
Abstract
Extracellular matrix (ECM) remodeling of the skin is a continuous process necessary for maintaining tissue homeostasis. Type VI collagen (COL6) is characterized as a beaded filament, located in the dermal ECM, where COL6-α6-chain has been demonstrated upregulated in atopic dermatitis. The aim of this study was to develop and validate a competitive ELISA, targeting the N-terminal of COL6-α6-chain, named C6A6, and evaluate its associations with the dermatological condition’s atopic dermatitis, psoriasis, hidradenitis suppurativa, systemic lupus erythematosus, systemic sclerosis, urticaria, vitiligo, and cutaneous malignant melanoma in comparison, to healthy controls. A monoclonal antibody was raised and employed in an ELISA assay. The assay was developed, technically validated, and evaluated in two independent patient cohorts. Cohort 1 showed C6A6 was significantly elevated in patients with atopic dermatitis (p < 0.0001), psoriasis (p < 0.0001), hidradenitis suppurativa (p = 0.0095), systemic lupus erythematosus (p = 0.0032) and melanoma (p < 0.0001) compared to healthy donors. Cohort 2 confirmed C6A6 being upregulated in atopic dermatitis compared to healthy controls (p < 0.0001), but also associated with disease severity (SCORAD, p = 0.046) and lowered in patients receiving calcineurin inhibitors (p = 0.014). These findings are hypothesis generating, and the utility of the C6A6 biomarker for disease severity and treatment response needs to be validated in larger cohorts and longitudinal studies.
Similar content being viewed by others


Introduction
Extracellular matrix (ECM) remodeling of the skin is a continuous process necessary for maintaining tissue homeostasis. The skin can be divided into three layers; epidermis, dermis and subcutis, which all have distinct tissue architecture and function1,2. The dermis provides tensile strength and elasticity, in addition to being the layer where fibroblasts play a key role in ECM synthesis and maintenance of tissue structure3,4. Dermal ECM can be divided into the papillary and reticular dermal ECM, and is composed by matricellular proteins (COMP, SPARC, thrombospondin-1, periostin, tenascin C and X), proteoglycans (decorin, versican, biglycan, fibromodulin and lumican), collagens (I, III, V, VI, XII, XIV and XV), fibrillin microfibrils (fibrillin-1 and -2) and elastic fiber proteins (elastin, EMLIN-1 and 2, LTBP-4, fibulin-4 and -5)2. Dysregulation of the papillary and reticular dermal ECM remodeling is a key event in the pathology of inflammatory skin diseases, including atopic dermatitis and psoriasis1,2,5.
Type VI collagen is characterized as a beaded filament collagen, found in the papillary and reticular dermal ECM, where it forms a microfibrillar network6. Six different chains of type VI collagen (α1, α2, α3, α4, α5, α6), have been identified and are expressed across connective tissues7. In vitro experiments, have demonstrated how type VI collagen α1-chain is important for ECM assembly in human dermal fibroblasts, and loss of type VI collagen resulted in loss of fibroblast motility8. In skin pathologies, the α3-chain, measured by the serum-biomarker PRO-C6, has previously been associated with progression of systemic sclerosis9. Based on transcriptomics, immunohistochemical staining and mRNA analysis, the type VI collagen α6-chain gene has been described to be upregulated in patients with atopic dermatitis10,11,12. It has also been suggested that increased levels of type VI collagen in subcutaneous tissue contributes to early phases of systemic sclerosis13. In addition, COL6Α6 is upregulated by IL-4 and IL-13 in mRNA from human keratinocytes10. Generally, the importance of type VI collagen in maintenance of tissue homeostasis in the skin, has been described, and quantifying type VI collagen in patients with dermatological disorders may be a useful tool for identification of patients and development of drugs.
We hypothesized that a specific fragment of COL6Α6 could be applied as a blood-biomarker for dermatological conditions. The aim of this study was to develop and validate a competitive ELISA, targeting the N-terminal of COL6Α6, named C6A6, and evaluate its associations with the dermatological conditions atopic dermatitis, psoriasis, hidradenitis suppurativa, systemic lupus erythematosus, systemic sclerosis, urticaria, vitiligo, and cutaneous malignant melanomaand in comparison to healthy controls.
Materials and methods
Synthetic peptides used for generation of monoclonal antibodies, assay development and assay validation were purchased from Genscript (Piscataway, NJ, US) (Table 1).
Monoclonal antibody development, production, and characterization
Monoclonal antibodies were generated by immunization of the following amino acid sequence 20'↓DSGPEYADVV 30', targeting the human α6 chain of type VI collagen. Immunization was initiated by subcutaneous injection of 200 μl emulsified antigen and 100 μg of immunogenic peptide (DSGPEYADVV-GGC-KLH) in 4- to 6-week-old Balb/C mice using Stimmune (Thermo Fisher). Immunizations were repeated every second week. The mouse with the highest stable serum titer were selected for fusion and boosted intravenously with 50 μg immunogenic peptide in 100 μl 0.9% NaCl solution 3 days before isolation of the spleen for cell fusion. Hybridoma cells were produced by fusion of the mouse spleen cells with SP2/0 myeloma cells as described by Gefter et al.14. The generated clones were plated into a 96-well microtiter plates for further growth, and the limiting dilution method was applied to promote monoclonal growth. Reactivity to the supernatant were tested by an indirect ELISA performed on streptavidin-coated plates. DSGPEYADVV -K-Biotin was used as screening peptide, while the standard peptide DSGPEYADVV was used to further test the specificity of the newly developed antibody clones. Supernatant was collected from the hybridoma cells and purified using HiTrap affinity columns (GEHealthcare Life Science, Little Chalfront, Buckinghamshire, UK) according to manufacturer’s instructions and antibody isotype was determined using Rapid ELISA Mouse monoclonal antibody Isotyping Kit (Invitrogen, Carlsbad, CA, USA) following the manufacturer’s protocol.
Reactivity toward human serum, citrate plasma, heparin plasma, EDTA plasma and rat serum was tested with purchased samples from a commercial supplier (Valley Biomedical, Winchester, VA). The monoclonal antibodies were selected to specifically recognize the standard peptide (DSGPEYADVV), and not an elongated or truncated sequence of the peptides (QDSGPEYADVV and SGPEYADVV, respectively).
C6A6 assay development
The development of the competitive chemiluminescence immunoassay (CLIA) included preliminary optimizing experiments to identify the right reagens, concentrations, incubation-time and -temperature. The final C6A6 competitive ELISA procedure was as follows: A 96-well streptavidin-coated white microplate (Greiner Bio-One, Kremsmünster, Austria) was coated with 3 ng/mL biotinylated synthetic peptide (DSGPEYADVV-K-Biotin) dissolved in assay buffer (10 mM phosphate buffered saline (PBS), 1% bovine serum albumin, 0.1% Tween-20, 0.36% Bronidox, 4 g/L NaCl, adjusted to pH 7.4 at 20 °C) and incubated for 30 min at 20 °C with constant shaking (300 rpm) in darkness. Next, 20 µL/well of standard peptide (100 ng/mL) and samples were added to the appropriate wells, followed by the addition of 100 μL/well of HRP-labelled antibody diluted in assay buffer to the concertation of 200 ng/mL and incubated for 1 h at 20 °C with constant shaking (300 rpm) in darkness. After each incubation step, wells were washed five times with the washing buffer (20 mM Tris, 50 mM NaCl, pH 7.2). The chemiluminescence substrate (Roche, BM Chemiluminescence ELISA substrate (POD), Basel, Switzerland) working solutions were mixed 15 min prior to use and 100 μL/well were added to plate and incubated for 3 min at 20 °C with constant shaking (300 rpm) in darkness. The relative light units were measured at all wavelengths within 5 min on a microplate luminometer reader (SpectraMax M5, Molecular Devices, CA, USA). A standard curve was plotted using a 4-parameter logistic curve fit Y = (A − D)/(1 + (x/C)^B) + D, where R > 0.9. Data were analyzed using the SoftMax Pro version 7.0.3 software.
Technical evaluation
Assay linearity was determined by two-fold dilutions of four human serum and two rat serum samples and calculated as percentage of recovery of the undiluted sample. To determine the assay accuracy, healthy human serum samples were spiked with standard peptide and a human serum sample with a known high C6A6 concentration and calculated as the percentage recovery of the measured value and the expected concentration of the peptide or human serum sample. Specificity of the generated monoclonal antibody was calculated as percentage of signal inhibition by two-fold diluted standard peptide (DSGPEYADVV), elongated peptide (QDSGPEYADVV), truncated peptide (SGPEYADVV), and non-sense peptide (YRDDLKKLLE). Interference of substances present in blood, was tested by adding a low/high content of hemoglobin (2.50/5 mg/mL), lipemia/lipids (1.50/5 mg/mL) and biotin (3/9 ng/mL) to a human serum sample with a known concentration of C6A6. The normal reference levels for hemoglobin, lipemia/lipids and biotin were 0–10 mg/dL (0–0.0016 mmol/L), < 150 mg/dl (< 1.69 mmol/L) and 0.22–3.00 ng/ml, respectively. The stability of the analyte was examined through temperature tests (0, 2-, 4-, 24-, and 48-h of incubation at either 4 °C or 20 °C) and five freeze–thaw cycles of human serum samples. The recovery was calculated with 0 h/0 cycle of the sample as a reference. The intra- and interassay variation was determined by 10 independent runs of five quality controls and two kit control runs in double determinations, while the measurement range was defined as the range between lower limit of measurement range (LLMR) and the upper limit of measurement range (ULMR) on the 10 runs. The standard curves from the 10 independent runs was used to determinate the IC50 (half-maximal inhibition concentration). All samples for the technical validation and biological measurements were run in double determination.
Biological evaluation of C6A6 and patient demographics
The biological capability of C6A6 was evaluated in serum samples from two cross-sectional studies. The first cohort (Cohort 1) was obtained from the commercial vendor Proteogenex (Culver City, CA, USA), and was approved by the local ethical committee (Russian Oncological Research Center, Blokhin Rams Ethics Committee review form, Protocol no. PG-ONC 2003/1). Informed consent was obtained from all participants. The second cohort (Cohort 2) was obtained from Department of Dermatology, Bispebjerg Hospital, University of Copenhagen, Denmark. This study was approved by the Committee of Biomedical Research Ethics of the Capital Region of Denmark, where all patients filed informed consent. The healthy donor samples were acquired from BioIVT (Westerbury, NY, USA) and Lee Biosolutions (Meryland Heights, MO, USA), which obtained informed concent from all participants.
Cohort 1 included patients with atopic dermatitis (n = 20), plaque psoriasis (n = 20), hidradenitis suppurativa (n = 6), systemic lupus erythematosus (n = 12), systemic sclerosis (n = 18), urticaria (n = 19), vitiligo (n = 20) and cutaneous malignant melanoma (n = 20), and matched healthy donors (n = 24) with no symptomatic or chronic disease. Cohort 2 included patients with atopic dermatitis (n = 158) and healthy age, gender, and ethnicity matched controls (n = 22). Serum samples were collected from January 2012 and June 201815. Patients with atopic dermatitis met the criteria defined by Hannifin and Rajka in 1980, assessed by a senior dermatologist. Severity was assessed by SCORAD, which is a commonly used severity index for atopic dermatitis (range 0–103 points; high score indicates severe disease). Patients were divided into disease severity groups based on SCORAD into mild (SCORAD < 25), moderate (SCORAD range 25–50), and severe disease (SCORAD > 50). Only age and gender were available for the healthy donor subjects. The study was executed in compliance with the Helsinki Declaration of 1975. Serum samples were obtained and stored at -80 °C until biomarker analysis.
Ethical statement
All animals were treated according to the guidelines for animal welfare. Monoclonal antibody production in mice was approved by the Danish National Authority (The Animal Experiments Inspectorate) under approval number 2013–15-2934–00,956. Mice were sacrificed by cervical dislocation. The study is reported in accordance with ARRIVE guidelines.
Statistical analysis
Patient characteristics of the two cohorts are presented as a number (frequency) and percentage for categorical variables and either mean with standard deviation or mean with range for continuous variables. Statistical differences for categorical variables were assessed using a Kruskal–Wallis test (nonparametric) for cohort 1, and Mann–Whitney U-test in cohort 2. For cohort 1, an ANCOVA analysis adjusted for age and gender was used to calculate the differences between the groups of patients. For cohort 2, an ANCOVA analysis adjusted for age was used to calculate the differences between the groups of patients ranging from 4 to 90 years of age. Graphs are shown as mean ± 95% CI. For all statistical analyses performed, a P-value below 0.05 was considered significant. Statistical analysis and graphs were performed using GraphPad Prism version 9 (GraphPad Software, Inc., La Jolla, CA) and MedCalc version 19.3 (MedCalc Software, Ostend, Belgium).
Results
Specificity, accuracy, and precision of the C6A6 assay
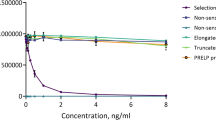
The C6A6 assay targets the N-terminal of type VI collagen, alpha 6 chain (Fig. 1A). The human sequence was aligned using UNIPROT, and the corresponding sequence in mouse and rat are 100% aligned, while bovine has one mismatch in position 1 (Fig. 1B). The hybridomas producing the best mAbs were screened for reactivity towards the standard peptide and native material. The clone NBH-306-11 8E7-2C11-1F10-2C10 was chosen for assay development and determined as an IgG1 subtype. To evaluate the specificity of the C6A6 assay, the mAb was tested towards the elongated peptide, truncated peptide, non-sense standard peptide and non-sense coater, and showed no reactivity towards those peptides (Fig. 1C). Technical validation was performed to evaluate the novel C6A6 assay. Overall, the C6A6 assay demonstrated good performance (see Table 2), including accepted inter- and intra-variations, analytes stability and limited interference from endogenous.

Overview of type VI collagen, the target of C6A6 and assay specificity. (A) The primary structure of type VI collagen including domains from all six alpha-chains, (B) Sequence alignment of the targeted COL6Α6 sequence in human, mouse, bovine and rat species (black box). The sequence was aligned using Uniprot, (C) Specificity of the C6A6 assay. Reactivity towards the standard peptide (DSGPEYADVV), truncated peptide (SGPEYADVV), elongated peptide (QDSGPEYADVV) and non-sense standard peptide (YRDDLKKLLE). No background signal was detected when coating with a non-sense coating peptide (YRDDLKKLLE-Biotin). Signals are shown as relative luminescence (RLU) per second, as a function of standard peptide.
C6A6 is elevated in patients with selected skin diseases compared to healthy controls
Cohort 1 included patients with atopic dermatitis (mean age: 52.3 years, 10% male), psoriasis (mean age: 50.7 years, 10% male), hidradenitis suppurativa (mean age: 49.5 years, 0% male), systemic lupus erythematosus (mean age: 50.5 years, 16.7% male), systemic sclerosis (mean age: 54.4 years, 5.6% male), urticaria (mean age: 43.6 years, 20% male), vitiligo (mean age: 56.9 years, 25% male) and melanoma (mean age: 55.6 years, 10% male), Table 3. C6A6 was significantly elevated in serum from patients with atopic dermatitis (p < 0.0001), psoriasis (p < 0.0001), hidradenitis suppurativa (p = 0.0095), systemic lupus erythematosus (p = 0.0032) and melanoma (p < 0.0001) compared to healthy donors (Fig. 2). No significant difference was found between patients with systemic sclerosis, urticaria, and vitiligo and healthy controls (p > 0.1).

Results from cohort 1. Serum levels of C6A6 were assessed in healthy donors (n = 20), and in patients with atopic dermatitis (n = 20), psoriasis (n = 20), hidradenitis suppurativa (n = 6), systemic lupus erythematosus (n = 12), systemic sclerosis (n = 14), urticaria (n = 19), vitiligo (n = 20), and melanoma (n = 20). Mean with 95% confidence interval. Data was analyzed using an ANCOVA corrected for age and gender. Data are depicted as mean ± 95%CI.
C6A6 is associated with disease severity in atopic dermatitis and lower in patients treated with topical immunomodulatory treatment
Cohort 2 included 158 patients with atopic dermatitis (mean age: 30.0, 52% male), and 22 healthy donors (mean age: 29.6, 50% male), Table 4. Patients with atopic dermatitis had significantly higher levels of C6A6 compared to healthy controls (p < 0.0001, Fig. 3). Out of 158 atopic dermatitis patients, 53 (33.3%) had mild disease, 72 (45.3%) had moderate disease and 33 (21.4%) had severe disease. We evaluated whether the C6A6 assay was associated with disease severity, by comparing patients with severe atopic dermatitis (SCORAD > 50) to patients with mild and moderate atopic dermatitis (SCORAD 0–50). C6A6 was significantly higher in patients with severe atopic dermatitis, compared to mild and moderate atopic dermatitis (p = 0.046, Fig. 4A). Out of 158 patients, 47 patients received topical immunomodulatory treatment with calcineurin inhibitors pimecrolimus or tacrolimus. Patients receiving treatment, had significantly lower levels than patients not receiving treatment (p = 0.014, Fig. 4B). In addition, patients with mild and moderate atopic dermatitis receiving topical calcineurin inhibitors had significantly lower levels of C6A6, compared to those without treatment (p = 0.035, Fig. 4C), while there was no difference in severe atopic dermatitis patients receiving topical calcineurin inhibitors (p > 0.1, Fig. 4D).

Levels of C6A6 in healthy donors (n = 22) and patients with atopic dermatitis (n = 158). C6A6 levels in healthy donors and patients with atopic dermatitis. Mean with 95% confidence interval. Data was analyzed using an ANCOVA corrected for age. Data are depicted as mean ± 95%CI.

Levels of C6A6 stratified into disease severity and treatment. (A) Levels of C6A6 divided into mild and moderate AD (SCORAD; 0–50), and severe AD (SCORAD; < 50), (B) Levels of C6A6 divided into AD patients’ immunosuppressant treatment (topical calcineurin inhibitors), (C) Levels of C6A6 for mild and moderate AD patients receiving immunosuppressant treatment, (D) Levels of C6A6 for severe AD patients receiving immunosuppressant treatment. Mean with 95% confidence interval. Data was analyzed using an ANCOVA corrected for age. Data are depicted as mean ± 95%CI.
Discussion
In this study, we developed and characterized a competitive ELISA for detection of C6A6 using a monoclonal antibody targeting the N-terminal of type VI collagen alpha-6 chain. The main findings of this study were as follows: 1) development of a robust and specific C6A6 assay towards the sequence DSGPEYADVV; 2) C6A6 was detectable in human, mouse and rat serum; 3) C6A6 was upregulated in patients diagnosed with atopic dermatitis, melanoma, psoriasis, hidradenitis suppurativa and systemic lupus erythematosus, compared to healthy donors; 5) C6A6 was associated with severe atopic dermatitis and decreased with immunomodulatory treatment. To our knowledge, this is the first study to show that C6A6 can be measured in serum from patients with dermatological conditions and is associated with disease severity and lowered in patients treated with topical immunomodulators in atopic dermatitis.
The C6A6 assay is characterized as a technically robust and accurate assay by showing acceptable dilution recovery, interference, and stability tests. The intra- and inter-variation was accepted with values of 5% and 12%, respectively. The assay was further characterized as being specific towards the N-terminal site of C6A6 after cleavage of the signal peptide.
Type VI collagen is located in the papillary and reticular dermal ECM and collagen VI microfibrils are closely associated with the basement membrane in skin, blood vessels and muscle, kidney and nerves, where they serve to attach the basement membrane into the surrounding extracellular matrix16. Type VI collagen is produced by fibroblasts1,2,3. Fibroblasts are activated and produce collagens in different disorders, including fibrosis and cancer. In dermatological diseases, fibroblasts are known to be implicated in impaired wound healing , fibrosis and cause extensive tissue remodeling4. As an example, in hidradenitis suppurativa fibroblasts are known to contribute to tunnel formation and inflammation, and thereby contribute to disease progression1, while in atopic dermatitis, different subpopulations of fibroblasts have been identified from lesions, where especially the inflammatory fibroblast population is suspected to signal to immune cells to mediate ECM breakdown, fibrotic remodeling and T-cell recruitment2.
Previously, the type VI collagen alpha-6 chain has been found to be upregulated in the blood vessels in the fibrotic dermis of wild type mice17 and in patients with atopic dermatitis by other analysis methods: transcriptomics, immunohistochemical staining and mRNA analysis10,11,12. These findings suggest that this particular collagen chain may be biologically relevant for patients with atopic dermatitis, and a blood-based biomarker may therefore be a tool to detect changes of this protein in circulation. Based on mRNA analysis from human keratinocytes, the level of type VI collagen alpha-6 was suppressed by addition of IL-4 and IL-1310. In this study, we found C6A6 to be suppressed in patients with mild and moderate atopic dermatitis when treated with topical calcineurin inhibitors. Topical calcineurin inhibitors, including pimecrolimus and tacrolimus, are widely used as first-line immunosuppressant topical treatment for atopic dermatitis and also in psoriasis18. This generates the hypothesis that C6A6 may be associated with treatment response. On the contrary, we did not see any inhibition in severe atopic dermatitis patients, which may indicate this group of patients need another type of treatment than topical calcineurin inhibitors. Nevertheless, this finding may be due to statistical power, with only seven patients in the treatment group. Topical calcineurin inhibitors are use for treatment of atopic dermatitis and can be found in two forms–tacrolimus (0.03–0.1% oinment, used for mild-moderate atopic dermatitis) or pimecrolimus (1.0%, used for moderate-severe atopic dermatitis) cream19. The drugs inhibit synthesis of proinflammatory cytokines and are used as an alternative to corticosteroids. Specifically, immunosuppressive activity results from suppressing the calcineurin activity, where calcineurin inhibitors have anti-inflammatory activity due to T-helper activity affected synthesis and release of pro-inflammatory cytokines. Tacrolimus and pimecrolimus inhibits mast cell and neutrophil activation, while releasing inflammatory mediators. Tacrolimus affects the basophils and eosinophil function, as well as apoptosis of Langerhans cells20,21.
Limitations of the study include assessment of C6A6 in relatively small cohorts with a cross-sectional design. Moreover, only limited clinical information was available from the two investigated patient cohorts. In conclusion, the C6A6 assay showed a high specificity towards the N-terminal peptide and was elevated in patients with dermatological conditions. It was able to distinguish AD patients from healthy donors, demonstrating a high discriminative power. The C6A6 assay was also upregulated in patients with severe AD, indicating that severe patients experience more fibroblast activity and general tissue remodeling. This may also be the case for the other skin indications, and not a specific AD remodeling process. In addition, we found the biomarker levels to be lowered in patients treated with topical immunomodulators (calcineurin inhibitors), indicating this biomarker may be associated with treatment response. These findings are hypothesis generating, and the utility of the C6A6 biomarker for disease severity and treatment response needs to be validated in larger cohorts and longitudinal studies.
Data availability
All data from this study are included in this article. Data are kept on file and are not publicly available due to privacy data legislation. Requests can be directed to the corresponding author.
References
Simon, D., Aeberhard, C., Erdemoglu, Y. & Simon, H. U. Th17 cells and tissue remodeling in atopic and contact dermatitis. Allergy 69, 125–131 (2014).
Dengjel, J., Bruckner-Tuderman, L. & Nyström, A. Skin proteomics–analysis of the extracellular matrix in health and disease. Expert Rev. Proteomics 17, 377–391 (2020).
Lynch, M. D. & Watt, F. M. Fibroblast heterogeneity: Implications for human disease. J. Clin. Invest. 128, 26–35 (2018).
Cescon, M., Gattazzo, F., Chen, P. & Bonaldo, P. Collagen VI at a glance. J. Cell Sci. 128, 3525–3531 (2015).
Wagner, M. F. M. G., Theodoro, T. R., Filho, C. D. A. S. M., Oyafuso, L. K. M. & Pinhal, M. A. S. Extracellular matrix alterations in the skin of patients affected by psoriasis. BMC Mol. Cell Biol. 22, 1 (2021).
Holm Nielsen, S. et al. A fragment of collagen type VI alpha-3 chain is elevated in serum from patients with gastrointestinal disorders. Sci. Rep. 10, 5910 (2020).
Fitzgerald, J., Holden, P. & Hansen, U. The expanded collagen VI family: New chains and new questions. Connect. Tissue Res. 54, 345–350 (2013).
Georgios, T. et al. Type VI collagen regulates dermal matrix assembly and fibroblast motility. J. Invest. Dermatol. 136, 74–83 (2016).
Dobrota, R. et al. Circulating collagen neo-epitopes and their role in the prediction of fibrosis in patients with systemic sclerosis: a multicentre cohort study. Lancet Rheumatol. 3, e175–e184 (2021).
Jung, H. J. et al. The role of collagen VI α6 chain gene in atopic dermatitis. Ann. Dermatol. 34, 46–54 (2022).
Ghosh, D. et al. Multiple transcriptome data analysis reveals biologically relevant atopic dermatitis signature genes and pathways. PLoS ONE 10, 1–23 (2015).
Heo, W. Il et al. Identification of novel candidate variants including COL6A6 polymorphisms in early-onset atopic dermatitis using whole-exome sequencing. BMC Med. Genet. 18, (2017).
Takasaki, S., Fujiwara, S., Shinkai, H. & Ooshima, A. Human type VI collagen: Purification from human subcutaneous fat tissue and an immunohistochemical study of morphea and systemic sclerosis. J. Dermatol. 22, 480–485 (1995).
Gefter, M. L., Margulies, D. H. & Scharff, M. D. A simple method for polyethylene glycol-promoted hybridization of mouse myeloma cells. Somatic Cell Genet. 3, 231–236 (1977).
Holm, J. G., Agner, T., Clausen, M. L. & Thomsen, S. F. Determinants of disease severity among patients with atopic dermatitis: Association with components of the atopic march. Arch. Dermatol. Res. 311, 173–182 (2019).
Lamandé, S. R. & Bateman, J. F. Collagen VI disorders: Insights on form and function in the extracellular matrix and beyond. Matrix Biol. 71–72, 348–367 (2018).
Lettmann, S. et al. Col6a1 null mice as a model to study skin phenotypes in patients with collagen VI related myopathies: Expression of classical and novel collagen vi variants during wound healing. PLoS ONE 9, e105686 (2014).
Wang, C. & Lin, A. Efficacy of topical calcineurin inhibitors in psoriasis. J. Cutan. Med. Surg. 18, 8–14 (2014).
Gutfreund, K., Bienias, W., Szewczyk, A. & Kaszuba, A. Topical calcineurin inhibitors in dermatology. Part I: Properties, method and effectiveness of drug use. Adv. Dermatol. Allergol. Dermatologii Alergol. 30, 165 (2013).
Gisondi, P., Ellis, C. N. & Girolomoni, G. Pimecrolimus in dermatology: atopic dermatitis and beyond. Int. J. Clin. Pract. 59, 969–974 (2005).
Nghiem, P., Pearson, G. & Langley, R. G. Tacrolimus and pimecrolimus: from clever prokaryotes to inhibiting calcineurin and treating atopic dermatitis. J. Am. Acad. Dermatol. 46, 228–241 (2002).
Author information
Authors and Affiliations
Contributions
Conceptualization: SHN, ACBJ, SFT; Data Curation: SFT; Formal Analysis: SHN, HP, ACBJ, MK, SFT; Investigation: SHN, HP, JGH, VWN, JPT, AE, SFT; Methodology: SHN, CMH, SFT; Resources: SHN, HP, CMH, JGH, JPT, SSG, MK, VWN, AE, ACBJ, SFT; Supervision: ACBJ, SFT; Visualization: SHN, HP, CMH, ACBJ, SFT; Writing Original Draft Preparation: SHN; Writing – Review and Editing: SHN, HP, CMH, JGH, JPT, SSG, MK, VWN, AE, ACBJ, SFT.
Corresponding author
Ethics declarations
Competing interests
SHN, HP, CMH, MK, and ACBJ are full-time employees at Nordic Bioscience A/S. Nord 9. Nordic Bioscience is a privately-owned, small–medium-size enterprise (SME) partly focused on developing biomarkers. None of the authors received fees, bonuses, or other benefits for the work described in the manuscript. SHN, MAK, and ACBJ hold stocks in Nordic Bioscience A/S. JGH, JPT, SSG, VWN, AE and SFT have no competing interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Holm Nielsen, S., Port, H., Møller Hausgaard, C. et al. A fragment of type VI collagen alpha-6 chain is elevated in serum from patients with atopic dermatitis, psoriasis, hidradenitis suppurativa, systemic lupus erythematosus and melanoma. Sci Rep 13, 3056 (2023). https://doi.org/10.1038/s41598-023-28746-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-28746-2
- Springer Nature Limited