
Abstract
Low-molecular-weight heparin (LMWH) is part of standard supportive care. We conducted a meta-analysis to investigate the efficacy and safety of LMWH in septic patients. We searched Pubmed, Embase, CKNI and Wanfang database prior to July 2015 for randomized controlled trials investigating treatment with LMWH in septic patients. We identified 11 trials involving 594 septic patients. Meta-analysis showed that LMWH significantly reduced prothrombin time (mean differences [MD] −0.88; 95% CI −1.47 to −0.29), APACHE II score (MD −2.50; 95% CI −3.55 to −1.46), and 28-day mortality (risk ratio [RR] 0.72; 95% CI 0.57–0.91) as well as increased the platelet counts (MD 18.33; 95% CI 0.73–35.93) than the usual treatment. However, LMWH did not reduce D-dimer (MD −0.34; 95% CI −0.85 to 0.18). LMWH also significantly increased the bleeding events (RR 3.82; 95% CI 1.81–8.08). LMWH appears to reduce 28-day mortality and APACHE II score among septic patients. Bleeding complications should be monitored during the LMWH treatment. As for limited data about LMWH and sepsis in the English literature, only trials published in the Chinese were included in the meta-analysis.
Similar content being viewed by others


Introduction
Sepsis is a clinical syndrome of microbial infection complicated by systemic inflammation. Sepsis remains a major public health problem. The incidence of severe sepsis is estimated up to 100 cases per 100 000 population1. Despite advances in intensive care technologies, the hospital mortality rate of severe sepsis was 48.7% in China2. Sepsis can induce coagulatory activation, which may contribute to deteriorate organ function3,4. Cross talk exists between inflammatory and coagulation system5. Therefore, targeting the hypercoagulable state should be a promising approach in the treatment of sepsis.
The survival benefits of coagulation inhibitors, recombinant human activated protein C as an adjunctive therapy for sepsis have been demonstrated6,7. However, the high cost and bleeding risk limit its application for the majority of patients. Heparin has the potential role in the treatment of sepsis because of similar anticoagulant actions8. Heparin can be divided into unfractionated and low-molecular-weight heparin(LMWH)9. Unfractionated heparin is the most commonly used anticoagulant worldwide. LMWH is an attractive alternative anticoagulant due to its superior antithrombotic efficacy and fewer reported bleeding risk10. Several studies11,12,13,14,15,16,17,18,19,20,21 have been published in the literature evaluating the effects of LMWH in sepsis. In general, findings from these studies suggested that LMWH might be useful in these septic patients. However, small sample size of each study might lack statistical power to draw definitive conclusions.
Here, we conducted a meta-analysis using the available randomized control trials (RCTs) to evaluate the efficacy and safety of LMWH treatment in septic patients.
Results
Search results and baseline characteristics
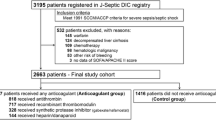
Our preliminary literature search yielded 286 potential articles, of which 260 were excluded after screening titles and abstracts. After retrieving for full-text manuscript, 15 citations were excluded for various reasons. Finally, 11 trials11,12,13,14,15,16,17,18,19,20,21 were eligible for the meta-analysis (Fig. 1). Baseline characteristics of the trials are listed in Table 1. All the trials were performed in China and published in Chinese. Eleven trials involved 594 patients with 329 in LMWH groups and 265 in the usual treatment groups. Patients in LMWH groups received two types of heparin: low-molecular weight heparin calcium and low-molecular weight heparin sodium. LMWH treatment durations were 7 and 14 days. Ten trials11,12,13,15,16,17,18,19,20,21 determined the circulating levels of prothrombin time, platelet, d-dimer, pro-inflammatory cytokines interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and clinical acute physiology and chronic health evaluationII (APACHE II) score after 7 days’ LMWH treatment, one trial14 measured above outcomes after 14 days’ treatment. The sample size ranged from 18 to 105. In general, the included trials were usually classified as low to moderate quality. The risk of bias of each trial is summarized in Fig. 2.

Diagram of trials’ selection process.

Risk of bias graph (A) and risk of bias summary (B).
Clinical outcomes
All the included trials provided the changes of APACHE II score. Treatment with LMWH significantly reduced APACHE II score (MD −2.50; 95% CI −3.55 to −1.46; I2 = 49%, P < 0.03) compared with the usual treatment group in a random effect model (Fig. 3A). Eight trials11,12,14,15,16,18,20,21 reported the 28-day mortality outcomes. Treatment with LMWH significantly reduced 28-day mortality (RR 0.72; 95% CI 0.57–0.91; I2 = 0%, P = 0.82) than the usual treatment group in a random effect model (Fig. 3B). There was no significant difference in the length of intensive care unit (ICU) stay (MD −2.26 days; 95% CI −4.74–0.23; I2 = 0%, P = 0.93) between the two groups (Fig. 2C) in three trials11,12,18.

APACHE II score (A); 28-day mortality (B); length of intensive care unit stay (C).
Changes of serum pro-inflammatory cytokines
Serum IL-6 level changes were available in three trials11,13,16. Treatment with LMWH significantly reduced serum IL-6 level (SMD −1.76; 95% CI −3.05 to −0.47; I2 = 92%, P < 0.00001) compared with the usual treatment group in a random effect model (Fig. 4A). Serum TNF-α level was reported in two trials13,16. Treatment with LMWH significantly reduced serum TNF-α level (MD −16.72; 95% CI −27.39 to −6.04; I2 = 89%, P = 0.002) compared with the usual treatment group in a random effect model (Fig. 4B).

Interleukin-6 (A); tumor necrosis factor-α (B).
Changes of anticoagulant activity
Nine trials11,12,13,14,15,16,18,19,20 provided the changes of platelet counts. Treatment with LMWH significantly increased platelet counts (MD 18.33; 95% CI 0.73–35.93; I2 = 94%, P < 0.001) than the usual treatment group in a random model (Fig. 5A). Nine trials11,12,13,14,15,16,18,19,20 provided the changes of prothrombin time. LMWH treatment significantly reduced PT (MD −0.88; 95% CI −1.47 to −0.29; I2 = 68%, P = 0.003) than the usual treatment group in a random model (Fig. 5B). Six trials12,13,15,16,17,20 reported the changes of serum D-dimer. There was no significant difference in the changes of D-dimer (MD −0.34; 95% CI −0.85 −0.18; I2 = 95%, P < 0.001) than the usual treatment group in a random model (Fig. 5C).

Platelet counts (A); prothrombin time (B); D-dimer (C).
Bleeding complications
Seven trials11,12,14,15,18,19,20 reported bleeding events. Of the total bleeding events, the frequency of tracheal intubation and deep vein puncture or injection site bleeding occurred 20 (6.07%) of 329 patient receiving LMWH, while frequency in the control group was 3 (1.13%) of 265 patients. Gastrointestinal hemorrhage occurred 14 (4.26%) of 329 patient receiving LMWH, while frequency in the control group was 2 (0.75%) of 265 patients. In addition, one case of small ecchymoses19 and gum bleeding20 was also noted. When we pooled total bleeding events from seven studies, the risk of any bleeding events was significantly increased to 3.82 (95% CI 1.81–8.08; I2 = 0%, P = 0.96) in a fixed effect model (Fig. 6).

Forest plots showing risk of total bleeding complications comparing low-molecular weight heparin to the usual treatment.
Subgroup analyses, sensitivity analyses, and publication bias
Subgroup analyses and publication bias were conducted based on changes in APACHE II score and 28-day mortality. The results of subgroup analyses were presented in Table 2.
Sensitivity analyses were performed by sequentially omitting one study at each turn. The results showed there was no change in the direction of effect sizes in APACHE II score and 28-day mortality outcomes. Evidence of publication bias for trial reporting the changes of APACHE II score was not observed by the Begg’s test (P = 0.119) and Egger’s test (P = 0.141). Potential publication bias for trial reporting 28-day mortality was observed in the Egger’s test (P = 0.041) but not in the Begg’s test (P = 0.266).
Discussion
Our meta-analysis suggests that treatment with LMWH appears to reduce 28-day mortality and APACHE II score, as well as improvement in pro-inflammatory cytokines and anticoagulant activity among septic patients. Increased any bleeding complications with LMWH administration are identified. However, these findings were concluded by the trials with methodological flaws, and recommendation of these findings should be cautioned.
Sepsis has been grouped into sepsis, severe sepsis, followed by the presence of multiorgan dysfunction, and septic shock22. Sepsis-related inflammation may activate the coagulation system, consume multiple clotting factors and resulting in disseminated intravascular coagulation (DIC)23,24. The Japanese guidelines supported the aggressive treatment of septic DIC25,26. In contrast, the guidelines of the Surviving Sepsis Campaign of the European Union and the USA did not recommend treatment for septic DIC27,28. Two previous systematic reviews and meta-analyses29,30 showed that heparin therapy may be associated with decreased mortality in patients with sepsis. However, these two studies mainly focused on the unfractioned heparin but not LMWH. Therefore, the efficacy and safety of LMWH for sepsis is not well established.
Severe sepsis is associated with higher levels of pro-inflammatory markers. The massive inflammatory activation played a key role in the development of sepsis to septic shock31. Of these proinflammatory cytokines, IL-6 and TNF-α, have got the most attention. Higher serum IL-6 or TNF-α levels indicate an increased risk of mortality32. In the current study, adjuvant treatment with LMWH reduced serum IL-6, TNF-α level to some extent which indicated LMWH had the potential to inhibit the inflammatory process. The potential anti-inflammatory property of LMWH might partly explain its beneficial mechanism.
Cytokine production contributes to the activation of platelets. Coagulation abnormalities are frequent complications of sepsis33. Manifestation coagulation abnormalities in sepsis range from a decrease in platelet counts and subclinical prolongation of prothrombin time to DIC34. The additional benefits of adjunctive use of recombinant human activated protein C in septic patients supported anticoagulation strategy in the treatment of sepsis. LMWH may exert similar beneficial effects as recombinant human activated protein C. Our study found that LMWH could increase platelet counts and reduce prothrombin time. D-dimer is a significant prognostic factor in patients with suspected infection and sepsis35. However, LMWH did not significantly change d-dimer. Therefore, anti-platelet aggregation and anticoagulant properties are another potential pharmacological mechanism.
Benefits of adjunctive use of LMWH have been demonstrated by improvement of APACHE II score. APACHE II score is a widely accepted indicator of disease severity. There was no significant difference in baseline APACHE II score. Adjunctive treatment with LMWH significantly reduced 2.5 points of APACHE II score compared with control, which suggested application of LMWH reduced the disease severity. In addition, adjunctive use LMWH was also associated with 28% lower 28-day mortality. However, there was no significant difference in length of ICU stay. Subgroup analysis indicated high dose LMWH appeared to have more benefits in improvement in APACHE II score and 28-day mortality. Despite the beneficial effect of LMWH in septic patients, a major concern is the occurrence of bleeding complications. Our pooled results indicated that LMWH administration significantly increased bleeding events 3.82 (95% CI 1.81–8.08). LMWH treatment increased both gastrointestinal hemorrhage and invasive operation bleeding events; however, these events were mild and did not need special management. Therefore, monitoring bleeding events in the use of LMWH is recommended.
Several limitations in the current analysis should be noted. First, all the included trials conducted in China and published in Chinese; evidence of publication bias reporting 28-day mortality outcome was observed in the Egger’s test (P= 0.041). Therefore, potential publication bias cannot be ruled out. Second, the methodological quality of individual trials was mainly suboptimal, particularly the sample size of individual trials was too small. Third, significant heterogeneity was noted in pooling the anticoagulant activity and pro-inflammatory cytokines. Type of LMWH, dose or intervention duration and diverse study populations, might partly contribute to the heterogeneity. Finally, all trials included only Chinese patients, the generalization of the current findings to other ethnic population should be cautioned.
In conclusion, this meta-analysis suggests that treatment with LMWH appears to reduce 28-day mortality and APACHE II score among septic patients. The beneficial effect might be related to its anti-inflammatory and anticoagulant/antiaggregant properties. Monitoring bleeding events in the use of LMWH is recommended. More well-designed studies with a larger sample size are required before definitive recommendations can be made.
Methods
Literature search
This study was performed based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) for reporting systematic reviews and meta-analyses of RCT36. We searched for relevant studies using Pubmed, Embase, Cochrane Library, VIP database, China National Knowledge Infrastructure, and Wanfang database up to July 2015. A combination of the following terms was used, including heparin OR low molecular weight heparin AND sepsis OR septic shock OR septicemia OR critically ill OR systemic inflammatory response syndrome AND randomized control trials OR RCTs. The search language was limited to publications that were written in Chinese and English. References lists from eligible studies were manually searched to identify additional trials.
Study selection
We included RCTs that used LMWH therapy in adult septic patients and reported at least prothrombin time, platelet, d-dimer, IL-6, TNF-α, APACHE II score, length of ICU stay, and 28-day mortality as outcome measures. Studies were excluded if the study designs were no RCTs or there were different regimen except for LMWH intervention between LMWH and control group. Studies were also excluded if presented a bleeding tendency because of coagulation disorders (platelet counts <30 × 109), application of anticoagulant <48h prior to enrollment or serious head injury, brain arteriovenous malformation, cerebral aneurysm.
Data extraction and methodological quality
The following items were independently extracted from each eligible studies by 2 authors (Y Fan and ML Jiang): first author name, years of publication, number and age of participant, percentage of female of participant, primary diseases distribution, and outcome measures. Any disagreements between authors were resolved through consensus. The risk of bias of each study was evaluated according to the Cochrane Handbook for Systematic Reviews of Invention37 on the basis of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome data, incomplete outcome data, and selective reporting, and others.
Statistical analysis
All statistical analyses were conducted using the RevMan version 5.1 software. Pooled estimate was presented as mean difference (MD) or standard mean difference (SMD) with 95% confidence interval (CI) for continuous outcomes and risk ratio (RR) with 95% CI for dichotomous outcomes. Comparisons were made as LMWH plus usual treatment versus usual treatment alone. Heterogeneity of the trials was assessed using the Cochrane Q test and I2 statistics38. If I2 value >50% or Cochrane Q test (P < 0.10) suggested significant heterogeneity, a random effects model was selected due to considerable heterogeneity among different trials; otherwise, a fixed-effect model was used. Potential publication bias was assessed by both the Begg’s test and Egger test. Subgroup analyses were conducted according to LMWH dose (once or twice daily) and treatment duration (7 or 14 days).
Additional Information
How to cite this article: Fan, Y. et al. Efficacy and safety of low-molecular-weight heparin in patients with sepsis: a meta-analysis of randomized controlled trials. Sci. Rep. 6, 25984; doi: 10.1038/srep25984 (2016).
References
Danai, P. & Martin, G. S. Epidemiology of sepsis: recent advances. Curr Infect Dis Rep 7, 329–34 (2005).
Cheng, B. et al. Epidemiology of severe sepsis in critically ill surgical patients in ten university hospitals in China. Crit Care Med 35, 2538–46 (2007).
Knoebl, P. Blood coagulation disorders in septic patients. Wien Med Wochenschr 160, 129–38 (2010).
Semeraro, N., Ammollo, C. T., Semeraro, F. & Colucci, M. Sepsis, thrombosis and organ dysfunction. Thromb Res 129, 290–5 (2012).
O’Brien, M. The reciprocal relationship between inflammation and coagulation. Top Companion Anim Med 27, 46–52 (2012).
Bernard, G. R. et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 344, 699–709 (2001).
Barie, P. S., Hydo, L. J., Shou, J. & Eachempati, S. R. Efficacy of therapy with recombinant human activated protein C of critically ill surgical patients with infection complicated by septic shock and multiple organ dysfunction syndrome. Surg Infect (Larchmt) 12, 443–9 (2011).
Cornet, A. D., Smit, E. G., Beishuizen, A. & Groeneveld, A. B. The role of heparin and allied compounds in the treatment of sepsis. Thromb Haemost 98, 579–86 (2007).
Gray, E. Standardisation of unfractionated and low-molecular-weight heparin. Handb Exp Pharmacol 207, 65–76, doi: 10.1007/978-3-642-23056-1_4 (2012).
Nandurkar, H. et al. Low-molecular-weight heparin biosimilars: potential implications for clinical practice. Intern Med J 44, 497–500 (2014).
Ai, Y. H. et al. Clinical study of low molecular weight heparin therapy for sepsis. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 17, 736–9 (2005).
Zhang, Z. C. et al. Clinical study of early application of low molecular weight heparin in the treatment of sepsis Shandong Medical Journal 48, 102–3 (2008).
Ren, L. B., Zhao, L. & Jiang, Z. Clinical observation of low molecular weight heparin as adjuvant treatment for 65 cases septic patients with acute kidney injury. Shandong Medical Journal 49, 81–2 (2009).
Huang, T. & Guan, Q. Clinical observation of low molecular weight heparin in the treatment of severe sepsis. Chinese Medicine Guides 7, 58–9 (2010).
Han, Y. et al. Study of changes and clinical significance of P-selcetin in low molecular weight heparin therapy for septic patients. Chi J Critl Care Med 30, 976–9 (2010).
Lin, Y. J. & Xiong, B. The efficacy of low molecular weight heparin in the treatment of sepsis: a report of 30 clinical cases. Journal of Youjiang Medical College For Nationalities 33, 3–5 (2011).
Song, H. Z., Hua, W. & Chen, Y. Z. Effect of low molecular weight heparin on prognosis of aged patients with sepsis. China Modern Medicine 19, 26–7 (2012).
Chen, P. & Qu, J. J. Therapeutic Effect of Low Molecular Weight Heparin on Sepsis. Zhejiang JITCWM 22, 336–8 (2012).
Liu, X. F. et al. Effect of low-molecular weight heparin calcium on APACHE II scores and blood coagulation function in septic patients. Chinese Journal of Gerontology 32, 3558–9 (2012).
Zhu, X. M., Shao, B. B., Zhang, W. H., Zheng, K. & Feng, H. B. Therapeutic effects of different doses administration of LMWH in patients with severe sepsis. Practical Pharmacy And Clinical Remedies 16, 1014–7 (2013).
Chen, J. et al. Effect of low molecular weight heparin in elderly patients with sepsis with myocardial injury. Prevention and Treatment of Cardio-Cerebral-Vascular Disease 13, 203–5 (2013).
Tang, C. H. et al. Non-invasive classification of severe sepsis and systemic inflammatory response syndrome using a nonlinear support vector machine: a preliminary study. Physiol Meas 31, 775–93 (2010).
Levi, M. & van der Poll, T. Inflammation and coagulation. Crit Care Med 38, S26–34 (2010).
Okamoto, K., Tamura, T. & Sawatsubashi, Y. Sepsis and disseminated intravascular coagulation. J Intensive Care 4, 23 (2016).
Oda, S. et al. The Japanese guidelines for the management of sepsis. J Intensive Care 2, 55 (2014).
Wada, H. et al. Expert consensus for the treatment of disseminated intravascular coagulation in Japan. Thromb Res 125, 6–11 (2010).
Dellinger, R. P. et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med 39, 165–228 (2013).
Dellinger, R. P. et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med 41, 580–637 (2013).
Wang, C. et al. Heparin therapy reduces 28-day mortality in adult severe sepsis patients: a systematic review and meta-analysis. Crit Care 18, 563 (2014).
Zarychanski, R. et al. The efficacy and safety of heparin in patients with sepsis: a systematic review and metaanalysis. Crit Care Med 43, 511–8 (2015).
Cinel, I. & Opal, S. M. Molecular biology of inflammation and sepsis: a primer. Crit Care Med 37, 291–304 (2009).
Hack, C. E., Aarden, L. A. & Thijs, L. G. Role of cytokines in sepsis. Adv Immunol 66, 101–95 (1997).
Fourrier, F. Severe sepsis, coagulation, and fibrinolysis: dead end or one way? Crit Care Med 40, 2704–8 (2013).
Levi, M., Schultz, M. & van der Poll, T. Sepsis and thrombosis. Semin Thromb Hemost 39, 559–66 (2013).
Rodelo, J. R. et al. D-dimer is a significant prognostic factor in patients with suspected infection and sepsis. Am J Emerg Med 30, 1991–9 (2012).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol 62, e1–34 (2009).
Higgins, J. P. T. & Green, S. Assessing risk of bias in included studies. Chapter 8, cochrane handbook for systematic reviews of interventions Version 5.1.0. Available at: www.cochrane.org/handbook/chapter-8-assessing-risk-bias-included-studies. Accessed July 8, 2014.
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. Bmj 327, 557–60 (2003).
Acknowledgements
This work was supported by Jiangsu Provincial Key&D Special Fund (BE2015666).
Author information
Authors and Affiliations
Contributions
C.Z. designed the study, performed the data analysis, and revised the manuscript; Y.F. and M.J. conducted literature research and extracted data; D.G. drafted the manuscript; All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Fan, Y., Jiang, M., Gong, D. et al. Efficacy and safety of low-molecular-weight heparin in patients with sepsis: a meta-analysis of randomized controlled trials. Sci Rep 6, 25984 (2016). https://doi.org/10.1038/srep25984
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep25984
- Springer Nature Limited
This article is cited by
-
Heparin Therapy and Mortality in Patients with Sepsis: An Observational Study Using a Marginal Structural Cox Model Based on MIMIC-IV Database
Intensive Care Research (2024)
-
Therapeutic Strategies Targeting Mitochondrial Dysfunction in Sepsis-induced Cardiomyopathy
Cardiovascular Drugs and Therapy (2024)
-
HMG-CoA reductase inhibitors and the attenuation of risk for disseminated intravascular coagulation in patients with sepsis
Journal of Thrombosis and Thrombolysis (2023)
-
Unfractionated heparin improves the clinical efficacy in adult sepsis patients: a systematic review and meta-analysis
BMC Anesthesiology (2022)
-
Recent advances in the research and management of sepsis-associated DIC
International Journal of Hematology (2021)