
Abstract
Purpose of Review
The purpose of this review is to thoroughly explore and document the potential uses of fruits and vegetables as baby food. It aims to achieve several key objectives, including the identification of phytochemical compounds present in fruits and vegetables, the assessment of their biological properties, and the examination of their practical applications in the baby food. Ultimately, this review seeks to provide a comprehensive understanding of how fruits and vegetables can be used as baby food and enhance food quality in terms of nutritional value.
Recent Findings
Nutritional challenges in babies due to dietary factors have become an escalating issue in recent times. The incorporation of solid foods into a baby’s diet is of utmost importance for their overall growth and well-being. Inappropriate dietary practices leads to nutrient deficiencies, food allergies, and obesity. Cereal foods gained prominence as a popular choice for complementary baby feeding due to their convenience, nutrient content, and ease of digestion. Fruits and vegetables are rich in vitamins, minerals, dietary fiber, and antioxidants, thus boost their immune system, regulates bowel, prevent constipation and makes babies healthier.
Summary
Fruits, vegetables and cereal products are essential for wellbeing of developing babies compared to dairy and cereal based food products. Furthermore, inclusion of fruit, vegetable, and cereal-based (rice) ingredients in baby food acts as prebiotics for enhancing probiotic growth. Additionally, exposing babies to variety of flavors and textures promote babies to eat these nutritious food products.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The nutritious and nutraceutical rich diet is essential for babies during their growth and development. Early-life nutritional imbalances can affect health of babies and leads to obesity, diabetes, hypertension, ischemic heart disease, and developmental delays in adults [1]. Among these, malnutrition is a contributing factor in roughly 60% of all fatalities among children under the age of five in developing nations [2•]. In 6–23 months old age range of children, malnutrition is most prevalent. This stage of life is "critical window" for promoting the best possible growth, health, and behavioral development because growth occurs at its fastest during the first year of life [3••]. Therefore, it is crucial to introduce nutrient-rich foods after six months of exclusive breastfeeding to complement continued breastfeeding, and gradually transition to the family diet after reaching two years of age in order to prevent growth faltering [4••]. During the initial 4–6 months of life, whether a baby is breastfed or formula-fed, their nutritional needs can be entirely met by milk [5]. However, after this timeframe, introducing complementary foods becomes necessary to provide additional energy and nutrients to support the infant’s growth. Recently, numerous studies have been conducted on infant diets, both in developing and industrialized nations [1]. Complementary feeding (CF) significantly influences both early and later life nutrition, playing a crucial role in the health status and proper growth of babies. It is recommended to initiate the transition from breast milk to solid foods around 6 months of age, as breast milk alone becomes insufficient to fully meet the nutritional needs of the infant at this stage [5]. During the complementary feeding period, special attention is required to ensure adequate nutrition for babies. Recommended practices include introducing complementary foods at approximately half a year old baby ensuring an adequate meal frequency and appropriately sized portions, diversifying the diet, ensuring appropriate food texture, and observing safety measures during preparation, storage, and hygiene. This transition to solid foods signifies a significant milestone in baby’s dietary journey. The World Health Organization and UNICEF recommend exclusive breastfeeding (EBF) for the initial 6 months of an infant’s life, followed by the gradual introduction of supplementary foods, while also continuing breastfeeding up to and beyond the age of 2 years [6]. Recently, there has been a substantial increase in the accessibility and diversity of a new category of commercial supplementary foods specially crafted for infants and toddlers. These foods are usually pureed or semiliquid, and they come packaged in squeezable plastic pouches equipped with a spout and screw cap [7]. The primary appeal of these pureed pouch products lies in the convenience they bring to families. With a straightforward twist of the lid, the contents can be directly dispensed into babies mouth, or the babies can independently draw out the contents from the spout, facilitating fast and hassle-free feeding, particularly when on the move. This contemporary approach to infant feeding has garnered substantial favor, to the extent that reusable pouches are now on the market, enabling the feeding of homemade pureed baby food to infants via a squeezable bag [7].
This review discusses detailed information regarding the diet induced problems in babies. Additionally the current review discusses the role of fruits, vegetables, and cereals in development of nutraceutical rich baby food products.
Status of Baby Foods
The infant nutritional products market is expected to grow from USD 88.31 billion in 2023 to USD 125.67 billion by 2028. This growth represents a compound annual growth rate (CAGR) of 7.31% during the forecast period spanning from 2023 to 2028 [8]. The primary driver of this growth is the Asia Pacific region, which is experiencing the most significant market expansion. This upswing can be attributed to various factors, including an upsurge in the number of employed mothers, a rise in family earning, an increased focus on infant health products, and a surge in the demand for organic baby foods. Sufficient intake of proteins, essential fatty acids, carbohydrates, vitamins, minerals, is important for growth and development of babies. This nutritious diet is crucial in supporting regular growth, physical and cognitive development, and fostering good health from infancy through childhood, adolescence, and beyond [9].
The introduction of complementary foods during childhood, which involves offering foods and liquids other than milk, has long-term implications for an individual’s physical, cognitive, and socio-emotional health. In several developed societies, mothers typically begin with feeding infants pureed foods using a spoon, followed by a gradual transition to coarser-textured purees, finger foods (foods that can be eaten with hands), and eventually incorporating family foods into their diet [10]. Extensive evidence supports the notion that childhood is a crucial period influencing later-life, with early nutrition playing a major role in health of babies [11]. In the past, baby foods were predominantly homemade, usually pureed or mashed. However, the concept of mass production of baby foods emerged in 1928. During the late nineteenth to mid-twentieth centuries, infant feeding guidelines underwent changes, resulting in the introduction of solids at earlier ages, around 4–6 weeks old in the 1950s [12]. This shift in advice, coupled with an increased birth rate after the Second World War, prompted manufacturers to produce commercial baby foods as part of the canned goods industry, particularly in the USA. Initially, the commercial production of infant foods aimed to provide a consistent supply of fruits and vegetables throughout the year. However, over time, the variety of products has expanded significantly. Today, there is a diverse range of commercially prepared baby food products available, categorized according to the infant’s stage/age and the type of food offered, including cereal products, baby snacks, and desserts, among others [13].
Diet Induced Problems in Babies
Adequate nutrition plays a crucial role in the health and developmental well-being of children. Research suggests that undernutrition is a direct or indirect factor in at least 35% of deaths among children under the age of five. Moreover, undernutrition significantly contributes to disabilities, hindering the full developmental potential of surviving children. In developing countries, approximately 32%, equivalent to 186 million children under five, experience stunted growth, while about 10%, or 55 million, suffer from wasting [14]. Concerns related to diet-related issues in babies are significant for both parents and healthcare professionals. The type and quality of food consumed by babies play a vital role in their growth and development. Studies have shown that inappropriate diet initiate several health problems, such as malnutrition, obesity, diabetes and gastrointestinal disorders.
Malnutrition is a common problem in babies that can be caused by an inappropriate diet. According to the World Health Organization, malnutrition is a condition that results from a lack of essential nutrients in the diet, including energy, protein, vitamins and minerals [15]. Kundu et al.[16] reported that malnutrition was prevalent in infants who were fed a low quantity diet such as one that was deficient in protein and vitamins. Malnutrition can lead to several health problems, including stunted growth, delayed cognitive development and increased susceptibility to infections [17]. Protein-energy malnutrition arises from inadequacies in protein, energy-rich foods, or both, in relation to the body’s requirements. Research indicates a correlation between caries in the primary dentition and malnutrition in early childhood. Typically, deficiencies in dietary energy and protein tend to co-occur [18, 19].
Obesity is another diet- induced problem that is becoming increasingly common in babies. Obesity is a condition in which there is an excessive accumulation of body fat, leading to an increased risk of health problems such as diabetes, cardiovascular diseases and hypertension [20]. Mayhew et al. [21] reported that inappropriate feeding practice such as overfeeding or feeding high calorie foods can lead to early onset of obesity in babies. In this study it was found that babies who were fed high calorie formula or solids had a higher risk of becoming overweight or obese compared to those who were breastfed or fed low calorie foods.
Diabetes is a chronic condition that is caused by the body’s inability to produce or use insulin effectively, leading to high levels of blood sugar. Diabetes can be diet induced especially in babies who are fed a high sugar diet. Clapin et al. [22] reported that a high sugar diet in infancy can lead to an increased risk of developing type-1 diabetes in childhood.
Additionally gastrointestinal disorders are a common problem in babies, and they can be diet induced. It has been reported that inappropriate feeding practices such as over feeding or feeding foods that are difficult to digest, can lead to gastrointestinal problems such as reflux, constipation and diarrhea. In this study it was found that babies who were fed a diet high in fiber, fat, or protein shows elevated risk of developing gastrointestinal problems compared to those who were fed a low-fiber, low fat, and low protein diet. It is essential for parents and healthcare professionals to ensure that babies are fed a balanced and appropriate diet that meets their nutritional needs [23].
In order to support a child’s regular growth and proper development, it’s crucial that their diet offers an adequate supply of energy while aligning with the prescribed nutrient requirements. This entails integrating a diverse array of fruits and vegetables into their daily meals, with every meal including at least one portion of these food groups. The daily consumption of fruit purees for children of 1–3, years is 1 cup while as for adolescents two cups have been recommended. In the case of vegetables, the recommended intake varies from three-quarters of a cup for children aged 1–3 years to 3 cups for adolescents [24]. Insufficient consumption of fruits and vegetables has been associated with higher rates of various types of gastrointestinal, lung and genitourinary cancers [25]. Unhealthy food habits have contributed to approximately one-third of children and youth being overweight or obese. Information collected from 2009–2012 reveals that approximately one out of every three children aged 2–19 years was classified as either overweight or obese. Additionally, 8% of children aged 8–17 years received diagnoses of borderline hypertension, while 2% were found to have hypertension [26]. To address these issues, the USDA recommends incorporating seasonal and locally produced foods into meals while emphasizing the importance of a wide variety of vegetables and fruits to ensure the intake of a diverse range of nutrients. Crucial guidelines also encompass the restriction of added sugar and saturated fat to levels below 10% of daily caloric intake, and maintaining daily sodium intake at levels less than 2,000 mgs [26]. Another research indicates that a diet rich in fruits and vegetables during early childhood can result in a sustained high intake of these foods, offering numerous benefits for weight management and overall health later in life. Nevertheless, there is a growing trend where a rising percentage of young children are not meeting the recommended levels of fruit and vegetable consumption, posing a universal public health concern [27]. Additionally, children in the 2–5 age groups tend to incorporate a higher quantity of vegetables in their diet compared to adolescents [28].
Nutritional Requirements of Babies
Babies possess a restricted stomach capacity, and their energy needs per kilogram of body weight are approximately three times higher than those of adults [29]. Ensuring adequate nutrition during infancy and childhood is crucial because these life stages involve numerous physical, mental, and behavioral changes. These changes include rapid growth, weight gain, the development of cognitive and psychomotor skills, and a shift in food preferences. Consequently, infants and children need small yet sufficient quantities of food to supply the energy and nutrients necessary to meet their daily basic requirements [30].
Carbohydrate
Carbohydrate plays an important part in infant nutrition and development. Carbohydrate spare proteins to be completely utilized for muscle growth and tissue repair processes. Less than 6 months baby needs 110–120 kcal/kg/day and 1-year infant need 100 kcal/kg/day [29]. In the early stages of life, the minimum carbohydrate intake for infants, primarily from lactose, should constitute 40% of their total energy intake [31]. This proportion should gradually increase to 55% of their energy intake by the age of 2 years. Concerning complementary foods for infants and young children, there are specific guidelines to limit the total carbohydrate content. For vegetable juices and beverages derived from them, the total carbohydrate content should not surpass 10 g per 100 ml. For fruit juices, nectars, and drinks based on them, it should not exceed 15 g per 100 mL. In the case of dishes comprised solely of fruit, the threshold is established at 20 g per 100 g. When it comes to desserts and puddings, the upper limit is 25 g per 100 g. Moreover, for non-milk-based beverages, the total carbohydrate content should not surpass 5 g per 100 g. It’s worth noting that there is a notable benefit to increasing dietary fiber intake [29].
Protein
A sufficient intake of dietary protein plays a vital role in maintaining cellular function, overall health, and promoting normal growth [29]. On the contrary, when there is a combination of protein deficiency and insufficient energy intake, it can result in protein-energy malnutrition, which is the most prevalent form of malnutrition globally [32]. The protein requirements for infants and young children rise as they grow older, with recommended daily allowances of 9.1 g for 6–8 months, 9.6 g for 9–11 months, and 10.9 g for 12–23 months [29]. Although breast milk serves as a significant source of daily protein for infants and young children, the introduction of complementary foods necessitates an increased protein intake from these foods. The suggested protein quantities for these foods are 1.9 g per day at 6–8 months (21%), 4.0 g per day at 9–11 months (42%), and 6.2 g per day at 12–23 months [33, 34] Protein plays a vital role as a fundamental building block in the nutrient composition of complementary foods.
Fats and Lipids
Dietary fats have a significant role in fulfilling the nutritional requirements of infants and young children, serving as a source of energy, essential fatty acids, and fat-soluble vitamins (A, D, E, and K) [29]. In the initial six months of life, fat constitutes roughly 50% of the energy content in breast milk, acting as the primary energy source for infants. As complementary foods are introduced, carbohydrates gradually take on the role of the main energy source, but fats continue to be vital for meeting the increasing energy requirements of the growing child [35]. Infants who consume limited breast milk should have complementary foods that contribute 34%, 38%, and 42% of their total energy needs in the form of dietary fats at ages six to eight, nine to eleven, and twelve to twenty -three months, respectively.
Minerals and Vitamins
Minerals and vitamins are vital for the growth and development of young children. Micronutrients, including zinc, iron and calcium, have a critical role in promoting ideal health, growth, and development in infants and young children [36, 37]. Calcium, phosphorus, and vitamin D are crucial for proper bone development, iodine is necessary for synthesizing thyroid hormones and brain myelination. Iron is essential for creating red blood cells and new tissues, and zinc significantly contributes to both growth and the regulation of the immune system [38]. Breast milk provides ample quantities of vitamins A, B, C, folate, iodine, and selenium for well-nourished mothers, resulting in limited to no need for these nutrients from complementary foods before 12 months [34, 39]. However, breast milk is relatively deficient in several other micronutrients, necessitating the inclusion of complementary foods to meet the growing child’s nutritional requirements. Complementary foods are expected to provide a significant percentage of total daily requirements for micronutrients, ranging from 30 to 97%, depending on the specific nutrient and age group [34, 39].
Insufficient iron levels in infants can lead to irreversible brain damage, this leads to the recommended iron intake for the population being set at 11 mg per day during the 6–12 month period. This recommendation decreases to 7 mg per day starting from the second year [38, 40]. Similarly, the recommended zinc requirement is 2.9 mg/day for young infants, increasing to 4.3 mg/day in toddlers [38]. Sufficient calcium intake for the 6–12 month period is 280 mg per day, and this level rises to 450 mg per day during the second year. Food fortification enables them to attain the appropriate iodine intake level for their age, which is 90 µg per day [38]. The recommended phosphorus intake is 160 mg/day for infants aged 6–12 months, and it increases to 250 mg/day for toddlers [38, 40].
Vitamins play a crucial role in the growth and development of infants and children. Vitamin B comprises water-soluble nutrients that participate in various metabolic processes, facilitating the utilization of lipids, carbohydrates and proteins for energy production. These vitamins are essential for the development of all organs and systems, with a particular emphasis on the nervous system. Since humans cannot synthesize B vitamins, they must introduce these nutrients into their diet [38]. Vitamin K plays a key role in activating clotting factors, and severe deficiency of it causes bleeding. Vitamin B2 is involved in oxidation–reduction reactions in metabolic pathways related to lipids, carbohydrates, and amino acids [41]. Vitamin B3 is a component of enzymatic cofactors that play a role in multiple oxidation–reduction metabolic reactions. It plays a key role in metabolizing carbohydrates, fats, and proteins, and it also contributes to the proper functioning of the nervous system, enhances circulation, and lowers blood cholesterol levels. A severe niacin deficiency can lead to pellagra, a condition characterized by dementia, dermatitis, and diarrhea [42]. Pyridoxine (Vit. B6) serves as a cofactor in the folate cycle and is crucial for the production of neurotransmitters like serotonin, dopamine, GABA, melatonin and norepinephrine. Vitamin C participates in enzymatic reactions, including the synthesis of carnitine, collagen, and norepinephrine. It also has a role in non-enzymatic processes, such as the neutralization of reactive oxygen species [43]. From the weaning stage, infants can obtain these vitamins through their diet. Furthermore, the detailed information regarding the deficiency signs and recommended doses of vitamins and minerals for infants and children are shown in Table 1.
Sources of Energy and Nutrients used in Baby Food
Food composition databases play a crucial role in estimating the energy, nutrient, and other dietary compound content of various foods. This data is essential for evaluating nutritional intakes and monitoring the effectiveness of dietary interventions and to decipher the role of the different dietary components in health and disease [44]. It is because of the importance of all the nutrients that the baby food should contain a balance from fruits, vegetables, cereals with added probiotics. The Important sources of Energy and nutrients are briefly discussed in detail as below;
Fruits
Baby foods incorporated with fruits serve as a vital source of energy, essential nutrients, fiber, vitamins, and minerals. Additionally, fruits provide good taste to the babies and hence these fruit based products can be liked by the babies [45]. Fruits play a pivotal role in preventing obesity and other chronic diseases because of the presence of various bio active components as shown in Fig. 1. Insufficient fruit intake has been highlighted as a contributing risk factor to global adult mortality. The formative years of childhood are critical for the development of eating behavior’s and food preferences, offering a window to cultivate healthy dietary habits that persist into adulthood [46]. Ongoing research underscores the potential health advantages of shifting dietary patterns towards increased consumption of plant-based foods, promoting both individual well-being and environmental sustainability [47, 48]. Notably, elevated fruit consumption has been linked to reduced obesity risk and lower rates of chronic illnesses. Insufficient fruit intake is recognized as a contributing risk factor for adult mortality worldwide, accounting for approximately 2.6 million deaths each year [49]. While most research on the health impacts of fruit and vegetable intake focuses on adults, the formative childhood years present a crucial juncture for shaping eating behavior’s and food preferences that endure into adulthood [46]. Fruits, categorized as a subgroup of vegetables containing seeds and pulpy tissue, are typically consumed raw for breakfast, as snacks, or as desserts. Vegetables, on the other hand, can be eaten raw or cooked as standalone dishes, mixed meals, or salads [46]. Owing to higher fiber, essential vitamins and minerals, fruits hold a prominent place in global food-based dietary guidelines (FBDGs), underlining their nutritional significance [50, 51]. The WHO recommends a daily minimum intake of 400 g (equivalent to five portions) of fruits and vegetables, excluding starchy tubers like potatoes, for maintaining general health [46, 52]. However, individual countries formulate their own FBDGs, and the Food and Agriculture Organization (FAO) compiles these guidelines into a comprehensive database [53].

Pictorial representation of benefits of flavonoids present in fruits
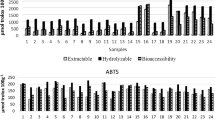
Various fruits have been utilized for the development of infant foods as fruits are rich sources of essential nutrients and bioactive components [54]. The fruits like apple, pear, apricot, plums etc. have been extensively used in the development of baby foods. These fruits are rich sources of various sugars, vitamins, minerals, organic acids and fiber contents which are essential for the health of infants, babies and adolescents. Wani et al. [55] documented the presence of various minerals in apricots, with Zinc (Zn), Calcium (Ca), Copper (Cu), Iron (Fe), Magnesium (Mg), Sodium (Na), Manganese (Mn), Phosphorus (P), and Potassium (K) falling within the ranges of 0.5–6.74, 15.62–372.66, 0–0.82, 0.9–12.62, 23.35–64.29, 14.85–28.06, 0–0.98, 9–696, and 2,150–5,416.66 ppm, respectively. Fruits are also rich sources of vitamins, which can play a prominent role in growth and development of babies. The vitamin content of various Himalayan fruits are shown in the Fig. 2. The apricots are also rich sources of antioxidants which can help in reducing various ailments in the infants, babies and adolescents. The Margulam variety of the apricots contains 30.90 GAE/g total phenolics, 82.34% reducing power and 35.44% DPPH inhibition activity as stated by Wani et al. [55]. Campeanu et al. [57] reported highest nutrient content in Jonathan apple variety with vitamin C of 25.75-77 mg/100 g, phosphorus 0.15–0.235%, potassium0.40–0.70%, calcium 2.5–7.8 mg/100 g and iron content of 0.20–0.28 mg/100 g. Akagic et al., [58] stated that pears are rich sources of carbohydrates and reported 59.2, 103.8, 79.4, 102.5, 116.9, 58.1, 89.7, 94.1, 86.9 and 75.0 g/kg total sugar from dolokrahan, takis, ahmetova, jeskovaca, hambarka, budaljaca, kacmorka, krakaca and sarajka président verities of pear respectively. The pears are also rich sources of phenolic components, hydroxycinnamic acid (chlorogenic acid), glycosylated hydroquinone (arbutin), flavan-3-ols (epicatechin and catechin), and flavonols (quercetin 3-O-glucoside and quercetin 3-O-rutinoside) are major phenolic compounds in pears [54]. The plum cultivars like acanska Lepotica, Stanley, and Jojo [59] have shown a significant content of micro- and macro elements such as Ca, K, Mg, Zn, Fe, Cu, B, and Mn. These plum cultivars have been reported to be the rich sources of sugars, polyphenols, anthocyanins, and organic acids [60]. Trendafilova et al. [61] stated that plums are rich sources of sugars and organic acids and `reported that wavit, janka, CF-667, ishtara and GXN-15 verities of plums contain 1.60, 1.35, 1.19, 1.34 and 1.5 g/kg sucrose and 0.77, 0.75, 0.83, 0.73 and 0.89 g/kg malic acid respectively.

Vegetables
Vegetables are an important but under consumed part of a healthy diet. There is growing interest in promoting vegetable acceptance and consumption among infants to help establish life-long healthy eating patterns. Vegetables constitute a crucial yet underappreciated component of a wholesome diet. There is a growing push to enhance the acceptance and consumption of vegetables among infants, as this can establish lifelong patterns of healthy eating. The advantages of incorporating vegetables into one’s diet are numerous. The Dietary Guidelines for Americans (2015–2020) recommend a diverse array of vegetable subgroups for optimal health, encompassing dark green, red and orange, legumes, starchy, and other varieties. However, over 80% of Americans aged one and above fall short of the recommended vegetable intake [62]. While the benefits of vegetable consumption from childhood onward are well-established, children tend to have limited vegetable intake. One potential barrier to introducing vegetables early in life is their bitter taste. Infants generally exhibit openness to new tastes, making it possible for them to readily accept vegetable flavors if introduced early. This initial experience significantly shapes their food preferences in later childhood. This is why complementary feeding guidelines encourage the introduction of fruits and vegetables as initial foods [63]. To encourage better dietary health, the World Health Organization advises a daily consumption of a minimum of five servings (equal to 400 g) of fruits and vegetables [52]. However, in Sub-Saharan Africa, daily intake falls below 200 g [64], leading to an estimated 27% of deaths being attributed to insufficient fruit and vegetable consumption [65]. On a global scale, only slightly more than half (52%) of young children achieve the minimum meal frequency, and less than a third (29%) reach the minimum dietary diversity threshold [66]. This results in increased malnutrition risk due to low meal frequency and micronutrient deficiency risk due to inadequate dietary variety. Vegetables play a pivotal role in a balanced children’s diet, furnishing essential nutrients for growth and health [67, 68]. More than 50% of the most economically disadvantaged children between the ages of 6 and 23 months have not been introduced to vegetables [69]. When these foods are offered, children tend to favour fruits over vegetables possibly due to fruits’ appealing sweetness and greater accessibility [70, 71]. The consumption of dark green vegetables, particularly among infants, is significantly limited according to data obtained from surveys such as the Feeding Infants and Toddlers Survey conducted in the United States [72]. The specific health benefits associated with vegetable consumption stem from bioactive components such as vitamins (A, C, E, K, folic acid), minerals (Mg, Ca, Zn, K), dietary fiber, and crucially, phytochemicals like flavonoids and carotenoids that exert anticarcinogenic and anti-inflammatory effects [73]. The vitamin content of various Himalayan based vegetables are shown in the Fig. 3. Consuming diets abundant in green leafy vegetables and those containing vitamin C has been associated with a decreased risk of developing coronary heart disease [74].

Phytochemicals derived from vegetables play a role in suppressing DNA damage caused by oxidative stress, a significant contributor to the development and progression of neurodegenerative diseases. The consumption of specific vegetables, recognized for their robust antioxidant properties, bestows both cognitive and physical health benefits, which are particularly critical for children residing in regions of the global south. Therefore, adhering to a well-balanced diet abundant in vegetables is acknowledged for its potential to mitigate the risk of various non-communicable diseases. Nevertheless, to fully harness the health-promoting advantages, substantial quantities of plant-based foods should be ingested in diverse forms. Vegetables stand out due to their higher fiber content and lower levels of sugar, sodium, fat, cholesterol, and energy density [68, 75, 76]. Despite the well-documented advantages of incorporating a range of vegetables in one’s diet, challenges persist in elevating vegetable intake in comparison to fruit consumption [77]. The factors contributing to low vegetable consumption among children, relative to fruits, encompass limited availability, elevated costs, and a universal aversion associated with sensory attributes like bitterness and unfamiliar textures [78]. Consequently, the phase of complementary feeding offers a strategic window for introducing vegetables, aiming to instil a liking and acceptance of these foods in children before their eating habits solidify and become resistant to change [79]. In a nutshell, even though their acknowledged health benefits and environmental merits as constituents of a plant-based diet are well-established, the consumption of vegetables continues to be inadequate. Therefore, advocating for increased vegetable intake during the initial 1000 days from conception could serve as a mechanism to foster familiarity even prior to the introduction of solid foods.
Cereals
Cereals are rich sources of protein, carbohydrate, minerals and vitamins crucial for the growth and advancement of babies [80]. In numerous countries, infant cereals are commonly introduced as the initial foods during the complementary feeding phase [79, 81]. The decision to initiate complementary feeding with infant cereals can be elucidated for several reasons.
-
a)
Cereals offer a valuable source of energy, crucial at around six months of age when exclusive breastfeeding becomes insufficient to meet the infant’s nutritional needs [82]. Furthermore, cereals supply substantial amounts of proteins and carbohydrates, while also containing minerals, vitamins, and bioactive compounds [83].
-
b)
Cereals are an excellent vehicle for iron fortification [84, 85]. Thus, introducing infant cereals aligns with the depletion of an infant’s iron stores at the start of complementary feeding [86].
-
c)
Cereals contribute non-digestible carbohydrates that play a role in shaping a mature gut microbiota by promoting the Bacteroides population [87]. Changes in gut microbiota of babies have been noted during weaning when various cereals, such as wheat, sorghum, rice, or oats, are introduced [88], additionally, increased quantities of complex carbohydrates in infant cereals have been shown to amplify the fermentative potential of the gut microbiota in infants ranging from six to ten months in age [89].
-
d)
Cereals have a mild taste, semi-solid texture, and consistency that suit the transition from milk to accepting solid foods. Although cereals play a vital role in the nutrition of infants and young children, there is a lack of agreement among pediatric organizations when it comes to determining the suitable cereal consumption, the types of cereals, and the degree of cereal processing (refined cereals versus whole grain).
In Europe, the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition “ESPGHAN” provides a recommendation to introduce complementary foods rich in iron, including cereals, starting from the age of four months while continuing breastfeeding [90, 91]. Likewise, the European Food Safety Authority “EFSA” suggests the introduction of iron-rich foods after the age of four to six months [92]. In contrast, New Zealand and the United States both advise against the introduction of cereals before six months of age [93]. Moreover, different countries convey their guidance regarding cereal consumption through various metrics, such as servings [94], tablespoons [95], or precise grams [93, 96], notably, both Europe and the US have organizations that refrain from specifying exact quantities [90, 91]. France and Spain advise introducing gluten-free cereals to infants between the ages of five to six months [97], ESPGHAN on the other hand, suggests that gluten may be introduced to babies between the ages of four and 12 months [91]. Infant rice cereals hold popularity as the initial complementary food in the Ireland and United Kingdom [98, 99]. In numerous cases throughout the Baltic and Nordic regions, oats are the preferred choice for the initial introduction of solid food for babies [100, 101]. However, Rice and maize are being the usual cereals used in the weaning foods [102]. In Spain, the primary choices for infant cereals are wheat and rice [93]. As per the findings of the Feeding Infants and Toddlers Study conducted in the United States, the most common sources of starch for infants and young children are iron-fortified infant cereals, predominantly made from rice or oats [84, 103]. Likewise, in Canada, the consumption of infant cereal predominantly revolves around choices that are based on rice [104], whereas mothers in African countries appear to begin with maize porridges [105, 106]. It is frequently uncertain to what extent the cereals used in infant cereal formulations should be processed, whether whole grain or refined. The Dietary Guidelines for Americans “2015–2020” promote the intake of nutrient-rich foods, with a specific focus on whole grains, for children between the ages of one to 18, aiming to increase dietary fiber, support healthy digestive function, and reduce the likelihood of chronic diseases. This recommendation suggests consuming 1.5 to four ounce-equivalents of whole grains in this age group [107].
Importance of Probiotics in Babies Health
As our society increasingly prioritizes health, there is a growing awareness and elevated concerns regarding diet, nutrition, and the safety of our food, all with the ultimate goal of improving our overall quality of life. The current global pandemic involving severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has underscored the significance of nutritional status as a risk factor for severe diseases, including malnutrition obesity [108]. Given this context, the role of healthy, nutritious, and functional foods has become crucial in strengthening the immune system to fight against illnesses [109].
Consumer preferences have led various stakeholders in the food industry to shift their focus toward producing foods with enhanced health benefits. Functional foods, which extend beyond basic nutrition to provide additional health advantages, are considered as the future of food. For a food product to be classified as functional, it must adhere to specific criteria, including compliance with a country’s food safety regulations or international standards, confirmation of the positive health advantages when incorporated into a well-rounded diet, as well as ease of access. Examples of functional foods include dietary supplements, prebiotics, probiotics, vitamins, dietary fiber, antioxidants, and other phytochemicals [110]. Probiotics, when consumed in sufficient amounts, confer health benefits to the host. These effects, observed after consuming probiotics in various food forms, include maintaining intestinal balance [111], enhancing the immune system [112], reducing cancer risks [113], assisting in the digestion of lactose [114], and other positive interactions between host and microorganisms, such as preventing diabetes, cardiovascular diseases, and allergic reactions [115]. Foods and beverages enriched with probiotics, considered as upcoming dietary options, have garnered significant consumer interest. This surge in popularity has propelled the global probiotics market to attain a value of 42.55 billion USD in 2017, with a projected increase to 94.48 billion USD by 2024. The Asia–Pacific region leads this growth, while Europe has seen a slower expansion of probiotic foods and beverages due to regulations concerning health claims [116].
Babies have a developing immune system that is susceptible to infections, and the use of probiotics in baby food has been shown to reduce the risk of infections such as diarrhea [117]. Probiotics have also been shown to improve the bioavailability of nutrients in baby food. The gut microbiota plays a crucial role in nutrient absorption and the use of probiotics in baby food has been shown to enhance nutrient absorption and promote overall health in infants [118]. The role of probiotics in prevention of diseases and enhancing immune system of babies is shown in the Fig. 4. Probiotics are being explored as a preventive measure to address potential health concerns in infants. However, the general use of probiotics has resulted in their inclusion in a wide range of products designed to support infant well-being. Within this landscape, the specificity, safety, and effectiveness of individual probiotic strains remain insufficiently defined. Among these strains, Bifidobacterium breve (M-16 V) is noteworthy as a commonly used probiotic in infant-related applications. It stands out as a well-established probiotic choice for infants. Research has indicated that M-16 V shows promise in providing protection to infants against serious conditions like necrotising enterocolitis and allergic diseases [119]. Various other studies like randomized controlled trial conducted by Lin et al. [120] have provided compelling evidence that supplementing with Bifidobacterium breve can be instrumental in mitigating the likelihood of gastrointestinal problems in infants. Lactobacillus rhamnosus represents another vital probiotic strain employed for infants. This probiotic is acclaimed for its ability to modulate the immune system, which can contribute to lowering the chances of allergies and infections among infants. Introducing Lactobacillus rhamnosus through supplementation can lead to a reduction in the occurrence of atopic dermatitis in infants [121]. Another probiotic strain Bifidobacterium infantis finds common usage in infant formula. It plays an indispensable part in enhancing the digestive processes and overall gastrointestinal well-being of infants. Research conducted by Saturio et al. [122] demonstrated that incorporating Bifidobacterium infantis into the formula for infants positively influenced the composition of their gut microbiota. Table 2

Importance of probiotics in preventing from diseases
Conclusion and future perspective
Fruit, vegetable, and probiotic based baby foods offer a nutritious and natural option for parents looking to provide their babies with a healthy start. The benefit of incorporating these foods into baby’s diet include essential vitamins and minerals, low calorie content, and the addition of beneficial probiotics that aid in digestion and improve immunity. Furthermore, these types of baby foods are often free from harmful additives and preservatives, which can be found in many processed foods. However, parents should exercise caution when selecting baby food products and ensure that they contain natural ingredients. Overall, fruit, vegetable and probiotic based baby foods offer a convenient and healthy solution for parents who want to promote their baby’s growth and development. There is great scope in the development of baby food and food products based on fruit, vegetable, cereal and probiotic constituents. Furthermore the limit of fruit, vegetable, cereal and probiotics in baby food formulations need to be investigated. Additionally, proper investigations are required to evaluate the presence of pesticide residues and various antinutritional factors in these baby food products.
Data Availability
No datasets were generated or analysed during the current study.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Zand N, Chowdhry BZ, Zotor FB, Wray DS, Amuna P, Pullen FS. Essential and trace elements content of commercial infant foods in the UK. Food Chem. 2011;128:123–8. https://doi.org/10.1016/j.foodchem.2011.03.005.
• Zaheer A, Qurrat-ul-Ain AB, Sharif A, Naseer D. Malnutrition in children of growing age and the associated health concerns. One health perspective. In: Abbas RZ, Saeed NM, Younus M, Aguilar-Marcelino L, Khan A, editors. One health triad; 2023. p. 153–61. Explores the malnutrition in children of growing age and the associated health concerns, also states that malnutrition is a contributing factor in roughly 60% of all fatalities among children under the age of five in developing nations.
•• Singh S, Dunkwal V. Development and nutritional evaluation of infant food premix to improve the nutritional status of the malnourished infants (06-24 months). Indian J Nutr Diet. 57(4):439–49. This study addresses the nutritional evaluation of infant food in order to improve the nutritional status of the malnourished Infants (06–24 months).
•• Choudhury S, Headey DD, Masters WA. First foods: Diet quality among infants aged 6–23 months in 42 countries. Food Policy. 2019;88:101762 (This paper analyzes data from 42 low- and middle-income countries, linking infant feeding practices to household and environmental factors. It finds that wealthier households, better parental education, improved local infrastructure, and favorable agro-climatic conditions are associated with earlier introduction of diverse foods to infants, supporting an infant-feeding version.).
Jose Bernal M, Roman S, Klerks M, Francisco Haro-Vicente J, Manuel Sanchez-Siles L. Are homemade and commercial infant foods different? A nutritional profile and food variety analysis in Spain. Nutrients. 2021;13(3):777.
Koletzko B, Hirsch NL, Jewell JM, Dos Santos Q, Breda J, Fewtrell M, Weber MW. National recommendations for infant and young child feeding in the World Health Organization European Region. J Pediatr Gastroenterol Nutr. 2020;71:672.
Koletzko B, Hirsch NL, Jewell JM, Caroli M, Breda JRDS, Weber M. Pureed fruit pouches for babies: child health under squeeze. J Pediatr Gastroenterol Nutr. 2018;67:561–3.
INMS- Infant Nutrition Market Size & Share Analysis - Growth Trends & Forecasts (2023 - 2028) Source: https://www.mordorintelligence.com/industry-reports/infant-nutrition-market.
Victora CG, Bahl R, Barros AJD, França GVA, Horton S, Krasevec J, Murch S, Sankar MJ, Walker N, Rollins NC. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387:475–90.
Addessi E, Galloway AT, Wingrove T, Brochu H, Pierantozzi A, Bellagamba F, Farrow CV. Baby-led weaning in Italy and potential implications for infant development. Appetite. 2021;164: 105286.
Nurliyana AR, Mohd Shariff Z, Mohd Taib MN, Gan WY, Tan KA. Early nutrition, growth and cognitive development of infants from birth to 2 years in Malaysia: a study protocol. BMC Pediatr. 2016;16:1–7.
Saraswat S, Khan R, Kumar A, Singh AP. Impact of mandatory food and agriculture laws on the food manufacturing industry: review of 75 years of challenges and changes. In: Convergence of cloud computing, AI, and agricultural science; 2023. p. 228–60.
K Maslin, C Venter, 2017 Nutritional aspects of commercially prepared infant foods in developed countries: A narrative review https://doi.org/10.1017/S0954422417000038
Addessi E, Galloway AT, Wingrove T, Brochu H, Pierantozzi A, Bellagamba F, Farrow CV. Baby-led weaning in Italy and potential implications for infant development. Appetite. 2021;164:105286.
Nurliyana AR, Mohd Shariff Z, Mohd Taib MN, Gan WY, Tan K-A. Early nutrition, growth and cognitive development of infants from birth to 2 years in Malaysia: a study protocol. BMC Pediatr. 2016;16:1–7.
Kundu S, Rai B, Shukla A. Prevalence and determinants of Vitamin A deficiency among children in India: Findings from a national cross-sectional survey. Clin Epidemiol Glob Heal. 2021;11: 100768.
Maslin K, Venter C. Nutritional aspects of commercially prepared infant foods in developed countries: A narrative review. 2017;30(1):138–48.
Singh A, Purohit BM. Malnutrition and its association with dental caries in the primary and permanent dentition: A systematic review and meta-analysis. Pediatr Dent. 2020;42:418–26.
Sheetal A, Hiremath VK, Patil AG, Sajjansetty S, Kumar SR. Malnutrition and its oral outcome–a review. J Clin Diagnostic Res JCDR. 2013;7:178.
Powell-Wiley TM, Poirier P, Burke LE, Després J-P, Gordon-Larsen P, Lavie CJ, Lear SA, Ndumele CE, Neeland IJ, Sanders P. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143:e984–1010.
Mayhew AJ, Pigeyre M, Couturier J, Meyre D. An evolutionary genetic perspective of eating disorders. Neuroendocrinology. 2018;106:292–306.
Clapin HF, Earnest A, Colman PG, Davis EA, Jefferies C, Anderson K, Chee M, Bergman P, de Bock M, Kao K-T. Diabetic Ketoacidosis at Onset of Type 1 Diabetes and Long-term HbA1c in 7,961 Children and Young Adults in the Australasian Diabetes Data Network. Diabetes Care. 2022;45:2918–25.
Vandenplas Y, Salvatore S, Hauser B. The diagnosis and management of gastro-oesophageal reflux in infants. Early Hum Dev. 2005;81:1011–24.
Thompson HR, Borger C, Paolicelli C, Whaley SE, Reat A, Ritchie L. The Relationship between Breastfeeding and Initial Vegetable Introduction with Vegetable Consumption in a National Cohort of Children Ages 1–5 Years from Low-Income Households. Nutrients. 2022;14:1740.
Care D. 6 Gycemic targets: standards of medical care in diabetes—2019. Diabetes Care. 2019;42:S61-70.
McGuire S. Scientific report of the 2015 dietary guidelines advisory committee. Washington, DC: US departments of agriculture and health and human services, 2015. Adv Nutr. 2016;7(1):202–4.
Okubo H, Miyake Y, Sasaki S, Tanaka K, Hirota Y. Feeding practices in early life and later intake of fruit and vegetables among Japanese toddlers: the Osaka Maternal and Child Health Study. Public Health Nutr. 2016;19:650–7.
Herrick KA, Rossen LM, Nielsen SJ, Branum AM, Ogden CL. Fruit consumption by youth in the United States. Pediatrics. 2015;136(4):664–71.
Maurya R, Mogra R, Mauriya SK. The Importance of Nutrition in Infancy: A Review. Asian Food Sci J. 2020;18:45–9.
S. McGuire, Scientific report of the 2015 dietary guidelines advisory committee. Washington, dc: Us departments of agriculture and health and human services, 2015, Advances in Nutrition (2016) 7(1) 202–204.
Gridneva Z, Rea A, Tie WJ, Lai CT, Kugananthan S, Ward LC, Murray K, Hartmann PE, Geddes DT. Carbohydrates in human milk and body composition of term infants during the first 12 months of lactation. Nutrients. 2019;11:1472.
K.A. Herrick, L.M. Rossen, S.J. Nielsen, A.M. Branum, C.L. Ogden, Fruit consumption by youth in the United States, Pediatrics (2015) 136(4) 664–671.
Abeshu MA, Lelisa A, Geleta B. Complementary feeding: review of recommendations, feeding practices, and adequacy of homemade complementary food preparations in developing countries–lessons from Ethiopia. Front Nutr. 2016;3:41.
Rajesh A, Sreenath N, Marmavula S, Krishnamoorthy C, Chidambaram R. Macro-and micronutrients in the development of food for babies and children. In: Food science technology and nutrition for babies and children; 2020. p. 99–117.
Monte CMG, Giugliani ERJ. Recommendations for the complementary feeding of the breastfed child. J Pediatr. 2004;80:s131–41.
Casha AR, Scarci M, The link between tuberculosis and body mass index. J Thorac Dis. 2017;9(3):E301.
Abeshu MA, Lelisa A, Geleta B. Complementary feeding: review of recommendations, feeding practices, and adequacy of homemade complementary food preparations in developing countries–lessons from Ethiopia. Front Nutr. 2016;3:41.
Savarino G, Corsello A, Corsello G. Macronutrient balance and micronutrient amounts through growth and development. Ital J Pediatr. 2021;47:1–14.
C.M.G. Monte, E.R.J. Giugliani, Recommendations for the complementary feeding of the breastfed child, Journal de Pediatria (2004) 80, pp. s131–s141.
A.R. Casha, M. Scarci, The link between tuberculosis and body mass index, Journal of Thoracic Disease (2017) 9(3), E301.
van der Kolk JH, Gross JJ, Gerber V, Bruckmaier RM. Disturbed bovine mitochondrial lipid metabolism: A review. Vet Q. 2017;37:262–73.
Naveen KN, Pai VV, Bagalkot P, Kulkarni V, Rashme P, Athanikar SB. Pellagra in a child–a rare entity. Nutrition. 2013;29:1426–8.
Zwolińska D, Grzeszczak W, Szczepańska M, Kiliś-Pstrusińska K, Szprynger K. Vitamins A, E and C as non-enzymatic antioxidants and their relation to lipid peroxidation in children with chronic renal failure. Nephron Clin Pract. 2006;103:c12–8.
Elmadfa I, Meyer AL. Importance of food composition data to nutrition and public health. Eur J Clin Nutr. 2010;64:S4–7.
Čížková H, Ševčík R, Rajchl A, Voldřich M. Nutritional quality of commercial fruit baby food, Czech. J Food Sci. 2009;27:134–7.
McCarthy R, Kehoe L, Flynn A, Walton J. The role of fruit and vegetables in the diets of children in Europe: Current state of knowledge on dietary recommendations, intakes and contribution to energy and nutrient intakes. Proc Nutr Soc. 2020;79:479–86.
Willett W, Rockström J, Loken B, Springmann M, Lang T, Vermeulen S, Garnett T, Tilman D, DeClerck F, Wood A. Food in the Anthropocene: the EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet. 2019;393:447–92.
Baden MY, Liu G, Satija A, Li Y, Sun Q, Fung TT, Rimm EB, Willett WC, Hu FB, Bhupathiraju SN. Changes in plant-based diet quality and total and cause-specific mortality. Circulation. 2019;140:979–91.
Domellöf M, Szitanyi P, Simchowitz V, Franz A, Mimouni F, Braegger C, Bronsky J, Cai W, Campoy C, Carnielli V. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: iron and trace minerals. Clin Nutr. 2018;37(6):2354–9.
Montagnese C, Santarpia L, Buonifacio M, Nardelli A, Caldara AR, Silvestri E, Contaldo F, Pasanisi F. European food-based dietary guidelines: a comparison and update. Nutrition. 2015;31:908–15.
Herforth A, Arimond M, Álvarez-Sánchez C, Coates J, Christianson K, Muehlhoff E. A global review of food-based dietary guidelines. Adv Nutr. 2019;10:590–605.
McCarthy R, Kehoe L, Flynn A, Walton J. The role of fruit and vegetables in the diets of children in Europe: current state of knowledge on dietary recommendations, intakes and contribution to energy and nutrient intakes. Proc Nutr Soc. 2020;79(4):479–86.
Ene-Obong H, Schönfeldt HC, Campaore E, Kimani A, Mwaisaka R, Vincent A, El Ati J, Kouebou P, Presser K, Finglas P. Importance and use of reliable food composition data generation by nutrition/dietetic professionals towards solving Africa’s nutrition problem: constraints and the role of FAO/INFOODS/AFROFOODS and other stakeholders in future initiatives. Proc Nutr Soc. 2019;78:496–505.
Salkić B, Cvrk R, Imširović E, Salkić A, Salkić E. Comparison of pomological and chemical properties of autochthonous pear varieties with standard pear varieties. Int J Plant Soil Sci. 2020;32:36–42.
Wani SM, Masoodi FA, Wani TA, Ahmad M, Gani A, Ganai SA. Physical characteristics, mineral analysis and antioxidant properties of some apricot varieties grown in North India. Cogent Food Agric. 2015;1:1118961.
J.A. Rather, S. Yousuf, Q.S. Ashraf, S.A. Mir, H.A. Makroo, D. Majid,.. & B.N. Dar, Nutritional and bioactive composition, nutraceutical potential, food and packaging applications of Cydonia oblonga and its byproducts: A review. Journal of Food Composition and Analysis, (2023) 115, 105000.
Campeanu G, Neata G, Darjanschi G. Chemical composition of the fruits of several apple cultivars growth as biological crop. Not Bot Horti Agrobot Cluj-Napoca. 2009;37:161–4.
W.H. Organization. Diet, nutrition, and the prevention of chronic diseases: report of a joint WHO/FAO expert consultation. World Health Organization. 2003;916.
VR Angelova, SG Tabakov, MN Petrov, Influence of rootstock cultivar combination on the content of heavy metals, micro and microelements in the fruits of plums., Agric Sci Nauk. (2020)12
SG Tabakov, AI Yordanov, PN Denev, DG Teneva, 2021 Study of the influence of rootstocks on fruit flesh quality of three plum cultivars, in: XII Int. Symp. Plum Prune Genet. Breed. Pomol. 1322 155–162.
Trendafilova A, Ivanova V, Trusheva B, Kamenova-Nacheva M, Tabakov S, Simova S. Chemical composition and antioxidant capacity of the fruits of European plum cultivar “Čačanska Lepotica” influenced by different rootstocks. Foods. 2022;11:2844.
Bakke AJ, Carney EM, Higgins MJ, Moding K, Johnson SL, Hayes JE. Blending dark green vegetables with fruits in commercially available infant foods makes them taste like fruit. Appetite. 2020;150: 104652.
Garcia AL, McLean K, Wright CM. Types of fruits and vegetables used in commercial baby foods and their contribution to sugar content. Matern Child Nutr. 2016;12:838–47. https://doi.org/10.1111/mcn.12208.
Uusiku NP, Oelofse A, Duodu KG, Bester MJ, Faber M. Nutritional value of leafy vegetables of sub-Saharan Africa and their potential contribution to human health: A review. J Food Compos Anal. 2010;23:499–509.
Pinho-Gomes A-C, Knight A, Critchley J, Pennington M. Addressing the low consumption of fruit and vegetables in England: a cost-effectiveness analysis of public policies. J Epidemiol Community Heal. 2021;75:282–8.
White JM, Bégin F, Kumapley R, Murray C, Krasevec J. Complementary feeding practices: Current global and regional estimates. Matern Child Nutr. 2017;13: e12505.
Kleinman RE, Coletta FA. Historical overview of transitional feeding recommendations and vegetable feeding practices for infants and young children. Nutr Today. 2016;51:7.
Boeing H, Bechthold A, Bub A, Ellinger S, Haller D, Kroke A, Leschik-Bonnet E, Müller MJ, Oberritter H, Schulze M. Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr. 2012;51:637–63.
Fanzo J, Covic N, Dobermann A, Henson S, Herrero M, Pingali P, Staal S. A research vision for food systems in the 2020s: defying the status quo. Glob Food Sec. 2020;26: 100397.
Barends C, Weenen H, Warren J, Hetherington MM, de Graaf C, de Vries JHM. A systematic review of practices to promote vegetable acceptance in the first three years of life. Appetite. 2019;137:174–97.
RL Bailey, S Jun, AL Eldridge, The 2016 Feeding Infants and Toddlers Study (FITS): dietary intakes and practices of children in the United States from birth to 48 months, in: Nurtur. a Heal. Gener. Child. Res. Gaps Oppor., Karger Publishers, 2019: pp. 99–109.
Reidy KC, Bailey RL, Deming DM, O’Neill L, Carr BT, Lesniauskas R, Johnson W. Food consumption patterns and micronutrient density of complementary foods consumed by infants fed commercially prepared baby foods. Nutr Today. 2018;53:68.
Liu RH. Dietary bioactive compounds and their health implications. J Food Sci. 2013;78:A18–25.
Bhupathiraju SN, Wedick NM, Pan A, Manson JE, Rexrode KM, Willett WC, Rimm EB, Hu FB. Quantity and variety in fruit and vegetable intake and risk of coronary heart disease. Am J Clin Nutr. 2013;98:1514–23.
Cooper AJ, Forouhi NG, al Ye Z, Buijsse B, Arriola L, Balkau B, Barricarte A, Beulens JWJ, Boeing H, Büchner FL. Fruit and vegetable intake and type 2 diabetes: EPIC-InterAct prospective study and meta-analysis. Eur J Clin Nutr. 2012;66:1082–92.
Loef M, Walach H. Fruit, vegetables and prevention of cognitive decline or dementia: a systematic review of cohort studies. J Nutr Health Aging. 2012;16:626–30.
Evans CEL, Christian MS, Cleghorn CL, Greenwood DC, Cade JE. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am J Clin Nutr. 2012;96:889–901.
Johnson SL. Developmental and environmental influences on young children’s vegetable preferences and consumption. Adv Nutr. 2016;7:220S-231S.
Nekitsing C, Hetherington MM. Implementing a ‘Vegetables First’Approach to Complementary Feeding. Curr Nutr Rep. 2022;11:301–10.
P Jeelani, A Ghai, N Saikia, M Kathed, A Mitra, A Krishnan, A Sharma, R Chidambaram, Baby foods based on cereals, Food Sci Technol Nutr Babies Child. (2020) 59–97.
Lange C, Visalli M, Jacob S, Chabanet C, Schlich P, Nicklaus S. Maternal feeding practices during the first year and their impact on infants’ acceptance of complementary food. Food Qual Prefer. 2013;29:89–98.
Michaelsen KF, Greer FR. Protein needs early in life and long-term health. Am J Clin Nutr. 2014;99:718S-722S.
Fardet A. New hypotheses for the health-protective mechanisms of whole-grain cereals: what is beyond fibre? Nutr Res Rev. 2010;23:65–134.
Finn K, Callen C, Bhatia J, Reidy K, Bechard LJ, Carvalho R. Importance of dietary sources of iron in infants and toddlers: lessons from the FITS study. Nutrients. 2017;9:733.
Grimes CA, Szymlek-Gay EA, Campbell KJ, Nicklas TA. Food sources of total energy and nutrients among US infants and toddlers: National Health and Nutrition Examination Survey 2005–2012. Nutrients. 2015;7:6797–836.
Domellöf M, Braegger C, Campoy C, Colomb V, Decsi T, Fewtrell M, Hojsak I, Mihatsch W, Molgaard C, Shamir R. Iron requirements of infants and toddlers. J Pediatr Gastroenterol Nutr. 2014;58:119–29.
Edwards CA. Determinants and duration of impact of early gut bacterial colonization. Ann Nutr Metab. 2017;70:246–50.
Gamage HKAH, Tetu SG, Chong RWW, Ashton J, Packer NH, Paulsen IT. Cereal products derived from wheat, sorghum, rice and oats alter the infant gut microbiota in vitro. Sci Rep. 2017;7:14312.
Bernal MJ, Periago MJ, Martínez R, Ortuño I, Sánchez-Solís M, Ros G, Romero F, Abellán P. Effects of infant cereals with different carbohydrate profiles on colonic function—randomised and double-blind clinical trial in infants aged between 6 and 12 months—pilot study. Eur J Pediatr. 2013;172:1535–42.
Miniello VL, Verga MC, Miniello A, Di Mauro C, Diaferio L, Francavilla R. Complementary feeding and iron status:“the unbearable lightness of being” infants. Nutrients. 2021;13:4201.
Nekitsing C, Hetherington MM. Implementing a ‘vegetables first’ approach to complementary feeding. Curr Nutr Rep 2022;11(2):301–10.
N. and A. (NDA) EFSA Panel on Dietetic Products, Scientific Opinion on nutrient requirements and dietary intakes of infants and young children in the European Union, EFSA J. 11 (2013) 3408.
Jeelani P, Ghai A, Saikia N, Kathed M, Mitra A, Krishnan A, Sharma A, Chidambaram R. Baby foods based on cereals. In: Food science technology and nutrition for babies and children; 2020. p. 59–97.
A. NHMRC, Modelling System to Inform the Revision of the Australian Guide to Healthy Eating, Natl Heal Med Res Counc Dep Heal Ageing Aust Gov. (2011).
Kenney EL, Barrett JL, Bleich SN, Ward ZJ, Cradock AL, Gortmaker SL. Impact Of The Healthy, Hunger-Free Kids Act On Obesity Trends: Study examines impact of the Healthy, Hunger-Free Kids Act of 2010 on childhood obesity trends. Health Aff. 2020;39:1122–9.
L Peña Quintana, L Ros Mar, D González Santana, R Rial González, Alimentación del preescolar y escolar, (2010).
Serra JD, Villares JMM. Alimentación complementaria: puesta al día. Pediatria (Santiago). 2017;47: e1.
Tarrant RC, Younger KM, Sheridan-Pereira M, White MJ, Kearney JM. Factors associated with weaning practices in term infants: a prospective observational study in Ireland. Br J Nutr. 2010;104:1544–54.
O’Donovan SM, Murray DM, Hourihane JO, Kenny LC, Irvine AD, Kiely M. Adherence with early infant feeding and complementary feeding guidelines in the Cork BASELINE Birth Cohort Study. Public Health Nutr. 2015;18:2864–73.
Knutsen SH. Oats and rye: production and usage in Nordic and Baltic countries. Cereal Foods World. 2010;55:12–4.
Nwaru BI, Takkinen H, Niemelä O, Kaila M, Erkkola M, Ahonen S, Tuomi H, Haapala A, Kenward MG, Pekkanen J. Introduction of complementary foods in infancy and atopic sensitization at the age of 5 years: timing and food diversity in a Finnish birth cohort. Allergy. 2013;68:507–16.
Lund-Blix NA, Stene LC, Rasmussen T, Torjesen PA, Andersen LF, Rønningen KS. Infant feeding in relation to islet autoimmunity and type 1 diabetes in genetically susceptible children: the MIDIA Study. Diabetes Care. 2015;38:257–63.
Quann E, Carvalho R. Starch consumption patterns in infants and young children. J Pediatr Gastroenterol Nutr. 2018;66:S39–41.
Friel JK, Hanning RM, Isaak CA, Prowse D, Miller AC. Canadian infants’ nutrient intakes from complementary foods during the first year of life. BMC Pediatr. 2010;10:1–11.
Klerks M, Roman S, Bernal MJ, Haro-Vicente JF, Sanchez-Siles LM. Complementary feeding practices and parental pressure to eat among spanish infants and toddlers: a cross-sectional study. Int J Environ Res Public Health. 2021;18:1982.
Klerks M, Bernal MJ, Roman S, Bodenstab S, Gil A, Sanchez-Siles LM. Infant cereals: current status, challenges, and future opportunities for whole grains. Nutrients. 2019;11(2):473.
NHMRC A. Modelling system to inform the revision of the Australian guide to healthy eating. National Health Medical Research Council Department of Health Ageing, Australian government; 2011.
PT James, Z Ali, AE Armitage, A Bonell, C Cerami, H Drakesmith, M Jobe, KS Jones, Z Liew, SE Moore, Could nutrition modulate COVID-19 susceptibility and severity of disease? A systematic review, MedRxiv (2020).
Aman F, Masood S. How Nutrition can help to fight against COVID-19 Pandemic. Pakistan J Med Sci. 2020;36:S121.
Granato D, Barba FJ, Bursać Kovačević D, Lorenzo JM, Cruz AG, Putnik P. Functional foods: Product development, technological trends, efficacy testing, and safety. Annu Rev Food Sci Technol. 2020;11:93–118.
Cordeiro MA, Souza ELS, Arantes RME, Balthazar CF, Guimarães JT, Scudino H, Silva HLA, Rocha RS, Freitas MQ, Esmerino EA. Fermented whey dairy beverage offers protection against Salmonella enterica ssp enterica serovar Typhimurium infection in mice. J Dairy Sci. 2019;102:6756–65.
Khaneghah AM, Abhari K, Eş I, Soares MB, Oliveira RBA, Hosseini H, Rezaei M, Balthazar CF, Silva R, Cruz AG. Interactions between probiotics and pathogenic microorganisms in hosts and foods: A review. Trends Food Sci Technol. 2020;95:205–18.
Galdeano CM, Cazorla SI, Dumit JML, Vélez E, Perdigón G. Beneficial effects of probiotic consumption on the immune system. Ann Nutr Metab. 2019;74:115–24.
Oak SJ, Jha R. The effects of probiotics in lactose intolerance: A systematic review. Crit Rev Food Sci Nutr. 2019;59:1675–83.
Shafi A, Naeem Raja H, Farooq U, Akram K, Hayat Z, Naz A, Nadeem HR. Antimicrobial and antidiabetic potential of synbiotic fermented milk: a functional dairy product. Int J Dairy Technol. 2019;72:15–22.
Yilmaz-Ersan L, Ozcan T, Akpinar-Bayizit A. Assessment of socio-demographic factors, health status and the knowledge on probiotic dairy products. Food Sci Hum Wellness. 2020;9:272–9.
Vandenplas Y, Veereman-Wauters G, De Greef E, Peeters S, Casteels A, Mahler T, Devreker T, Hauser B. Probiotics and prebiotics in prevention and treatment of diseases in infants and children. J Pediatr (Rio J). 2011;87:292–300.
Oozeer R, Van Limpt K, Ludwig T, Ben Amor K, Martin R, Wind RD, Boehm G, Knol J. Intestinal microbiology in early life: specific prebiotics can have similar functionalities as human-milk oligosaccharides. Am J Clin Nutr. 2013;98:561S-571S.
Wong CB, Iwabuchi N, Xiao J. Exploring the science behind Bifidobacterium breve M-16V in infant health. Nutrients. 2019;11:1724.
Lin C, Lin Y, Zhang H, Wang G, Zhao J, Zhang H, Chen W. Intestinal ‘infant-type’bifidobacteria mediate immune system development in the first 1000 days of life. Nutrients. 2022;14:1498.
Cukrowska B, Ceregra A, Maciorkowska E, Surowska B, Zegadło-Mylik MA, Konopka E, Trojanowska I, Zakrzewska M, Bierła JB, Zakrzewski M. The effectiveness of probiotic Lactobacillus rhamnosus and Lactobacillus casei strains in children with atopic dermatitis and cow’s milk protein allergy: a multicenter, randomized, double blind, placebo controlled study. Nutrients. 2021;13:1169.
Saturio S, Nogacka AM, Alvarado-Jasso GM, Salazar N, de los Reyes-Gavilán CG, Gueimonde M, Arboleya S. Role of bifidobacteria on infant health. Microorganisms. 2021;9(1):29. https://doi.org/10.3390/microorganisms9122415.
Bhat MS, Lone FA, ul Shafiq M, Rather JA. Evaluation of long term trends in apple cultivation and its productivity in Jammu and Kashmir from, 1975 to 2015. GeoJournal. 2021;86:1193–202.
Hassan B, Bhattacharjee M, Wani SA. Economic analysis of high-density apple plantation scheme in Jammu and Kashmir. Asian J Agric Rural Dev. 2020;10:379–91.
Naqash F, Wani SA, Hamid N. Economics of controlled atmosphere storage of apple in Jammu and Kashmir State. J Pharmacogn Phytochem. 2019;8:308–12.
S Saraswat, R Khan, A Kumar, AP Singh, Impact of Mandatory Food and Agriculture Laws on the Food Manufacturing Industry: Review of 75 Years of Challenges and Changes, Converg. Cloud Comput AI Agric Sci. (2023) 228–260.
Lapillonne A, Mis NF, Goulet O, van den Akker CHP, Wu J, Koletzko B, Braegger C, Bronsky J, Cai W, Campoy C. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Lipids. Clin Nutr. 2018;37:2324–36.
Domellöf M, Szitanyi P, Simchowitz V, Franz A, Mimouni F, Braegger C, Bronsky J, Cai W, Campoy C, Carnielli V. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: iron and trace minerals. Clin Nutr. 2018;37:2354–9.
Saini RK, Sivanesan I, Keum Y-S. Phytochemicals of Moringa oleifera: a review of their nutritional, therapeutic and industrial significance. 3 Biotech. 2016;6:1–14.
J Kaparapu, PM Pragada, MNR Geddada, Fruits and Vegetables and its Nutritional Benefits, Funct Foods Nutraceuticals Bioact Components Formul Innov. (2020) 241–260.
Oozeer R, Van Limpt K, Ludwig T, Ben Amor K, Martin R, Wind RD, Boehm G, Knol J. Intestinal microbiology in early life: specific prebiotics can have similar functionalities as human-milk oligosaccharides. Am J Clin Nutr. 2013;98(2):561S–71S.
Banerjee D, Zhang Z, Plonka AM, Li J, Parise JB. A calcium coordination framework having permanent porosity and high CO2/N2 selectivity. Cryst Growth Des. 2012;12:2162–5.
Chun J, Lee J, Ye L, Exler J, Eitenmiller RR. Tocopherol and tocotrienol contents of raw and processed fruits and vegetables in the United States diet. J Food Compos Anal. 2006;19:196–204.
Płonka J, Toczek A, Tomczyk V. Multivitamin analysis of fruits, fruit–vegetable juices, and diet supplements. Food Anal Methods. 2012;5:1167–76.
Saturio S, Nogacka AM, Alvarado-jasso GM, Salazar N, de los Reyes-Gavilán CG, Gueimonde M, Arboleya S. Role of bifidobacteria on infant health. Microorganisms. 2021;9(12):2415.
Ceclu L, Nistor OV. Red beetroot: Composition and health effects—A review. J Nutr Med Diet Care. 2020;6:1–9.
Dreher ML. Whole fruits and fruit fiber emerging health effects. Nutrients. 2018;10:1833.
Mennella JA, Trabulsi JC. Complementary foods and flavor experiences: setting the foundation. Ann Nutr Metab. 2012;60:40–50.
Rather JA, Akhter N, Ayaz Q, Mir SA, Singh A, Goksen G, Majid D, Makroo HA, Dar BN. Fruit Peel Valorization, Phytochemical Profile, Biological Activity, and Applications in Food and Packaging Industries: Comprehensive Review. Curr Food Sci Technol Reports. 2023;1:63–79.
Maier-Nöth A. Early development of food preferences and healthy eating habits in infants and young children. Nurtur a Heal Gener Child Res Gaps Oppor. 2019;91:11–20.
Schwartz C, Scholtens PAMJ, Lalanne A, Weenen H, Nicklaus S. Development of healthy eating habits early in life Review of recent evidence and selected guidelines. Appetite. 2011;57:796–807.
Alam MD, Islam M, Ziaul MD, Tayab MD, Alam K, Sahid H, Kamrul MD, Mahmood S, Haque ATM. Role of Probiotic Lactobacillus reuteri in Improving Gut Health and Immunity in Infants and Toddlers: A Review. Int J Nutr Sci. 2022;7:75–80.
Wilkins T, Sequoia J. Probiotics for gastrointestinal conditions: a summary of the evidence. Am Fam Physician. 2017;96:170–8.
Ballini A, Gnoni A, De Vito D, Dipalma G, Cantore S, Gargiulo Isacco C, Saini R, Santacroce L, Topi S, Scarano A. Effect of probiotics on the occurrence of nutrition absorption capacities in healthy children: A randomized double-blinded placebo-controlled pilot study. Eur Rev Med Pharmacol Sci. 2019;23:8645–57.
Author information
Authors and Affiliations
Contributions
Najmeenah Akhter: Writing original draft, editing, conceptualization Darakshan Majid: Supervision, editing, reviewing Jahangir Ahmad Rather: Writing original draft, editing, conceptualization Mehvish majeed: Writing original draft Syeda tu Mehvish: Writing original draft B.N Dar: Supervision, editing, reviewing Hilal A. Makroo: Supervision, editing, reviewing Khalid Muzaffar: conceptualization, Reviewing Sajad Sofi: conceptualization, Reviewing.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Human and Animal Rights
The article does not contain any studies with humans or animal subjects performed by any of the authors.
Permissions
No permissions are needed for the figures or tables.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Akhter, N., Majid, D., Rather, J.A. et al. A Comprehensive Review on Formulation of Baby Foods: Nutraceutical potential of Fruits, Vegetables, Cereals and Probiotics in Baby Food Preparation. Curr Food Sci Tech Rep 2, 255–270 (2024). https://doi.org/10.1007/s43555-024-00034-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43555-024-00034-8