
Abstract
This study retrospectively examined the effects of low-intensity extracorporeal shockwave therapy and tadalafil on erectile dysfunction patients. 116 patients got low-intensity extracorporeal shockwave therapy twice weekly for 3 weeks, 5 mg of tadalafil daily for 3 weeks, and adjuvant therapy for 6 months. Group A (1 year), Group B (2 years), Group C (3 years), and Group D (4+ years) were treated patients’ follow-up groups. The patients’ International Index of Erectile Function-5 (IIEF-5) scores were gathered at the start of treatment via face-to-face interviews and at the end of follow-ups by telephone conversations. IIEF-5 scores and the minimal clinically significant differences were the main outcomes. Mean follow-up length, age, and IIEF-5 scores of the patients were 2 ± 1.16 years, 47.34 ± 12.65 years, and 12.09 ± 3.66 points, respectively. Compared to baseline, treatment increased the median IIEF-5 scores of patients in groups A, B, C, and D by 7 [3–12], 6 [0–8], 7 [1–9], and 6.5 [2.5–10] points, respectively (p = 0.001). 71%, 63%, 65.8%, and 65% of treated patients in groups A, B, C, and D met the minimal clinically significant differences criteria (n = 77). Mild disease patients were 9.14 times more likely to respond to treatment than severe illness patients (OR, 9.14; 95% CI, 1.28–65.46; P = 0.02). Low-intensity extracorporeal shockwave therapy and 5 mg of tadalafil can treat erectile dysfunction for up to 4 years with sustained outcomes. This treatment is optimal for mild illnesses.
Similar content being viewed by others

Introduction
Erectile dysfunction (ED) is defined as the persistent inability to achieve or maintain penile erection sufficient for satisfactory sexual performance [1]. This condition is frequently observed in men in their forties who have vascular risk factors [2, 3], and it significantly impacts their quality of life [4]. Phosphodiesterase-5 inhibitors (PDE5Is) are the primary treatment for men with ED [5].
Nevertheless, they can cause adverse effects and reduce the frequency of natural sexual intercourse. Furthermore, other treatment modalities may be necessary as they are not effective for all ED patients [6].
The conventional treatments for ED, such as PDE5Is, vacuum devices, and intracavernous therapy, share the same limitations. Firstly, they do not address the underlying pathophysiology, unlike penile prosthesis implantation, as their effects are not permanent. Secondly, they must be applied at a suitable time before sexual intercourse. Thirdly, they are invasive, expensive, and may not be successful for some ED patients [7,8,9,10,11]. These limitations can lead to dissatisfaction among patients and treatment abandonment [12, 13]. Thus, it is essential to explore novel and effective treatment options with minimal side effects. In 2010, Vardi et al. conducted a pivotal well-designed study that demonstrated that low-intensity extracorporeal shockwave therapy (Li-ESWT) has beneficial effects and can enhance erectile function with minimal side effects [14, 15]. These findings have been corroborated by an animal study [16] and meta-analyses [17, 18]. However, the long-term effects of Li-ESWT in combination with PDE5Is on men with ED have not been adequately explored. In this retrospective, observational study, we assessed the effect of 4 years of treatment combining Li-ESWT and tadalafil on ED patients.
Materials and methods
Study design and patients
This retrospective, observational study was conducted at a single center, following the principles of the Declaration of Helsinki for research involving human subjects, and with approval from the institutional review board (approval number: ESH/GOEK2022/1). Formal informed consent was not obtained due to the retrospective nature of the study. The study enrolled 116 participants with erectile dysfunction (ED), diagnosed based on initial symptoms, medical workup results, sexual history, and International Index of Erectile Function-5 (IIEF-5) questionnaire scores [19, 20] self-reported by patients.
All patients, including those with no response to phosphodiesterase-5 inhibitors (PDE5Is) and those without psychogenic disorders, received the same treatment protocol consisting of six sessions of low-intensity extracorporeal shockwave therapy (Li-ESWT) combined with 5 mg of tadalafil daily for 3 weeks. Adjuvant therapy with 5 mg of tadalafil daily was then prescribed for 6 months. Patients were followed up and their sexual and medical histories, physical examination, and laboratory test results were recorded. No additional treatment was given to patients after the 6-month adjuvant treatment with tadalafil.
Baseline and follow-up IIEF-5 questionnaire scores were recorded for each patient, with the latter obtained via a follow-up telephone call performed by a staff member from the clinic. Patients were divided into four groups based on the interval between treatment and the telephone call: group A (1-year follow-up), group B (2 years follow-up), group C (3 years follow-up), and group D (4 years or more follow-up).
Inclusion and exclusion criteria
This trial employed the following inclusion criteria: age above 18 years, absence of prior response to PDE5Is, diagnosis of non-psychogenic ED, and an ED history of less than 6 months.
The exclusion criteria included ED arising after radiation or chemotherapy of the pelvic organs, untreated hypogonadism, and hormonal, anatomical, and/or neurological defects. Patients who did not complete all treatments and those who received concurrent psychiatric treatments were also excluded. Patients whose IIEF-5 scores and satisfaction status could not be obtained were also excluded from the study.
Details of Li-ESWT
The patients were instructed to lie in a supine position on an examination table. A standard sonographic gel was applied to the penis, without the use of local analgesics. A specialized focused shockwave probe (Omnispec ED1000; Medispe Ltd., Yehud, Israel) that produces shocks with an energy density of 0.09 mJ/m2 was used to administer shockwaves on the proximal, mid, and distal penile shaft, as well as on the right and left sides of the penis. At each of the five treatment points, three-hundred shocks were applied at a frequency of 160 shocks per minute.
Study endpoints and assessments
To evaluate ED severity, IIEF-5 scores with Turkish validation were utilized [20]. Although we did not have the IIEF-5 erectile function domain scores of the patients, we used IIEF-5 scores to detect minimal clinically important differences (MCIDs) [21]. Patients who showed clinically meaningful improvement in their IIEF-5 score at the end of the follow-up period were considered responders to treatment. Based on the baseline ED severity, increases in the IIEF-5 scores of 2 points for mild ED, 5 points for moderate ED, and 7 points for severe ED were deemed as MCIDs. In addition, overall patient satisfaction with the treatment was evaluated through yes/no questions.
Statistical methods
The Shapiro–Wilk test was utilized to assess the normality of continuous variables. Student’s t-test was employed to compare two independent groups if the data was normal, while the Mann–Whitney U test was used for non-normal data. Non-normal measurements between two-time points were compared using the Wilcoxon test. For comparing numerical data among the four groups, a one-way analysis of variance was used for normal data, and the Kruskal–Wallis test was used for non-normal data. The chi-square test was utilized to examine the relationship between categorical variables. Multivariate binary logistic regression analysis was performed to calculate the adjusted odds ratios and 95% confidence intervals, and variance inflation factors were computed to prevent multicollinearity. During the univariate analysis, variables with p < 0.10 were included in the model. Statistical analysis was conducted using SPSS for Windows (version 24.0), with a p-value of ≤0.05 indicating statistical significance.
Results
Patients
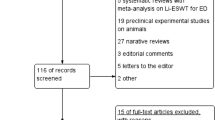
This study included 168 patients who visited our ED clinic between December 2017 and December 2021. During the screening, 52 men were excluded from the evaluation phase for various reasons, resulting in 116 patients being included in the study (Fig. 1). The study groups were comprised of 31, 27, 38, and 20 patients in groups A, B, C, and D, respectively. The patients’ median age was 47 years (range, 19–71 years), and the mean follow-up duration was 2 years (±1.16 years). Table 1 displays patient demographics and clinical characteristics, and Table 2 demonstrates that all traits assessed at baseline were homogenous in all groups.

Consort diagram.
Endpoint measures
In comparison to baseline values, treatment resulted in a significant increase in the median IIEF-5 scores by 7 points (range, 3–12 points), 6 points (range, 0–8 points), 7 points (range, 1–9 points), and 6.5 points (range, 2.5–10 points) in groups A, B, C, and D, respectively (p = 0.001). However, there were no significant differences in the changes in the median IIEF-5 scores between groups (p = 0.611) (Table 3). A clinically substantial improvement in IIEF-5 scores was observed in response to treatment (n = 77) using the MCIDs criteria, with 71%, 63%, 65.8%, and 65% of patients achieving the criteria in groups A, B, C, and D, respectively. No significant differences were observed in the proportions of patients achieving MCIDs between groups (p = 0.928) (Fig. 2). Patient satisfaction rates were 74.2%, 66.7%, 71.1%, and 80% in groups A, B, C, and D, respectively, with no notable variations between groups (p = 0.775). The response to treatment was not associated with the baseline IIEF-5 score, age, smoking status, or ED severity (p = 0.053, p = 0.082, p = 0.086, and p = 0.094, respectively) (Table 4). However, after controlling for the impact of other factors, patients with moderate ED responded to treatment 9.14 times better than those with severe ED (odds ratio, 9.14; 95% confidence interval, 1.2–0.02). No adverse effects were observed at the Li-ESWT treatment sites. Eight patients (4.76%) were unable to complete the treatment regimen due to adverse effects of tadalafil, with five experiencing back pain and three experiencing headaches.

Relationships between the treatment response and follow-up data.
Discussion
Current urological guidelines recommend PDE5Is as the first-line treatment for patients with erectile dysfunction (ED), but these drugs have limitations. First, PDE5Is have palliative and transient effects as they do not address the underlying pathology of ED. Second, PDE5Is may not be effective for patients with severe ED, despite positive outcomes in many studies. Third, adverse effects are associated with PDE5I use. Moreover, patients must plan sexual activity and take the medication in advance, which can lead to dissatisfaction and treatment discontinuation [22,23,24].
To address the limitations of PDE5Is and provide curative and non-invasive therapy for ED, low-intensity extracorporeal shockwave therapy (Li-ESWT) has gained attention in andrological practice as a promising treatment option in recent years [14]. While numerous studies report positive and long-lasting effects of Li-ESWT on the IIEF-5 erectile function domain scores, some investigations suggest that the effects may diminish over time, and the therapy may not be effective for patients with severe ED [25].
Li-ESWT has been shown to stimulate the release of angiogenic factors, such as vascular endothelial growth factor, endothelial nitric oxide synthase, and proliferating cell nuclear antigen, resulting in the promotion of tissue regeneration and neoangiogenesis, and improving the local blood supply and hemodynamics. In addition, Li-ESWT has been found to partially treat peripheral neuropathy, endothelial dysfunction, and pathological fibromuscular alterations in the corpus cavernosum [26]. Li-ESWT also enhances the synthesis of cGMP, the second messenger underlying smooth muscle relaxation required for erection [16], and its combination with PDE5Is could result in a synergistic effect to increase its influence on erectile function. Several studies have explored the effects of combining Li-ESWT with PDE5Is on IIEF-5 erectile function scores in men with ED and found that the combination is more effective than either treatment alone [27,28,29].
Our findings demonstrate a significant improvement (approximately 6 to 7 points) in median IIEF-5 scores of patients with ED who received our treatment regimen compared to baseline values of all groups, with no significant differences between groups. The improvement in median IIEF-5 scores remained stable for up to 4 years or more, and 65% of patients remained responders for this duration. Our study suggests that the long-term administration of tadalafil, both during the Li-ESWT period and as an adjuvant treatment (for 6 months), may have long-lasting beneficial effects on IIEF-5 scores. Our results suggest that the use of such a combination of Li-ESWT and PDE5Is for the treatment of ED should be investigated by well-designed clinical studies.
According to meta-analyses, patients with severe ED, hypertension, diabetes mellitus, longer ED durations, and no response to PDE5Is may not be good candidates for Li-ESWT [17, 18]. Our study found associations, although not significant, between response to treatment and baseline IIEF-5 score, age, smoking status, and ED severity. The strongest association was between ED severity and response to treatment, with a 9.14-fold higher response rate for individuals with mild ED compared to those with severe ED. Therefore, patient selection is crucial for the success of LiESWT.
Patient satisfaction rates were high among those treated with our protocol, even after 4 years, and were similar to the percentage of patients who were responders to treatment. However, further studies are needed to evaluate the long-term effects of this treatment on patient satisfaction.
It is important to note that patient safety was not compromised with only a small percentage of patients (4.76%) discontinuing treatment due to side effects caused by tadalafil. Although this study had some limitations such as the absence of a placebo group and a retrospective design, the sizable patient population and long follow-up period (4 years or more) make this study significant. Future studies should address the efficacy and safety of this combined treatment modality with larger samples and placebo-controlled designs.
Conclusions
The combination of daily 5 mg tadalafil and Li-ESWT as adjuvant therapy proved to be both safe and effective in treating ED patients who did not respond to PDE5Is. The beneficial effects of this combination persisted for at least 4 years after the last application, and the magnitude of improvement remained stable. While this treatment was effective for all patients regardless of ED severity, those with mild ED were the most suitable candidates.
Data availability
The data generated during this study can be found within the published article and its supplementary files. The additional data are available from the corresponding author upon reasonable request.
References
Consensus NIH. Conference. Impotence. NIH consensus development panel on impotence. JAMA. 1993;270:83–90.
Benet AE, Melman A. The epidemiology of erectile dysfunction. Urol Clin North Am. 1995;22:699–709.
Sullivan ME, Keoghane SR, Miller MA. Vascular risk factors and erectile dysfunction. BJU Int. 2001;87:838–45.
Salonia A, Castagna G, Saccà A, Ferrari M, Capitanio U, Castiglione F, et al. Is erectile dysfunction a reliable proxy of general male health status? The case for the international index of erectile function—erectile function domain. J Sex Med. 2012;9:2708–15.
Salonia A, Bettocchi C, Carvalho J, Corona G, Jones TH, Kadioglu A, et al. 2020 EAU guidelines on sexual and reproductive health. Arnhem: EAU Guidelines Office; 2020. https://uroweb.org/guideline/sexual-and-reproductive-health.
Yuan J, Zhang R, Yang Z, Lee J, Liu Y, Tian J, et al. Comparative effectiveness and safety of oral phosphodiesterase type 5 inhibitors for erectile dysfunction: a systematic review and network meta-analysis. Eur Urol. 2013;63:902–12.
Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, Wicker PA. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. N. Engl J Med. 1998;338:1397–404.
Porst H, Rosen R, Padma-Nathan H, Goldstein I, Giuliano F, Ulbrich E, et al. The efficacy and tolerability of vardenafil, a new, oral, selective phosphodiesterase type 5 inhibitor, in patients with erectile dysfunction: the first at-home clinical trial. Int J Impot Res. 2001;13:192–9.
Brock GB, McMahon CG, Chen KK, Costigan T, Shen W, Watkins V, et al. Efficacy and safety of tadalafil for the treatment of erectile dysfunction: results of integrated analyses. J Urol. 2002;168:1332–6.
Porst H. The rationale for prostaglandin E1 in erectile failure: a survey of worldwide experience. J Urol. 1996;155:802–15.
Kohn TP, Rajanahally S, Hellstrom WJG, Hsieh TC, Raheem OA. Global trends in prevalence, treatments, and costs of penile prosthesis for erectile dysfunction in men. Eur Urol Focus. 2022;8:803–13.
Porst H, Giuliano F, Glina S, Ralph D, Casabé AR, Elion-Mboussa A, et al. Evaluation of the efficacy and safety of once-a-day dosing of tadalafil 5mg and 10mg in the treatment of erectile dysfunction: results of a multicenter, randomized, double-blind, placebo-controlled trial. Eur Urol. 2006;50:351–9.
Mulhall JP, Jahoda AE, Ahmed A, Parker M. Analysis of the consistency of intraurethral prostaglandin E(1) (MUSE) during at-home use. Urology. 2001;58:262–6.
Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol. 2010;58:243–8.
Vardi Y, Appel B, Kilchevsky A, Gruenwald I. Does low intensity extracorporeal shock wave therapy have a physiological effect on erectile function? Short-term results of a randomized, double-blind, sham controlled study. J Urol. 2012;187:1769–75.
Aicher A, Heeschen C, Sasaki K, Urbich C, Zeiher AM, Dimmeler S. Low-energy shock wave for enhancing recruitment of endothelial progenitor cells: a new modality to increase efficacy of cell therapy in chronic hind limb ischemia. Circulation. 2006;114:2823–30.
Clavijo RI, Kohn TP, Kohn JR, Ramasamy R. Effects of low-intensity extracorporeal shockwave therapy on erectile dysfunction: a systematic review and meta-analysis. J Sex Med. 2017;14:27–35.
Lu Z, Lin G, Reed-Maldonado A, Wang C, Lee YC, Lue TF. Low-intensity extracorporeal shock wave treatment improves erectile function: a systematic review and meta-analysis. Eur Urol. 2017;71:223–33.
Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11:319–26.
Turunc T, Deveci S, Güvel S, Peşkircioğlu L. The assessment of Turkish validation with 5 question version of International Index of Erectile Function (IIEF-5). Turk J Urol. 2007;33:45–49.
Rosen RC, Allen KR, Ni X, Araujo AB. Minimal clinically important differences in the erectile function domain of the International Index of Erectile Function scale. Eur Urol. 2011;60:1010–6.
Porst H, Buvat J, Meuleman E, Michal V, Wagner G. Intracavernous Alprostadil Alfadex—an effective and well tolerated treatment for erectile dysfunction. Results of a long-term European study. Int J Impot Res. 1998;10:225–31.
Zucchi A, Costantini E, Scroppo FI, Silvani M, Kopa Z, Illiano E, et al. The first-generation phosphodiesterase 5 inhibitors and their pharmacokinetic issue. Andrology. 2019;7:804–17.
Shah T, Wang R. A review of factors affecting patient satisfaction with inflatable penile prosthesis. Sex Med Rev. 2021;9:350–7.
Kitrey ND, Vardi Y, Appel B, Shechter A, Massarwi O, Abu-Ghanem Y, et al. Low intensity shock wave treatment for erectile dysfunction-how long does the effect last. J Urol. 2018;200:167–70.
Sokolakis I, Dimitriadis F, Teo P, Hatzichristodoulou G, Hatzichristou D, Giuliano F. The basic science behind low-intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic scoping review of pre-clinical studies. J Sex Med. 2019;16:168–94.
Gallo L, Pecoraro S, Sarnacchiaro P. Adjuvant daily therapy with L-arginine 2,500 mg and tadalafil 5 mg increases efficacy and duration of benefits of low-intensity extracorporeal shock wave therapy for erectile dysfunction: a prospective, randomized, single-blinded study with 1-year follow-up. Investig Clin Urol. 2022;63:83–91.
Verze P, Capece M, Creta M, La Rocca R, Persico F, Spirito L, et al. Efficacy and safety of low-intensity shockwave therapy plus tadalafil 5 mg once daily in men with type 2 diabetes mellitus and erectile dysfunction: a matched-pair comparison study. Asian J Androl. 2020;22:379–82.
Palmieri A, Arcaniolo D, Palumbo F, Verze P, Liguori G, Mondaini N, et al. Low intensity shockwave therapy in combination with phosphodiesterase-5 inhibitors is an effective and safe treatment option in patients with vasculogenic ED who are PDE5i non-responders: a multicenter single-arm clinical trial. Int J Impot Res. 2021;33:634–40.
Author information
Authors and Affiliations
Contributions
Yurdaer Kaynak designed the study and contributed to data extraction. The study was written by Yurdaer Kaynak. Ilan Gruenwald contributed to the writing of the paper and editing. Both of them approved the final version and submitted the paper to the journal.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was done under ethical approval (approval number: ESH/GOEK2022/1).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kaynak, Y., Gruenwald, I. Long-term effects of combination treatment comprising low-intensity extracorporeal shockwave therapy and tadalafil for patients with erectile dysfunction: a retrospective study. Int J Impot Res 36, 601–606 (2024). https://doi.org/10.1038/s41443-023-00757-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41443-023-00757-7
- Springer Nature Limited