
Abstract
In young patients with acute pulmonary embolism (PE), the predictive value of currently available prognostic tools has not been evaluated. Our objective was to compare prognostic value of 7 available tools (GPS, PESI, sPESI, Prognostic Algorithm, PREP, shock index and RIETE) in patients aged <50 years. We used the RIETE database, including PE patients from 2001 to 2017. The major outcome was 30-day all-cause mortality. Of 34,651 patients with acute PE, 5,822 (17%) were aged <50 years. Of these, 83 (1.4%) died during the first 30 days. Number of patients deemed low risk with tools was: PREP (95.9%), GPS (89.6%), PESI (87.2%), Shock index (70.9%), sPESI (59.4%), Prognostic algorithm (58%) and RIETE score (48.6%). The tools with a highest sensitivity were: Prognostic Algorithm (91.6%; 95% CI: 85.6–97.5), RIETE score (90.4%; 95%CI: 84.0–96.7) and sPESI (88%; 95% CI: 81–95). The RIETE, Prognostic Algorithm and sPESI scores obtained the highest overall sensitivity estimates for also predicting 7- and 90-day all-cause mortality, 30-day PE-related mortality, 30-day major bleeding and 30-day VTE recurrences. The proportion of low-risk patients who died within the first 30 days was lowest using the Prognostic Algorithm (0.2%), RIETE (0.3%) or sPESI (0.3%) scores. In PE patients less 50 years, 30-day mortality was low. Although sPESI, RIETE and Prognostic Algorithm scores were the most sensitive tools to identify patients at low risk to die, other tools should be evaluated in this population to obtain more efficient results.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
The incidence and severity of acute pulmonary embolism (PE) progressively increase with patient’s age1,2,3. In the elderly, PE generally develops in patients with impaired mobility and a number of co-morbidities or the use of concomitant drugs4,5,6. In young individuals, PE frequently affects women with hormonal alterations (including pregnancy or use of contraceptives), with minor co-morbidities, or in presence thrombophilia4,5,6,7,8. Unfortunately, data on the clinical presentation, treatment, and outcomes during the course of anticoagulation in young patients with PE remain scarce. Although mortality in this population is low, the impact in terms of avoidable deaths and complications is relevant. Further, it remains unclear whether the widely available risk prediction tools (e.g., PESI, sPESI, and others) – primarily validated in older patients with a high burden of co-morbidities – do perform well in the young9.
In the Emergency wards, prognostic tools are commonly used to classify patients with PE into high-, medium- or low-risk categories, aimed at selecting the most appropriate management strategy at the individual level. However, a number of systematic reviews of prognostic models showed inconsistent results across the studies10,11,12,13,14. In 2016, a systematic review and meta-analysis provided evidence-based information on the validity and utility of several prognostic tools9, although their performances in patients aged <50 years remains unclear.
The most severe short-term complication of PE is 30-day all-cause death. The RIETE (Registro Informatizado Enfermedad TromboEmbólica) registry was established in Spain in 2001. It is an ongoing, multicenter, international observational registry of consecutive patients with objectively confirmed venous thromboembolism (VTE)15. The aim of this study was to compare seven currently available prognostic tools in terms of their ability to identify low-risk patients with acute PE aged <50 years.
Methods
Study design
We retrospectively compared seven different prognosis tools in patients aged <50 years with no-high risk acute PE. The major outcome measure was 30-day all-cause mortality. Secondary outcomes included 7-day and 90-day all-cause mortality as well as the 30-day PE-related mortality, major bleeding, and VTE recurrences rates.
Inclusion criteria
Patients included in the RIETE registry we deemed eligible in presence of acute symptomatic PE confirmed by objective testing (pulmonary angiography, ventilation-perfusion lung scintigraphy or helical computed tomography scan). Patients were excluded if they were currently participating in a therapeutic clinical trial with a blinded study drug. The methodology of RIETE has been previously published15. Data were recorded from each participating hospital and submitted to a coordinating center through a secure website. Each patient was assigned with a unique identification number to maintain patient confidentiality, and data quality was regularly monitored electronically. Patients received anticoagulant treatment according to current guidelines16,17,18. All patients provided oral or written informed consent to be included in the registry, according to the requirements of ethics committees within each hospital (Authorization of clinical research ethics committee Germans Trias i Pujol and Institut Catalá de la Salud, 05122006). Researchers assessed mortality by using patient or proxy interviews and/or through review of hospital clinical records. In case of death, we performed a thorough review of medical records (accompanied by proxy interviews when necessary) to clarify the date and cause of death. Investigators were instructed to classify a death as due to PE in the following cases: 1) PE-related death confirmed on necropsy or 2) death following a clinically severe PE event (either initially or shortly after an objectively confirmed recurrent event) in the absence of any alternative diagnosis. Major bleeding was defined as bleeding occurring at high-risk anatomic locations (intracranial, intra-spinal, intraocular, retroperitoneal, intra-articular, pericardial, or intramuscular bleeding with compartment syndrome), or overt bleeding requiring a transfusion of two or more units of packed red blood cells. Confirmation of recurrent PE was documented by evidence of a novel intraluminal filling defect on CT, enlargement of a previous filling defect on CT, or evidence of a new perfusion scan defect involving >75% of a lung segment.
Study variables and definitions
The following parameters are recorded in RIETE: patient’s baseline characteristics; clinical status (including any coexisting or underlying conditions such as chronic heart or lung disease), recent major bleedings; presence of anemia; creatinine levels; risk factors for PE; treatment received upon PE diagnosis; therapeutic outcomes; and risk factors for PE according to the ISTH criteria19. Recent bleeding was considered to be present in subjects who suffered a major bleeding <30 days before PE.
Prognostic tools
Comparison of prognostic tools was performed through discrimination20,21. In accordance with the current guidelines22,23, the tools aimed at identifying low-risk PE patients were evaluated according to their sensitivity. The following prognostic tools were investigated: Geneva prognostic score (GPS)24, Pulmonary Embolism Severity Index (PESI)25, simplified PESI (sPESI)26, Prognostic Algorithm27, Facteurs PRonostiques dans l’Embolie Pulmonaire (PREP)28, shock index29, and RIETE score30. The prognostic tools are depicted in detail in Supplement Table 1.
Follow-up
Patients were managed according to the clinical practice of each participating hospital and were not subjected to any predetermined intervention. For the study purpose of the study and in light of the primary outcome measure, patients were followed up for a minimum of 30 days. In addition, data at 90 days were collected for analyzing the secondary outcome. During follow-up, special attention was paid to any signs or symptoms suggestive of recurrent PE or bleeding complications. Each episode of suspected recurrent deep vein thrombosis (DVT) or PE required documented objective imaging findings. Most outcomes were classified as reported by the participating centers. However, a central adjudicating committee reviewed all outcomes reported as uncertain (less than 10% of all events).
Statistical analysis
A descriptive analysis was performed using relative frequencies for categorical variables and means (SD) for continuous variables. We used the Student’s t-test and the χ2 test (or Fisher’s exact test where appropriate) to compare continuous or categorical variables, respectively. The 95% confidence interval (CI) for proportions was calculated using the Clopper-Pearson exact method. The discrimination of models was evaluated by the degree to which they distinguished between subjects who reached the outcome versus those who did not. We used the area under curve (AUC) and determined the percentage of patients deemed to be at low-risk. We assessed sensitivity, specificity, positive and negative predictive values. All calculations were performed with the SPSS statistical software, version 20 (IBM, Armonk, NY, USA). Two-sided p values < 0.05 were considered statistically significant.
Results
Of the 34,651 patients with acute PE enrolled in RIETE by August 2017, 5,822 (17%) were aged <50 years (Fig. 1). Patients aged <50 years were less likely to have concomitant diseases (Table 1). Moreover, they had a higher likelihood to have chest pain or tachycardia at baseline and a lower likelihood to present with syncope, hypoxemia, raised troponin levels, atrial fibrillation, right bundle branch block on the electrocardiogram, right ventricle dysfunction or raised pulmonary artery pressure levels on the echocardiogram. Finally, patients aged <50 years were more likely to score at low-risk according to PESI or sPESI. Eight of the 5,822 patients (0.14%) did not receive anticoagulant therapy. Of them, five did not start anticoagulation because they died on the same day of PE diagnosis. Three cases underwent inferior vena cava filter placement because of contraindications to anticoagulation.

Flow diagram.
Overall, 38 patients aged <50 years (0.65%; 95% CI: 0.46–0.89%) died within the first 7 days, 83 (1.43%; 95% CI: 1.14–1.76%) within the first 30 days, and 148 (2.54%; 95% CI: 2.15–2.98%) within the first 90 days. The most common causes of death at 30 days were pulmonary embolism (39.7%) and disseminated cancer (32.4%). Moreover, 45 patients (0.77%) developed major bleeding and 63 (1.08%) had VTE recurrences within the first 30 days (55.5% recurred as PE and 44.5% as DVT).
30-day all-cause mortality
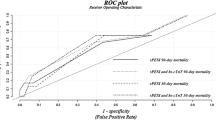
The proportion of patients considered to be at low risk was highest using the PREP (95.9%), GPS (89.6%) or PESI (87.2%) scores, whereas the proportion of low-risk patients who died within the first 30 days was lowest using the Prognostic Algorithm (0.2%), RIETE (0.3%), or sPESI (0.3%) scores (Table 2). The highest sensitivity was obtained using the Prognostic Algorithm (91.6%; 95% CI: 85.6–97.5%), RIETE (90.4%; 95% CI: 84–96.7%), or sPESI scores (88%; 95% CI: 81–95%; Table 3). All prognostic tools had an excellent negative predictive value. The tools that performed better in terms of specificity were PREP (96.2%; 95% CI: 95.7–96.7%), GPS (90.2%; 95% CI: 89.4–90.9%), and PESI (87.8%; 95% CI: 87–88.7%).
7- and 90-day all-cause mortality and other outcomes
With regard to the prediction of 30-day PE-related mortality, the highest sensitivity estimates were obtained using the Prognostic Algorithm (90.3%; 95% CI: 79.9–100%), RIETE score (87.1%; 95% CI: 75.3–98.9%), and sPESI (83.8%; 95% CI: 70.9–96.8%; Table 4). As far as major bleeding is concerned, the highest sensitivity estimates were obtained using the RIETE (73.3%; 95%CI: 60.4–86.3%), Prognostic Algorithm (66.7%; 95% CI: 52.9–80.4%), and sPESI scores (64.4%; 95% CI: 50.5–78.4%). With regard to VTE recurrences, the highest sensitivity estimates were obtained using the RIETE (68.3%; 95% CI: 56.8–79.8%), Prognostic Algorithm (66.7%; 95% CI: 55–78.3%), and sPESI scores (65.1%; 95% CI: 53.3–76.9%). For 7- or 90-day all-cause mortality, 30-day major bleeding and 30-day VTE recurrences, the highest sensitivity estimates were obtained using the RIETE, Prognostic Algorithm, and sPESI scores (Table 5).
Discussion
The risk for PE progressively increases with the patient’s age. However, young patients are not uncommon, with one in every 6 cases in our cohort (17%) being aged <50 years. These patients had fewer co-morbidities, different risk factors, and different signs or symptoms at baseline compared with those aged ≥50 years. The 30-day mortality rate in our patients <50 years was low (1.43%) compared with the rate of 7.4% observed in the entire sample9. Despite these favorable figures, tools to identify low-risk patients should be sensitive and efficient. An improved identification of patients at risk and the use of accurate prognostic tools may pave the way to optimized management strategies (i.e., drug selection, optimal dosing, treatment settings), ultimately reducing mortality rates. The current study compared seven distinct prognostic tools in the same patient cohort. Our main results indicated that sPESI, RIETE, and the Prognostic Algorithm scores were the most efficient tools to identify PE patients aged <50 years at low risk of death within the first 30 days. Notably, these three tools also had the highest sensitivity in the prediction of 7- and 90-day all-cause mortality, 30-day PE-related mortality, 30-day major bleeding, and 30-day VTE recurrences.
Prognostic tools to identify low-risk patients with PE need to have the highest overall sensitivity and negative predictive value. Most of the tools examined in our study were effective and associated with a low event rate in patients considered at low risk. One important prerequisite is the definition of an incidence limit for a specific outcome that should be clinically relevant9. The correct identification of low-risk patients is paramount in real-life clinical practice. Tools characterized by a low incidence of events in the low-risk group identifies a smaller proportion of patients, being more effective but less efficient. In our study, tools with the higher proportion of patients considered to be at low-risk were PREP, Geneva, and PESI, although their sensitivity was low. The selection of the best prognostic tool in a specific population is crucial to identify subjects at low risk that may be safely discharged home or managed in an outpatient setting. Although 30-day all-cause mortality was overall low in patients aged <50 years, the social, psychological, and economic impact of such deaths is not negligible. In 2017, the HOPPE score has been specifically developed to identify low-risk patients31. It is characterized by a good sensitivity (96–99%) and negative predictive value (95–96%) in the prediction of 30-day mortality. The HOPPE score consists of five ordinal variables (scored as 1, 2, or 3 points, respectively), as follows: systolic blood pressure values (>120, 100 to 119, <99 mmHg), diastolic blood pressure values (>80, 65 to 79, <64 mmHg), heart rate (<80, 81 to 100, > 101 beats/min), arterial partial pressure of oxygen (>80, 60 to 79, <59 mmHg), and modified electrocardiographic score (<2, 2 to 4, >4). The following modified electrocardiographic score with adjusted variables and point values is used: tachycardia: 2 points; incomplete right bundle branch block: 1 point; complete right bundle branch block: 3 points; T-wave inversion in V1 to V3: 4 points; S1Q3T3: 4 points. The HOPPE score finally identifies three prognostic groups, as follows: low-risk: 0–6 points; intermediate-risk: 7–10 points; high-risk: 11–15 points. Although Subramanian and co-workers31 reported a short-term mortality of 0% (95% CI: 0–0.8%) in the low-risk group, the authors maintained that prospective validation of the HOPPE score is required before its implementation in clinical practice. Assessment of other tools or biomarkers may lead to the development of a more efficient model while maintaining a high sensitivity in the detection of low-risk patients.
The sPESI, RIETE, and Prognostic Algorithm scores are based on 6, 11, and 10 variables, respectively. The similar performances of the scores may be explained by the fact that five items are shared (Supplement Table 2) – including cancer, heart failure, pulse ≥110 beats per minute, systolic blood pressure <100 mmHg, and arterial blood oxygen saturation <90%. The Prognostic Algorithm and sPESI also have age in common, whereas the Prognostic Algorithm and RIETE score share common chronic renal disease. For the sake of simplicity, the use of sPESI may be recommended. One of the most interesting findings was that PESI, a consistently validated tool, did not perform well in this patient population. Although patients deemed at low risk according to PESI had a low 30-day mortality rate (0.7%; 95% CI: 0.5–0.9%), the sensitivity of the tool was low as well (59%; 95% CI: 48.5–69.6%). We speculate that this may stem from the influence of patient’s age on the score calculation. Accordingly, age is treated as a quantitative variable in PESI.
This work has several limitations. First, the design of RIETE does not randomize patients to different strategies or drugs, although quality-control audits are periodically implemented. We believe that our registry may provide relevant real-life data in a large number of patients observed outside the rigorous and controlled conditions of clinical trials. As such, it may be helpful to identify risk factors for clinical outcomes in an unselected patient population. Second, it is likely that patients who died early after PE (i.e., within 2–3 days) were not included in the cohort (because of lack of informed consent or death in emergency room). Third, the attribution of deaths to PE may be difficult owing to the lack of a validated definition based on broadly accepted criteria. Although causes of death were investigated by a thorough review of medical records, an overestimation of PE-related mortality cannot be ruled out32.
This study has two strengths. First, we simultaneously analyzed seven different prognostic tools in a large population of over 5,000 patients. This approach overcomes the caveats of heterogeneity in meta-analyses or propensity scores matching. Second, this study evaluated not only 30-day all-cause mortality but also other short-term complications of PE (i.e., PE-related death, VTE recurrences, and bleedings).
Conclusion
We compared seven prognostic tools to identify which was the most sensitive to identify patients aged <50 years with acute PE at low risk for 30-day mortality. The most performing tools were sPESI, RIETE, and Prognostic Algorithm. Because the mortality rates in our population were low, more efficient tools or biomarkers are required to improve the prognostic categorization of this patient group. Compared with elderly cases, PE patients aged <50 years have a different profile, with less co-morbidities, different risk factors, and different signs and symptoms.
References
Spencer, F. A. et al. Venous thromboembolism in the elderly. A community-based perspective. Thromb. Haemost. 100, 780–788 (2008).
Robert-Ebadi, H. & Righini, M. Diagnosis and management of pulmonary embolism in the elderly. Eur. J. Intern. Med. 25, 343–349 (2014).
Kokturk, N., Oguzulgen, I. K., Demir, N., Demirel, K. & Ekim, N. Differences in clinical presentation of pulmonary embolism in older vs younger patients. Circ. J. 69, 981–986 (2005).
Stein, P. D. et al. Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. Am. J. Med. 120, 871–879 (2007).
Lee, E. Y. et al. Pulmonary embolism detected by pulmonary MDCT angiography in older children and young adults: risk factor assessment. AJR. Am. J. Roentgenol. 198, 1431–1437 (2012).
Castelli, R., Bergamaschini, L., Sailis, P., Pantaleo, G. & Porro, F. The impact of an aging population on the diagnosis of pulmonary embolism: comparison of young and elderly patients. Clin. Appl. Thromb. Hemost. 15, 65–72 (2009).
Cefalo, P. et al. A comparison of patients diagnosed with pulmonary embolism who are ≥65 years with patients <65 years. Am. J. Cardiol. 115, 681–686 (2015).
Kiluk, I. E. et al. Different manifestations of pulmonary embolism in younger compared to older patients: Clinical presentation, prediction rules and long-term outcomes. Adv. Med. Sci. 62, 254–258 (2017).
Elias, A., Mallett, S., Daoud-Elias, M., Poggi, J. N. & Clarke, M. Prognostic models in acute pulmonary embolism: a systematic review and meta-analysis. BMJ. Open. 6, e010324 (2016).
Becattini, C., Vedovati, M. C. & Agnelli, G. Prognostic value of troponins in acute pulmonary embolism: a meta-analysis. Circulation. 116, 427–433 (2007).
Klok, F. A., Mos, I. C. & Huisman, M. V. Brain-type natriuretic peptide levels in the prediction of adverse outcome in patients with pulmonary embolism: a systematic review and meta-analysis. Am. J. Respir. Crit. Care. Med. 178, 425–430 (2008).
Sanchez, O. et al. Prognostic value of right ventricular dysfunction in patients with haemodynamically stable pulmonary embolism: a systematic review. Eur. Heart. J. 29, 1569–1577 (2008).
Jiménez, D. et al. Troponin-based risk stratification of patients with acute nonmassive pulmonary embolism: systematic review and metaanalysis. Chest. 136, 974–982 (2009).
Lega, J. C., Lacasse, Y., Lakhal, L. & Provencher, S. Natriuretic peptides and troponins in pulmonary embolism: a meta-analysis. Thorax. 64, 869–875 (2009).
Bikdeli, B. et al. RIETE Investigators. Rationale, Design and Methodology of the Computerized Registry of Patients with Venous Thromboembolism (RIETE). Thromb. Haemost. 118, 214–224 (2018).
Kearon, C. et al. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 133, 454S–545S (2008).
Kearon, C. et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 141, e419S–e496S (2012).
Kearon, C. et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 149, 315–352 (2016).
Kearon, C. et al. Subcommittees on Control of Anticoagulation, and Predictive and Diagnostic Variables in Thrombotic Disease. Categorization of patients as having provoked or unprovoked venous thromboembolism: guidance from the SSC of ISTH. J. Thromb. Haemost. 14, 1480–1483 (2016).
Van, Houwelingen, H. C. Validation, calibration, revision and combination of prognostic survival models. Stat. Med. 19, 3401–3415 (2000).
Royston, P. & Altman, D. G. External validation of a Cox prognostic model: principles and methods. BMC. Med. Res. Methodol. 13, 33 (2013).
Authors/Task Force Members: Konstantinides, S. V. et al. Document Reviewers: 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Respir. J. 54, https://doi.org/10.1183/13993003.01647 (2019).
Konstantinides, S. V. et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart. J. https://doi.org/10.1093/eurheartj/ehz405 (2019).
Wicki, J., Perrier, A., Perneger, T. V., Bounameaux, H. & Junod, A. F. Predicting adverse outcome in patients with acute pulmonary embolism: a risk score. Thromb. Haemost. 84, 548–552 (2000).
Aujesky, D. et al. Derivation and validation of a prognostic model for pulmonary embolism. Am. J. Respir. Crit. Care. Med. 172, 1041–1046 (2005).
Jiménez, D. et al. RIETE Investigators. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch. Intern. Med. 170, 1383–1389 (2010).
Aujesky, D. et al. A prediction rule to identify low-risk patients with pulmonary embolism. Arch. Intern. Med. 166, 169–175 (2006).
Sanchez, O. et al. Prognostic factors for pulmonary embolism: the prep study, a prospective multicenter cohort study. Am. J. Respir. Crit. Care. Med. 181, 168–173 (2010).
Toosi, M. S., Merlino, J. D. & Leeper, K. V. Prognostic value of the shock index along with transthoracic echocardiography in risk stratification of patients with acute pulmonary embolism. Am. J. Cardiol. 101, 700–705 (2008).
Maestre, A. et al. RIETE Investigators. Identification of Low-Risk Patients with Acute Symptomatic Pulmonary Embolism for Outpatient Therapy. Ann. Am. Thorac. Soc. 12, 1122–1229 (2015).
Subramanian, M. et al. Derivation and Validation of a Novel Prediction Model to Identify Low-Risk Patients With Acute Pulmonary Embolism. Am. J. Cardiol. 120, 676–681 (2017).
Lakkireddy, D. R., Gowda, M. S., Murray, C. W., Basarakodu, K. R. & Vacek, J. L. Death certificate completion: how well are physicians trained and are cardiovascular causes overstated? Am. J. Med. 117, 492–498 (2004).
Acknowledgements
This study received funding: SEPAR (1/2016) grupo GeCIR. We express our gratitude to Sanofi Spain for supporting this Registry with an unrestricted educational grant. We also wish to thank Bayer Pharma AG for supporting this Registry. Bayer Pharma AG’s support was limited to the part of RIETE outside Spain, which accounts for a 25.20% of the total patients included in the RIETE Registry. We also thank the RIETE Registry Coordinating Center, S&H Medical Science Service, for their quality control data, logistic and administrative support. We acknowledge the statistical support of Prof. Salvador Ortiz (Universidad Autónoma de Madrid) and Silvia Galindo – who both acted as both Statistical Advisors in the S&H Medical Science Service.
Author information
Authors and Affiliations
Author notes
A comprehensive list of consortium members appears at the end of the paper
Consortia
Contributions
Dr. Jara-Palomares confirms that the study objectives and procedures were honestly disclosed. L. Jara-Palomares: Study concept and design of the study; acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis and study supervision. M. Monreal: Study concept and design of the study; acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis and study supervision. M. Alfonso: Study concept and design of the study; acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content and study supervision. A. Maestre: acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content and study supervision. D. Jimenez: Acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. F. Garcia-Bragado: Acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. C. Font: Acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. C. Font: Acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. R. Lopez-Reyes: Acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. L. Hernandez Blasco: Acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. G. Vidal: Acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. R. Otero: Acquisition, analysis, or interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. RIETE investigators: critical revision of the manuscript for important intellectual content. Coordinator of the RIETE Registry: Manuel Monreal. RIETE Steering Committee Members: Paolo Prandoni, Benjamin Brenner and Dominique Farge-Bancel. RIETE National Coordinators: Raquel Barba (Spain), Pierpaolo Di Micco (Italy), Laurent Bertoletti (France), Sebastian Schellong (Germany), Inna Tzoran (Israel), Abilio Reis (Portugal), Marijan Bosevski (R. Macedonia), Henri Bounameaux (Switzerland), Radovan Malý (Czech Republic), Peter Verhamme (Belgium), Joseph A. Caprini (USA), Hanh My Bui (Vietnam). RIETE Registry Coordinating Center: S & H Medical Science Service.
Corresponding author
Ethics declarations
Competing interests
Dr. Jara-Palomares reports personal fees from Bayer Hispania, personal fees from Actelion, personal fees from Rovi, personal fees from PFIZER, personal fees from Menarini, personal fees from Leo-Pharma, outside the submitted work. Dr. Monreal reports grants from Sanofi, grants from Bayer, during the conduct of the study. All remaining authors have declared no conflicts of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jara-Palomares, L., Alfonso, M., Maestre, A. et al. Comparison of seven prognostic tools to identify low-risk pulmonary embolism in patients aged <50 years. Sci Rep 9, 20064 (2019). https://doi.org/10.1038/s41598-019-55213-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-55213-8
- Springer Nature Limited