
Abstract
Background
Progressive multifocal leukoencephalopathy is a severe demyelinating disease caused by the polyoma JC virus in patients with reduced immunocompetence. A few cases of progressive multifocal leukoencephalopathy have been reported in patients treated with fumaric acid esters.
Case presentation
A 53-year-old Caucasian woman reported to our clinic with a first focal epileptic seizure and mild cognitive impairment. Since 1.5 years, she was treated with fumaderm for her psoriasis. During that time, her lymphocyte counts ranged between 450 and 700/μl. Cerebral magnet resonance imaging showed multifocal subcortical T2 hyperintense lesions with partial gadolinium enhancement. She did not have antibodies against human immunodeficiency virus 1 and 2 and cerebrospinal fluid-polymerase chain reaction for viral infections including a sensitive JC-virus polymerase chain reaction were negative. The diagnosis of progressive multifocal leukoencephalopathy was established by histological analysis and detection of JC-virus desoxyribonucleic acid in brain biopsy specimens. Dimethyl fumarate was stopped and Mirtazapin and Mefloquin were initiated. Neurological examination and imaging remained stable.
Conclusions
Progressive multifocal leukoencephalopathy can occur in patients with lymphocyte counts between 450 and 700/μl, produce only faint symptoms and is not excluded by negative JC-virus-polymerase chain reaction in cerebrospinal fluid. The incidence of progressive multifocal leukoencephalopathy may thus be underestimated and a more careful surveillance of patients would be necessary.
Similar content being viewed by others


Background
Progressive multifocal leukoencephalopathy (PML) is a severe demyelinating disease of the central nervous system (CNS) caused by the polyoma JC virus in patients with reduced immunocompetence within the CNS. PML may develop in patients treated with immunomodulatory treatment such as natalizumab, rituximab, efalizumab, infliximab or mycophenolat mofetil [1]. Recently, a few cases of PML in patients with psoriasis treated with fumaric acid esters have been reported [2–4]. In one case no severe lymphopenia was detected as the reported nadir of lymphocytic count was 792/μl [5]. The active antipsoriatic agent monomethylfumarate inhibits the expression of proinflammatory cytokines, tumor necrosis factor alpha, interleukin-6, interleukin-1 alpha [6] and increases the secretion of interleukin-4 and interleukin-10 by helper T-cells [7]. Dimethyl fumarate was also introduced as an oral drug for relapsing remitting forms of multiples sclerosis (MS) [8]. Regarding the fact that we are already facing the problem of inducing PML in MS patients treated with natalizumab and dimethyl fumarate becoming an alternative drug in these cases, it is of major interest to understand more about the risk of developing PML by fumarate therapy.
Case presentation
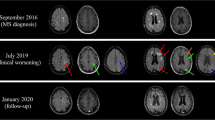
A 53-year-old Caucasian woman reported to our clinic in September 2014 with a first and acute episode of transient confusion and sensory aphasia and a two days history of headache. She was on medication for arterial hypertension and hypothyroidism. Since May 2013 she received dimethyl fumarate (Fumaderm®) for the treatment of psoriasis. The patient only received topical treatment prior to dimethyl fumarate. Her clinical examination on admission was unremarkable. Cerebral magnet resonance imaging (MRI) showed several subcortical T2 hyperintense and partially contrast-enhancing lesions in the right frontal and left parietal lobes, which were increased in size on follow-up MRI two weeks later (Fig. 1).

MRI of the patient’s brain in the course of the disease. shows MR imaging of the brain at the onset of symptoms and imaging controls after two weeks and 3.5 months. Several subcortical lesions are located in the right frontal and left parietal lobe and show progression during the first two weeks. They present hyperintense lesions in T2/FLAIR with partial increased signal in contrast-enhanced imaging.
Cerebrospinal fluid (CSF) protein was slightly elevated (54 mg/l), cell count and IgG-Index were normal and she had identical oligoclonal bands in serum and CSF. She did not have antibodies against (Human immunodeficiency virus) HIV 1 and 2 and polymerase chain reaction (PCR) for JC-virus desoxyribonucleic acid (DNA) (University Tübingen (sensitivity of JC-virus DNA: > 1000 copies) and University Düsseldorf (sensitivity of JC-virus DNA: > 4 copies/assay [9]), Germany) of CSF was negative. Histological analysis of a biopsy of the right frontal lesion showed infiltration of lymphocytes, perivascular CD45-positive cells, CD68-positive microglia, reactive astrocytosis and focal demyelination (Fig. 2). Some cells had intranuclear inclusions and stained positive with an antibody against JC virus. PCR of brain tissue for JCV DNA was positive and confirmed the diagnosis of PML.

Histological analysis of a brain biopsy from the right frontal lesion. (a) Enlarged nuclei containing viral inclusions (arrows). Hematoxylin and eosin. (b) Enlarged nuclei appear immunopositive when labeled with an antibody to JC-virus/SV40.
Treatment with dimethyl fumarate was stopped and she was put on 250 mg Mefloquin per week and 45 mg Mirtazapin per day. The patients peripheral lymphocyte counts during treatment with dimethyl fumarate were retrospectively evaluated (Fig. 3) and ranged between 450 and 700 cells/μl while her leucocyte counts were higher than 3000/μl during the whole treatment period. The initial symptoms were considered to be epileptic and treatment with 1000 mg/day Levetiracetam was initiated. Upon follow-up three months later, the patient reported of persistent difficulties with concentration and word retrieval. Aphasia could not be detected in simple conversation and bed side tests. Neurological examination as well as repeated cerebral MRI showed no evidence for disease progression or immune reconstitution inflammatory syndrome. Upon 7-month follow-up the patient reported a stable course of disease with unchanged minor difficulties with concentration and word retrieval, which were very mild and could not be detected in conversation or neurological examination. The MRI showed an increase of the T2 hyperintense lesion in the right frontal lobe, while gadolinium enhancement and the other lesions remained unaltered. The patient tolerated the treatment well and reported no adverse events.

Absolute numbers of lymphocytes and dose of fumaric acid. After two months of application the lymphocyte count fell to a level of 700 cells/μl. At that point treatment was stopped until lymphocyte count recovered to a number of 900/μl after two and a half months. Dimethyl fumarate was given in an increasing dose up to 360 mg per day. When the symptoms of the psoriasis remained stable, the daily dose was decreased to 240 mg and increased again when the symptoms remitted. At the same time lymphocytes remained at an average level of about 600/μl. When they first fell under 500 cells/μl in October 2014, dimethyl fumarate dose was reduced to 120 mg. Finally, the therapy was stopped by the diagnosis of a PML. During the following months lymphocytes recovered slowly and reaching a number of 3000 – 5000 cells/μl.
Conclusions
A few cases of PML in patients treated with fumarates have been reported [3, 10, 11]. This case demonstrates that clinical examination, imaging of the brain and a sensitive JCV DNA PCR of CSF may not be sufficient to establish the diagnosis. There is evidence that an important risk factor for the development of PML is prolonged therapy-associated lymphopenia [12]. In these cases, discontinuation of the treatment is inevitable. The recommended acceptable threshold for therapy-associated lymphopenia is specific for any given drug. While the dosage of dimethyl fumarate has to be reduced when lymphocyte counts are lower than 700/μl, this threshold is 200/μl for fingolimod. Our patient demonstrates that PML can occur in patients with lymphocyte counts ranging between 450 and 700/μl for prolonged time periods. In another reported case, the lymphocyte nadir was 792/μl, indicating that no severe lymphopenia is required for PML to develop [5]. An alteration of immune surveillance for months or years appears to be critical for the development PML as it is the case in patients treated with natalizumab or efalizumab [13]. This case further demonstrates that PML may cause no or only faint symptoms and is not excluded by negative sensitive PCR for JCV DNA. Sensitivity of the assay used in the reference laboratory in Düsseldorf was 3.9 copies/assay (117 copies/ml), as they used an amplification protocol identical to the one used by Ryschekowitsch et al. [9]. As the sensitivity in various laboratories differs it could be necessary to analyse the CSF in a more sensitive laboratory in case of a negative result. Moreover, reactivation of JCV may not only lead to PML, but also to JCV associated granule cell neuronopathy [4, 14, 15], JCV encephalopathy [16] or JCV associated meningitis [17].
The incidence of PML in patients with long term immunomodulating or immunosuppressive therapy is thus possibly currently underestimated and a more careful surveillance of these patients would be necessary.
Consent
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Abbreviations
- CNS:
-
central nervous system
- CSF:
-
cerebrospinal fluid
- DNA:
-
desoxyribonucleic acid
- HIV-1/HIV-2:
-
human immunodeficiency virus
- JC-Virus:
-
polyoma JC-virus
- MRI:
-
magnet resonance imaging
- MS:
-
multiples sclerosis
- PCR:
-
polymerase chain reaction
- PML:
-
progressive multifocal leukoencephalopathy
References
Ferenczy MW, Marshall LJ, Nelson CD, Atwood WJ, Nath A, Khalili K, et al. Molecular biology, epidemiology, and pathogenesis of progressive multifocal leukoencephalopathy, the JC virus-induced demyelinating disease of the human brain. Clin Microbiol Rev. 2012;25(3):471–506. doi:10.1128/CMR.05031-11 25/3/471 [pii].
Sweetser MT, Dawson KT, Bozic C. Manufacturer's response to case reports of PML. N Engl J Med. 2013;368(17):1659–61. doi:10.1056/NEJMc1300283.
van Oosten BW, Killestein J, Barkhof F, Polman CH, Wattjes MP. PML in a patient treated with dimethyl fumarate from a compounding pharmacy. N Engl J Med. 2013;368(17):1658–9. doi:10.1056/NEJMc1215357.
Stoppe M, Thoma E, Liebert UG, Major EO, Hoffmann KT, Classen J, et al. Cerebellar manifestation of PML under fumarate and after efalizumab treatment of psoriasis. J Neurol. 2014;261(5):1021–4. doi:10.1007/s00415-014-7311-1.
Nieuwkamp DJ, Murk JL, van Oosten BW, Cremers CH, Killestein J, Viveen MC, et al. PML in a patient without severe lymphocytopenia receiving dimethyl fumarate. N Engl J Med. 2015;372(15):1474–6. doi:10.1056/NEJMc1413724.
Helwa I, Patel R, Karempelis P, Kaddour-Djebbar I, Choudhary V, Bollag WB. The antipsoriatic agent monomethylfumarate has antiproliferative, prodifferentiative, and anti-inflammatory effects on keratinocytes. J Pharmacol Exp Ther. 2015;352(1):90–7. doi:10.1124/jpet.114.218818 jpet.114.218818 [pii].
idec b. Fachinformation Fumaderm. 2013. http://www.fachinfo.de/pdf/000847.
Gold R, Kappos L, Arnold DL, Bar-Or A, Giovannoni G, Selmaj K, et al. Placebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosis. N Engl J Med. 2012;367(12):1098–107. doi:10.1056/NEJMoa1114287.
Ryschkewitsch C, Jensen P, Hou J, Fahle G, Fischer S, Major EO. Comparison of PCR-southern hybridization and quantitative real-time PCR for the detection of JC and BK viral nucleotide sequences in urine and cerebrospinal fluid. J Virol Methods. 2004;121(2):217–21. doi:10.1016/j.jviromet.2004.06.021.
Ermis U, Weis J, Schulz JB. PML in a patient treated with fumaric acid. N Engl J Med. 2013;368(17):1657–8. doi:10.1056/NEJMc1211805.
Sweetser MT, Dawson KT, Bozic C. Case reports of PML in patients treated for psoriasis. N Engl J Med. 2013;369(11):1082.
Bellizzi A, Nardis C, Anzivino E, Rodio D, Fioriti D, Mischitelli M, et al. Human polyomavirus JC reactivation and pathogenetic mechanisms of progressive multifocal leukoencephalopathy and cancer in the era of monoclonal antibody therapies. J Neurovirol. 2012;18(1):1–11. doi:10.1007/s13365-012-0080-7.
Kothary N, Diak IL, Brinker A, Bezabeh S, Avigan M, Dal PG. Progressive multifocal leukoencephalopathy associated with efalizumab use in psoriasis patients. J Am Acad Dermatol. 2011;65(3):546–51. doi:10.1016/j.jaad.2010.05.033.
Koralnik IJ, Wuthrich C, Dang X, Rottnek M, Gurtman A, Simpson D, et al. JC virus granule cell neuronopathy: A novel clinical syndrome distinct from progressive multifocal leukoencephalopathy. Ann Neurol. 2005;57(4):576–80. doi:10.1002/ana.20431.
Schippling S, Kempf C, Buchele F, Jelcic I, Bozinov O, Bont A, et al. JC virus granule cell neuronopathy and GCN-IRIS under natalizumab treatment. Ann Neurol. 2013;74(4):622–6. doi:10.1002/ana.23973.
Wuthrich C, Dang X, Westmoreland S, McKay J, Maheshwari A, Anderson MP, et al. Fulminant JC virus encephalopathy with productive infection of cortical pyramidal neurons. Ann Neurol. 2009;65(6):742–8. doi:10.1002/ana.21619.
Agnihotri SP, Wuthrich C, Dang X, Nauen D, Karimi R, Viscidi R, et al. A fatal case of JC virus meningitis presenting with hydrocephalus in a human immunodeficiency virus-seronegative patient. Ann Neurol. 2014;76(1):140–7. doi:10.1002/ana.24192.
Acknowledgments
We thank our patient for her participation and her consent to publish these data. We acknowledge support by Deutsche Forschungsgemeinschaft and Open Access Publishing Fund of University of Tübingen.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
FB receives compensation for serving on Scientific Advisory Boards for Bayer Healthcare, Biogen Idec, Genzyme and Novartis, speaker honoraria and travel support from Biogen Idec, Fresenius Medical Care, Genzyme and Novartis and research support from Novartis. The other authors declare that they have no competing interests.
Authors’ contribution
ND took care of the patient, evaluated data and drafted the manuscript. VS took care of the patient and helped to draft the manuscript, TKH evaluated the MRI and designed the figures of the MRI, and AB evaluated the histological analysis and designed the figures of the histological analysis. FB suggested the case report, took care of the patient and drafted the manuscript. All authors read and approved the final manuscript.
Authors’ information
ND and VS are resident physicians in neurology, TKH is senior physician in neuroradiology AB is senior physician in neuropathology FB is senior physician in neurology and group leader at the Hertie Institute for Clinical Brain Research Tübingen. All authors work at the University Tübingen.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Dammeier, N., Schubert, V., Hauser, TK. et al. Case report of a patient with progressive multifocal leukoencephalopathy under treatment with dimethyl fumarate. BMC Neurol 15, 108 (2015). https://doi.org/10.1186/s12883-015-0363-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-015-0363-8