
Abstract
The nexus of the ambient air quality and the COVID-19 pandemic is a topic that has attracted much attention and remains of current interest. The study area of Turkey is one of the countries with high case numbers, but there is no detailed investigation dealing with it in the literature. For this reason, the correlation and links between COVID-19 cases and deaths in Turkey with the air pollutants of PM10, PM2.5, SO2, CO, NO2 and O3 were determined between 1 April and 31 July 2021 using the statistical methods of cross-correlation and wavelet coherence analysis. According to the findings, for the COVID-19 pandemic parameters, there were positive significant correlations with PM2.5, SO2, CO, and NO2 and an inverse significant correlation with O3. Although the wavelet transform is not convincing to suggest a standalone coherence, it reveals that air pollution and the spread and mortality of the pandemic in Turkey have short-term periods of co-movement. Additionally, it is notable that the national air quality improved during full lockdown periods in the country. The findings obtained in this study are expected to attract the attention of legislating and enforcing authorities and support more decisive steps being taken to reduce environmental pollutants and to control air pollution.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
The novel Corona Virus Disease 2019 (COVID-19), emerging in Wuhan city in China at the end of 2019 and affecting the whole world in a short duration, was declared a global pandemic by the WHO on 11 March 2020 (BBC 2020). Severe Acute Respiratory Syndrome Corona Virus 2 (SARS-CoV-2) caused the third coronavirus epidemic in the last 20 years after the Severe Acute Respiratory Syndrome (SARS) and the Middle East Respiratory Syndrome (MERS) epidemics caused by coronaviruses in China in 2002 and Saudi Arabia in 2012, respectively (Kuiken et al. 2003; Assiri et al. 2013). Coronaviruses contain nucleic material in single-strand RNA, have 65–125 nm diameter (Shereen et al. 2020) and are spread by human-to-human transmission through direct contact and droplets in the air (Chan et al. 2020; Sohrabi et al. 2020; Wang et al. 2020b). Studies of individuals infected with COVID-19 reported similar clinical symptoms to diseases caused by other coronaviruses, like sore throat, cough, high fever, muscle pain and respiratory failure (Huang et al. 2020; Wang et al. 2020d).
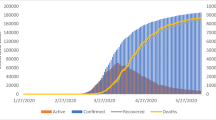
By 25 July 2021, Turkey was in sixth place after USA, India, Brazil, Russia and France with more than five million confirmed cases (WHO 2020). The first COVID-19 case in the country was confirmed by the Turkish Ministry of Health on 10 March 2020 and within only one month, the number of those who lost their lives linked to COVID-19 had passed one thousand (Republic of Turkey Ministry of Health 2021). Faced with this worrying picture, similar to many countries, Turkey implemented a range of restrictions with the aim of controlling the pandemic. Implementations like flexible working hours, distance education, border closures, suspending flights and curfews for certain hours and days targeted minimization of human mobility. Within a short time, social distancing (1–2 m) and mask use were mandatory in public spaces (Coşkun et al. 2021). With the effect on the developing economy, short full lockdown periods were applied encompassing weekends, official and religious holidays when industrial activities were less intense. Due to rapidly rising cases and daily deaths from April 2021 especially, there was a need to take more decisive steps to control the pandemic. With this aim, the longest lockdown in the history of the country, which encompassed the time interval of the research, was implemented with 17 days of full lockdown (29 April–17 May). Figure 1 shows the COVID-19 distribution map according to province for the week of 10–16 April 2021 when cases in Turkey rapidly increased. The Marmara region in the northwest of the country, which includes Istanbul with highest cases recorded on the map, is the region with most development in terms of industry and highest population density in the country (Şahin 2020b). With the relative reduction in daily case numbers in the following period, and the effect of being a tourism destination, many restrictions were eased and gradual normalization began from 1 July.

Overview of COVID-19 cases between 10 and 16 April in Turkey
The authorities forced changes in routine living habits by implementing severe restrictions for the majority of the world’s population and left deep impacts on health, environment, climate tourism and many industrial and socioeconomic areas (Bashir et al. 2020a; Habib et al. 2021; Goodell and Goutte 2021). To date, the pandemic has caused human deaths, disruption of health services and economic losses with costs of billions of dollars and effects are predicted to last until 2023–2024. The clear effects of the pandemic in every area has made it an emergency agenda topic for most researchers (Iqbal et al. 2020; Forni and Mantovani 2021; Kim et al. 2021). In Turkey, the closure of workplaces and factories will affect the blue collar and service sectors especially, and the already high unemployment rate (13.7%) is expected to rise (Açikgöz and Günay 2020). Additionally, one of the most important sources of income for the country of tourism is estimated to lose 34.5 billion dollars in economic damage with the loss of 50 million visitors (Ali et al. 2021). Contrary to this, perhaps the only positive change in this period when industrial activities, transport density and human activity were minimized was experienced in environmental terms as reported in several studies. During lockdown periods, the air quality in most countries was stated to improve by up to 30% (Girdhar et al. 2021). The main indicator for atmospheric particulate matter of aerosol optical depth (AOD) reduced by up to 50% (Srivastava 2020). Ozone concentrations at ground level generally increased. In one of the world’s most crowded places of Manhattan, New York, air quality improved by over 55% compared to 2018 (Shehzad et al. 2021). Research encompassing all provinces in Turkey revealed that PM10 and SO2 amounts reduced by 67% and 59%, respectively, compared to five-year historical records (Orak and Ozdemir 2021). Another study compared with averages for the previous year and found this rate was about 52% for both pollutants (Sari and Esen 2021). Another research including 20 regions of the country measured a 34.5% reduction in PM2.5 and 50% increase in O3 amounts (Aydın et al. 2021). However, the same study reported no clear changes in waste water properties like flow, chemical oxygen demand and suspended solid matter. In short, the pandemic period in Turkey can be said to have positively affected air pollutants, especially, similar to global findings (Ghasempour et al. 2021).
The spread of COVID-19 may be affected by many factors like climate conditions, environmental pollution and demographic structure (Zhang et al. 2020; Bilal et al. 2021). Coşkun et al. (2021) proposed that wind and population density in Turkey had large effects on case numbers. Additionally, considering there is human-to-human transmission in the air through droplets formed when coughing, sneezing and speaking, it is necessary to better understand the role played by air quality in the spread and mortality of the infection (Girdhar et al. 2021). Studies investigated some regions with high air pollution reported air quality has a significant effect on COVID-19 (Setti et al. 2020). The findings show that infected individuals exposed to poor ambient air quality have more severe symptoms and increased hospitalization and mortality risk. The type, amount and exposure duration for air pollutants were stated to play significant roles in the pandemic (Srivastava 2020). Wu et al. (2020) investigated the effects of fine particulate matter on COVID-19 in the USA and concluded that for every 1 µg/m3 increase in PM2.5 emissions, there may be up to 10% increase in mortality rate. Highly polluted areas with fine particulate matter have been shown to increase the spread of infection, suggesting that direct microbial pathogenic transmission is airborne (Setti et al. 2020; Travaglio et al. 2021). Air pollution has been suggested to contribute to the severity of COVID-19, either directly by reducing the lungs’ immunity to infection or indirectly by exacerbating underlying respiratory or cardiovascular diseases (Brandt et al. 2020; Conticini et al. 2020). Along with aerosols, other gas pollutants at high levels may lead to an increase in hospital admissions and crowding of intensive care services by exacerbating respiratory tract symptoms (Conticini et al. 2020; De Weerdt et al. 2020). Ambient air pollution may cause many diseases or increase the effects of disease leading to serious medical care requirements and hence are known to put pressure on national health systems (Ghozikali et al. 2016).
The Turkish Environment Problems and Priorities Assessment report published by the Ministry of Environment and Urbanization in Turkey in 2020 observed air pollution was the top priority environmental problem in 27 provinces (The Ministry of Environment and Urbanization 2020). While the most important source of air pollution in the country was domestic heating, this was followed by mining operations, road traffic, manufacturing industry operations, thermal power stations, other industrial activities and stubble fires. Provinces where the primary source of air pollution was industry are densely located in the Marmara, central Aegean and western Black Sea regions. In 98% of 51 provinces where healthy measurements could be taken in 2019, limit values determined by the WHO were exceeded (Right to Clean Air Platform 2020). If air pollution had been reduced below limit values in this period, it was predicted that about 8% of total deaths in the country could be prevented. A study in Istanbul, where deaths linked to air pollution are observed most, revealed that poor air quality had greatest effect on individuals over 65 years of age (Çapraz et al. 2017). Air pollutants have been found to be associated with higher mortality in hospitalized patients and community-dwellers and have different effects on severe acute respiratory, cardiovascular, and cerebrovascular diseases (Lee et al. 2007; Simoni et al. 2015). Regarding the age of individuals affected by outdoor air pollution, especially the respiratory system, elderly people are one of the most vulnerable groups (Kotaki et al. 2019; Domingo and Rovira 2020). This situation makes the elderly, a target in the pandemic, even more vulnerable to COVID-19. Another study including provinces with highest population density in the country found significant positive correlations between the current pandemic and air pollutants (Şahin 2020a).
In the literature, there is a lack of adequate research revealing the effects of air pollution on the pandemic in Turkey, one of the countries with highest case numbers. This situation comprises the most important source of motivation for the present study. The study focuses on the interaction between the spread and mortality of COVID-19 with air quality indicators and targets determination of the directions of probable connections and periods. Additionally, the effects of short-term exposure to air pollution on the pandemic was determined by investigating the lead and lag relationships between the pandemic and PM10, PM2.5, SO2, CO, NO2 and O3 air pollutants. Additionally, changes in the air quality of the country during the full lockdown period were researched. It is hoped that the outcomes obtained in this research will guide precautions by encouraging the authorities to take stronger steps about improving air quality.
2 Data and Methodology
2.1 Data and Study Area
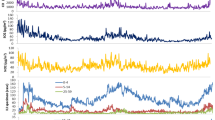
The study included daily confirmed COVID-19 cases and daily deaths for 1 April 2021 to 31 July 2021 from the Republic of Turkey Ministry of Health (https://covid19.saglik.gov.tr/). Hourly and daily values for particulate matter with diameter less than 10 µm (PM10) and 2.5 µm (PM2.5), sulfur dioxide (SO2), carbon monoxide (CO), nitrogen dioxide (NO2) and ozone (O3) were obtained from 224 air quality monitoring stations around the country included in the Republic of Turkey Ministry of Environment and Urbanization National Air Quality Monitoring Network (https://www.havaizleme.gov.tr/). During the time interval, no data could be provided by stations in Uşak and Mersin provinces. Apart from these two provinces, data collected from 79 provinces represented more than 97% of the country’s population (http://www.tuik.gov.tr). The atmospheric air pollutant daily values were calculated with population-weighed mean. The time series of pandemic and air pollutant parameters between 1 April 2021 and 31 July 2021 are given in Fig. 2. The vertical axis on the graph has units of person for COVID-19 data and µg/m3 is the unit for air pollutants. The horizontal axis shows the 4-month time interval for the study.

COVID-19 and air pollution time series in Turkey
2.2 Methodology
In this study, correlation analysis and wavelet transform coherence analytical methods were used to investigate the relationships between the COVID-19 pandemic and air pollution. The fit of data to normal distribution was determined with the Jarque–Bera test used for time series (Aladağ 2021). To investigate the correlation between variables without normal distribution, the non-parametric Kendall and Spearman rank correlation tests were used. Additionally, the cross-correlation function (CCF) was used to determine the lead and lag relationships between air pollutants and the COVID-19 pandemic.
The wavelet transform coherence (WTC) based on the wavelet analytical approach is commonly used in many areas like geophysics, meteorology, environment, climate and finance (Grinsted et al. 2004; Bashir et al. 2020a; Habib et al. 2021; Iqbal et al. 2020; Goodell and Goutte 2021). This method can reveal irregular correlations between two time series by allowing the possibility of identifying common movements in both time and frequency fields. This statistical tool allowing flexible use in unstable time series is very effective to investigate non-linear correlations. Additionally, the power and direction of the correlation and differences between short-, moderate- and long-term correlations can be determined. Wavelet coherence can be simply defined by the following equation.
where S is the smoothing operator, and Wx and Wy represent the wavelet transformation for x(t) and y(t) time series, respectively. 0 ≤ R2 (k, p) ≤ 1, in other words the wavelet coherence value, is between 0 and 1; here 0 indicates no coherence and 1 indicates perfect coherence between variables. The Monte Carlo simulation method is used to determine the statistical significance of the results.
The phase difference ɸ between x(t) and y(t) time series can be written as follows.
where \(\mathfrak{I}\left({W}_{xy}\right)\) and \(\mathfrak{R}\left({W}_{xy}\right)\) represent the imaginary and reel sections of the wavelet transform, respectively. The phase difference indicated by an arrow on wavelet coherence graphs shows the lead/lag phase relationship and positive or inverse correlation between two time series. Zero phase difference means that the investigated time series act together on a certain frequency. When there is a two series phase, a right arrow ( →) is used to represent movement in the same direction, while a left arrow ( ←) shows out-of-phase, or inverse, movement. Arrows pointing upward (↑) mean the first time series leads the second by 90°, while arrows pointing downward (↓) show the second time series leads the first by 90°.
3 Results and Discussion
Descriptive statistics for all observed data are included on Table 1. According to the results, mean 19,753 people caught the disease daily and a total of 19,795 people died linked to COVID-19 during the time interval of the study. Within this period, the highest daily confirmed cases in Turkey reached 63,082 cases on 16 April 2021, with highest mortality for 394 people on 30 April 2021. Mean PM10, PM2.5, SO2, CO, NO2 and O3 were calculated as 38.31, 15.54, 11.80, 882.19, 29.47 and 52.38 µg/m3, respectively. Additionally, according to the Jarque–Bera test, apart from NO2 and O3, other datasets did not have normal distribution. For the period from 29 April–17 May when the strictest lockdown precautions were applied, a clear fall was experienced in air pollution indicators, as seen in Fig. 2. In this period, the PM10, PM2.5, SO2, CO and NO2 concentrations reduced by 6%, 15%, 14%, 27% and 11% rates, while the O3 amount increased by nearly 12% compared to the mean for the previous 17-day period. The results overlap with findings from other studies investigating air pollution in Turkey during the pandemic (Ali et al. 2021; Orak and Ozdemir 2021; Sari and Esen 2021).
The results for Spearman and Kendall correlation tests used to investigate the relationship between air pollutants and COVID-19 in Turkey are presented in Table 2. According to both correlation tests, for confirmed cases and mortality, there were positive correlations with PM2.5, SO2, CO and NO2 and a negative correlation with O3. The variation in air pollution appeared to have a more significant correlation with those infected with the disease rather than reported deaths. Positive correlation coefficients were obtained between COVID-19 and air pollutants in the order SO2 > CO > PM2.5 > NO2 > PM10. However, no significant correlation was encountered between PM10 and any dataset related to the pandemic (p > 0.1). Additionally, Spearman correlation coefficients were higher and had more significance compared to Kendal coefficients. Findings are similar to studies researching crowded cities like New York and those in California in the USA (Bashir et al. 2020c, b).
Figures 3 and 4 show the CCF results between daily COVID-19 cases and deaths with air pollution indicators. Here, positive lag [1; 14] indicates the COVID pandemic is ahead, while negative lag [− 1; − 14] indicates air pollutants are ahead and lag [0] indicates both time series have no lag. For daily cases and PM10, PM2.5, SO2, CO, NO2 and O3, the highest values were obtained on the 11th day (0.316), day 0 (0.483), -7th day (0.751), -7th day (0.624), day 0 (0.331) and day 0 (− 0.621), respectively. Additionally, as seen in the correlogram in Fig. 3, there was increasing CCF trend with PM2.5, SO2 and CO ahead and PM10, NO2 and O3 behind. When the CCF values between daily mortality and air pollutants in Fig. 4 are examined, all air pollutants were ahead of COVID-19 with an increasing profile dominant. The highest CCF values were calculated for PM10, PM2.5, SO2, CO, NO2 and O3 on the 2nd day (0.295), − 14th day (0.42), − 14th day (0.715), − 14th day (0.596), − 2nd day (0.331) and − 2nd day (− 0.689). In other words, the variation in PM2.5, SO2, CO, NO2 and O3, especially, has more significant effects in the progressive periods of the pandemic. Research investigating the effect of meteorological factors revealed evidence that air pressure, wind speed and precipitation in India had a delaying effect on the spread of the pandemic, similar to air pollution (Kulkarni et al. 2021).

Cross-correlation factors of confirmed cases with air pollutants. All cross-correlograms were assessed for lags of − 14 to 14 days

Cross-correlation factors of daily deaths with air pollutants. All cross-correlograms were assessed for lags of − 14 to 14 days
The graphical presentation of the wavelet transform coherence analysis for COVID-19 with air pollutants is given in Figs. 5 and 6. The horizontal axis represents time, while the vertical axis represents periods on the scale of days. The cone of influence showing the region remaining at 5% significance level is separated by a fine black line. Areas with consistency within this region are surrounded by thick black contours and are filled with a blue-red color gradient indicating higher correlations toward red. The color correlation scale is given on the right side of each graph. The small arrows inside circles represent the direction of the correlation between COVID-19 and air pollutants.

Wavelet transform coherence (WTC) between new confirmed cases and air pollutants

Wavelet transform coherence (WTC) between daily deaths and air pollutants
Figure 5 shows the WTC graphs between confirmed daily case and PM10, PM2.5, SO2, CO, NO2 and O3. Four correlation circles appear for PM10. The first is in the 0–4 frequency band at the end of May beginning of June. The left-up arrows dominating this region indicated a lead non-phase correlation for PM10 according to daily cases (R2 > 0.8). The second is in the 4–8 frequency band at the end of June and the other two are in the 8–16 frequency interval in May and July, respectively. For PM2.5, there were three correlation circles in the 0–4, 4–8 and 8016 frequency domains. The left-up arrows in the islet at the end of May indicates a direct negative and high correlation between PM10 and daily cases. The right-up and left-down arrows in other areas show in-phase and out-of-phase correlations leading daily cases. For the SO2 graph, the 0–4 frequency band had two regions in May and July, respectively. The dominant left arrows in these regions indicate negative correlations. For CO there are three coherence regions with two in the 0–4 band and the other in the 4–8 frequency band. Here, the left and up arrows show CO leads and has non-phase correlation. The NO2 graph has six islets surrounded by thick contours. The left and up arrows in the 0–4 frequency band in May show NO2 had a negative correlation leading COVID-19 cases. The right arrows in the other regions indicate in-phase correlation and the down arrows represent NO2 leading, while the up arrow indicates daily cases leading. For O3, there are five large and small correlation islets. Here, there are correlation regions for the 0–4 frequency band in May, June and July, for the 4–8 frequency band in June and the 8–16 frequency band in April. The left arrows indicate non-phase correlations and left-down arrows show daily cases were leading.
Figure 6 shows the wavelet coherence graphs between daily mortality and air pollutants. Three high-correlation regions are notable for PM10. For the frequency domains of 0–4, 4–8 and 8–16 the right arrows for the regions during April and May indicate high positive correlations (R2 > 0.9). For the region from the end of April beginning of May in the 4–8 frequency band, the left-up arrows show out-of-phase extending from PM10 to daily deaths. The 0–4 and 4–8 frequency domains remaining within the cone of influence for PM2.5 contain five coherence regions. The dominant left arrows in these regions indicate negative correlations. Similarly, for SO2, there are several correlation islets in the 0–4 and 4–8 frequency bands and in different time intervals. Here the left-up and right-down arrows show the lead of daily deaths. For all time intervals on the CO graph, 0–4, 4–8 and 8–16 frequency bands have five coherence areas. The dominant left-down arrows for the region at the end of April encompassing the 4–8 and 8–16 frequency bands indicate daily deaths lead compared to CO. The small islet in May for the 8–16 frequency band shows CO leads and has positive correlation. There are islets in the 0–4 and 4–8 frequency interval for NO2. There is a mutual relationship for regions in both frequency areas in May. In July, an out-of-phase relationship is present. Additionally, for the frequency area above 16, there are down and left arrows showing positive correlation with NO2 leading for the region in May. Finally, the O3 graph appears to have many scattered islets in a broad time interval in the 0–4, 4–8 and 8–16 frequency intervals. The right arrows showing in-phase correlation are dominant in the 0–4 frequency band. The down arrows in the 4–8 and 8–16 frequency domains indicate O3 leads compared to deaths.
Results for wavelet coherence reveal that PM2.5 and NO2 are the main determinants for daily confirmed cases. PM2.5 has short-term effects and NO2 has short-medium-term effects on the spread of COVID-19. The other pollutants have effects in narrower time intervals. Between daily mortality and all air pollutants, links with high correlation were identified in different periods. While the effects of PM10 and O3 spread over a larger period, PM2.5, SO2, CO and NO2 have short- and medium-term effects on mortality.
Research investigating the short- and medium-term effects of atmospheric particulate matter on COVID-19 reported the highest mortality risk (relative risk: 1.23, 95% CI) was exposure to aerosols in the outdoors on the 14th day (Wang et al. 2020a). Martelletti and Martelletti (2020) reported a significant correlation between high concentrations of atmospheric aerosols (PM10 and PM2.5) with high transmission and mortality rates for northern regions of Italy most affected by COVID-19. Several studies revealed that particulate matter amounts play a key role in the spread of COVID-19 (Bashir et al. 2020a; Yao et al. 2020). Additionally, Zhao et al. (2019) reported that PM10 contained higher levels of avian influenza virus compared to PM2.5, but that PM2.5 spread more in air. According to a study encompassing 120 major cities in China, PM2.5 is more effective than PM10 on new COVID-19 cases (Zhu et al. 2020). The present study obtained findings showing PM2.5 had more effect compared to PM10.
Bashir et al. (2020b) found a significant correlation between PM10, PM2.5, SO2, NO2 and CO levels in California with the COVID-19 pandemic. A study applying the generalized additive model by Zhu et al. (2020) proposed that a 1 mg/m3 increase in CO caused a 15% increase in daily confirmed cases. Research including 10 provinces in Turkey found significant correlations between major air pollutants and the pandemic and the highest positive correlation was obtained for SO2 (Şahin 2020a). For people dying due to COVID-19 in Milan, Italy, Zoran et al. (2020) found a negative correlation with NO2 and a positive significant correlation with ground ozone levels. Additionally, they mentioned the significant negative effects on human immunity and respiratory systems of air pollutants, which are probable carriers of viral infections. According to Ogen (2020), long-term exposure to NO2 has severe effects on the mortality of COVID-19. Research investigating the effects of air pollutants on COVID-19 in Germany proposed that PM2.5, NO2 and O3 were the main determinants of the pandemic (Bashir et al. 2020a). In South America, PM10, NO2, CO and O3 were included among the most important pollutant parameters that need to be controlled in the struggle against the pandemic (Bilal et al. 2021). A study in Dhaka city revealed O3 was the essential pollutant determining the spread of the pandemic (Rahman et al. 2021).
According to empirical findings, high levels of air pollution can be said to contribute to the spread and mortal effects of COVID-19 by notable amounts. Many studies confirm that air quality has key importance in reducing the effects of the pandemic (Lolli et al. 2020; Xu et al. 2020; Zhang et al. 2020). When assessed from this aspect, it is considered greatly important that in addition to limiting human interactions, the authorities take sustainable environmental precautions about developing air quality.
4 Conclusions
This research presents the co-movement of the pandemic by determining nexus in time–frequency space for the correlation between the spread and mortality of COVID-19 with six main components of air pollution. This study, focusing on Turkey one of the country’s most affected by COVID-19 included daily cases and deaths along with daily data about PM10, PM2.5, SO2, CO, NO2 and O3 air pollutants collected from 79 provinces. Empirical findings reveal positive correlations for PM2.5, SO2, CO and NO2 and a negative correlation for O3. There was no lag between daily cases and PM2.5, NO2 and O3, while an increasing correlation with 7-day lag was present for SO2 and CO. A correlation increasing to 14 days was present between lives lost due to the pandemic and PM2.5, SO2 and CO. For PM10, NO2 and O3, the highest correlation values were obtained for a 2-day lag. Aerosols have a more rapidly increasing correlation trend compared to pollutants in gas form. Short-term exposure to air pollutants affects the spread of the pandemic. Additionally, according to wavelet coherence results, all pollutants were identified to have co-movement and correlations within certain periods. Air pollutant levels may be said to have certain short- and medium-term effects on COVID-19. However, though wavelet coherence is a new and effective approach to determine pandemic vectors, it is not sufficient to mention the direction and causality of the correlation. In order to provide validity for the findings obtained limited to Turkey, there is a need for evidence from larger regions using different methods.
At the same time, the author wishes to draw attention to the improvement in air quality in Turkey during the longest full lockdown period. Precautions limiting human activities to minimize transmission of the pandemic provide short-term positive contribution to air pollution. This study, similar to previous ones, revealed national air pollution is linked to anthropogenic factors (Wang et al. 2020c; Gautam et al. 2021; Mor et al. 2021). Perhaps the only promising aspect of this global pandemic with deep social effects is that it shows that environmental pollution is preventable. Promising findings for national air quality in the lockdown period are expected attract greater attention from regulators of environmental laws that affect public health. It is recommended that national and local governments enact more effective environmental policies to reduce and control air pollution, determined to be an important factor in the struggle with the COVID-19 pandemic, where certain age groups and those with chronic disease are more vulnerable. The study predicts that providing more developed ambient air quality in Turkey will prevent much loss of life.
Data Availability
Not applicable.
References
Açikgöz Ö, Günay A (2020) The early impact of the Covid-19 pandemic on the global and Turkish economy. Turkish J Med Sci 50:520–526
Aladağ E (2021) Forecasting of particulate matter with a hybrid ARIMA model based on wavelet transformation and seasonal adjustment. Urban Clim 39:100930
Ali H, Yilmaz G, Fareed Z et al (2021) Impact of novel coronavirus (COVID-19) on daily routines and air environment: evidence from Turkey. Air Qual Atmos Heal 14:381–387
Assiri A, McGeer A, Perl TM et al (2013) Hospital outbreak of Middle East respiratory syndrome coronavirus. N Engl J Med 369:407–416
Aydın S, Nakiyingi BA, Esmen C et al (2021) Environmental impact of coronavirus (COVID-19) from Turkish perceptive. Environ Dev Sustain 23:7573–7580
Bashir MF, Benghoul M, Numan U et al (2020a) Environmental pollution and COVID-19 outbreak: insights from Germany. Air Qual Atmos Heal 13:1385–1394
Bashir MF, Jiang B, Komal B et al (2020b) Correlation between environmental pollution indicators and COVID-19 pandemic: a brief study in Californian context. Environ Res 187:109652
Bashir MF, Ma B, Komal B et al (2020c) Correlation between climate indicators and COVID-19 pandemic in New York, USA. Sci Total Environ 728:138835
BBC (2020) Coronavirus confirmed as pandemic by World Health Organization - BBC News. https://www.bbc.com/news/world-51839944. Accessed 20 Mar 2021.
Bilal MFB, Komal B, Benghoul M et al (2021) Nexus between the COVID-19 dynamics and environmental pollution indicators in South America. Risk Manag Healthc Policy 14:67
Brandt EB, Beck AF, Mersha TB (2020) Air pollution, racial disparities, and COVID-19 mortality. J Allergy Clin Immunol 146:61–63
Çapraz Ö, Deniz A, Doğan N (2017) Effects of air pollution on respiratory hospital admissions in İstanbul, Turkey, 2013 to 2015. Chemosphere 181:544–550
Chan JF-W, Yuan S, Kok K-H et al (2020) A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet 395:514–523
Conticini E, Frediani B, Caro D (2020) Can atmospheric pollution be considered a co-factor in extremely high level of SARS-CoV-2 lethality in Northern Italy? Environ Pollut 261:114465
Coşkun H, Yıldırım N, Gündüz S (2021) The spread of COVID-19 virus through population density and wind in Turkey cities. Sci Total Environ 751:141663
De Weerdt A, Janssen BG, Cox B, Bijnens EM, Vanpoucke C, Lefebvre W, El Salawi O, Jans M, Verbrugghe W, Nawrot TS, Jorens PG (2020) Pre-admission air pollution exposure prolongs the duration of ventilation in intensive care patients. Intensive Care Med 46:1204–1212
Domingo JL, Rovira J (2020) Effects of air pollutants on the transmission and severity of respiratory viral infections. Environ Res 187:109650
Forni G, Mantovani A (2021) COVID-19 vaccines: where we stand and challenges ahead. Cell Death Differ 28:626–639
Gautam AS, Dilwaliya NK, Srivastava A et al (2021) Temporary reduction in air pollution due to anthropogenic activity switch-off during COVID-19 lockdown in northern parts of India. Environ Dev Sustain 23:8774–8797
Ghasempour F, Sekertekin A, Kutoglu SH (2021) Google Earth Engine based spatio-temporal analysis of air pollutants before and during the first wave COVID-19 outbreak over Turkey via remote sensing. J Clean Prod 319:128599
Ghozikali MG, Heibati B, Naddafi K et al (2016) Evaluation of chronic obstructive pulmonary disease (COPD) attributed to atmospheric O3, NO2, and SO2 using Air Q Model (2011–2012 year). Environ Res 144:99–105
Girdhar A, Kapur H, Kumar V, Kaur M, Singh D, Damasevicius R (2021) Effect of COVID-19 outbreak on urban health and environment. Air Qual Atmos Health 14:389–397
Goodell JW, Goutte S (2021) Co-movement of COVID-19 and Bitcoin: evidence from wavelet coherence analysis. Financ Res Lett 38:101625
Grinsted A, Moore JC, Jevrejeva S (2004) Application of the cross wavelet transform and wavelet coherence to geophysical time series. Nonlinear Process Geophys 11:561–566
Habib Y, Xia E, Fareed Z, Hashmi SH (2021) Time–frequency co-movement between COVID-19, crude oil prices, and atmospheric CO2 emissions: fresh global insights from partial and multiple coherence approach. Environ Dev Sustain 23:9397–9417
Huang C, Wang Y, Li X et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395:497–506
Iqbal N, Fareed Z, Shahzad F et al (2020) The nexus between COVID-19, temperature and exchange rate in Wuhan city: new findings from partial and multiple wavelet coherence. Sci Total Environ 729:138916
Kim JH, Marks F, Clemens JD (2021) Looking beyond COVID-19 vaccine phase 3 trials. Nat Med 27(2):205–211
Kotaki K, Ikeda H, Fukuda T, Yuhei K, Yuki F, Kawasaki M, Wakamatsu K, Sugahara K (2019) Trends in the prevalence of COPD in elderly individuals in an air-polluted city in Japan: a cross-sectional study. Int J Chron Obstruct Pulmon Dis 14:791–798
Kuiken T, Fouchier RAM, Schutten M et al (2003) Newly discovered coronavirus as the primary cause of severe acute respiratory syndrome. Lancet 362:263–270
Kulkarni H, Khandait H, Narlawar UW et al (2021) Independent association of meteorological characteristics with initial spread of Covid-19 in India. Sci Total Environ 764:142801
Lee J-T, Son J-Y, Cho Y-S (2007) The adverse effects of fine particle air pollution on respiratory function in the elderly. Sci Total Environ 385:28–36
Lolli S, Chen Y-C, Wang S-H, Vivone G (2020) Impact of meteorological conditions and air pollution on COVID-19 pandemic transmission in Italy. Sci Rep 10:1–15
Martelletti L, Martelletti P (2020) Air pollution and the novel Covid-19 disease: a putative disease risk factor. SN Compr Clin Med 2:383–387
Mor S, Kumar S, Singh T et al (2021) Impact of COVID-19 lockdown on air quality in Chandigarh, India: understanding the emission sources during controlled anthropogenic activities. Chemosphere 263:127978
Ogen Y (2020) Assessing nitrogen dioxide (NO2) levels as a contributing factor to coronavirus (COVID-19) fatality. Sci Total Environ 726:138605
Orak NH, Ozdemir O (2021) The impacts of COVID-19 lockdown on PM10 and SO2 concentrations and association with human mobility across Turkey. Environ Res 197:111018
Rahman MS, Azad MAK, Hasanuzzaman M et al (2021) How air quality and COVID-19 transmission change under different lockdown scenarios? A case from Dhaka city. Bangladesh Sci Total Environ 762:143161
Republic of Turkey Ministry of Health (2021) Republic of Turkey Ministry of Health - COVID-19 Information Page. https://covid19.saglik.gov.tr/. Accessed 29 June 2021.
Right to Clean Air Platform (2020) Dark report 2020: air pollution and health impacts. İstanbul
Şahin M (2020a) The association between air quality parameters and COVID-19 in Turkey. Pharm Biomed Res 6:49–58
Şahin ÜA (2020b) The effects of COVID-19 measures on air pollutant concentrations at urban and traffic sites in Istanbul. Aerosol Air Qual Res 20:1874–1885
Sari MF, Esen F (2021) Effect of COVID-19 on PM10 and SO2 concentrations in Turkey. Environ Forens 23:445
Setti L, Passarini F, De Gennaro G et al (2020) SARS-Cov-2RNA found on particulate matter of Bergamo in Northern Italy: first evidence. Environ Res 188:109754
Shehzad K, Bilgili F, Koçak E et al (2021) COVID-19 outbreak, lockdown, and air quality: fresh insights from New York City. Environ Sci Pollut Res. https://doi.org/10.1007/s11356-021-13556-8
Shereen MA, Khan S, Kazmi A et al (2020) COVID-19 infection: origin, transmission, and characteristics of human coronaviruses. J Adv Res 24:91
Simoni M, Baldacci S, Maio S et al (2015) Adverse effects of outdoor pollution in the elderly. J Thorac Dis 7:34
Sohrabi C, Alsafi Z, O’neill N et al (2020) World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg 76:71–76
Srivastava A (2020) COVID-19 and air pollution and meteorology-an intricate relationship: a review. Chemosphere 263:128297
The Ministry of Environment and Urbanization (2020) Inventory of environmental problems and priorities assessment report of Turkey. Ankara
Travaglio M, Yu Y, Popovic R et al (2021) Links between air pollution and COVID-19 in England. Environ Pollut 268:115859
Wang B, Liu J, Li Y et al (2020a) Airborne particulate matter, population mobility and COVID-19: a multi-city study in China. BMC Public Health 20:1–10
Wang C, Horby PW, Hayden FG, Gao GF (2020b) A novel coronavirus outbreak of global health concern. Lancet 395:470–473
Wang P, Chen K, Zhu S et al (2020c) Severe air pollution events not avoided by reduced anthropogenic activities during COVID-19 outbreak. Resour Conserv Recycl 158:104814
Wang Y, Wang Y, Chen Y, Qin Q (2020d) Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J Med Virol 92:568–576
WHO (2020) WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int/. Accessed 25 June 2021.
Wu X, Nethery RC, Sabath BM, Braun D, Dominici F (2020) Air pollution and COVID-19 mortality in the United States: strengths and limitations of an ecological regression analysis. Sci Adv 6(45):eabd4049
Xu H, Yan C, Fu Q et al (2020) Possible environmental effects on the spread of COVID-19 in China. Sci Total Environ 731:139211
Yao Y, Pan J, Liu Z et al (2020) Temporal association between particulate matter pollution and case fatality rate of COVID-19 in Wuhan. Environ Res 189:109941
Zhang Z, Xue T, Jin X (2020) Effects of meteorological conditions and air pollution on COVID-19 transmission: evidence from 219 Chinese cities. Sci Total Environ 741:140244
Zhao Y, Richardson B, Takle E et al (2019) Airborne transmission may have played a role in the spread of 2015 highly pathogenic avian influenza outbreaks in the United States. Sci Rep 9:1–10
Zhu Y, Xie J, Huang F, Cao L (2020) Association between short-term exposure to air pollution and COVID-19 infection: evidence from China. Sci Total Environ 727:138704
Zoran MA, Savastru RS, Savastru DM, Tautan MN (2020) Assessing the relationship between ground levels of ozone (O3) and nitrogen dioxide (NO2) with coronavirus (COVID-19) in Milan. Italy Sci Total Environ 740:140005
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
EA: conceptualization, visualization, investigation, editing, validation, writing—original draft.
Corresponding author
Ethics declarations
Conflict of interest
Not applicable.
Ethical Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Aladag, E. The Nexus Between Air Pollution and the COVID-19 Pandemic in Turkey: Further Insights from Wavelet Coherence Analysis. Aerosol Sci Eng 8, 108–119 (2024). https://doi.org/10.1007/s41810-023-00209-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41810-023-00209-1