
Abstract
Introduction The success of root canal treatment (RCTx) relies on the technical quality of the root canal filling, often assessed through radiographic evaluation.
Aims This audit aims to evaluate the technical proficiency of Peninsula Dental School (PDS) undergraduate dental students in RCTx, comparing it with established European standards.
Design Conducted as a retrospective study, this evaluation focuses on assessing the technical quality of RCTx performed by undergraduate dental students at PDS across various academic years.
Setting PDS, a primary care-based dental school in the UK, serves as the focal point for this evaluation.
Materials and methods Reviewed 2021-2022 endodontic cases by supervised undergraduates. Analysed radiographs for obturation, voids and errors based on established benchmarks. Randomly selected unbiased cases, assessing voids, filling proximity, missed canals and canal anatomy preservation.
Interventions Comparative analysis of RCTx quality between PDS students and counterparts from other dental schools, exemplified by Dublin Dental University Hospital (DDUH).
Results Findings revealed that 62.07% of single-rooted and 60% of multi-rooted teeth treated by PDS students met European standards.
Discussion The implications highlight the proficiency of PDS students in RCTx, comparing favourably to DDUH.
Conclusion Recommendations emphasise conducting regular educational audits in dental schools to continually enhance RCTx techniques and ensure high-quality clinical teaching.
Key points
-
Favourable comparative performance: Peninsula Dental School students matched or slightly surpassed peers in root canal treatment (RCTx) proficiency, showcasing effective teaching and clinical training.
-
Impact of voids and alternative techniques: voids notably affected RCTx outcomes. Recommending alternate techniques (for example, single cone, hydraulic cement) to diminish voids for better acceptability.
-
Educational audits for enhancement: stressing dental school audits to continually refine clinical teaching. Identifying areas for RCTx improvement ensures ongoing betterment in patient care quality.
Similar content being viewed by others


Introduction
It is highly recommended that undergraduate dental students should be competent enough to undertake the treatment of uncomplicated posterior and anterior teeth before graduation, as shown in the 2013 European Society of Endodontology (ESE) undergraduate guidelines. This can be achieved by first gaining adequate experience in the treatment of incisors, canines, premolars and molars in both the simulated dental learning environment and real clinical environment.1,2,3 In order to prevent compromising patient care after graduation, the standard of root canal treatment (RCTx) completed by undergraduate dental students must be maintained at as high a level as possible.2
It has been shown that the outcome of RCTx is strongly correlated with the technical quality of the root canal filling as assessed radiographically. Likewise, low-technical-quality RCTx has been linked to poor treatment outcomes and increased post-treatment disease.1,2 Radiographic judgement can be used as a helpful tool to indicate the likely success of the root canal filling and as a proxy measure of overall treatment quality being a useful parameter to show the RCTx quality delivered by the practitioner.2,4 This view is supported by several other studies that assessed the technical quality of RCTx carried out by undergraduate dental trainees in various regions.1,2,4,5 It is well-established that radiographs should be taken pre-, intra- and post-operatively during any course of RCTx.6 As a result of several outcome studies, radiographic analyses of a series of technical features correlating to different stages of the RCTx have been introduced.1,2,7 These recommended outcomes have also been incorporated into European quality guidelines.3,6 These ‘best practice' recommendations include the lack of voids radiographically, no evidence of fractured instruments, obturation of all major root canals and no canal deviation from the original anatomy.6
In one UK dental school, an earlier audit demonstrated that the quality of RCTx completed by undergraduate trainees was poor, with only 13% deemed satisfactory.8 The recorded parameters were radiographic quality of the RCTx and the level of root canal filling termination relative to the radiographic apex. Other studies have shown a higher rate of satisfactory RCTx among several UK and Irish dental schools.1,2,3 One of these studies revealed a significant improvement in the quality of the RCTx completed by undergraduate students after incorporation of new technology and teaching practices.1,2 Their evaluation was based on four criteria: presence of voids, distance from the radiographic apex (within 2 mm), unfilled canals and whether the filled canal maintained the original anatomy.2 Notably, their re-audit results revealed remarkable increases in the rate of acceptable root filling quality in single and multi-rooted teeth - 57.5% and 52.7%, respectively - compared with their first audit.1,2 It is worth mentioning that a subjective assessment of the technical quality of RCTx can be directly influenced by the chosen evaluation criteria. The ESE undergraduate curriculum guidelines have highlighted the importance of dental trainees being competent in performing good-quality RCTx during their time as undergraduate dental students.3 Since the introduction of technologies into many dental schools in the UK, there has been a noticeable improvement in the quality of RCTx carried out by undergraduate dental students.2,5,9 This has included using nickel titanium manual and mechanical files, and electronic apex locators. However, the introduction of these new technologies can be expensive. Therefore, some dental schools are continuing the use of stainless-steel hand instruments (K-files).10,11 These additional factors can play a role in the quality of RCTx provided by undergraduate dental students.
To ensure that an adequate standard of RCTx is being delivered by our undergraduate dental students, and in agreement with the clinical director at Peninsula Dental School (PDS), we undertook an audit study in this area.
Undergraduates at PDS commence seeing patients in the third term of first year Bachelor of Dental Surgery, with the bulk of endodontic treatment taking place in the final term of third year and throughout fourth and fifth year. As the school is based in primary care, there is no endodontic department and supervision is provided mainly by visiting general dental practitioners, with support from endodontic specialists on clinic. Students use ProTaper hand files and ProTaper Gold rotary files. The bulk of undergraduate endodontic cases involve hand instrumentation and cold lateral condensation for obturation. Future audits will make greater differentiation with regards to this, but this was not assessed in this audit. Clear assessment criteria for endodontics exist, with endodontic treatment assessed in clinical proficiency assessments (one assessor) and clinical capability assessments (two assessors) as suggested by the ESE undergraduate curriculum guidelines.3 The clinical proficiency assessments cover any tooth or endodontic procedure and are graded ‘excellent', ‘satisfactory', ‘borderline', or ‘unsatisfactory'. Borderline or unsatisfactory do not count to minimal competency requirements. Borderline grades can be remediated for at chairside, but unsatisfactory grades mean the student is suspended from carrying this procedure out and returns to the simulated environment for a bespoke support package. Once this support package is completed satisfactorily, this is signed off by a General Dental Council registrant and the clinical director before the student can commence again on clinic.
The clinical capability assessment, unlike the clinical proficiency assessment, is carried out on a molar tooth and the student has to finish this from access to final obturation. This is similarly graded with two assessors signing this procedure off, ensuring all students are exposed and assessed on multi-rooted teeth to ensure students qualify as safe practitioners with regards to endodontics.
The aim of this quality assurance audit was to evaluate the technical quality of undergraduate de novo RCTx competence cases in the PDS at the University of Plymouth in comparison to agreed European standards. Likewise, results from this audit study would be compared with similar audits carried out in Dublin Dental University Hospital (DDUH). To identify suitable benchmarks, previous audit studies1,2,6and a classic endodontic outcome study by Sjogren (1990) were used.12
Methodology
The audit was registered with the University of Plymouth, Faculty of Health, Research Ethics and Integrity Committee. It was agreed that ethical approval was not required for this audit as this was a retrospective analysis of clinical records and all patient consent for radiographs and endodontic treatment had already been obtained in line with Peninsula Dental Social Enterprise consent policy.
A radiographic analysis was carried out of the number of canals in endodontic cases completed by undergraduate students under supervision of a qualified registrant (completed between 2021 and 2022). In this retrospective audit study, an inclusion criterion was that an acceptable diagnostic post-operative radiograph was available. To prevent selection bias, the cases were randomly selected by a dental nurse from the PDS database, as well as cases with no diagnostic x-ray being discarded and excluded a priori. Based on identified benchmarks from previous studies,1,2,6technical factors were analysed. These included the apical extent of obturation, the presence of voids and technical errors. The evaluation was based on four criteria: presence of voids, root canal filling termination (within 2 mm of radiographic apex), presence of missed canals and preservation of the original anatomy in the filled canals, as previously described.2
Statistical analysis
Contingency tables and chi-squared analysis was used to determine statistically significant improvements in quality in comparison with other studies conducted in secondary care (p <0.05). A pro forma sheet for data collection was generated as previously described in studies.1,2 This audit was conducted by a middle grade doctor (non-consultant hospital doctor [PDS]) and two senior members of the endodontic faculty (consultants).
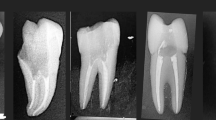
Multi-rooted teeth were analysed and treated as one unit, where if one root was deemed technically inadequate, the unit was categorised as being unacceptable (Fig. 1).

Post-operative intra-oral periapical radiograph of RCTx in tooth 47, showing RCTx which contained no voids, but evidence of under-obturation in mesial root. This categorises tooth 47 as unsatisfactory under the selected criteria of this audit study
Results
A total of 103 teeth were included in this audit study: 45 multi-rooted and 58 single-rooted (Table 1). Each tooth examined in this study had clear evidence of root canal filling material. Demographic information including the prevalence of tooth type and position in this audit study is demonstrated in Table 2.
Single-rooted teeth
From 58 teeth, 96.55% of cases were within 0-2 mm of the radiographic apex. All roots were obturated in 100% of cases and no extrusions were observed in 94.83% of cases. The preparation contained the original canal in 100% of cases, with no evidence of separated instruments in 94.83% of cases and no presence of voids in 70.69% of cases (Fig. 2). Overall (62.07%), the quality of the root canal-treated single-rooted teeth delivered by the undergraduate dental students met the agreed European standard for RCTx.

Post-operative intra-oral periapical radiograph of tooth 23, showing RCTx which contains no voids, is within 0-2 mm of the radiographic apex and contained within the original canal anatomy. This categorises tooth 23 as satisfactory under the selected criteria of this audit study
Multi-rooted teeth
From 45 teeth, 71.11% of cases were within 0-2 mm of the radiographic apex, while the remaining 28.89% were unacceptable due to being under-obturated. All canals were obturated in 100% of cases, without extrusions in 97.78% of cases, the preparation contained the original canal in 100% of cases, with no evidence of separated instruments in 97.78% of cases and no presence of voids in 93.33% of cases (Fig. 3). Overall (60%), the quality of RCTx in multi-rooted teeth delivered by the undergraduate students met the agreed European standard of RCTx.

Post-operative intra-oral periapical radiograph of tooth 46, showing RCTx which contains no voids, is within 0-2 mm of the radiographic apex and contained within the original canal anatomy. This categorises tooth 46 as satisfactory under the selected criteria of this audit study
Discussion
The main purpose of this audit study was to evaluate the technical quality of root canal-treated teeth at PDS, University of Plymouth compared to acceptable European standards and secondary care. This was achieved by evaluating post-operative intra-oral periapical radiographs, retrospectively, and as shown previously.1,2,6 To the best of our knowledge, this is the first audit study of its kind to evaluate the outcome of RCTx in a solely primary care dental school. Furthermore, as a well-established dental school, we intended to investigate whether the introduction of new technologies to the endodontics undergraduate curriculum and accompanying educational changes resulted in higher-quality RCTx compared with other recent audit studies done in secondary care.1,2
It is widely accepted that this kind of audit study only assesses the technical standard of RCTx, which might not be a measure of the longitudinal treatment outcome. Nevertheless, it could be used as a surrogate endpoint of the overall quality of RCTx and their outcome.2,13,14 In this audit study, the quality of RCTx carried out by undergraduate dental students was carried out using similar criteria of assessment to those used by other studies, which also aids comparison.2,6 Interestingly, a re-audit study conducted in secondary care to assess the overall quality of RCTx performed by undergraduate students in the DDUH revealed that acceptable technical treatment overall per tooth amounted to 57.5% in single-rooted teeth and 45.2% in multi-rooted teeth. Although it was not statistically significant, our audit study-recorded percentages were higher - 62.07% and 60% (p = 0 0.31), respectively - suggesting a high-standard-quality of RCTx provided by our undergraduate students in the primary care setup, where non-complex molars were treated (Table 3).
This audit study shows that the technical quality of undergraduate root canal treated teeth in PDS is comparable with that in other dental schools nationwide. Notably, our results confirm that a high-standard-quality of RCTx is delivered by our undergraduate dental students compared to those at other dental schools.2,6 It is widely accepted that the quality of endodontic teaching and level of students' exposure to RCTx might vary across different dental schools.6 Thus, similar education audit studies should be conducted in dental schools to investigate the quality of current clinical teaching and stimulate improvement.
Interestingly, one of the factors most widely affecting RCTx quality is the presence of voids within the obturation. According to Ng et al. (2011),15,16 the presence of voids plays a variable role in the outcome of RCTx, in particular if a void in primary treatment is within 5 mm of the apex. Interestingly, the outcome appears higher than in the absence of voids (86.7% versus 82.8%). Conversely, in secondary treatment, presence of voids is associated with significant lower outcome than when obturation is homogenous (42.9% versus 80.3%). The obturation technique used may also affect the presence of voids. In the current study, cold lateral obturation was used, which can inherently present more radiographic voids compared with single cone and warm vertical obturation techniques.2Adopting a single cone and hydraulic cement obturation technique may reduce the number of voids and improve the overall prevalence of technically acceptable RCTx.
Conclusion
This study revealed that undergraduate dental students at PDS performed RCTx with high technical quality, surpassing the European standard and other dental schools. This indicates that PDS provides effective clinical teaching and training in RCTx as a primary care-based dental school. Further audits are suggested to monitor and enhance the quality of RCTx in dental schools and to compare it with the one obtained by dental schools where endodontic supervision is carried out by endodontic specialists.
References
Kumar M, Duncan H F. Radiographic evaluation of the technical quality of undergraduate endodontic ‘competence' cases in the Dublin Dental University Hospital an audit. J Ir Dent Assoc 2012; 58: 162-166.
Donnelly A, Coffey D, Duncan H F. A re-audit of the technical quality of undergraduate root canal treatment after the introduction of new technology and teaching practices. Int Endod J 2017; 50: 941-950.
De Moor R, Hülsmann M, Kirkevang L-L, Tanalp J, Whitworth J. Undergraduate curriculum guidelines for endodontology. Int Endod J 2013; 46: 1105-1114.
Ng Y-L, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - Part 2. Influence of clinical factors. Int Endod J 2008; 41: 6-31.
Moussa-Badran S, Roy B, Bessart du Parc A S, Bruyant M, Lefevre B, Maurin J C. Technical quality of root fillings performed by dental students at the dental teaching centre in Reims, France. Int Endod J 2008; 41: 679-684.
European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J 2006; 39: 921-930.
Schäfer E, Bürklein S. Impact of nickel-titanium instrumentation of the root canal on clinical outcomes: a focused review. Odontology 2012; 100: 130-136.
Hayes S J, Gibson M, Hammond M, Bryant S T, Dummer P M. An audit of root canal treatment performed by undergraduate students. Int Endod J 2001; 34: 501-505.
Qualtrough A J, Whitworth J M, Dummer P M. Preclinical endodontology: an international comparison. Int Endod J 1999; 32: 406-414.
Balto H, Al Khalifah S, Al Mugairin S, Al Deeb M, Al-Madi E. Technical quality of root fillings performed by undergraduate students in Saudi Arabia. Int Endod J 2010; 43: 292-300.
Khabbaz M G, Protogerou E, Douka E. Radiographic quality of root fillings performed by undergraduate students. Int Endod J 2010; 43: 499-508.
Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod 1990; 16: 498-504.
Bołtacz-Rzepkowska E, Pawlicka H. Radiographic features and outcome of root canal treatment carried out in the Łódź region of Poland. Int Endod J 2003; 36: 27-32.
Burke F M, Lynch C D, Ní Ríordáin, R, Hannigan A. Technical quality of root canal fillings performed in a dental school and the associated retention of root-filled teeth: a clinical follow-up study over a 5-year period. J Oral Rehabil 2009; 36: 508-515.
Ng Y-L, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J 2011; 44: 583-609.
Ng Y-L, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J 2011; 44: 610-625.
Author information
Authors and Affiliations
Contributions
This paper was developed by Araz Ahmed and Ewen McColl, who also oversaw its editing process. Federico Foschi and Henry F. Duncan provided valuable insights and contributed to the editing phase. Araz Ahmed serves as the primary author, while Ewen McColl acts as the corresponding author for this publication.
Corresponding author
Ethics declarations
None of the authors have any conflicts of interest.
The audit was registered with the University of Plymouth, Faculty of Health, Research Ethics and Integrity Committee. It was agreed that ethical approval was not required for this audit as this was a retrospective analysis of clinical records and all patient consent for radiographs and endodontic treatment had already been obtained in line with Peninsula Dental Social Enterprise consent policy. Appropriate consent gained for clinical images and data.
Data availability
For access to the data supporting our study's conclusions, please contact the corresponding author. However, due to patient data confidentiality and in adherence to the Data Protection Act of 2018, we are unable to publicly share this data.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ahmed, A., Foschi, F., Duncan, H. et al. Investigating the technical quality of undergraduate endodontic treatment in a primary care-based dental school. Br Dent J (2024). https://doi.org/10.1038/s41415-024-7130-4
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41415-024-7130-4
- Springer Nature Limited