
Abstract
Background/Objectives
Malnutrition is a prevalent problem in patients with cancer and is associated with poor prognosis. The European Society for Clinical Nutrition and Metabolism (ESPEN) recommends the provision of nutritional support and evaluation. This study aims to describe the nutritional management of patients with cancer, including assessment of adherence, from the perspective of both patients and healthcare professionals (HCPs).
Subjects/Methods
A cross-sectional descriptive observational study was carried out through two surveys addressed to patients and HCPs.
Results
A total of 230 cancer patients and 461 HCPs completed the questionnaire. The survey found 55.0% of patients experienced eating problems during treatment and 64.0% reported sequelae affecting nourishment. However, 60.1% of patients and 42.6% of HCPs indicated that nutritional status is not generally assessed. While 86.6% of HCPs stated that nutritional information is provided to patients, only 33.5% of patients reported having received it. Regarding nutritional adherence, 87.4% of HCPs stated that it is assessed whereas only 49.2% of patients receiving nutritional supplements confirmed this. General discomfort or gastrointestinal problems were the main issues hampering correct adherence perceived by both patients (41.8%) and HCPs (95.4%).
Conclusions
Our study demonstrate that different perceptions exist between patients and HCPs about nutritional management in cancer and suggests that in Spain nutritional approach is suboptimal in terms of screening/assessment of malnutrition, nutritional information provided to the patient, nutritional intervention and assessment of adherence to nutritional support. Therefore, measure should be taken to foster the adoption of ESPEN recommendations in clinical practice and to promote nutritional education of HCPs.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Malnutrition is a prevalent problem in cancer patients and is associated with poor prognosis [1]. Its prevalence depends on the stage of the disease and the type of cancer, rising to 80.0% in some types such as oesophageal cancer [2, 3]. Malnutrition can be a consequence of the disease itself, treatment, or inadequate nutritional planning by healthcare professionals (HCPs) [4,5,6].
Malnutrition worsens health-related quality of life (HRQoL) and increases morbidity and mortality, resulting in prolonged hospitalizations and increased costs [7,8,9]. Recognizing its importance, the European Society for Clinical Nutrition and Metabolism (ESPEN) and the Spanish Society of Medical Oncology (SEOM) recommend the identification, prevention, and treatment of reversible aspects of malnutrition in cancer patients [10, 11]. Despite these recommendations, several studies report a sub-optimal nutritional management of cancer patients [12,13,14,15]. Indeed, early intervention and nutritional adherence are essential to maintain or improve malnourished patients’ nutritional status. In this respect, research shows patients who adhere to nutritional supplements experience less weight loss and enjoy greater protection against disease progression than non-adherent patients [15]. However, nutritional counselling of patients and assessment/promotion of adherence are rarely undertaken [13, 15]. For this reason, patient education in self-care of their disease (including nutritional care) and the implementation of strategies to assess and promote adherence to nutritional counselling are also recommended [16, 17]. To achieve this, the awareness of nutrition relevance must be fostered among healthcare professionals and patients.
Malnutrition and its symptoms are perceived differently among HCPs, patients, and caregivers [18]. Therefore, a greater understanding of both HCPs and patients’ opinions and experiences of nutritional management during the oncological process can help to identify barriers and develop optimization strategies. Accordingly, the ONA study aims to describe the nutritional management of cancer patients, including assessment of adherence, from the perspectives of patients and HCPs.
Subjects and methods
Study design
An observational, descriptive, cross-sectional study, based on a structured ad hoc questionnaire, was conducted in the Spanish public healthcare context between January and April 2020.
A scientific committee composed by five HCP [General Practitioner, (GP), Endocrinologist (En), Radiation Oncologist (RO), Medical oncologist (MO) and nurse (Nu)] and two representatives of the Spanish Cancer advocacy group (Grupo Español de pacientes con cancer, GEPAC), participated in the questionnaires design.
Two online structured questionnaires were developed, one addressed to cancer patients and the other to HCPs involved in the nutritional management of cancer. Both questionnaires were designed based on relevant aspects of nutritional management and perceived needs, elicited from a literature review, of a focus group of cancer patients. The focus group was composed of six patients with different profiles in terms of their age, sex, type of cancer, and nutritional support received.
Questionnaires
The HCPs and patient questionnaires were composed of 32 and 28 items, respectively (Supplementary Material). Both questionnaires were organized in six sections: (1) Socio-demographic and work-related (HCPs)/Clinical (Patients) variables; (2) Perception of nutritional management in cancer patients; (3) Nutritional assessment in clinical practice: screening/complete nutritional assessment, the timing of performance/referral and tools used; (4) Nutritional information provided to the patient: information process, timing and topics covered; (5) Nutritional intervention in clinical practice: prescription/recommendation of nutritional support, consideration of patient preferences, adherence control and strategies to improve adherence; (6) Existing barriers preventing proper adherence to nutritional support and strategies for improvement.
The questionnaires included open and closed-ended questions (dichotomous or multiple choice), numerical rating scales (from 0 to 10), and 4-point Likert-scale questions.
The HCPs were invited (via newsletters, the societies’ websites, e-mail, and social networks) to participate in the survey by various scientific societies endorsing the study: Sociedad Española de Nutrición Clínica y Metabolismo (SENPE), Sociedad Española de Hematología y Hemoterapia (SEHH), Sociedad Española de Médicos de Atención Primaria (SEMERGEN), Sociedad Española de Endocrinología y Nutrición (SEEN), Sociedad Española de Oncología Médica (SEOM) and Sociedad Española de Oncología Radioterápica (SEOR). Patients were invited to participate by the GEPAC through its websites, and social networks. In addition, the members of the committee and the study promoter participated in the dissemination of the study.
Participants
The study sample size was estimated based on the assumption of maximum uncertainly [n = N· Z2α· p· q/e2 · (N-1) + Z2α · p ·q] with a 95.0% confidence interval and 10.0% precision. The calculation included the number of HCPs (GP, En, RO, MO, and Nu) who practice within the Spanish public healthcare (n = 218.035) [19, 20] and the number of patients >18 years with cancer in Spain (n = 767.449) [21]. As a result, the minimum required sample size was estimated at 96 HCPs and 97 patients.
All patients over 18 years of age diagnosed with cancer and HCPs practising in Spain were eligible.
Statistical analysis
Data were analyzed with the STATA statistical package, version 14. The absolute and relative frequencies of qualitative variables were calculated to describe qualitative variables. The mean, standard deviations (SD) and interquartile ranges were calculated to express quantitative variables. Missing data were not included in the analysis.
Results
A total of 461 HCPs and 230 patients with cancer from all Spanish regions completed the questionnaire. There was a higher proportion of women among HCPs (63.1%) and patients (81.3%). Most HCPs were general practitioner (41.0%) while the most common type of cancer among patients was breast (35.7%) and haematological cancer (34.8%). Socio-demographic characteristics of study participants are shown in Table 1. The HCPs were highly experienced in cancer management, reporting a mean experience of 16.3 (SD 10.2) years. Specific nutritional protocols were not available in most cases (66.2%), and half of the HCPs (51.8%) had not received nutritional education. However, most of HCPs (77.2%) could refer the patient to a nutrition expert via an inter-consultation service (73.1%) or a multidisciplinary committee (4.1%). More than half of the patients reported eating problems during cancer treatment (55.0%) and cancer sequelae affecting nourishment (64.0%).
Perception of nutritional management in cancer patient
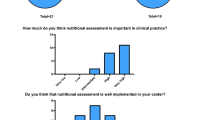
The HCPs considered that nutritional assessment and treatment of patients with cancer were suboptimal, with an average score (out of 10) of 5.2 (SD 2.0) and 5.4 (SD 1.9), respectively. In this regard, most of them considered that the nutrition expert (95.0%) and specific nutritional education (96.7%) were essential for the nutritional management of patients. Moreover, 96.3% considered that nutritional management of cancer patients should be multidisciplinary and coordinated by the nutrition expert.
Meanwhile, 60.4% of patients felt that their nutritional status was inadequate during their illness, and 97.8% considered that optimal nutrition could help to improve cancer treatment efficacy and patients’ health-related quality of life.
Nutritional assessment in clinical practice
The HCPs reported that nutritional screening in cancer patients (58.4%) was conducted either by themselves (46.0%) or by another HCP after referral (12.4%). In malnourished patients or those at risk of malnutrition, a complete nutritional assessment was performed (73.1%), by the HCPs themselves (50.5%), or by another HCP after referral (22.6%). According to patients, 40.9% stated their nutritional status had been assessed. Both HCPs and patients stated that nutritional screening/assessment was mainly evaluated during treatment (56.1% and 61.8%, respectively).
The HCPs who stated they had performed nutritional screening or undertaken a complete nutritional assessment cited the following tools: weight loss (76.4% and 77.7%, respectively), body mass index (72.2% and 62.2%), reduced intake in recent weeks/ dietary register (72.2% and 53.6%) and specific questionnaires (19.3% and 83.7%). Analytical parameters (83.7%), muscle mass (40.3%), and functional activity (41.2%) were also used to undertake a complete nutritional assessment. Patients reported that their nutritional status was evaluated using body weight (71.0%), dietary habits (47.6%), and specific questionnaires (67.7%).
According to HCP responses RO (84.2%), and En (77.8%) assessed nutritional status most frequently, followed by MO (55.3%), AP (36.9%), Nu (32.4%) and haematologist (25.0%). From the patients’ perspective, MO (23.9%), haematologist (19.1%) assessed nutritional status most frequently followed by NU (11.7%), En (9.1%), GP (7.4%) and RO (4.8%).
Nutritional information provided to the patient
Most HCPs (86.6%) indicated that nutritional information was provided to patients by themselves or by their team members. However, only 33.5% of patients reported having received such information. Of these patients, 67.5% had been satisfied with the information provided. From the patient’s perspective, the most important issue concerned foods to be consumed or avoided (79.1%), followed by the importance of healthy nutrition in cancer (50.0%), recommendations to prevent/treat possible side effects (46.1%), and the impact of disease/treatment on nutritional status (44.8%). According to HCP responses, all these topics are commonly addressed (>68.0%). Of the total, 79.1% of patients sought additional information from different sources such as internet (54.3%), patient associations (27.0%), and other patients with cancer (13.5%).
Both HCPs and patients stated that nutritional information is mainly provided during treatment (78.9% and 68.8%, respectively) and to a lesser extent during diagnosis (31.1% and 15.6%) and post-treatment follow-up (36.1% and 27.3%).
Nutritional intervention in clinical practice
Most HCPs (87.4%) reported prescribing or recommending nutritional support if needed. Moreover, 91.1% of HCPs stated they considered the patient’s preferences during treatment prescription. However, among those patients receiving nutritional support (70.9%), a total of 55.0% stated that the HCPs had not taken their preferences into account.
The majority of HCPs (86.8%) reported that adherence was evaluated, either by themselves or by a team member. By contrast, only 49.2% of patients receiving nutritional support confirmed this. Among HCPs who assessed adherence, the clinical interview was the most commonly used tool (94.6%), followed by a dispensation record (29.1%), self-reported questionnaires (15.4%), and pill count (9.4%).
Barriers to proper adherence to nutritional support and strategies for improvement
The majority of patients who had received nutritional support felt that the listed hurdles had a limited impact on adherence. By contrast, most HCPs considered that these barriers had a considerable impact on nutritional adherence (Fig. 1). General discomfort or gastrointestinal problems were the main barriers perceived for correct adherence by patients (41.8%) and by HCPs (95.4%) (Fig. 1).

HCPs healthcare professionals, Pt patient, GI gastrointestinal.
The strategies proposed were considered highly useful for improving nutritional management of cancer patients (mean >8.2, from none = 0 to a lot = 10). Availability of support staff with nutritional knowledge, nutritional advice in action protocols, nutritional screening in routine clinical practice, and establishing multidisciplinary nutritional protocols adapted to the centre were the most highly rated strategies (mean > 8.8) (Fig. 2).

HCPs healthcare professionals, Pt patient, GI gastrointestinal.
Discussion
Malnutrition is a common issue in patients with cancer; however, there is limited evidence related to the nutritional approaches targeting these patients in Spanish clinical practice. The present study aims to describe the nutritional management of patients with cancer from the perspective of patients and HCPs, including nutritional screening and/or nutritional assessment, the information provided/received, and adherence to nutritional treatment.
This study shows that HCPs and patients often have different perceptions about the nutritional management of the disease. In particular, compared to patients, HCPs overestimated patient information, patient involvement in decision-making, and adherence assessment. In addition, the results suggest that the nutritional management of patients with cancer in Spain is suboptimal, as indicated by the HCPs with a modest average score (5 out of 10) rated on the nutritional management process. HCPs responses revealed that most centres did not have specific nutritional protocols, and almost a quarter of the HCPs stated that they did not refer the patient to a nutrition expert, which could be an underlying reason for the suboptimal nutritional management of patients with cancer. Thus, most HCPs stated that multidisciplinary management coordinated by a nutrition expert would be essential to optimize nutritional management of cancer patients.
Interestingly, despite the low prevalence of cancers that are correlated with higher rates of malnutrition (e.g. gastrointestinal, pancreatic, head and neck) [22], most patients reported eating problems and sequelae affecting nourishment and considered that their nutritional status during their disease was inadequate. Despite this, more than half of them reported that their nutritional status was not evaluated, which is in concordance with the views expressed by the HCPs. In accordance with these results, in a cross-sectional study involving 1073 cancer survivors [23], 45.0% suffered from a diet-related problem, but only 39.0% of the total had access to a nutrition expert.
The main clinical guidelines that address the nutritional management of cancer patients recommend continuous assessment of their nutritional status [10, 11]. Despite this, nearly one-third of patients did not receive nutritional screening/assessment, as stated by the HCPs. Lack of routine nutritional assessment in Spain [16] and other European countries such as Italy and France [24, 25] has been reported in previous studies, implying that nutritional assessment should be critically reviewed and improved in these patients.
One study indicates that nearly 60.0% of oncologists did not recognize malnutrition, highlighting the importance of HP education [26]. Hence, to guarantee consistency of practice and improved patient care, it is necessary to ensure adequate nutritional education among HCPs, particularly in centres where a nutrition expert is unavailable. In our study, most HCPs had not received specific nutritional education. Similarly, several studies have reported that less than 40.0% of HCPs have received such training [25,26,27]. Conversely, in the specific case of oncologists and En we found high nutritional education rates, as previously reported by Van Cutsem et al., [28] where more than 60.0% of participants had received training in nutrition.
The ESPEN guidelines consider nutrition counselling by a health care professional as the first line of nutrition therapy [10]. Therefore, HCP must provide helpful and applicable advice on nutrition-related issues. However, while most HCPs stated that they informed patients about nutritional issues, only 33.5% of patients reported having received this information. Furthermore, even among those patients who received information, the majority sought alternative information sources such as the Internet.
Patients with cancer need the correct information at the right time and support to use that information effectively [23]. The issues discussed with patients should be those that are likely to have the most significant impact on their quality of life and matter to them most. In this context, we have found that the most important issues for patients, such as the type of food to be consumed or avoided and the importance of healthy eating during illness, are often addressed by HCPs. In general, our results are in line with a cross-sectional study carried out in Germany with more than a thousand patients with cancer [13]. Consistent with previous studies [29], we also found that the information process mainly occurs during cancer treatment. However, nutritional support is scarce after treatment. It is worth noting that receiving information in a cross-disciplinary manner can enhance and reinforce the information [30]. However, the lack of coordination during the patient journey and the conflicting message from HCPs is described as a source of uncertainty and confusion [31].
The prescription of nutritional formulas to patients who need them is pivotal to improving nutritional status. However, even though most patients reported eating problems and sequelae affecting nutrition, less than one-third received nutritional support. Our data are consistent with previous studies which report that less than 40.0% of oncological patients received support on nutrition [13, 14, 32, 33].
In addition, other authors have reported that less than 50.0% of patients are adherents to nutritional support [34]. Therefore, the assessment of adherence is a key point to identify non-adherent patients in order to establish strategies to improve nutritional adherence. However, although most HCPs reported that patients on nutritional support are monitored to assess adherence, only half of the patients confirmed this. Among all the strategies defined to enhance adherence, those related to training and implementing action protocols were the most highly rated by HCPs, as previously described by Kiss et al. [35]. In this respect, promoting the nutritional education of HCPs, implementing multidisciplinary nutrition teams, and raising awareness among patients could lead to an increased detection of malnutrition, optimized management, and improved efficacy during cancer treatments.
Our study has several limitations. Firstly, most items included in the questionnaires were closed questions, which may hamper their interpretation. Nevertheless, the questionnaires were reviewed by a scientific committee composed of HCPs involved in the management of cancer patients and patient representatives. Secondly, because the questionnaire was addressed to all scientific society members endorsing the study, those members who were more aware of nutritional aspects were more likely to participate. Consequently, “good practice” may be overestimated. In addition, most patients had breast or haematological cancers. In contrast, endocrine, gastrointestinal or head and neck cancers, where nutritional strategies are usually developed, were very poorly represented. This may partly explain the perception differences observed between HCPs and patients. Unfortunately, the small sample size of the subgroups did not allow analysis by cancer type. Thirdly, general practitioners are over-represented compared to other specialties. Therefore, the findings obtained in this study cannot be generalized to the whole population. By contrast, one of the main strengths is the large sample of participants (HCPs and patients). Thus, the results of this study highlight potential critical points of the current situation and the current needs related to the nutritional management of cancer patients, helping to define strategies for improvement.
In conclusion, the present study demonstrate that different perceptions exist between patients and professionals about nutritional management in cancer and suggests that nutritional approach is suboptimal in Spain. Therefore, there is a need to incorporate routine nutritional assessment and the monitoring of adherence into clinical practice. Moreover, different perceptions exist between HCPs and patients regarding nutritional counselling and adherence monitoring of nutritional support. Thus, it is necessary to improve HCP-patient communication and to engage in the adoption of ESPEN recommendations.
Data availability
The datasets generated during and/or analysed during the current study are not publicly available due to privacy and ethical concerns but are available from the corresponding author on reasonable request and with permission of the study promoter.
References
Yim GW, Eoh KJ, Kim SW, Nam EJ, Kim YT. Malnutrition identified by the nutritional risk index and poor prognosis in advanced epithelial ovarian carcinoma. Nutr Cancer. 2016;68:772–9. https://doi.org/10.1080/01635581.2016.1159702.
Escortell Sanchez R, Reig Garcia-Galbis M. [Enteral Nutrition on the Nutritional Status of Cancer]. Nutr Hosp. 2015;32:1408–16. https://doi.org/10.3305/nh.2015.32.4.9227.
Capra S, Ferguson M, Ried K. Cancer: impact of nutrition intervention outcome-nutrition issues for patients. Nutrition. 2001;17:769–72. https://doi.org/10.1016/s0899-9007(01)00632-3.
Van Cutsem E, Arends J. The causes and consequences of cancer-associated malnutrition. Eur J Oncol Nurs. 2005;9:S51–63. https://doi.org/10.1016/j.ejon.2005.09.007.
Guo ZQ, Yu JM, Li W, Fu ZM, Lin Y, Shi YY, et al. Survey and analysis of the nutritional status in hospitalized patients with malignant gastric tumors and its influence on the quality of life. Support Care Cancer. 2020;28:373–80. https://doi.org/10.1007/s00520-019-04803-3.
Zhang X, Pang L, Sharma SV, Li R, Nyitray AG, Edwards BJ. Prevalence and factors associated with malnutrition in older patients with cancer. J Geriatr Oncol. 2019;10:763–9. https://doi.org/10.1016/j.jgo.2019.01.021.
Khalatbari-Soltani S, Marques-Vidal P. Impact of nutritional risk screening in hospitalized patients on management, outcome and costs: a retrospective study. Clin Nutr. 2016;35:1340–6. https://doi.org/10.1016/j.clnu.2016.02.012.
Rinninella E, Fagotti A, Cintoni M, Raoul P, Scaletta G, Quagliozzi L, et al. Nutritional interventions to improve clinical outcomes in ovarian cancer: a systematic review of randomized controlled trials. Nutrients. 2019;11. e-pub ahead of print 2019/06/27; https://doi.org/10.3390/nu11061404.
Zhang X, Tang T, Pang L, Sharma SV, Li R, Nyitray AG, et al. Malnutrition and overall survival in older adults with cancer: a systematic review and meta-analysis. J Geriatr Oncol. 2019;10:874–83. https://doi.org/10.1016/j.jgo.2019.03.002.
Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36:11–48. https://doi.org/10.1016/j.clnu.2016.07.015.
de Las Penas R, Majem M, Perez-Altozano J, Virizuela JA, Cancer E, Diz P.et al. SEOM clinical guidelines on nutrition in cancer patients 2018. Clin Transl Oncol. 2019;21:87–93. https://doi.org/10.1007/s12094-018-02009-3.
Caccialanza R, Goldwasser F, Marschal O, Ottery F, Schiefke I, Tilleul P, et al. Unmet needs in clinical nutrition in oncology: a multinational analysis of real-world evidence. Ther Adv Med Oncol. 2020;12:1758835919899852. https://doi.org/10.1177/1758835919899852.
Maschke J, Kruk U, Kastrati K, Kleeberg J, Buchholz D, Erickson N, et al. Nutritional care of cancer patients: a survey on patients’ needs and medical care in reality. Int J Clin Oncol. 2017;22:200–6. https://doi.org/10.1007/s10147-016-1025-6.
Ginzburg Y, Shmilovitz I, Monastyrsky N, Endevelt R, Shahar DR. Barriers for nutritional care in the transition from hospital to the community among older patients. Clin Nutr ESPEN. 2018;25:56–62. https://doi.org/10.1016/j.clnesp.2018.04.004.
de Oliveira Faria S, Alvim Moravia R, Howell D, Eluf Neto J. Adherence to nutritional interventions in head and neck cancer patients: a systematic scoping review of the literature. J Hum Nutr Diet. 2020. e-pub ahead of print 2020/12/15; https://doi.org/10.1111/jhn.12848.
Duran-Poveda M, Jimenez-Fonseca P, Sirvent-Ochando M, Garcia-Luna PP, Pereira-Cunill JL, Lema-Marques B, et al. Integral nutritional approach to the care of cancer patients: results from a Delphi panel. Clin Transl Oncol. 2018;20:1202–11. https://doi.org/10.1007/s12094-018-1846-z.
Volkert D, Beck AM, Cederholm T, Cruz-Jentoft A, Goisser S, Hooper L, et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr. 2019;38:10–47. https://doi.org/10.1016/j.clnu.2018.05.024.
Gyan E, Raynard B, Durand JP, Lacau Saint Guily J, Gouy S, Movschin ML, et al. Malnutrition in patients with cancer: comparison of perceptions by patients, relatives, and physicians-results of the NutriCancer2012 Study. JPEN J Parenter Enter Nutr. 2018;42:255–60. https://doi.org/10.1177/0148607116688881.
Barber Pérez P, González López-Valcárcel B Estimación de la oferta y demanda de médicos. España 2018-2030. Ministerio de Sanidad, Servicios Sociales e Igualdad, 2019.
SNS Sdid. Principales datos del Sistema Nacional de Salud. In: Ministerio de Sanidad, Consumo y Bienestar Social, 2019.
Cancer IafRo. Data visualization tools for exploring the global cancer burden in 2020. In. Cancer today, 2020.
Muscaritoli M, Lucia S, Farcomeni A, Lorusso V, Saracino V, Barone C, et al. Prevalence of malnutrition in patients at first medical oncology visit: the PreMiO study. Oncotarget. 2017;8:79884–96. https://doi.org/10.18632/oncotarget.20168.
Sullivan ES, Rice N, Kingston E, Kelly A, Reynolds JV, Feighan J, et al. A national survey of oncology survivors examining nutrition attitudes, problems and behaviours, and access to dietetic care throughout the cancer journey. Clin Nutr ESPEN. 2021;41:331–9. https://doi.org/10.1016/j.clnesp.2020.10.023.
Caccialanza R, Cereda E, Pinto C, Cotogni P, Farina G, Gavazzi C, et al. Awareness and consideration of malnutrition among oncologists: Insights from an exploratory survey. Nutrition. 2016;32:1028–32. https://doi.org/10.1016/j.nut.2016.02.005.
Corbaux P, Fontaine-Delaruelle C, Souquet PJ, Couraud S, Morel H, Tronc F, et al. Is nutritional screening of patients with Lung Cancer optimal? An expert opinion survey of French physicians and surgeons. Nutr Cancer. 2019;71:971–80. https://doi.org/10.1080/01635581.2019.1595051.
Kirbiyik F, Ozkan E. Knowledge and practices of medical oncologists concerning nutrition therapy: a survey study. Clin Nutr ESPEN. 2018;27:32–7. https://doi.org/10.1016/j.clnesp.2018.07.004.
Murphy JL, Munir F, Davey F, Miller L, Cutress R, White R, et al. The provision of nutritional advice and care for cancer patients: a UK national survey of healthcare professionals. Support Care Cancer. 2021;29:2435–42. https://doi.org/10.1007/s00520-020-05736-y.
Hilmi M, Pellat A, Benoit O, Foucaut AM, Mino JC, Kauffmann A, et al. Nutrition and physical activity professional education in gastrointestinal oncology: a national multidisciplinary survey. BMJ Support Palliat Care. 2020;10:324–30. https://doi.org/10.1136/bmjspcare-2020-002342.
Hiatt JS, Brown TE, Banks M, Lewis CA, Bauer J. Patient and carer experience of nutrition care throughout treatment for head and neck cancer: a systematic qualitative review and thematic synthesis. Support Care Cancer. 2020;28:5633–47. https://doi.org/10.1007/s00520-020-05576-w.
van Veen MR, Mols F, Smeets L, Kampman E, Beijer S. Colorectal cancer survivors’ beliefs on nutrition and cancer; correlates with nutritional information provision. Support Care Cancer. 2020;28:1255–63. https://doi.org/10.1007/s00520-019-04934-7.
Alberda C, Alvadj-Korenic T, Mayan M, Gramlich L. Nutrition care in patients with head and neck or esophageal cancer: the patient perspective. Nutr Clin Pr. 2017;32:664–74. https://doi.org/10.1177/0884533617725050.
Qato DM, Alexander GC, Guadamuz JS, Lindau ST. Prevalence of dietary supplement use in US children and adolescents, 2003–2014. JAMA Pediatr. 2018;172:780–2. https://doi.org/10.1001/jamapediatrics.2018.1008.
Lacau St Guily J, Bouvard E, Raynard B, Goldwasser F, Maget B, Prevost A, et al. NutriCancer: a French observational multicentre cross-sectional study of malnutrition in elderly patients with cancer. J Geriatr Oncol. 2018;9:74–80. https://doi.org/10.1016/j.jgo.2017.08.003.
Gea Cabrera A, Sanz-Lorente M, Sanz-Valero J, Lopez-Pintor E. Compliance and adherence to enteral nutrition treatment in adults: a systematic review. Nutrients. 2019;11. e-pub ahead of print 2019/11/07; https://doi.org/10.3390/nu11112627
Kiss N, Bauer J, Boltong A, Brown T, Isenring L, Loeliger J, et al. Awareness, perceptions and practices regarding cancer-related malnutrition and sarcopenia: a survey of cancer clinicians. Support Care Cancer. 2020;28:5263–70. https://doi.org/10.1007/s00520-020-05371-7.
Acknowledgements
We thank all scientific societies for the dissemination of the questionnaire and the institutional and/or social endorsement of this study. In addition, we thank the participation of all members of the ONA working group listed in the Supplementary Material. The study was supported by Nestlé Health Science. This funding source was involved in the review of the study design and manuscript, but not in the collection, analysis and interpretation of the data, nor in the writing of the report or the decision to submit the article for publication.
Author information
Authors and Affiliations
Contributions
EC contributed to designing the protocol, designing the questionnaire, interpreting data, and co-writing the manuscript. ESS contributed to designing the protocol, designing the questionnaire, interpreting data, and co-writing the manuscript. IO contributed to designing the protocol, reviewing the questionnaire, interpreting data, and reviewing the manuscript. JAG contributed to designing the protocol, reviewing the questionnaire, interpreting data, and reviewing the manuscript. MAE contributed to designing the protocol, reviewing the questionnaire, interpreting data, and reviewing the manuscript. BB contributed to reviewing the protocol, reviewing the questionnaire, and reviewing the manuscript. MB contributed to reviewing the protocol and reviewing the manuscript. MC contributed to reviewing the protocol, reviewing the questionnaire, extracting the survey data, and reviewing the manuscript.
Corresponding author
Ethics declarations
Competing interests
MB is an employee in the medical department of Nestlé Health Science. MC works for an independent scientific consultancy (Outcomes’10) that has received honoraria to develop and coordinate the project and write the current manuscript. The other authors declare no conflicts of interest.
Ethics approval
The study followed the international ethical recommendations contained in the Declaration of Helsinki. The Clinical Research Ethics Committee of the Hospital Universitario Puerta de Hierro (Madrid) was consulted before conducting the study. Since the study consisted of an opinion questionnaire, the Clinical Research Ethics Committee considered that ethical approval was unnecessary. All participants received appropriate information on the study and agreed to participate. All documents were duly encoded to ensure data confidentiality complying with the provisions of Organic Law 3/2018, of 5 December, on the protection of Personal Data and guarantee of digital rights.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sánchez-Sánchez, E., Orúe, I., Guerra, J.A. et al. Nutritional management of cancer patients in clinical practice in Spain: patients’ and multidisciplinary health care professionals’ perceptions. Eur J Clin Nutr 77, 454–459 (2023). https://doi.org/10.1038/s41430-022-01251-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-022-01251-x
- Springer Nature Limited