
Abstract
Gender dysphoria (GD) in children and adolescents is a condition that is characterized by an incongruence between the assigned and experienced gender. Despite the diversity in clinical presentation, literature demonstrates that GD might lead to poor mental health and high rates of co-occurring psychopathology. Due to the overlap of physical aspects as well as psychological needs in these children, a multidisciplinary approach is highly desirable. The aim of this narrative review is to give an overview of recent literature on several topics relevant in this domain. Guidelines on psychological counseling and hormonal treatment are given and challenging topics subject to controversy are explained. Furthermore, attention is drawn to the risks and protective factors in psychological functioning, including the growing evidence of a frequent co-occurrence with Autism Spectrum Disorder. Finally the psycho-sexual development in these children, the impact on fertility and fertility preservation are discussed.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
For most children, gender role expressions, behavioral interests and preferences are largely in congruence with their experience of being male or female. In contrast with gender divers children and adolescents, an incongruence between experienced gender and assigned gender can occur and is often then the origin of significant distress or gender dysphoria (GD). However, the clinical expression and psychological functioning of these children may be highly variable. International literature demonstrates convincingly that GD on the clinical spectrum in this population can lead to poor mental health and high rates of co-occurring psychopathology [1]. In the line of these observations, gender divers children and adolescents, with or without a clear GD, and their families are often in need of clinical attention, counseling and treatment [2].
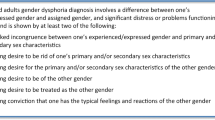
Although there has been many opposition against labeling gender diversity in diagnostic classification systems, today, GD is included in the current edition of the ‘Diagnostic and Statistical Manual of Mental Disorders (DSM 5)’ [2]. Especially in prepubescent children, the use of this classification system as such, is discussed. Opponents clearly mark the impact of stigmatization of having a mental disorder while medical interventions are still not considered. Revising the 10th version of the International Classification of Diseases and Related Health Problems (ICD-10) by the World Health Organization (WHO) in 2017, a reconceptualization of the definition and positioning of Gender Incongruence of Childhood (GIC) was included. Beek et al. collected the views of transgender individuals and professionals regarding the utility and the retention of the diagnosis [3]. The study suggests that, although in an ideal world a diagnosis is not welcomed, several participants felt the diagnosis should not be removed, likely due to concerns about restricting access to reimbursed health care. The choice for positioning of a diagnosis of GIC within the ICD-11 finally was a chapter dealing with symptoms and/or disorders regarding sexual and gender health [3]. According to the DSM-5, a diagnosis of GD in childhood can be made if gender incongruence is experienced for at least 6 months, as presented by six out of eight criteria. One dominant criterion must be ‘the feeling of a strong, insistent desire to be of another gender’. Two more criteria focus on anatomic dysphoria: a dislike of one’s sexual anatomy as such and the desire for primary/secondary sex characteristics of the experienced gender. Other criteria refer to the preference of gender roles, dressing in the preferred gender and rejection of the typical gender congruent interests. The condition must be associated with significant distress or impairment in important areas of functioning (Fig. 1).

Classification of the GD criteria according to the DSM-5. DSM Diagnostic and Statistical Manual of Mental Disorders, GD gender dysphoria.
One of the main questions which seems difficult to answer is the prevalence of childhood GD. Valid information is scarce. Earlier in the Netherlands, the Child Behavior Checklist (CBCL) was used (item 5: ‘Behaves like the opposite sex’ and item 10: ‘Wishes to be of the opposite sex’) to estimate the prevalence of gender diversity in children. The questionnaire was completed by the parents. The 5th item scored for boys versus girls 2.6% versus 5.0%, the 10th 1.4 versus 2.6%. These data should be interpreted carefully. Not only are they the result of a parent’s opinion who completed the questionnaire, which might differ from the child’s feelings; also, a sociological shift in knowledge, acceptance and recognition today may have an important impact on the replication of these items.
Another possible bias in prevalence studies, usually published by expertise centers, is the fact that only GD children and adolescents who are seeking for help in these centers are counted. We do not have a real insight in the number of young people in the general population who struggle with their gender identity and/or feel distressed about it. Neither do we know how many of them finally seek out for help, how many do not but want to and how many do not feel the need to.
Limited epidemiological data on the sex ratio exist. Steensma et al. reported on two different clinics (Amsterdam 1988–2016, Toronto; 1975–2015) and demonstrated that in both clinics, the sex ratio significantly favored assigned male at birth over assigned female at birth (Amsterdam 1,25:1; Toronto 4,33:1) with higher rates in Toronto for ages 9–12 years [4]. Clearly, by age 9–12 years, in Amsterdam, the number of birth assigned female was higher than birth assigned but not significant. Between the years 2006 to 2013, a certain shift in this sex ratio occurred in favoring birth assigned female; this was less pronounced in the Toronto clinic but still statistically significant [5]. In both clinics, children birth assigned male were referred at a significant younger age. Another study on the sex ratio in the United Kingdom demonstrated a significant higher number of birth assigned male (from 2000–2017) and not unlike the Amsterdam/Toronto results, a significant decrease was seen in the percentage of referred birth assigned male for the years 2007–2017 compared to the years 2000–2006. As expected, they were also referred at a younger age [6]. A clear scientific explanation for this shift is still lacking. We can assume that the sex difference and or alteration in the age probably reflect greater parental concerns about gender nonconforming behavior in sons compared to daughters. The observation of increasing referrals of adolescents birth assigned female is not clear, but might be explained by an earlier puberty onset in this group. Perhaps for GD adolescents assigned female, their ‘coming out’ is facilitated by less social stigmata and may result in an earlier search for counseling and/or medical treatment.
Psychological counseling and treatment of children with GD
The care for children and adolescents with gender incongruence has been changing rapidly over the past years. There is not only the growing number of specialized gender clinics [7,8,9]. Gender management clinics have emerged to assess, support and provide treatment for transgender adolescents across Europe and North America [10,11,12,13,14]. On a general basis, agreement exists on the need to diminish the distress of gender incongruent children by focusing on psychological difficulties, optimizing adjustment and well-being of the child and the family [15, 16]. The American Academy of Child & Adolescent Psychiatry has clearly stated that psychological treatment aiming to change gender nonconforming behavior is against good clinical practice [17]. However, when it comes to the prepubescent child, the best clinical practice remains often debated among professionals. We will come back on this topic later.
Despite the positive evolution, there still is a mismatch between provider education and expectations. Only a minority of the medical schools offer transgender-specific care [18]. In the next part, we will highlight 1/the guidelines regarding gender affirming treatment, but also 2/shed a light on the persisting challenges such as the social transition in young children and in addition 3/the related factors for persistence of GD.
Guidelines
The World Professional Association for Transgender Health (WPATH) first published Standards of Care for the health of gender non-conforming people in 1980 with its 7th edition in 2012 and is revising at this moment [16]. The American Psychological Association published in 2015 ‘Guidelines for psychological practice with transgender and gender nonconforming people’. These guidelines are recommendations for psychologists to assist with ‘cultural competent, developmentally appropriate and trans-affirmative psychological practice’ [19]. On the medical treatment side, the Endocrine Society (ES) recently (2017) issued clinical practice guidelines for the treatment of transgender persons, including pubertal suppression and cross-sex hormone therapy in adolescents [20]. The WPATH Standards of Care requires adolescents meet eligibility criteria before proceeding with hormone treatments. Medical interventions can be initiated after a referral from a qualified mental health professional. The ES formulated on his turn recommendations more specifically that children and adolescents with GD should be seen by a professional with training in child and adolescent developmental psychology. The mental health care professional [1] determines whether the individual fulfills DSM-5 criteria for gender dysphoria [2]; informs the individual and parents of sex reassignment and other treatments and [3] assess for potential psychopathology. An important obstacle is the lack of mental health care professionals with expertise in this area, which often results in long waiting lists, poor access to health care systems and insurance coverage issues.
Gender affirming treatment should be mitigate mental health disparities and improve outcomes. Outcome studies in children and adolescents are rather scarce. The Dutch group who were pioneers in this area of care, described results on subjective and objective well-being in adolescents who received puberty suppression and were treated by a multidisciplinary team. Significantly improvement was seen on GD and body satisfaction after treatment with cross-sex hormones and surgery, but persisted through puberty suppression. Objective well-being in adolescents after treatment with cross-sex hormone and surgery was similar compared to the general Dutch population, however, adolescents who demonstrated higher scores on this measurements were more likely to live with parents, studying or pursuing a higher education [21]. This suggests that other factors such as social integration and acceptance by family and peers influence the psychological outcome of well-being. In the same study, positive effects on feelings of anger, anxiety were seen only in participants assigned female at birth. Over time, in global functioning, clinical scores were improved in both groups birth assigned female and male.
Psychological counseling in prepubescent children and the question of persisting-desisting GD
Counseling of young children with gender variant behavior and/or gender dysphoria remains an area of debate. In general, three approaches are to be distinguished. The first position refers to a reparative therapy. It is clear that in the past, these therapies failed and are, according to WPATH, designated as unethical [16]. The second approach is often referred to as ‘watchful waiting’. Counseling implies support in dealing with ‘uncertainty’ and in providing psycho-education. In practice, the child an parents are encouraged to find a balance between accepting and a supportive attitude towards the GD, while at the same time the counseling should protect the child against any negative reactions and should remain realistic or unsure about the GD feelings in the future [22]. The third approach is the one that helps the child to build a positive self-identity and gender resilience by affirming the child’s wished gender. The rationale for supporting social transition before puberty is that these children can revert to their originally assigned gender if necessary. Critics mention that this argument cannot be decisive because to revert again might be difficult for the child, who has to make a social transition for another time. Steensma et al illustrated this in his paper on persisting and desisting GD [23]. Other critics point out that perhaps the social transition might increase the likelihood of the persistence, but scientific relevance for this is lacking.
Today this actual debate is flourishing and fundamental questions, we can poorly answer, arise: what do we know about gender identity as a developmental ‘task’ in humans? How fluid is such an identity? Who will persist in their desired gender, who will not? In a study of 53 adolescents in the Netherlands, this persisting or desisting of GD was evaluated [23]. It was clear that adolescents who experienced increased GD in early puberty stage (10–13 years) were unlikely to cease the transgender process. Also, children who persist may have more severe symptoms of GD in childhood. However, the uncertainty of future persistence, coupled with the reasoning that perhaps early social transition can lead to difficulties to reverse or even to persistence, has led to controversy regarding the appropriate counseling and mental health treatment strategies for prepubescent children with GD. In contrast, worsening of the GD beyond puberty is generally accepted as a diagnostic tool for clinicians and might be an important criterion for medical intervention [16]. Empirical answers how to counsel young prepubescent children and their families are not available. Balanced and informed care with shared decision making combined with respect for any particularity is probably the best way. Professionals together with the child and family should make a decision on which steps they agree and which particular choices are necessary to make. Psychological distress, global functioning of the child will have an important weight in this decision.
Hormonal treatment: puberty suppression and cross-sex hormone therapy
Puberty is the life stage in which developmental changes appear. Secondary sex characteristics gradually emerge together with brain development. Pulsatile gonadotropin release (GnRH) in the hypothalamus, results in the production of luteinizing hormone (LH) and follicle stimulating hormone (FSH), consequently followed by cell maturation and testicular enlargement in males and the growth of ovarian follicles in females. Clinically, the onset of puberty can be assessed by the development of testicular enlargement in boys and breast buddying in girls (Tanner stage 2). Children who experience GD, worsening in this developmental puberty stage, are eligible for medical treatment.
As mentioned earlier, the WPATH Standards of Care as well as the ES clinical practice guidelines recommend both the diagnosis of GD to be made by a mental health professional with expertise in gender identity prior to considering a hormonal intervention [16, 20]. Primary goals of the medical interventions include: (1) prevention of the development of the inconvenient biological secondary sex characteristics and (2) promotion of the development of desired secondary sex characteristics of the affirmed gender. An additional aim is to ameliorate psychological problems (anxiety, depression) so that they become less pronounced, together with the aim to enhance ability to ‘pass’ as the affirmed gender.
Hormonal interventions include puberty suppression using GnRH agonists and cross-sex hormone therapy (Fig. 2).

Left: age and/or Tanner Stage at which treatment is recommanded and applied at the pediatric gender clinic in Ghent. Right: hormonal treatment options. GD gender dysphoria, GnRH gonadotropin-releasing hormone.
Puberty suppression therapy starting at Tanner 2 stage was first developed by the pioneer center in Amsterdam [24, 25]. The rationale for using GnRH analogs to suppress puberty is clear: it allows the child and family to have more time to further explore the gender identity without the fear that irreversible sex characteristics will appear and have a potential esthetical impact in the case a transition is preferred. Starting puberty suppression prior to Tanner stage 2 is not recommended by the guidelines because persistence of GD during early puberty is an important factor in the persistence of GD in later adolescence and should be used as a diagnostic tool [16, 20].
GnRH analogs are being used in children with precocious puberty for more than 25 years and are considered to be safe and reversible [26]. In GD children, they are usually started with the intent to treat with cross-sex hormones later on in life. Importantly, the child who has started with a GnRH analog and continues with cross-sex hormone therapy will never have spermatogenesis nor menarche. Therefore, patients and families should be informed repeatedly on this and have to outweigh the risk and/or benefits of this treatment. Unfortunately, GnRH agonists are often subject to availability problems. Moreover, the cost is high and reimbursement depends on local insurance rules. Alternatively, in older children with an evolving puberty (Tanner stage 3–4) other medications as progestins and antiandrogens can reduce the production of sex hormones or inhibit their actions. They are cheap and in the case of unavailability of GnRH analogs, welcomed, even when their suppressive actions are incomplete [5, 27]. Tack et al. demonstrated that pro-androgenic and anti-androgenic progestins induce body composition changes in line with the desired appearance within 1 year of treatment [28]. Progestins can be useful in adolescents assigned female who started menstruating and have completed breast development but are too young or still in process considering starting with testosterone. Antiandrogens can be used in adolescents assigned male (Tanner 3-4) when they are worried about body and facial hair grow. The medication does not cause regression of the hair follicles, but implies often less need to shave and consequently includes better esthetic results for electrolysis therapy later on. Also, a significant reduction of spontaneous erections is often experienced as a relief.
The WPATH Standards of Care do not specify the age at with cross-sex gender affirming hormones can be administered. The ES advises to start ‘around 16 years’. The main goals are to improve general well-being and quality of life as well as to enhance the ability for adolescents to present in their experienced gender in society. In our experience, 16 years of age can be an unnecessary long time especially when gender identity is stable over time (e.g., in children with puberty suppression counseling for various years). Age 15 is than applied, other centers will even start at age 14 [10, 11]. Attention to parental consent and fertility counseling must be taken seriously and proportional. Again, a multi-interdisciplinary shared decision making is probably the best clinical practice in this.
GnRH analogs as well as pro-androgenic and anti-androgenic progestins can be continued during treatment with cross-sex hormones until gonadectomy is performed, or, in adolescents assigned female, until masculinizing chest surgery, at which point monotherapy with testosterone should be suffice to prevent menstruation.
In general, long term effects of hormonal treatment on body systems and organs in children and adolescents are sparsely studied. Few research data focused on metabolic parameters and the impact of testosterone on ovarian tissue. More recently, attention was also put on the effect of hormonal therapy on the brain, an organ abundant with androgen and estrogen receptors.
The impact of estrogen therapy in trans gender male adolescents and young adults on psychological functioning and general quality of life are not conclusive to be negative. The study done by de Vries et al. in which the outcome was investigated in a follow up study with participants who received puberty suppression, showed stable or slightly more symptomatology on the measures of anger and anxiety, but improved on the total T scores of the Child behavior checklist or Adult behavior checklist (CBCL/ABCL) [21].
In transgender children, the intake of GnRH analogs might include a risk of a reduction in bone mineral density z-score during treatment. Also, bone health, especially at the lumbar spine, was found to be severely affected by androgen suppressive therapy [28]. However, scarce evidence suggested bone density accrual might improve after starting treatment with cross-sex hormones [25, 29]. Another important issue regarding the use of GnRH analogs is the underdevelopment of the penis, which might compromise future vaginoplasy [9].
The brain is clearly influenced by endogenous levels of sex hormones which can be observed during puberty and the menstrual cycle e.g. [30]. Adult brain studies in trans persons before and after several months of hormone treatment showed that estrogen plus anti-androgen treatment (in assigned male) is associated with a decrease in volume towards ‘female proportions’; the ventricles were seen to increase in volume [31]. Moreover, testosterone treatment (in assigned female) resulted in increased total brain and hypothalamus volumes. Identical results were found by Zubiaurre-Elorza et al. [32]. These changes were suggested to be caused by the anabolic effects of testosterone, while the opposite decrease and expansion of the ventricles might be due to the suppression of normal anabolic effects of testosterone by the anti-androgens and the deleterious effects of estradiol [32]. Testosterone treatment also was demonstrated to effect white matter microstructure [33]. Information about the impact of GnRH analogs (suppressing puberty) on specific brain structures in prepubescent children is not available.
Cross sex hormone therapy was shown to be safe regarding metabolic and cardiovascular parameters on the short-term [34]. Data from adolescents between 14 and 25 years were collected in 4 clinics in the US. Recorded blood pressure, BMI, testosterone, estradiol, prolactin, lipids, electrolytes, liver function test, hemoglobin/hematocrit and hemoglobin A1c were reviewed. Data were collected until 6 months of cross sex hormone therapy and supported the short-term safety of this treatment in GD adolescents. A review of cross sex hormone therapy in adults, also mentioned an insufficient follow-up duration to make clear conclusions of cardio-metabolic effects from cross sex hormone therapy. Most data are retrospective but are comforting. However, in (older, >40 years) transgender women, transdermal patches or gel (or parenteral estrogen injections if available) may be safer with regard to triglycerides and clotting risk than oral oestradiol by passing hepatic metabolism, but randomized controlled trials comparing these formulae are not available. Smoking and the use of synthetic etinyl oestradiol (which is no longer used) on the contrary, were risk factors [35, 36].
In the past century, investigators reported that the androgen-exposed ovaries of transgender males showed polycystic ovary (PCO) syndrome-like features, that is: a thickened ovarian cortex and marked collagenization, with a greater number of cystic (atretic) follicles in the ovarian stroma. Recent studies replicated these findings in drug naive transgender male persons without PCO and found, to some extent, similar results after testosterone administration [37, 38]. A novel technique, texture profile analysis of the ovarian cortex of transgender males, was compared with the ovarian cortex of oncological patients and concluded that the superficial part of cortex appeared to be significantly stiffer in the trans group [39]. It is clear that long term follow up and more research is necessary to comprehend the complete impact of cross sex hormone therapy in trans people.
Psychological well-being and co-existing problems in children and adolescents with GD
Children with GD are considered to be a more vulnerable group regarding psychological problems and generally report higher rates of mental health difficulties. The occurrence of behavioral and emotional problems in this group has been measured in several studies [40,41,42,43,44]. The absolute scores on questionnaires or answers on diagnostic interviews are interesting, but unfortunately most of them do not include a control population.
However, in Canada, a large well-designed randomized case control study was performed in which 923 transgender youth were recruited and asked about different aspects concerning their mental health: emotional distress, suicidality, self-harm and general mental health [45]. The results were striking: mental health disparities were significantly higher for transgender youth, compared with the general population-based estimates. Transgender youth between 14 and 18-years old had five times the risk of suicidal thoughts and 79.2% reported self-harming in the past year. Remarkably is the finding that non-binary youth consistently reported even worse mental health on average than trans adolescents. Another American retrospective observational cohort study, compared 180 transgender youth (aged 12–29) to a cisgender control group. Compared to cisgender matched controls, transgender participants had a two- to three-fold increased risk of depression, anxiety disorder, suicidal ideation, suicide attempt, self-harm without lethal intent, and both inpatient and outpatient mental health treatment [46].
The question how these findings of being at high risk to report mental health difficulties in GD youth can be understood, was answered by other studies showing that the effect is largely mediated through social (in)tolerance toward gender variant, gender non-congruent behavior and identity [47,48,49,50]. De Vries et al. concluded that the ‘Peer Relations Scale’ was the strongest predictor of both the CBCL and YSR ‘Total Problem Score’. Other variables with a positive correlation were a lower IQ and a lower socioeconomic background [51].
A cross-international comparison study examining psychological functioning in gender diverse adolescents across Europe was published in 2018 [52]. All adolescents aged 12–18 who were referred to one of the four European specialist gender clinics (Amsterdam, Ghent, Zurich and London) were included. Data from the CBCL and the YSR were analyzed. A similar pattern was found across the different clinics. A notable finding was that birth assigned girls reported more total problems and externalizing problems in the clinical range than the birth assigned boys. In the previous discussed study, birth assigned girls also reported a significantly higher externalizing problem score (although not in the clinical range) [51]. The hypothesis of a general pattern of an “inversion” of internalizing vs. externalizing problems in relation to the sex-typical pattern of more internalizing problems in girls and more externalizing problems in boys thus seems plausible, but further research is needed. Not unlike the previous findings of De Vries et al., a positive correlation between the Peer Relation Scale and both the CBCL and YSR was found here [51]. Across the four clinics, the highest prevalence of problem scores was found in the UK, the least problems were reported by the Dutch adolescents. Most likely, these differences can be explained by a difference in tolerance and acceptance of gender variance in the Dutch culture on the one hand and differences in the availability of GnRH treatment in the UK on the other hand until 2011.
The co-occurrence of GD and Autism
There is growing evidence concerning co-occurrence and/or overlap between GD and Autism Spectrum Disorder (ASD). The DSM-5 core criteria for an ASD diagnosis include significant impairments in social communication and interaction and restricted, repetitive patterns of behaviors, specific interests or activities. Most studies in this area examine the presence of ASD in GD populations [10, 53, 54]. The converse approach, investigating GD symptoms within an ASD population has also been used [55,56,57].
In a recent Dutch study, a sample of 542 children and adolescents with GD were investigated and compared to two groups from a normative study: 196 children and adolescents with ASD and 2507 TD (Typical Developing) children and adolescents. The Children’s Social Behavior Questionnaire (CSBQ) was used to investigate symptoms of ASD and was completed by parents or caregivers. On average, the scores of the children and adolescents with GD were all in between the scores of TD children and adolescents and those diagnosed with ASD. There was no main effect of assigned gender at birth nor a group by gender interaction effect [58].
In a second, international study, the association between gender variance (GV) and ASD was explored in a group of 2245 children between the age of 6 and 12 years of age [59]. In an online questionnaire parents were asked if their children had received a developmental/mental health diagnosis from a healthcare professional and were asked to complete both the Gender Identity Questionnaire for Children (GIQC) and the CSBQ. A positive association between characteristics of ASD and GV in this nonclinical sample was found. This indicates that the association exists beyond the clinical domain. Furthermore, children with ASD showed significantly higher level of parent-reported GV compared to the reference group of children without reported clinical diagnosis [59]. This finding is thus in line with the previous mentioned study [58].
These studies confirm the bidirectional assumption that, not only children and adolescents with GD show more symptoms of ASD, but also that children with ASD show a higher level of reported GV in comparison to children without a reported diagnosis. However, concerns were expressed by some authors, about the specificity of using screening instruments to search for ASD symptoms instead of a confirmed ASD diagnosis on the one hand and search for GV symptoms rather than the real gender identity or confirmed GD on the other hand [60]. Even more, they critically state that sound underlying evidence for a GD-ASD link is currently still lacking. This publication led to a heated debate between several authors in this search field. Even when holding stigma and sexual minority stress into account as possible explanations for social difficulties individuals with GD, elevations on all of the subdomains of ASD were found, van der Miesen at al responded [61]. Strang et al. at their turn, reacted by referring to 7 studies where clinical ASD diagnosis rates were 4,1 to 17,5 times more common than in the general population and stated that these findings are directly contradicting the argument that the reported over-occurrence of ASD in gender-diverse individuals is due to nonspecific ASD measures [62].
Several suggestions on how the understand the link between GD and ASD have been formulated but remain hypothetical [53, 63, 64]. As for now, causal relations between the two conditions cannot be withheld at this moment and further research is recommended.
Because of the fact that the co-occurrence of GD and ASD in adolescents is often complex and includes significant diagnostic and treatment challenges, specific guidelines for the assessment and care are needed. Initial guidelines were published and are provided in Fig. 3 [65]. The importance of screening for ASD among gender referrals and the importance of screening for gender issues among ASD referrals was one of the main recommendations. There is also a clear statement that the diagnosis of ASD should not exclude an adolescent from also receiving a GD diagnosis and, when indicated, appropriate GD treatment.

Fertility and psychosexual development in adolescents with GD
People with GD who are treated, either medically or surgically, are at risk for infertility [37, 66, 67]. Information should be provided early in the transition process which effects of treatment can be expected. Information about fertility preservation (FP) should be available. Additionally, it is interesting to understand how children and adolescents with GD judge fertility issues.
Pubertal suppression with GnRH analogs is reversible, but it does pause the maturation of germ cells, and this could affect fertility potential [68,69,70]. The long-term effects of gender affirming hormone therapy with testosterone on future fertility are unknown. Literature does not provide uniform results. Polycystic ovarian morphology was found whereas preservation of normal cortical follicle distribution was documented as well [71, 72]. The same conflicting results apply for estrogen therapy [73, 74]. The WPATH recommends counseling regarding fertility and reproductive options before initiating hormonal treatment [16]. Cryopreservation of oocytes or embryos for adolescents assigned female or cryopreservation of sperm or embryos for those assigned male can be applied. For prepubescent children and adolescents who opt for FP before initiating hormonal therapy, the option of ovarian tissue or testicular tissue cryopreservation is still experimental [68, 75, 76].
Two different studies looked at the utilization rates of FP in transgender adolescents [77, 78]. In both studies, the authors concluded that these rates were low. Chen et al. reported 13 out of 105 transgender adolescents who were seen in formal consultation of FP before initiating hormone treatment. Five completed the FP process (four sperm and one oocyte cryopreservation) [77]. Nahata et al. reported only 2 out of 72 patients having attempted fertility preservation [78]. In adult studies, 51% of the birth assigned male say that they would have considered sperm banking if it had been offered, and 37.5% of the birth assigned female would have considered freezing germ cells [79, 80]. This discrepancy does raise questions as how many transgender youth change their perspectives about FP later in life and which barriers exist for using FP: invasiveness and/or costs of the procedures, a sense of urgency to move forward with the medical transition [77, 78]? Further research to examine the reproductive desires and attitudes regarding fertility preservations is needed. The “Transgender Youth Fertility Attitudes Questionnaire” was recently developed by Strang et al. [81]. The study builds on existent approaches and measures developed to assess fertility attitudes in youth with cancer and their parents [82,83,84]. In a pilot trial, more than 50% of the trans adolescents indicated the wish to have children, 24% expressed the desire to have their own biological child. Many wondered or did not know if their feelings about having a biological child might change in the future.
Little is known about the sexual development process in youth with GD. A study in the Netherlands was conducted to evaluate sexual and romantic experiences in adolescents with GD compared with a matched cisgender control group [85]. In the GD group gender differences were not observed for falling in love and romantic relationships, but adolescents assigned female at birth were more experienced in the areas of sexual fantasies, french kissing and petting while undressed. Adolescents birth assigned male however were more experienced in sexual intercourse. With respect to self-defining their sexual orientation, 27% of the participants assigned male and 44% of the assigned female reported defining themselves as heterosexual whereas 50% of the assigned male group and 43% of the assigned female group describe themselves as undecided. Compared with the control group, adolescents with GD had less sexual experience, 44% chose “being ashamed of my own body” as a reason not to have intercourse. Of the sexually active transgender adolescents, 50% reported not involving their genitals. These results doubtless underline the importance of appropriate sexual counseling for this young people.
References
Alberse AE, de Vries AL, Elzinga WS, Steensma TD. Self-perception of transgender clinic referred gender diverse children and adolescents. Clin Child Psychol Psychiatry. 2019;24:388–401.
Association AP. Diagnostic and statistical manual of mental disorders (5th ed.). 2013.
Beek TF, Cohen-Kettenis PT, Bouman WP, de Vries AL, Steensma TD, Witcomb GL, et al. Gender incongruence of childhood: clinical utility and stakeholder agreement with the World Health Organization’s proposed ICD-11 criteria. PLoS ONE 2017;12:e0168522.
Steensma TD, Cohen-Kettenis PT, Zucker KJ. Evidence for a change in the sex ratio of children referred for gender dysphoria: data from the center of expertise on gender dysphoria in Amsterdam (1988-2016). J Sex Marital Ther. 2018;44:713–5.
Aitken M, Steensma TD, Blanchard R, VanderLaan DP, Wood H, Fuentes A, et al. Evidence for an altered sex ratio in clinic-referred adolescents with gender dysphoria. J Sex Med. 2015;12:756–63.
de Graaf NM, Carmichael P, Steensma TD, Zucker KJ. Evidence for a change in the sex ratio of children referred for gender dysphoria: data from the gender identity development service in London (2000–2017). J Sex Med. 2018;15:1381–3.
Hsieh S, Leininger J. Resource list: clinical care programs for gender-nonconforming children and adolescents. Pediatr Ann 2014;43:238–44.
Kaltiala-Heino R, Sumia M, Tyolajarvi M, Lindberg N. Two years of gender identity service for minors: overrepresentation of natal girls with severe problems in adolescent development. Child Adolesc Psychiatry Ment Health. 2015;9:9.
Khatchadourian K, Amed S, Metzger DL. Clinical management of youth with gender dysphoria in Vancouver. J Pediatr 2014;164:906–11.
Spack NP, Edwards-Leeper L, Feldman HA, Leibowitz S, Mandel F, Diamond DA, et al. Children and adolescents with gender identity disorder referred to a pediatric medical center. Pediatrics 2012;129:418–25.
Rosenthal SM. Approach to the patient: transgender youth: endocrine considerations. J Clin Endocrinol Metab. 2014;99:4379–89.
Sherer I, Rosenthal SM, Ehrensaft D, Baum J. Child and Adolescent Gender Center: a multidisciplinary collaboration to improve the lives of gender nonconforming children and teens. Pediatr Rev 2012;33:273–5.
de Vries AL, Cohen-Kettenis PT. Clinical management of gender dysphoria in children and adolescents: the Dutch approach. J Homosex. 2012;59:301–20.
Zucker KJ, Bradley SJ, Owen-Anderson A, Kibblewhite SJ, Cantor JM. Is gender identity disorder in adolescents coming out of the closet? J Sex Marital Ther. 2008;34:287–90.
Byne W, Bradley SJ, Coleman E, Eyler AE, Green R, Menvielle EJ, et al. Report of the American Psychiatric Association Task Force on treatment of gender identity disorder. Arch Sex Behav. 2012;41:759–96.
Coleman E, Bockting W, Botzer M, Cohen-Kettenis P, DeCuypere G, Feldman J, et al. Standards of care for the health of transsexual, transgender, and gender-nonconforming people, Version 7. Int J Transgenderism. 2012;13:165–232.
Adelson SL. Practice parameter on gay, lesbian, or bisexual sexual orientation, gender nonconformity, and gender discordance in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2012;51:957–74.
Obedin-Maliver J, Goldsmith ES, Stewart L, White W, Tran E, Brenman S, et al. Lesbian, gay, bisexual, and transgender-related content in undergraduate medical education. JAMA 2011;306:971–7.
Association A. Guidelines for psychological practice with transgender and gender nonconforming people. Am Psychologist 2015;70:832–64.
Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an endocrine society clinical practice guideline. Endocr Pract 2017;23:1437.
de Vries AL, McGuire JK, Steensma TD, Wagenaar EC, Doreleijers TA, Cohen-Kettenis PT. Young adult psychological outcome after puberty suppression and gender reassignment. Pediatrics 2014;134:696–704.
Drescher J. Controversies in gender diagnoses. LGBT Health. 2014;1:10–4.
Steensma TD, Biemond R, de Boer F, Cohen-Kettenis PT. Desisting and persisting gender dysphoria after childhood: a qualitative follow-up study. Clin Child Psychol Psychiatry. 2011;16:499–516.
Cohen-Kettenis PT, van Goozen SH. Pubertal delay as an aid in diagnosis and treatment of a transsexual adolescent. Eur Child Adolesc Psychiatry. 1998;7:246–8.
Delamarre-van der Waal H, Cohen-Kettenis P. Clinical management of gender identity disorder in adolescents: a protocol on psychological and paediatric endocrinology aspects. Eur J Endocrinol. 2006;155:131–7.
Boepple PA, Mansfield MJ, Wierman ME, Rudlin CR, Bode HH, Crigler JF Jr., et al. Use of a potent, long acting agonist of gonadotropin-releasing hormone in the treatment of precocious puberty. Endocr Rev 1986;7:24–33.
Tack LJ, Craen M, Dhondt K, Vanden Bossche H, Laridaen J, Cools M. Consecutive lynestrenol and cross-sex hormone treatment in biological female adolescents with gender dysphoria: a retrospective analysis. Biol Sex Differ. 2016;7:14.
Tack LJW, Craen M, Lapauw B, Goemaere S, Toye K, Kaufman JM, et al. Proandrogenic and antiandrogenic progestins in transgender youth: differential effects on body composition and bone metabolism. J Clin Endocrinol Metab. 2018;103:2147–56.
Klink D, Caris M, Heijboer A, van Trotsenburg M, Rotteveel J. Bone mass in young adulthood following gonadotropin-releasing hormone analog treatment and cross-sex hormone treatment in adolescents with gender dysphoria. J Clin Endocrinol Metab. 2015;100:E270–5.
Kreukels BP, Guillamon A. Neuroimaging studies in people with gender incongruence. Int Rev Psychiatry. 2016;28:120–8.
Hulshoff Pol H, Cohen-Kettenis P, Haren NEM, Peper J, Brans R, Cahn W, et al. Changing your sex changes your brain: Influences of testosterone and estrogen on adult human brain structure. Eur J Endocrinol. 2006;155:107–14.
Zubiaurre-Elorza L, Junque C, Gomez-Gil E, Segovia S, Carrillo B, Rametti G, et al. Cortical thickness in untreated transsexuals. Cereb Cortex. 2013;23:2855–62.
Rametti G, Carrillo B, Gomez-Gil E, Junque C, Zubiaurre-Elorza L, Segovia S, et al. Effects of androgenization on the white matter microstructure of female-to-male transsexuals. A diffusion tensor imaging study. Psychoneuroendocrinology. 2012;37:1261–9.
Jarin J, Pine-Twaddell E, Trotman G, Stevens J, Conard LA, Tefera E, et al. Cross-sex hormones and metabolic parameters in adolescents with gender dysphoria. Pediatrics. 2017;139:e20163173. https://doi.org/10.1542/peds.2016-3173.
Iwamoto SJ, Defreyne J, Rothman MS, Van Schuylenbergh J, Van de Bruaene L, Motmans J, et al. Health considerations for transgender women and remaining unknowns: a narrative review. Ther Adv Endocrinol Metab. 2019;10:2042018819871166.
Defreyne J, Van de Bruaene LDL, Rietzschel E, Van Schuylenbergh J, T’Sjoen GGR. Effects of gender-affirming hormones on lipid, metabolic, and cardiac surrogate blood markers in transgender persons. Clin Chem. 2019;65:119–34.
Ikeda K, Baba T, Noguchi H, Nagasawa K, Endo T, Kiya T, et al. Excessive androgen exposure in female-to-male transsexual persons of reproductive age induces hyperplasia of the ovarian cortex and stroma but not polycystic ovary morphology. Hum Reprod. 2013;28:453–61.
Baba T, Endo T, Honnma H, Kitajima Y, Hayashi T, Ikeda H, et al. Association between polycystic ovary syndrome and female-to-male transsexuality. Hum Reprod. 2007;22:1011–6.
De Roo C, Tilleman K, Vercruysse C, Declercq H, T’Sjoen G, Weyers S, et al. Texture profile analysis reveals a stiffer ovarian cortex after testosterone therapy: a pilot study. J Assist Reprod Genet. 2019;36:1837–43.
de Vries ALC, Steensma TD, Doreleijers TAH, Cohen-Kettenis PT. Puberty suppression in adolescents with gender identity disorder: a prospective follow-up study. J Sex Med. 2011;8:2276–83.
Steensma TD, Zucker KJ, Kreukels BPC, Vanderlaan DP, Wood H, Fuentes A, et al. Behavioral and emotional problems on the Teacher’s Report Form: a cross-national, cross-clinic comparative analysis of gender dysphoric children and adolescents. J Abnorm Child Psychol. 2014;42:635–47.
Cohen-Kettenis PT, Owen A, Kaijser VG, Bradley SJ, Zucker KJ. Demographic characteristics, social competence, and behavior problems in children with gender identity disorder: a cross-national, cross-clinic comparative analysis. J Abnorm Child Psychol. 2003;31:41–53.
de Vries ALC, Doreleijers TAH, Steensma TD, Cohen-Kettenis PT. Psychiatric comorbidity in gender dysphoric adolescents. J Child Psychol Psychiatry. 2011;52:1195–202.
Wallien MSC, Swaab H, Cohen-Kettenis PT. Psychiatric comorbidity among children with gender identity disorder. J Am Acad Child Adolesc Psychiatry. 2007;46:1307–14.
Veale JF, Watson RJ, Peter T, Saewyc EM. Mental health disparities among Canadian transgender youth. J Adolesc Health. 2017;60:44–9.
Reisner SL, Vetters R, Leclerc M, Zaslow S, Wolfrum S, Shumer D, et al. Mental health of transgender youth in care at an adolescent urban community health center: a matched retrospective cohort study. J Adolesc Health. 2015;56:274–9.
Carter B, McCloskey L A. LM. Peers and the maintenance of sex-typed behavior: the development of children’s conceptions of cross-gender behavior in their peers. Soc Cogn. 1984;2:294–314.
Levy GD, Taylor MG, Gelman SA. Traditional and evaluative aspects of flexibility in gender roles, social conventions, moral rules, and physical laws. Child Dev. 1995;66:515–31.
Liben LS, Signorella ML. Gender-schematic processing in children: the role of initial interpretations of stimuli. Dev Psychol. 1993;29:141–9.
Stoddart T, Turiel E. Children’s concepts of cross-gender activities. Blackwell Publishing; 1985. p. 1241–52.
de Vries AL, Steensma TD, Cohen-Kettenis PT, VanderLaan DP, Zucker KJ. Poor peer relations predict parent- and self-reported behavioral and emotional problems of adolescents with gender dysphoria: a cross-national, cross-clinic comparative analysis. Eur Child Adolesc Psychiatry. 2016;25:579–88.
de Graaf NM, Cohen-Kettenis PT, Carmichael P, de Vries ALC, Dhondt K, Laridaen J, et al. Psychological functioning in adolescents referred to specialist gender identity clinics across Europe: a clinical comparison study between four clinics. Eur Child Adolesc Psychiatry. 2018;27:909–19.
de Vries AL, Noens IL, Cohen-Kettenis PT, van Berckelaer-Onnes IA, Doreleijers TA. Autism spectrum disorders in gender dysphoric children and adolescents. J Autism Dev Disord. 2010;40:930–6.
Skagerberg E, Di Ceglie D, Carmichael P. Brief report: autistic features in children and adolescents with gender dysphoria. J Autism Dev Disord. 2015;45:2628–32.
Strang JF, Kenworthy L, Dominska A, Sokoloff J, Kenealy LE, Berl M, et al. Increased gender variance in autism spectrum disorders and attention deficit hyperactivity disorder. Arch Sex Behav. 2014;43:1525–33.
Janssen A, Huang H, Duncan C. Gender variance among youth with autism spectrum disorders: a retrospective chart review. Transgend Health 2016;1:63–8.
May T, Pang K, Williams KJ. Gender variance in children and adolescents with autism spectrum disorder from the National Database for Autism Research. Int J Transgenderism. 2017;18:7–15.
van der Miesen AIR, de Vries ALC, Steensma TD, Hartman CA. Autistic symptoms in children and adolescents with gender dysphoria. J Autism Dev Disord. 2018;48:1537–48.
Nabbijohn AN, van der Miesen AIR, Santarossa A, Peragine D, de Vries ALC, Popma A, et al. Gender variance and the autism spectrum: an examination of children ages 6-12 years. J Autism Dev Disord. 2019;49:1570–85.
Turban JL, van Schalkwyk GI. “Gender Dysphoria” and autism spectrum disorder: is the link real? J Am Acad Child Adolesc Psychiatry. 2018;57:8–9.e2.
van der Miesen AIR, Cohen-Kettenis PT, de Vries ALC. Is there a link between gender dysphoria and autism spectrum disorder? J Am Acad Child Adolesc Psychiatry. 2018;57:884–5.
Strang JF, Janssen A, Tishelman A, Leibowitz SF, Kenworthy L, McGuire JK, et al. Revisiting the link: evidence of the rates of autism in studies of gender diverse individuals. J Am Acad Child Adolesc Psychiatry. 2018;57:885–7.
Baron-Cohen S. The extreme male brain theory of autism. Trends Cogn Sci. 2002;6:248–54.
Parkinson J. Gender dysphoria in Asperger’s syndrome: a caution. Australas Psychiatry 2014;22:84–5.
Strang JF, Meagher H, Kenworthy L, de Vries ALC, Menvielle E, Leibowitz S, et al. Initial clinical guidelines for co-occurring autism spectrum disorder and gender dysphoria or incongruence in adolescents. J Clin Child Adolesc Psychol. 2018;47:105–15.
Pache TD, Chadha S, Gooren LJ, Hop WC, Jaarsma KW, Dommerholt HB, et al. Ovarian morphology in long-term androgen-treated female to male transsexuals. A human model for the study of polycystic ovarian syndrome? Histopathology 1991;19:445–52.
Schulze C. Response of the human testis to long-term estrogen treatment: morphology of Sertoli cells, Leydig cells and spermatogonial stem cells. Cell Tissue Res. 1988;251:31–43.
Finlayson C, Johnson EK, Chen D, Dabrowski E, Gosiengfiao Y, Campo-Engelstein L, et al. Proceedings of the working group session on fertility preservation for individuals with gender and sex diversity. Transgend Health 2016;1:99–107.
Johnson EK, Finlayson C. Preservation of fertility potential for gender and sex diverse individuals. Transgend Health 2016;1:41–4.
Hagen CP, Sorensen K, Anderson RA, Juul A. Serum levels of antimullerian hormone in early maturing girls before, during, and after suppression with GnRH agonist. Fertil Steril 2012;98:1326–30.
Grynberg M, Fanchin R, Dubost G, Colau JC, Bremont-Weil C, Frydman R, et al. Histology of genital tract and breast tissue after long-term testosterone administration in a female-to-male transsexual population. Reprod Biomed Online. 2010;20:553–8.
De Roo C, Lierman S, Tilleman K, Peynshaert K, Braeckmans K, Caanen M, et al. Ovarian tissue cryopreservation in female-to-male transgender people: insights into ovarian histology and physiology after prolonged androgen treatment. Reprod Biomed Online. 2017;34:557–66.
Kent MA, Winoker JS, Grotas AB. Effects of feminizing hormones on sperm production and malignant changes: microscopic examination of post orchiectomy specimens in transwomen. Urology 2018;121:93–6.
Schneider F, Kliesch S, Schlatt S, Neuhaus N. Andrology of male-to-female transsexuals: influence of cross-sex hormone therapy on testicular function. Andrology. 2017;5:873–80.
Wyns C, Curaba M, Vanabelle B, Van Langendonckt A, Donnez J. Options for fertility preservation in prepubertal boys. Hum Reprod Update. 2010;16:312–28.
Donnez J, Dolmans MM. Ovarian cortex transplantation: 60 reported live births brings the success and worldwide expansion of the technique towards routine clinical practice. J Assist Reprod Genet. 2015;32:1167–70.
Chen D, Simons L, Johnson EK, Lockart BA, Finlayson C. Fertility preservation for transgender adolescents. J Adolesc Health. 2017;61:120–3.
Nahata L, Tishelman AC, Caltabellotta NM, Quinn GP. Low fertility preservation utilization among transgender youth. J Adolesc Health. 2017;61:40–4.
Sutter P, Kira K, Verschoor A, Hotimsky A. The desire to have children and the preservation of fertility in transsexual women: A survey. Int J Transgend. 2002;6:215–21.
Wierckx K, Van Caenegem E, Pennings G, Elaut E, Dedecker D, Van de Peer F, et al. Reproductive wish in transsexual men. Hum Reprod 2012;27:483–7.
Strang JF, Jarin J, Call D, Clark B, Wallace GL, Anthony LG, et al. Transgender youth fertility attitudes questionnaire: measure development in nonautistic and autistic transgender youth and their parents. J Adolesc Health. 2018;62:128–35.
Wenzel L, Dogan-Ates A, Habbal R, Berkowitz R, Goldstein DP, Bernstein M, et al. Defining and measuring reproductive concerns of female cancer survivors. J Natl Cancer Inst Monogr. 2005;34:94–8.
Quinn GP, Murphy D, Wang H, Sawczyn KK, Knapp C. Having cancer does not change wanting a baby: healthy adolescent girls’ perceptions of cancer-related infertility. J Adolesc Health. 2013;52:164–9.
Meneses K, McNees P, Azuero A, Jukkala A. Development of the fertility and cancer project: an internet approach to help young cancer survivors. Oncol Nurs Forum. 2010;37:191–7.
Bungener SL, Steensma TD, Cohen-Kettenis PT, de Vries ALC. Sexual and romantic experiences of transgender youth before gender-affirmative treatment. Pediatrics. 2017;139:e20162283. https://doi.org/10.1542/peds.2016-2283.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Baetens, L., Dhondt, K. Psychosocial challenges and hormonal treatment in gender diverse children and adolescents. A narrative review. Int J Impot Res 33, 217–227 (2021). https://doi.org/10.1038/s41443-020-0291-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41443-020-0291-z
- Springer Nature Limited
This article is cited by
-
The role of the pediatrician in the management of the child and adolescent with gender dysphoria
Italian Journal of Pediatrics (2023)
-
Out of the dark, into the light: sexuality and fertility in pediatric urological conditions
International Journal of Impotence Research (2021)