
Abstract
Introduction
The estimated dose of radiation to immune cells (EDRIC) has been shown to correlate with the overall survival (OS) of patients who receive definitive thoracic radiotherapy. However, the planning target volume (PTV) may be a confounding factor. We assessed the prognostic value of EDRIC for non-small cell lung cancer (NSCLC) in patients who underwent postoperative radiotherapy (PORT) with homogeneous PTV.
Methods
Patients with NSCLC who underwent PORT between 2004 and 2019 were included. EDRIC was computed as a function of the number of radiation fractions and mean doses to the lungs, heart, and remaining body. The correlations between EDRIC and OS, disease-free survival (DFS), locoregional-free survival (LRFS), and distant metastasis-free survival (DMFS) were analyzed using univariate and multivariate Cox models. Kaplan–Meier analysis was performed to assess the survival difference between low- and high-EDRIC groups.
Results
In total, 345 patients were analyzed. The mean EDRIC was 6.26 Gy. Multivariate analysis showed that higher EDRIC was associated with worse outcomes in terms of OS (hazard ratio [HR] 1.207, P = .007), DFS (HR 1.129, P = .015), LRFS (HR 1.211, P = .002), and DMFS (HR 1.131, P = .057). In the low- and high-EDRIC groups, the 3-year OS was 81.2% and 74.0%, DFS 39.8% and 35.0%, LRFS 70.4% and 60.5%, and DMFS 73.9% and 63.1%, respectively.
Conclusions
EDRIC is an independent prognostic factor for survival in patients with NSCLC undergoing PORT. Higher doses of radiation to the immune system are associated with tumor progression and poor survival. Organs at risk for the immune system should be considered during radiotherapy planning.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The use of postoperative radiotherapy (PORT) for non-small cell lung cancer (NSCLC) remains a topic of debate. Although some retrospective studies and large database analyses suggested that PORT provides survival benefits for patients with pathologic N2 (pN2) NSCLC [1, 2], two recent randomized controlled trials (RCTs) have shown no improvement in disease-free survival (DFS) or overall survival (OS) with the use of PORT in these patients [3, 4]. Furthermore, the side effects of PORT [5], especially cardiopulmonary toxicity [6,7,8,9], raise many concerns. Radiation to the immune system might diminish the benefits of PORT [10].
Radiation-induced lymphopenia is a common occurrence in lung cancer therapy [11,12,13]. To quantify the impact of radiation on immune cells, a model [14] was developed to estimate the effective dose of radiation to immune cells (EDRIC) based on the mean lung dose (MLD), mean heart dose (MHD), mean body dose (MBD), while considering the fraction number. EDRIC has been found as significant factor for OS in patients with NSCLC [15,16,17], small cell lung cancer (SCLC) [18], and esophageal cancer [19] undergoing definitive radiotherapy. However, none of these studies considered the planned target volume (PTV) in multivariate analysis. Tumor burden, such as tumor size and lymph node ratio, could confound the effect of EDRIC on OS.
There is no gross tumor volume (GTV) in patients with NSCLC receiving PORT, and the PTV is homogeneous in these patients; hence, we aimed to examine the influence of EDRIC on survival in this group of patients.
Methods
Patients
This was a post hoc analysis of our recently published phase III PORT-C RCT [3] and a retrospective review of the PORT database at China’s National Cancer Center. Patients with pN2 NSCLC between January 2004 and June 2019 were analyzed. The eligibility criteria were 18–70 years of age, complete resection (R0), systemic lymph node dissection, and adjuvant chemotherapy followed by PORT. The exclusion criteria were a history of other cancers and receipt of neoadjuvant chemotherapy. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of China’s National Cancer Center. The requirement for informed consent was waived by the Institutional Review Board of China’s National Cancer Center because of the retrospective nature of the study.
Treatments
The surgical procedures included lobectomy, bilobectomy, pneumonectomy, and meticulous dissection of the mediastinal lymph nodes. PORT was administered to all patients. Experienced radiotherapists outlined the target volumes and organs at risk. The clinical target volume comprised the ipsilateral hilum, subcarinal area, ipsilateral mediastinum, and stump of central lesions. Automatic thresholding was used to outline the lungs excluding gross malignancies. The heart was outlined, as previously described [20]. The range of MBD calculation was determined from the skull base to the lower margin of the first lumbar spine.
A dose of 50 Gy was administered in 25 fractions of 2 Gy each and five times weekly. All patients underwent intensity-modulated or three-dimensional conformal radiation therapy using linear accelerators with a 6-MV beam. Simulation computed tomography (CT) images with a 5-mm slice thickness were acquired using a Brilliance Big Bore scanner (Philips Healthcare, Andover, MA, USA) with iodine-based intravenous contrast while the patient was in the supine position. Treatment plans were developed using the Pinnacle treatment planning system (v9.0; Philips, Fitchburg, WI, USA).
Follow-up
Patients were followed up every three months for the first two years, every six months for the subsequent three to five years, and yearly thereafter. All patients were assessed based on their symptoms using blood and imaging examinations (chest CT, abdominal CT, or B-ultrasonography) and other relevant procedures. Disease progression was established based on clinical evaluation, radiographic inspection, and pathology reports when necessary.
Calculation of EDRIC
The radiation dose information was retrieved from the treatment planning systems. The EDRIC was estimated using the mean dose to the lung, heart, and remaining body, as well as the number of radiation fractions, using the model developed by Jin et al. [14]. and modified by Ladbury et al. [16]. , who substituted the dosage to the circulating immune pool for the dose to the immune system. The exact formula is as follows:
Statistics
Continuous variables are shown as the mean and standard deviation for normally distributed data and the median and interquartile range (IQR) for non-normally distributed data. Variables representing categories are expressed as counts and percentages. Continuous variables were compared using t-tests or Wilcoxon rank-sum tests, and categorical variables were compared using χ2 tests or Fisher’s exact tests, as appropriate. Endpoints included OS (time from the date of surgery to the date of death from any cause), DFS (time from the date of surgery to the date of any disease recurrence or death from any cause, whichever occurred first), locoregional recurrence-free survival (LRFS; time from the date of surgery to the date of locoregional recurrence or death, whichever occurred first), and distant metastasis-free survival (DMFS; time from the date of randomization to the date of DM or death, whichever occurred first). Endpoints were calculated using the Kaplan–Meier technique with right censoring at the time of the most recent follow-up if no event had occurred. The median follow-up duration was determined using the Kaplan–Meier technique. The endpoints were computed using the Kaplan–Meier curve and compared using the log-rank test. The unadjusted and adjusted effects of EDRIC on OS were evaluated using univariate and multivariate Cox proportional hazard models. The multivariate analysis included prognostic variables with a P-value less than 0.1 in the univariate analysis or were of clinical significance. We classified the patients into low- and high-EDRIC groups by maximizing the log-rank statistic between the two groups to determine the appropriate cut-off value. The median EDRIC value was also used as the threshold to confirm the findings. Statistical significance was set at P < .05. All analyses were performed using R (version 4.2.1; R Foundation, Vienna, Austria).
Results
Patient characteristics and EDRIC distribution
A total of 345 patients were eligible: 127 from the prospective database and 218 from the retrospective database. The patients were followed up for a median of 59.40 months (IQR: 34.79–80.16 months). The median age was 56 years (IQR: 49–62); 41.2% of the patients were women, and 51.6% had a smoking history. The median MLD, MHD, and MBD were 9.80 Gy, 8.95 Gy, and 6.39 Gy, respectively (Table 1). The median EDRIC was 6.26 Gy (IQR: 5.51–7.51).
Overall survival
Univariate analysis showed that higher EDRIC, larger PTV and male sex were related to shorter OS, while poorer Eastern Cooperative Oncology Group performance status (ECOG PS) and tumor stage were marginally related to shorter OS (Table 2). Multivariate analysis revealed that EDRIC (hazard ratio [HR]: 1.21, P = .007) and sex (HR: 0.39, P = .003) were significantly associated with shorter OS, while PTV was no longer related to OS.
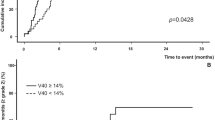
In the entire population, the 3-year OS rate was 77.5%, and the median survival time was not reached. According to the optimal cut-off values of EDRIC, patients with high EDRIC had a significantly shorter OS than those with low EDRIC (median OS of 43.53 months vs. not reached, P < .01; Fig. 1A). According to the median EDRIC, the 3-year OS rates were 81.2% and 74.0% in low and high-EDRIC groups.

Kaplan–Meier curves for (A) overall survival, (B) locoregional-free survival, (C) distant metastasis-free survival, and (D) disease-free survival. Patients are stratified by optimal cutoff of the estimated dose of radiation to immune cells
Disease-free survival
The 3-year DFS rate for the total population was 37.4%, with a median PFS of 21.6 months. EDRIC (HR: 1.13, P = .015), tumor stage (HR: 1.43, P = .048), and positive lymph node ratio (HR: 1.04, P = .003) were significantly associated with DFS in multivariate analysis (Table 3). According to the optimal cut-off values of EDRIC, patients with high EDRIC had a significantly shorter DFS than those with low EDRIC (median DFS: 39.23 months vs. not reached, P < .01; Fig. 1B). According to the median EDRIC, the 3-year DFS rates were 39.8% and 35.0% in low and high-EDRIC groups.
Locoregional-free survival
The 3-year LRFS rate for the entire population was 65.4%, with a median LRFS of 102 months. The univariate analysis revealed that greater EDRIC, male sex, and poorer ECOG PS were related to a lower LRFS, but histology was marginally insignificantly associated with LRFS (Table 4). The multivariate analysis revealed that a greater EDRIC (HR: 1.21, P = .002) and male sex were significantly related to a lower LRFS. According to the optimal cut-off values of EDRIC, patients with a high EDRIC had a significantly shorter LRFS than those with a low EDRIC (median LRFS: 12.65 vs. 25.43 months, P < .01; Fig. 1C). According to the median EDRIC, the 3-year LRFS rates were 70.4% and 60.5% in low and high-EDRIC groups.
Distant metastasis-free survival
The 3-year DMFS rate in the total study population was 42.0%. The median DMFS was 25.76 (12.65-140.22) months. EDRIC (HR = 1.113, P = .038), histology (HR = 1.717, [1.112, 2.651]), pT stage (HR = 1.455, [1.003, 2.110]) and PLN (HR = 1.040, [1.015, 1.066]) were significantly associated with DMFS in the multivariate analysis (Table 5). According to the optimal cut-off values of EDRIC, patients with high EDRIC had a significantly shorter DMFS than those with low EDRIC (median DMFS: 24.5 vs. 28.4 months, P < .01; Fig. 1D). According to the median EDRIC, the 3-year DMFS rates were 45.76% and 38.46% in low- and high- EDRIC groups.
Discussion
We found a correlation between higher EDRIC and worse OS, DFS, LRFS, and DMFS in patients with NSCLC undergoing PORT, which may explain why these patients did not benefit from PORT in two recent RCTs [3, 4]. EDRIC is a quantifiable risk factor that may be controllable, particularly with the most recent radiation treatment approaches such as proton therapy. The prospect of attaining lower EDRIC levels while retaining acceptable tumor coverage requires further investigation.
In our study, multivariate analysis showed that EDRIC was one of the most critical variables associated with OS, DFS, LRFS, and DMFS in patients with NSCLC undergoing PORT, even when considering the PTV, tumor stage, and positive lymph node ratio. In multivariate analyses, neither PTV nor tumor stage was associated with OS, LRFS, or DMFS. Previous studies have identified EDRIC as a significant factor for OS in patients with NSCLC [15,16,17], SCLC [18], and esophageal cancer [19] who received definitive radiotherapy. However, none of these studies considered PTV in the multivariate analysis. One study incorporated the GTV in the multivariate analysis; however, EDRIC was no longer associated with OS [15]. Tumor burden, such as tumor size and number of positive lymph node [21], may confound the effect of EDRIC on the OS. In our cohort, there was no GTV for PORT, and our institution’s delineation of PTV was uniform. We considered PTV in multivariate analysis and verified that EDRIC was an independent predictor of survival.
Multivariate analysis showed that EDRIC was the only variable associated with OS, except for sex, whereas EDRIC, pathologic tumor stage, and positive lymph nodes were associated with DFS. DFS is mainly affected by tumor burden, including primary tumors and lymph nodes, whereas OS is affected by both tumor and patient-related factors. EDRIC was the only factor related to both DFS and OS, implying that the effect of EDRIC is independent of tumor burden, such as tumor stage and positive lymph nodes. The main effect of EDRIC is the irritation of immune cells; thus, it is important to protect the immune system.
The impact of radiation on the immune system is bilateral, involving stimulation and suppression [10]. Immune suppression may diminish the efficacy of cancer treatment. This immunosuppression might be caused by the irradiation of the bone marrow, activation of inhibitory cytokines or regulatory cells, or direct death of mature circulating lymphocytes in the blood or lymphoid spaces, which are vulnerable to very low radiation doses [22]. There may be an inherent trade-off between radiation to promote tumor cell killing and immunosuppression, which counteracts the advantages of radiation. Advanced radiation technologies, such as proton beam therapy, allow for a more significant dose fall-off and may provide considerable dosimetric advantages over intensity-modulated radiation therapy in some patients [23, 24]. Our study suggests that radiation-induced immunosuppression may account for the poor benefit of PORT, which explains the lack of DFS benefit of PORT in the PORT-C [3] and LUNG ART [4] trials.
The results of our study have implications for integrating radiotherapy and immunotherapy. The detrimental effects of higher EDRIC on survival outcomes highlight the importance of preserving immune system function during radiotherapy. This is particularly relevant for patients receiving immunotherapy, where a robust immune response is crucial for treatment efficacy [25, 26]. Minimizing radiation exposure to immune cells could enhance the therapeutic synergy between radiotherapy and immunotherapy. In the neoadjuvant setting, the combination of radiotherapy and immunotherapy holds promise [27]. However, our results indicate that careful planning is required to avoid excessive radiation to immune cells, which could compromise the immune-mediated anti-tumor effects of neoadjuvant immunotherapy.
The EDRIC model has two limitations. EDRIC is a simplistic model that may not accurately depict how radiation affects the immune system. The essential assumption is that EDRIC measures the radiation dose to circulating immune cells; however, this association may be obscured by other risk factors, such as the use of granulocyte colony-stimulating factor. Second, only organs included in the model were considered. Therefore, the contributions of the lymphatics, nodes, thoracic duct, thymus, and bone marrow were not considered. The EDRIC model only expressly included the dosage to the lungs and heart, while the remaining dose was obtained from the whole body and with inherent imprecisions from a generalizing dose across a vast volume. A method that involves more detailed segmentation per organ would provide a better model with a procedure that might be automated with forthcoming artificial intelligence technologies [28]. Nonetheless, the current EDRIC model produced a repeatable immune cell dosage estimate that could be efficiently compared among individuals.
Our study had several limitations. First, as this was a single-institution retrospective study, biases such as selection bias could not be avoided, and all relevant variables could not be evaluated. Second, our cohort included only patients with pN2 NSCLC who underwent PORT. Thus, caution should be exercised when extrapolating these results to patients with NSCLC who underwent definitive radiotherapy or patients with other cancers. Finally, we did not analyze the association between EDRIC and the decrease in lymph node count because a large subset of patients did not undergo blood tests before radiotherapy.
Conclusion
EDRIC efficiently predicts OS, DFS, LRFS, and DMFS in patients with NSCLC undergoing PORT. Future treatment benefits may be improved by customizing radiation therapy to minimize damage to the immune system.
Data availability
The datasets and codes are available from the corresponding author on reasonable request and only for academic use.
References
Lally BE, Zelterman D, Colasanto JM, Haffty BG, Detterbeck FC, Wilson LD. Postoperative radiotherapy for stage II or III non-small-cell lung cancer using the surveillance, epidemiology, and end results database. J Clin Oncol. 2006;24:2998–3006. https://doi.org/10.1200/JCO.2005.04.6110.
Robinson CG, Patel AP, Bradley JD, DeWees T, Waqar SN, Morgensztern D, et al. Postoperative radiotherapy for pathologic N2 non-small-cell lung cancer treated with adjuvant chemotherapy: a review of the National Cancer Data Base. J Clin Oncol. 2015;33:870–6. https://doi.org/10.1200/JCO.2014.58.5380.
Hui Z, Men Y, Hu C, Kang J, Sun X, Bi N, et al. Effect of postoperative radiotherapy for patients with pIIIA-N2 Non-small Cell Lung Cancer after Complete Resection and Adjuvant Chemotherapy: the phase 3 PORT-C randomized clinical trial. JAMA Oncol. 2021;7:1178–85. https://doi.org/10.1001/jamaoncol.2021.1910.
Le Pechoux C, Pourel N, Barlesi F, Lerouge D, Antoni D, Lamezec B, et al. Postoperative radiotherapy versus no postoperative radiotherapy in patients with completely resected non-small-cell lung cancer and proven mediastinal N2 involvement (lung ART): an open-label, randomised, phase 3 trial. Lancet Oncol. 2022;23:104–14. https://doi.org/10.1016/S1470-2045(21)00606-9.
Ma Z, Liang B, Wei R, Liu Y, Bao Y, Yuan M, et al. Enhanced prediction of postoperative radiotherapy-induced esophagitis in non-small cell lung cancer: dosiomic model development in a real-world cohort and validation in the PORT-C randomized controlled trial. Thorac Cancer. 2023;14:2839–45. https://doi.org/10.1111/1759-7714.15068.
Ma Z, Yang X, Hui Z. Association of Heart Base Dose with overall survival in patients with NSCLC undergoing postoperative Radiotherapy. J Thorac Oncol. 2023;18:e62–4. https://doi.org/10.1016/j.jtho.2023.03.007.
Ma Z, Liu Y, Bao Y, Yuan M, Yang X, Men Y, et al. Higher lung and heart doses decrease early and long-term survival, Respectively, in patients with Non-small Cell Lung Cancer Undergoing Postoperative Radiation. Adv Radiation Oncol. 2023;8:101213. https://doi.org/10.1016/j.adro.2023.101213.
Sun X, Men Y, Wang J, Bao Y, Yang X, Zhao M, et al. Risk of cardiac-related mortality in stage IIIA-N2 non-small cell lung cancer: analysis of the Surveillance, Epidemiology, and end results (SEER) database. Thorac Cancer. 2021;12:1358–65. https://doi.org/10.1111/1759-7714.13908.
Ma Z, Liu Q, Hui Z. The cardiac effects of postoperative radiotherapy in patients with non-small cell lung cancer warrants further evaluation. Radiother Oncol. 2024;110315. https://doi.org/10.1016/j.radonc.2024.110315.
Cytlak UM, Dyer DP, Honeychurch J, Williams KJ, Travis MA, Illidge TM. Immunomodulation by radiotherapy in tumour control and normal tissue toxicity. Nat Rev Immunol. 2022;22:124–38. https://doi.org/10.1038/s41577-021-00568-1.
Abravan A, Faivre-Finn C, Kennedy J, McWilliam A, van Herk M. Radiotherapy-Related Lymphopenia affects overall survival in patients with Lung Cancer. J Thorac Oncol. 2020;15:1624–35. https://doi.org/10.1016/j.jtho.2020.06.008.
Contreras JA, Lin AJ, Weiner A, Speirs C, Samson P, Mullen D, et al. Cardiac dose is associated with immunosuppression and poor survival in locally advanced non-small cell lung cancer. Radiother Oncol. 2018;128:498–504. https://doi.org/10.1016/j.radonc.2018.05.017.
Venkatesulu B, Giridhar P, Pujari L, Chou B, Han J, Block AM, et al. Lymphocyte sparing normal tissue effects in the clinic (LymphoTEC): a systematic review of dose constraint considerations to Mitigate Radiation-Related Lymphopenia in the era of Immunotherapy. Radiother Oncol. 2022. https://doi.org/10.1016/j.radonc.2022.10.019.
Jin J-Y, Hu C, Xiao Y, Zhang H, Paulus R, Ellsworth SG et al. Higher Radiation Dose to the Immune Cells Correlates with Worse Tumor Control and Overall Survival in Patients with Stage III NSCLC: A Secondary Analysis of RTOG0617. Cancers. 2021. https://doi.org/10.3390/cancers13246193
Yin X, Luo J, Xu C, Meng C, Zhang J, Yu H, et al. Is a higher estimated dose of radiation to immune cells predictive of survival in patients with locally advanced non-small cell lung cancer treated with thoracic radiotherapy? Radiother Oncol. 2021;159:218–23. https://doi.org/10.1016/j.radonc.2021.03.026.
Ladbury CJ, Rusthoven CG, Camidge DR, Kavanagh BD, Nath SK. Impact of Radiation Dose to the Host Immune System on Tumor Control and Survival for Stage III Non-small Cell Lung Cancer treated with definitive Radiation Therapy. Int J Radiat Oncol Biol Phys. 2019;105:346–55. https://doi.org/10.1016/j.ijrobp.2019.05.064.
Wang X, Bai H, Gao M, Guan Y, Yu L, Li J, et al. Impact of radiation dose to the immune system on disease progression and survival for early-stage non-small cell lung cancer treated with stereotactic body radiation therapy. Radiother Oncol. 2023;186:109804. https://doi.org/10.1016/j.radonc.2023.109804.
Yu Y, Fu P, Jin J-Y, Gao S, Wang W, Machtay M, et al. Impact of effective dose to immune cells (EDIC) on lymphocyte nadir and survival in limited-stage SCLC. Radiother Oncol. 2021;162:26–33. https://doi.org/10.1016/j.radonc.2021.06.020.
Xu C, Jin J-Y, Zhang M, Liu A, Wang J, Mohan R, et al. The impact of the effective dose to immune cells on lymphopenia and survival of esophageal cancer after chemoradiotherapy. Radiother Oncol. 2020;146:180–6. https://doi.org/10.1016/j.radonc.2020.02.015.
Feng M, Moran JM, Koelling T, Chughtai A, Chan JL, Freedman L, et al. Development and validation of a heart atlas to study cardiac exposure to radiation following treatment for breast cancer. Int J Radiat Oncol Biol Phys. 2011;79:10–8. https://doi.org/10.1016/j.ijrobp.2009.10.058.
Ma Z, Men Y, Liu Y, Bao Y, Liu Q, Yang X, et al. Preoperative CT-based radiomic prognostic index to predict the benefit of postoperative radiotherapy in patients with non-small cell lung cancer: a multicenter study. Cancer Imaging. 2024;24:61. https://doi.org/10.1186/s40644-024-00707-6.
Formenti SC, Demaria S. Combining radiotherapy and cancer immunotherapy: a paradigm shift. J Natl Cancer Inst. 2013;105:256–65. https://doi.org/10.1093/jnci/djs629.
Chang JY, Verma V, Li M, Zhang W, Komaki R, Lu C, et al. Proton Beam Radiotherapy and Concurrent Chemotherapy for Unresectable Stage III Non-small Cell Lung Cancer: final results of a phase 2 study. JAMA Oncol. 2017;3:e172032. https://doi.org/10.1001/jamaoncol.2017.2032.
Xi M, Xu C, Liao Z, Chang JY, Gomez DR, Jeter M, et al. Comparative outcomes after definitive Chemoradiotherapy using Proton Beam Therapy Versus Intensity Modulated Radiation Therapy for Esophageal Cancer: a retrospective, single-institutional analysis. Int J Radiat Oncol Biol Phys. 2017;99:667–76. https://doi.org/10.1016/j.ijrobp.2017.06.2450.
Yuan M, Zhai Y, Men Y, Zhao M, Sun X, Ma Z, et al. Anlotinib enhances the Antitumor activity of high-dose irradiation combined with Anti-PD-L1 by potentiating the Tumor Immune Microenvironment in Murine Lung Cancer. Oxid Med Cell Longev. 2022;2022:5479491. https://doi.org/10.1155/2022/5479491.
Yuan M, Zhai Y, Men Y, Zhao M, Sun X, Ma Z, et al. Famitinib enhances the antitumor effect of radioimmunotherapy in murine lung cancer. Thorac Cancer. 2022;13:3331–40. https://doi.org/10.1111/1759-7714.14689.
Altorki NK, Walsh ZH, Melms JC, Port JL, Lee BE, Nasar A, et al. Neoadjuvant durvalumab plus radiation versus durvalumab alone in stages I-III non-small cell lung cancer: survival outcomes and molecular correlates of a randomized phase II trial. Nat Commun. 2023;14:8435. https://doi.org/10.1038/s41467-023-44195-x.
Huynh E, Hosny A, Guthier C, Bitterman DS, Petit SF, Haas-Kogan DA, et al. Artificial intelligence in radiation oncology. Nat Rev Clin Oncol. 2020;17:771–81. https://doi.org/10.1038/s41571-020-0417-8.
Funding
This study was supported by National key research and development program (2022YFC2705001), Capital’s Funds for Health Improvement and Research (2022-1-4022), Beijing Xisike Clinical Oncology Research Foundation (Y-HR2020ZD-0779), Beijing Hope Run Special Fund of Cancer Foundation of China (ZZ2021A02).
Author information
Authors and Affiliations
Contributions
Zeliang Ma: Conceptualization; Data curation; Formal analysis; Software; Writing - original draft; Writing - review & editing.Yunsong Liu, Yongxing Bao, Qian Liu, Xu Yang: Data curation.Yu Men, Jianyang Wang, Lei Deng, Yirui Zhai, Nan Bi, Luhua Wang: Project administration. Chen Hu: Methodology.Zhouguang Hui: Conceptualization; Validation; Funding acquisition; Supervision; Writing - review & editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (No. 22/292–3494). Written informed consent was waived for the use of anonymized retrospective data. The principles of the Declaration of Helsinki were followed.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ma, Z., Liu, Y., Bao, Y. et al. Higher immune cell radiation dose is correlated with poor tumor control and survival in patients with non-small cell lung cancer receiving postoperative radiotherapy. BMC Cancer 24, 968 (2024). https://doi.org/10.1186/s12885-024-12699-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12699-4