
Abstract
Background
To evaluate the current prevalence of prediabetes in northeast China, and further determine the association between prediabetes alone or coexistent with hypertension and cardiovascular disease (CVD) mortality.
Methods
In the prospective study, 15,557 participants without diabetes among aged ≥40 years in northeast China, were followed for a median of 5.5 years. Following the American Diabetes Association, prediabetes was defined as fasting plasma glucose (FPG) range of 5.6-6.9 mmol/L or glycated hemoglobin (HbA1c) range of 5.7-6.4% in people without diabetes.
Results
The prevalence of prediabetes was 44.3% among population aged ≥40 years in northeast China. Prediabetes alone did not promote risk of CVD mortality. However, when the subgroups were stratified by hypertension, the CVD mortality risk in prediabetes plus hypertension subjects increased significantly compared with population without prediabetes and hypertension. Multivariate-adjusted hazard ratios for CVD mortality in prediabetes subgroups plus hypertension were 2.28 (95% CI: 1.50, 3.47) for those diagnosed by FPG < 5.6 mmol/L & HbA1c 5.7-6.4%, 2.18 (95% CI: 1.53, 3.10) for those diagnosed by FPG 5.6-6.0 mmol/L & HbA1c < 6.5% and 2.35 (95% CI: 1.65, 3.35) for those diagnosed by FPG 6.1-6.9 & HbA1c < 6.5% compared with the reference group. Moreover, the percentage of hypertension in prediabetes subjects was high (60.4%), but the awareness, treatment and control rates were far from satisfactory (45.3, 35.1 and 4.8%, respectively).
Conclusions
The prevalence of prediabetes remains high in northeast China, and the CVD mortality was elevated significantly in prediabetes coexistent with hypertension. Considering the high percentage and low control rate of hypertension in prediabetes, strategies focused on HbA1c screening, FPG lowering and blood pressure management should be emphasized in northeast China.
Similar content being viewed by others


Background
Prediabetes refers to blood glucose concentrations higher than normal but lower than diabetic thresholds, is a high-risk state for progressing to diabetes. The prevalence of prediabetes is rising globally, a previous study has projected that more than 470 million individuals will have prediabetes by 2030 [1]. In China, possibly due to rapid socio-demographic changes and health transitions, the prevalence of prediabetes has reached 35.7% in 2016, [2] which was relatively higher than that in many other countries, [3] despite the conversion rate differs with prediabetes criteria and population characteristics [4].
Approximately 5-10% of people with prediabetes develop diabetes each year, which is much higher than the 3.5% in the general population, [5] In addition, prediabetes itself is also a risk factor for cardiovascular and cerebrovascular disease (CVD). Previous studies have suggested that prediabetes alters vascular status, worsens the prognosis of stroke, [6, 7] significantly increases the morbidity and mortality [8].
Moreover, the Jackson Heart Study indicated the associations between prediabetes and risk of CVD and mortality may be explained by concomitant hypertension [9]. Participants with both prediabetes and hypertension experienced a higher risk than those with prediabetes or hypertension alone [9]. According to the World Health Organization (WHO), prediabetes is characterized by fasting plasma glucose (FPG) of 6.1-6.9 mmol/L [10]. However, the American Diabetes Association (ADA) uses a lower cutoff value (FPG, 5.6-6.9 mmol/L) and has additionally introduced hemoglobin A1c (HbA1c) levels of 5.7-6.4% to diagnose prediabetes [11]. Compared with normoglycemic populations, the risk of CVD and mortality was related to hemoglobin A1c (HbA1c) 5.7-6.4% defined prediabetes (relative risk, 1.17), but not FPG (5.6-6.0 mmol/L, 6.1-6.9 mmol/L or 5.6-6.9 mmol/L) according to the Whitehall II study [12].
However, previous epidemiological studies on prediabetes have been criticized because of single diagnostic index, [13, 14] or lack of adverse health outcomes [9]. Therefore, we conducted a prospective study to profile the characteristics of prediabetes according to ADA recommendations, and further analyze the CVD mortality in different phenotypes of prediabetes as well as coexistent with hypertension, aiming to provide population-based evidence for formulating strategies to alleviate CVD burden.
Methods
Subjects and study design
This prospective cohort study is based on a cross-sectional study which was conducted between September 2017 and March 2019 in northeast China. The design of the study has been described previously. In brief, a total of 18,796 participants aged 40 years and older were enrolled from four rural counties (Donggang, Lingyuan, Chaoyang and Liaoyang) and three urban districts (Zhennan, Liuerbao and Gongchangling) in Liaoning Province, using a multi-stage stratified cluster random sampling method. Detailed information was collected at baseline for each participant, the detailed information has been described previously [15].
Subsequently, individuals with diabetes or missing information on FPG or HbA1c were excluded, a total of 15,557 subjects were enrolled finally. The study was approved by the Ethics Commission of the CPC Central Committee of the China Cardiovascular Disease Center (Beijing). All participants provided written informed consent. Patients and public will not be involved in the development of the research question or in the design of the study. Patients will receive written information about this trial.
Data collection
Data is in a single clinic visit, through face-to-face interview using self-management questionnaire to collect. Take fasting blood samples in the morning after overnight fasting ≥8 hours. Samples were injected from the anterior elbow vein into BD Vacutainer tubes containing EDTA (Becton, Dickinson and Co, Franklin Lakes, New Jersey, USA). Serum samples from whole blood separation, at 20 °C-cryopreservation. FPG was measured by using oxidase enzymatic method on an Abbott Diagnostics C800i auto-analyzer (Abbott Laboratories, Abbott Park, IL, USA) with commercial kits. HbA1c was measured by using quantitative high-performance liquid chromatography from venous blood samples directly.
Blood pressure was measured by a standardized electronic sphygmomanometer (HEM-907; Omron, Kyoto, Japan) in a quiet and warm room. The participants were asked to avoid smoking, caffeine intake and exercise for at least 30 minutes before the measurement. For each participant, blood pressure was measured three times at 2-min intervals after at least 5 min of rest in a seat position. Information on demographic data, medication and lifestyle were obtained from questionnaire.
Definitions
According to the American Diabetes Association (ADA) guideline, [11] prediabetes was defined as fasting plasma glucose (FPG) range of 5.6-6.9 mmol/L, or HbA1c range of 5.7-6.4% in people without diabetes. Prediabetes was divided into 3 subgroups according to FPG and HbA1c levels: FPG < 5.6 mmol/L & HbA1c 5.7-6.4%, FPG 5.6-6.0 mmol/L & HbA1c < 6.5%, and FPG 6.1-6.9 mmol/L & HbA1c < 6.5%.
Diabetes was identified if the participant met either of the following criteria: (1) self-reported diagnosis that was made by a certified physician previously, (2) an FBG ≥ 7.0 mmol/L or HbA1c ≥ 6.5% according to the ADA guideline. Hypertension was diagnosed if the individual met either of the following criteria: (1) mean systolic blood pressure (SBP) ≥ 140 mmHg and/or mean diastolic blood pressure (DBP) ≥ 90 mmHg, (2) use of antihypertensive medication in the past 2 weeks. Atrial fibrillation (AF) was determined based on electrocardiogram (ECG) findings and/or previous diagnosis by a physician. Current smoking was considered as the consumption of ≥1 cigarette per day and lasted for ≥1 year, while current drinking was defined as any alcohol consumption ≥1 time per week. Regular exercise was defined as moderate-intensity exercise or equivalent to walking for at least 30 minutes and 3 times per week; participants with moderate and heavy manual work were considered to fulfill the criteria. Lack of exercise was identified when participants failed to meet the criteria for regular exercise.
Each participant had a medical history of hypertension. We divided hypertension into 4 subgroups according to severity of hypertension defined by the European Society of Hypertension (ESH) guideline: HBP (normal), HBP(1+), HBP(2+), HBP(3+) [16]. Awareness of hypertension was defined as having an answer of “Yes” to the question “Have you been diagnosed with hypertension by a certified doctor?” Treatment of hypertension was defined as use of anti-hypertensive medication in the past 2 weeks. Hypertension control was defined as an average SBP < 140 mmHg and an average DBP < 90 mmHg, while uncontrolled hypertension was considered as not meeting these criteria.
Outcomes
Our study endpoint was CVD death. Mortality data was obtained from the National Population Registry of the China National Statistical Office. We accessed the database containing death certificates for CVD deaths that occurred between the cross-sectional study conducted date and September 30, 2023. The cause of death was determined by reviewing the death certificates and classified according to the International Classification of Diseases (10th Revision) codes I00 to I99.
Statistical analysis
Descriptive statistics were calculated for all variables. Continuous variables with normal distribution were described as means and standard deviations, categorical variables were reported as medians and inter-quartile ranges. Differences between groups were compared with t-test or chi-square test. The direct age- and sex- standardization method was used to evaluate the standardized prevalence according to the 2010 Chinese census, and corresponding 95% confidence intervals (CIs) were estimated.
Cox proportional hazards models were used to estimate associations between subgroups of prediabetes or coexistent with hypertension and the risk of CVD death, hazard ratios (HRs) and 95% CIs were calculated. Model 1 was unadjusted. Model 2 was adjusted for age and sex. Model 3 was further adjusted for body mass index (BMI), history of atrial fibrillation, stroke and heart disease, level of triglyceride (TG), low-density lipoprotein-cholesterol (LDL-C), high-density lipoprotein-cholesterol (HDL-C) and total cholesterol (TC), treatment for hypertension, current smoking, current drinking, education, income, physical activity. All statistical analyses were performed using SPSS 22.0 (SPSS, Chicago, Illinois, USA). P value < 0.05 was considered statistically significant.
Results
Characteristics of the study population without diabetes
The study included 15,557 subjects without diabetes, with an average age of 59.9 ± 10.1 years, 6115 (39.3%) were males, 72.2% came from rural areas and 32.9% lower income families (< 5000 yuan), half of whom (48.9%) had received education to primary school or below (Table 1).
At baseline, 8308 (53.4%) participants were identified to have prediabetes according to ADA definition. Among those subjects, 25.4% were current smokers, 28.5% were current drinkers, 12.9% lacked exercise and 60.4% had hypertension (Table 1) (Fig. 1).

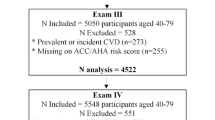
Flow chart of the population selection process
Prevalence of prediabetes and subgroups
Based on the 2010 ADA criteria, the prevalence of prediabetes was 44.3%, with a higher prevalence in the rural population than in the urban population (49.3% vs 31.8%, P < 0.001). We also found that the prevalence in the male group and female group was 46.4 and 42.9%, respectively (P < 0.001). The prevalence of prediabetes increased from 39.1% among those 40-49 years to 47.6% among those 70-79 years, however, the prediabetes prevalence decreased slightly among those ≥80 years (45.4%). The age-standardized prevalence was 42.8% (rural 47.4% and urban 30.2%; males 46.0% and females 40.8%) (Table 2) (Fig. 2).

Age-standardized prevalence of prediabetes and subgroups. A. Region B. Sex
In the subgroup analysis, the prevalence of FPG < 5.6 mmol/L & HbA1c 5.7-6.4%, FPG 5.6-6.0 mmol/L & HbA1c < 6.5% and FPG 6.1-6.9 mmol/L & HbA1c < 6.5% was 7.8, 20.8 and 15.7% respectively. Young men and residents living in rural areas were tended to had higher FPG, in contrast, older women and residents living in urban areas were tended to have raised HbA1c (Table 2) (Fig. 2).
CVD mortality in individuals with prediabetes
There were 548 CVD death among 15,557 participants over a median follow-up of 5.5 years, the mortality rate of CVD was 6.6/1000 person-years. The corresponding mortality rates of CVD events in FPG < 5.6 mmol/L & HbA1c 5.7-6.4%, FPG 5.6-6.0 mmol/L & HbA1c < 6.5% and FPG 6.1-6.9 mmol/L & HbA1c < 6.5% groups were 7.20, 6.53 and 7.51 per 1000 person-years respectively. However, all subgroups of prediabetes were not associated with risk of CVD mortality (Table 3).
CVD mortality in prediabetes stratified by hypertension
Given the high prevalence of hypertension (60.4%) in prediabetes individuals, we stratified the 8 subgroups according to with or without hypertension: [preDM(−)/HBP(−) as reference, preDM(−)/HBP(+), FPG < 5.6 mmol/L & HbA1c 5.7-6.4%/HBP(−), FPG 5.6-6.0 mmol/L & HbA1c < 6.5%/HBP(−), FPG 6.1-6.9 mmol/L & HbA1c < 6.5%/HBP(−), FPG < 5.6 mmol/L & HbA1c 5.7-6.4%/HBP(+), FPG 5.6-6.0 mmol/L & HbA1c < 6.5%/HBP(+), and FPG 6.1-6.9 mmol/L & HbA1c < 6.5%/HBP(+)](Table 4).
Hypertension alone group [preDM (−)/HBP (+)] increased the risk of CVD mortality, with adjusted HR of 2.19 (95% CI: 1.59, 3.02) for CVD death compared with the reference group. In contrast, isolated prediabetes groups [FPG (+) /HBP (−), HbA1c (+) /HBP (−)] were not associated with an elevated risk of CVD mortality in the fully adjusted models (all P > 0.05). When prediabetes is combined with hypertension, the risk of CVD death increases significantly. Multivariate-adjusted hazard ratios for CVD mortality in prediabetes subgroups combined with hypertension were as follows: 2.28 (95% CI: 1.50, 3.47) for individuals diagnosed with FPG<5.6 mmol/L & HbA1c 5.7-6.4%, 2.18 (95% CI: 1.53, 3.10) for those diagnosed with FPG 5.6-6.0 mmol/L & HbA1c<6.5%, and 2.35 (95% CI: 1.65, 3.35) for those diagnosed with FPG 6.1-6.9 & HbA1c<6.5%, compared to the reference group (Table 4). Kaplan-Meier curves also revealed that the cumulative risk of CVD mortality in the preDM(+)/HBP(+) group was substantially higher than the preDM(+)/HBP(−) group in the fully adjusted model (Fig. 3).

Cumulative rate of CVD mortality according to the blood glucose and hypertension at baseline
Moreover, when hypertension was stratified into subgroups, the CVD mortality risk increased significantly with increasing severity of hypertension (Additional Table 1). However, the rates of awareness, treatment and control of hypertension in prediabetes were frustratingly low (45.3, 35.1 and 4.8%, respectively) (Table 5).
Discussion
The major findings of the present study are as follows: (1) The prevalence of prediabetes was 44.3% according to the ADA criteria among participants aged ≥40 years in northeastern China. (2) Prediabetes alone did not promote risk of CVD mortality. However, when prediabetes subgroups coexist with hypertension, the CVD mortality risk increased significantly. (3) Hypertension was a frequent comorbidity in prediabetes, however, the control rate of hypertension in prediabetes was dramatically low, indicating the substantial CVD risk burden in those areas.
Our results showed that the age-standardized prevalence of prediabetes was 42.8%, the prevalence was higher than the national survey (35.8%) undertaken in 2013 in the same age group and diagnostic criteria [2]. When compared to previous study reported 25.65% among adults aged ≥45 years in northwestern China [14] and other countries, such as the United States (32.74%), the prevalence of prediabetes was high in northeast China according to ADA criteria [17].
When compared to WHO criteria (FPG 6.1-6.9 mmol/L), ADA applies a lower cutoff value (FPG 5.7-6.9 mmol/L) for prediabetes. The prevalence of prediabetes increased by 20.8% using ADA fasting glucose criteria in this study, and most of population were young men living in rural areas. In 2010, ADA introduced HbA1c as a new category to diagnose prediabetes [11]. In the present study, 6.9% prediabetes were newly diagnosed after introducing HbA1c, and those subjects tended to be older women living in urban areas. Although the WHO criteria have incorporated HbA1c in the diagnosis of diabetes in 2019, the definition of prediabetes did not change, and China still adopted the WHO criteria [18]. Thus, our study suggested that HbA1c screening should be enhanced in Chinese population.
Prediabetes is a high-stake condition for diabetes, and the prevalence of diabetes in urban areas is consistently higher than in rural areas among middle-aged and elderly adults in China [19]. In contrast, our study showed that the prevalence of prediabetes was significantly higher in rural areas than in urban areas, consistent with previous studies [20]. The reason for this discrepancy is possibly due to the rapid economic progress in rural areas in recent years [21]. Coinciding with previous studies, [2, 22] we also found that men were more likely to develop prediabetes than women, and lifestyles may be responsible for these differences.
Similar to Whitehall II study, all prediabetes subgroups were not associated with an increased risk of CVD mortality in our study [12]. After stratification by hypertension, all normotensive prediabetes subgroups did not promote risk of CVD mortality compared with normotensive non-prediabetic participants. However, when prediabetes coexists with hypertension, the risk for CVD mortality increased significantly, especially when combined with grade III hypertension. Hypertension increased risk of death significantly either alone or concurrent with prediabetes, indicating hypertension plays a more significant role than prediabetes in the development of CVD mortality. The relationship between blood pressure and blood glucose remains unclear [23]. According to our study, hypertension was a frequent comorbidity in prediabetes, but the awareness, treatment and control rates among the prediabetes population were remarkably low. Thus, the lagging blood pressure management in northeast China indicated the increased cardiovascular risk in the next few decades.
Previous large-sample meta-analyses had shown that prediabetes was associated with the risk of CVD in people with or without baseline CVD, [24] and associated with increased risk and poor prognosis of heart failure, [25, 26], which further validated our findings. Compared to those studies, an advantage of our prospective study was the large-sized representative sample in northeast China, a region with a high burden of prediabetes and cardiovascular disease. Thus, our findings might provide an important guideline for the management of prediabetes patients, and might provide a reasonably reliable and relatively stable estimation of prediabetes epidemiology and CVD mortality in northeast China.
However, the present study still has several limitations. Firstly, oral glucose tolerance test (OGTT) recommended by ADA was not performed in this study, and thus impaired glucose tolerance (IGT) was not introduced to evaluate prediabetes due to lack of OGTT. The prevalence of prediabetes might be underestimated. The major reason is the difficulty of the performance of OGTT in a large sample population. Additionally, a previous study suggested that the combined application of FPG and HbA1c was associated with higher levels of detection of prediabetes compared to the joint application of FPG and 2 h PG [27]. Therefore, the combination of HbA1c and FPG was recommended in epidemiologic screening for prediabetes. Secondly, bias in the relationship between prediabetes and CVD events was inevitable due to subject loss of contact during follow-up. Thirdly, the population was recruited from one province of northeast China, the findings cannot be generalized to all participants across China.
Conclusions
In summary, the estimated prevalence of prediabetes diagnosed by the ADA criteria was 44.3% among the participants aged ≥40 years in northeastern China. All prediabetes subgroups were not associated with an increased risk of CVD mortality, however, when hypertension was incorporated as a stratifying factor, the risk of CVD mortality elevated significantly in subjects with prediabetes and hypertension. Moreover, the CVD mortality risk was significantly increased in different FPG levels groups in prediabetes plus hypertension group. Therefore, additional HbA1c screening and lower FPG levels as well as blood pressure management strategies for prediabetes are needed in northeast China.
Availability of data and materials
The data analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CVD:
-
Cerebrovascular disease
- FPG:
-
Fasting plasma glucose
- HbA1c:
-
Hemoglobin A1c
- WHO:
-
World Health Organization
- ADA:
-
the American Diabetes Association
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- AF:
-
Atrial fibrillation
- ECG:
-
Electrocardiogram
- ESH:
-
European Society of Hypertension
- CIs:
-
Confidence intervals
- HRs:
-
hazard ratios
- BMI:
-
Body mass index
- TG:
-
Triglyceride
- LDL-C:
-
Low-density lipoprotein-cholesterol
- HDL-C:
-
High-density lipoprotein-cholesterol
- TC:
-
Total cholesterol
- OGTT:
-
Oral glucose tolerance test
- IGT:
-
Impaired glucose tolerance
References
Aramo C, Oyom AP, Okello E, Acam V, Okiria JC, Mwambi B, et al. Assessing the prevalence and risk factors of pre-diabetes among the community of Iganga municipality, Uganda: a cross sectional study. BMC Res Notes. 2019;12(1):553.
Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. Jama. 2017;317(24):2515–23.
Shen J, Kondal D, Rubinstein A, Irazola V, Gutierrez L, Miranda JJ, et al. A multiethnic study of pre-diabetes and diabetes in LMIC. Glob Heart. 2016;11(1):61–70.
Tabak AG, Herder C, Rathmann W, Brunner EJ, Kivimaki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279–90.
Adler AI, Shine BS, Chamnan P, Haworth CS, Bilton D. Genetic determinants and epidemiology of cystic fibrosis-related diabetes: results from a British cohort of children and adults. Diabetes Care. 2008;31(9):1789–94.
Tanaka R, Ueno Y, Miyamoto N, Yamashiro K, Tanaka Y, Shimura H, et al. Impact of diabetes and prediabetes on the short-term prognosis in patients with acute ischemic stroke. J Neurol Sci. 2013;332(1-2):45–50.
Liu J, Grundy SM, Wang W, Smith SC Jr, Vega GL, Wu Z, et al. Ten-year risk of cardiovascular incidence related to diabetes, prediabetes, and the metabolic syndrome. Am Heart J. 2007;153(4):552–8.
Huang Y, Cai X, Mai W, Li M, Hu Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. BMJ. 2016;355:i5953.
Hubbard D, Colantonio LD, Tanner RM, Carson AP, Sakhuja S, Jaeger BC, et al. Prediabetes and risk for cardiovascular disease by hypertension status in black adults: the Jackson heart study. Diabetes Care. 2019;42(12):2322–9.
Organization WH: CLASSIFICATION OF DIABETES MELLITUS 2019.
American Diabetes A. Standards of medical care in diabetes--2013. Diabetes Care. 2013;36(Suppl 1):S11–66.
Vistisen D, Witte DR, Brunner EJ, Kivimaki M, Tabak A, Jorgensen ME, et al. Risk of cardiovascular disease and death in individuals with prediabetes defined by different criteria: the Whitehall II study. Diabetes Care. 2018;41(4):899–906.
Liu HH, Cao YX, Li S, Guo YL, Zhu CG, Wu NQ, et al. Impacts of prediabetes Mellitus alone or plus hypertension on the coronary severity and cardiovascular outcomes. Hypertension. 2018;71(6):1039–46.
Wang R, Zhang P, Li Z, Lv X, Cai H, Gao C, et al. The prevalence of pre-diabetes and diabetes and their associated factors in Northeast China: a cross-sectional study. Sci Rep. 2019;9(1):2513.
Xing L, Lin M, Du Z, Jing L, Tian Y, Yan H, et al. Epidemiology of atrial fibrillation in Northeast China: a cross-sectional study, 2017-2019. Heart. 2020;106(8):590–5.
Mancia G, Kreutz R, Brunstrom M, Burnier M, Grassi G, Januszewicz A, et al. 2023 ESH guidelines for the management of arterial hypertension the task force for the management of arterial hypertension of the European Society of Hypertension: endorsed by the International Society of Hypertension (ISH) and the European renal association (ERA). J Hypertens. 2023;41(12):1874–2071.
Vatcheva KP, Fisher-Hoch SP, Reininger BM, McCormick JB. Sex and age differences in prevalence and risk factors for prediabetes in Mexican-Americans. Diabetes Res Clin Pract. 2020;159:107950.
Liu M, Yang SS, Wang SS, Li J, Kou FY, Tai PG, et al. Prevalence of diabetes and associated factors in Hainan centenarians. Zhonghua liu xing bing xue za zhi = Zhonghua liuxingbingxue zazhi. 2021;42(1):68–72.
Wang Z, Li X, Chen M. Socioeconomic factors and inequality in the prevalence and treatment of diabetes among middle-aged and elderly adults in China. J Diabetes Res. 2018;2018:1471808.
Basit A, Fawwad A, Qureshi H, Shera AS. Members N: prevalence of diabetes, pre-diabetes and associated risk factors: second National Diabetes Survey of Pakistan (NDSP), 2016-2017. #N/A. 2018;8(8):e020961.
Hamoudi R, Saheb Sharif-Askari N, Saheb Sharif-Askari F, Abusnana S, Aljaibeji H, Taneera J, et al. Prediabetes and diabetes prevalence and risk factors comparison between ethnic groups in the United Arab Emirates. Sci Rep. 2019;9(1):17437.
Nguyen QM, Srinivasan SR, Xu JH, Chen W, Berenson GS. Changes in risk variables of metabolic syndrome since childhood in pre-diabetic and type 2 diabetic subjects: the Bogalusa heart study. Diabetes Care. 2008;31(10):2044–9.
Mancia G, Facchetti R, Bombelli M, Polo Friz H, Grassi G, Giannattasio C, et al. Relationship of office, home, and ambulatory blood pressure to blood glucose and lipid variables in the PAMELA population. Hypertension. 2005;45(6):1072–7.
Cai X, Zhang Y, Li M, Wu JH, Mai L, Li J, et al. Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis. BMJ. 2020;370:m2297.
Cai X, Liu X, Sun L, He Y, Zheng S, Zhang Y, et al. Prediabetes and the risk of heart failure: a meta-analysis. Diabetes Obes Metab. 2021;23(8):1746–53.
Mai L, Wen W, Qiu M, Liu X, Sun L, Zheng H, et al. Association between prediabetes and adverse outcomes in heart failure. Diabetes Obes Metab. 2021;23(11):2476–83.
Okosun IS, Davis-Smith M, Paul Seale J, Ngulefac J. Applicability of a combination of hemoglobin a(1c) and fasting plasma glucose in population-based prediabetes screening. J Diabetes. 2012;4(4):407–16.
Acknowledgements
We would like to thank the CDC of Chaoyang, Liaoyang, Dandong, and Donggang city in Liaoning province, who worked hard to ensure the reliability and accuracy of data.
Funding
This study was supported by the Department of Science and Technology of Liaoning Province (2018225065, 2019JH2/10300001), the National Natural Science Foundation of China (62171472), LiaoNing Revitalization Talents Program (XLYC2007058) and Natural Science Foundation of LiaoNing (2021- MS-171).
Author information
Authors and Affiliations
Contributions
LX and SL were responsible for the concept and design of the study. LY and MM contributed to the drafting of the manuscript. LJ, YT, and SL collected and analyzed the data. LX, SL, QS, LS, GL, LY and MM interpreted the data. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Commission of the CPC Central Committee of the China Cardiovascular Disease Center (Beijing). All participants provided written informed consent. Patients and public will not be involved in the development of the research question or in the design of the study. Patients will receive written information about this trial. The data were used only for research purposes. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Rates and hazard ratios of CVD mortality according to the blood glucose and severity of hypertension.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yue, L., Tian, Y., Ma, M. et al. Prevalence of prediabetes and risk of CVD mortality in individuals with prediabetes alone or plus hypertension in Northeast China: insight from a population based cohort study. BMC Public Health 24, 475 (2024). https://doi.org/10.1186/s12889-024-17996-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17996-y