
Abstract
To achieve accreditation standards and train residents for clinical practice, ACGME placed a lot of emphasis on ethical competence and professionalism. A crucial requirement for enhancing the standard of future medical practice is ethics education. This study sought to identify the requirement for ethics knowledge in clinical training from the perspective of the residents and determine the most effective methods for education. A cross-sectional descriptive study was conducted between March and May 2023. Participants included Lebanese postgraduate medical students, 210 completed a Google Forms survey via WhatsApp. A validated questionnaire adapted from a previous study was used, focusing on demographics, ethical experience, attitudes, educational goals, and training effectiveness. Analyses were performed on IBM SPSS Statistics software (version 26.0) and R software. 210 residents representing a range of specialties participated in the survey. predominantly in internal medicine (54.8%). Residents strongly affirmed the importance of professionalism and ethics education. Participants overwhelmingly agreed that it should improve patient care and clinical decision-making (p < 0.05). The best way to learn is also through clinical rounds, which feature peer discussion groups facilitated by experienced physicians (p < 0.001). Topics identified as needing more attention were obtaining informed consent and discussing treatment risks(p < 0.05). In order to develop the best teaching strategies for the trainees and produce the most competent doctors possible in the future, this study shed light on the ethical weak points in the clinical training of residents. and lay the groundwork for establishing an ethical curriculum to direct future medical practice.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Without an ethical foundation, it is no longer feasible to practice medicine purely on the basis of medical knowledge and clinical reasoning. (Milestones et al. 2014). In the Hippocratic Oath, which was written centuries ago, the relationship between medical practice and ethics was addressed. (Emery 2013). Every time the doctor puts on a white coat, he must keep in mind the vows that he has made to himself, his profession, and society as a member of a respectable “profession.“(Arawi 2010).
The Lebanese Code of Medical Ethics was first written in 1994 and recently amended in 2004 when the Rights of Patients and Informed Consent article was introduced. Still, the changes that have been made are not enough and some are still vague and give the physician the power of personal interpretation. This Code is not well taught to students of medicine; however, physicians are expected to be aware of its content and are held accountable for it (Arawi 2010).
Most medical programs in Lebanon seek the Accreditation Council for Graduate Medical Education (ACGME) accreditation. The later claims that generating competent residents requires training that is ethically guided. This can be accomplished by providing students with the required education and training to improve their communication skills, allowing them to successfully handle any ethical difficulties that may occur. (ACGME-I 2022). Numerous studies have shown the beneficial effects that residency programs can have when they incorporate adequate ethics education into their curricula for their residents. Such instruction has been demonstrated to increase residents’ knowledge, self-esteem, and ultimately the caliber of the patient care they deliver. (Andersson et al. 2022; Helft, Eckles, and Torbeck 2009).
The integration of ethics into medical education and curriculum should be the current priority. (Vergano et al. 2019). In clinical practice, healthcare professionals and medical residents frequently have to navigate what is right and wrong when making decisions and providing quality treatment. (Torabi et al. 2020). Several studies have been undertaken to evaluate the value of ethics education in medical training, revealing its influence on raising awareness, knowledge, and capacity to make decisions in complex instances as well as enhancing self-esteem and ethical thinking. (Lehmann, Sulmasy, and Desai 2018).
Medical Ethics is a relatively new field in Lebanon. The importance of courses and training in ethics are not sufficiently appreciated. Such courses must become part of the core curriculum and must be taken seriously. This study was designed to assess the perception of the Lebanese medical residents on ethics training through their clinical years, and to shed light on the importance of this field on the ethical competence and the communication skills of the future doctors.
Methods
A cross-sectional descriptive study was conducted in 2023 between March and May. Participants in the study were postgraduate medical students (residents and fellows) rotating at various Lebanese hospitals affiliated with the Lebanese University (LU), including both government-funded and private institutions.
The study was approved by the LU ethics review board and it followed the Declaration of Helsinki guidelines, ensuring informed consent, confidentiality with unique participant codes, and restricted access to personal information.
A total of 250 medical residents were targeted given that LU offers 60 residency spots on average each year. Most residents expressed interest in responding upon reviewing the questionnaire. However, some declined due to its length. We ensured no data were missed by using a Google Form via WhatsApp for survey completion. Reminders were sent three times to enhance response rates, leading to the completion of the survey by 210 residents and fellows.
A self-administered validated questionnaire was adapted from a 2005 study conducted at the University of New Mexico in the United States (Roberts et al. 2004). It was adjusted to focus on key topics without overwhelming participants’ time. The questionnaire comprised six sections: demographic data, ethical experience and attitudes, agreement with education goals in ethics and professionalism, assessment of ethics training methods’ effectiveness, evaluation of assessment methods for professional attitudes and skills, and assessment of ethics education needs. Residents’ experiences, attitudes, and educational needs in ethics were gauged using a 9-point Likert scale ranging from (1) strongly disagree, much less, never, or not at all to (9) strongly agree, much more, very much, or all.
The reliability of this US questionnaire is checked using Cronbach’s coefficient alpha. Nunnally and Bernstein (1994) described that if Cronbach’s coefficient alpha is above 0.70, then the questionnaire becomes reliable.
Frequencies and proportions for categorical variables, mean and standard deviation (SD) or range (Minimum - Maximum) for continuous variables were given as descriptive statistics. Some continuous variable responses were represented as categorical variables, with scores of 1 to 4 interpreted as disagreement, 5 as neutral, and 6 to 9 as agreement, and they were displayed in pie chart or column charts.
Some other continuous variable responses were subjected to multivariate analyses of variance (one-way MANOVA) using separately the demographic characteristics: age class (< 30 vs. ≥30), gender (male vs. female), specialty (Internal Medicine vs. Surgery vs. Pediatrics vs. Obstetrics and Gynecology vs. Radiology vs. Emergency Medicine vs. Family Medicine vs. Anesthesia vs. Laboratory Medicine vs. Psychiatry), and level of residency (Junior resident vs. Senior resident vs. Fellow > R3) as independent variables. Separate analyses were conducted for each survey section. Only results that were significant were reported in tables and several statistically significant differences were also shown in line charts.
Considering resident’s attitudes toward professionalism and ethics education, some variables were combined into the composite variables “Mean of Professionalism” and “Mean of Ethics Education” and were included in the multivariate analyses. In another perspective, all 12 variables relating to residents’ attitudes toward professionalism and ethics education were combined into an overall score. The overall score was calculated so that the higher the score, the higher the perceived needs and attitude toward ethics education and vice versa. As a result, the scores for the two variables indicating whether physicians are more ethical than the general population and whether ethical conflicts are frequent in daily medical practice were flipped to have a positive interpretation. The median value of the overall score was used as a cutoff point for attitude categorization. Residents were classified as having a positive attitude toward ethics education if they had an overall score of ≥ 75 and as having a negative attitude if they had a score of < 75. Association between baseline characteristics of respondents and perceived needs and attitudes towards ethics education were performed using Chi-square tests.
Considering the effectiveness of ethics training methods, as well as knowledge and skills assessment methods and topics that need more attention, repeated measures ANOVA analyses were performed to identify any variations among the different methods or topics studied. Furthermore, Bonferroni post hoc tests were conducted for pairwise comparisons to specifically pinpoint the methods or topics where such differences emerged.
Statistical analyses were all performed using IBM SPSS Statistics software, version 26.0except for Cronbach’s coefficient alpha which was calculated using R software; and p < 0.05 was considered statistically significant (Bolded values in tables).
Results
Reliability of the US questionnaire for the Lebanese population using Cronbach’s test
Table 1. Reliability of the US questionnaire for the Lebanese population using Cronbach’s Test shows that the values of Cronbach’s coefficient alpha exhibited satisfactory internal consistency in most of the questions domain, highlighting the robustness of these questions in collecting feedback from Lebanese residents on ethics education. As a conclusion, the US questionnaire used on Lebanese population in this study is reliable.
Respondent characteristics
Two hundred and ten residents participated in the study and returned completed questionnaires. For certain variables, there were 1 to a maximum of 9 missing values found. Table 2 shows their age range as between 23 and 34 years (mean: 27.07 ± SD: 1.88). Residents were more female (56.2%). The main specialties of these residents were internal medicine (54.8%), surgery (15.2%), pediatrics (8.1%), and obstetrics and gynecology (5.7%). The other 16% of residents were in specialties such as anesthesia, radiology, emergency medicine, laboratory medicine, family medicine and psychiatry.
The majority were enrolled in a residency program (74.3%), with 26.2% being junior residents (in PGY1) and 48.1% being senior residents (PGY2/PGY3). The rest were enrolled in a fellowship program (25.2%, > PGY3).
Experience with ethical conflicts and ethics training
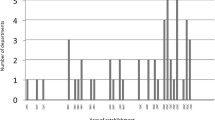
Table 3 summarizes residents’ experiences with ethical problems and ethics education, showing variations based on their ages. All residents reported experiencing a moderate level of ethical conflicts (mean = 6.02 ± 1.89, p > 0.05), moderate helpfulness of medical education in dealing with these conflicts (mean = 5.61 ± 2.13, p > 0.05), and a reasonable amount of supervision from residents and faculty members who serve as good examples of moral and professional conduct (mean = 5.2 ± 1.69, p > 0.05). Although the amount of knowledge in ethics was perceived low, younger residents (under 30) reported receiving more education in ethics and experiencing more ethically treatment form others and supervising residents, compared to older residents (over 30) (mean = 4.87 ± 2.07 vs. 3.6 ± 1.88, p = 0.009; mean = 5.46 ± 1.66 vs. 4.45 ± 2.01, p = 0.012, respectively). Results also showed that approximately 76% of residents attended ethics courses, with younger residents having a higher attendance rate than older residents (mean = 6.84 ± 2.17 vs. 5.05 ± 3.17, p = 0.001). Figure 1 illustrate that most residents who did not attend ethical courses felt that the classes were poorly scheduled (17.22%), while a small minority (4.31%) believed that the courses were less significant because they did not affect their GPA, and a negligible percentage (0.96%) believed that ethics could be learned through daily interactions with others.

Distribution of residents who did not attend ethical courses (24%, n = 50 out of 209) by their reasons for no attendance
Attitudes concerning ethics, professionalism, and values in medical training
Table 4 summarizes residents’ agreement with statements regarding various aspects of training in professionalism, ethics education, ethical issues and conflicts, and the impact of ethics training. It also shows how residents’ attitudes varied based on their ages and gender.
In the professionalism domain, including six statements that addressing different topics, residents of all ages and genders (all p > 0.05) strongly affirmed the importance of professionalism, highly endorsed its use in evaluating residents, and firmly supported swearing to uphold the profession’s values. They took a neutral stance regarding whether physicians are more ethical than the general population (mean = 5.09 ± 2.08, p > 0.05), and disagreed with the notion that most faculty physicians behave ethically toward trainees (mean = 4.53 ± 1.98, p > 0.05). However, older residents (over 30) rated the ethical practice of most faculty physicians toward patients lower than younger residents (under 30) (mean = 4.62 ± 2.06 vs. 5.47 ± 1.74 p = 0.04, respectively).
In the domain of ethics education, consisting of four statements, residents of all ages and genders (all p > 0.05) agreed that professionalism can be taught and learned, that ethics should be adequately taught in residency curricula (mean = 8.1 ± 1.27, p > 0.05), that ethical conflicts frequently arise during clinical practice, and that receiving ethics training promotes ethical conduct and helps in managing ethical conflicts. However, they all disagreed that their training was sufficient for managing the ethical dilemmas they encounter (mean = 4.39 ± 1.95, p > 0.05). On the other hand, female residents, compared to males accepted the idea that morals and values are learned through family, culture, and religious institutions (mean = 7.25 ± 1.72 for women vs. 6.6 ± 2.2 for men p = 0.021). Overall, residents’ acceptance of ethics education was moderately positive (mean = 6.73 ± 1, p > 0.05).
Goals of education in ethics, professionalism, and values
Table 5 presents residents’ agreement with educational goals related to ethics, professionalism, and values, along with gender differences in residents’ opinions toward these goals.
All assessed goals were considered desirable (agreement means > 5). Both female and male residents strongly affirmed goals (all p > 0.05) such as becoming better people and acquiring ethically valuable interpersonal skills, recognizing ethical issues, and reducing the likelihood of future legal or ethical errors by physicians.However only female residents showed stronger agreement with all goals, and significantly the ones of improving patient care and clinical decision-making (mean = 8.28 ± 1.14 for women vs. 7.8 ± 1.44 for men, p = 0.009), and developing pertinent interpersonal skills to heal and treat patients (mean = 7.94 ± 1.39 for women vs. 7.47 ± 1.75 for men, p = 0.04). Additionally, results indicated no statistically significant differences in the residents’ opinions toward educational goals based on their age, level of training, or their specialization.
Learning methods in ethics training
All eight methods of learning professional attitudes, values, and ethics were deemed effective, with mean effectiveness scores exceeding 5. Conducting an ANOVA with repeated measures, incorporating a Greenhouse-Geisser correction, revealed statistically significant differences in the mean effectiveness scores of these learning methods (F (4.77, 992.98) = 44.25, p < 0.001). Figure 2; Table 6 data indicate that clinical rounds (discussion groups of peers led by a knowledgeable clinician) and multidisciplinary expertise approaches (clinical ethics discussions with ethics consultants) emerged as the most effective learning methods (mean = 7.99 and 7.86, respectively, with a mean difference of 0.12 ± 0.097, p > 0.05). Case conferences, nontraditional methods (such as watching ethics-related videos followed by discussions led by knowledgeable clinicians), and the formal didactic approach through grand rounds presentations were ranked equally effective as the second most effective methods (mean = 7.55, 7.49, and 7.3, respectively, with mean differences of 0.062 ± 0.088 and 0.249 ± 0.122, p > 0.05). Lectures, as a formal didactic approach, were rated as the third most effective method. The least effective methods were the independent approaches (independent reading and web-based education) (mean = 6.48 and 6.4, respectively, with mean differences of 0.077 ± 0.109, p > 0.05).

Mean effectiveness of methods of learning about professional attitudes, values, and ethics as rated by residents (n = 208), the methods with the same color were perceived as not statistically different in effectiveness
Residents from various specialties rated the nontraditional watching videotaped on ethics topics followed by a discussion led by a knowledgeable clinician and the discussions on clinical ethics with ethics consultants significantly differently, as indicated in Table 6 (p = 0.009 and p = 0.03, respectively). Figure 3 showed that residents in internal medicine, surgery, pediatrics, obstetrics and gynecology, family medicine, anesthesiology, and laboratory medicine favored these two learning methods (means > 7), whereas those in radiology and emergency medicine found them less effective (means between 5 and 7).

Mean effectiveness of some methods of learning about professional attitudes, values, and ethics by residency specialty
Psychiatric specialty residents were a smaller group, with a preference for discussions on clinical ethics with ethics consultants (mean = 7.5 ± 0.71) and a lack of preference for the watching videotaped method (mean = 5 ± 2.83).
Methods of assessing skills and knowledge
For knowledge assessment
Figure 4 illustrates the variation in residents’ agreement level regarding the appropriateness of assessment methods for evaluating their knowledge related to professional attitudes, values, and ethics (p < 0.001).
Pairwise comparisons showed that Clinical supervision emerged as the top-rated assessment method among residents (mean ± SD = 8.04 ± 1.3), followed by oral examinations (mean ± SD = 7.1 ± 1.96). Conversely, multiple-choice examinations, short answer questions, and essays received similar and comparatively lower ratings compared to the other methods (mean ± SD = 6 ± 2.25, 6.45 ± 2.11, 6.22 ± 2.09, respectively).

Mean agreement with assessment methods appropriates for assessing the residents’ knowledge related to professional attitudes, values, and ethics as rated by residents (n = 210), the methods with the same color were perceived as similar in agreement levels
When examining the agreement levels for these assessment methods based on residents’ age, gender, university of graduation, as well as their specialization and level of training, no statistically significant differences were observed (results not reported here).
For skills assessment
Table 7 shows residents’ agreement with the appropriateness of various assessment methods for assessing their skills related to professional attitudes, values, and ethics. Residents’ ratings of the appropriateness of the 6 assessed skills assessment methods varied significantly (P < 0.001). Particularly, residents gave higher ratings to three methods: faculty direct observation of residents’ interactions with actual patients (mean = 7.4 ± 1.47), faculty observation of residents’ interactions with clinical team members (mean = 7.31 ± 1.63), and standardized patients’ assessment of their interactions with residents (mean = 7.02 ± 1.64). Conversely, lower ratings were given to evaluation of residents by patients (mean = 6.28 ± 2.3), evaluation of residents by non-faculty staff (mean = 6.03 ± 2.41), and faculty observation of videotaped interactions of residents with actual patients (mean = 5.78 ± 2.43). Additionally, there were differences in appropriateness ratings based on residents’ gender. Female residents rated the three top-performing assessment methods higher than their male residents did (mean = 7.62 ± 1.44 vs. mean = 7.11 ± 1.48, p = 0.013; mean = 7.55 ± 1.53 vs. mean = 6.99 ± 1.71, p = 0.014; and mean = 7.23 ± 1.63 vs. mean = 6.74 ± 1.64, p = 0.034, respectively).
Residents’ age and training level did not show any statistically significant differences in their agreement. However, when considering residents’ specialties, there were variations in the ratings of the appropriateness of faculty direct observation of residents’ interactions with actual patients. Specifically, residents in Laboratory Medicine, obstetrics and gynecology, and pediatrics specialties reported higher levels of appropriateness for this assessment method (results not reported here).
Residents’ opinions on ethics topics that need more attention
Figure 5 displays ethics topics that require more attention. More than 90% of residents reported that they needed more guidance on how to obtain informed consent from patients who are capable of making decisions (91.4%), more instruction on how to engage patients in discussing the risks, benefits, and alternatives to the recommended treatment with patient (91.4%), more training on conducting assessments of decision making capacity (90.4%), and more guidance on how to obtain informed refusal from patients who decline the recommended treatment (90%). Most residents (87.1%) reported that they needed more training on taking decisions on how much clinical information to share with patients and more guidance on how to obtain informed consent or refusal from surrogate decision makers (86.6%) and on deciding when to withhold information from patients (85.2%). A few other residents (81.9%) mentioned that they needed more guidance on how to obtain informed consent from non-English speaking patients, and how to obtain informed consent from patients whose capacity to make decisions is compromised (73.3%).

Residents’ opinion on ethical topics that need more attention (% of agreement) (n = 210)
Table 8 shows residents’ opinions on some common ethical, social, philosophical, and legal topics. It shows that 121 residents (57.9%) reported that acceptance of gifts from patients is an issue that should receive more attention while (61.43%) reported that the issue of receiving gifts and meals from drug companies should receive more attention. Above 80% of residents reported that the topics involving interaction with patients’ families (81.43%), responding to a colleague who was incapacitated (79.05%), resolving conflicts between allied health professionals (85.24%), resolving conflicts between attending physicians and trainees (88.57%), giving medical advice to friends and family (85.24%), keeping the confidentiality of the medical records (88.04%), maintaining medicine as a profession (82.78%), having social and political responsibilities (82.38%), coping with mistakes in clinical care (83.25%), and introducing students to patients as “doctors” (79.05%) should receive more attention. Between 70% and 80% of residents reported that mistreatment of residents (78.57%) and of medical students (75.71%) should be addressed, as well as gender bias in clinical care (73.21%), writing prescriptions for friends, co-workers, or family members (72.73%), learning procedures on cadavers (69.52%), having personal relationships with patients (69.05%), and experiencing sexual harassment (70%). Less than 60% of residents asked to give sexual contact between patients and physicians (54.76%) and sexual/romantic relationships between residents and medical students (58.85%) more attention
Discussion
To develop well-prepared trainees who can give high-quality management and reduce ethical difficulties, providing ethics training to post-graduate residents has become increasingly important. According to medical residents who participated in this study, ethics education is essential because it helps doctors deal with ethical challenges that arise regularly in clinical settings, which in turn promotes ethical actions and improves problem-solving abilities (mean agreement > 5). In observational research of 210 medical residents, the gender, age, specialty, and number of years of residency were considered. In many medical schools around the world, especially during the clinical years, ethics training is not well-established or maintained. (Lehmann et al. 2004).
Effective ethics training is now required for residents to prepare them to handle ethical issues that emerge in their everyday practice. (Bremer and Holmberg 2020). Experienced medical professionals must also develop the abilities and strategies to handle such issues. (Svensson et al. 2022). However, a study found that ethics education instruction intended to enhance ethical competence abilities did not necessarily correspond with how ethical problems are dealt with in actual practice (Bowsher et al. 2018). Establishing an effective ethics curriculum that starts in medical school and continues through clinical practice is therefore essential.
As far as we are aware, this is the first investigation of the importance of incorporating ethics education in the curriculum for medical residents in Lebanon. This study plants the seed for the creation of efficient teaching strategies and the development of appropriate ethics training during the clinical years as a standard for medical programs in general and Lebanese medical schools specifically.
Our study discovered that the ineffective timing and scheduling of these lectures throughout the year is the main cause of medical students’ lack of commitment to ethics courses in medical school. This draws attention to a crucial problem that demands attention. This result contradicts with Lisa et al. study’s which found that medical students’ low commitment to ethics knowledge was primarily caused by a lack of full-time ethics lecturers and inadequate financing. (Lehmann et al. 2004).
Regardless of age, gender, specialty, or medical school, more than two-thirds of residents stressed the need for greater attention to be given to nearly all ethical, social, philosophical, and legal themes mentioned in the study. This indicates either a lack of understanding on these subjects or a failure to practically use that information in clinical practice. Similar findings were made in a study by Robert et al., which highlights the difficulties medical residents confront and the necessity for further ethics training as they develop their clinical expertise (Hammond et al. 2005).
An established grasp of ethical principles, competence in carrying out crucial ethical duties, training in and adherence to values specific to a specialty, and residents’ interests in discussing and recognizing ethical issues should all be part of ethics education (Roberts et al. 2005). According to our survey, 76% of residents overall had taken an ethics course when they were in medical school, with younger residents participating more frequents reported receiving more ethics training and being treated more ethically by others and supervising residents than older residents, even though the amount of ethics training was thought to be low. This shows that medical schools are paying more attention to ethics education. Most residents did not, however, think that their preparation was enough for handling the ethical challenges they encountered during their clinical years.
In our study, there were no gender-related variations that were statistically significant in the incidence of ethical difficulties or in the usefulness of ethics courses in resolving ethical disputes. This result deviates from previous research findings (Ghamri and Al-Raddadi 2017; Roberts et al. 2004). This might be explained by the more ethics knowledge of the medical students now than in the study conducted in USA two decades ago (Roberts et al. 2004), and cultural differences (Ghamri and Al-Raddadi 2017). In addition, female residents had a higher likelihood than male residents of agreeing that morals and values are learnt through family, culture, and religious institutions (p = 0.021). Modern definitions, however, distinguish between morals and values and define ethics as a set of principles and guidelines that help people or groups decide what is right or wrong in a particular situation. Morals, on the other hand, are personal beliefs about right and wrong that are based on one’s conscience or cultural norms. As for the values, which are firmly held convictions and ideals that act as a foundation for moral decision-making and decency in conduct (Vergano et al. 2019). Results from Roberts et al. did not show this observation with respect to gender (Roberts et al. 2004). This could be explained by virtue thatthe Lebanese community has a conservative culture and a predominantly religious population; this can help to explain the discrepancy between our study’s findings and Robert’s findings.
The trainees in our study stressed the significance of this mindset for doctors in terms of professionalism. Surprisingly, most responses revealed a serious lack of ethical conduct on the part of faculty doctors toward both trainees and patients. This merits additional investigation (p = 0.04) as it was seen that older residents were more aware of it than younger residents. According to the report, medical residents do not receive adequate support from their advisers about ethical issues, and attending physicians should receive more training on how to handle such issues (Boer et al. 2022).
Many residents agreed with the objectives of ethics education, which include detecting ethical issues and enhancing ethical interactions and communication. In line with this, the emphasis on patient-centered care and interpersonal teamwork in healthcare was stated by Doolittle et al. (Doolittle et al. 2015). However, medical education does not place enough weight on the abilities and values required for compassionate, team-based treatment (Lown et al. 2016). The fact that female residents were more in agreement than male residents on objectives pertaining to patient care and clinical decision-making may be explained by their emotional and empathic upbringing. These results concur with similar investigations (Ghamri and Al-Raddadi 2017; Roberts et al. 2004). Therefore, postgraduate medical education should include a curriculum that promotes interprofessional competency (Gantayet-Mathur, Chan, and Kalluri 2022).
The study offered various learning methods to the residents, and the most effective one was clinical rounds with an expert clinician, followed by multidisciplinary rounds including ethics consultants. This coincide with the findings of the survey done in Saudi Arabia (Ghamri and Al-Raddadi 2017). Discussions among groups were found to reduce unethical behavior as reported by Chunbok et al. (Lee et al. 2021). To explore delicate subjects in ethical education, contact in clinical rounds and an open environment are also necessary (Kuhn et al. 2021). Healthcare workers and students can also make better decisions by concentrating on “thinking ethically” and developing their own rationale (Sánchez-Izquierdo et al. 2019). Reading on your own and attending theoretical courses on ethics are two ways to learn about ethics (Koo, Ryu, and Kim 2018; Shamim et al. 2021). As a result, theoretical learning and practical training can be combined to give medical residents real-world experiences (Shamim et al. 2021). However, our analysis found that individual reading and online learning were the least efficient approaches. It is worth to note that radiology and emergency residents’ perceptions of the benefits of clinical rounds were insignificantly lower from those of the remaining specialties. Both departments’ infrequent follow-up with patients and discussions of cases with clinicians can be used to explain this.
There is a general lack of an assessment tool for ethical competency of medical residents (Hong et al. 2021). Our study showed that more than 80% of the residents agreed that oral examination and clinical supervision were the best ways to assess their ethical understanding, nominating these assessment methods to be applied in medical residency training. The residents wanted a faculty member to observe and shadow them directly while they interacted with actual patients, members of the clinical team, and other residents in order to assess their ethical skills, since ethical competency is a real-life experience not just rules that can be memorized but an attitude and way of thinking that need to be acquired within clinical year residency training, this approach was investigated by several studies too (Cummings 2016; Goodrich, Irvine, and Boccher-Lattimore 2005).
This survey revealed a concerning finding: more than 50% of the trainees said they needed more attention and guidance, especially when it came to obtaining informed consent from capable patients (91.4%), educating patients about the risks, advantages, and treatment alternatives (91.4%), and determining patients’ capacity for decision-making (90.4%). Surprisingly, topics concerning social and legal issues such pharmaceutical drug company offerings, confidentiality, gender bias, and sexual harassment also attracted the attention of more than half of the residents under study. This shows the importance of our study in highlighting some of the common ethical issues that need education and training experience among the residents.
Study impact
The topic of ethics and professionalism education, which is still a relatively new area of medicine, is strongly supported by the findings of our study. Some significant investigations in this area have been started by academic authorities (Blank et al. 2003). Consequently, our research highlights the need for creating a strong ethics training program that equips residents and fellows with the necessary skills. Click or tap here to enter text.
Limitation
When evaluating the findings, it is important to consider the limitations of this study. First of all, because it is a cross-sectional study, it is possible that the sample size is not representative of all medical residents. Second, because the study depended on self-reporting, flaws including social desirability bias or response bias might have occurred. Thirdly, the study only examined residents’ attitudes and views rather than evaluating how the training affected their actual ethical behavior and decision-making.
Although the study has several weaknesses, it also offers some advantages. The fact that the study includes significant participants with respect to the population boosts the sample’s diversity and the generalizability of the results. Furthermore, the high response rate demonstrates that residents are highly interested in and concerned about training in medical ethics and professionalism. The perspectives from the many medical residency specialties were first collected in our study, which is another noteworthy point. The study also sheds light on areas that need to be improved upon and the challenges facing the training of medical residency programs’ ethics and professionalism education.
Conclusion
It is essential to recognize the areas of weakness and take necessary action to solve them to build an effective curriculum and training program for medical ethics. This study encourages the development of guidelines for structured ethics education during the clinical years, which is crucial for enhancing the competency of medical residents. Trainees can improve patient care and the healthcare system by concentrating on improving interpersonal communication skills.
Change history
11 July 2024
A Correction to this paper has been published: https://doi.org/10.1007/s40889-024-00195-z
References
Accreditation Council for Graduate Medical Education. 2021. ACGME program requirements for graduate medical education in internal medicine. … E At Http://Www.Acgme.Org/… (1): 1–35. http://www.acgme.org/acgmeweb/Portals/0/PFAssets/2013-PR-FAQ-PIF/140_internal_medicine_07012013.pdf.
ACGME-I. 2022. Accreditation Council for Graduate Medical Education - International. Requirements and Process Overview 11(1): 2–4.
Andersson, Henrik, Anders Svensson, Catharina Frank, Andreas Rantala, Mats Holmberg, and Anders Bremer. 2022. Ethics education to support ethical competence learning in healthcare: An integrative systematic review. BMC Medical Ethics 23(1): 1–26. https://doi.org/10.1186/s12910-022-00766-z.
Arawi, Thalia. 2010. The Lebanese physician: A Public’s viewpoint. Developing World Bioethics 10(1): 22–29. https://doi.org/10.1111/j.1471-8847.2009.00258.x.
Blank, Linda, Harry Kimball, Walter McDonald, and Jaime Merino. 2003. Medical professionalism in the new millennium: A physician charter 15 months later. Annals of Internal Medicine 138(10): 839–841. https://doi.org/10.7326/0003-4819-138-10-200305200-00012.
Bowsher, Gemma, Laura Parry-Billings, Anna Georgeson and Paula Baraitser. 2018. Ethical learning on international medical electives: A case-based analysis of medical student learning experiences. BMC Medical Education 18(1): 1–9. https://doi.org/10.1186/s12909-018-1181-7.
Bremer, Anders and Mats Holmberg. 2020. Ethical conflicts in patient relationships: Experiences of ambulance nursing students. Nursing Ethics 27(4): 946–959. https://doi.org/10.1177/0969733020911077.
Cummings, Christy L. 2016. Teaching and assessing ethics in the newborn ICU. Seminars in Perinatology 40(4): 261–269. https://doi.org/10.1053/j.semperi.2015.12.016.
den Boer, M., A. C., J. M. Zanin, Latour, and J. Brierley. 2022. Paediatric residents and fellows ethics (PERFEct) Survey: Perceptions of European trainees regarding ethical dilemmas. European Journal of Pediatrics 181(2): 561–570. https://doi.org/10.1007/s00431-021-04231-8.
Doolittle, Benjamin R., Daniel Tobin, Inginia Genao, Matthew Ellman, Christopher Ruser and Rebecca Brienza. 2015. Implementing the patient centered medical home in residency education. Education for Health: Change in Learning and Practice 28(1): 74–78. https://doi.org/10.4103/1357-6283.161916.
Emery, Alan E. H. 2013. Hippocrates and the oath. Journal of Medical Biography 21(4): 198–199. https://doi.org/10.1177/0967772013513395.
Gantayet-Mathur, Arpita, Karenn Chan and Meena Kalluri. 2022. Patient-centered care and interprofessional collaboration in medical resident education: Where we stand and where we need to go. Humanities and Social Sciences Communications 9(1): 1–24. https://doi.org/10.1057/s41599-022-01221-5.
Ghamri, Ranya A. and Rajaa M. Al-Raddadi. 2017. Assessment of perceived needs and preferences with regard to the education of residents in medical ethics in King Abdulaziz University Hospital. Journal of Family and Community Medicine 24(3): 189–195. https://doi.org/10.4103/jfcm.JFCM_34_17.
Goodrich, Thelma Jean, Craig A. Irvine and Daria Boccher-Lattimore. 2005. Narrative ethics as collaboration: A four-session curriculum. Families Systems and Health 23(3): 348–357. https://doi.org/10.1037/1091-7527.23.3.348.
Hammond, Katherine A. Green, Cynthia M. A. Geppert, Teddy Warner, Laura W. Roberts and Thomas W. Heinrich. Becoming a good doctor: Perceived need for Ethics Training focused on practical and professional development topics. Academic Psychiatry 29(3): 301–309.
Helft, Paul R., Rachael, E. Eckles and Laura Torbeck. 2009. Ethics education in surgical residency programs: A review of the literature. Journal of Surgical Education 66(1): 35–42. https://doi.org/10.1016/j.jsurg.2008.10.001.
Hong, Daniel Zhihao, Jia Ling Goh, Zhi Yang Ong, Jacquelin Jia Qi Ting, Mun Kit Wong, Jiaxuan Wu, Xiu Hui Tan et al. 2021. Postgraduate ethics training programs: A systematic scoping review. BMC Medical Education 21(1). https://doi.org/10.1186/s12909-021-02644-5.
Koo, Ok Hee, Young Mi Ryu and Myung Sook Kim. 2018. Effects of ethics education on ethical values in nursing students. Journal of Engineering and Applied Sciences 13(2): 2903–2908. https://doi.org/10.3923/jeasci.2018.2903.2908.
Kuhn, Eva, Laura Lunden, Penelope Moysich, Kai Rogge, Marijke Roscher, Lotta Caning and Annette Rogge. 2021. Ethik first – extracurricular support for medical students and young physicians facing moral dilemmas in hospital routine. GMS Journal for Medical Education 38(4): 1–15. https://doi.org/10.3205/zma001470.
Lee, Chunbok, Sunman Kim, Kwisoon Choe and Sunghee Kim. 2021. Effect of ethics seminar on moral sensitivity and ethical behavior of clinical nurses. International Journal of Environmental Research and Public Health 18(1): 1–7. https://doi.org/10.3390/ijerph18010241.
Lehmann, Lisa Soleymani, Wilard S. Kasoff, Phoebe Koch and Daniel D. Federman. 2004. A survey of medical ethics education at U.S. and canadian medical schools. Academic Medicine 79(7): 682–689. https://doi.org/10.1097/00001888-200407000-00015.
Lehmann, Lisa Soleymani, Lois Snyder Sulmasy and Sanjay Desai. 2018. Hidden curricula, ethics, and professionalism: Optimizing clinical learning environments in becoming and being a physician: A position paper of the American College of Physicians. Annals of Internal Medicine 168(7): 506–508. https://doi.org/10.7326/M17-2058.
Lown, Beth A., Martha E. Gaines, Sharrie McIntosh, Kathy McGuinn and David S. Hatem. 2016. Integrating compassionate, collaborative care (the ‘Triple C’) into health professional education to advance the triple aim of health care. Academic Medicine 91(3): 310–316. https://doi.org/10.1097/ACM.0000000000001077.
Milestones, Medical, Communication Knowledge, Practice-based Skills, Learning, and Systems-based Practice. 2014. The neurology milestone project. Journal of Graduate Medical Education 6(1s1): 105–115. https://doi.org/10.4300/jgme-06-01s1-33.
Nunnally, J. and I. Bernstein 3rd. 1994. Psychometric theory, 3rd edn. New York: McGrawHill
Roberts, Laura Weiss, Katherine A. Green Hammond, Cynthia M. A. Geppert and Teddy D. Warner. 2004. The positive role of professionalism and ethics training in medical education: a comparison of medical student and resident perspectives. Academic Psychiatry 28(3): 170–182. https://doi.org/10.1176/appi.ap.28.3.170.
Roberts, Laura Weiss, Cynthia M. A. Geppert, Teddy D. Warner, Katherine A. Green Hammond and Leandrea Prosen Lamberton. 2005. Bioethics principles, informed consent, and ethical care for special populations: Curricular needs expressed by men and women physicians-in-training. Psychosomatics 46(5): 440–450. https://doi.org/10.1176/appi.psy.46.5.440.
Sánchez-Izquierdo, Macarena, Marta Santacreu, Ricardo Olmos, and Rocío Fernández-Ballesteros. 2019. A training intervention to reduce paternalistic care and promote autonomy: A preliminary study. Clinical Interventions in Aging 14: 1515–1525. https://doi.org/10.2147/CIA.S213644.
Shamim, Muhammad Shahid, Adrienne Torda, Lubna A. Baig, Nadeem Zubairi, and Chinthaka Balasooriya. 2021. Systematic development and refinement of a contextually relevant strategy for undergraduate medical ethics education: a qualitative study. BMC Medical Education 21(1): 1–12. https://doi.org/10.1186/s12909-020-02425-6.
Svensson, Anders, Anders Bremer, Andreas Rantala, Henrik Andersson, Scott Devenish, Julia Williams and Mats Holmberg. 2022. Ambulance clinicians’ attitudes to older patients’ self-determination when the patient has impaired decision-making ability: A Delphi study. International Journal of Older People Nursing 17(2): 1–14. https://doi.org/10.1111/opn.12423.
Torabi, Mohammad, Fariba Borhani, Abbas Abbaszadeh and Foroozan Atashzadeh-Shoorideh. 2020. Barriers to ethical decision-making for pre-hospital care professionals. Nursing Ethics 27(2): 407–418. https://doi.org/10.1177/0969733019848044.
Vergano, Marco, Giuseppe Naretto, Fabrizio Elia, Enrico Gandolfo, Chiara Nebris Calliera, and Giuseppe R. Gristina. 2019. ELS (ethical life support): A new teaching tool for medical ethics. Critical Care 23(1): 3–5. https://doi.org/10.1186/s13054-019-2474-x.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: In this article Yasmine Choucair has mistakenly been mentioned as last author. Instead Dr. Fadi Abou-Mrad, as the project coordinator, should be placed as last author in the author group.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kanso, A., Farfour, I., Mansour, P. et al. Ethics training as a crucial scope in the various specialties of the medical residency. International Journal of Ethics Education (2024). https://doi.org/10.1007/s40889-024-00192-2
Accepted:
Published:
DOI: https://doi.org/10.1007/s40889-024-00192-2