
Abstract
Background
Serum lipoprotein(a) [Lp(a)] is an independent risk factor for atherosclerotic cardiovascular disease (ASCVD) in the general population, its association with ASCVD incidence in Chinese maintenance hemodialysis (MHD) patients remains unclear. We aimed to evaluate the relationship between Lp(a) levels and ASCVD incidence among MHD patients in Beijing, China.
Methods
This retrospective, observational cohort study included MHD patients at Beijing Tongren Hospital from January 1, 2013 to December 1, 2020, and followed until December 1,2023. The primary outcome was ASCVD occurrence. Kaplan-Meier survival analysis was used to evaluate ASCVD-free survival in MHD patients, with stratification based on Lp(a) levels. Cox regression analyses were conducted to assess the association between Lp(a) levels and the occurrence of ASCVD.
Results
A total of 265 patients were enrolled in the study. The median follow-up period were 71 months.78 (29.4%) participants experienced ASCVD events, and 118 (47%) patients died, with 58 (49.1%) deaths attributed to ASCVD. Spearman rank correlation analyses revealed positive correlations between serum Lp(a) levels and LDL-c levels, and negative correlations with hemoglobin, triglyceride, serum iron, serum creatinine, and albumin levels. Multivariate Cox regression analysis showed that Lp(a) levels ≥ 30 mg/L, increased age, decreased serum albumin levels, and a history of diabetes mellitus were significantly associated with ASCVD incidence.
Conclusions
This study demonstrated an independent and positive association between serum Lp(a) levels and the risk of ASCVD in MHD patients, suggesting that serum Lp(a) could potentially serve as a clinical biomarker for estimating ASCVD risk in this population.
Similar content being viewed by others

Introduction
Lipoprotein (a) (Lp(a)) is a complex particle present in human plasma. Its structure closely resembles that of low-density lipoprotein (LDL), but it is distinguished by the presence of a specific glycoprotein called apolipoprotein(a) [apo(a)] [1,2,3,4]. This glycoprotein is similar to plasminogen and is covalently linked to apolipoprotein B-100 through a disulfide bond. Lp(a) plays a role in promoting arteriosclerosis and blood coagulation [4,5,6,7,8]. Lp(a) has been observed in atherosclerotic lesions of saphenous vein bypass grafts and native coronary arteries, distributed similarly to LDL. In the general population, elevated levels of Lp(a) are an independent risk factor for atherosclerotic cardiovascular diseases (ASCVD) due to mechanisms associated with increased atherogenesis, inflammation, and thrombosis [9,10,11].
ASCVD mortality is the leading cause of death, among individuals undergoing hemodialysis, with a mortality rate at least 10 times higher than that of the general population [9, 12, 13]. Additionally, 40% of end-stage renal disease (ESRD) patients have CVD at the initiation of dialysis, and the risk for recurrent ASCVD events is likely to be much higher [14, 15]. However, the research findings on the correlation between Lp(a) and ASCVD risk among ESRD patients are inconsistent [16,17,18,19].
On the other hand, Lp(a) concentrations have been observed to exhibit racial disparities, surpassing those of any other cardiovascular biomarker [10, 20,21,22]. Limited research has been conducted on the correlation between Lp(a) and the risk of ASCVD in the Chinese population undergoing hemodialysis. The present retrospective study analyzed the association between serum Lp(a) and the risk of ASCVD in a longitudinal cohort of patients treated with maintenance hemodialysis (MHD), with a median follow-up of 71 months.
Patients and methods
Study population
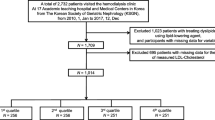
This retrospective, observational cohort study included all patients who underwent maintenance hemodialysis (MHD) at Capital Medical University, Beijing Tongren Hospital from January 1, 2013 to December 1, 2020, and followed until December 1,2023. Eligible subjects were aged 18 years or older at the start of MHD and survived for at least 90 days from their initial hemodialysis therapy. Patients who underwent renal transplantation or peritoneal dialysis (PD), were excluded. Before starting the study, all participants signed informed consent forms, wherein they were informed that the research would entail collecting their medical information without including any personal details. The medical data obtained from participants was exclusively used for research purposes and was securely stored to maintain confidentiality and prevent any unauthorized disclosure. The study protocol was approved by the institute’s ethics committee of Beijing Tongren Hospital. The ethics approval number for this study is TREC2024-KY110.
Data collection and measurements
Baseline demographic data, including age, gender, complications, and medication use, were obtained from the patients’ medical records. Biochemical data at baseline, including Lp(a), Kt/V, urea reduction ratio (URR), leukocyte counts(WBC), hemoglobin, serum creatinine, blood urea nitrogen (BUN), serum uric acid, serum albumin, corrected serum calcium, serum phosphate, intact parathyroid hormone (PTH) values, serum iron, ferritin, total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c), and C-reactive protein (CRP), were assessed in the biochemical laboratory of Capital Medical University, Beijing Tongren Hospital. The concentrations of plasma TG, TC, LDL-c, HDL-c, serum creatinine, BUN, uric acid, and serum albumin were measured using an automatic biochemistry analyzer (Hitachi 7150, Tokyo, Japan). All laboratory testing were in accord with standard biochemical analysis procedures. Lp(a) was measured on a Siemens Atellica (Siemens, Munich, Germany) platform and using the immunoturbidimetric Denka Seiken developed Roche 2nd generation assay (Roche Professional Diagnostics, Rotkreuz, Switzerland) with minimal apolipoprotein(a) isoform size bias. The intraassay coefficient of variation was ≤ 10%. A threshold of 30 mg/dL was used to classify patients into an elevated Lp(a) group and a normal Lp(a) group. Corrected serum calcium = calcium + 0.8 × (4 – serum albumin). URR = (BUN before dialysis-BUN after dialysis)/BUN before dialysis. Kt/V was calculated according to the second-generation formula of Daugirdas [23]. All data were obtained within three months after the initiation of hemodialysis.
Outcomes
The primary outcome of this study was the occurrence of atherosclerotic cardiovascular disease (ASCVD) during the follow-up period. ASCVD was defined as a composite outcome including hospitalization for myocardial infarction (MI), hospitalization for ischemic stroke, hospitalization for peripheral artery disease (PAD), death due to coronary heart disease (CHD), or death due to stroke. Incident cases of ASCVD were identified using death certificate data and hospital record linkage. To confirm the occurrence of study outcomes, medical records were reviewed and validated by three nephrologists in our HD center. MI hospitalization was defined based on symptoms, levels of cardiac biomarkers, and electrocardiograms consistent with acute myocardial ischemia. Ischemic stroke hospitalization was defined based on sudden neurological symptoms and neuroimaging consistent with acute cerebral infarction. PAD hospitalization was defined based on peripheral artery bypass or angioplasty, or major amputation due to occlusive PAD. Deaths were identified through the retrieval of death certificates, as well as hospital and outpatient records.
Statistical analysis
Results were reported as mean ± standard deviation (SD) or median and interquartile range, depending on the distribution of the data, for continuous variables. Categorical variables were expressed as frequencies. Statistical analyses were performed using SPSS 23 for Windows (SPSS, Inc., Chicago, IL, USA). ANOVA analysis was used to compare groups for normally distributed continuous variables, while nonparametric tests were used for non-normally distributed variables. The chi-square test was utilized for categorical variables. Spearman correlation was used to assess the relationship between Lp(a) levels and baseline clinical parameters. Kaplan-Meier survival analysis was used to evaluate ASCVD-free survival in MHD patients, with stratification based on Lp(a) levels. Cox regression analyses were conducted to assess the association between Lp(a) levels and the occurrence of ASCVD. To assess the proportional hazards assumption in the Cox regression models, each covariate was transformed into a time-dependent covariate x*ln(t) and simultaneously included in the single-factor Cox regression equation. Covariates with P-values above 0.05 were considered to meet the assumption and included in the model. However, for covariates such as age with P-values < 0.05, further stratified analysis was performed to ensure compliance with the proportional hazards assumption before reintroducing them into the Cox regression model. Missing data were handled using multiple imputation techniques to minimize bias and ensure study validity. Statistical significance was defined as p < 0.05.
Results
A total of 290 patients undergoing MHD at dialysis center of Beijing Tongren Hospital, since January 1, 2013 to December 1, 2020. Of 290 MHD patients, 25 patients were transferred to transplantation. Thus, a total of 265 MHD patients were eligible for the study. The baseline characteristic data of patients are shown in Table 1. The mean age of the study participants was 63.78 ± 14.89 years, with 176 (66.4%) being men. Among the participants, 102(38.5%)had higher Lp(a) levels (≥ 30 mg/dL), and these individuals were more likely to have lower hemoglobin and serum iron levels. Compared to the normal Lp(a) group, the elevated Lp(a) group exhibited significantly lower serum albumin and lower serum creatinine. There were no significant differences in the prevalence of hypertension and ASCVD among the baseline characteristics. The median concentration of Lp(a) was 19.5 mg/dL, with the 25th and 75th percentiles being 10.2 and 42.3 mg/dL, respectively. The participants were categorized by quartiles based on their Lp(a) levels, and the baseline data are presented in Table 2.
Spearman rank correlation analyses revealed that serum Lp(a) levels positively correlated with LDL-c levels and negatively correlated with hemoglobin, triglyceride, serum iron, serum creatinine, and albumin levels (P<0.05) (Table 3).
During a median follow-up period of 71 months (interquartile[IQR] 36–119), 78(29.4%)participants experienced ASCVD events. These events consisted of 49 cases of MI, 17 cases of ischemic stroke, and 12 cases of PAD. Additionally, 118 (44.5%) patients died, with 45 (38.1%) attributed to cardiovascular disease (CVD), 13 (11.0%) to stroke, 7 (5.9%) to malignant tumors, 38 (32.2%) to infection, 2 (1.7%) to gastrointestinal bleeding, 5 (4.2%) to malnutrition, and 6 (5.1%) to other causes.
The percentage of patients free from ASCVD at the first, third, and fifth year of follow-up were as follows: in the normal Lp(a) group, 96.1%, 91.9%, and 85.1%; in the elevated Lp(a) group, 89%, 72.8%, and 60.4%. Patients in the elevated Lp(a) group exhibited a lower cumulative ASCVD-free survival rate (log-rank test χ2 = 38.46, p = 0.000) compared to those in the normal Lp(a) group (Fig. 1).

Subgroups analysis of Lp(a) with ASCVD incidence
Univariate Cox regression analyses revealed that a history of diabetes mellitus, decreased Hct levels, Lp(a) ≥ 30 mg/L, higher fasting blood-glucose levels, elevated uric acid (UA) levels, higher phosphorus levels, lower serum albumin levels, and an inflammatory status were significantly associated with an increased incidence of ASCVD. Based on these univariate findings, multivariate Cox regression analyses were conducted to further investigate the risk factors associated with ASCVD. The results showed that Lp(a) levels ≥ 30 mg/L, increased age, decreased serum albumin levels, and a history of diabetes mellitus were significantly associated with the incidence of ASCVD (Table 4). To further explore the relationship between Lp(a) and ASCVD under different conditions, a stratified univariate Cox regression analysis was performed to assess the association between elevated Lp(a) levels and the risk of ASCVD. The study population was stratified based on albumin levels, history of diabetic mellitus, history of ASCVD, age, statin in use, and gender. Figure 2 illustrated a significant association between lipoprotein(a) levels ≥ 30 mg/dL and an elevated incidence of ASCVD, irrespective of history of ASCVD at baseline, history of diabetes status, and statin use. However, the impact of Lp(a) on ASCVD risk appeared to be attenuated in the subgroup with albumin levels below 35 g/L (HR 5.37[0.94–2.24], P = 0.071). Table 5 presented the results of the association between lipoprotein(a) levels and the risk of ASCVD events after adjusting for various confounding factors. The analysis revealed that individuals with Lp(a) levels ≥ 30 mg/dL had a significantly increased risk of ASCVD (HR 17.84 [4.03–78.97], P = 0.000) even after accounting for factors such as age, gender, disease history, statin use history, clinical data, and dialysis adequacy index. Furthermore, it found that for every 1 mg/L increase in Lp(a) levels, there was a corresponding increase in the risk of ASCVD events even after adjusting for multiple confounding factors.

Kaplan-Meier survival analysis of ASCVD-free status in MHD patients with different serum Lp(a) levels
Discussion
This study aimed to investigate the relationship between serum Lp(a) levels and the incidence of ASCVD in Chinese MHD patients. Our findings indicated that a high serum Lp(a) level is an independent predictor of incident ASCVD in MHD patients.
The kidney has been shown to play a role in the degradation of Lp(a), as evidenced by the impact of chronic kidney disease on Lp(a) levels, the presence of apo(a) fragments in urine, and the difference in Lp(a) concentrations between arterial and venous blood in the renal circulation [8]. Several studies have demonstrated that Lp(a) levels increase as renal function declines [24, 25].
A large-scale meta-analysis involving 126,634 participants and 1.3 million person-years of follow-up has confirmed previous findings that identified an inflection point for the risk of myocardial infarction at Lp(a) levels exceeding 30 mg/dL [1, 26]. The 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia consider Lp(a) greater than 30 mg/dL to be a risk factor for CAD [27]. Similarly, the 2023 Chinese Guidelines for Lipid Management indicate that Lp(a) levels above 30 mg/dL increase the risk of ASCAD [28]. In our study, a threshold of 30 mg/dL was used to classify patients into an elevated Lp(a) group and a normal Lp(a) group. Previous research has reported that the proportion of elevated Lp(a) in the general population is approximately 12-20.3% [29]. However, our study revealed that in the MHD population, this proportion reaches 38.5%, suggesting higher levels of Lp(a) in MHD patients compared to the general population.
In MHD patients, Lp(a) levels were found to inversely correlate with serum creatinine and albumin concentrations prior to hemodialysis sessions. Serum creatinine and albumin are commonly used as markers of nutritional status in this patient population. This inverse association suggests that MHD patients with suboptimal nutritional status may exhibit higher Lp(a) concentrations. Physiologically, diminished albumin levels may instigate an upregulation in the synthesis of apolipoprotein B (apo[B])-containing lipoprotein particles, including Lp(a), thereby contributing to their elevated levels [30, 31]. Notably, there was no correlation between Lp(a) levels and the adequacy indicators of hemodialysis, namely KT/V and URR, suggesting that conventional hemodialysis techniques are ineffective in removing Lp(a).
Furthermore, Lp(a) was positively correlated with LDL-c levels and negatively correlated with TG levels. Interestingly, we found a significantly higher proportion of statins in the group with elevated Lp(a) compared to the normal group. Previous studies have reported that statins can increase Lp(a) levels by 10–20% [1], which may explain why some patients do not respond well to statin therapy in terms of lowering LDL-c levels, as their cholesterol may primarily be present in Lp(a) rather than LDL particles [32]. Statins induce upregulation of LDL receptors (LDLR), however, the role of the LDLR in Lp(a) clearance is minor [33], on the other hand, statin treatment increased LPA expression and apolipoprotein(a) production and secretion [34]. The mechanism of Lp(a) cellular uptake remains unclear, with other receptors such as macrophage scavenger receptors, megalin receptors, asialoglycoprotein receptors being considered to be involved in Lp(a) uptake. The capacity of macrophages to uptake Lp(a) is crucial, as the excessive uptake of lipoproteins by macrophages, leading to their transformation into foam cells, is a major mechanism of atherogenesis [35]. Similar to LDL-c, Lp(a) does not originate from the catabolism of another lipoprotein. In individuals with elevated triglyceride levels, Lp(a) is reduced, likely due to increased plasma lipoprotein clearance [36]. In the present study, elevated Lp(a) levels were found to be a risk factor for ASCVD events, independent of statin use. Univariate cox regression analyses showed that statin use was associated with an increased ASCVD risk, while multivariate cox regression analysis showed the association was not significant after adjusting for Lp(a) levels.
Elevated levels of Lp(a) have been associated with a negative impact on iron metabolism, often leading to lower serum iron and hemoglobin levels. This inverse relationship may stem from the inflammatory role of Lp(a), which can activate the NF-κB pathway in monocytes, and increase inflammation [4, 37,38,39]. Heightened inflammation can affect hepcidin levels, a master regulator of iron homeostasis, leading to disturbances in iron metabolism and an increased risk of anemia, especially in conditions such as maintenance hemodialysis (MHD) [40]. Thus, Lp(a) may be indirectly contributing to iron utilization impairment and anemia.
Previous studies have shown that high levels of Lp(a) are associated with the progression of atherosclerosis and an increased risk of ASCVD events in the general population [29]. However, the research findings on the role of Lp(a) in relation to incident ASCVD among patients with renal failure are inconclusive and contradictory. Koda et al [41] conducted a study on Japanese hemodialysis patients and found that those with Lp(a) values ≥ 30 mg/dl had a significantly higher risk of cardiovascular mortality (RR 3.93). Xu et al [16] reported that high serum Lp(a) levels were associated with an increased risk of death from cardiovascular events in peritoneal dialysis patients. However, another study involving 440 hemodialysis patients did not find a significant association between Lp(a) levels and outcomes related to coronary artery disease [17]. Similarly, Poudel et al [18] found no association between Lp(a) and the risk of recurrent ASCVD events in adults with CKD. Additionally, a retrospective study investigated the predictive value of baseline serum Lp(a) levels for subsequent stroke and found that higher levels were associated with a lower risk of hemorrhagic stroke [19].
At the initiation of hemodialysis, we conducted a baseline assessment that showed no significant difference in the prevalence of ASCVD among patients irrespective of their serum Lp(a) levels. However, as the study progressed, we observed a significant difference in the incidence rate of ASCVD between patients with elevated Lp(a) levels and those with normal levels during the follow-up period. Notably, patients with elevated Lp(a) levels had a higher incidence rate of ASCVD compared to those with normal levels. This highlights the potential of Lp(a) as a prognostic marker for cardiovascular risk among the hemodialysis population.
Furthermore, the multivariate Cox regression analyses showed that demonstrated significant associations between increased age, decreased serum albumin levels, a history of diabetes mellitus, and the incidence of ASCVD. Diabetes has been widely recognized as a conventional risk factor for ASCVD [8], particularly in individuals with MHD [42, 43].
Previous studies have reported a higher prevalence of malnutrition and inflammation in patients with CKD [44].Proinflammatory cytokines and malnutrition play a crucial role in the development of atherosclerosis in ESRD [45]. Univariate Cox regression analyses revealed that lower serum albumin levels and higher CRP levels were associated with an increased incidence of ASCVD during the follow-up period. After adjusting for other confounding factors, the multivariate Cox regression analysis indicated that hypoproteinemia is a significant risk factor for ASCVD. Furthermore, Lp(a) was not identified as a risk factor for ASCVD in individuals with serum albumin levels < 35 g/L, whereas it remained a significant predictor of ASCVD in those with normal serum albumin levels. This suggests that albumin as a crucial mediator in the relationship between Lp(a) and ASCVD. Firstly, Serum albumin plays a pivotal role in lipoprotein metabolism, encompassing processes such as synthesis, secretion, and clearance [46]. Decreased serum albumin levels have been associated with elevated Lp(a) levels, potentially attenuating the predictive capacity of Lp(a) for ASCVD. Secondly, low albumin levels may reflect poor nutritional status or the presence of other underlying diseases, which may be related to ASCVD risk and not solely influenced by Lp(a). Additionally, low albumin levels may be associated with other inflammatory factors or metabolic abnormalities that could also influence the development and progression of ASCVD, making the link between lipoprotein(a) and ASCVD risk less evident.
Several limitations should be acknowledged in the present study. Firstly, the study focused exclusively on the Chinese Han population in a single center. Conducting a multi-center study would improve the generalizability of the results by including diverse populations from different regions, providing a more comprehensive understanding of the association between Lp(a) levels and ASCVD risk in MHD patients. Secondly, although Lp(a) was measured using the immunoturbidimetric Denka Seiken developed Roche 2nd generation assay with minimal apolipoprotein(a) isoform size bias, our study did not measure apo(a) isoforms in the study population. It potentially introduced bias into our results because apo(a) isoforms are associated with Lp(a) concentration and can partly predict ASCVD risk. However, recent research suggests that circulating plasma Lp(a) concentration is a more accurate predictor of ASCVD risk than apo(a) isoform size or variations within the LPA gene locus [3, 47]. Mendelian randomization studies also indicate that reducing Lp(a) concentration may be beneficial in preventing ASCVD, as shown by Gudbjartsson et al. highlighting the superiority of circulating plasma Lp(a) concentration as a predictor of ASCVD risk compared to apo(a) isoform size [48]. Lastly, it is essential to acknowledge that the retrospective observational design of our study limits our ability to establish causal relationships based on the findings. To further clarify the relationship between Lp(a) levels and ASCVD events, we recommend conducting a prospective cohort study in the future.
Conclusions
The present study demonstrated an independent and positive association between serum Lp(a) levels and the risk of ASCVD in patients undergoing MHD. These findings suggest that serum Lp(a) could potentially serve as a clinical biomarker for estimating the risk of ASCVD in HD-treated patients.
Data availability
The datasets analyzed in the current study are not publicly available to ensure privacy of research participants and comply with regulations of the ethics approval. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ASCVD:
-
Atherosclerotic cardiovascular diseases
- BUN:
-
Blood urea nitrogen
- CRP:
-
C-reactive protein
- HDL:
-
High-density lipoprotein cholesterol
- LDL:
-
Low-density lipoprotein cholesterol
- Lp(a):
-
Lipoprotein a
- MHD:
-
Maintenance hemodialysis
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- UA:
-
Uric acid
- URR:
-
Urea reduction ratio
- PTH:
-
Intact parathyroid hormone
References
Tsimikas S. A test in Context: lipoprotein(a): diagnosis, prognosis, controversies, and emerging therapies. J Am Coll Cardiol. 2017;69(6):692–711.
Kamstrup PR. Lipoprotein(a) and Cardiovascular Disease. Clin Chem. 2021;67(1):154–66.
Ruscica M, Sirtori CR, Corsini A, Watts GF, Sahebkar A. Lipoprotein(a): knowns, unknowns and uncertainties. Pharmacol Res. 2021;173:105812.
Lampsas S, Xenou M, Oikonomou E et al. Lipoprotein(a) in atherosclerotic diseases: from pathophysiology to diagnosis and treatment. Molecules. 2023. 28(3).
Sanchez Muñoz-Torrero JF, Rico-Martín S, Álvarez LR, Aguilar E, Alcalá JN, Monreal M. Lipoprotein (a) levels and outcomes in stable outpatients with symptomatic artery disease. Atherosclerosis. 2018;276:10–4.
Madsen CM, Kamstrup PR, Langsted A, Varbo A, Nordestgaard BG. Lipoprotein(a)-Lowering by 50 mg/dL (105 nmol/L) may be needed to reduce Cardiovascular Disease 20% in secondary Prevention: a Population-based study. Arterioscler Thromb Vasc Biol. 2020;40(1):255–66.
Koji Yanaka HA, Takahiro Imanaka KM, Nagataka Yoshihara TK, Takamasa Tanaka MAaMI. Relationship Between Lipoprotein(a) and Angiographic Severity of Femoropopliteal Lesions. J Atheroscler Thromb, 2021; 28: 555–561. https://doi.org/10.5551/jat.56457. 2021. 28: 555–561.
Hussain Z, Iqbal J, Liu H, Zhou HD. Exploring the role of lipoprotein(a) in cardiovascular diseases and diabetes in Chinese population. Int J Biol Macromol. 2023;233:123586.
Cressman MD, Heyka RJ, Paganini EP, et al. Lipoprotein(a) is an independent risk factor for cardiovascular disease in hemodialysis patients. Circulation. 1992;86(2):475–82.
Reyes-Soffer G, Ginsberg HN, Berglund L, et al. Lipoprotein(a): a genetically determined, causal, and prevalent risk factor for atherosclerotic Cardiovascular Disease: A Scientific Statement from the American Heart Association. Arterioscler Thromb Vasc Biol. 2022;42(1):e48–60.
Marcovina SM. Lipoprotein(a): a genetically determined risk factor for Cardiovascular disease. Crit Rev Clin Lab Sci. 2023;60(8):560–72.
Zheng J, Zhang Y, Rasheed H, et al. Trans-ethnic mendelian-randomization study reveals causal relationships between cardiometabolic factors and chronic kidney disease. Int J Epidemiol. 2022;50(6):1995–2010.
Zhang J, Jia L, Yang Y, Xiao A, Lin X. Lipoprotein (a) and myocardial infarction: impact on long-term mortality. Lipids Health Dis. 2023;22(1):70.
Stack AG, Bloembergen WE. Prevalence and clinical correlates of coronary artery disease among new dialysis patients in the United States: a cross-sectional study. J Am Soc Nephrol. 2001;12(7):1516–23.
Parekh RS, Zhang L, Fivush BA, Klag MJ. Incidence of atherosclerosis by race in the dialysis morbidity and mortality study: a sample of the US ESRD population. J Am Soc Nephrol. 2005;16(5):1420–6.
Xu LC, Zhou FF, Li M et al. The correlation between serum lipoprotein(a) and risk of mortality in patients on peritoneal Dialysis. Clin Lab. 2022. 68(8).
Kronenberg F, Neyer U, Lhotta K, et al. The low molecular weight apo(a) phenotype is an independent predictor for coronary artery disease in hemodialysis patients: a prospective follow-up. J Am Soc Nephrol. 1999;10(5):1027–36.
Poudel B, Rosenson RS, Kent ST, et al. Lipoprotein(a) and the risk for recurrent atherosclerotic Cardiovascular events among adults with CKD: the chronic renal insufficiency cohort (CRIC) study. Kidney Med. 2023;5(7):100648.
Chen Y, Zhan X, Zhao Q, et al. Serum lipoprotein(a) and risk of hemorrhagic stroke among incident peritoneal dialysis patients: a large study from a single center in China. Ren Fail. 2019;41(1):800–7.
Tsimikas S, Clopton P, Brilakis ES, et al. Relationship of oxidized phospholipids on apolipoprotein B-100 particles to race/ethnicity, apolipoprotein(a) isoform size, and cardiovascular risk factors: results from the Dallas Heart Study. Circulation. 2009;119(13):1711–9.
Deo RC, Wilson JG, Xing C, et al. Single-nucleotide polymorphisms in LPA explain most of the ancestry-specific variation in lp(a) levels in African americans. PLoS ONE. 2011;6(1):e14581.
Li Y, Luke MM, Shiffman D, Devlin JJ. Genetic variants in the apolipoprotein(a) gene and coronary heart disease. Circ Cardiovasc Genet. 2011;4(5):565–73.
Daugirdas JT. Second generation logarithmic estimates of single-pool variable volume Kt/V: an analysis of error. J Am Soc Nephrol. 1993;4(5):1205–13.
Hopewell JC, Haynes R, Baigent C. The role of lipoprotein (a) in chronic kidney disease. J Lipid Res. 2018;59(4):577–85.
Li Q, Chen Y, Yu L, et al. The relationship between lipoprotein(a) and cardiovascular events in acute coronary syndrome patients with and without chronic kidney disease. Atherosclerosis. 2022;349:204–10.
Erqou S, Kaptoge S, Perry PL, et al. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302(4):412–23.
Anderson TJ, Grégoire J, Pearson GJ, et al. 2016 Canadian Cardiovascular Society Guidelines for the management of Dyslipidemia for the Prevention of Cardiovascular Disease in the adult. Can J Cardiol. 2016;32(11):1263–82.
[Chinese guidelines for lipid management. (2023)]. Zhonghua Xin Xue Guan Bing Za Zhi. 2023. 51(3): 221–255.
Patel AP, Wang M, Pirruccello JP. Lp(a) (Lipoprotein[a]) concentrations and Incident Atherosclerotic Cardiovascular Disease: New insights from a large National Biobank. Arterioscler Thromb Vasc Biol. 2021;41(1):465–74.
Hirano T, Furukawa S, Kurokawa M, Ebara T, Dixon JL, Nagano S. Intracellular apoprotein B degradation is suppressed by decreased albumin concentration in Hep G2 cells. Kidney Int. 1995;47(2):421–31.
Chakraborty B, Vishnoi G, Goswami B, Gowda SH, Chowdhury D, Agarwal S. Lipoprotein(a), ferritin, and albumin in acute phase reaction predicts severity and mortality of acute ischemic stroke in north Indian patients. J Stroke Cerebrovasc Dis. 2013;22(7):e159–67.
Yeang C, Witztum JL, Tsimikas S. LDL-C’ = LDL-C + lp(a)-C: implications of achieved ultra-low LDL-C levels in the proprotein convertase subtilisin/kexin type 9 era of potent LDL-C lowering. Curr Opin Lipidol. 2015;26(3):169–78.
Villard EF, Thedrez A, Blankenstein J, et al. PCSK9 modulates the Secretion but not the Cellular Uptake of Lipoprotein(a) Ex vivo: an Effect blunted by Alirocumab. JACC Basic Transl Sci. 2016;1(6):419–27.
Pirillo A, Catapano AL. Statins increase Lp(a) plasma level: is this clinically relevant. Eur Heart J. 2020;41(24):2285–7.
Maranhão RC, Carvalho PO, Strunz CC, Pileggi F. Lipoprotein (a): structure, pathophysiology and clinical implications. Arq Bras Cardiol. 2014;103(1):76–84.
Bartens W, Rader DJ, Talley G, Brewer HB Jr. Decreased plasma levels of lipoprotein(a) in patients with hypertriglyceridemia. Atherosclerosis. 1994;108(2):149–7.
Dangas G, Mehran R, Harpel PC, et al. Lipoprotein(a) and inflammation in human coronary atheroma: association with the severity of clinical presentation. J Am Coll Cardiol. 1998;32(7):2035–42.
Sotiriou SN, Orlova VV, Al-Fakhri N, et al. Lipoprotein(a) in atherosclerotic plaques recruits inflammatory cells through interaction with Mac-1 integrin. FASEB J. 2006;20(3):559–61.
Bouchareb R, Mahmut A, Nsaibia MJ, et al. Autotaxin Derived from Lipoprotein(a) and valve interstitial cells promotes inflammation and mineralization of the aortic valve. Circulation. 2015;132(8):677–90.
Ueda N, Takasawa K. Impact of inflammation on Ferritin, Hepcidin and the management of Iron Deficiency Anemia in chronic kidney disease. Nutrients. 2018. 10(9).
Koda Y, Nishi S, Suzuki M, Hirasawa Y. Lipoprotein(a) is a predictor for cardiovascular mortality of hemodialysis patients. Kidney Int Suppl. 1999;71:S251–3.
Tonelli M, Karumanchi SA, Thadhani R. Epidemiology and mechanisms of Uremia-related Cardiovascular Disease. Circulation. 2016;133(5):518–36.
Hahr AJ, Molitch ME. Management of diabetes Mellitus in patients with CKD: Core Curriculum 2022. Am J Kidney Dis. 2022;79(5):728–36.
Peev V, Nayer A, Contreras G. Dyslipidemia, malnutrition, inflammation, cardiovascular disease and mortality in chronic kidney disease. Curr Opin Lipidol. 2014;25(1):54–60.
Pecoits-Filho R, Lindholm B, Stenvinkel P. The malnutrition, inflammation, and atherosclerosis (MIA) syndrome -- the heart of the matter. Nephrol Dial Transpl. 2002;17(Suppl 11):28–31.
Yang WS, Min WK, Park JS. Effect of increasing serum albumin on serum lipoprotein(a) concentration in patients receiving CAPD. Am J Kidney Disease. 1997;30(4):507–13.
Nordestgaard BG, Chapman MJ, Ray K, et al. Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J. 2010;31(23):2844–53.
Gudbjartsson DF, Thorgeirsson G, Sulem P, et al. Lipoprotein(a) concentration and risks of Cardiovascular Disease and Diabetes. J Am Coll Cardiol. 2019;74(24):2982–94.
Acknowledgements
Not applicable.
Funding
This present study was supported by Beijing Municipal Natural Science Foundation (grant number 7212021).
Author information
Authors and Affiliations
Contributions
Guojuan Zhang was responsible for the study conception and design and critically reviewed the final manuscript. Qiaojing Liang and Liping Jiang was responsible for data acquisition, analysis, interpretation of data, initial drafting and revising the manuscript. All the authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is in conformity with the Helsinki and Istanbul declarations and its amendments. The study was approved by the Ethics Committee of Beijing Tongren Hospital. The ethics approval number for this study is TREC2024-KY110. Before starting the study, all participants signed informed consent forms, wherein they were informed that the research would entail collecting their medical information without including any personal details. The medical data obtained from participants was exclusively used for research purposes and was securely stored to maintain confidentiality and prevent any unauthorized disclosure.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liang, Q., Zhang, G. & Jiang, L. Association between lipoprotein (a) and risk of atherosclerotic cardiovascular disease events among maintenance hemodialysis patients in Beijing, China: a single-center, retrospective study. BMC Nephrol 25, 250 (2024). https://doi.org/10.1186/s12882-024-03690-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-024-03690-z