
Abstract
Genetic variation may partly explain asthma treatment response heterogeneity. We aimed to identify common and rare genetic variants associated with asthma that was not well controlled despite inhaled corticosteroid (ICS) treatment. Data of 110 children was collected in the Children Asthma Therapy Optimal trial. Associations of genetic variation with measures of lung function (FEV1%pred), airway hyperresponsiveness (AHR) to methacholine (Mch PD20) and treatment response outcomes were analyzed using the exome chip. The 17q12-21 locus (containing ORMDL3 and GSMDB) previously associated with childhood asthma was investigated separately. Single-nucleotide polymorphisms (SNPs) in the 17q12-21 locus were found nominally associated with the outcomes. The strongest association in this region was found for rs72821893 in KRT25 with FEV1%pred (P=3.75*10−5), Mch PD20 (P=0.00095) and Mch PD20-based treatment outcome (P=0.006). No novel single SNPs or burden tests were significantly associated with the outcomes. The 17q12-21 region was associated with FEV1%pred and AHR, and additionally with ICS treatment response.
Similar content being viewed by others


Introduction
Childhood asthma is a chronic inflammatory disease of the airways, which is associated with significant morbidity.1, 2 Asthma is characterized by airway inflammation, airway hyperresponsiveness (AHR) and recurrent episodes of reversible airway obstruction.3 Despite international guidelines on asthma treatment advising inhaled corticosteroids (ICS) as treatment to provide asthma control,4 some patients still have respiratory symptoms, exacerbations and get admitted to the hospital. There is increasing evidence that, in addition to environmental factors, genetic variation may partly explain heterogeneity in asthma treatment response.5 Genome-wide association studies (GWAS) have mainly focused on (childhood) asthma susceptibility or severity6 and have identified the 17q12-21 locus, containing IKZF, GSDMB and ORMLD3, which was consistently replicated in other studies.7, 8, 9 One genome-wide study focusing on ICS treatment response has identified a single-nucleotide polymorphism (SNP) in the GLCCI1 gene to be associated with change in forced expiratory volume in 1 s (FEV1%pred) upon ICS treatment in asthma.10 Although providing cost-effective genome-wide coverage of common variation (SNPs >5%), GWAS yields little information about rare variation. To specifically investigate the role of functional variation in protein-coding genes, the exome chip was developed which contains not only the putatively functional and mostly rare (minor allele frequency (MAF) <1%) exonic variants but also includes more common SNPs selected for a specific purpose (for example, validated SNPs by GWAS,11 ancestry informative SNPs, human leukocyte antigen SNPs and so on).
In the current study we have performed a post-hoc pharmacogenomic analysis using exome-chip12 data of participants of the Children Asthma Therapy Optimal (CATO) study.13 This trial compared stepwise treatment of asthmatic children based on AHR and symptoms, or based on symptoms only.
We aimed to identify both common and rare genetic variation associated with asthma that was not well controlled despite ICS treatment, focusing on lung function and AHR as main outcomes. We investigated common genetic variation in a per-SNP approach, both genome-wide and focusing specifically on the previously mentioned 17q12-21 locus. Rare genetic variation was separately investigated in a gene-based approach.
Materials and methods
CATO study
The CATO study is a 2-year randomized clinical multicenter trial (ClinicalTrials.gov: NCT00158834) designed to compare treatment guidance of asthmatic children based on methacholine (Mch) bronchial provocation testing (provocative dose of methacholine that caused a fall in (FEV1) of 20%, Mch PD20) and asthma symptoms, or based on asthma symptoms only. The design of the study has been published previously.13 Briefly, atopic asthmatic children using ICS, who had a positive radioallergosorbent test result (⩾0.35 KU l−1) for ⩾1 airborne allergen were included based on current symptoms and/or AHR. Children were randomized to adjustment of treatment on symptom scores or to adjustment of treatment based on bronchial provocation testing and symptom scores. Participants were followed up for 2 years, with study visits every three months. During each visit the following parameters were measured: symptom-free days in the 2 weeks before each visit based on diary cards, lung function (FEV1%pred)14 and AHR (Mch PD20). AHR was tested by methacholine challenge using a dosimeter method.15 Treatment dosage was when necessary adjusted upon each study visit according to the algorithm of the symptom (reference) or the AHR/symptom (intervention) strategy. The study was approved by the medical ethical committees of all the participating centers.
Medication levels
Study medication was divided into five increasing levels (Table 1). Levels 1 and 2 consisted of ICS maintenance treatment only. In levels 3–5 a long-acting beta agonist was added to the ICS regime. All medication was administered via Diskus dry powder inhalers (GlaxoSmithKline, Brentford, UK).
Outcomes
Four outcomes were studied (specified below), two reflecting continuous measurements of phenotypes relevant to asthma, and two binary outcomes reflecting poor treatment response. As there was no significant effect of the intervention in the CATO study,13 we did not adjust for the treatment arm in these analyses.
Outcomes reflecting lung function and AHR
The measured outcomes FEV1%pred and Mch PD20 were used to find SNPs affecting these parameters during treatment which was closely monitored (for further explanation see statistical methods). These outcomes are referred to as ‘continuous outcomes’.
-
FEV1%pred expressed as a percentage of the average value for sex and height, corrected for medication level.
-
Mch PD20 as a continuous variable was log-transformed, and adjusted for age, sex and medication level.
Outcomes reflecting treatment response
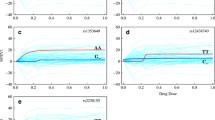
To assess treatment response, we calculated a summary statistic to describe the increase or decrease of FEV1%pred and AHR. We fitted a linear regression model for each subject and continuous outcome (FEV1%pred and log PD20), with time as the independent variable. A positive or a negative value of the regression coefficient indicates an overall increase or decrease in the outcome (Figure 1). The following outcomes are referred to as ‘treatment response outcomes’.
-
Poor treatment response based on decrease in lung function despite high levels of treatment

Progress over time of FEV1% pred, PD20 and current level of medication for three subjects during the course of the study.
Poor treatment response based on lung function was defined as a decreasing FEV1%pred during the trial. Furthermore, children were required to have an FEV1%pred<100% at baseline, while medication administered was at levels 4 or 5 for at least five out of nine visits. Children not belonging to this group were considered to be responders to treatment. This outcome is referred to as ‘Lung function-based treatment outcome’.
-
Poor treatment response based on persistent AHR (low PD20) despite high levels of treatment
Poor treatment response for AHR was defined as starting with a PD20 value lower than the median of the whole group, which decreased over time, while medication administered was at level 4 or 5 for at least five out of nine visits. Children not belonging to this group were considered to be responders to treatment. This outcome is referred to as ‘AHR-based treatment outcome’.
Genotyping
DNA, isolated from buccal swabs, was available from 143 individuals and was extracted using a salt extraction method. Genotyping was performed using the Infinium HumanExome chip (Illumina, San Diego, CA, USA), version 1.1, which contains 242 902 variants. The chip is designed to focus on nonsynonymous variation, but also features SNPs found associated to various phenotypes in previous GWAS, human leukocyte antigen tagging SNPs, ancestry informative markers and so on. Genotype calling was done using zCall16 to facilitate calling of rare SNPs.
Quality control
The genetic data set was filtered to include only SNPs with genotyping call rates ⩾95%, which were nonmonomorphic (MAF>0%), and had a Hardy–Weinberg Equilibrium P-value>1 × 10−6. Samples were filtered to include those with a call rate ⩾95%, which were of European ancestry, verified using EIGENSTRAT.17 Identity-by-descent estimates from PLINK were used to identify siblings or otherwise related children (pi-hat >0.2), one of which was randomly excluded.
Common SNP analysis
Using a cutoff of MAF⩾1%, 36 519 SNPs were selected for the common SNP analysis. The continuous outcomes FEV1%pred and the log-transformed Mch PD20 were measured longitudinally. A linear mixed model approach was used to incorporate all data available in the trial, taking into account the correlated data within individuals. The results thus show the effect a SNP has on the outcome, adjusting for the fact that it has this effect at every time point.
Using the nlme R package,18 a mixed model was fitted with age, sex (both only for AHR), and current level of medication as covariates. The random part of the model consisted of random slopes (allowing for systematic effects in the data) and random intercepts. Significance of each SNP was assessed using a likelihood ratio test comparing the model with and the model without the SNP.
Common SNP analyses for treatment response (a binary outcome) were performed using PLINK19 for logistic regression analysis,19 grouping children with a poor treatment response as ‘cases’, and the rest of the group as ‘controls’, adjusting for age and sex.
P-values were Bonferroni corrected for 36 519 tests to adjust for multiple testing, giving a cutoff value of 1.4 × 10−6 for the common SNP analyses.
Rare SNP analyses
We used rare variant burden testing to group rare variants per gene, as these are unsuitable for single SNP testing. Gene and exon locations were based on RefSeq, including all nonsynonymous, splice and stop variants with a MAF<1%. 24 944 SNPs were available for the rare SNP analyses in 10 157 genes, which resulted in a Bonferroni corrected P-value threshold of 4.9 × 10−6. Calculations were performed using R version 2.15.2 (ref 20) and the nlme package for the continuous outcomes FEV1%pred and Mch PD20. For these outcomes a T1 test was used, summing the number of variant alleles in a gene for each participant. This number is then used as the independent variable in the linear mixed model analysis.
For the treatment response outcomes two tests were used in SCORE-SEQ version 5.2:21 a simple sum of variants in a gene for each participant (T1 test) and the Sequence Kernel Association Test (SKAT).22 SKAT allow for different directions of effect, possibly giving more power to detect effects.
Analysis of the 17q12-21 locus
We selected the whole 17q12-21 locus that is known to be associated with childhood-onset asthma6, 8 and asthma treatment response,23 to specifically investigate variants previously found to be associated with asthma, lung function and AHR. We compared the frequency of the rs7216389 T-allele (the strongest previous association with asthma in this region) in the study population to the frequency in the Dutch population (samples of 500 parents from the GoNL project [23]) using a Χ2-test.
For the association analyses the locus was defined as the region starting 100 kb upstream of the first SNP found associated with asthma in GWAS (rs907092 in GSDMB, base pair (BP) 37922259) and ending 100 kb downstream of the last SNP found associated with asthma (rs758632, upstream of KRT25, BP 38892689), the region of interest thus ranging from BP 37822259 to BP 38992689 on chromosome 17. All BP locations are based on NCBI build 37. This region contained 47 SNPs with a MAF⩾1% on the genotyping array used. When adjusting for multiple testing with a Bonferroni correction, this results in a significance threshold of 0.001.
Results
Baseline statistics
Hundred and ten children with European ancestry (80%) were included in the analyses, with age ranging from 6 to 16 years; 66 of which were boys (Table 2). During the trial, the mean FEV1%pred remained stable, while the geometric mean PD20 rose from 88.7 to 333 μg. Fifteen out of 110 subjects were classified as nonresponders based on lung function, and 10 out of 110 subjects were nonresponders when considering AHR. There was little overlap between the two nonresponder phenotypes, three subjects being nonresponders for both outcomes. Nonresponders were on average a bit younger, and received more medication. Airway hyperresponsiveness decreased (higher Mch PD20) on average, and increased for AHR nonresponders. Lung function did not change for the whole group, both nonresponder groups showed decreasing lung function over time.
Genetic data quality control
After quality control, 64 581 variants were retained for analysis. 24 944 SNPs had a MAF < 1% and were included in the rare SNP analyses, leaving 39 637 SNPs for the common SNP analysis.
Lung function and AHR
Common SNPs
Using FEV1%pred as the outcome and the mixed model approach to account for the correlated measured within individuals, we did not find chip-wide significant statistically results (Supplementary Figure S1). Lead SNPs from the loci with P<1 × 10−4 are shown in Table 3.
Using AHR as the outcome, the most significant finding was rs921561 at P=8.26 × 10−6. Rs10484568 in the human leukocyte antigen region was associated with nominal statistical significance with both the FEV1%pred outcome (at P=7.28 × 10−5) and the AHR outcome (P=9.30 × 10−5).
Rare SNPs (burden tests)
Using the T1 burden test with 10 157 genes, we found three genes associated at P<1 × 10−4 (LAG3, ANK3 and NPBWR2; Table 4). LAG3 and ANK3 were associated with both FEV1%pred and PD20.
17q21
The frequency of the T-allele of rs7216389, the SNP in the 17q21 region with the strongest association in earlier research, and incurring a higher risk for asthma,6 was higher (61 vs 50%, P=0.00165) in the CATO population compared to a representative sample of the Dutch population (GoNL24).
Several common SNPs in the 17q12-21 region were found to be nominally statistically significantly associated with the outcomes of this study when investigating the 17q12-21 region. For the FEV1%pred outcome (Supplementary Table S1), the most significant SNP was rs72821893 in the KRT25 gene (P=3.97 × 10−5), ranked third in the chip-wide analysis of common SNPs. One SNP reached nominal significance for PD20 Mch (Supplementary Table S2), rs72821893 (P=0.000954), which is the same SNP as the most significant SNP for the FEV1%pred outcome.
Treatment response phenotypes
Common SNPs
Neither for treatment response based on FEV1%pred, nor when based on AHR as the outcome, we found chip-wide significant results (Manhattan and QQ-plots in Supplementary Material). The five most significant loci for both outcomes are shown in Table 5.
Rare SNPs (burden tests)
Using the T1 and SKAT burden tests, we tested 10 157 genes on their association with treatment response. The most significant result for the burden tests of treatment response was the DOCK2 gene, with a P-value of 7.10 × 10−4 for the T1 test and 2.62 × 10−4 for the SKAT test (Table 6).
For the treatment response based on AHR, the gene GAB1 was ranked in the top 5 of both types of test (P=4.12 × 10−4 for T1 and P=4.12 × 10−4 for SKAT, Table 6).
17q21
Several SNPs in the 17q12-21 locus were found to be associated at P<0.05 to FEV1%pred-based treatment response (Supplementary Table S3), such as rs907092 (P=0.0275) and rs9303277 (P=0.0271). The risk allele of the lead SNP at this locus found in GWAS, rs7216389, is found at an allele frequency of 50% in a Dutch reference population,24 at 61% in the CATO participants and 73% in the group not responding to treatment based on FEV1%pred (P=0.0551 in the association analysis).
For the ARH-based treatment outcome (Supplementary Table S4), the same SNP found associated to the continuous outcomes FEV1%pred and PD20 MCh, rs72821893, was found as the strongest association in this region (P=0.00593).
Discussion
In an analysis of 36 519 common SNPs, no SNP was statistically significantly associated with lung function or AHR during ICS treatment. Several other findings seem relevant since analyses of the different phenotypes in this study pointed in the same direction. Our results show that in an asthmatic population treated with ICS, enriched for SNPs associated with asthma, these same SNPs may affect lung function and AHR. When investigating the 17q12-21 locus we found an enrichment of the risk allele of the lead SNP previously found in GWAS,8 rs7216389, in our population when compared with the general Dutch population. Furthermore, several SNPs in this locus were nominally associated with FEV1%pred, including SNPs previously associated with asthma susceptibility. The SNP in this locus with the strongest associations, rs72821893 (in the keratin 25 (KRT25) gene), was associated with a reduction in FEV1%pred by 20.8 percentage points per T-allele (95%CI −30.4; −11.3, P=3.75 × 10−5). Rs72821893 lowered PD20 Mch by 2.00 μg per T-allele (95% confidence interval −3.16; −0.830, P=0.001), agreeing in direction with the effect found for FEV1%pred. This same SNP was found to be associated with AHR treatment response. A sevenfold risk increase for being a poor responder was found per T-allele (odds ratio 7.73, 95% confidence interval 1.31; 45.5; P: 0.00593). The effect sizes found are very large compared to results from most GWAS, for example, an odds ratio larger than seven is very rare in these studies. Since the SNP is relatively rare (MAF in this study 4%), and not often directly genotyped, it is possible that it is partly responsible for the associations of the 17q12-21 region as a whole and was not picked up in earlier genome-wide studies. There is considerable discussion on which gene(s) in this locus are responsible for the associations with asthma, and our result suggests another gene than the often quoted GSDMA, GSDMB and ORMDL3. KRT25 is a keratin gene, an important protein in epithelial cells, but this family of proteins was not previously associated with asthma or pulmonary function. While rs72821893 is a nonsynonymous SNP, further investigation is necessary to explain this association. It has to be added that the three phenotypes associated with this SNP are correlated, and an agreement between the separate results was therefore anticipated.
The common SNP analysis for both treatment response outcomes showed no statistically significant results. However the first-ranking SNP, rs12748961 (close to SLC45A3) which was previously described in relation with the number of peripheral blood basophils (components of allergic inflammation),25 is 2 kb away from a SNP associated with lung function decline in asthma (rs16856186, r2 with rs12748961=0.002).26
The burden tests for treatment response did not reveal statistically significant associations. DOCK2 was found in the top-20 of both the T1 and SKAT test of FEV1%pred-based treatment response, as was BACH2. The fact that we did not find rare variants with a large effect size might suggest that their importance for complex diseases such as asthma is small.
The greatest strength of our study is the longitudinal nature of the data, with follow-up for 2 years, and measurements of several clinically relevant phenotypes in a standardized way. Using a mixed model, we made optimal use of this data. In addition the cohort was well characterized, and treatment was standardized. With these features this study is a unique albeit small resource for asthma related investigations. The main weakness of our study is the low number of participants. This results in low power to find associations, although this is partially compensated by the longitudinal data. Our replication of associations at the 17q12-21 locus shows that a relatively low number of participants may be useful in (pharmaco)genetic research, if detailed phenotype data are available. The assessment of treatment responses in children with asthma is complex and response phenotypes are often simplified and do not take into account fluctuations of symptoms over time.27 We were able to assess phenotypes over a longer time period, diminishing the impact of fluctuating phenotypes and measurement errors.
In conclusion, we used the exome chip to find SNPs associated with lung function and AHR, and their treatment response based on the improvement of both variables during ICS treatment. We could not identify rare SNPs with major effects on these asthma phenotypes. We did show that the main asthma risk allele from GWAS8 (in the 17q12-21 locus) was more frequent in our population than in unaffected Dutch controls. This locus is associated with FEV1%pred, AHR to methacholine and AHR-based treatment response, with rs72821893 in KRT25 as the most significant result for all three outcomes. Our study suggests that the 17q12-21 locus affects both asthma and treatment response to ICS in asthma.
References
O’Byrne PM, Pedersen S, Schatz M, Thoren A, Ekholm E, Carlsson L-G et al. The poorly explored impact of uncontrolled asthma. Chest 2013; 143: 511–523.
Bahadori K, Doyle-Waters MM, Marra C, Lynd L, Alasaly K, Swiston J et al. Economic burden of asthma: a systematic review. BMC Pulm Med 2009; 9: 24.
Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J 2008; 31: 143–178.
Brannan JD . Bronchial hyperresponsiveness in the assessment of asthma control: Airway hyperresponsiveness in asthma: Its measurement and clinical significance. Chest 2010; 138: 11S–17S.
Tse SM, Tantisira K, Weiss ST . The pharmacogenetics and pharmacogenomics of asthma therapy. Pharmacogenomics J 2011; 11: 383–392.
Moffatt MF, Kabesch M, Liang L, Dixon AL, Strachan D, Heath S et al. Genetic variants regulating ORMDL3 expression contribute to the risk of childhood asthma. Nature 2007; 448: 470–473.
Wan YI, Shrine NRG, Soler Artigas M, Wain LV, Blakey JD, Moffatt MF et al. Genome-wide association study to identify genetic determinants of severe asthma. Thorax 2012; 67: 762–768.
Moffatt MF, Gut IG, Demenais F, Strachan DP, Bouzigon E, Heath S et al. A large-scale, consortium-based genomewide association study of asthma. N Engl J Med 2010; 363: 1211–1221.
Torgerson DG, Ampleford EJ, Chiu GY, Gauderman WJ, Gignoux CR, Graves PE et al. Meta-analysis of genome-wide association studies of asthma in ethnically diverse North American populations. Nat Genet 2011; 43: 887–892.
Tantisira KG, Lasky-Su J, Harada M, Murphy A, Litonjua AA, Himes BE et al. Genomewide association between GLCCI1 and response to glucocorticoid therapy in asthma. N Engl J Med 2011; 365: 1173–1183.
Hindorff L, MacArthur J, Morales J, Junkins H, Hall P, Klemm A et al A Catalog of Published Genome-Wide Association Studies www.genome.gov/gwastudies.
Exome chip design http://genome.sph.umich.edu/wiki/Exome_Chip_Design.
Nuijsink M, Hop WCJ, Sterk PJ, Duiverman EJ, de Jongste JC . Long-term asthma treatment guided by airway hyperresponsiveness in children: a randomised controlled trial. Eur Respir J 2007; 30: 457–466.
Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC . Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J Suppl 1993; 16: 5–40.
Birnie D, Thoe Schwartzenberg GW, Hop WC, van Essen-Zandvliet EE, Kerrebijn KF . Does the outcome of the tidal breathing and dosimeter methods of assessing bronchial responsiveness in children with asthma depend on age? Thorax 1990; 45: 199–202.
Goldstein JI, Crenshaw A, Carey J, Grant GB, Maguire J, Fromer M et al. zCall: a rare variant caller for array-based genotyping: genetics and population analysis. Bioinformatics 2012; 28: 2543–2545.
Price AL, Patterson NJ, Plenge RM, Weinblatt ME, Shadick NA, Reich D . Principal components analysis corrects for stratification in genome-wide association studies. Nature 2006; 38: 904–909.
Pinheiro J, Bates D, DebRoy S, Sarkar D, R Core Team. nlme: Linear and Nonlinear Mixed Effects Models 2012.
Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MAR, Bender D et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet 2007; 81: 559–575.
R Development Core Team R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing: Vienna, Austria, 2012.
Tang Z-Z, Lin D-Y . MASS: meta-analysis of score statistics for sequencing studies. Bioinformatics 2013; 29: 1803–1805.
Wu MC, Lee S, Cai T, Li Y, Boehnke M, Lin X . Rare-variant association testing for sequencing data with the sequence kernel association test. Am J Hum Genet 2011; 89: 82–93.
Tavendale R, Macgregor DF, Mukhopadhyay S, Palmer CN . A polymorphism controlling ORMDL3 expression is associated with asthma that is poorly controlled by current medications. J Allergy Clin Immunol 2008; 121: 860–863.
Boomsma DI, Wijmenga C, Slagboom EP, Swertz MA, Karssen LC, Abdellaoui A et al. The Genome of the Netherlands: design, and project goals. Eur J Hum Genet 2013; 22: 221–227.
Okada Y, Hirota T, Kamatani Y, Takahashi A, Ohmiya H, Kumasaka N et al. Identification of nine novel loci associated with white blood cell subtypes in a Japanese population. PLoS Genet 2011; 7: e1002067.
Imboden M, Bouzigon E, Curjuric I, Ramasamy A, Kumar A, Hancock DB et al. Genome-wide association study of lung function decline in adults with and without asthma. J Allergy Clin Immunol 2012; 129: 1218–1228.
Reddel HK, Taylor DR, Bateman ED, Boulet L-P, Boushey HA, Busse WW et al. An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med 2009; 180: 59–99.
Acknowledgements
We acknowledge Mariska Olivier for her technical support. The CATO study has been sponsored by GlaxoSmithKline.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the The Pharmacogenomics Journal website
Supplementary information
PowerPoint slides
Rights and permissions
About this article

Cite this article
Leusink, M., Vijverberg, S., Koenderman, L. et al. Genetic variation in uncontrolled childhood asthma despite ICS treatment. Pharmacogenomics J 16, 158–163 (2016). https://doi.org/10.1038/tpj.2015.36
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/tpj.2015.36
- Springer Nature Limited
This article is cited by
-
Genetic associations of the response to inhaled corticosteroids in asthma: a systematic review
Clinical and Translational Allergy (2019)