
Abstract
To investigate the psychophysiological mechanisms of attentional processes in 34 schizophrenic patients and 50 healthy volunteers, we conducted the analysis of the data from the immediate memory task (IMT) version of continuous performance test (CPT), the N100 and P300 auditory event-related potentials (ERPs), and their relationship. The sequence of five-digit numbers was presented on a computer screen during 10 min (500 ms presentation, 500 ms inter-stimulus interval). Participants were told to press the key when the current number coincided with the previous one. Evoked potentials were obtained in the two-stimulus oddball paradigm by averaging the target stimuli. IMT performance was significantly worse in schizophrenic patients compared to healthy participants: elevated percent of error responses, reduced sensory sensitivity (A') values, and increased reaction time variability were observed along with altered characteristics of ERP, such as lower amplitudes of N100 and P300, and P300 elevated latency. Most of significant correlations (p < 0.01) between IMT and ERP in the control group were related to N100 peak. In the patient group, all correlations were related to the P300 component: decreased amplitude and elevated latency were associated with poorer CPT results. The revealed differences in the profiles of correlations may result from abnormal psychophysiological mechanisms involved in the sustained attention in schizophrenia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In recent years, there have been a plethora of studies aimed at revealing neurobiological mechanisms of cognitive disorders in schizophrenia which demonstrate a role of genetic determinants, can be detected in the prodromal phase, and are characterized by progression and therapy resistance [1, 2].
Disorders of attention are viewed as a central component of cognitive deficit in schizophrenia and comprise such aspects as sustained and selective attention deficits, with no regard for the modality of external stimuli [3–5].
Continuous performance task (CPT) is one of the most commonly used tests for sustained attention, or maintaining vigilance towards external stimuli over time. Schizophrenia patients demonstrate much poorer CPT results, including patients in early stages of the disease [6–10]. Besides, healthy relatives of the patients do worse in CPT as well [11–13], which points to an important role of genetic determinants in the disturbances.
Various versions of CPT have been developed; they differ in the modality and characteristics of stimuli, frequency of their presentation, probability of the target stimuli, working memory load, and stimulation duration (usually varies between 6 and 22 min) [6, 14].
The immediate memory task (IMT) is a modified complex version of CPT-IP (identical pairs) test for sustained attention [15, 16]. Five-digit numbers presented on the monitor screen are used as stimuli in IMT. Participants are instructed to press the key when the current number coincides with the previous one. This test allows the evaluation of sustained attention, working memory, and central inhibitory processes; it proved efficient in studying both normal and clinical populations [15–17]. Currently, attention deficit revealed by CPT, including CPT-IP, is included in the list of schizophrenia neurocognitive endophenotypes [7, 18], and thus is viewed as genetic marker of the disease.
Despite the urgency of the problem, the neurophysiological mechanisms underlying sustained attention, particularly in schizophrenia, are not well understood. It is obvious that low level of CPT performance in schizophrenia patients may result from involving dysfunctional neural networks in the task [19, 20].
Event-related potentials (ERPs) are widely used to study neurophysiological correlates of attention and information processing. The oddball paradigm is commonly used to record ERPs. Two-stimulus oddball paradigm is suitable for simple version of CPT where target and non-target stimuli alternate with a probability of 20 and 80%, respectively [6]. An ERP induced by the target stimulus includes several components which reflect the functional activity of the brain at successive, functionally determined phases of information processing [21–23]. The amplitude and latency of the N100 and P300 components of auditory ERPs allow the quantification of the activation level of the brain neural networks, as well as of the timing parameters of basic cognitive processes associated with recording, sensory discrimination, detection of the target stimuli, working memory, and decision making.
ERP recording immediately upon CPT allows the evaluation of the brain activity associated with completing the test [19, 24, 25]. However, simultaneous recording of EEG imposes substantial restrictions on the complexity of the task, primarily on the duration of the stimuli and the frequency of stimulation demanding the increase of inter-stimulus intervals (up to 2 s and more) which, nonetheless, are important parameters in evaluating sustained attention.
In the present study, in order to estimate sustained attention deficits in schizophrenia, we examined the interrelation between the IMT results and ERPs recorded in a single session in the oddball paradigm. IMT has not been analyzed in schizophrenia patients before. The aim of this study was comparative analysis between groups of healthy people and schizophrenia patients: (1) IMT and oddball test performance, (2) N100 and P300 ERP characteristics, and (3) relationship between IMT measures and the brain functional activity in terms of the N100 and P300 parameters.
METHODS
The study was conducted on 50 healthy subjects and 34 schizophrenia patients (ICD-10, code F20; duration of the disease, 1–20 years). All subjects were right-handed men aged 22 to 40 years. The average age of healthy subjects was 27.0 ± 0.5 years; of schizophrenia patients – 28.6 ± 0.9 years. The patients had not received psychotropic medications for seven days prior to the experiment.
The experimental scheme included: (1) continuous performance test, and (2) recording of event-related potentials while performing oddball task. The interval between sessions (1) and (2) was 30–40 min.
CPT–IMT continuous performance test. Stimuli were produced on the PC monitor. The test consisted of a sequence of 5-digit numbers displayed in black on the white monitor screen (Fig. 1). Each digit was 2.8 × 4.3 cm in size. Numbers were generated in pseudorandom order, each number was produced for 500 ms with inter-stimulus interval of 500 ms.

Example of stimulus sequence in CPT-IMP test. (a) Catch stimulus, differs from the previous stimulus by one digit; (b) target stimulus, identical to the previous stimulus. Stimulus presentation, 500 ms; inter-stimulus interval, 500 ms.
Three types of stimuli were used in the test:
(1) Target stimuli, five-digit number identical to the previous one. Pressing the key in response to the target stimulus was counted as a correct answer (hit).
(2) Catch stimuli, number differing from the previous one by one randomly chosen digit. Response to such stimuli was counted as false alarm; increased number of such responses was viewed as a sign of impulsiveness [15, 16].
(3) Simple stimuli (fillers), random five-digit numbers with all digits different from the previous stimulus.
Before the study, the subjects completed a short training session.
The main stage of the study consisted of two experimental sets 300 stimuli in each, 5 min long. The interval between sets was about 30 s.
The probability of target and catch stimulus appearance in each set was 33%, whereas filler stimulus was produced in 34% of cases.
The evaluation of results included calculating the percentage of missed target stimuli (MT), false alarms in response to catch stimuli (FA_C) and false alarms in response to filler stimuli (FA_F), as well as reaction time (ms) of hits (RT) and its variability (as a standard deviation, ms). Along with this, integral indices of sensory sensitivity (А') and sensory strategy (B ") were calculated.
Sensory sensitivity index (А') reveals the subject’s ability to detect target stimuli against non-target. This value is based on the subject’s sensitivity to the stimulus which includes perception and attention aspects. The value varies from 0 to 1. Higher values of А' are correlated with better ability to differentiate between target and non-target stimuli. А' is calculated as follows [15]:
where Hits is the response to target stimuli; False Alarm is the response to non-target stimuli; pHits is the ratio of the number of hits to the total number of stimuli (hit probability); pFalse Alarms is the ratio of the number of non-target responses to the total number of stimuli (false alarm probability).
The B " indicator reflects the test strategy aspect that appears in the decision-making process. The liberal strategy is characterized by a large number of responses to non-target stimuli (false alarms) in an attempt to respond to a greater number of target stimuli, whereas the conservative strategy is characterized by a tendency to miss target stimuli in an attempt to avoid error responses to non-target stimuli and thus increasing the number of missed target stimuli. B " value varies from –1 to 1. Negative B " value points to liberal strategy, positive—to conservative strategy. The calculation formula for B " sensory strategy indicator [15]:
Event-related potentials. Recording of auditory ERPs was conducted in a semi-dark shielded room, the subjects were seated in chairs with eyes closed.
The STIM2 stimulator was used for stimulation (Compumedics Neuroscan, USA). The binaural presentation of auditory stimuli (75 dB, 50 ms) via headphones was performed in accordance with standard 2‑stimulus oddball paradigm. The probability of target stimulus presentation (2000 Hz) was 20%, whereas 80% of the stimuli were non-target (1000 Hz); total number of stimuli amounted to 360. The interval between stimuli was 1800 to 2200 ms.
The subject was instructed to press the key as fast as possible in response to the target stimulus. Training session was conducted prior to the experiment.
The oddball test performance was evaluated based on the number of errors (in %) including missed targets and delayed responses (latency over 600 ms). The reaction time (RT2) of hits and its variability were also detected.
EEG was recorded using a Neuroscan Synamps System electroencephalograph (Compumedics, United States) from 19 channels (the 10–20 System) with reference electrodes on the earlobes. Low-frequency (70 Hz) and high-frequency (1 Hz) filters were used, the sampling frequency was at 1000 Hz.
ERPs were obtained using a specialized Scan 4.5 software block. After selection of artifact-free runs, we conducted averaging triggered at the moment of target stimulus presentation. The recording was segmented into analysis epochs of 1000 ms (200 ms before the target stimulus and 800 ms after the target stimulus) which were subjected to low-frequency filtration (with cut-off frequency of 16 Hz for the N100 component and 8.5 Hz for the P300 component) prior to averaging. Overall number of target stimuli included in averaging was about 30 runs.
The N100 component was defined as a peak negative deviation in the range of 60 to 140 ms after stimulus presentation, the P300 component, as a peak positive deviation in the range of 250 to 400 ms after stimulus presentation. Average potential value in the pre-stimulus interval (200 ms) was used as the baseline.
In the analysis of the N100 component, the data from frontal (Fz, F3, F4) and central (Cz, C3, C4) channels where N100 is the most stable were included. P300 was analyzed in nine channels, including parietal channels (P3, P4, Pz).
Statistical analysis of the dependent variables was conducted by means of SPSS 11.5 software using standard pattern including ANOVA and analysis of means.
Correlation analysis between CPT and oddball test results with ERPs was conducted using the nonparametric Spearman method. When correction for correlation multiplicity (overall correlation number for each subject was 330) was introduced [26], the analysis included correlations with significance level p < 0.01.
RESULTS
IMT results. Comparing CPT results in the studied groups revealed significant decrease in the test performance in schizophrenia patients compared to healthy subjects (Table 1). In schizophrenia patients, the number of missed target stimuli (p < 0.001) and false alarms in response to simple stimulus (p < 0.01) was much higher; at the same time, the number of false alarms in response to catch stimulus was similar to control group. The patient group also demonstrated pronounced increase in the variability of reaction time (RT1) in response to target stimuli (p < 0.001) compared to controls, whereas RT1 values were similar.
The analysis of integral indices revealed a decrease in sensory sensitivity (A ', p < 0.001) and an increase in sensory strategy (B ", p < 0.001) values in the patient group pointing to a more conservative test strategy.
Oddball test results. Oddball test performance in the patient group was also lower compared to controls: the total number errors per target stimulus demonstrated statistically significant increase (р < 0.01). At the same time, the number of missed target stimuli in the studied groups was similar, whereas the percent of delayed responses (hits with RT2 > 600 ms) in the patient group exceeded controls by a factor of more than seven (p < 0.001) (Table 2). In addition, the patient group exhibited an increased reaction time in response to target stimuli (RT2, p < 0.01) and its variability (p < 0.001) (Table 2).
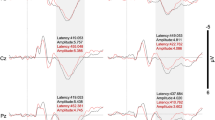
Characteristics of event-related potentials. Comparison of the N100 potential component revealed a significant decrease in the amplitude in the schizophrenia patient group compared to controls (“Group”: F(1,62) = 5.35, p = 0.024) (Fig. 2a). The latency of N100 in the patient group was shorter compared to controls, the “Group” factor significance was at tendency level (F(1,62) = 3.81, p = 0.055) (Fig. 2a). However, if only frontal channels were included in the analysis the “Group” effect was statistically significant (F(1,62) = 5.73, p = 0.020).

Characteristics of (a) N100 and (b) P300 ERPs in healthy subjects (a, solid line) and schizophrenia patients (b, dotted line). Vertical axis: at the top, amplitude (µV) (for N100 absolute values of amplitude are presented); at the bottom, latency (ms). Horizontal axis, EEG channels. Level of significance: P300, mean differences for all cases, p < 0.01; N100, * p < 0.05, ** p < 0.01. Variation is shown as the error of the mean.
P300 analysis in schizophrenia patients revealed a pronounced decrease in the amplitude (“Group”: F(1,66) = 24.32, p < 0.001) and increase in latency (“Group”: F(1,66) = 17.14, p < 0.001) (Fig. 2b).
Correlations between IMT parameters and ERPs. In healthy subjects, most correlations between IMT results was revealed for N100 component amplitude, the absolute value of which was negatively correlated with the number of missed targets, as well as with sensory strategy value, and positively correlated with sensory sensitivity (Table 3). False alarms in response to simple stimuli showed negative correlation with the latency period of N100 (n = 2) at the central channels (C3, C4) (Table 3).
In the case of P300, significant positive correlations have been revealed between the number of false alarms in response to catch stimulus and P300 latency at 8 out of 9 channels included in the analysis (Table 3).
In schizophrenia patients no statistically significant correlations between IMT results and N100 component parameters have been revealed, however, a substantial number (n = 24) of statistically significant correlations have been shown for P300 wave (Table 4). The number of missed targets and sensory sensitivity value showed a negative correlation with P300 amplitude and positive correlation with P300 latency. The variability of reaction time (RT1) demonstrated a negative correlation with P300 amplitude. No regional specificity was shown for correlations.
Correlations between oddball test parameters and ERPs. In healthy subjects, no statistically significant correlations between behavioral measures of oddball test and ERPs have been found.
In the patient group, statistically significant correlations between oddball test performance, as well as for IMT task, have only been shown for P300 test (n = 19). The number of delayed responses correlated negatively with P300 amplitude and positively with P300 latency. The RT2 variability, in contrast, correlated negatively with P300 amplitude and positively with P300 latency (Table 4).
DISCUSSION
Thus, our comparative analysis of attention function in healthy subjects and schizophrenia patients based on IMT results revealed a significant decrease in the performance quality in the patient group. It was particularly evident from the increase in the number of missed target stimuli and false alarms in response to filler stimuli (FA_F), whereas the number of false alarms in response to catch stimuli (FA_C) was close to controls. Missed targets and FA_Fs reflect sustained attention deficit in time, i.e., vigilance, whereas FA_Cs indicate increased impulsiveness [6, 9, 15, 16, 19]. Significant differences from controls have also been revealed in the patient group in integral indices A ' and B ': decrease of sensory sensitivity A ', i.e., the ability to identify target stimuli, and increase of B " index pointing to a more conservative test strategy. It should be noted that hit RT in schizophrenia patients did not differ from controls while its variability was significantly increased. This increase in RT variability in CPT is in accord with other studies and is viewed, along with missed targets, as fluctuations in the level of brain activity which cause sustained attention deficit [14, 15, 19].
The oddball test performance were also poorer in the patient group compared to controls: the percentage of delayed responses (RT over 600 ms) was much higher, hit RT was longer, as well as its variability. According to the literature, increase in RT together with increase in inter-stimulus intervals (as in the case of oddball test in this study) reflects the tendency for lower level of vigilance [14].
Thus, the analysis of IMT and oddball test performance showed sustained attention deficit, decreased ability to identify significant stimuli, and fluctuations in the level of vigilance in the patient group.
The analysis of the N100 and P300 ERP components revealed pronounced decrease in the amplitude of N100 and P300, along with increased P300 latency in schizophrenia patients. Deviations in the N100 and P300 components in schizophrenia have been widely mentioned [27–32] and point to disruptions in the functional activity of the brain systems involved in providing sustained attention. The P300 and N100 decreased amplitudes are included in the list of schizophrenia neurophysiological endophenotypes [29–32].
We have also found that schizophrenia patients are characterized by decreased N100 latency, which was more pronounced in frontal channels. According to Strelets et al., decreased ERP latency below normative values may indicate deficits in some stages of information processing [33].
In order to understand neurophysiological mechanisms involved in the continuous performance test and their deficits in schizophrenia better, the analysis of relationship between IMT performance and ERPs has been conducted. Various patterns of correlations in healthy subjects and patients have been revealed.
In healthy subjects, correlations with the N100 component prevailed. Higher absolute values of N100 amplitude showed correlation with better test results: decreased number of missed targets and sensory sensitivity increase. Earlier, in a combined sample of healthy subjects and schizophrenia patients, an association was demonstrated between decreased N100 amplitude and poorer attention test results, including CPT [34].
Lower N100 latency values displayed correlation with increased number of false alarms in response to filler stimuli, which proves the suggested association between lower N100 latency values and information processing deficits.
Thus, all indicators demonstrating association with N100 parameters, mainly reflect maintaining the adequate level of vigilance. These correlations can be explained by the fact that N100 reflects early stages of the attention responsible for distributing attention, analyzing stimulus specificities, and associated with non-specific arousal in the brain [35–37].
The increased P300 latency in controls correlated with a higher number of false alarms in response to catch stimuli; i.e., it was associated with misidentification of the stimulus and poor decision-making. P300 latency is known to reflect the speed of central processes [22] and therefore its increase in the case of fast stimuli presentation, such as in IMT, is critical. In addition, correlation between P300 latency and vigilance has been shown for healthy subjects [38].
In the patient group, no significant correlations between IMT results and N100 were found. Correlations with P300 have been found for the measures related to sustained attention indices. Increased number of missed targets and decrease in sensory sensitivity were associated with decreased amplitude and longer P300 latency, whereas the increased RT variability was only associated with decreased amplitude.
The analysis of correlations between oddball test performance and ERPs did not reveal statistically significant correlations in the healthy group, which may be attributed to the simplicity of the test for healthy people. However, in the patient group a substantial number of correlations with P300 was found, with an increased percentage of delayed responses and RT2 variability associated with a decreased amplitude and an increased latency of P300.
Thus, according to the analysis, poorer IMT and oddball test performance of schizophrenia patients are closely related to the abnormalities in the P300 characteristics.
The analysis of correlation patterns between IMT performance and ERPs in controls and patients did not reveal any similar associations, which points to differences in the central mechanisms providing sustained attention. Lack of correlations between test performance and N100 component in the patient group seems to be the most important. This means that in healthy subjects sustained attention is connected with the activity of neuronal networks involved in generating N100, whereas in the patient group it is the activity of neuronal networks involved in generating P300.
N100 is generated in the distributed neuronal network of the cortex that includes regions of the temporal, prefrontal, and motor cortex [39]. Studies aimed at identifying the localization of N100 generators (using LORETA analysis) revealed sources in the temporal cortex (the primary and secondary associative auditory cortex) and anterior cingulate gyrus [40–42]. However, the comparison between healthy subjects and schizophrenia patients did not show differences in the activity of temporal generators, whereas the activity of generators in the cingulate gyrus was substantially decreased in the patient group.
Data on the involvement of the cingulate gyrus and some other regions of the PFC in the generation of N100 [39, 40] suggest that sensory cortex areas are modulated by the PFC, which miscrostructural and functional abnormalities are considered as the key factor of cognitive deficit in schizophrenia [4]. In the PET study of the brain activity during CPT performance decreased activity of PFC has also been shown in schizophrenia patients compared to healthy subjects [43].
Our results are in accord with the data of inherent to schizophrenia deficit at the early stages of auditory and visual information processing, which do not include conscious control and are associated with sensory overload, working memory disturbances, conceptual disorganization, and with a risk of psychotic states [29, 44]. This relates to the deficit in auditory ERP P50 suppression and prepulse inhibition of acoustic startle reaction (most pronounced when the interval between pre-stimulus and startle stimulus is 60 ms) [29, 45], and to an increased thresholds of test stimulus recognition in backward masking [46, 47].
ERP recording during the tasks related to attention attraction showed that schizophrenia patients, in contrast to healthy subjects, exhibited no modulation of N100 parameters depending on the level of complexity and context of the task [39, 48]. The analysis of ERPs recorded in P50 suppression paradigm (presentation of paired stimuli with inter-stimulus interval of 500 ms) has demonstrated a substantial decrease in the level of inhibition of both the P50 and N100 components in response to the second stimulus in the pair in the patient group [34]. These data also show the deficit in the early stages of information processing in schizophrenia and are in accord with the results of the present study.
CONCLUSIONS
Different correlation patterns obtained in groups of healthy subjects and schizophrenia patients, apparently, result from disturbed psychophysiological mechanisms providing sustained attention in schizophrenia. The conducted analysis revealed two main factors of sustained attention deficit in schizophrenia: (1) deficit in the involvement of neuronal networks providing the early stages of information processing caused by abnormalities in the central processes related to N100 generation; (2) a decrease in the functional state of neuronal networks involved in P300 generation revealed as pronounced decrease of amplitude and latency prolongation.
REFERENCES
Ivanov, M.V. and Neznanov, N.G., Negativnye i kognitivnye rasstroistva pri endogennykh psikhozakh: diagnostika, klinika, terapiya (Negative and Cognitive Disorders in Endogenous Psychoses: Diagnostics, Clinics, and Therapy), St. Petersburg: Evropeiskii Dom, 2008.
Liddle, P.F., Schizophrenic syndromes, cognitive performance and neurological dysfunction, Psychol. Med., 1987, vol. 17, no. 1, p. 49.
Seidman, L.J., van Manen, K.J., Turner, W.M., et al., The effects of increasing resource demand on vigilance performance in adults with schizophrenia or developmental attentional/learning disorders: a preliminary study, Schizophr. Res., 1998, vol. 34, nos. 1–2, p. 101.
Eisenberg, D.P. and Berman, K.F., Executive function, neural circuitry, and genetic mechanisms in schizophrenia, Neuropsychopharmacology, 2010, vol. 35, no. 1, p. 258.
Tan, H.Y., Callicott, J.H., and Weinberger, D.R., Prefrontal cognitive systems in schizophrenia: towards human genetic brain mechanisms, Cognit. Neuropsychiatry, 2009, vol. 14, no. 4, p. 277.
Cornblatt, B.A. and Keilp, J.G., Impaired attention, genetics, and pathophysiology of schizophrenia, Schizophr. Bull., 1994, vol. 20, no. 1, p. 31.
Cornblatt, B.A. and Malhotra, A.K., Impaired attention as an endophenotype for molecular genetic studies of schizophrenia, Am. J. Med. Genet., 2001, vol. 105, no. 1, p. 11.
Cremasco, L. and Cappa, S.F., Attentional dysfunction of chronic schizophrenia: no association with long-term institutionalization, Psychiatry Clin. Neurosci., 2002, vol. 56, no. 4, p. 419.
Suwa, H., Matsushima, E., Ohta, K., and Mori, K., Attention disorders in schizophrenia, Psychiatry Clin. Neurosci., 2004, vol. 58, no. 3, p. 249.
Hilti, C.C., Delko, T., Orosz, A.T., et al., Sustained attention and planning deficits but intact attentional set-shifting in neuroleptic-naïve first-episode schizophrenia patients, Neuropsychobiology, 2010, vol. 61, no. 2, p. 79.
Laurent, A., Biloa-Tang, M., Bougerol, T., et al., Executive/attentional performance and measures of schizotypy in patients with schizophrenia and in their nonpsychotic first-degree relatives, Schizophr. Res., 2000, vol. 46, nos. 2–3, p. 269.
Finkelstein, J.R., Cannon, T.D., Gur, R.E., et al., Attentional dysfunctions in neuroleptic-naive and neuroleptic-withdrawn schizophrenic patients and their siblings, J. Abnorm. Psychol., 1997, vol. 106, no. 2, p. 203.
Chen, W.J., Chang, C.H., Liu, S.K., et al., Sustained attention deficits in nonpsychotic relatives of schizophrenic patients: a recurrence risk ratio analysis, Biol. Psychiatry, 2004, vol. 55, no. 10, p. 995.
Egeland, J. and Kovalik-Gran, I., Measuring several aspects of attention in one test: the factor structure of Conners’s continuous performance test, J. Atten. Disord., 2010, vol. 13, no. 4, p. 339.
Dougherty, D.M., Marsh, D.M., Moeller, F.G., et al., Effects of moderate and high doses of alcohol on attention, impulsivity, discriminability, and response bias in immediate and delayed memory task performance, Alcohol Clin. Exp. Res., 2000, vol. 24, no. 11, p. 1702.
Dougherty, D.M., Marsh, D.M., and Mathias, C.W., Immediate and delayed memory tasks: a computerized behavioral measure of memory, attention, and impulsivity, Behav. Res. Methods Instrum. Comput., 2002, vol. 34, no. 3, p. 391.
Lijffijt, M., Lane, S.D., Meier, S.L., et al., P50, N100, and P200 sensory gating: relationships with behavioral inhibition, attention, and working memory, Psychophysiology, 2009, vol. 46, no. 5, p. 1059.
Nuechterlein, K.H., Green, M.F., Calkins, M., et al., Attention/vigilance in schizophrenia: performance results from a large multi-site study of the Consortium on the Genetics of Schizophrenia (COGS), Schizophr. Res., 2015, vol. 163, no. 1, p. 38.
Riccio, C.A, Reynolds, C.R., Lowe, P., and Moore, J.J., The continuous performance test: a window on the neural substrates for attention? Arch. Clin. Neuropsychol., 2002, vol. 17, no. 3, p. 235.
Tana, M.G., Montin, E., Cerutti, S., and Bianchi, A.M., Exploring cortical attentional system by using fMRI during a Continuous Perfomance Test, Comput. Intell. Neurosci., 2010, vol. 2010, art. ID 329213.
Ivanitskii, A.M., Strelets, V.B., and Korsakov, I.A., Informativnye protsessy mozga i psikhicheskaya deyatel’nost’ (Information Processes in Brain and Psychical Activity), Moscow: Nauka, 1984.
Polich, J., Updating P300: an integrative theory of P3a and P3b, Clin. Neurophysiol., 2007, vol. 118, no. 10, p. 2128.
Rissling, A.J. and Light, G.A., Neurophysiological measures of sensory recording, stimulus discrimination, and selection in schizophrenia patients, in Behavioral Neurobiology of Schizophrenia and Its Treatment, Curr. Topics Behav. Neurosci. vol. 4, Swerdlow, N.R., Ed., New York: Springer-Verlag, 2010, p. 284.
Behzadnia, A., Ghassimi, F., Chermahini, S.A., et al., The neural correlation of sustained attention in performing conjunctive continuous performance task: an event-related potential study, Neuroreport, 2018, vol. 1, no. 1, p. 1.
Verbaten, M.N., Overtoom, C.C., Koelega, H.S., et al., Methylphenidate influences on both early and late ERP waves of ADHD children in a continuous performance test, J. Abnorm. Child Psychol., 1994, vol. 22, no. 5, p. 561.
Zaykin, D.V., Zhivotovsky, L.A., Westfall, P.H., and Weir, B.S., Truncated product method for combining p-values, Genet. Epidemiol., 2002, vol. 22, no. 2, p. 170.
Ford, J.M., Schizophrenia: the broken P300 and beyond, Psychophysiology, 1999, vol. 36, no. 6, p. 667.
Jeon, Y.W. and Polich, J., Meta-analysis of P300 and schizophrenia: patients, paradigms, and practical implications, Psychophysiology, 2003, vol. 40, no. 5, p. 684.
Turetsky, B.I., Calkins, M.E., Light, G.A., et al., Neurophysiological endophenotypes of schizophrenia: the viability of selected candidate measures, Schizophr. Bull., 2007, vol. 33, no. 1, p. 69.
Turetsky, B.I., Greenwood, T.A., Olincy, A., et al., Abnormal auditory N100 amplitude: a heritable endophenotype in first-degree relatives of schizophrenia probands, Biol. Psychiatry, 2008, vol. 64, no. 12, p. 1051.
Luck, S.J., Mathalon, D.H., and O’Donnell, B.F., A roadmap for the development and validation of event-related potential biomarkers in schizophrenia research, Biol. Psychiatry, 2011, vol. 70, no. 1, p. 28.
Lebedeva, I.S., Kaleda, V.G., and Abramova, L.I., Neurophysiological abnormalities in the P300 paradigm as endophenotypes of schizophrenia, Zh. Nevropatol. Psikhiatr. im. S.S. Korsakova, 2009, no. 1, p. 61.
Strelets, V.B., Garakh, Zh.V., Mar’ina, I.V., et al., Temporal characteristics of the initial stage of verbal information processing in normal conditions and in schizophrenia, Zh. Vyssh. Nervn. Deyat. im. I.P. Pavlova, 2012, vol. 62, no. 2, p. 165.
Smith, K.A., Edgar, C., Huang, M., et al., Cognitive abilities and 50 and 100 ms paired-click processes in schizophrenia, Am. J. Psychiatry, 2010, vol. 167, no. 10, p. 1264.
Näätänen, R. and Picton, T., The N1 wave of the human electric and magnetic response to sound: a review and analysis of component structure, Psychophysiology, 1987, vol. 24, no. 4, p. 375.
Hansen, J.C. and Hillyard, S.A., Temporal dynamics of human auditory selective attention, Psychophysiology, 1988, vol. 25, no. 3, p. 316.
Rockstroh, B., Müller, M., Wagner, M., et al., Event-related and motor responses to probes in a forewarned reaction time task in schizophrenic patients, Schizophr. Res., 1994, vol. 13, no. 1, p. 23.
Ramautar, J.R., Romeijn, N., Gomez-Herrero, G., et al., Coupling of infraslow fluctuations in autonomic and central vigilance markers: skin temperature, EEG beta power and ERP P300 latency, Int. J. Psychophysiol., 2013, vol. 89, no. 2, p. 158.
Rosburg, T., Boutros, N.N., and Ford, J.M., Reduced auditory evoked potential component N100 in schizophrenia—a critical review, Psychiatry Res., 2008, vol. 161, no. 3, p. 259.
Gallinat, J., Mulert, C., Bajbouj, M., et al., Frontal and temporal dysfunction of auditory stimulus processing in schizophrenia, NeuroImage, 2002, vol. 17, no. 1, p. 110.
Giard, M.H., Perrin, F., Echallier, J.F., et al., Dissociation of temporal and frontal components in the human auditory N1 wave: a scalp current density and dipole model analysis, Electroencephalogr. Clin. Neurophysiol., 1994, vol. 92, no. 3, p. 238.
Mulert, C., Gallinat, J., Pascual-Marqui, R., et al., Reduced event-related current density in the anterior cingulate cortex in schizophrenia, NeuroImage, 2001, vol. 13, no. 4, p. 589.
Buchsbaum, M.S., Haier, R.J., Potkin, S.G., et al., Frontostriatal disorder of cerebral metabolism in never-medicated schizophrenics, Arch. Gen. Psychiatry, 1992, vol. 49, no. 12, p. 935.
Kirenskaya, A.V., Storozheva, Z.I., Myamlin, V.V., and Tkachenko, A.A., The concept of endophenotypes in neurophysiological research of schizophrenia, Zh. Vyssh. Nervn. Deyat. im. I.P. Pavlova, 2013, vol. 63, no. 6, p. 625.
Storozheva, Z.I., Kirenskaya, A.V., Novototsky-Vlasov, V.Y., et al., Startle modification and P50 gating in schizophrenia patients and controls: Russian population, Span. J. Psychol., 2016, vol. 19, p. E8.
Zakharov, I.M., Myamlin, V.V., and Kirenskaya, A.V., Psychophysiological mechanisms of perception and attention in conditions of reverse masking in health people and with schizophrenia, Ross. Psikhiatr. Zh., 2011, no. 5, p. 37.
Myamlin, V.V., Kirenskaya, A.V., and Novototsky-Vlasov, V.Y., Use of backward masking test for the study of visual information processing in healthy subjects and schizophrenic patients, Hum. Physiol., 2016, vol. 42, no. 5, p. 492.
Iwanami, A., Isono, H., Okajima,Y., et al., Event-related potentials during a selective attention task with short interstimulus intervals in patients with schizophrenia, J. Psychiatry Neurosci., 1998, vol. 23, no. 1, p. 45.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
COMPLIANCE WITH ETHICAL STANDARDS
All experiments were conducted in accordance with the principles of biomedical ethics formulated in the 1964 Helsinki declaration and its further updates and approved by local committee on bioethical problems of V. Serbsky National Medical Research Centre for Psychiatry and Narcology (Moscow).
INFORMED CONSENT
Each participant produced a voluntary written informed consent signed by him after being explained potential risks and advantages, as well as the character of the coming study.
CONFLICT OF INTERESTS
The authors declare no obvious or potential conflicts of interests connected with publishing this article.
Additional information
Translated by A. Deryabina
Rights and permissions
About this article

Cite this article
Kirenskaya, A.V., Myamlin, V.V. & Tkachenko, A.A. Psychophysiological Study of the Mechanisms of Sustained Attention Deficit in Schizophrenia. Hum Physiol 47, 113–122 (2021). https://doi.org/10.1134/S0362119721010060
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S0362119721010060