
Abstract
Study design
Multicenter retrospective.
Objective
To determine the long-term complication rate associated with surgical treatment of spondylolisthesis in adolescents.
Summary of background data
There is limited information on the complication rate associated with posterior spinal fusion (PSF) of spondylolisthesis in the pediatric and adolescent population.
Methods
Patients who underwent PSF for spondylolisthesis between 2004 and 2015 at four spine centers, < 21 years of age, were included. Exclusion criteria were < 2 years of follow-up or anterior approach. Charts and radiographs were reviewed.
Results
50 patients had PSF for spondylolisthesis, 26 had PSF alone, while 24 had PSF with trans-foraminal lumbar interbody fusion (TLIF). Mean age was 13.9 years (range 9.6–18.4). Mean follow-up was 5.5 years (range 2–15). Mean preoperative slip was 61.2%. 20/50 patients (40%) experienced 23 complications requiring reoperation at a mean of 2.1 years (range 0–9.3) for the following: implant failure (12), persistent radiculopathy (3), infection (3), persistent back pain (2), extension of fusion (2), and hematoma (1). In addition, there were 22 cases of radiculopathy (44%) that were transient. Rate of implant failure was related to preoperative slip angle (p = 0.02). Reoperation rate and rates of implant failure were not associated with preoperative % slip (reoperation: p = 0.42, implant failure: p = 0.15), postoperative % slip (reoperation: p = 0.42, implant failure: p = 0.99), postoperative kyphosis of the lumbosacral angle (reoperation: p = 0.81, implant failure: p = 0.48), change in % slip (reoperation: p = 0.30, implant failure: p = 0.12), change in slip angle (reoperation: p = 0.42, implant failure: p = 0.40), graft used (reoperation: p = 0.22, implant failure: p = 0.81), or addition of a TLIF (reoperation: p = 0.55, implant failure: p = 0.76).
Conclusion
PSF of spondylolisthesis in the adolescent population was associated with a 40% reoperation rate and high rate of post-operative radiculopathy. Addition of a TLIF did not impact reoperation rate or rate of radiculopathy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Spondylolisthesis is typically treated first with non-surgical methods, with surgical intervention reserved for refractory cases. Indications for operative treatment include the presence of deformity, pain despite conservative management, stenosis, neurologic deficits, and radiographic progression [1,2,3].
Surgical treatment of spondylolisthesis in both children and adults is associated with a high rate of post-operative complications, including neurologic injury, implant failure, continued deformity progression, and infection [4,5,6,7,8,9,10,11,12,13,14]. However, the majority of published papers have small sample sizes and high complication rates, which make elucidating risk factors difficult. Additionally, many of them were prior to routine use of instrumentation with pedicle screws and the use of trans-foraminal lumbar interbody fusion (TLIF). The purpose of this study was to use data from multiple high-volume spine centers to investigate the risk factors and complication rates for operative treatment of spondylolisthesis in the pediatric population.
Methods
This study was an institutional review board-approved retrospective review. Patients < 21 years of age who underwent operative procedures for spondylolisthesis at four high-volume spine centers, each of which perform more than 50 pediatric spine surgeries annually, from 2004 to 2015 were eligible for inclusion. Patients were excluded if they had < 2 years of follow-up or underwent an anterior approach. Preoperative information included patient demographics and symptoms related to spondylolisthesis, such as back pain on extension and radiculopathy. Intraoperative information collected included type of procedure, operative time, use of bone morphogenic protein (BMP), use of bone graft, and if a reduction of the spondylolisthesis was attempted. Postoperative protocols varied by institution, with two institutions utilizing postoperative bracing blocking hip flexion to 45° with an extension to the femur for 3 months. Complications were defined as issues requiring a return to the operating room related to the index procedure. Preoperative and postoperative radiographs were reviewed for percent slip and slip angle. All measurements were done in accordance with the Spinal Deformity Study Group Radiographic Measurement Manual [15].
Statistical analysis
Descriptive data were summarized using mean, range, and standard deviation. Correlation between continuous variables and development of complications was analyzed using independent t-tests or one-way ANOVA. Relationship between categorical variables and development of complications was analyzed using Chi-square analysis or Fisher’s exact test. In general, the indication for operative intervention for spondylolisthesis is a grade of 3 or greater or persistent pain in a grade 1 or 2 slip. As such, additional analysis was performed comparing those patients with slips of grades 1 and 2 versus grades 3, 4, and 5.
Results
50 patients met the inclusion criteria. Mean BMI was 21.4 (range 14.5–34.4, SD 4.7). Mean age at time of surgery was 13.9 years (range: 9.6–18.4, SD: 2.2). Mean follow-up was 5.5 years (range 2.0–15.0, SD 3.0). 52.0% (n = 26/50) of spondylolistheses were dysplastic, 46.0% (n = 23/50) were acquired. In one patient, the type of spondylolisthesis was unable to be determined. 96.0% (n = 48/50) of slips were at the L5–S1 level, 4% (n = 2/50) slips were at the L4–L5 level. Mean preoperative slip was 61.1% (range: 3–104.9, SD 31.3). 9 patients (18%) had grade 1 slips, 5 (10%) had grade 2, 15 (30%) had grade 3, 16 (32%) had grade 4, and 5 (10%) had grade 5 (spondyloptosis) slips. Although, as one would predict, there were higher preoperative and postoperative slip angles in the patients who had spondylolisthesis of grades 3, 4, or 5 versus Grades 1 or 2, the percent change in slip angle was no different (p = 0.95) (Table 1). There was no relationship between slip grade and reoperation rate (p = 0.84). Mean preoperative slip angle was 27.3° (range 5–65, SD 14.7) (Table 2).
All 50 patients underwent PSF for their spondylolisthesis. Site A performed 12 cases, site B performed 18 cases, site C performed 15 cases, and site D performed 5 cases for a total of 50 cases. 48 patients had PSF with instrumentation and 2 had PSF without instrumentation. Of those who were instrumented, 24 had PSF augmented with TLIF. The preoperative grade was slightly lower in the non-instrumented group (mean 1.5) compared to the instrumented PSF group (mean 3.5), although this did not achieve statistical significance in a Tukey post hoc analysis (p = 0.06) There was no difference in preoperative kyphosis of the lumbosacral angle between groups (Table 3). 3/5 spondyloptosis cases underwent reduction, while the other 2 cases were instrumented in situ. 1 of the reduced cases and 1 of the non-reduced cases went on to implant failure.
Of the 48 patients who had lumbosacral slips, 40 patients had bilateral S1 implants, and 8 had both S1 and sub-S1 implants. Of the 50 patients, 30 (60%) had instrumentation to L5 proximally and 20 (40%) had instrumentation to the L4 level. None of the patients had fusion above L4. Of the patients who had L5–S1 instrumentation, one went on to have an extension of their fusion to the L4 level at the time of reoperation for pseudarthrosis and implant failure. This occurred in the acute postoperative period. No other patients had proximal extension of their constructs during the follow-up period. Information on reduction was available for 35 patients; 60% (n = 21/35) had an attempted reduction. BMP was used in 4.0% (n = 2/50) of patients. Bone graft was used in all patients; 68.0% (n = 34/50) had autograft only, 18.0% (n = 9/50) had both autograft and allograft, and 14.0% (n = 7/50) had allograft only. Of those who received autograft, 74.4% (32/43 received local bone graft, 20.9% (9/43) received iliac crest bone graft, and 4.7% (2/43) were unspecified. 34.0% (n = 17/50) of patients had postoperative bracing (Table 7).
40% of patients (n = 20/50) experienced 23 complications requiring reoperation at a mean of 2.1 years (range 0–9.3, SD 2.3) for the following: implant failure (12), persistent radiculopathy (3), infection (3), persistent back pain (2), extension of fusion (2), and hematoma (1) (Table 4). Implant failures included pseudarthrosis (8), prominent implants (2), screw breakage (1), and rod displacement (1). Details for the implant failures can be seen in Table 5. Reoperation rates did not differ between the 4 surgical sites (p = 0.18). Overall, the reoperation rate was not associated with patient BMI (none = 22.2, reoperation = 20.6, p = 0.23), type of spondylolisthesis (dysplastic = 50.0%, 13/26; acquired = 39.1%, 9/23, p = 0.45), grade of spondylolisthesis (p = 0.84), pre-op % slip (none = 60.6%, reoperation = 61.7%, p = 0.91), post-op % slip (none = 28.3% reoperation = 32.9%, p = 0.43), post-op kyphosis of the lumbosacral angle (none = 36.6°, reoperation = 40.4°, p = 0.81), change in slip angle (none = − 2.7%, reoperation = − 15.6%; p = 0.42) or change in percent slip (none = − 52.1%, reoperation = − 45.5%, p = 0.30) (Table 6). There was also no correlation between reoperation rate and type of graft used (allograft = 71%, 5/7; autograft = 35%, 12/34, allograft and autograft = 66.6%, 6/9; p = 0.22), addition of a TLIF (PSF = 50%, 13/26; PSF and TLIF = 42%, 10/24; p = 0.55), additional fixation below S1 (p = 1.0), fusion to the L4 level (p = 0.24), or use of postoperative bracing (bracing = 4/17, 23.5%, none = 16/33, 48.5%, p = 0.09) (Table 7).
Implant failure was associated with preop slip angle (none = 24.0°, failure = 34.1°, p = 0.02) and a spondylolisthesis grade greater than 2 (grades 1–2 = 7.1% failure rate, grades 3–5 = 55% failure rate; p = 0.04). Implant failure and pseudarthrosis were not associated with patient BMI (none = 21.7, failure = 20.9, p = 0.61), type of spondylolisthesis (dysplastic = 30.7%, 8/26; acquired = 30.4%, 7/23; p = 0.98), pre-op % slip (none = 55.7%, failure = 70.9%, p = 0.12), post-op % slip (none = 27.2%, failure = 36.3%, p = 0.12), post-op slip angle (none = 24.9°, failure = 18.3°, p = 0.28) post-op kyphosis of the lumbosacral angle (none = 34.6°, failure = 46.1°, p = 0.48), change in slip angle (none = − 4.1%, fail = − 18.4%; p = 0.40), or change in percent slip (none = − 49.2%, fail = − 49.2%, p = 0.99) (Table 6). Implant failure/pseudarthrosis was not correlated with type of graft used (allograft = 43%, 3/7; autograft = 29%, 10/34, allograft and autograft = 33.3%, 3/9; p = 0.81), addition of a TLIF (PSF = 26.9%, 7/26, PSF and TLIF = 37.5%, 9/24; p = 0.76), additional fixation below S1 (p = 0.41), fusion to the L4 level (p = 0.80), or use of postoperative bracing (bracing = 6/17, 35.3%, none = 10/33, 30.3%, p = 0.72). (Table 7). Additional fixation below S1 was not a significant predictor of implant failure when grade of spondylolisthesis (p = 0.44) or preoperative slip angle (p = 0.15) was taken into account.
All patients had intraoperative neuromonitoring without any demonstrable changes in MEPs. 14% (7/50) of patients had L5 motor weakness postoperatively, though the extent of this varied and in all cases the weakness improved; while there was persistent radicular pain in 3 cases prompting reoperation. 50% (n = 25/50) of patients experienced a radiculopathy with the following symptoms: radiating leg pain (9), numbness (4), weakness (3), or a combination of these symptoms (4). 5 patients were noted to have a radiculopathy but the symptoms were not specified beyond that. In 22 of these patients, the radiculopathy was transient and resolved without intervention. In 3 cases, the radiculopathy was persistent or significantly impacting patient function and they underwent reoperation at a mean of 2.7 weeks after their initial procedure. A higher rate of radiculopathy was not associated with patient BMI (none = 21.9, failure = 20.8, p = 0.41), type of spondylolisthesis (dysplastic = 60.0%, 15/25; acquired = 34.7%, 8/23; p = 0.08), pre-op % slip (none = 53.7%, radiculopathy = 70.3%, p = 0.08), post-op % slip (none = 26.1%, radiculopathy = 34.4%, p = 0.14), post-op kyphosis of the lumbosacral angle (none = 35.3°, radiculopathy = 41.6°, p = 0.67), change in slip angle (none = − 3.1%, radiculopathy = − 21.2%; p = 0.23), or change in percent slip (none = -45.8%, radiculopathy = − 53.4%, p = 0.24) (Table 6). There was a higher rate of postoperative radiculopathy in the patients who underwent attempted reduction, although this did not achieve statistical significance (no reduction: 4/14, 28.6%; reduction: 57.1%; p = 0.166). The addition of a TLIF (PSF = 46%, 12/26; PSF and TLIF = 50%, 12/24; p = 0.89) or postoperative bracing (bracing = 10/17, 58.8%, none = 14/33, 42.4%, p = 0.32) was not correlated with the occurrence of radiculopathy (Table 7). In 22 of these patients, the radiculopathy was transient and resolved without intervention; while in 3 cases, patients underwent reoperation for persistent radiculopathy symptoms.
Discussion
Numerous techniques have been described for the surgical treatment of adolescent spondylolisthesis [2, 7, 9, 16,17,18,19]. In 2015, Shoenleber et al. published a review of current treatment methods for high-grade spondylolisthesis and reported that the preferred operative technique was reduction and decompression with instrumentation and circumferential fusion [1]. Despite this, the choice of operative technique remains controversial. Our objective was to better define the risk factors and complication rates for operative treatment of spondylolisthesis in adolescents by combining data from multiple high-volume spine centers.
The overall reoperation rate for surgical correction of spondylolisthesis in this series was 40% (n = 20/50), much higher than expected and also higher than previously documented. Other studies in the literature report complication rates ranging from 10 to 30% [9,10,11, 13, 18]. In a smaller series of 24 patients, Lundine et al. found a 23% rate of return to the OR, most commonly for painful implants and pseudarthrosis [11]. Both Fu et al. and Kasliwal et al. generated larger series for review by analyzing the SRS morbidity and mortality database. Fu et al. identified 605 spondylolisthesis cases with an overall complication rate of 10.4%, the most common complication being new postoperative neurologic deficits (5.1%) [10]. Kasliwal et al. included only cases of high-grade spondylolisthesis, both adult and pediatric. There was an overall 29.7% short-term complication rate and 17% reoperation rate, not significantly different between adult and pediatric patients [13]. One contributing difference between the Fu and Kasilwal papers and this series may be a longer follow-up, as the mean time to revision was more than 2 years postoperatively and our mean follow-up was over 5 years. Additionally, database studies may be limited by underreporting [10, 13, 20, 21].
This research began as many of the involved centers were independently observing a higher rate of complications than were encountered with other aspects of spine surgery. Nevertheless, everyone was surprised by how high the rate turned out to be in this analysis. In addition to the points previously discussed, one factor that likely contributed is the long-term follow-up with a mean of over 5 years, especially given that many of the complications were encountered years after initial instrumentation. Additionally, the surgeons involved in this series encouraged their patients to resume full activity and sports participation. One could argue that perhaps limiting them to lower impact activities or encouraging them to be less competitive might have strained the implants less and resulted in fewer issues. However, for many of these children, sports were important not only to their quality of life, but also to their future in the form of college scholarships or even their intended profession. Consequently, many of the surgeons involved in this series now obtain limited CT scans at 3–6 months postoperatively to confirm that there is a solid osseous union prior to releasing patients to full activity. One can certainly argue for waiting to perform a CT scan at 6 or 12 months. However, many of these cases are often high-level athletes whose college prospects or general happiness will be limited significantly by postponing the CT further. While we have seen many cases that show solid union at 3 months, this is not universal and the optimal timing and method to evaluate for union prior to return to sport is an area that warrants further investigation. Intuitively, this will decrease the late implant complications encountered in this series though further research is needed to confirm if that is in fact the case.
There are conflicting data regarding the association between complications and the addition of intraoperative reduction. In this study, there was no correlation between return to the OR and the change in slip angle (p = 0.42) or percent slip (p = 0.30), both of which are surrogates for the amount of reduction performed. It should also be noted that, in the series, the mean preoperative and postoperative slip angles were minimally different (27.3° and 23.8°). However, the range was quite large, with postoperative slip angles ranging from 0 to 62. Although the risks and benefits of reduction are often debated, it is possible that the persistent slip angle in some of these cases contributed to construct failure and need for reoperation. Shufflebarger and Geck reported no significant complications or implant failures requiring revision, although they did have 2 patients with “structural complications,” in their series of 18 consecutive patients with high-grade isthmic spondylolisthesis treated via aggressive reduction of the slip with anterior column structural support and posterior compressive instrumentation. In their series, there was a mean reduction in slip angle from 35° to 3.8° [22] Although this was a smaller series, it raises the question as to whether more aggressive reductions may have fared better. However, it is also worth noting that the mean follow-up in our series is considerably longer and that on average implant issues were encountered after 2 years.
In addition, rate of reoperation trended towards significance with addition of postoperative bracing. Those patients who were braced had a 25% lower rate of reoperation versus those who were not braced (bracing = 4/17, 23.5%, none = 16/33, 48.5%, p = 0.09. This suggests that bracing helped to support the deformity correction when it was achieved and/or prevented activity that strained the construct, though the numbers were not large enough to confirm this with only 17 braced patients. Additionally, the protocol, type of bracing, and any additional activity limitations (period of bedrest) may also have been factors, but are difficult to ascertain from a multicenter retrospective series. Additionally, bracing studies for scoliosis have demonstrated highly variable compliance; so, without the use of a bracing compliance monitor it is difficult to truly evaluate how much bracing may or may not have contributed. This is another area ripe for study moving forward as we work towards lowering this shockingly high reoperation rate.
In our series, implant failure correlated significantly with preoperative slip angle (p = 0.02) and with a higher initial grade of spondylolisthesis (p = 0.04), indicating that patients with larger initial deformity were more likely to experience implant complications. Intuitively, we anticipated higher rates of complications with higher-grade slips. However, as low-grade slips can often be treated successfully with conservative management, 72% of the patients in this series were grade 3 or higher, making some of the sub-analysis on this topic challenging. We did not have an overall higher rate of reoperation in the high-grade slips, though this was likely underpowered to detect a small difference. We did see an increase rate of implant failure that was markedly higher with high-grade slips (55%) compared to low-grade slips (7%). On sub-analysis of the high-grade slips, we could not find any variables significantly affecting complication and implant failure rate, again likely due to sample size. We were both surprised by just how high this rate was with high grade slips; however, this also demonstrated, while less common, the low-grade slips are not immune to implant failure either as their rate was still substantial at 7%.
In addition, implant failure trends to significance with postop percent slip, which may indicate that larger residual deformity after reduction impacts the stability of fixation. This has been suggested by other series [23, 24]; however, it has to be balanced against the potential increased neurologic risk encountered with reduction, though this continues to be a topic of debate. This may also explain the lack of difference between patients who received a TLIF and those who did not. There was essentially no difference in kyphosis of the lumbosacral angle between groups, which may have limited the mechanical impact of the additional anterior column support of TLIF. Muschik et al., in a comparison of anterior fusion in situ with anterior fusion and posterior instrumentation with reduction, found that the overall complication rate was higher in the reduced and instrumented group (13% vs 7%) [18]. Additionally, Fu et al. found that the complication rate was almost double, and rates of neurological deficits were 5 times higher in patients who received a reduction versus those who did not. These results may be exaggerated, as patients with more severe spondylolisthesis were more likely to undergo reduction and develop postoperative neurological complications in their series [10]. In contrast, Burkus et al., in a comparison of in situ fusion with in situ fusion and reduction, found a lower complication rate and better maintenance of correction in those patients who received a reduction (16.7% vs 22.2% complication rate) [9].
The 16% of patients who had “sub-S1” fixation had an assortment of pelvic fixation, including more traditional iliac screws, S2AI screws and screws below S1 into the ilium. As the overall number was small, we did not feel that there was an adequate number for a meaningful sub-analysis. Regardless, pelvic fixation in general was surprisingly not associated with a lower implant failure rate. While this may have been underpowered, we did not even observe a notable trend in that direction. It is possible that some of the lack of demonstrable benefit reflects selection bias though this is difficult to conclude in a retrospective study. Additionally, the addition of a TLIF did not appear to have the intended benefit of improving the fusion rate. Some of the patients treated with TLIF had a structural allograft as opposed to more rigid anterior support, though even in the presence of the rigid anterior support complications were still observed. Another potential option is a shortening sacral dome osteotomy which may have been an underutilized option in this series. Currently, many of the authors have gone to a true anterior spinal fusion with a rigid interbody and instrumentation as this provides circumferential support, though additional follow-up is needed to see if this is having the intended effect of lowering the pseudarthrosis rate in these patients.
Another consideration is the extent to which a decompression was performed. Some, but not all, of these patients had nerve root decompressions and/or laminectomies. The extent to which this was performed and the magnitude of bone removed varied considerably and we did not feel could be adequately evaluated retrospectively. We did, however, have several cases where a decompression was not performed that subsequently had implant failure; so, anecdotally, we do not feel that it is the key variable. However, this warrants further investigation.
Strengths of this series include that it utilized data from multiple sites. Additionally, radiographic measures were used for reduction instead of relying on operative notes or surgeon definition. More specifically, the reduction may have an impact on pseudarthrosis rate. In comparison to the literature, Transfeldt et al. found that pseudarthrosis rates appeared to be lower in reduced cases, but with no overall difference in clinical outcomes [16]. Similarly, Muschik et al. found that reduced and instrumented patients had a significantly lower rate of pseudarthrosis than those fused in situ (7% versus 24%) [18]. Our series found no correlation between rates of pseudarthrosis and reduction (change in slip angle: p = 0.40, change in percent slip: p = 0.84), which is consistent with results by Boxall et al., who found approximately equal rates of pseudarthrosis in reduced and non-reduced patients [2].
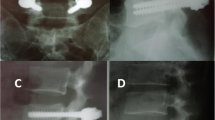
The most common reason for reoperation in this series was implant failure, 55.6% (n = 15/27) (Table 5). Many of these complications were experienced several years postoperatively, following an initially positive result. Not surprisingly, these cases of late implant failure were associated with pseudoarthrosis which contributed to the eventual failure of the implants. An example of implant failure was seen in a 16-year-old female who initially presented with 3 years of low back pain with right sided radicular symptoms. Initial imaging showed an L5/S1 spondylolisthesis with a slip of 50% and slip angle of 16° with evidence of a previously healed fracture (Fig. 1). She underwent L5/S1 PSF using structural allograft and crushed cancellous allograft and Gill procedure (Fig. 2). At 2 weeks postoperatively, her initial pain had resolved; however, she had new onset left-sided radicular pain. Imaging showed no interval change in implant position or nerve root compression. Radicular symptoms began improving and resolved prior to her 6-month postoperative visit without further surgical intervention. She subsequently did well until 32 months postoperatively she presented with recurrence of her LBP and new right-sided radicular symptoms. Radiographs demonstrated bilateral broken S1 screws and an increase in kyphosis of the lumbosacral angle. A CT scan was not done as implant failure could be visualized and pseudarthrosis was presumed to be present. However, an MRI was obtained which showed no concern for nerve root compression. After initially trying to avoid reoperation, she continued to be symptomatic and ultimately moved forward with revision surgery. She underwent reoperation at 36.1 months for removal of instrumentation and reimplantation (Fig. 3) with an ALIF system for the anterior disc replacement (Fig. 3). She was asymptomatic until 15 months postoperatively at which point she began having recurrent LBP; however, the implants remained (Fig. 4) and this seemed more muscular in etiology. She subsequently graduated from high school and moved across the country. We were unable to contact her despite attempts to do so and so were unable to determine if her LBP is currently resolved or not. This case demonstrates both the short-term and long-term complications associated with correction of spondylolisthesis in adolescents. Due to the high rate of complications at many years out from index surgery, it is perhaps advisable to follow these patients for longer than the average pediatric spine patient.

Reproduced with Permission from the Children’s Orthopaedic Center, Los Angeles
Initial preoperative radiographs of a 16-year-old female presenting with low back pain and radicular symptoms. X-rays demonstrate L5/S1 spondylolisthesis. Percent slip was measured as 50%.

Reproduced with Permission from the Children’s Orthopaedic Center, Los Angeles
Initial postoperative radiographs demonstrating L5–S1 posterior spinal fusion with soft bony TLIF and Gill procedure. Patient was asymptomatic postoperatively.

Reproduced with Permission from the Children’s Orthopaedic Center, Los Angeles
At 32 months postoperatively, she presented with recurrence of her LBP and right-sided radicular symptoms. X-rays showed bilateral broken S1 screws and an increase in kyphosis of the lumbosacral angle. She was taken back to the operating room for removal of instrumentation and re-implantation.

Reproduced with Permission from the Children’s Orthopaedic Center, Los Angeles
She was asymptomatic until 15 months postoperatively at which point she began having recurrent LBP; however, the implants remained stable until she transitioned to adult care 31 months postoperatively.
Radiculopathy is another common complication reported in the literature with treatment of spondylolisthesis. Our series had a 44% (n = 22/50) rate of transient radiculopathy and a 6% (n = 3/50) rate of return to the OR for persistent radiculopathy. Rate of radiculopathy was not associated with change in slip angle (p = 0.23) or change in percent slip (p = 0.24). Patient’s with dysplastic type spondylolisthesis had a higher rate of postoperative radiculopathy than patients with acquired type (60.0% vs 34.7%, p = 0.08). This is similar to the rate of neurologic complications found by Bouyer et al. (41.7%) [8] and Schwend et al. (35%) in their series of fused and reduced spondylolisthesis cases. The majority of neurological deficits reported was transient [8, 14]. Other studies show a more moderate rate of neurological deficits. Molinari et al., Lundine et al., and Bourassa-Moreau et al. [3, 7, 11]all reported rates under 20%, although in the series by Molinari et al., 11% of patient required a return to the OR for persistent symptoms [7].
The limitations of this study include those inherent to retrospective chart review. In addition, although our sample size is larger than other reports in the literature outside of those utilizing the SRS database, it still likely underpowered to detect small or subtle differences. The sample size was improved by involving multiple, high-volume spine centers in the study, but the frequency of surgical correction for spondylolisthesis in adolescents is fairly low. Despite a high number of spinal deformity surgeries being performed at each center, there are only a small number of spondylolisthesis cases that require operative management. In adolescents with spondylolysis/spondylolisthesis, the majority of patients can be successfully managed with conservative management (bracing, activity modifications, core strengthening) and in some cases, parents and patients prefer altering their activities rather than choosing operative management. Consequently, these are relatively rare operative procedures. It is possible that with larger numbers some of the trends in this data set may have been significant.
Surgical treatment of adolescent spondylolisthesis was associated with a 40% overall reoperation rate and a 50% rate of radiculopathy in this series. Patients at highest risk for implant complications are those with the largest preoperative slip. Having observed this pattern, many of the surgeons in this study have begun using a more aggressive approach for treatment, combining anterior spinal fusion (ASF) with PSF for management. Initial results are promising, but there are currently not have enough ASF and PSF patients with long-term follow-up to establish whether these patients have a lower complication rate than those treated with PSF with or without TLIF. However, increased correction of deformity, especially in patients with the largest slip angles, may be one method of reducing rates of implant failure. Addition of postoperative bracing may also help to reduce reoperation rates. Those patients who were braced had a 25% lower rate of reoperation, although it was not significant. Until further studies are conducted on the efficacy of bracing in the spondylolisthesis population, the addition of a brace may be left up to surgeon and patient discretion based on risk factors and patient activity level. In addition, the authors recommend thorough preoperative counseling of patients and their parents regarding the high complication rates observed with surgical treatment of this condition.
Key points
-
Posterior surgical treatment of spondylolisthesis in adolescents was associated with a 40% reoperation rate and 50% rate of postoperative radiculopathy at four high-volume spine centers.
-
Reoperation occurred at a mean of 2.1 years postoperatively.
-
Rate of implant failure was correlated with a larger preoperative slip angle.
-
Rate of reoperation and rate of radiculopathy were not improved with addition of a trans-foraminal lumbar interbody fusion.
References
Schoenleber SJ, Shufflebarger HL, Shah SA (2015) The assessment and treatment of high-grade lumbosacral spondylolisthesis and spondyloptosis in children and young adults. JBJS Rev 3(12)
Boxall D et al (1979) Management of severe spondylolisthesis in children and adolescents. J Bone Jt Surg Am 61(4):479–495
Bourassa-Moreau E et al (2013) Quality of life of patients with high-grade spondylolisthesis: minimum 2-year follow-up after surgical and nonsurgical treatments. Spine J 13(7):770–774
Maurice HD, Morley TR (1989) Cauda equina lesions following fusion in situ and decompressive laminectomy for severe spondylolisthesis. Four case reports. Spine (Phila Pa 1976) 14(2):214–216
Schoenecker PL et al (1990) Cauda equina syndrome after in situ arthrodesis for severe spondylolisthesis at the lumbosacral junction. J Bone Jt Surg Am 72(3):369–377
Lykissas MG et al (2014) Paresis of the L5 nerve root after reduction of low-grade lumbosacral dysplastic spondylolisthesis: a case report. J Pediatr Orthop B 23(5):461–466
Molinari RW et al (1999) Complications in the surgical treatment of pediatric high-grade, isthmic dysplastic spondylolisthesis. A comparison of three surgical approaches. Spine (Phila Pa 1976) 24(16):1701–1711
Bouyer B et al (2014) High-grade lumbosacral spondylolisthesis reduction and fusion in children using transsacral rod fixation. Childs Nerv Syst 30(3):505–513
Burkus JK et al (1992) Long-term evaluation of adolescents treated operatively for spondylolisthesis. A comparison of in situ arthrodesis only with in situ arthrodesis and reduction followed by immobilization in a cast. J Bone Jt Surg Am 74(5):693–704
Fu KM et al (2011) Morbidity and mortality in the surgical treatment of six hundred five pediatric patients with isthmic or dysplastic spondylolisthesis. Spine (Phila Pa 1976) 36(4):308–312
Lundine KM et al (2014) Patient outcomes in the operative and nonoperative management of high-grade spondylolisthesis in children. J Pediatr Orthop 34(5):483–489
DeWald RL et al (1981) Severe lumbosacral spondylolisthesis in adolescents and children. Reduction and staged circumferential fusion. J Bone Jt Surg Am 63(4):619–626
Kasliwal MK et al (2012) Short-term complications associated with surgery for high-grade spondylolisthesis in adults and pediatric patients: a report from the scoliosis research society morbidity and mortality database. Neurosurgery 71(1):109–116
Schwend RM et al (1992) Treatment of severe spondylolisthesis in children by reduction and L4–S4 posterior segmental hyperextension fixation. J Pediatr Orthop 12(6):703–711
O'Brien MFK, Blanke KM, Lenke LG (eds) (2008) Spinal deformity study group radiographic measurement manual. Medtronic Sofamor Danek USA, Inc
Transfeldt EE, Mehbod AA (2007) Evidence-based medicine analysis of isthmic spondylolisthesis treatment including reduction versus fusion in situ for high-grade slips. Spine (Phila Pa 1976) 32(19 Suppl):S126–S129
Ilharreborde B et al (2007) Jackson's intrasacral fixation in the management of high-grade isthmic spondylolisthesis. J Pediatr Orthop B 16(1):16–18
Muschik M, Zippel H, Perka C (1997) Surgical management of severe spondylolisthesis in children and adolescents. Anterior fusion in situ versus anterior spondylodesis with posterior transpedicular instrumentation and reduction. Spine (Phila Pa 1976) 22(17):2036–2042 (discussion 2043)
Poussa M et al (1993) Surgical treatment of severe isthmic spondylolisthesis in adolescents. Reduction or fusion in situ. Spine (Phila Pa 1976) 18(7):894–901
Cook JA, Collins GS (2015) The rise of big clinical databases. Br J Surg 102(2):e93–e101
Yoshihara H, Yoneoka D (2014) Understanding the statistics and limitations of large database analyses. Spine (Phila Pa 1976) 39(16):1311–1312
Shufflebarger HL, Geck MJ (2005) High-grade isthmic dysplastic spondylolisthesis: monosegmental surgical treatment. Spine (Phila Pa 1976) 30(6):S42–48
Lonner BS et al (2007) Reduction of high-grade isthmic and dysplastic spondylolisthesis in 5 adolescents. Am J Orthop (Belle Mead NJ) 36(7):367–373
Lenke LG, Bridwell KH (2003) Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 52:525–532
Funding
This study has been carried out with approval from the Institutional Review Board at Children’s Hospital Los Angeles. None of the authors received financial support for this study.
Author information
Authors and Affiliations
Contributions
EN data collection, data analysis, manuscript preparation, final approval of manuscript. LMA study design, manuscript preparation, manuscript review, final approval of manuscript. AS data collection, manuscript preparation, final approval of manuscript. NM data collection, manuscript review, final approval of manuscript. SG study design, manuscript review, final approval of manuscript. MP study design, manuscript review, final approval of manuscript. BKB study design, manuscript review, final approval of manuscript. EF study design, manuscript review, final approval of manuscript. KM study design, manuscript review, final approval of manuscript. BI study design, manuscript review, final approval of manuscript. DLS study design, manuscript review, final approval of manuscript.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nielsen, E., Andras, L.M., Siddiqui, A.A. et al. 40% reoperation rate in adolescents with spondylolisthesis. Spine Deform 8, 1059–1067 (2020). https://doi.org/10.1007/s43390-020-00121-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43390-020-00121-5