
Abstract
We study, for the first time, stillbirth differentials among native and migrant populations in Greece using national vital registration microdata for the period of 2010–2014. We employ conventional demographic measures and propose a standardization procedure to delineate the effect of selected distributions of livebirths on the observed stillbirth rates. The stillbirth rate among immigrant mothers is 40% higher than among natives, an excess which persists throughout gestational intervals and age groups. Our findings also show a clear gradient of stillbirth rates by maternal education, favoring more educated women, and this finding applies to both native and immigrant mothers. Our standardization methodology shows that the distribution of births by maternal educational level and age play a role; this finding implies that elevated immigrant stillbirth rates may be attributed to a certain extent to the specific characteristics of this group, since immigrant women have, on average, a younger age structure and lower educational attainment.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Fetal mortality is an adverse health outcome that significantly burdens families and poses a challenge both to society and to antenatal and health care systems. Spontaneous intrauterine death may arise at any time during pregnancy. Fetal deaths occurring in the third trimester of gestation are referred to as stillbirths. International statistical information on stillbirths is rather imprecise, largely due to varying definitions of fetal death and different reporting requirements and practices. For the purposes of international comparisons, a stillbirth refers to babies born with no sign of life at or after 28 weeks of gestation. In most countries, statistics on livebirths and stillbirths derive from national vital registration systems; population registers comprise a valuable source of information mainly in the Nordic countries, while sampling surveys also offer useful information.
Due to the poor quality of stillbirth statistics, it is difficult to form a clear picture of the level and pattern of stillbirths worldwide. It is estimated, however, that in 2015, there were approximately 2.6 million stillbirths recorded globally; this figure implies a daily number of around 7100 stillbirths and corresponds to a rate of 18.4 stillbirths per 1000 births on average, worldwide. Despite the sizeable decrease in overall stillbirth numbers (− 19% between 2000 and 2015), the pace of the decline in stillbirths has been slower than that of maternal mortality or mortality of children under five. The vast majority of stillbirths (98%) take place in low- and middle-income countries, while about half occur in the intrapartum period, which represents the period of greatest risk. It is widely argued that a large number of stillbirths could be prevented through targeted prenatal and health care policies (Blencowe et al 2016; Frøen et al 2011; Lawn et al 2009, 2011; Stanton et al 2006; WHO 2006).
A number of studies attribute stillbirth incidence to a range of causes. Among them, maternal disorders and infections (hypertension post-term pregnancy, malaria, HIV, etc.) are perhaps the most common. Fetal and placental causes also play a role (intrauterine fetal growth restriction, congenital anomalies, placental abruption, etc.), while some external causes (such as birth asphyxia and obstetric trauma) are relevant mainly in regions where modern obstetric methods are not widely practiced (Da Silva et al. 2016; Frøen et al 2004; WHO 2006; Woods 2008). Additional risk factors associated with a stillbirth outcome include age of mother, period of gestation, birthweight, birth order, multiplicity of births, maternal BMI, and unhealthy behaviors during pregnancy, smoking or drinking, for example (Aminu et al 2014; Flenady et al 2011; Frøen et al 2001; Lawn et al. 2016; Reddy et al 2010). With regard to maternal age, which is the most important demographic characteristic, studies reveal elevated stillbirth risk for women younger than 20 and older than 35 years (MacDorman and Kirmeyer 2009; Davies-Tuck et al. 2017).
It has been observed that socioeconomic disparities in stillbirth outcomes exist even in high-income countries. Women living in poor socioeconomic conditions have twice the risk of a stillbirth compared to women living in more advantageous ones (Flenady et al 2016). Research based on data from 29 European countries shows a significantly elevated risk of stillbirth for women of low education, as compared to highly educated mothers; similarly (Zeitlin et al 2016). Analogous findings are presented for England, showing a substantial gap between most and least deprived population groups for almost all causes of fetal deaths (Seaton et al 2012).
Among the indicators determining socio-cultural position, maternal education is perhaps the most important factor associated with stillbirth risk. A large-scale study in Canada on stillbirths and livebirths found greater stillbirth rates for women of lower educational level compared to more educated ones, and this finding persisted over the whole gestational period (Auger et al 2012). Another study based on national birth registries during 1980s and 1990s found sizeable educational inequalities and gradients in stillbirth risk in Scandinavian countries (Rom et al 2012); similar results have also been reported for Spain (Luque-Fernadez et al 2011).
Numerous studies find striking differences in stillbirth rates and risks by native-migrant status and by ethnic group, which in turn are linked to educational disparities and health-related practices. For Spain, it is found that the average stillbirth rate of non-Spanish women over the period of 2007–2012 was 58% higher than among Spanish mothers (3.99 and 2.51 per 1000, respectively) (Fuster et al. 2014). It is also shown for Spain that, for the period 2007–2010, African-born mothers had almost twice the risk of a stillbirth compared to native women (Luque-Fernandez et al 2013). Both studies support the importance of education in explaining observed differences. Analysis of German data from 2004 to 2007 shows elevated stillbirth rates among mothers who originated from the Middle East, North Africa, and Turkey, which are also associated with low socioeconomic status and low birthweight (Reeske et al 2011). High stillbirth risk for immigrant mothers from Africa and the Middle East relative to native mothers is also observed in Swedish data for the period of 1992–2005; recent migrants who have spent less than five years in the host country are found to exhibit elevated risks (Ekéus et al 2011). Ethnic stillbirth differentials have also been studied in Denmark for the period of 1981–2003 and they showed that women from Turkey, Pakistan and Somalia had significantly higher fetal mortality than Danish women, although, in this instance, immigrant fetal mortality surplus was not attributed to socioeconomic factors (Villadsen et al. 2009). Studies in Canadaalso reveal the importance of the origin of immigrants reporting that immigrants originating from high fetal mortality regions tended to have elevated stillbirth rates in Ontario over 2002–2011, but this may be partly attributed to genetic and environmental factors (Bartsch et al 2015). In the USA, ethnic and racial differentials in stillbirth rates show elevated risks for black women compared to white women, which in part reflects varying accessibility to health and medical care (Kallan 2001; Rowland-Hogue and Silver 2011; Vintzileos et al 2002).
Purpose of the paper
Disparities in stillbirth rates by socioeconomic position and migrant status of mothers for Greece have hitherto not been analyzed. Moreover, Greece lends itself for this analysis because it has undergone a series of waves of migration, and so there are sufficient women from particular foreign origins on which to base the analysis.
We use national vital registration microdata on stillbirths and livebirths recorded during the period of 2010 to 2014 with two objectives. First, to study demographic differentials and socioeconomic inequalities in stillbirth levels among native and foreign-origin mothers living in Greece; second, to propose a quantitative approach, based on the well-known demographic technique of direct standardization, to assess the influence of the distribution of births by key maternal socio-demographic characteristics on the stillbirth rates of native and selected foreign-origin populations.
Data
In Greece, national statistical information on livebirths and stillbirths can be derived from birth certificate records available through the national vital registration system. Vital registration data are compiled and published by the Hellenic Statistical Authority (ELSTAT). Birth registration in Greece is complete and, since virtually all births (99.9%) take place in maternity wards and hospitals, the information recorded on birth certificates is considered reliable. Nevertheless, there may be under-registration of a small, but undefined, number of stillbirths, particularly in non-metropolitan areas. In Greece, vital statistics on stillbirths are available for fetal deaths of 18 weeks of gestation or more; however, in this study, we focus on fetal deaths of babies born with no sign of life at or after 28 weeks of gestation, so as to be in accordance with the international recommendations for data comparability.
The analysis is based on microdata on livebirths and stillbirths registered nationwide during the period of 2010–2014. The aforementioned statistical material is unpublished and has been kindly offered to the authors by the Hellenic Statistical Authority (ELSTAT) upon request. The dataset contains the statistical information included in the birth certificate and refers to the number of vital events of livebirths and stillbirths cross-classified by various socio-demographic characteristics of the mother and the father, as well as of the newborn. The available data include the date of birth, sex of the newborn, the place where the event occurred (maternity hospital, clinic, private residence, other), birthweight (in grams), birth order (1, 2,…6 +), period of gestation (in weeks), type of delivery (single birth, multiple births, i.e., twins, triple or more), and legitimacy (based on the marital status of mother at confinement); with respect to the parents of the newborn, there is information on the age of the mother/father (in years), the exact place of their usual residence, as well as their citizenships. The dataset includes also two variables related to the socioeconomic status of the parents, though paternal characteristics are not provided for births outside of marriage (about 7.5% of the sample). The first variable concerns the occupation of the mother and of the father. This information, however, is not suitable for analysis due to a relatively large proportion of people who do not report their occupation and mainly because the information that is reported is vague or invalid; for example, 36% of native mothers and 79% of foreign mothers declare that they are retired or engaged in family duties or they are students. The second variable concerns the level of education of the parents. The mother and father of the newborn report the level of education they have completed; in this case, the quality of data is much better. Hence, in this study, the socioeconomic position of mothers is determined by their reported level of education; this variable distinguishes mothers with no formal education (illiterates), from mothers who have completed primary education, lower secondary, upper secondary and post-upper secondary, and tertiary education. However, due to recent changes in the system of collecting and verifying vital statistics performed by ELSTAT, since 2013, the distribution of livebirths and stillbirths by educational level is of poor quality with information on education missing in over 50% of the recorded vital events. Hence, although the entire analysis relies on vital events registered during the 5-year period from 2010 to 2014, the analysis concerning indices and measures involving educational characteristics refers to the 3-year period from 2010 to 2012.
For the purpose of the analysis, we focus on age, educational level, and citizenship of the mother. Due to the rather small annual number of fetal deaths, as well as the confidentiality requirements imposed for material compiled at individual level, the analysis assigned to migrant and non-migrant mothers distinguishes four subgroups only, Greek-natives, Albanians, Bulgarians, and all other immigrants combined. To identify the immigrant populations, the notion of citizenship is employed as this is the official definition used by the Ministry of the Interior and the Greek statistical authorities (HMPI 2007; MIPAD 2007). Throughout the paper, the terms “migrant,” “immigrant,” “foreign-origin,” as well as “Greek” and “native” women are used interchangeably.
Methods
In the first part of the study, we employ formal demographic techniques to delineate stillbirth differentials. In the second part, we propose a standardization procedure to assess the effect of the distribution of births by socio-demographic attributes on fetal mortality rates observed among native and migrant populations.
Stillbirth measures
To measure the fetal mortality, two types of indices are used: the stillbirth ratio, which expresses number of stillbirths per 1000 livebirths, and the stillbirth rate which is defined as the ratio of stillbirths per 1000 total births (i.e., stillbirths and livebirths).
The stillbirth ratio is the preferred measure for international comparisons due to cross-country variation in the quality of vital statistics and the effectiveness of vital registration systems. On the other hand, the stillbirth rate relates the fetal outcome more closely to the population at risk, and hence, it has some theoretical advantages over the stillbirth ratio (Siegel and Swanson 2004); nevertheless, in practice, at least for developed countries, the difference in magnitude between stillbirth rates and ratios is trivial.
For the purpose of this study, we use the stillbirth rate. Let S denote the number of stillbirths and L the number of livebirths registered during a specified period of time. The stillbirth rate (\(SBR\)) is given by:
while the relative standard error (RSE) of the stillbirth rate is:
In the case of large numbers of stillbirths (100 or more), the statistical significance of a difference between two stillbirth rates (let us say \(SBR_{1}\) and \(SBR_{2}\)) can be assessed on the basis of the Z-statistic:
but for a small number of observations (stillbirths < 100), appropriate formulae based on the Poisson distribution should be employed (MacDorman et al 2012).
Standardization of stillbirth rates
Let \(S_{i}\) and \(B_{i} = S_{i} + L_{i}\) be the numbers of stillbirths and all births (= stillbirths + livebirths), respectively, cross-classified by a characteristic i, for instance, age of mother, years of educational attainment, etc.
For all \(i\):
-
the total number of stillbirths is
$$ S = \sum\limits_{i} {S_{i} } $$(4) -
and the total number of births is
$$ B = \sum\limits_{i} {(S_{i} + L_{i} ) = } \sum\limits_{i} {B_{i} } $$(5)
Hence, the stillbirth rate (\(SBR\)) is:
or
where, \(r_{i} = \frac{{S_{i} }}{{B_{i} }}\) is the stillbirth rate specific for characteristic i, and \(c_{i} = \left( {\frac{{B_{i} }}{B}} \right)\) is the relative distribution of all births by characteristic i.
Hence, differences between two or more overall stillbirth rates may arise from differences in either the specific stillbirth rates (\(r_{i}\)) or the relative distribution of births by characteristic \(i\) (\(c_{i}\)). We follow this standardization procedure to investigate stillbirth variations between Greek, Albanian, and Bulgarian mothers. Thus, we are computing counterfactuals and comparing with observed patterns; for instance, considering \(c_{i}\) as a “standard” schedule, we explore what the SBR would be for, say, Albanian mothers, if they had the same educational profile or age structure as Greek mothers.
Results
Descriptive findings
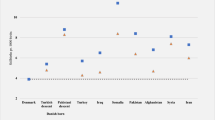
Over the period of 2010 to 2014, 1669 stillbirths and 502,112 livebirths were recorded in Greece, corresponding to about 335 and 102,500 per year, respectively. 78% of stillbirths and 84% of livebirths were assigned to Greek mothers. The average stillbirth rate of the population from 2010 to 2014 is 3.3 stillbirths per 1,000 births, which is somewhat lower than the median rate (3.6) observed in EU countries over the same period. Our data show sizable and statistically significant differences in the stillbirth rates between natives (3.1) and immigrant populations (4.5) living in Greece (z-statistic = 11.5). With respect to the most frequent foreign-origin populations, the stillbirth rate among Albanians is 3.7 and among Bulgarians 5.9 (Fig. 1); these rates, however, are lower compared to the corresponding rates observed in their respective countries of origin (5.3 and 7.6 per 1000 births in Albania and Bulgaria, respectively).

Stillbirth rates by citizenship: Greece 2010–2014
Stillbirth rates by age of mother reveal a U-type curve exhibiting an increasing pace of fetal loss for young mothers (< 20 years) and from the age of 35 onwards; this age pattern holds for both the native and immigrant populations, while the excess of immigrant over native stillbirth rates is present across all age groups (Fig. 2).

Age-specific stillbirth rates by citizenship: Greece 2010–2014
Our analysis also reveals considerable socioeconomic inequality in stillbirth rates on the basis of educational level attained by the mother. Figure 3 portrays a gradient of rates with illiterate mothers experiencing the highest rate (7.0), which gradually declines to 2.4 per 1000 among the most educated mothers. This pattern is replicated across all age groups of mothers (Fig. 4). Socioeconomic differentials in stillbirth rates are exhibited among both native and immigrant populations; however, variations of stillbirth rates by educational level are greater among Greek than among foreign-origin mothers (Fig. 5). Among native mothers, the stillbirth rates range from 2.4 (tertiary) to 7.2 (illiterates) per 1000 births (coefficient of variation = 43%) while among immigrant mothers, the corresponding rates range from 3.4 (tertiary) to 6.3 (illiterates) per 1000 births (coefficient of variation = 24%).

Stillbirth rates by education of mother: Greece 2010–2012

Age-specific stillbirth rates by education of mother: Greece 2010–2012

Stillbirth rates by citizenship and education of mother: Greece 2010–2012
Standardization of stillbirth rates
The distribution of births by certain maternal characteristics differs considerably between native and migrant populations and ethnic groups. For instance, immigrant mothers are younger than natives (the median ages are 27 and 31 years, respectively). Furthermore, native mothers are more educated than immigrants (the proportion of births assigned to Greek and immigrant mothers with at least upper secondary education are 87.1% and of 37.7%, respectively). These situations tend, to some extent, to compress or expand aggregate measures of fetal loss.
In the direct standardization technique used in demography, a “standard” age distribution is applied to observed age-specific death rates to eliminate age effects and delineate differences in mortality levels. Here, we follow a similar approach and apply a “standard” birth distribution to observed stillbirth rates specific for a chosen maternal characteristic, in order to unveil differentials in stillbirth rates that cannot be captured using conventional indices. The procedure described in “Stillbirth measures” applied here to assess the effect of the distribution of births by age and by education of the mother on recorded stillbirth rates. In the Appendix, Tables 1 and 2 present in detail the computational procedure employed.
With respect to education, the distribution of births of Greek mothers by educational level is taken as the “standard schedule” and is applied to the observed education-specific stillbirth rates of Albanian and Bulgarian mothers, as well as to the broad category of “all other” immigrants. The standardized rates allow estimation of what would have been the stillbirth rates of the selected populations, if they had the same educational distribution of births as native mothers. The results are presented in Fig. 6 and are consistent with our a priori expectation that the standardized stillbirth rates would be lower than the observed ones. The variation in the overall stillbirth rates across the four population groups (Greek, Albanian, Bulgarian, all Other) is substantially reduced but not eliminated. The most marked outcome is that for Bulgarian mothers, who exhibit a more pronounced decline in stillbirth rates compared to other ethnic groups.

Observed and standardized stillbirth rates (per 1000) of selected foreign-origin populations using the relative distribution of births by education of the Greek mothers as standard schedule: Greece 2010–2012
Figure 7 presents the standardized stillbirth rates calculated using the age distribution of births of Greek mothers as “standard.” The results are also in accordance with our a priori expectations. For all immigrant groups, the age-standardized stillbirth rates are higher than the observed ones; hence, the difference compared to native mothers appears wider. The variation of the observed and standardized stillbirth rates across immigrant groups remains about the same.

Observed and standardized stillbirth rates (per 1000) of selected foreign-origin populations using the relative distribution of births by age of the Greek mothers as standard schedule: Greece 2010–2014
Discussion
In this paper, we study for the first time stillbirth levels and differentials among natives and migrants living in Greece, using national vital registration microdata for the period of 2010 to 2014. Our analysis is representative of the period of 2010–2018, since stillbirth rates in Greece remained virtually constant over that period. Stillbirth rates seem to have increased somewhat in 2019 and 2020, according to the most recently published data, possibly due to the covid-19 pandemic affecting both livebirths and stillbirths. However, data for 2019 and 2020 are available in total numbers only and thus do not allow for a detailed study of the most recent period. In our analysis, we employ conventional demographic measures as well as a standardization procedure to delineate the influence of selected distributions of births on the observed stillbirth rates.
The average stillbirth rate from 2010 to 2014 among immigrant mothers is 40% higher than among natives. The difference is statistically significant, and the migrant stillbirth excess persists throughout gestational intervals and age groups. The age pattern of stillbirth rates outlines a U-type curve, with higher rates for younger (< 20 years) and older (35 +) women. Our findings also show a clear socioeconomic gradient favoring more educated women; this finding applies to both native and immigrant mothers. The elevated immigrant stillbirth rates may be attributed to a certain extent to dissimilarities between native and migrant mothers regarding certain characteristics associated with high stillbirth risk; immigrant mothers are less educated while the majority originates from countries of high stillbirth rates. Although immigrant mothers from Albania and Bulgaria exhibit higher rates than Greek native mothers, they experience lower stillbirth outcomes compared to their origin countries. This may be partly due to migrant selection (immigrant women have better health compared to their counterparts in their country of origin) but may also reflect the relative effectiveness of the Greek health care system and better use of obstetrics practices in Greece.
The results based on the standardization methodology show that the distribution of births may also influence the stillbirth indices. In our analysis, the effect is more pronounced with respect to the educational distribution, but both factors act in line with the a priori expectations. Clearly, the standardization technique can be employed more broadly to study further cross-sectional differentials as well as over time changes (Kitagava 1964). A multiple standardization procedure might further delineate the workings of these factors but would result in palpable and meaningful outcomes only if the effect of the population characteristics under investigation acts toward the same direction (Preston et al 2001). However, the application of a multiple-standardized methodology to our data resulted in unclear results because the distributions of births by education and by age of mother operate in different ways.
Some limitations of the study should be noted. First, in this study, due to data availability, we used only maternal educational attainment as a proxy for socioeconomic status, which could result in interpretational complexities caused by cross-country differences in definitions between educational systems (Psaki et al 2014). In this research, we are not making comparisons across countries but we consider educational effects on stillbirth rates across national and immigrant populations. From this point of view, therefore, some biases may exist, as the notion of “completed level of education,” which is employed in birth certificates, may be perceived in different ways by immigrant groups; unfortunately, possible effects cannot be quantified. Second, vital statistics do not provide information on certain characteristics or health behaviors (e.g., smoking and drinking during pregnancy), which the literature points to as highly relevant factors. Finally, the time of migration is not recorded, so that associations of stillbirth rates with length of living in the receiving country or with naturalizations cannot be studied.
Conclusion
When the data allow it, the application of demographic standardization methodology can mark out interesting aspects of stillbirth differentials between populations. This study shows that among the socio-demographic factors associated with stillbirth outcome, the level of education of the mother proves to be an important determinant for both native and migrant populations. Therefore, policies directed at reducing educational disparities, or broad information campaigns, might be effective in diminishing migrant disadvantage.
Data availability
The data that support the findings of this study are available from the Hellenic Statistical Authority (ELSTAT) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with the permission of ELSTAT.
References
Aminu M, Unkels R, Mdegela M et al (2014) Causes of and factors associated with stillbirth in low- and middle-income countries: a systematic literature review. BJOG 121(Suppl 4):141–153
Auger N, Delézire P, Harper S, Platt W (2012) Maternal education and stilbirth, estimating gestational-age-specific and cause-specific associations. Epidemiology 23(2):247–254
Bartsch E, Park AL, Pulver AJ et al (2015) Maternal and paternal birthplace and risk of stillbirth. J Obstet Gynaecol Can 37(4):314–323
Blencowe J, Cousens S, Jassir FB et al (2016) National, regional and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. The Lancet 4:e98–e108
Da Silva FT, Gonik B, McMillan M (2016) Stillbirth: case definition and guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine 34:6057–6068. https://doi.org/10.1016/j.vaccine.2016.03.044
Davies-Tuck ML, Davey M-A, Wallace EM (2017) Maternal region of birth and stillbirth in Victoria, Australia 2000–2011: a retrospective cohort study of Victorian perinatal data. PLoS ONE 12(6):e0178727. https://doi.org/10.1371/journal.pone
Ekéus C, Cnttingius S, Essén B, Hjern A (2011) Stillbirth among foreign-born women in Sweden. Eur J Public Health 21(6):788–792. https://doi.org/10.1093/eurpub/ckq200
Flenady V, Koopmans L, Middleton P et al (2011) Major risk factors for stillbirth in high-income countries: a systematic review and meta-analysis. Lancet 377:1331
Flenady V, Wojcieszek AM, Middleton PM et al (2016) Stillbirths: recall to action in high-income countries. Ending preventable stillbirths 4. The Lancet. https://doi.org/10.1016/S0140-6736(15)01020-X
Frøen JF, Arnestad M, Frey K et al (2001) Risk factors for sudden intrauterine unexplained death: epidemiologic characteristics of singleton cases in Oslo, Norway, 1986–1995. Am J Obstet Gynecol 184:694
Frøen JF, Cacciatore J, McClure EM et al (2011) Stillbirths: why the matter. The Lancet 377:1353–1366. https://doi.org/10.1016/S0140-6736(10)62232-5
Frøen JF, Gardosi JO, Thurmann A et al (2004) Restricted fetal growth in sudden intrauterine unexplained death. Acta Obstet Gynecol Scand 83:801–807
Fuster V, Zuluaga P, Roman-Busto J (2014) Stillbirth incidence in Spain: a comparison of native and recent immigrant mothers. Demogr Res 31:889–912
HMPI (2007) Legislation and requirements concerning acquisition of the Greek citizenship. Hellenic Migration Policy Institute. On line State Documentation. http://www.imepo.gr
Kallan JE (2001) Rates of fetal death by maternal race, ethnicity, and nativity: New Jersey 1991–1998. JAMA 285:2978–9
Kitagava EM (1964) Standardized comparisons in population research. Demography I(1):296–315
Lawn JE, Blencowe H, Pattinson R et al (2011) Stillbirths: Where? When? Why? How to make the data count? The Lancet 377:1448–1463. https://doi.org/10.1016/S0140-6736(10)62187-3
Lawn JE, Blencowe H, Waiswa P et al (2016) Stillbirths: rates, risk factors, and acceleration towards 2030. The Lancet 387:587–603. https://doi.org/10.1016/S0140-6736(15)00837-5
Lawn JE, Yakoob MY, Haws RA et al (2009) 3.2 million stillbirths: epidemiology and overview of the evidence review. BMC Pregnancy Childbirth 9(Suppl1):S2. https://doi.org/10.1186/1471-2393-9-S1-S2
Luque-Fernadez MÁ, Lone NI, Gutiérrez-Garitano I, Bueno-Cavanillas A (2011) Stillbirth risk by maternal socio-economic status and country of origin: a population-based observational study in Spain 2007–08. Eur J Public Health 22(4):524–529. https://doi.org/10.1093/eurpub/ckr074
Luque-Fernandez MA, Franco M, Gelaye B et al (2013) Unemployment and stillbirth risk among foreign-born and Spanish pregnant women in Spain, 2007–2010: a multilevel analysis study. Eur J Epidemiol 28:991–999
MacDorman MF, Kirmeyer S (2009) The challenge of fetal mortality. NCHS data brief, no. 16. National Center for Health Statistics, Hyattsville
MacDorman MF, Kirmeyer SE, Wilson EC (2012) Fetal and perinatal mortality United States 2006. National Center for Health Statistics National Vital Statistics Reports, Hyattsville, pp 1–17
MIPAD (2007) Legislation concerning the foreign citizens in Greece. Ministry of the Interior, Public Administration and Decentralization. On line State Documentation http://www.ypes.gr
Preston SH, Heuveline P, Guilot M (2001) Demography, measuring and modeling population processes. Blackwell, Oxford
Psaki SR, Seidman JC, Miller M et al (2014) Measuring socioeconomic status in multicountry studies: results from the eight-country MAL-ED study. Popul Health Metrics. https://doi.org/10.1186/1478-7954-12-8
Reddy UM, Laughon SK, Sun L et al (2010) Pregnancy risk factors for antepartum stillbirth in the United States. Obstet Gynecol 116:1119
Reeske A, Kutschmann M, Razum O, Spallek J (2011) Stillbirth difference according to regions of origin: an analysis of the German perinatal database, 2004–2007. BMC Pregnancy Childbirth 11:63
Rom AL, Mortensen LH, Cnattingius A et al (2012) A comparative study of educational inequality in the risk of stillbirth in Denmark, Finland, Norway and Sweden 1981–2000. J Epidemiol Community Health 66:240–246. https://doi.org/10.1136/jech.2009.101188
Rowland-Hogue CJ, Silver RM (2011) Racial and ethnic disparities in United States: stillbirth rates: trends, risk factors, and research needs. Semin. Perinatol. 35(4):221–233
Seaton SE, Field DJ, Draper ES et al (2012) Socioeconomic inequalities in the rate of stillbirths by cause: a population-based study. BMJ Open 2:e001100. https://doi.org/10.1136/bmjopen-2012-001100
Siegel JS, Swanson DA (eds) (2004) The methods and materials of demography. Academic Press-Elsevier, New York
Stanton C, Lawn JE, Rahman H et al (2006) Stillbirth rates: delivering estimates in 190 countries. The Lancet 367:1487–1494
Villadsen SF, Mortensen LH, Andersen AM (2009) Ethnic disparity in stillbirth and infant mortality in Denmark 1981–2003. J Epidemiol Community Health 63:106–112. https://doi.org/10.1136/jech.2008.078741
Vintzileos AM, Ananth CV, Smulian JC et al (2002) Prenatal care and black-white fetal death disparity in the United States: heterogeneity by high-risk conditions. Obstet Gynecol 99:483–489
WHO (2006) Neonatal and perinatal mortality: country, regional and global estimates. World Health Organization. https://apps.who.int/iris/handle/10665/43444
Woods R (2008) Long-term trends in fetal mortality: implications for developing countries. Bull. WHO 86:460–466
Zeitlin J, Mortensen L, Prunet C et al (2016) Socioeconomic inequalities in stillbirth rates in Europe: measuring the gap using routine data from the Euro-Peristat Project. BMC Pregnancy Childbirth 16:15. https://doi.org/10.1186/s12884-016-0804-4
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors have no competing interests to declare that are relevant to the content of this article.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Tsimbos, C., Verropoulou, G. & Petropoulou, D. Socioeconomic inequality and stillbirth rate disparities among native and foreign mothers: evidence from Greece. SN Soc Sci 2, 140 (2022). https://doi.org/10.1007/s43545-022-00410-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s43545-022-00410-y