality: A Science Advisory from the American Heart Association. Circulation. 2016;134(13):e262–79.
Jones MA, Skidmore PM, Stoner L, Harrex H, Saeedi P, Black K, et al. Associations of accelerometer-measured sedentary time, sedentary bouts, and physical activity with adiposity and fitness in children. J Sports Sci. 2020;38(1):114–20.
Marques A, Minderico C, Martins S, Palmeira A, Ekelund U, Sardinha LB. Cross-sectional and prospective associations between moderate to vigorous physical activity and sedentary time with adiposity in children. Int J Obes (Lond). 2016;40(1):28–33.
Santos DA, Magalhães JP, Júdice PB, Correia IR, Minderico CS, Ekelund U, et al. Fitness mediates activity and sedentary patterns associations with Adiposity in Youth. Med Sci Sports Exerc. 2019;51(2):323–9.
Júdice PB, Hetherington-Rauth M, Northstone K, Andersen LB, Wedderkopp N, Ekelund U et al. Changes in Physical Activity and Sedentary Patterns on Cardiometabolic Outcomes in the Transition to Adolescence: International Children’s Accelerometry Database 2.0. J Pediatr. 2020;225:166– 73.e1.
Biddle SJ, Garcia Bengoechea E, Wiesner G. Sedentary behaviour and adiposity in youth: a systematic review of reviews and analysis of causality. Int J Behav Nutr Phys Act. 2017;14(1):43.
Biddle SJH, Pearson N, Salmon J. Sedentary behaviors and adiposity in Young people: causality and conceptual model. Exerc Sport Sci Rev. 2018;46(1):18–25.
Cliff DP, Hesketh KD, Vella SA, Hinkley T, Tsiros MD, Ridgers ND, et al. Objectively measured sedentary behaviour and health and development in children and adolescents: systematic review and meta-analysis. Obes Rev. 2016;17(4):330–44.
Chaput J-P, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, et al. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: summary of the evidence. Int J Behav Nutr Phys Activity. 2020;17(1):141.
Oliveira RGd, Guedes DP, Physical Activity S, Behavior. Cardiorespiratory Fitness and metabolic syndrome in adolescents: systematic review and Meta-analysis of Observational evidence. PLoS ONE. 2016;11(12):e0168503.
Skrede T, Steene-Johannessen J, Anderssen SA, Resaland GK, Ekelund U. The prospective association between objectively measured sedentary time, moderate-to-vigorous physical activity and cardiometabolic risk factors in youth: a systematic review and meta-analysis. Obes Rev. 2019;20(1):55–74.
Renninger M, Hansen BH, Steene-Johannessen J, Kriemler S, Froberg K, Northstone K, et al. Associations between accelerometry measured physical activity and sedentary time and the metabolic syndrome: a meta-analysis of more than 6000 children and adolescents. Pediatr Obes. 2020;15(1):e12578.
Froberg A, Raustorp A. Objectively measured sedentary behaviour and cardio-metabolic risk in youth: a review of evidence. Eur J Pediatr. 2014;173(7):845–60.
Mitchell JA, Pate RR, Beets MW, Nader PR. Time spent in sedentary behavior and changes in childhood BMI: a longitudinal study from ages 9 to 15 years. Int J Obes (Lond). 2013;37(1):54–60.
Cliff DP, Okely AD, Burrows TL, Jones RA, Morgan PJ, Collins CE, et al. Objectively measured sedentary behavior, physical activity, and plasma lipids in overweight and obese children. Obes (Silver Spring). 2013;21(2):382–5.
Ridgers ND, Salmon J, Ridley K, O’Connell E, Arundell L, Timperio A. Agreement between activPAL and ActiGraph for assessing children’s sedentary time. Int J Behav Nutr Phys Act. 2012;9(1):15.
Hardy LL, Hills AP, Timperio A, Cliff D, Lubans D, Morgan PJ, et al. A hitchhiker’s guide to assessing sedentary behaviour among young people: deciding what method to use. J Sci Med Sport. 2013;16(1):28–35.
Carlson JA, Ridgers ND, Nakandala S, Zablocki R, Tuz-Zahra F, Bellettiere J, et al. CHAP-child: an open source method for estimating sit-to-stand transitions and sedentary bout patterns from hip accelerometers among children. Int J Behav Nutr Phys Act. 2022;19(1):109.
Stockwell SL, Smith LR, Weaver HM, Hankins DJ, Bailey DP. Associations of sitting behavior patterns with cardiometabolic risk in children: the Sit Less for Health cross-sectional study. J Phys Act Health. 2019;12(10):856–42.
Contardo Ayala AM, Salmon J, Dunstan DW, Arundell L, Timperio A. Does light-intensity physical activity moderate the relationship between sitting time and adiposity markers in adolescents? J Sport Health Sci. 2022;11(5):613–9.
Contardo Ayala AM, Salmon J, Dunstan DW, Arundell L, Parker K, Timperio A. Longitudinal changes in sitting patterns, physical activity, and Health outcomes in adolescents. Child [Internet]. 2019; 6(1).
Salmon J, Arundell L, Cerin E, Ridgers ND, Hesketh KD, Daly RM, et al. Transform-Us! Cluster RCT: 18-month and 30-month effects on children’s physical activity, sedentary time and cardiometabolic risk markers. Br J Sports Med. 2023;57(5):311–9.
Salmon J, Arundell L, Hume C, Brown H, Hesketh K, Dunstan DW, et al. A cluster-randomized controlled trial to reduce sedentary behavior and promote physical activity and health of 8–9 year olds: the Transform-Us! Study. BMC Public Health. 2011;11:759.
Australian Bureau of Statistics. Socio-Economic Indexes for Areas (SEIFA). 2016(27/03/2018).
Ridley K, Ridgers ND, Salmon J. Criterion validity of the activPAL and ActiGraph for assessing children’s sitting and standing time in a school classroom setting. Int J Behav Nutr Phys Act. 2016;13(1):75.
Cain KL, Sallis JF, Conway TL, Van Dyck D, Calhoon L. Using accelerometers in youth physical activity studies: a review of methods. J Phys Act Health. 2013;10(3):437–50.
Janssen X, Basterfield L, Parkinson KN, Pearce MS, Reilly JK, Adamson AJ, et al. Objective measurement of sedentary behavior: impact of non-wear time rules on changes in sedentary time. BMC Public Health. 2015;15:504.
Gabel L, Ridgers ND, Della Gatta PA, Arundell L, Cerin E, Robinson S, et al. Associations of sedentary time patterns and TV viewing time with inflammatory and endothelial function biomarkers in children. Pediatr Obes. 2016;11(3):194–201.
Mattocks C, Ness A, Leary S, Tilling K, Blair SN, Shield J, et al. Use of accelerometers in a large field-based study of children: protocols, design issues, and effects on precision. J Phys Act Health. 2008;5(Suppl 1):S98–111.
Ridgers ND, Timperio A, Cerin E, Salmon J. Within- and between-day associations between children’s sitting and physical activity time. BMC Public Health. 2015;15(1):950.
Freedson P, Pober D, Janz KF. Calibration of accelerometer output for children. Med Sci Sports Exerc. 2005;37(11 Suppl):S523–30.
Carson V, Ridgers ND, Howard BJ, Winkler EA, Healy GN, Owen N, et al. Light-intensity physical activity and cardiometabolic biomarkers in US adolescents. PLoS ONE. 2013;8(8):e71417.
Cole TJ, Flegal KM, Nicholls D, Jackson AA. Body mass index cut offs to define thinness in children and adolescents: international survey. BMJ. 2007;335(7612):194.
World Health Organisation. Growth, reference, study, Group. WHO Child Growth standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva: World Health Organization; 2006.
Vidmar SI, Cole TJ, Pan H. Standardizing anthropometric measures in children and adolescents with functions for egen: update. Stata J. 2013;13(2):366–78.
Eisenmann JC. Waist circumference percentiles for 7- to 15-year-old Australian children. Acta Paediatr. 2005;94(9):1182–5.
National High Blood Pressure Education Program Working Group on High Blood Pressure in C, Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(2 Suppl 4th Report):555– 76.
Cooper AR, Goodman A, Page AS, Sherar LB, Esliger DW, van Sluijs EM, et al. Objectively measured physical activity and sedentary time in youth: the international children’s accelerometry database (ICAD). Int J Behav Nutr Phys Act. 2015;12(1):113.
van Dijk JW, Venema M, van Mechelen W, Stehouwer CD, Hartgens F, van Loon LJ. Effect of moderate-intensity exercise versus activities of daily living on 24-hour blood glucose homeostasis in male patients with type 2 diabetes. Diabetes Care. 2013;36(11):3448–53.
Garcia-Hermoso A, Saavedra JM, Ramirez-Velez R, Ekelund U, Del Pozo-Cruz B. Reallocating sedentary time to moderate-to-vigorous physical activity but not to light-intensity physical activity is effective to reduce adiposity among youths: a systematic review and meta-analysis. Obes Rev. 2017;18(9):1088–95.
Dempsey PC, Larsen RN, Dunstan DW, Owen N, Kingwell BA. Sitting less and moving more: implications for hypertension. Hypertension. 2018;72(5):1037–46.
Ekelund U, Anderssen SA, Froberg K, Sardinha LB, Andersen LB, Brage S. Independent associations of physical activity and cardiorespiratory fitness with metabolic risk factors in children: the European youth heart study. Diabetologia. 2007;50(9):1832–40.
Strizich G, Kaplan RC, Sotres-Alvarez D, Diaz KM, Daigre AL, Carnethon MR, et al. Objectively measured sedentary behavior, physical activity, and Cardiometabolic Risk in Hispanic Youth: Hispanic Community Health Study/Study of latino youth. J Clin Endocrinol Metabolism. 2018;103(9):3289–98.
Carson V, Janssen I. Volume, patterns, and types of sedentary behavior and cardio-metabolic health in children and adolescents: a cross-sectional study. BMC Public Health. 2011;11(1):274.
Bell JA, Hamer M, Richmond RC, Timpson NJ, Carslake D, Davey Smith G. Associations of device-measured physical activity across adolescence with metabolic traits: prospective cohort study. PLoS Med. 2018;15(9):e1002649.
Barone Gibbs B, Pettee Gabriel K, Reis JP, Jakicic JM, Carnethon MR, Sternfeld B. Cross-sectional and longitudinal associations between objectively measured sedentary time and metabolic disease: the coronary artery Risk Development in Young adults (CARDIA) study. Diabetes Care. 2015;38(10):1835–43.
Silva TO, Norde MM, Vasques AC, Zambom MP, Antonio MARGM, Rodrigues AMDB et al. Association of physical activity and sitting with metabolic syndrome and hyperglycemic clamp parameters in adolescents– BRAMS pediatric study. Front Endocrinol. 2023;14.
Lim J, Kim JS, Park S, Lee O, So WY. Relationship of physical activity and sedentary time with metabolic health in children and adolescents measured by accelerometer: a narrative review. Healthc (Basel). 2021;9(6).
Sherry AP, Pearson N, Ridgers ND, Barber SE, Bingham DD, Nagy LC, et al. activPAL-measured sitting levels and patterns in 9–10 years old children from a UK city. J Public Health (Oxf). 2019;41(4):757–64.
Hinckson EA, Hopkins WG, Aminian S, Ross K. Week-to-week differences of children’s habitual activity and postural allocation as measured by the ActivPAL monitor. Gait Posture. 2013;38(4):663–7.
Milagres LC, Rocha NP, Albuquerque FM, Castro APP, Filgueiras MS, Pessoa MC, et al. Sedentary behavior is associated with lower serum concentrations of vitamin D in Brazilian children. Public Health. 2017;152:75–8.
da Silva ACM, Cureau FV, de Oliveira CL, Giannini DT, Bloch KV, Kuschnir MCC, et al. Physical activity but not sedentary time is associated with vitamin D status in adolescents: study of cardiovascular risk in adolescents (ERICA). Eur J Clin Nutr. 2019;73(3):432–40.
Hoffmann B, Kobel S, Wartha O, Kettner S, Dreyhaupt J, Steinacker JM. High sedentary time in children is not only due to screen media use: a cross-sectional study. BMC Pediatr. 2019;19(1):154.
Acknowledgements
Not applicable.
Funding
TransformUs was supported by a National Health and Medical Research Council (NHMRC) Project Grant (2009–2013; ID533815) and a Diabetes Australia Research Trust (DART) grant. JS is supported by a Leadership Level 2 Fellowship, National Health and Medical Research Council (APP 1176885). NDR was supported by a National Heart Foundation of Australia Future Leader Fellowship (ID 101895). LA is supported by an Australian Research Council Discovery Early Career Researcher Award (DE220100847). DWD was supported Senior Research Fellowship (APP1078360) from the National Health and Medical Research Council and the Victorian Government’s Operational Infrastructure Support Program. KDH is supported by a Heart Foundation Future Leader Fellowship (105929). Aspects of this work were supported by a National Health and Medical Research Council, Centre of Research Excellence (APP1057608).
Author information
Authors and Affiliations
Contributions
AMCA, AT, LA, JS conceived the study. AMCA analysed and interpreted the data; and wrote the first manuscript. NDR, AT, LA, DWD, KDH, RMD and JS assisted with data analysis and interpretation of the data. All authors commented on the conception of this manuscript and the data analysis plan, critically reviewed and revised the manuscript and approved the final manuscript as submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
TransformUs obtained ethical approval from the Deakin University Human Research Ethics Committee (EC 141–2009), the Victorian Department of Education and Early Childhood Development (2009_000344) and the Catholic Education Office (Project Number 1545).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Contardo Ayala, A.M., Ridgers, N.D., Timperio, A. et al. The association between device-measured sitting time and cardiometabolic health risk factors in children. BMC Public Health 24, 1015 (2024). https://doi.org/10.1186/s12889-024-18495-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18495-w