
Abstract
Diminished cognitive and physical functions negatively affect the daily functions of individuals. Although combined cognitive and physical training prevents instrumental activities of daily living (IADL) disability in older adults, no predictive model or mediation analysis of IADL after combined training exists. This study aims to employ prediction and mediation analysis to identify the predictors of IADL performance and to elucidate the mediators of the association between baseline global cognition and subsequent IADL performance following combined cognitive and physical training. This study involved 177 participants aged 60 years and older who underwent combined training. Cognitive function was measured with the Montreal Cognitive Assessment (MoCA), Digit Symbol Substitution Test (DSST), Color Trails Test, Word List, and a dual task; physical function with the Timed Up and Go (TUG) test; daily function with the Lawton IADL Scale. We conducted regression analyses to identify the predictors of IADL performance, and mediation analysis to examine whether DSST and TUG mediate the relationship between MoCA and IADL. The pre-intervention DSST and TUG were significant independent predictors of post-intervention IADL. The association between the pre-intervention MoCA and post-intervention IADL was mediated by pre-intervention DSST and TUG. This study highlighted the importance of measuring and improving processing speed and functional mobility before and during interventions to enhance IADL outcomes.
Trial registration: NCT03619577, 23/07/2018; NCT04689776, 29/12/2020.
Similar content being viewed by others


Introduction
Cognitive decline, such as deterioration in attention, processing speed, memory, and executive functions1,2,3 and physical decline, such as reduced muscle mass, weakness, and slowness2,4,5,6, commonly occur with increasing age. Diminished cognitive and physical functions negatively affect individuals’ abilities to perform everyday activities, such as managing finances and preparing meals (i.e., instrumental activities of daily living, IADL) and contribute to dependency in daily life, which increases the care burden and costs for families and society. Previous studies have shown that combined cognitive and physical training prevents disability in IADL and is beneficial for the ability to perform IADL in older adults7,8,9. Predictive modeling and mediation analysis of IADL performance after combined training can provide valuable information for clinical decision-making and outcome research; however, but this issue has not been widely addressed.
The ability to perform IADL is an essential cornerstone of independent living and personal autonomy. Previous studies have shown that IADL ability depends on cognitive10,11 and physical functions12,13,14. Existing evidence has shown that multi-dimensional cognitive abilities are associated with IADL in older adults15,16,17,18,19,20,21,22,23; these abilities include processing speed (the ability to process information rapidly)24, sustained attention (the ability to maintain vigilance on a particular task over an extended period)25,26, verbal memory (the ability to store and recall phonological information)27, and executive functions (a collection of top-down mental control processes, including inhibition, working memory, and cognitive flexibility)28. Similarly, global cognition, referring to a family of cognitive capacities, including orientation, attention, memory, language, and executive function29 is related to functional independence30,31,32. On the other hand, previous studies show that functional mobility, referring to the ability to independently and safely move across environments to engage in functional activities33,34, is related to IADL performance in older adults13,35,36. These studies highlight the cognitive and physical abilities concurrently in relation to the IADL performance in this population. However, existing evidence does not suggest which abilities of older adults could serve as indicators to predict IADL outcomes following combined training. Establishing predictive modeling for IADL outcomes after combined cognitive and physical training can identify the characteristics of individuals who would benefit the most, which helps clinical practitioners recruit a certain population and effectively deliver tailored interventions.
Since age-related deterioration in cognition that may impede functional independence is a primary concern, combined cognitive and physical training is intended to enhance cognition in older adults based on the guided plasticity facilitation framework37. Previous studies have demonstrated that combined training improves the global cognition of older adults38,39,40,41,42, and that global cognition and IADL performance show a strong association30,31,32. However, given global cognition as a collection of cognitive capacities, it remains unclear how global cognition may improve IADL performance following combined training. Numerous variables may play a role in the relationship between global cognition and IADL performance. Evidence suggests that in addition to global cognition, improved processing speed and functional mobility exert a positive impact on the IADL performance of older adults13,19,35,36,43,44. Processing speed is the fundamental ability to rapidly process information and lay the basis for higher-order cognitive processes24,45. Functional mobility is the ability to move across environments and quickly switch motor programs according to changes in the environment and task requirements33,46, which involves both physical and cognitive functions. The mechanism underlying the association between global cognition and IADL performance needs to be elucidated, which would be helpful in targeting specific abilities for interventions.
Developing interventions to prevent disability in IADL among older adults is crucial, and a better understanding of the factors that predict the response to combined cognitive and physical training is needed to direct interventions to those who will potentially benefit from it. Through a mediation analysis, we gain insight and acquire a deep understanding of the pathways of intervention effects, and this information helps to determine efficient and efficacious intervention strategies. We investigated whether better global cognition before combined training would result in better processing speed and functional mobility and, in turn, contribute to better IADL performance after combined training. The aims of this study were to (1) identify the characteristics of older adults who would benefit most in terms of IADL performance from combined cognitive and physical training, and (2) clarify the contribution of processing speed and functional mobility to the association between baseline global cognition and subsequent IADL performance of older adults after combined training.
Materials and methods
Participants
This study was a secondary analysis of data from two pre-post studies of combined cognitive and physical training with convenience sampling. Those who were (1) aged 60 years or over, (2) having the ability to follow instructions (a score of Mini-Mental State Evaluation ≥ 20), (3) not diagnosed with dementia by physicians, and (4) having no difficulties in basic ADLs were recruited in this study. Individuals with self-reported diagnoses of neurological disorders or unstable medical conditions were excluded.
Procedure
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of National Taiwan University (201711EM006, 201912EM016) for studies involving humans. Participants were invited from community facilities or daycare centers. All participants were screened to ensure eligibility in the study. According to the temporal order of cognitive and physical training, the combined interventions can be categorized into sequential (at a separate time) and simultaneous (at the same time) training. The participants engaged in either a sequential or simultaneous combination of cognitive and physical training. The instructors were community occupational therapists. Before conducting the interventions, all instructors were trained with the same program regarding motor-cognitive training concepts to minimize staff training weaknesses due to multisite sampling. Four researchers, who were unaware of the assigned interventions, evaluated the participants’ daily cognitive and physical functions before and after the interventions. If the participants were absent from more than 30% of the sessions, they were excluded from the study.
Intervention
In the present study, we conducted sequential and simultaneous cognitive and physical training. The doses of the two interventions were matched at 120 min per session, once a week, for 12 sessions. Each session consisted of physical and cognitive exercises. The cognitive components included attention, processing speed, short-term memory, working memory, visuospatial skills, calculation, and language; one or more cognitive components were included in every session. The physical components consisted of stretching, muscle strengthening, aerobic, and balance exercises.
Measures
For prediction analysis, the potential predictors were global cognition, processing speed, sustained attention, verbal memory, executive functions, and functional mobility, which were assessed using the Montreal Cognitive Assessment (MoCA), Digit Symbol Substitution Test (DSST), Color Trails Test (CTT), Word List (WL), a dual task that we designed, and Timed Up and Go (TUG) test, respectively. For mediation analysis, the mediator variables were processing speed and functional mobility, which were assessed using the DSST and TUG, respectively. For both prediction and mediation analyses, the outcome variable was IADL performance, which was assessed using the Lawton IADL Scale.
MoCA
The MoCA is a validated and sensitive tool for evaluating general cognition and detecting mild cognitive impairment. It is also widely recognized as a reliable measure of cognitive function47. It comprises 12 items that assess the executive functions, visuospatial abilities, language, short-term memory, attention, concentration, working memory, and orientation to time and place. The education level of the examinee was considered; one point was added to the total score if an examinee had 12 years or less of formal education. The scores on the MoCA ranged from 0 to 30, with higher scores indicating a higher function. A total score of 26 or above is considered normal and a total score of 19 to 25 indicates mild cognitive impairment29. In this study, we used a certified Chinese paper version (MoCA-T), this measurement tool has good reliability and validity48.
DSST
The DSST is designed to assess the processing speed; it is a subtest from the corpus of the Chinese version of the Wechsler Adult Intelligence Scale, Third Edition49. A participant is asked to transcribe a unique geometric symbol with its corresponding Arabic number. Initially, the participant was presented with a series of boxes containing numbers from 1 to 9 sequentially; there was a corresponding geometric symbol under each number. Subsequently, he/she is shown a series of boxes containing numbers in the top boxes and blank boxes below them, and is asked to copy the corresponding geometric symbol under each number. After the practice trial, the participant copied as many geometric symbols as possible in 120 s. The raw score was the number of correct items and was transformed into a scaled score based on the age range. It is considered to be a valid and sensitive measure of cognitive dysfunction, particularly in the working memory50.
CTT
The CTT was designed to assess sustained attention. Each participant was presented with numbered circles printed on pink and yellow backgrounds. For CTT Part 1 (CTT1), the participant was asked to connect circles numbered 1–25 in sequence using a pencil, as rapidly as possible. For CTT Part 2 (CTT2), the participant was asked to rapidly connect circles numbered 1–25 in sequence, but alternated between pink and yellow. The time taken to complete each trial, errors, near-misses, and prompts were recorded. The time was transformed into scaled time based on sex, age, and years of formal education. In this study, we used the Taiwanese Version of CTT51. This test has shown good reliability and validity in healthy adults51.
WL
WL is designed to assess the ability to recall information presented in verbal form immediately after a 30-min delay. It is a subtest from the corpus of the Chinese version of the Wechsler Memory Scale, Third Edition52. For WL Part I (WL-I), a participant is verbally presented with a 12-item list of unrelated words over a series of four trials and then is asked to recall the list immediately. For WL Part II (WL-II), 30 min after WL-I, the participants were asked to recall the 12-item list of words verbally presented earlier. The raw score of WL-I is the number of the sum of the correct responses of the four trials and that of WL-II is the number of the correct responses of one trial. Raw scores were transformed into scaled scores based on the age range.
Dual task: Box and Block Test and Serial Seven Test
We designed this dual task to assess executive functions. Each participant was instructed to simultaneously conduct the Box and Block Test and Serial Seven Test (SST) for 60 s. Each participant was seated at a table and presented with a rectangular box divided into two square compartments. One hundred and fifty colored wooden blocks were placed in each compartment. A participant is asked to move a block, one at a time, from one compartment to the other as many as he/she can for 60 s53. At the same time, a participant is asked to conduct serial subtraction by seven beginning with 300. The number of blocks moved was recorded. The difference between the correct and incorrect SST responses was calculated as the corrected number.
TUG
The TUG is a reliable and valid test designed to assess the mobility, balance (static and dynamic), and walking ability. The participants were asked to perform sequential motor tasks: stand up from a chair, walk a distance of 3 m, turn around, walk back to the chair, and sit down. Timing begins at the verbal instruction “go” and stops when a participant is seated. The score given is the time taken to complete the test, in seconds54. In this study, the score is calculated as the average time of three trials for each participant, in seconds.
Lawton IADL scale
The Lawton IADL Scale is a valid tool designed to evaluate the ability to perform tasks and detect early functional decline. The reliability and validity of the Lawton IADL scale have been established. In a semi-structured interview lasting 10 to 15 min, a participant was asked to describe in detail how IADLs were currently being performed. The IADL include eight items: using the telephone, shopping, preparing food, doing laundry, housekeeping, using transportation, handling medications, and managing finances. Each item was rated based on the level of competence, from independent in performing the activity to not performing it at all. Higher scores indicate better functioning55.
Data analysis
Descriptive statistics were used to present the demographic characteristics of participants. Paired t-tests were used to compare pre- and post-intervention differences. Pearson’s correlation analysis was used to analyze the demographic variables and pre-intervention functional measures that were potentially related to post-intervention IADL. A Pearson’s r-value of 0.35 was considered the cut-off value in this study. Regression analyses were conducted to identify significant predictors of post-intervention IADL. A mediation analysis was used to clarify the mechanism underlying the observed relationship between an independent and dependent variable that could be explained by a third variable known as a mediator variable. We conducted a parallel mediation analysis to examine whether pre-intervention MoCA influenced post-intervention IADL through mediator variables, pre-intervention DSST, or TUG. We conducted serial mediation analyses to examine the direct and indirect effects of pre-intervention MoCA on post-intervention IADL while modeling a process in which better pre-intervention MoCA caused better pre-intervention DSST, and, in turn, caused better pre-intervention TUG, and, so forth, concluding with better post-intervention IADL as the final consequence35. Mediation analyses were conducted with age, sex, group, years of formal education, and pre-intervention IADL as covariates.
Data analysis for this study was performed using SAS software, Version 9.4 of the SAS System. Mediation analyses were performed using the PROCESS functions for SAS designed by Hayes (2018). Specifically, we employed PROCESS Model 4 for the parallel mediation model and Model 6 for the serial mediation model. All mediation models were analyzed using 5000 bootstrap samples and 95% bias-corrected confidence intervals (CIs).
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of National Taiwan University (201711EM006, 201912EM016) for studies involving humans. Before conducting the study, all participants were provided with a written and oral explanation of the study protocol. After obtaining written informed consent, the participants started to participate in the study. As this article does not include the identifiable data of any participant in any form, consent for publication is not applicable.
Results
Demographic characteristics
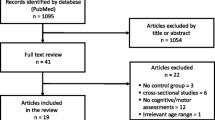
Initially, 177 participants were recruited for the study. However, participants who were absent for more than 30% of the intervention sessions were excluded from the data analysis, and twelve and seven participants in the sequential and simultaneous groups, respectively were excluded. Therefore, 158 participants completed the pre- and post-intervention measures and were included in the data analysis. The demographic characteristics and pre- and post-intervention measures are presented in Table 1. The participants showed significant improvements in the IADL, MoCA, DSST, WL-I, and WL-II scores after the intervention.
Correlation analyses
We examined the correlations between age, years of formal education, pre-intervention IADL, MoCA, DSST, WL-I, WL-II, CTT1, CTT2, dual-task, TUG, and post-intervention IADL; the results are presented in Table 2.
Univariate and multivariate regression analyses
First, we conducted univariate regression analyses to identify the potential predictors of post-intervention IADL. The results showed that age, pre-intervention IADL, MoCA, DSST, and TUG were five significant predictors (Table 3). Subsequently, we included age, pre-intervention MoCA, DSST, and TUG as predictors for multivariate regression analysis while controlling for pre-intervention IADL, sex, and group. The results showed that pre-intervention DSST and TUG significantly predicted post-intervention IADL, with an adjusted R2 of 0.514 (Table 3).
Parallel mediation analysis
We assumed that the pre-intervention DSST and TUG mediated the relationship between the pre-intervention MoCA and post-intervention IADL (Fig. 1).

Parallel mediation model. Indirect effects of pre-intervention MoCA on post-intervention IADL through pre-intervention DSST and TUG. The direct effect was insignificant depicted by dotted line. *p < 0.05, †p < 0.01, ‡p < 0.001.
The results showed that better pre-intervention global cognition was associated with higher levels of post-intervention IADL performance (β = 0.128, 95% CI [0.040, 0.216]). Better pre-intervention global cognition was associated with better pre-intervention processing speed (β = 0.302, 95% CI [0.192, 0.413]) and functional mobility (β = − 0.302, 95% CI [− 0.513, − 0.093]). The pre-intervention processing speed and functional mobility were linked to improved post-intervention IADL performance. The total indirect link between pre-intervention global cognition and post-intervention IADL performance via processing speed and functional mobility was significant (β = 0.094, 95% CI [0.029, 0.187]). The direct link between pre-intervention global cognition and post-intervention IADL performance was insignificant after adjusting for the mediators (β = 0.034, 95% CI [− 0.061, 0.130]), supporting a full mediation model (Table 4).
Serial mediation analysis
We assumed that increased cognitive function would lead to elevated physical function and enhanced IADL (Fig. 2). However, the results showed that there was no serial causal relationship between the two mediators (Table 4).

Serial mediation model. Indirect effects of pre-intervention MoCA on post-intervention IADL through pre-intervention DSST and TUG. The direct and indirect effects were insignificant depicted by dotted line. *p < 0.05, †p < 0.01, ‡p < 0.001.
Discussion
To the best of our knowledge, this study is the first to identify the characteristics of older adults who would benefit most in terms of IADL performance after combined cognitive and physical training, and to disentangle the mechanisms underlying the relationship between baseline global cognition and IADL performance following training. The findings showed that the important predictors and mediators of IADL performance in older adults after the intervention were processing speed and functional mobility.
In the univariate regression model, age and global cognition before the intervention were predictors of IADL performance after the intervention, but were no longer predictors in the multivariate regression model. On the other hand, the processing speed and functional mobility before intervention were independent predictors of IADL performance after intervention in both univariate and multivariate regression models. The findings indicated that processing speed and functional mobility before intervention better predicted the ability to perform IADL after intervention than age and global cognition, and that older adults who possessed better baseline performance on processing speed and functional mobility benefited the IADL performance from combined training. Therefore, considering the improvement in IADL performance in the targeted population, evidence suggests that clinical practitioners can measure the processing speed and functional mobility of older adults to recruit participants for combined cognitive and physical training instead of global cognition.
The results of the parallel mediation analysis showed that the processing speed and functional mobility before the intervention fully mediated the relationship between baseline global cognition and IADL performance following intervention in older adults. The current study provides evidence suggesting that global cognition before the intervention by itself may have a small positive effect on the IADL performance after the intervention. However, global cognition can indirectly benefit the IADL performance in older adults by enhancing the processing speed and functional mobility.
Our findings indicate that a high level of global cognition in older adults can boost the processing speed and functional mobility and, in turn, improve IADL performance following the intervention. Processing speed is considered a fundamental component of cognitive ability and is often considered the baseline for higher-order cognitive processes such as memory and executive function24,45. Age-related reduction in processing speed may lead to compromised cognitive performance since the cognitive operations that are relevant to cognitive tasks cannot be completed within a limited time and the cognitive information is not simultaneously available for higher-order cognitive processes1,3,24,45,56,57,58. Therefore, an individual requires good processing speed, which supports them to perform complex activities involving higher-order cognition, such as IADL15,17,21,22,23. Our finding coincided with previous studies stating that enhanced processing speed may contribute to lesser limitations in IADL in older adults59,60,61. Therefore, targeting processing speed ability through trainings may be an important priority for promoting healthy aging and maintaining functional independence in older adults, regardless of their baseline global cognitive function. Alternatively, functional mobility requires not only physical but also cognitive function; it involves postural control, balance, locomotion, lower-extremity strength, continuous evaluation of cues from environments, and rapid shifting motor programs based on task demands and changes in environments33,46. A prior study also suggested that among older adults, routine walking was a task involving cognitive abilities rather than an automated and rhythmic motor task62. Our findings were in line with previous studies that showed that functional mobility was associated with global cognition63,64,65,66,67. An individual with good functional mobility is able to go to different places and participate in functional and meaningful activities, such as IADL13,35,36. The results align with previous research which determined that elevated functional mobility may lead to the increased ability to perform IADL in older adults35,36,60,68. To ameliorate the IADL performance of older adults using an effective intervention strategy, the evidence suggests that the combined cognitive and physical training should target to address and enhance the processing speed and functional mobility of older adults.
Limitations
The current study had several limitations. First, the convenience sample mainly consisted of women (69.77%) and was area-specific. To increase the generalizability of our findings, a robust sampling strategy and large samples are needed in future research. Second, this was a secondary data analysis study, and we collected data from community-dwelling older adults who participated in either sequential or simultaneous interventions. However, the sample sizes of the two intervention groups were unequal due to practical considerations, and this group was included as a covariate in the analyses. Third, the measurements of the predictors and mediators (DSST and TUG) were performance-based, whereas the measurement of outcomes (IADL) was based on self-reporting. The performance-based measurement of IADL may be considered in future research.
Conclusions
With a rapidly growing aging population, identifying modifiable factors that can prevent the loss of independence is an urgent priority. To enhance the IADL performance of older adults using effective intervention strategies, our findings provide evidence that clinical practitioners can measure the processing speed and functional mobility of older adults to determine recruitment for combined cognitive and physical training and that the content of combined cognitive and physical training for older adults should aim to improve the processing speed and functional mobility for the best IADL outcomes.
Data availability
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CTT:
-
Color Trails Test
- CTT1:
-
Color Trails Test Part 1
- CTT2:
-
Color Trails Test Part 2
- DSST:
-
Digit Symbol Substitution Test
- IADL:
-
Instrumental Activities of Daily Living
- MoCA:
-
Montreal Cognitive Assessment
- TUG:
-
Timed Up and Go
- WL:
-
Word List
- WL-I:
-
Word List-Part I
- WL-II:
-
Word List-Part II
References
Harada, C. N., Natelson, L. M. C. & Triebel, K. L. Normal cognitive aging. Clin. Geriatr. Med. 29, 737–752 (2013).
Lord, S. R., Delbaere, K. & Sturnieks, D. L. Aging. Handb. Clin. Neurol. 159, 157–171 (2018).
Murman, D. L. The impact of age on cognition. Semin. Hear. 36, 111–121 (2015).
Billot, M. et al. Preserving mobility in older adults with physical frailty and sarcopenia: Opportunities, challenges, and recommendations for physical activity interventions. Clin. Interv. Aging 15, 1675–1690 (2020).
Cruz-Jimenez, M. Normal changes in gait and mobility problems in the elderly. Phys. Med. Rehabil. Clin. N. Am. 28, 713–725 (2017).
Zullo, A. et al. Structural and functional changes in the coupling of fascial tissue, skeletal muscle, and nerves during aging. Front. Physiol. 11, 592 (2020).
Chuang, I. C. et al. Baseline global cognitive function affects cognitive and functional outcomes of combined physical and cognitive training among older adults with cognitive decline. Am. J. Occup. Ther. 76, 7602205140 (2022).
Law, L. L. F., Mok, V. C. T. & Yau, M. M. K. Effects of functional tasks exercise on cognitive functions of older adults with mild cognitive impairment: A randomized controlled pilot trial. Alzheimer’s Res. Ther. 11, 1–10 (2019).
Fiatarone Singh, M. A. et al. The Study of Mental and Resistance Training (SMART) study-resistance training and/or cognitive training in mild cognitive impairment: A randomized, double-blind, double-sham controlled trial. J. Am. Med. Dir. Assoc. 15, 873–880 (2014).
Bruderer-Hofstetter, M. et al. Development of a model on factors affecting instrumental activities of daily living in people with mild cognitive impairment—A Delphi study. BMC Neurol. 20, 1–15 (2020).
Mlinac, M. E. & Feng, M. C. Assessment of activities of daily living, self-care, and independence. Arch. Clin. Neuropsychol. 31, 506–516 (2016).
Albert, S. M., Bear-Lehman, J. & Anderson, S. J. Declines in mobility and changes in performance in the instrumental activities of daily living among mildly disabled community-dwelling older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 70, 71–77 (2015).
Wang, D. X. M. et al. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 11, 3–25 (2020).
Moriyama, N. et al. Association of instrumental activities of daily living, physical function and mental health among older returnees after the Fukushima Daiichi nuclear power station accident. Int. J. Environ. Res. Public Health 18, 11639 (2021).
Cornelis, E. et al. The relationship between basic, instrumental, and advanced activities of daily living and executive functioning in geriatric patients with neurocognitive disorders. Int. J. Geriatr. Psychiatry 34, 889–899 (2019).
Reppermund, S. et al. The relationship of neuropsychological function to instrumental activities of daily living in mild cognitive impairment. Int. J. Geriatr. Psychiatry 26, 843–852 (2011).
Tomaszewski Farias, S. et al. Longitudinal changes in memory and executive functioning are associated with longitudinal change in instrumental activities of daily living in older adults. Clin. Neuropsychol. 23, 446–461 (2009).
Tomaszewski Farias, S. et al. Self-perceived difficulties in everyday function precede cognitive decline among older adults in the ACTIVE study HHS Public Access. J. Int. Neuropsychol. Soc. 24, 104–112 (2018).
Owsley, C. et al. Timed instrumental activities of daily living tasks: Relationship to cognitive function and everyday performance assessments in older adults. Gerontology 48, 254–265 (2002).
Tucker-Drob, E. M. Neurocognitive functions and everyday functions change together in old age. Neuropsychology 25, 368–377 (2011).
Bell-Mcginty, S. et al. Standard measures of executive function in predicting instrumental activities of daily living in older adults. Int. J. Geriatr. Psychiatry 17, 828–834 (2002).
Cahn-Weiner, D. A., Boyle, P. A. & Malloy, P. F. Tests of executive function predict instrumental activities of daily living in community-dwelling older individuals. Appl. Neuropsychol. 9, 187–191 (2002).
Nguyen, C. M. et al. Contribution of executive functioning to instrumental activities of daily living in older adults. Appl. Neuropsychol. Adult 27, 326–333 (2020).
Kail, R. & Salthouse, T. A. Processing speed as a mental capacity. Acta Psychol. (Amst.) 86, 199–225 (1994).
Harvey, P. D. Domains of cognition and their assessment. Dialogues Clin. Neurosci. 21, 227–237 (2019).
Glisky, E. L. Changes in cognitive function in human aging. In Brain Aging: Models, Methods, and Mechanisms (ed Riddle, D. R.) (CRC Press, 2007).
Lindsay, K., Bone, I. & Fuller, G. Clinical presentation, anatomical concepts and diagnostic approach. In Neurol Neurosurg Illus 5th edn 67–216 (Elsevier, 2010).
Diamond, A. Executive functions. Annu. Rev. Psychol. 64, 135–168 (2013).
Nasreddine, Z. S. et al. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699 (2005).
Gold, D. A. An examination of instrumental activities of daily living assessment in older adults and mild cognitive impairment. J. Clin. Exp. Neuropsychol. 34, 11–34 (2012).
Rajan, K. B. et al. Disability in basic and instrumental activities of daily living is associated with faster rate of decline in cognitive function of older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 68, 624–630 (2013).
Sigrist, A. A. F., Becattini-Oliveira, A. C. & Charchat-Fichman, H. Patterns of instrumental activities of daily living between community-dwelling older adults. Dement. Neuropsychol. 15, 366–372 (2021).
Boucą-Machado, R., Maetzler, W. & Ferreira, J. J. What is functional mobility applied to Parkinson’s disease?. J. Parkinsons Dis. 8, 121–130 (2018).
Forhan, M. & Gill, S. V. Obesity, functional mobility and quality of life. Best Pract. Res. Clin. Endocrinol. Metab. 27, 129–137 (2013).
Donoghue, O. A. et al. Using timed up and go and usual gait speed to predict incident disability in daily activities among community-dwelling adults aged 65 and older. Arch. Phys. Med. Rehabil. 95, 1954–1961 (2014).
Shimada, H. et al. Predictive validity of the classification schema for functional mobility tests in instrumental activities of daily living decline among older adults. Arch. Phys. Med. Rehabil. 91, 241–246 (2010).
Herold, F. et al. Thinking while moving or moving while thinking—Concepts of motor-cognitive training for cognitive performance enhancement. Front. Aging Neurosci. 10, 1–11 (2018).
Karssemeijer, E. G. A. et al. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 40, 75–83 (2017).
Meng, Q. et al. The effect of combined cognitive intervention and physical exercise on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Aging Clin. Exp. Res. 34, 261–276 (2022).
Lam, L. C. W. et al. Would older adults with mild cognitive impairment adhere to and benefit from a structured lifestyle activity intervention to enhance cognition?: A cluster randomized controlled trial. PLoS One 10, 1–17 (2015).
Jardim, N. Y. V. et al. Dual-task exercise to improve cognition and functional capacity of healthy older adults. Front. Aging Neurosci. 13, 589299 (2021).
Maffei, L. et al. Randomized trial on the effects of a combined physical/cognitive training in aged MCI subjects: The Train the Brain study. Sci. Rep. 7, 1–15 (2017).
Ball, K., Edwards, J. D. & Ross, L. A. The impact of speed of processing training on cognitive and everyday functions. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 62, 19–31 (2007).
Edwards, J. D. et al. An examination of mediators of the transfer of cognitive speed of processing training to everyday functional performance. Psychol. Aging 28, 314–321 (2013).
Salthouse, T. The Processing-speed theory of adult age differences in cognition. Psychol. Rev. 103, 403–428 (1996).
Demnitz, N. et al. A systematic review and meta-analysis of cross-sectional studies examining the relationship between mobility and cognition in healthy older adults. Gait Posture. 50, 164–174 (2016).
Bruijnen, C. J. W. H. et al. Psychometric properties of the Montreal Cognitive Assessment (MoCA) in healthy participants aged 18–70. Int. J. Psychiatry Clin. Pract. 24, 293–300 (2020).
Tsai, C. F. et al. Psychometrics of the Montreal Cognitive Assessment (MoCA) and its subscales: Validation of the Taiwanese version of the MoCA and an item response theory analysis. Int. Psychogeriatr. 24, 651–658 (2012).
Chen, R. H. & Chen, H. Y. Chinese Version of Wechsler Adult Intelligence Scale Manual 3rd edn. (Chinese Behavioral Science Corporation, 2002).
Jaeger, J. Digit symbol substitution test: The case for sensitivity over specificity in neuropsychological testing. J. Clin. Psychopharmacol. 38, 513–519 (2018).
Kuo, H. Y. & Hua, M. S. Chinese version of Color Trails Test Manual (Chinese Behavioral Science Corporation, 2015).
Hua, M. S. et al. Chinese Version of Wechsler Memory Scale Manual 3rd edn. (Chinese Behavioral Science Corporation, 2005).
Mathiowetz, V. et al. Adult norms for the Box and Block Test of manual dexterity. Am. J. Occup. Ther. 39, 386–391 (1985).
Podsiadlo, D. & Richardson, S. The Timed “Up & Go”: A test of basic functional mobility for frail elderly persons. Jags 39, 142–148 (1991).
Lawton, M. P. & Brody, E. M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 9, 179–186 (1969).
Cohen, R. A., Marsiske, M. M. & Smith, G. E. Neuropsychology of Aging, Handb. Clin. Neurol. 1st edn. (Elsevier, 2019).
Gkotzamanis, V. et al. Determinants of processing speed trajectories among middle aged or older adults, and their association with chronic illnesses: The English longitudinal study of aging. Life 11, 1–12 (2021).
Salthouse, T. Consequences of age-related cognitive declines. Annu. Rev. Psychol. 63, 201–226 (2012).
Kuo, H. K. et al. Cognitive function, habitual gait speed, and late-life disability in the National Health and Nutrition Examination Survey (NHANES) 1999–2002. Gerontology 53, 102–110 (2007).
Makizako, H. et al. Cognitive functioning and walking speed in older adults as predictors of limitations in self-reported instrumental activity of daily living: Prospective findings from the Obu Study of Health Promotion for the elderly. Int. J. Environ. Res. Public Health 12, 3002–3013 (2015).
Wadley, V. et al. Cognitive processing speed is strongly related to driving skills, financial abilities, and other instrumental activities of daily living in persons with mild cognitive impairment and mild dementia. J. Gerontol. Med. Sci. 76, 1829–1838 (2020).
Hausdorff, J. M. et al. Walking is more like catching than tapping: Gait in the elderly as a complex cognitive task. Exp. Brain Res. 164, 541–548 (2005).
Bruce-Keller, A. J. et al. Relationship between cognitive domains, physical performance, and gait in elderly and demented subjects. J. Alzheimer’s Dis. 30, 899–908 (2012).
Demnitz, N. et al. Cognition and mobility show a global association in middle- and late-adulthood: Analyses from the Canadian Longitudinal Study on Aging. Gait Posture 64, 238–243 (2018).
Morris, R. et al. Gait and cognition: Mapping the global and discrete relationships in ageing and neurodegenerative disease. Neurosci. Biobehav. Rev. 64, 326–345 (2016).
Rajtar-Zembaty, A. et al. Global cognitive functioning and physical mobility in older adults with and without mild cognitive impairment: Evidence and implications. Folia Med. Cracov. 59, 75–88 (2019).
Toots, A. T. M. et al. Associations between gait speed and cognitive domains in older people with cognitive impairment. J. Alzheimer’s Dis. 71, S15–S21 (2019).
Artaud, F. et al. Decline in fast gait speed as a predictor of disability in older adults. J. Am. Geriatr. Soc. 63, 1129–1136 (2015).
Acknowledgements
We thank all the participants of this study and all the occupational therapists who helped with the recruitment. This project was funded by the Healthy Aging Research Center at Chang Gung University and the Ministry of Science and Technology, Taiwan.
Funding
This project was partly supported by the Chang Gung Memorial Hospital [BMRPJ29, BMRPC58], Healthy Aging Research Center at Chang Gung University [EMRPD1M0411], the Ministry of Science and Technology, Taiwan [MOST 109-2314-B-182-008-MY2; MOST 110-2314-B-182-014; MOST 111-2314-B-182-039-MY3], and the National Science and Technology Council [NSTC 112-2314-B-182-020].
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of this study. Material preparation and data collection were performed using the IC and YW software. Data analysis was performed using the IC and KL software. The first draft of the manuscript was written by IC and IC, and all the authors commented on the previous versions of the manuscript. All the authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chuang, IC., Chen, IC., Wu, YR. et al. Prediction and mediation analysis for treatment responses to combined cognitive and physical training for older adults. Sci Rep 14, 10571 (2024). https://doi.org/10.1038/s41598-024-61407-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-61407-6
- Springer Nature Limited