
Abstract
Neonatal hypoxemic respiratory failure (HRF), a deficiency of oxygenation associated with insufficient ventilation, can occur due to a variety of etiologies. HRF can result when pulmonary vascular resistance (PVR) fails to decrease at birth, leading to persistent pulmonary hypertension of newborn (PPHN), or as a result of various lung disorders including congenital abnormalities such as diaphragmatic hernia, and disorders of transition such as respiratory distress syndrome, transient tachypnea of newborn and perinatal asphyxia. PVR changes throughout fetal life, evident by the dynamic changes in pulmonary blood flow at different gestational ages. Pulmonary vascular transition at birth requires an interplay between multiple vasoactive mediators such as nitric oxide, which can be potentially inactivated by superoxide anions. Superoxide anions have a key role in the pathophysiology of HRF. Oxygen (O2) therapy, used in newborns long before our knowledge of the complex nature of HRF and PPHN, has continued to evolve. Over time has come the discovery that too much O2 can be toxic. Recommendations on the optimal inspired O2 levels to initiate resuscitation in term newborns have ranged from 100% (pre 1998) to the currently recommended use of room air (21%). Questions remain about the most effective levels, particularly in preterm and low birth weight newborns. Attaining the appropriate balance between hypoxemia and hyperoxemia, and targeting treatments to the pathophysiology of HRF in each individual newborn are critical factors in the development of improved therapies to optimize outcomes.
Similar content being viewed by others


Introduction
Hypoxemic respiratory failure (HRF) is a deficiency of oxygenation associated with insufficient ventilation. HRF can occur in neonates owing to parenchymal lung disease, such as meconium aspiration syndrome, pneumonia or respiratory distress syndrome, secondary to lung hypoplasia as in congenital diaphragmatic hernia, or as a consequence of pulmonary vascular remodeling in the absence of lung disease (idiopathic pulmonary hypertension). HRF may be associated with unsuccessful cardiovascular transition when pulmonary vascular resistance (PVR) fails to decrease at birth, leading to persistent pulmonary hypertension of newborn (PPHN).1, 2, 3
In the United States, the incidence of respiratory failure requiring mechanical ventilation is estimated at ~18 per 1000 live births.4 HRF is associated with considerable mortality (between 10% and 15%) and morbidity, including hospitalization and disability.5, 6 Oxygen (O2) supplementation is an important component of HRF management. O2 therapy has evolved from its early use to current approaches, based on our increasing understanding of HRF. This article discusses the etiology and pathophysiology of HRF in neonates, as well as the evolution of O2 therapy in the management of this condition. It is part of a series summarizing presentations and discussions from a roundtable discussion focused on HRF in neonates (see the Introduction to this issue).
Fetal circulation and PVR
In fetal life there are two sources of preload to the left ventricle: (1) the primary source, oxygenated blood from the placenta to the umbilical vein through the foramen ovale, with 85% O2 saturation and (2) deoxygenated blood returning from the lung, with ~45% O2 saturation.7, 8, 9 However, pulmonary blood flow is low in the fetus, with the lungs receiving only about one-fifth of combined cardiac ventricular output at term gestation.7 Because of the low volume of pulmonary venous return, the combination of these two sources of preload in the left ventricle results in a 65% blood O2 saturation that circulates to the fetal brain and coronary circulation. The O2 level in blood to the brain is higher than that circulating to the lower half of the body (~55% O2 saturation) including umbilical arteries.7, 10
The dynamic nature of the pulmonary circulation and the O2 gradient across the placenta maintains O2 delivery to the fetal brain in a narrow window. Maternal arterial blood in the pregnant ewe has an arterial partial pressure of oxygen (PaO2) of 90 to 100 mm Hg. There is a large partial pressure of oxygen (PO2) gradient across the placenta, with a PO2 of 32 to 35 mm Hg in the umbilical vein, protecting the fetus from exposure to high O2 levels. Left ventricular and ascending aorta blood perfusing the brain has a PO2 of 25 to 28 mm Hg (65% O2 saturation). Administering 100% O2 to the ewe raises PaO2 to >400 mm Hg but the umbilical venous PO2 increases only to 40 to 50 mm Hg and fetal ascending aorta PaO2 increases to only 30 to 35 mm Hg (Figure 1).7 The reciprocal, complementary relationship between oxygenated flow across foramen ovale and deoxygenated blood flowing from the pulmonary veins to the left ventricle can partly explain this O2-buffering effect. Maternal hyperoxemia increases fetal left pulmonary arterial blood flow from 20±10 to 68±18 mL/min,11 possibly by increasing pulmonary arterial PO2. This hyperoxic effect in turn increases pulmonary venous return of desaturated blood entering the left ventricle, thereby lowering the O2 levels to the brain. Thus, even though the mother’s PaO2 is increased by 300 mm Hg, the PaO2 in the ascending aorta of the fetus only increases by 5 to 7 mm Hg.7 Furthermore, pulmonary vasodilation reduces right-to-left shunt across the foramen ovale. In a human study, fetuses that had a high pulmonary foramen ovale shunt (that is, a bigger component of left ventricular input from umbilical venous return) had a low pulmonary venous return. The opposite was true for fetuses that had a low pulmonary foramen ovale shunt, and a high pulmonary venous return.12 Thus, the placenta and pulmonary circulation play a vital role in reducing O2 toxicity to the fetal organs.

Protective role of placenta and fetal pulmonary circulation from maternal hyperoxia: administering 100% oxygen (solid bars) to the ewe raises maternal PaO2 by over 300 mm Hg compared with 21% oxygen (hatched bars) but the umbilical venous (UV) PO2 increases by only 10 to 15 mm Hg, whereas the fetal ascending arterial PO2 increases by only 5 mm Hg but markedly increases pulmonary blood flow compared with 21% oxygen. Copyright Drs Satyan Lakshminrusimha and Ola D Saugstad. PaO2, arterial partial pressure of oxygen; PO2, partial pressure of oxygen.
During fetal life, when the placenta is the organ of gas exchange, placental vascular resistance is low and fetal PVR is high. Blood flow is diverted from the pulmonary artery to the aorta and umbilical arteries toward the placenta.3, 13 As previously mentioned, PVR is known to change throughout fetal life as demonstrated by the varying levels of blood circulating to the lungs during different gestation stages (Figure 2).3, 14 At 20 weeks (canalicular stage), when the fetus is immature, only 13% of combined ventricular output circulates to the lungs. The cross-sectional area of pulmonary vasculature is low in the canalicular stage, resulting in high PVR. At 30 weeks (saccular stage), an increase in pulmonary blood vessels leads to a decrease in PVR and 25% to 30% of combined ventricular output goes to the lungs. At 38 weeks’ gestation (alveolar stage, pre-birth), active vasoconstriction drops the amount of combined ventricular output circulating the lungs to ~19% to 23% in spite of an increase in pulmonary vasculature. The decrease in pulmonary blood flow at this gestational age is secondary to the fact that pulmonary vasculature develops sensitivity to O2, leading to fetal hypoxic pulmonary vasoconstriction and elevation of PVR.3, 14, 15

Changes in pulmonary vascular resistance (PVR) and systemic vascular resistance (SVR) during gestation. During the canalicular phase of lung development, high PVR is caused by low density of the vasculature. In the saccular stage, broad intersaccular septae contain the double capillary network and, with increasing vascular density, PVR decreases. In the alveolar phase, despite the rapid increase in the number of small pulmonary arteries, high PVR is maintained by active vasoconstriction. The dashed line represents the delay in decrease of PVR observed following elective C-section. SVR markedly increases after occlusion of the umbilical cord and removal of the low-resistance placental circuit from the systemic circulation.3 Copyright Dr Satyan Lakshminrusimha.
The U-shaped curve of PVR in the last half of gestation is mimicked by regional data on the use of inhaled nitric oxide (iNO), as a vasodilator, in babies born at various gestational ages (as a surrogate for the incidence of moderate-to-severe PPHN). This pattern was especially apparent prior to the National Institutes of Health 2010 Consensus Development Conference Statement indicating insufficient evidence to recommend routine use of iNO in preterm infants,16 but continues to be reflected in variations in local practices. Of note, data from California show that the use of iNO is lowest ~30 to 33 weeks’ gestational age,17 reflective of the low PVR that occurs at this time in fetal development. A similar pattern of iNO use was observed among neonatal level III patients given invasive ventilation in the Australia and New Zealand Neonatal Network in 2013 (18% at <24 weeks, 5.5% at 30 to 33 weeks and 17.7% at 37 to 43 weeks postmenstrual age at birth.18
Transition from in utero to birth: factors to consider in PPHN
Ventilation of the lungs at birth reduces PVR, and the removal of the low vascular resistance placenta from the systemic circulation at birth increases systemic vascular resistance (Figure 2).3 The mode of delivery affects PVR. A vaginal birth is associated with a rapid reduction in fetal PVR, whereas birth by elective cesarean section slows reduction in PVR, as does the use of delayed (or late) cord clamping.3, 19, 20
With the increasing use of delayed cord clamping, it is important to assess whether this technique affects the pulmonary vascular transition at birth. In clinically normal, full-term, newborn infants (N=32) early cord clamping (<10 s after birth, n=10) resulted in a rapid decline in the pulmonary artery to aortic pressure ratio, whereas late cord clamping (3 to 5 min until umbilical pulsations stop, n=22), resulted in a slow decline.20 However, there is no evidence of increased respiratory distress or neonatal intensive care unit admission among term infants following late cord clamping.21 In fact, there may be a trend toward higher incidence of PPHN associated with early cord clamping and lower hematocrit presumed to be due to the absence of placenta transfusion.22 This may be as a result of increased hemoglobin levels in the blood following placental transfusion that contribute to an increased O2 carrying capacity.
The pathophysiology of HRF
Nitric oxide (NO), a cellular signaling molecule, is a powerful vasodilator that modulates pulmonary vascular tone.23 It is one of the most volatile molecules in the body, avidly combining with superoxide anion to form peroxynitrite,3, 24, 25, 26 which causes pulmonary vasoconstriction.27 A key factor determining the bioavailability of NO in a tissue is the local concentration of superoxide anions. Minimizing the superoxide anion concentration may enhance the effect of endogenous NO.
The superoxide anion concentration is dependent on its rate of production and the activity of various superoxide dismutases (SOD).24 Extracellular SOD, an enzymatic scavenger of extracellular superoxide highly expressed in the lungs and vascular smooth muscle, can reduce superoxide levels and contribute to the modulation of vascular O2 levels.24, 28, 29 Increased superoxide anions have been demonstrated in PPHN induced by antenatal ductal ligation in fetal lambs. Vascular adventitia provides an active source of superoxide anions and can inactivate NO.30 Exogenous NO delivered from the adventitial side does not cause vasodilation;31, 32 and in remodeled vessels, the thickened, superoxide anion-producing adventitia may further blunt the effect of NO.33
In the fetal lamb model of PPHN, which in many ways resembles a human infant with PPHN, there is an increase in the expression of genes that induce pulmonary vasoconstriction and a reduction in those that induce vasodilation.34 Superoxide is twofold higher and hydrogen peroxide is fourfold higher in the pulmonary arteries of lambs with PPHN compared with controls without PPHN, and both enhance pulmonary vasoconstriction.33, 35 Superoxide anions also inactivate NO to produce peroxynitrite, which is a potent vasoconstrictor and cytotoxic agent.24, 36 Peroxynitrite formation is also increased when ventilated PPHN lambs are exposed to 100% O2. Administration of catalase or allopurinol, which reduces production of reactive O2 species, reduced pulmonary hypertension in young pigs induced by hypoxanthine and xanthine oxidase.37 Furthermore, the administration of intratracheal recombinant human SOD was shown to reduce superoxide levels and improve oxygenation in PPHN lambs.36 Similarly, administration of catalase or allopurinol, which reduces production of reactive O2 species, reduced pulmonary hypertension induced by hypoxanthine and xanthine oxidase in young pigs.37 Hydrogen peroxide has a possible role in downregulating extracellular SOD activity and further contributing to the pathogenesis of PPHN. This is evident from increased pulmonary arterial hydrogen peroxide, which decreases extracellular SOD activity in PPHN. Thus, removal of hydrogen peroxide by catalase or other scavengers may restore extracellular SOD function, thereby facilitating vasodilation.38
Common etiologies in HRF and PPHN
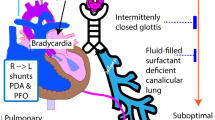
Transient tachypnea of newborn has been associated with HRF and PPHN. For example, following elective cesarean section, newborns with transient tachypnea of newborn who have hypoxemia may be placed on high concentrations of inspired O2 (~100%) by hood or low-flow nasal cannula (without any positive pressure). In these cases absorption atelectasis can develop, resulting in increasing O2 requirements and respiratory failure (Figure 3). Furthermore, the formation of reactive oxygen species from the high alveolar O2 concentrations can increase pulmonary vascular reactivity thereby contributing to PPHN.3, 19 The term ‘malignant transient tachypnea of newborn’ has been used to describe severe respiratory morbidity and subsequent mortality in newborns delivered by elective cesarean section who developed PPHN.19, 39 One possible strategy when managing these newborns (and to prevent malignant transient tachypnea of newborn) may be early use of positive pressure to inflate and recruit the lungs versus merely administering high amounts of O2 without positive pressure.

Absorption atelectasis—administration of high concentration of inspired oxygen without positive pressure in an infant with respiratory distress can lead to nitrogen washout and alveolar collapse. Atelectasis can result in V/Q mismatch, shunting and hypoxemic respiratory failure with PPHN. Copyright Drs Bobby Mathew and Satyan Lakshminrusimha. Modified from Polin RA, Yoder MC. Workbook in Practical Neonatology, 5th edn. St Louis, MO: Saunders; 2014.
Perinatal asphyxia is another well-known predisposing factor for PPHN. Perinatal asphyxia can interfere with pulmonary transition during birth, thereby impeding the decrease in PVR and increasing the risk for PPHN.3, 40 Various mechanisms cause respiratory failure in asphyxia, including fetal hypoxemia, ischemia, meconium aspiration, ventricular dysfunction and acidosis, all of which can increase PVR.3, 40
In asphyxiated term neonates, hypothermia has been established as an effective neuroprotective strategy,41 which could potentially exacerbate PPHN. In addition to direct effects, hypothermia affects blood gas parameters including pH and partial pressure of carbon dioxide.42 Partial pressure of carbon dioxide is known to affect vascular tone,43 raising potential concerns that therapeutic hypothermia may increase the risk of PPHN. In a randomized controlled trial, infants (gestational age ⩾36 weeks) with moderate or severe hypoxic–ischemic encephalopathy, were assigned to standard therapy at either 37 °C (control group, n=106) or to whole-body cooling (hypothermia group, n=102) at 33.5 °C. Of the infants in the control group 22% had PPHN, whereas 25% of infants in the hypothermia group had PPHN (P=not significant).44 Pooled analyses of other randomized trials have not shown an increase in the incidence of PPHN in neonates undergoing hypothermia.45 The effect of the degree of hypothermia on PPHN was also examined in a subsequent study that compared the temperature and duration of cooling in the same patient population (N=364).46 In this study, whole-body hypothermia at 32 °C, compared with 33.5 °C, changed the rate of PPHN from 25% to 34% (not significant); however, the need for iNO therapy changed from 24% (33.5 °C) to 34% (32 °C) (P<0.05) and extracorporeal membrane oxygenation from 4% (33.5 °C) to 9% (32 °C) (P<0.05).46 Thus, although standard hypothermia at 33.5 °C does not worsen PPHN, it is important to avoid deeper hypothermia (⩽32 °C). Frequent blood gas monitoring is mandatory in these patients, which can be done either by the α-stat (reporting blood gases at patient’s temperature) or pH-stat (reporting at 37 °C) methods.42 It is important to be aware of the method used, as it is possible to hypoventilate or hyperventilate a neonate, which can have positive or negative consequences on pulmonary and cerebral circulation. For example, an infant on whole-body hypothermia with a PaCO2 of 49 mm Hg at 33.5 °C (α-stat) may be reported as 54 mm Hg at 37 °C (pH-stat). If the clinicians use same PaCO2 parameters (such as 45 to 50 mm Hg) for both methods, the α-stat method results in better preservation of cerebral circulation but can reduce pulmonary blood flow. Similarly, hypothermia shifts the O2 dissociation curve to the left, and decreases PaO2 at a given peripheral oxygen saturation. Careful attention to gas exchange is therefore vital during therapeutic hypothermia.
The primary goal of PPHN treatment is to improve O2 delivery to the tissues and decrease PVR by selective pulmonary vasodilation.47, 48 Various techniques have been employed including intubation, ventilator support and hyperventilation to induce hypocarbia and alkalosis, the latter producing a direct vasodilatory effect on pulmonary vasculature.47 Intravenous bicarbonate and tromethamine have also been used when ventilation does not produce sufficient alkalization to achieve the desired (alkaline) pH, as acidosis can act as a pulmonary vasoconstrictor.47, 48 However, such therapies are associated with increased need for extracorporeal membrane oxygenation and neurodevelopmental concerns, and are no longer recommended.49 Previous therapies have also included intravenous dilators such as prostacyclin and tolazoline; however, these can produce non-selective effects on the systemic circulation, leading to hypotension.48 A more detailed discussion on the evolving knowledge in O2 therapy is provided below. Further discussion regarding current and investigational therapeutic approaches for PPHN is provided in the articles that follow within this publication.
The evolution of O2 use in neonates
O2 therapy for neonatal conditions such as asphyxia, HRF and PPHN, was in use well before their complex etiologies and pathologies were known. The use of O2 in the delivery room increased following the description in 1861 of cerebral palsy in newborns with asphyxia,50, 51, 52 and again after the introduction of the Apgar score in the mid-1950s.53
Ongoing investigation has served to increase our understanding of both the life-giving and toxic nature of O2 therapy (Figure 4).54, 55, 56, 57, 58, 59 One important discovery was that O2 was toxic based on its ability to generate free O2 radicals.60 Hypoxanthine, a free radical generator and breakdown product of adenosine triphosphate, has been shown to accumulate in hypoxic newborns.61 Oxidation of hypoxanthine to uric acid results in the generation of free radicals.62 A study in dogs showed that resuscitation with O2 increased hypoxanthine levels exponentially in the first 12 min.63 Experiments in rabbits established that antioxidant enzyme activities were low in fetal life, and that these increased during late gestation as important preparations for birth. Premature birth may affect the ability to tolerate hyperoxic exposure,64 which forms a basis of the concept of O2 radical disease in the newborn.65 Investigation into the existence of O2 radical disease in neonatology established that oxidative stress and inflammation were closely associated, and that factors, other than O2, could generate oxidative stress in preterm newborns (Figure 5).65, 66, 67

Key milestones in oxygen use from its discovery as a gas in the atmosphere to its use in neonatology. ELBWI, extremely low birth weight infants; ILCOR, International Liaison Committee on Resuscitation; NEOPROM, NEOnatal oxygenation PROspective Meta-analyses; WHO, World Health Organization.72 Copyright Dr Satyan Lakshminrusimha and Ola D Saugstad.

‘Oxygen radical disease’ in preterm neonates manifesting as bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), necrotizing enterocolitis (NEC), patent ductus arteriosus (PDA), periventricular leukomalacia (PVL) and mortality are presented in the form of a ‘diagrammatic forest plot’. NO, nitric oxide; PPHN, persistent pulmonary hypertension of newborn. Copyright Drs Satyan Lakshminrusimha and Ola D Saugstad.
Resuscitation of term and near-term babies (~⩾36 weeks)
Although earlier approaches to ventilation often included use of 100% O2, results of the Resair 1 pilot study and Resair 2 clinical study (N=591) in the 1990s demonstrated the feasibility of resuscitating asphyxiated newborns with room air just as efficiently as with 100% O2.68, 69
Subsequent meta-analyses showed that neonatal mortality was reduced by ~30% when room air (21% O2) was used instead of 100% O2 to resuscitate term or late preterm babies.70, 71, 72 One explanation for this finding may be related to the results from another study, in which term neonates resuscitated with 100% O2 exhibited biochemical findings reflective of prolonged oxidative stress even after 4 weeks of postnatal life, compared with neonates resuscitated with room air. In addition, there was an increase in markers of myocardial and kidney injury in neonates resuscitated with 100% O2 compared with those who received air (Figure 6).73, 74 These findings led to a worldwide change in oxygenation and resuscitation practices in neonates. In 2010, the International Liaison Committee on Resuscitation recommended using air (21%) rather than 100% O2, when resuscitating term or near-term newborns in need of positive pressure ventilation at birth.75

Consequences (short- and long-term) of 100% oxygen resuscitation in term neonates: the course of events following resuscitation of neonates with 21 or 100% oxygen. The blue lines represent fetal PaO2 levels; the red line and pink line represent postnatal PaO2 levels with 100 and 21% oxygen resuscitation, respectively. The shaded red and pink areas represent the degree of free radical injury following 100% and 21% oxygen resuscitation. Short-term and long-term consequences of 100% oxygen resuscitation are shown in the figure. Copyright Drs Saugstad and Lakshminrusimha. PaO2, arterial partial pressure of oxygen.
The potential adverse effects of resuscitating with 100% O2 were demonstrated in a study in which infants ⩾36 weeks’ gestation with perinatal acidemia and hyperoxemia on their admission blood gas had a higher incidence of hypoxic–ischemic encephalopathy than those without hyperoxemia (58% vs 27%; P=0.003).76 The effect of 100% O2 has also been shown in newborn lambs with PPHN delivered by cesarean section. Resuscitation with 100% O2 did not enhance pulmonary vasodilation compared with 21% and 50% O2. In fact, 100% O2 impaired the subsequent response to iNO in these lambs (Figure 7).77, 78 Thus, although hypoxia markedly increased PVR, hyperoxemia did not confer significant additional pulmonary vasodilation in lambs with PPHN.77

The effect of initial resuscitation with 21%, 50% and 100% O2 in newborn lambs with acute PPHN induced by thromboxane analog on subsequent pulmonary vasodilation by inhaled nitric oxide (20 ppm) and infusion of acetylcholine. The decrease in PVR in response to inhaled nitric oxide and acetylcholine, as a percent of baseline, was significantly higher in PPHN lambs resuscitated with 21% O2 compared with 100% (*P<0.05).79, 80 Ach, acetylcholine; FiO2, fraction of inspired oxygen; NO, nitric oxide; PPHN, persistent pulmonary hypertension of newborn; PVR, pulmonary vascular resistance.
Resuscitation of preterm and/or low birth weight babies (<32 weeks)
A few meta-analyses have investigated the issue of the optimal O2 concentration for resuscitation of preterm and/or low birth weight babies. A systematic review and meta-analysis of six randomized controlled trials (N=484) determined the effect of using lower (21% to 50%) versus higher (>50%) O2 concentrations for delivery room transition support of preterm newborns (born before 32 weeks’ gestation) on mortality and morbidity. Lower O2 concentrations were associated with reduced risk of death (pooled risk ratio 0.65, 95% confidence interval: 0.43 to 0.98), but this effect disappeared when four trials with allocation concealment were included. Thus, there was no strong evidence that using lower versus higher O2 concentrations for delivery room transition support for preterm infants conferred benefits or harm.79
A systematic review and meta-analysis of 10 randomized studies in 677 newborns ⩽32 weeks' gestation showed the relative risk for mortality as 0.62 (95% confidence interval: 0.37 to 1.04, I2=0%, Pheterogeneity=0.88) for those receiving low (0.21 to 0.30, n=321) versus high (0.60 to 1.0, n=356) initial fraction of oxygen. There was no significant association for bronchopulmonary dysplasia (BPD) or intraventricular hemorrhage when comparing low and high initial fraction of oxygen. These findings suggest that premature babies (⩽32 weeks’ gestation) in need of stabilization in the delivery room should be given an initial fraction of oxygen of 0.21 to 0.30.80 More recently, the TO2RPIDO study reported a higher mortality in babies <29 weeks’ gestation who were resuscitated with air (21%) compared with 100% O2,81 The Canadian neonatal intensive care units have reported higher risk of severe neurologic injury or death among preterm infants ⩽27 weeks’ gestation following a change in practice to initiating resuscitation with either 21% O2 or an intermediate O2 concentration.82 These findings demonstrate the difficulty in establishing guidelines, particularly for the most premature infants <32 weeks of gestational age.
O2 saturation levels in premature newborns (<28 weeks’ gestation), beyond delivery, have been assessed in the NEOnatal oxygenation PROspective Meta-analyses (NEOPROM), a collaborative study examining the effect of low and high O2 saturation levels. NEOPROM assessed data from SUPPORT (Surfactant, Positive Pressure and Pulse Oximetry Randomized Trial), the three BOOST II (Benefits of Oxygen Saturation Targeting) studies and the COT (Canadian Oxygen Trial) study in extremely low birth weight newborns (N=4911) at <28 weeks’ gestation. O2 targets in the low saturation group were 85% to 89%, versus 91% to 95% in the high O2 group. To date, NEOPROM are the largest meta-analyses in preterm newborns <28 weeks’ gestation at birth.83 Findings from the meta-analysis of these studies showed the relative risk for mortality and necrotizing enterocolitis was increased, whereas severe retinopathy of prematurity (ROP) was decreased, in low compared with high O2 saturation ranges in these extremely low birth weight infants. Overall, there was an 18% increased risk of mortality in the low saturation target.83 The recommendation from this study was that functional O2 saturation should be targeted at 90% to 95% in newborns with a gestational age of <28 weeks until 36 weeks’ postmenstrual age.83
A more recent meta-analysis of NEOPROM accounted for the risk of bias of each included study, as well as the quality of evidence for each outcome. In this analysis, preterm newborns (<28 weeks’ gestation at birth) administered a 91% to 95% O2 target had a lower mortality before hospital discharge, compared with those managed within an 85% to 89% O2 target. In addition, necrotizing enterocolitis occurred less frequently in the 91% to 95% O2 group. However, there was no difference in death or disability at 24 months, BPD, ROP, neurodevelopmental outcomes, or hearing loss at 24 months. Based on the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) criteria, the quality of evidence for the outcomes in this analysis was graded as moderate to low.84
Findings from NEOPROM present an ‘oxygen dilemma,’ in that, if O2 saturation targets are kept high, mortality and necrotizing enterocolitis is reduced but other complications may arise (for example, ROP, BPD), and vice versa when O2 targets are low. Thus, identifying the optimum O2 concentration in extremely small (low birth weight or preterm (<28 weeks)) newborns remains an important question to be addressed. The current available data make it difficult to recommend appropriate guidelines, particularly in newborns with a gestational age <28 weeks. The recent post hoc analysis of the SUPPORT trial showed that increased mortality in infants randomized to the low peripheral oxygen saturation target group was predominantly due to the high rate of death before discharge among small-for-gestational-age infants. The leading causes of mortality in preterm small-for-gestational-age infants were respiratory distress syndrome and BPD, which may have been accompanied by PH and HRF.85 These results suggest that O2 saturation targeting among preterm infants may even benefit from a ‘precision-medicine’ individualized approach based on growth (small-for-gestational-age vs appropriate-for-gestational-age infants), pulmonary (respiratory distress syndrome, BPD and PPHN) and ophthalmological (presence of pre-threshold ROP) status.
Considerations when interpreting clinical trial findings that target O2 saturation levels
For clinicians, interpreting results from clinical trials that target precise O2 saturation levels can be challenging. A potential consideration for future such trials may be to include a third group (in addition to high and low O2 saturation targets or alarm limits), to reflect real-world clinical practice with a wider gap between lower and higher O2 saturation alarm limits that can be effectively achieved by bedside nurses. This type of study design might suggest a medium mean between no increased mortality and less ROP.
But to date, no study has provided definitive evidence and recommendations for the optimum O2 saturation targets in preterm newborns (<28 weeks’ gestation at birth). This poses an important question that remains to be addressed.
It is likely that there will be more genomic studies in this area in the future. One such study used a hypoxia mouse model to assess how hyperoxic reoxygenation, following hypoxia, affected transcriptional changes in the newborn lung.86 Findings from this study suggest that acute hyperoxia induces hypoxia-inducible factor 1 targets (or example, Vegfc, Adm and Aqp1) irrespective of the reoxygenation regimen. In addition, hyperoxic reoxygenation mediated ~70% of gene expression changes, particularly pathways regulating cell growth and survival (for example, mTOR signaling pathway). Effects included upregulation of genes involved in inflammation, inhibition of cell growth, angiogenesis and stress; whereas there was downregulation of genes involved in oxidative phosphorylation. Thus, adenosine triphosphate production may be impacted or reduced when newborns are resuscitated with 60% to 100% O2.86
Summary
The newborn period presents a unique time during which there is reduced protection from oxidative stress and reduced oxidative phosphorylation. Failed circulatory transition at birth, pulmonary parenchymal lung disease, pulmonary alveolar/vascular hypoplasia and asphyxia are key factors in HRF and PPHN. Excessive O2 has a role in the exacerbation of PPHN and possibly of hypoxic to ischemic encephalopathy. A better understanding of hemodynamic, biochemical and histologic changes in HRF and PPHN will enhance our ability to develop new therapeutic strategies.
The challenge remains as to how best to approach resuscitation with O2, particularly in preterm newborns. Attaining the balance between hypoxia and hyperoxia is critical to prevent iatrogenic toxicity and optimize outcomes. There should be consideration of the varied pathophysiology of HRF to design appropriate treatments and to effectively employ those currently available.
References
Clark RH . The epidemiology of respiratory failure in neonates born at an estimated gestational age of 34 weeks or more. J Perinatol 2005; 25: 251–257.
Konduri GG, Kim UO . Advances in the diagnosis and management of persistent pulmonary hypertension of the newborn. Pediatr Clin North Am 2009; 56: 579–600.
Lakshminrusimha S . The pulmonary circulation in neonatal respiratory failure. Clin Perinatol 2012; 39: 655–683.
Angus DC, Linde-Zwirble WT, Clermont G, Griffin MF, Clark RH . Epidemiology of neonatal respiratory failure in the United States: projections from California and New York. Am J Respir Crit Care Med 2001; 164: 1154–1160.
Eriksen V, Nielsen LH, Klokker M, Greisen G . Follow-up of 5- to 11-year-old children treated for persistent pulmonary hypertension of the newborn. Acta Paediatr 2009; 98: 304–309.
Lipkin PH, Davidson D, Spivak L, Straube R, Rhines J, Chang CT . Neurodevelopmental and medical outcomes of persistent pulmonary hypertension in term newborns treated with nitric oxide. J Pediatr 2002; 140: 306–310.
Rudolph A . The fetal circulation. Congenital Diseases of the Heart: Clinical-Physiological Considerations, 3rd edn. Wiley-Blackwell: Hoboken, NJ, USA, 2009, pp 1–24.
Gao Y, Raj JU . Regulation of the pulmonary circulation in the fetus and newborn. Physiol Rev 2010; 90: 1291–1335.
Kiserud T . Physiology of the fetal circulation. Semin Fetal Neonatal Med 2005; 10: 493–503.
Lakshminrusimha S, Steinhorn RH . Pathophysiology of PPHN. Fetal and Neonatal Physiology, 5th edn. Elsevier: Philadelphia, PA, USA. In press (note: expected publication is July 2016. Chapter 155. ISBN 9780323352147).
Konduri GG, Gervasio CT, Theodorou AA . Role of adenosine triphosphate and adenosine in oxygen-induced pulmonary vasodilation in fetal lambs. Pediatr Res 1993; 33: 533–539.
Prsa M, Sun L, van AJ, Yoo SJ, Grosse-Wortmann L, Jaeggi E et al. Reference ranges of blood flow in the major vessels of the normal human fetal circulation at term by phase-contrast magnetic resonance imaging. Circ Cardiovasc Imaging 2014; 7: 663–670.
Lakshminrusimha S, Steinhorn RH . Pulmonary vascular biology during neonatal transition. Clin Perinatol 1999; 26: 601–619.
Rasanen J, Wood DC, Weiner S, Ludomirski A, Huhta JC . Role of the pulmonary circulation in the distribution of human fetal cardiac output during the second half of pregnancy. Circulation 1996; 94: 1068–1073.
Kinsella JP, Ivy DD, Abman SH . Ontogeny of NO activity and response to inhaled NO in the developing ovine pulmonary circulation. Am J Physiol 1994; 267: H1955–H1961.
National Institutes of Health. NIH Consensus Development Conference Statement: Inhaled Nitric Oxide Therapy for Premature Infants. 27–29 October 2010.
Handley SC, Steinhorn RH, Hopper AO, Govindaswami B, Van Meurs KP, Ariagno RL et al. Patterns of Inhaled Nitric Oxide Use in California NICUs. Abstract presented at the 2015 Pediatric Academic Societies' Annual Meeting; 25–28 April 2015; San Diego, CA, USA. Abstract 2894.369.
Chow SSW, Le Marsney R, Hossain S, Haslam R, Lui K . Report of the Australian and New Zealand Neonatal Network. 2013. Report No. 18.
Ramachandrappa A, Jain L . Elective cesarean section: its impact on neonatal respiratory outcome. Clin Perinatol 2008; 35: 373–393.
Arcilla RA, Oh W, Lind J, Gessner IH . Pulmonary arterial pressures of newborn infants born with early and late clamping of the cord. Acta Paediatr Scand 1966; 55: 305–315.
McDonald SJ, Middleton P, Dowswell T, Morris PS . Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Evid Based Child Health 2014; 9: 303–397.
Totapally B, Raju N, Perlman M . Decreased placental transfusion may lead to persistent pulmonary hypertension of the newborn (PPHN) 1156. Pediatr Res 1998; 43: 198.
Muraca MC, Negro S, Sun B, Buonocore G . Nitric oxide in neonatal hypoxemic respiratory failure. J Matern Fetal Neonatal Med 2012; 25 (Suppl 1): 47–50.
Faraci FM, Didion SP . Vascular protection: superoxide dismutase isoforms in the vessel wall. Arterioscler Thromb Vasc Biol 2004; 24: 1367–1373.
Saugstad OD . Mechanisms of tissue injury by oxygen radicals: implications for neonatal disease. Acta Paediatr 1996; 85: 1–4.
Dawson TM, Dawson VL, Snyder SH . A novel neuronal messenger molecule in brain: the free radical, nitric oxide. Ann Neurol 1992; 32: 297–311.
Steinhorn RH . Nitric oxide and beyond: new insights and therapies for pulmonary hypertension. J Perinatol 2008; 28 (Suppl 3): S67–S71.
Marklund SL . Extracellular superoxide dismutase and other superoxide dismutase isoenzymes in tissues from nine mammalian species. Biochem J 1984; 222: 649–655.
Jung O, Marklund SL, Geiger H, Pedrazzini T, Busse R, Brandes RP . Extracellular superoxide dismutase is a major determinant of nitric oxide bioavailability: in vivo and ex vivo evidence from ecSOD-deficient mice. Circ Res 2003; 93: 622–629.
Wang HD, Pagano PJ, Du Y, Cayatte AJ, Quinn MT, Brecher P et al. Superoxide anion from the adventitia of the rat thoracic aorta inactivates nitric oxide. Circ Res 1998; 82: 810–818.
Steinhorn RH, Morin FC III, Russell JA . The adventitia may be a barrier specific to nitric oxide in rabbit pulmonary artery. J Clin Invest 1994; 94: 1883–1888.
Lakshminrusimha S, Russell JA, Gugino SF, Ryan RM, Mathew B, Nielsen LC et al. Adjacent bronchus attenuates pulmonary arterial contractility. Am J Physiol Lung Cell Mol Physiol 2006; 291: L473–L478.
Brennan LA, Steinhorn RH, Wedgwood S, Mata-Greenwood E, Roark EA, Russell JA et al. Increased superoxide generation is associated with pulmonary hypertension in fetal lambs: a role for NADPH oxidase. Circ Res 2003; 92: 683–691.
Black SM, Johengen MJ, Soifer SJ . Coordinated regulation of genes of the nitric oxide and endothelin pathways during the development of pulmonary hypertension in fetal lambs. Pediatr Res 1998; 44: 821–830.
Wedgwood S, Steinhorn RH, Bunderson M, Wilham J, Lakshminrusimha S, Brennan LA et al. Increased hydrogen peroxide downregulates soluble guanylate cyclase in the lungs of lambs with persistent pulmonary hypertension of the newborn. Am J Physiol Lung Cell Mol Physiol 2005; 289: L660–L666.
Lakshminrusimha S, Russell JA, Wedgwood S, Gugino SF, Kazzaz JA, Davis JM et al. Superoxide dismutase improves oxygenation and reduces oxidation in neonatal pulmonary hypertension. Am J Respir Crit Care Med 2006; 174: 1370–1377.
Sanderud J, Norstein J, Saugstad OD . Reactive oxygen metabolites produce pulmonary vasoconstriction in young pigs. Pediatr Res 1991; 29: 543–547.
Wedgwood S, Lakshminrusimha S, Fukai T, Russell JA, Schumacker PT, Steinhorn RH . Hydrogen peroxide regulates extracellular superoxide dismutase activity and expression in neonatal pulmonary hypertension. Antioxid Redox Signal 2011; 15: 1497–1506.
Keszler M, Carbone MT, Cox C, Schumacher RE . Severe respiratory failure after elective repeat cesarean delivery: a potentially preventable condition leading to extracorporeal membrane oxygenation. Pediatrics 1992; 89: 670–672.
Lapointe A, Barrington KJ . Pulmonary hypertension and the asphyxiated newborn. J Pediatr 2011; 158: e19–e24.
Jacobs S, Hunt R, Tarnow-Mordi W, Inder T, Davis P . Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev 2007; CD003311.
Groenendaal F, De Vooght KM, van BF . Blood gas values during hypothermia in asphyxiated term neonates. Pediatrics 2009; 123: 170–172.
Greisen G . Autoregulation of cerebral blood flow in newborn babies. Early Hum Dev 2005; 81: 423–428.
Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE, McDonald SA, Donovan EF et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med 2005; 353: 1574–1584.
Thoresen M . Hypothermia after perinatal asphyxia: selection for treatment and cooling protocol. J Pediatr 2011; 158: e45–e49.
Shankaran S, Laptook AR, Pappas A, McDonald SA, Das A, Tyson JE et al. Effect of depth and duration of cooling on deaths in the NICU among neonates with hypoxic ischemic encephalopathy: a randomized clinical trial. JAMA 2014; 312: 2629–2639.
DeBoer SL, Stephens D . Persistent pulmonary hypertension of the newborn: case study and pathophysiology review. Neonatal Netw 1997; 16: 7–13.
Steinhorn RH . Neonatal pulmonary hypertension. Pediatr Crit Care Med 2010; 11: S79–S84.
Walsh-Sukys MC, Tyson JE, Wright LL, Bauer CR, Korones SB, Stevenson DK et al. Persistent pulmonary hypertension of the newborn in the era before nitric oxide: practice variation and outcomes. Pediatrics 2000; 105: 14–20.
Little WJ . On the influence of abnormal parturition, difficult labors, premature birth, and asphyxia neonatorum, on the mental and physical condition of the child, especially in relation to deformities. Transactions of the Obstetrical Society of London. Longmans, Green and Co, 1861; 293.
Flagg PJ . Treatment of asphyxia in the new-born. Preliminary report of the practical application of modern scientific methods. JAMA 1928; 91: 788–791.
Obladen M . History of neonatal resuscitation. Part 2: oxygen and other drugs. Neonatology 2009; 95: 91–96.
Apgar V . A proposal for a new method of evaluation of the newborn infant. Curr Res Anesth Analg 1953; 32: 260–267.
Lane N . Oxygen: the Molecule that Made the World. Oxford University Press: Oxford, England, UK, 2002.
Saugstad OD . Is oxygen more toxic than currently believed? Pediatrics 2001; 108: 1203–1205.
Howell M, Ford P . The paradoxes of a small American disaster. The beetle of Aphrodite and other medical mysteries. Random House: New York, NY, USA, 1985.
Patz A . The role of oxygen in retrolental fibroplasia. Pediatrics 1957; 19: 504–524.
Northway WH Jr, Rosan RC, Porter DY . Pulmonary disease following respirator therapy of hyaline-membrane disease. Bronchopulmonary dysplasia. N Engl J Med 1967; 276: 357–368.
Saugstad OD . Chronic lung disease: oxygen dogma revisited. Acta Paediatr 2001; 90: 113–115.
Gerschman R, Gilbert DL, Nye SW, Dwyer P, Fenn WO . Oxygen poisoning and x-irradiation: a mechanism in common. Science 1954; 119: 623–626.
Saugstad OD . Hypoxanthine as a measurement of hypoxia. Pediatr Res 1975; 9: 158–161.
Saugstad OD, Aasen AO . Plasma hypoxanthine concentrations in pigs. A prognostic aid in hypoxia. Eur Surg Res 1980; 12: 123–129.
Aasen AO, Saugstad OD . Hypoxanthine in lethal canine endotoxin shock. Circ Shock 1979; 6: 277–283.
Frank L, Groseclose EE . Preparation for birth into an O2-rich environment: the antioxidant enzymes in the developing rabbit lung. Pediatr Res 1984; 18: 240–244.
Saugstad OD . Hypoxanthine as an indicator of hypoxia: its role in health and disease through free radical production. Pediatr Res 1988; 23: 143–150.
Saugstad OD . Oxygen radicals and pulmonary damage. Pediatr Pulmonol 1985; 1: 167–175.
Saugstad OD . Oxidative stress in the newborn—a 30-year perspective. Biol Neonate 2005; 88: 228–236.
Saugstad OD, Rootwelt T, Aalen O . Resuscitation of asphyxiated newborn infants with room air or oxygen: an international controlled trial: the Resair 2 study. Pediatrics 1998; 102: e1.
Ramji S, Ahuja S, Thirupuram S, Rootwelt T, Rooth G, Saugstad OD . Resuscitation of asphyxic newborn infants with room air or 100% oxygen. Pediatr Res 1993; 34: 809–812.
Saugstad OD, Ramji S, Soll RF, Vento M . Resuscitation of newborn infants with 21% or 100% oxygen: an updated systematic review and meta-analysis. Neonatology 2008; 94: 176–182.
Saugstad OD . Resuscitation of newborn infants: from oxygen to room air. Lancet 2010; 376: 1970–1971.
World Health Organization. Guidelines on basic newborn resuscitation. http://www.who.int/maternal_child_adolescent/documents/basic_newborn_resuscitation/en/2012. Published 2012. Accessed 5 November 2015.
Vento M, Asensi M, Sastre J, Garcia-Sala F, Pallardo FV, Vina J . Resuscitation with room air instead of 100% oxygen prevents oxidative stress in moderately asphyxiated term neonates. Pediatrics 2001; 107: 642–647.
Vento M, Sastre J, Asensi MA, Vina J . Room-air resuscitation causes less damage to heart and kidney than 100% oxygen. Am J Respir Crit Care Med 2005; 172: 1393–1398.
Perlman JM, Wyllie J, Kattwinkel J, Atkins DL, Chameides L, Goldsmith JP et al. Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2010; 122: S516–S538.
Kapadia VS, Chalak LF, DuPont TL, Rollins NK, Brion LP, Wyckoff MH . Perinatal asphyxia with hyperoxemia within the first hour of life is associated with moderate to severe hypoxic-ischemic encephalopathy. J Pediatr 2013; 163: 949–954.
Lakshminrusimha S, Swartz DD, Gugino SF, Ma CX, Wynn KA, Ryan RM et al. Oxygen concentration and pulmonary hemodynamics in newborn lambs with pulmonary hypertension. Pediatr Res 2009; 66: 539–544.
Lakshminrusimha S, Russell JA, Steinhorn RH, Swartz DD, Ryan RM, Gugino SF et al. Pulmonary hemodynamics in neonatal lambs resuscitated with 21%, 50%, and 100% oxygen. Pediatr Res 2007; 62: 313–318.
Brown JV, Moe-Byrne T, Harden M, McGuire W . Lower versus higher oxygen concentration for delivery room stabilisation of preterm neonates: systematic review. PLoS One 2012; 7: e52033.
Saugstad OD, Aune D, Aguar M, Kapadia V, Finer N, Vento M . Systematic review and meta-analysis of optimal initial fraction of oxygen levels in the delivery room at ≤32 weeks. Acta Paediatr 2014; 103: 744–751.
Oei JL, Lui K, Wright IM et al. Targeted oxygen in the resuscitation of preterm infants and their developmental outcomes (To2rpido): a randomised controlled study. Abstract presented at the 2015 Pediatric Academic Societies Annual Meeting; April 25–28, 2015; San Diego, CA, USA. Abstract 3130.2.
Rabi Y, Lodha A, Soraisham A, Singhal N, Barrington K, Shah PS . Outcomes of preterm infants following the introduction of room air resuscitation. Resuscitation 2015; 96: 252–259.
Saugstad OD, Aune D . Optimal oxygenation of extremely low birth weight infants: a meta-analysis and systematic review of the oxygen saturation target studies. Neonatology 2014; 105: 55–63.
Manja V, Lakshminrusimha S, Cook DJ . Oxygen saturation target range for extremely preterm infants: a systematic review and meta-analysis. JAMA Pediatr 2015; 169: 332–340.
Walsh MC, Di Fiore JM, Martin RJ, Gantz M, Carlo WA, Finer N . Association of oxygen target and growth status with increased mortality in small for gestational age infants: further analysis of the surfactant, positive pressure and pulse oximetry randomized trial. JAMA Pediatr 2016; 1–3.
Wollen EJ, Sejersted Y, Wright MS, Bik-Multanowski M, Madetko-Talowska A, Gunther CC et al. Transcriptome profiling of the newborn mouse lung after hypoxia and reoxygenation: hyperoxic reoxygenation affects mTOR signaling pathway, DNA repair, and JNK-pathway regulation. Pediatr Res 2013; 74: 536–544.
Acknowledgements
This article is based on discussions at a roundtable meeting supported by a grant from Mallinckrodt Pharmaceuticals, formerly Ikaria. Presentations and discussions were developed solely by the participants, without grantor input. The meeting chair Robin Steinhorn, MD, determined the agenda and attendees. SL and ODS developed the presentations and led the discussions upon which this article is based, provided critical review and revisions to the outline and manuscript drafts, provided final approval of the version to be published, and are accountable for the integrity of the content and for addressing questions. We gratefully acknowledge Robin Steinhorn, MD, for critical review of the manuscript and the contributions of the following individuals who participated in discussion that shaped the content of this article: Namasivayam Ambalavanan, MD; Judy L Aschner, MD; Jason Gien, MD; John Kinsella, MD; G Ganesh Konduri, MD; Robin Steinhorn, MD. Writing and editorial assistance was provided by Saema Magre, Sharon Suntag and Julie Gerke of Quintiles.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
SL and ODS received honoraria for their participation in a roundtable meeting supported by a grant from Mallinckrodt Pharmaceuticals, formerly Ikaria. SL was a member of the speaker’s bureau for Ikaria from June 2010 to October 2014 and has received grant support from the American Academy of Pediatrics and Canadian Pediatric Society. SL also received an NIH grant (5R01HD072929-03).
Rights and permissions
About this article

Cite this article
Lakshminrusimha, S., Saugstad, O. The fetal circulation, pathophysiology of hypoxemic respiratory failure and pulmonary hypertension in neonates, and the role of oxygen therapy. J Perinatol 36 (Suppl 2), S3–S11 (2016). https://doi.org/10.1038/jp.2016.43
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2016.43
- Springer Nature America, Inc.
This article is cited by
-
Care of the critically ill neonate with hypoxemic respiratory failure and acute pulmonary hypertension: framework for practice based on consensus opinion of neonatal hemodynamics working group
Journal of Perinatology (2022)
-
Renal biomarkers of acute kidney injury in response to increasing intermittent hypoxia episodes in the neonatal rat
BMC Nephrology (2021)
-
Effect of continuous positive airway pressure versus nasal cannula on late preterm and term infants with transient tachypnea of the newborn
Journal of Perinatology (2021)
-
Perioperative management of arteriovenous malformation guided by integrated evaluation of hemodynamics
European Journal of Pediatrics (2021)
-
Venovenous versus venoarterial extracorporeal membrane oxygenation among infants with hypoxic-ischemic encephalopathy: is there a difference in outcome?
Journal of Perinatology (2021)