
Abstract
Objectives
Optic nerve sheath meningioma (ONSM) is a rare benign tumour that accounts for approximately 2% of all orbital tumours. Radiotherapy has gradually become an important treatment for ONSM because of its good effect in preserving or improving vision. We aimed to explore the effect of radiotherapy on tumour control and vision preservation/improvement in patients with ONSM.
Methods
Forty-three patients with primary ONSM treated in our institution from 2015 to 2021 were enrolled. The irradiation dose was from 50.4 to 54 Gy with 28–30 fractions. We evaluated the tumour volume on MRI or CT, and visual acuity before and after the radiotherapy.
Results
Thirty-four patients (79%) experienced a vision decrease at diagnosis. The mean duration of follow-up was 54.1 months (ranges: 18–93, median: 56). Among 25 patients who had tumour evaluation using MRI, 16 patients (37.2%) showed stable tumours, 7 patients (16.3%) had tumour shrinkage, but 2 patients (4.7%) experienced tumour progression. Among the 39 patients performing vision acuity evaluation, 16 patients (37.2%) had vision improvement or recovery. 16 of the 23 patients without vision improvement demonstrated severe visual loss at diagnosis. Two patients had evidence of tumour progression during the follow-up. Additionally, 4 (10.2%) patients had dry eyes, 7 (17.9%) patients experienced watery eyes, and 3 (7.7%) patients had eye swelling. Patients with vision loss for more than 12 months had a lower possibility of vision recovery than those with vision loss for less than 12 months.
Conclusions
Radiotherapy such as IMRT, VMAT, and 3D-CRT plays an important role in the treatment of ONSM. The probability of vision recovery is lower in patients with severe vision loss at diagnosis or the duration of vision loss is more than 12 months.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Optic nerve sheath meningioma (ONSM) is a rare meningeal tumour that accounts for approximately 2% of all orbital tumours [1]. The mean age of presentation with ONSM is around 40 years old (42.5 for females and 36.1 for males, range 3-80), and ONSM usually occurs in females (61%). Symptoms of ONSM include painless vision loss, proptosis, visual field defects, afferent pupillary defects, colour blindness, optic disc oedema, and ocular motility disorders [2, 3]. MRI is currently regarded as the gold standard for diagnosis of ONSM, and the double-track sign is the typical characteristic [3, 4]. As the optic nerve is easily impaired by radiotherapy and surgery, treatment of primary ONSM remains a challenge. Adeberg et al. [5] demonstrated that up to 94% of patients had postoperative visual loss due to the impaired vascular supply to optic nerve. Meningioma shows characteristic indolent growth, management therefore should be conservative in most cases. Radiotherapy is indicated in patients with progressive visual deterioration [6]. Radiation therapy is a non-invasive alternative to surgery and is proved to be highly effective in tumour control for ONSM [7]. New radiation therapies such as spatially-fractionated radiation therapy (SFRT), volumetric-modulated arc therapy (VMAT), intensity-modulated radiation therapy (IMRT), stereotactic radiosurgery (SRS), and proton-beam therapy (PBT) have fewer complications compared to the two-dimensional radiation therapy (2D-RT) and three-dimensional conformal radiation therapy (3D-CRT) [8, 9]. Increasing studies have recommended radiotherapy as the first-line therapy for ONSM regardless of initial clinical symptoms [10]. SFRT, VMAT, IMRT, SRS, and PBT have identical treatment outcomes in tumour control and visual acuity preservation with no significant differences in complication rates and can be recommended for clinical practice [4, 7]. There are few reports on vision recovery and its impact factor after radiotherapy in ONSM. Hence, we conducted a retrospective study of the efficacy of radiation therapy in patients with ONSM, and the factors related to visual acuity improvement were explored.
Method and materials
Patient selection
Forty-three patients with ONSM who underwent radiotherapy were enrolled in this study at Eye & ENT Hospital, Fudan University, between 2015 and 2021. Magnetic resonance is an excellent diagnostic criterion for ONSM, and we use different sequences to differentiate ONSM from inflammation of the optic nerve. ONSM shows isointense on flat scans of MRI and high signal on enhancement, whereas some inflammatory diseases often do not have a difference in the signal before and after enhancement. On the other hand, the clinical presentation of the two diseases is different. Inflammatory diseases often show ocular pain, and the signs and symptoms will ebb and flow over time. However, patients with ONSM do not show inflammation-related symptoms. Patients who previously received ocular radiotherapy were excluded. The diagnosis of ONSM was based on the characteristic clinical symptoms and typical findings on MRI by the experienced ophthalmologists, radiation oncologists, and radiologists at our institution. Patient characteristics, including age, sex, tumour volume, vision acuity, imaging finding, and radiotherapy information, were collected retrospectively from patients’ records. This study received ethical approval from the Ethical Committee of the Eye & ENT Hospital, Fudan University. Informed consent was waived for the nature of the retrospective study.
Treatment
All the patients received radiotherapy alone. Radiotherapy was applied with IMRT, 3D-CRT, or VMAT. 3D-CRT refers to the adjustment of the three-dimensional shape of the radiation beam by certain means (e.g. lead block used during treatment), so that it conforms to the shape of the target area of disease. IMRT is a development of the 3D-CRT, which enables dose intensity adjustment within the irradiation field. VMAT is an advanced IMRT technique that can shorten the treatment time to 2–6 min. Patients were simulated in the supine position and immobilised with a thermoplastic mask. Computed tomography (CT) images were acquired with a slice thickness of 1.25 mm. Gross tumour volume (GTV) was defined as the visible tumour on diagnostic MRI or CT. Organs at risk were also contoured. The tumour volumes before and after treatment were measured on the treatment planning system. The tumour volume change was evaluated as far as possible.
Follow-up
Visual acuity, visual field, and optic disc findings were assessed before and after radiotherapy. Visual acuity worse than 6/12–6/18 was defined as mild visual loss, worse than 6/18–6/60 was defined as moderate visual loss, and 6/60 to 3/60 was defined as severe visual loss [11, 12]. According to the International Classification of Diseases, vision greater than 0.8 is defined as normal vision, 0.79–0.32 is mild vision loss, and 0.1–0.05 is severe vision loss. The ocular and systemic complications were also evaluated during and after treatment. In addition, the subjective visual assessment by the patients was also recorded. The tumour volume was calculated before and after radiotherapy. Assessment using CT and/or MRI was routinely performed at three months after treatment. For patients who cannot be assessed by MRI, they were assessed by CT images before and after radiotherapy on the radiotherapy treatment planning system. Patients were followed up every 6 months for the first 2 years and every 12 months after radiotherapy. Up to now, all the patients have a follow-up of 1–2 years.
Statistical analysis
The results of the study were analysed using SPSS. A comparison of tumour volume between pre-treatment and post-treatment was performed using the paired t-test. Subgroup analyses were performed using logistic regression analysis to assess the effect of gender, age, duration of symptoms, tumour volume, and severe visual impairment. Progression-free survival (PFS) rate was estimated using the Kaplan–Meier analysis. P < 0.05 was considered significant.
Results
Patient characteristics
Patient information and tumour characteristics were presented in Table 1. The median age of the patients was 48 years (range 15–64 years), and the mean age was 45.3 years. Among them, ten were male and 33 were female, with a female-to-male ratio of 3.3. Eleven patients (25.6%) received treatment at the time for more than 12 months after the symptom occurrence, while the other 32 (74.4%) were treated within 12 months. Proptosis was found in 26 (60.5%) patients, 2(4.7%) had eyeball mobility limitation, and 34 (79.1%) had decreased visual acuity. Swelling (16.3%), visual field impairment (2.3%), epiphora (2.3%), and pain (4.7%) were presented as initial symptoms at diagnosis. The typical image characteristics of primary ONSM were shown in Supplementary Fig. 1.
Radiotherapy treatment
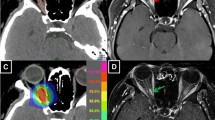
Fifteen (34.9%) patients underwent 3D-CRT, 19 (44.2%) had IMRT, and 9 (20.9%) received VMAT (Fig. 1). A total dose of 50.4-54 Gy was delivered to the primary tumour with 1.8 Gy/fraction. The average dose to the ipsilateral optic nerve, optic chiasm, cornea, lens, and the eyeball was 5067.3 ± 996.2 cGy, 3199.9 ± 857.5 cGy, 1243.2 ± 717.1 cGy, 1675.1 ± 959.4 cGy, and 2963.7 ± 995.8 cGy, respectively (Supplementary Table 1).

Axial (A), (B), sagittal (C), and coronal (D) showed the dose distribution of radiation therapy. E presented the dose-volume histogram of the tumour and several vital organs at risk.
Tumour volume change assessment
Only 25 patients performed MRI examinations both before and after radiotherapy. The MRI analysis showed that 7 patients (16.3%) had significant tumour regression after radiotherapy and 2 typical patients were shown in Supplementary Figure 2, while 16 (37.2%) were with stable diseases, and 2 (4.7%) had tumour progression after treatment (Table 2). We calculated the tumour volume on the patient’s anterior and posterior CT on Treatment Planning System (TPS), and the average tumour volume decreased significantly from 2.33 cubic centimetres (cc) before radiotherapy to 1.77cc after radiotherapy (p = 0.044).
Vision recovery
Among thirty-nine patients who performed visual acuity assessment, 23 patients (53.5%) had no improvement in vision, and 16 patients (47.2%) had improved or recovered vision. The relationship between visual acuity recovery and gender, age, duration time, tumour volume, and vision loss degree was analysed in all patients by logistics regression. Patients with a duration of fewer than 12 months between symptom onset and receiving treatment had a significantly higher probability of visual recovery than those with more than 12 months (odds ratio = 4.13, 95% confidence interval = 1.06–6.10, p = 0.04). The severe visual loss at the time of treatment was also an important factor affecting whether the visual acuity could be improved after treatment (odds ratio = 4.73, 95% confidence interval = 1.06–21.15, p = 0.04) (Fig. 2).

Degree of association between visual acuity improvement and related factors, 95% confidence interval.
Treatment efficacy
Two patients experienced tumour progression at 3 and 6 months after radiotherapy, respectively. No patients underwent orbit exenteration. No patient developed a second tumour in the brain or head and neck during the follow-up period. During the follow-up, 4 patients can not be accessed, 4 patients experienced dry eyes, 7 patients had watery eyes, and 3 patients experienced swollen eyes.1, 3, and 5-year overall survival rates were all 100%. The estimated PFS rates at 3, 6, 12, and 60 months after radiotherapy was 97.4%, 94.9%, 94.9%, and 94.9%, respectively (Fig. 3).

Patients at risk after 3, 6, 12, and 69 months after RT were 97.4%, 94.9%, 94.9%, and 94.9%, respectively.
Discussion
Although ONSM is not a malignant tumour, it can lead to vision loss and blindness [10, 13]. Because the ONSM surrounds the optic nerve, tumour resection is nearly impossible without significant vision loss [14]. Due to the high incidence of vision loss and frequent tumour recurrence, recent reports have not yet shown any advantage of surgery over other treatment options. Radiotherapy is an important treatment modality for the treatment of ONSM, and there is no significant difference in the prognosis with different radiotherapy techniques [12, 15]. However, what is the relationship between radiotherapy and the recovery or improvement of vision and how to grasp the optimal time of treatment to help patients achieve a higher quality of life needs to be considered [10, 16]. Literature indicates that a 54 Gy radiation dose can improve or restore visual acuity in ONSM. According to a study by Ravi Pandit et al. [17], 69% of patients had stable visual performance after radiotherapy. In our study, 53.5% of patients had stable visual acuity. In contrast to the common result of no vision improvement after radiotherapy [12], 37.2% of the cohort conferred with visual acuity improvement from radiotherapy. We further investigated the factors that impact vision recovery and found that patients who had severe visual loss at diagnosis and who (11/43) endured more than 12 months had less recovery possibility. Hence, it is more likely to improve vision for patients without severe vision loss and timely treatment. High-precision radiotherapies of ONSM must take into account planning goals as well as the preservation of organs at risk [15, 18]. The local control rate is quite good, with the usual radiation dose of 50.4-54.0 Gy [19]. In our cohort, we achieved a 94.9% 5-year local control rate, which is consistent with another study of 90-100% radiological control rate [6]. Although there were no statistically significant differences in visual outcomes between the different radiotherapy technique groups [20, 21], IMRT and VMAT were recommended for greater precision to avoid damaging normal tissue with excessive doses that 3D-CRT [22].
Limitations of this study included its retrospective nature and some missing outcome data such as colour vision, visual fields, and MRI examination. We retrospectively analysed the efficacy of radiotherapy in a limited number of cases in a single study centre. Due to the length of the follow-up period, the time to assess the final visual function was different in each case. Second, late complications of radiation therapy have not been evaluated due to the short observation period. In further studies, we will continue to follow these cases and evaluate visual function and complications after long-term treatment. Additionally, while the diagnosis of ONSM largely depends on clinical and imaging examinations, most cases lack tissue diagnosis, which increases the little but important possibility of alternative diagnoses that may mimic ONSM (e.g., idiopathic orbital inflammation, sarcoma). What’s more, the risk of serious post-treatment complications is considered low. A longer follow-up is required to fully assess the risk of complications and the durability of response to treatment.
Conclusion
Radiation therapy such as VMAT, IMRT and 3D-CRT is one of the important treatments for ONSM. The visual acuity improvement of patients after treatment was related to the severity of visual impairment and the duration of symptoms before treatment. The better the patient’s visual acuity before treatment, the better or even restore the original vision after treatment. Patients whose symptoms persisted for less than 12 months had a higher chance of improving or recovering their vision after radiation therapy than those with more than 12 months.
Summary
What was known before
-
Optic nerve sheath meningioma (ONSM) is a rare meningeal tumour.
-
Radiation therapy is a non-invasive alternative to surgery and is proved to be highly effective in tumour control for ONSM.
What this study adds
-
Radiotherapy could play an important role in decreasing the tumour volume and improving the vision for ONSM.
-
The probability of vision recovery is lower in patients with severe vision loss.
-
The probability of vision recovery is higher in patients with a duration of fewer than 12 months.
Data availability
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request.
References
Eddleman CS, Liu JK. Optic nerve sheath meningioma: current diagnosis and treatment. Neurosurg Focus. 2007;23:E4. https://doi.org/10.3171/FOC-07/11/E4.
Jin J, Joo JD, Han JH, Yang HK, Hwang JM, Kim YJ, et al. Optic nerve sheath meningioma: preliminary analysis of the role of radiation therapy. Brain Tumor Res Treat. 2018;6:8–12. https://doi.org/10.14791/btrt.2018.6.e2.
Douglas VP, Douglas K, Cestari DM. Optic nerve sheath meningioma. Curr Opin Ophthalmol. 2020;31:455–61. https://doi.org/10.1097/ICU.0000000000000700.
Vaishnav YJ, Singh R, Didwania P, Lehrer EJ, Bakaeva T, Harris TJ, et al. Radiotherapy and radiosurgery in the management of optic nerve sheath meningiomas: an international systematic review and meta-analysis of twenty studies. World Neurosurg. 2022;164:e929–e944. https://doi.org/10.1016/j.wneu.2022.05.064.
Adeberg S, Welzel T, Rieken S, Debus J, Combs SE. Prior surgical intervention and tumor size impact clinical outcome after precision radiotherapy for the treatment of optic nerve sheath meningiomas (ONSM). Radiat Oncol. 2011;6:117. https://doi.org/10.1186/1748-717X-6-117.
Saeed P, Blank L, Selva D, Wolbers JG, Nowak PJ, Geskus RB, et al. Primary radiotherapy in progressive optic nerve sheath meningiomas: a long-term follow-up study. Br J Ophthalmol. 2010;94:564–8. https://doi.org/10.1136/bjo.2009.166793.
de Melo LP, Arruda Viani G, de Paula JS. Radiotherapy for the treatment of optic nerve sheath meningioma: a systematic review and meta-analysis. Radiother Oncol. 2021;165:135–41. https://doi.org/10.1016/j.radonc.2021.10.009.
Bloch O, Sun M, Kaur G, Barani IJ, Parsa AT. Fractionated radiotherapy for optic nerve sheath meningiomas. J Clin Neurosci. 2012;19:1210–5. https://doi.org/10.1016/j.jocn.2012.02.010.
Ratnayake G, Oh T, Mehta R, Hardy T, Woodford K, Haward R, et al. Long-term treatment outcomes of patients with primary optic nerve sheath meningioma treated with stereotactic radiotherapy. J Clin Neurosci. 2019;68:162–7. https://doi.org/10.1016/j.jocn.2019.07.005.
Sasano H, Shikishima K, Aoki M, Sakai T, Tsutsumi Y, Nakano T. Efficacy of intensity-modulated radiation therapy for optic nerve sheath meningioma. Graefes Arch Clin Exp Ophthalmol. 2019;257:2297–306. https://doi.org/10.1007/s00417-019-04424-w.
Patodia Y, Golesic E, Mao A, Hutnik CM. Clinical effectiveness of currently available low-vision devices in glaucoma patients with moderate-to-severe vision loss. Clin Ophthalmol. 2017;11:683–7. https://doi.org/10.2147/OPTH.S128425.
Hamilton SN, Nichol A, Truong P, McKenzie M, Hsu F, Cheung A, et al. Visual outcomes and local control after fractionated stereotactic radiotherapy for optic nerve sheath meningioma. Ophthalmic Plast Reconstr Surg. 2018;34:217–21. https://doi.org/10.1097/IOP.0000000000000914.
Kahraman-Koytak P, Bruce BB, Peragallo JH, Newman NJ, Biousse V. Diagnostic errors in initial misdiagnosis of optic nerve sheath meningiomas. JAMA Neurol. 2019;76:326–32. https://doi.org/10.1001/jamaneurol.2018.3989.
Lestak J, Haninec P, Kyncl M, Tintera J. Optic nerve sheath meningioma-findings in the contralateral optic nerve tract: aA case report. Mol Clin Oncol. 2020;12:411–4. https://doi.org/10.3892/mco.2020.2012.
Senger C, Kluge A, Kord M, Zimmermann Z, Conti A, Kufeld M et al.. Effectiveness and safety of robotic radiosurgery for optic nerve sheath meningiomas: a single institution series. Cancers. 2021;13. https://doi.org/10.3390/cancers13092165.
Ovens C, Dean B, Gzell C, Patanjali N, Jonker B, O’Connor M, et al. Optimal management in optic nerve sheath meningioma - A multicentre study and pooled data analysis. J Clin Neurosci. 2020;80:162–8. https://doi.org/10.1016/j.jocn.2020.08.017.
Pandit R, Paris L, Rudich DS, Lesser RL, Kupersmith MJ, Miller NR. Long-term efficacy of fractionated conformal radiotherapy for the management of primary optic nerve sheath meningioma. Br J Ophthalmol. 2019;103:1436–40. https://doi.org/10.1136/bjophthalmol-2018-313135.
Inoue T, Mimura O, Masai N, Ohashi A, Ikenaga K, Okuno Y, et al. Early intervention using high-precision radiotherapy preserved visual function for five consecutive patients with optic nerve sheath meningioma. Int J Clin Oncol. 2018;23:826–34. https://doi.org/10.1007/s10147-018-1284-5.
Brower JV, Amdur RJ, Kirwan J, Mendenhall WM, Friedman W. Radiation therapy for optic nerve sheath meningioma. Pract Radiat Oncol. 2013;3:223–8. https://doi.org/10.1016/j.prro.2012.06.010.
Lesser RL, Knisely JP, Wang SL, Yu JB, Kupersmith MJ. Long-term response to fractionated radiotherapy of presumed optic nerve sheath meningioma. Br J Ophthalmol. 2010;94:559–63. https://doi.org/10.1136/bjo.2009.167346.
Eckert F, Clasen K, Kelbsch C, Tonagel F, Bender B, Tabatabai G, et al. Retrospective analysis of fractionated intensity-modulated radiotherapy (IMRT) in the interdisciplinary management of primary optic nerve sheath meningiomas. Radiat Oncol. 2019;14:240. https://doi.org/10.1186/s13014-019-1438-2.
Vakharia K, Hasegawa H, Stafford SL, Link MJ. Salvage radiosurgery for optic nerve sheath meningioma. Cureus. 2021;13:e16450. https://doi.org/10.7759/cureus.16450.
Author information
Authors and Affiliations
Contributions
TT and JW studied concept and designed; analysis and interpretation of data; and wrote initial draft. TL re-examined the clinical data of all patients. ZZ provided study materials. XS studied concept and edited the draft and study supervision. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

{kind=link}
{kind=link}
Cite this article
Tang, T., Wang, J., Lin, T. et al. The treatment efficacy of radiotherapy for optic nerve sheath meningioma. Eye 38, 89–94 (2024). https://doi.org/10.1038/s41433-023-02640-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-023-02640-7
- Springer Nature Limited