
Abstract
Background
Prevalence and risk factors for Chlamydia trachomatis infection among young men in Switzerland is still unknown. The objective of the present study was to assess prevalence and risk factors for C. trachomatis infection in young Swiss men.
Methods
517 young Swiss men were enrolled in this cross-sectional study during their compulsory military recruitment. Participants completed a questionnaire and gave urine samples which were screened for C. trachomatis DNA by PCR. Genotyping of positive samples was done by amplification and sequencing the ompA gene.
Results
The prevalence of chlamydial infection among young Swiss male was 1.2% (95% confidence interval [95%CI], 0.4–2.5%). C. trachomatis infection was only identified among the 306 men having multiple sexual partner. Although frequent, neither unprotected sex (absence of condom use), nor alcohol and drug abuse were associated with chlamydial infection. Men living in cities were more frequently infected (2.9%, 95%CI 0.8–7.4%) than men living in rural areas (0.5%, 95%CI 0.1–1.9%, p = 0.046). Moreover, naturalised Swiss citizens were more often positive (4.9%, 95%CI 1.3–12.5%) than native-born Swiss men (0.5%, 95%CI 0.1–1.7%, p = 0.003).
Conclusion
In comparison with other countries, the prevalence of chlamydial infection in men is extremely low in Switzerland, despite a significant prevalence of risky sexual behaviour. C. trachomatis infection was especially prevalent in men with multiple sexual partners. Further research is required (i) to define which subgroup of the general population should be routinely screened, and (ii) to test whether such a targeted screening strategy will be effective to reduce the prevalence of chlamydial infection among this population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Chlamydia trachomatis infection is the commonest sexually transmitted bacterial disease in European countries [1, 2] and in the United States [3, 4]. Although the major impact of disease is on the female genital tract [1, 2], men may suffer from urethritis, prostatitis, infertility and Reiter's syndrome [1].
The most frequent risk factors associated with chlamydial infection are related to sexual behaviour, i.e. early age of first intercourse, multiple partners, and inconsistent condom use [1]. Since most infections caused by C. trachomatis are asymptomatic, the establishment of screening programs, as already done in some developed countries, is necessary to control the disease [5].
The studies carried out in Europe on C. trachomatis infection among young males have shown high rates ranging from 7.8–13.3%[1, 6–11]. Similar prevalence were observed in other developed (3.7–5.3% [4, 12–14]) and developing countries (3.1–7.9% [15, 16]).
However, no data are available from Switzerland. The present cross-sectional study is intended to determine the prevalence of and risk factors for C. trachomatis infection among young healthy Swiss males.
Methods
In this study approved by the ethical committee of the University of Lausanne (n° 177/06), we included all 18–26 years-old Swiss men who presented for their medical entry examination at the Army Recruitment Centre of Lausanne, Switzerland during winter 2006–2007 and who gave written consent for urinary C. trachomatis screening. The volunteers completed a questionnaire on sociodemographic, sexual and behavioral risk factors. Our questionnaire was adapted from questionnaires used in previous published studies measuring sexually transmitted infections [6, 12, 17–19]. Completion of the questionnaire was accurately done, since answers to similar and complementary questions formulated in different ways were 97% and 95% congruent for demographic questions and for questions on their sexual activities, respectively. DNA was extracted from centrifuged first-void urine and analyzed by real-time Taqman PCR, as described [20]. This PCR exhibited an excellent analytical sensitivity of 1 copy per reaction, good intrarun and interrun reliability, and a specificity of 100% when considering Cobas Amplicor as gold standard [20]. Positive samples were then genotyped using ompA sequencing [21]. Statistical analyses were performed using STATA (College-Station, USA). Confidence Intervals were calculated using the Daly method [22].
Results
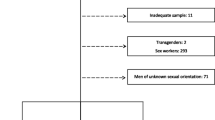
Among 521 eligible men, four did not complete the questionnaire and were excluded. The sociodemographic characteristics of the 517 remaining volunteers are shown in Table 1. The mean age was 20.6 years (standard deviation ± 1.4 years). A total of 87% of the participants reported being sexually-experienced and 59.9% of the participants reported having more than two sexual partners in their life span. The consistent use of condoms for all sexual relations was reported by 32.3% of the 517 volunteers. Among those with more than 4 partners (n = 178), 21.3% regularly used condoms. While 67.9% of the study participants drank alcohol at least every week-end, 3.5% drank alcohol every day. Almost half (47.6%) of the participants were cigarette smokers, and 28.1% of them smoke more than 20 cigarettes per day. Occasional or daily cannabis consumption was reported by 27.1% and 7.8% of the participants, respectively. Ecstasy, heroin or cocaine have been taken by 6.4% of the studied population.
The prevalence of chlamydial infection was 1.2% (95%CI 0.4–2.5%) among all 517 volunteers and of 1.3% (95%CI 0.3–2.4%) among the 450 sexually-experienced men. No participants without or with only a single lifetime sexual partner were diagnosed with chlamydial infection. Conversely, 1.9% (95%CI 0.7–4.2%) of those with multiple sexual partners were C. trachomatis positive. Two men who tested positive for Chlamydia reported having consistently used condoms during all sexual relations. Among the 9 men who reported having had a male sexual partner, none had a positive Chlamydia test. When considering only Swiss born men, the prevalence was 0.5% (95%CI 0.2–2.1%). Conversely, among foreign born naturalized men who originated from Europe, the prevalence was 2.4% (95CI 0.1–13.3%). For those originated from foreign countries outside Europe, a prevalence of 7.5% (95%CI 1.5–21.9%) was observed. Young men living in cities more than 10'000 inhabitants and/or earning more than 2000 SFrs (1600 US$) were at increased risk of C. trachomatis infection (Table 1). Alcohol, cigarette, cannabis and illegal drug consumption were frequently recorded, but were not associated with chlamydial infection. Chlamydial serotypes were E (n = 3), J, Ia and D (n = 1 each).
Discussion
Our cross-sectional study provides, for the first time, prevalence data of C. trachomatis infection in young Swiss men. In Switzerland, previous studies mainly focused on women and evaluated highly selected study populations [23]. A 2.8% prevalence was recorded among asymptomatic sexually active Swiss women in 1998 [23]. However, studied women were mainly from urban area, where the prevalence is higher. Moreover, age of first sexual intercourse is lower for women or occur with older partner [24], likely also contributing to increased prevalence in women. C. trachomatis is a reportable disease in Switzerland. Since 1999, there has been a significant increase (64%) in the number of official reports of C. trachomatis infection in Switzerland [25, 26]. However, among the 517 asymptomatic young Swiss men we investigated, the prevalence was only 1.2%. This Chlamydia prevalence is much lower than that reported for young asymptomatic males in Norway (7.8%)[6], Scotland (9.8%) [8] and the entire UK (13.3%) [1]. In USA, prevalence is also higher than that found in Switzerland, ranging from 3.7% [4] to 5.3% [13].
Multiple partners and inconsistent condom use are recognised as important predictors of C. trachomatis infection [1, 6, 16]. However, screening on the basis of condom use would have missed a substantial number of infections in the population we studied, since two of six infected men reported having always used condoms. The effect or no effect of condom use as a preventive mesure should ideally be confirmed in a larger cohort. In our study, variables associated with C. trachomatis infection were "multiple sexual partners", "living in a large city" and "foreign born, naturalized". The higher prevalence observed in the latter subgroup, similar to that of other European and non-European countries, demonstrate that the overall low prevalence of 1.2% we observed was not due to a low sensitivity of the PCR, but rather reflects a true local difference in prevalence. Serotype E was more prevalent in Switzerland, as it is the case in other European countries [21, 27].
Conclusion
This is the first study of the prevalence of C. trachomatis infection conducted in young Swiss males. Since military service is compulsory for all Swiss men, the study population we screened corresponds to an unselected and unbiased representative sample of young healthy Swiss men. Despite a prevalence of sexual risk behaviour which is similar to that recorded in other countries [24], C. trachomatis prevalence in Swiss males is extremely low. In the future, in order to identify populations with a high prevalence that may benefit from mass screening, it will be important to more precisely identify risks factors associated with chlamydial infection.
References
Manavi K: A review on infection with Chlamydia trachomatis. Best Pract Res Clin Obstet Gynaecol. 2006, 20: 941-951. 10.1016/j.bpobgyn.2006.06.003.
Fenton KA, Lowndes CM: Recent trends in the epidemiology of sexually transmitted infections in the European Union. Sex Transm Infect. 2004, 80: 255-263. 10.1136/sti.2004.009415.
Schillinger JA, Dunne EF, Chapin JB, Ellen JM, Gaydos CA, Willard NJ, Kent CK, Marrazzo JM, Klausner JD, Rietmeijer CA, Markowitz LE: Prevalence of Chlamydia trachomatis infection among men screened in 4 U.S. cities. Sex Transm Dis. 2005, 32: 74-77. 10.1097/01.olq.0000149670.11953.ca.
Miller WC, Ford CA, Morris M, Handcock MS, Schmitz JL, Hobbs MM, Cohen MS, Harris KM, Udry JR: Prevalence of chlamydial and gonococcal infections among young adults in the United States. JAMA. 2004, 291: 2229-2236. 10.1001/jama.291.18.2229.
Low N: Screening programmes for chlamydial infection: when will we ever learn?. BMJ. 2007, 334: 725-728. 10.1136/bmj.39154.378079.BE.
Bakken IJ, Skjeldestad FE, Halvorsen TF, Thomassen T, Storvold G, Nordbo SA: Chlamydia trachomatis among young Norwegian men: sexual behavior and genitourinary symptoms. Sex Transm Dis. 2007, 34: 245-249. 10.1097/01.olq.0000233737.48630.03.
Wagenlehner FM, Weidner W, Naber KG: Chlamydial infections in urology. World J Urol. 2006, 24: 4-12. 10.1007/s00345-005-0047-x.
McKay L, Clery H, Carrick-Anderson K, Hollis S, Scott G: Genital Chlamydia trachomatis infection in a subgroup of young men in the UK. Lancet. 2003, 361: 1792-10.1016/S0140-6736(03)13398-3.
Lamontagne DS, Fenton KA, Randall S, Anderson S, Carter P: Establishing the National Chlamydia Screening Programme in England: results from the first full year of screening. Sex Transm Infect. 2004, 80: 335-341. 10.1136/sti.2004.012856.
Kang M, Rochford A, Johnston V, Jackson J, Freedman E, Brown K, Mindel A: Prevalence of Chlamydia trachomatis infection among 'high risk' young people in New South Wales. Sex Health. 2006, 3: 253-254. 10.1071/SH06025.
van der Snoek EM, Gotz HM, Mulder PG, Verkooyen RP, van der Meijden WI: Prevalence of STD and HIV infections among attenders of the Erasmus MC STD clinic, Rotterdam, The Netherlands, during the years 1996 to 2000. Int J STD AIDS. 2003, 14: 119-124. 10.1258/095646203321156890.
Arcari CM, Gaydos JC, Howell MR, McKee KT, Gaydos CA: Feasibility and short-term impact of linked education and urine screening interventions for Chlamydia and gonorrhea in male army recruits. Sex Transm Dis. 2004, 31: 443-447. 10.1097/01.OLQ.0000129950.91427.34.
Cecil JA, Howell MR, Tawes JJ, Gaydos JC, McKee KT, Quinn TC, Gaydos CA: Features of Chlamydia trachomatis and Neisseria gonorrhoeae infection in male Army recruits. J Infect Dis. 2001, 184: 1216-1219. 10.1086/323662.
Scholes D, Heidrich FE, Yarbro P, Lindenbaum JE, Marrazzo JM: Population-Based Outreach for Chlamydia Screening in Men: Results from a Randomized Trial. Sex Transm Dis. 2007
Buve A, Weiss HA, Laga M, Van DE, Musonda R, Zekeng L, Kahindo M, Anagonou S, Morison L, Robinson NJ, Hayes RJ: The epidemiology of gonorrhoea, chlamydial infection and syphilis in four African cities. AIDS. 2001, 15 Suppl 4: S79-S88. 10.1097/00002030-200108004-00009.
Fioravante FC, Costa Alves MF, Guimaraes EM, Turchi MD, Freitas HA, Domingos LT: Prevalence of Chlamydia trachomatis in asymptomatic Brazilian military conscripts. Sex Transm Dis. 2005, 32: 165-169. 10.1097/01.olq.0000152897.44969.02.
Jennings JM, Luo RF, Lloyd LV, Gaydos C, Ellen JM, Rietmeijer CA: Age-bridging among young, urban, heterosexual males with asymptomatic Chlamydia trachomatis. Sex Transm Infect. 2006
Marrazzo JM, Ellen JM, Kent C, Gaydos C, Chapin J, Dunne EF, Rietmeijer CA: Acceptability of urine-based screening for Chlamydia trachomatis to asymptomatic young men and their providers. Sex Transm Dis. 2007, 34: 147-153. 10.1097/01.olq.0000230438.12636.eb.
Fenton KA, Korovessis C, Johnson AM, McCadden A, McManus S, Wellings K, Mercer CH, Carder C, Copas AJ, Nanchahal K, Macdowall W, Ridgway G, Field J, Erens B: Sexual behaviour in Britain: reported sexually transmitted infections and prevalent genital Chlamydia trachomatis infection. Lancet. 2001, 358: 1851-1854. 10.1016/S0140-6736(01)06886-6.
Jaton K, Bille J, Greub G: A novel real-time PCR to detect Chlamydia trachomatis in first-void urine or genital swabs. J Med Microbiol. 2006, 55: 1667-1674. 10.1099/jmm.0.46675-0.
Lysen M, Osterlund A, Rubin CJ, Persson T, Persson I, Herrmann B: Characterization of ompA genotypes by sequence analysis of DNA from all detected cases of Chlamydia trachomatis infections during 1 year of contact tracing in a Swedish County. J Clin Microbiol. 2004, 42: 1641-1647. 10.1128/JCM.42.4.1641-1647.2004.
Daly L: Simple SAS macros for the calculation of exact binomial and Poisson confidence limits. Comput Biol Med. 1992, 22: 351-361. 10.1016/0010-4825(92)90023-G.
Paget WJ, Zbinden R, Ritzler E, Zwahlen M, Lengeler C, Sturchler D, Matter HC: National laboratory reports of Chlamydia trachomatis seriously underestimate the frequency of genital chlamydial infections among women in Switzerland. Sex Transm Dis. 2002, 29: 715-720. 10.1097/00007435-200211000-00016.
Wellings K, Collumbien M, Slaymaker E, Singh S, Hodges Z, Patel D, Bajos N: Sexual behaviour in context: a global perspective. Lancet. 2006, 368: 1706-1728. 10.1016/S0140-6736(06)69479-8.
Abraham S, Toutous-Trellu L, Pechere M, Hugonnet S, Liassine N, Yerly S, Rohner P, Ninet B, Hirschel B, Piguet V: Increased incidence of sexually transmitted infections in Geneva, Switzerland. Dermatology. 2006, 212: 41-46. 10.1159/000089021.
Lautenschlager S: Sexually transmitted infections in Switzerland: return of the classics. Dermatology. 2005, 210: 134-142. 10.1159/000082569.
Jonsdottir K, Kristjansson M, Hjaltalin OJ, Steingrimsson O: The molecular epidemiology of genital Chlamydia trachomatis in the greater Reykjavik area, Iceland. Sex Transm Dis. 2003, 30: 249-256. 10.1097/00007435-200303000-00015.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/8/45/prepub
Acknowledgements
We thank all employees from the Recruitment Centre of the Swiss Army who were involved in this study. We particularly thank Cordula Equey and Manuela Bersier for help for sampling, André Baud for computer assistance, and Ana Palma for technical assistance. We also thank Philip E. Tarr and Anthony Staines (reviewer) for their critical review of the manuscript. Gilbert Greub is supported by the Leenards Foundation through a "Bourse Leenards pour la relève académique en médecine clinique à Lausanne".
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
DB and GG initiated and designed the study, interpreted the results. DB, CB and GG performed the statistical analyses. DB and JPK were responsible for patient recruitment, clinical assessment, data management and blood sampling. KJ and GG did the laboratory analyses. The paper was written by DB and GG, and reviewed by all other contributors.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Baud, D., Jaton, K., Bertelli, C. et al. Low prevalence of Chlamydia trachomatisinfection in asymptomatic young Swiss men. BMC Infect Dis 8, 45 (2008). https://doi.org/10.1186/1471-2334-8-45
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2334-8-45