
Abstract
Purpose of Study
Although the current treatment option of exogenous insulin administration for type 1 diabetes mellitus (T1DM) corrects hyperglycemia, it has its own limitations and complications in long-term use. Thus, alternative approaches such as immune therapies, glucose transporter inhibitors, gastro-enteric protein-hormone pathway modulators, and cell- and tissue-based therapies are being developed. Among these therapies, islet transplantation has been shown to be a more physiological means of treating type 1 diabetes. However, the shortage of donor tissues and the use of immunosuppressive agents have led to the development of immune isolation techniques such as cell encapsulation.
Recent findings
Although macroencapsulation of islets has been shown with some success, microencapsulation mostly with permselectively coated alginate hydrogel has been demonstrated to be superior among the variety of developed encapsulation technologies including nanoencapsulation and thus, has led to several clinical trials. While microencapsulated islet transplantation has shown promise in correcting the pathological symptoms of T1DM, the technology still requires improvement in a few areas in order to achieve sustained performance in long-term application.
Summary
Some approaches suggested for improvement include incorporation of immunomodulatory stem cells such as mesenchymal stem cells, substitution of current crosslinking agents with stable safe divalent cations, improving the chemistry of alginate by adding functional groups, and including extracellular matrix (ECM) components of the pancreas in the encapsulated islet construct. With thorough investigation and improvement on the pitfalls of the technology, and more clinical trials, the microencapsulation technology would provide a viable option for a sustainable and more physiological means of insulin delivery in T1DM.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus is a heterogeneous disorder characterized by polyuria and polydipsia. Type 1 diabetes mellitus (T1DM), previously referred to as insulin-dependent diabetes mellitus (IDDM), is mainly caused by destruction of the beta cells (β-cells) of pancreatic islets. Unlike type 2 diabetes, T1DM is not caused by lifestyle habits, but instead it is caused by either autoimmune reaction destroying the β-cells in pancreatic islets (type 1a) or due to other factors (type 1b) including idiopathic destruction, viral infection, and beta cell failure. If it is caused by autoimmune reaction, it might take time anywhere from months to years before symptoms manifest. Even though hereditary factors might play a role, they are not necessarily always the major causative agents for the disease.
Epidemiology of Diabetes
While about 463 million people worldwide are reported to be affected by diabetes, in the USA 23 million were diagnosed with the disease in 2016 [1]. Diabetes is ranked as the 7th leading cause of death [2, 3]. It has been estimated that up to another 7 million more adults in the USA may have the condition but have not yet been diagnosed. In addition, approximately 79 million more people in USA have been predicted to have pre-diabetes, where blood glucose levels are high, but not high enough yet to be classified as diabetes. Among all the diabetes cases, T1DM constitutes about 5–10% [3,4,5]. Reports from large epidemiologic studies have revealed that the incidence of T1DM has been increasing by 2–5% globally and the prevalence of T1DM is approximately 1 in 250 in the USA [3, 6]. In the USA alone, ~ 1.6 million are living with T1DM and another 40,000 people are diagnosed every year [3, 7]. T1DM has been the prevalent type of diabetes among children and adolescents who have been estimated to be more than 200,000, albeit T2DM is also increasing among youth [8, 9].
Current Therapies for Type 1 Diabetes
Exogenous Insulin Administration
The destruction of pancreatic beta cells (b cells) with concomitant loss of insulin, the endocrine secretion of this cell, is the primary cause for T1DM.. Therefore, insulin replacement therapy has been the first-line therapeutic option for treating T1DM. Ever since Banting and Best reported a century ago the glucose-lowering effects of their pancreatic extract [10••], there have been several improved extraction, biosynthesis, and administration techniques. Based on the size, molecular structure, half-life, and pharmacokinetics of insulin, various forms of injectable insulin analogs have been developed. These include (a) rapid-acting insulins, whose biological activity begins from 4 min and lasts for about 30 min; (b) short-acting insulins that are regular insulin whose biological actions begin from 30 min after administration and last for 4 h; (c) intermediate-acting insulins whose duration of action is from 4 to 6 h; (d) long-acting insulins that possess biological activity from 24 to 36h; and (e) ultra-long-acting insulins that start acting between 30 and 90 min and last up to 42 h [11]. The insulin replacement therapy requires administration of the hormone anywhere from once to thrice daily depending on the pharmacokinetics profile of the type of insulin.
A recent development in insulin therapy is research on ingestible oral insulin delivery systems such as self-orienting millimeter scale applicator (SOMA). These devices self-position themselves to engage with gastrointestinal tissues and deliver the milliposts directly through the mucosa membrane [12, 13]. The results from the rodent study using the SOMA have shown a comparable outcome with those achieved with subcutaneous insulin administration [13]. However, there is currently no oral insulin delivery system available to human patients afflicted with diabetes.
Insulin Pumps and Artificial Pancreas
The next level of improvement in administering exogenous insulin is the use of insulin pumps. This is an automatic continuous insulin infusion system which first senses the circulating levels of glucose and sends computer-controlled signal to the delivery pump to release the required amount of insulin [14,15,16]. This insulin infusion pump provides a better control on the glycemic index and delivers precise amount of required insulin with reduced insulin spikes and less hypoglycemic episodes (<70 mg/dL). However, these automatic insulin pumps also face some challenges such as occasional hypoglycemic episodes due to the inherent pharmacokinetic nature of the insulin analogs. This has led to the development of an automatic infusion system to deliver two hormones of the pancreas (insulin and glucagon) instead of insulin alone, and hence this automatic pump system that mimics the physiology of the pancreas is termed as “artificial pancreas.” These dual-hormone–delivering artificial pancreas devices administer both glucagon and insulin simultaneously to have tight regulation on the blood glucose level [17]. After improving the designs, undergoing various safety tests and efficacy tests, the artificial pancreas systems have shown beneficial effects in clinical trials [18].
Compared to insulin pumps, artificial pancreas systems have demonstrated significantly improved control on blood glucose with improvement in time and target range [19]. Considering the metabolic benefits, these artificial pancreas systems have been approved by the US Food and Drug Administration (FDA) to be used in T1DM patients [20]. However, there still exist some critical concerns about these artificial pancreas systems including affordability of such expensive devices by the average patient, high sensor replacement costs, build up in scar tissues due to repeated microneedle insertions, and the premature failure of sensors [21].
Alternative Approaches
Some alternative approaches that are being developed in treating T1DM include immunotherapies, sodium-glucose co-transporter 2 (SGLT2) inhibitors, peptide hormone–based therapies, and tissue-based therapies. The available knowledge on the root cause of T1DM shows that the beta cells of islets being destroyed by the immune system through autoimmune reactions, sustained suppression of auto regeneration of the tissue from stem cells around the β-cells by immune system, interplay of other hormones in the onset, and sustention of the disease form the basis of these alternative approaches. The interaction between beta cells and components of the immune system (both innate and adaptive immune system) involves various pathways, and therefore many immunomodulatory strategies have been proposed to abate or eliminate the autoimmune attack. Cyclosporin A was utilized in a therapeutic approach in a large clinical study during the late 1980s [22]. This immunomodulatory agent is known for its inhibition of cytokines such as interleukin-2 (IL-2) and thereby regulating the activation of T-lymphocytes (T-cells) [23]. Although the outcome of the study was promising, the remission of T1DM was only for a short duration and soon the daily requirement for insulin slowly increased with time [24]. Similarly, clinical intervention studies using monoclonal antibodies (mAb) such as anti-CD3 and anti-CD20 also resulted in only a transient preservation of beta cell functions based on the circulating C-peptide levels [25]. Other mAb approaches including anti-thymocyte globulin (ATG) and anti-human IL-1 (canakinumab) and use of IL-1 receptor antagonists (Anakinra) also failed to provide effective long-term management for T1DM [26, 27].
Studies are currently underway in developing the next generation of immunotherapies based on strategies modulating the activities of regulatory T-cells (Tregs) including anti-human IL-21 therapy (NCT02443155) [28]. Tregs have suppressive functions on other immune cells such as dendritic cells and cytotoxic T-cells. Hence approaches based on Tregs have been developed as biological alternatives to chemical immune suppression drugs to enhance islet graft survival [29]. A recent development along this line of work is the isolation of Tregs from T1DM patients using CD4, CD25, and CD127 surface markers and their expansion in vitro. These in vitro expanded Tregs, when administered into T1DM patients, have been reported to enhance the functional activities of Tregs for up to 1 year with detection of C-peptide in circulation [30]. In this same direction of work, another type of immunomodulatory study has been performed in a preclinical model where the immune system has been primmed with nanoparticles coated with pancreatic peptides and major histocompatibility complex class-II (MHC-II) proteins [31]. This triggers the generation and expansion of antigen-specific CD4(+) Treg type 1 cells (TR1), and these TR1 suppress the autoantigen-presenting immune cells, thereby suppressing beta cell–attacking immune cells and thus intervening to halt further progression of T1DM, in other words, enhancing the survival of islet grafts [32]. The Treg approach appears to be very attractive as it suppresses only the immune response that selectively targets pancreatic β-cells and does not interfere in any other immune reactions. Further studies and safety evaluations are needed before these approaches become part of T1DM therapies.
SGLT2 inhibition was initially developed as a therapeutic intervention for treating T2DM and has been evaluated in preclinical models [33] and patients [34]. Later this same approach has been investigated in a streptozotocin (STZ)-induced T1DM model and was reported to show direct beneficial effect in protecting and preserving the beta cell regenerative capacity. In addition, the SGLT2 inhibitor has also been reported to lower the body weight when combined with insulin, thus correcting the mild obesity caused by insulin monotherapy [35, 36]. The observations from preclinical studies led to the combination therapy of insulin and SGLT2 inhibitors (dapagliflozin and sotagliflozin) in recent clinical trials (dapagliflozin evaluation [DEPICT-1] phase II trial and Tandem3 phase III trial) [37]. However, long-term clinical trials and observational investigations are required to assess any potential side effect of this approach in order to assess the benefits of the combination therapy.
Other peptide hormones that constitute part of the digestive tract endocrine system have also been studied for their therapeutic values such as preservation of beta cell mass, suppression of beta cell apoptosis, enhanced insulin secretion, increasing insulin sensitivity, and glucose excursion [38]. The glucagon-like peptide 1 (GLP-1) pathway has been a main target in this approach where GLP-1 receptor (GLP-1R) agonists such as exenatide and liraglutide have been used as an adjunct to insulin therapy in T1DM patients [39, 40]. The findings in these studies have demonstrated a significant reduction in postprandial glucose excursions, decrease in glucagon production, and delay in gastric emptying in T1DM patients taking GLP-1R agonists along with insulin compared to the insulin monotherapy. Based on these studies, a proof-of-principle trial is currently underway (NCT02443155) combining IL-21 and GLP-1R agonist liraglutide. Oxyntomodulin (Oxm) is another peptide hormone of the digestive system, which is known to simultaneously activate both GLP-1R and glucagon receptor [41], as well as regulate beta cell functions [42]. Even though Oxm activates the receptors of glucagon and GLPs, a preclinical study has shown effects such as lowering of blood glucose and an increase in number of small-sized islets following Oxm monotherapy [43]. Similar to GLP-1, GLP-2 a peptide hormone released from endocrine L-cells of the small intestine also has been studied, and the data suggest a protective role of this hormone on pancreas, especially diminishing the stress-induced adoptive response of pancreatic islets [44].
Intestinal endocrine L-cells are known to produce another peptide hormone named peptide YY (PYY) found to be co-localized with GLP-1 and GLP-2. Interestingly, the PYY also expressed in alpha-cells, F cells (pancreatic polypeptide–producing cells), and delta-cells of pancreatic islets as well [45]. Hence, it has been suggested that PYY may play a critical role in preserving the islet mass and regulating the islet functions directly, thereby enhancing insulin secretion. Although most of the glucagon/GLP pathway–regulating peptides seem to be counterintuitive in T1DM treatment, the preclinical studies suggest otherwise such as lowering of blood glucose and preserving islet mass function. These observations highlight the therapeutic potentials of peptide hormones either as an adjunct with insulin or with other therapeutic agents. More clinical trials evaluating the benefits and side effects of these approaches will provide good guidance on their therapeutic values in the near future.
(Stem) Cell–Based Therapies
Since T1DM is an insulin-dependent condition caused by the destruction of native β-cells, treating the disease through replenishing the β-cell population using various approaches have been attempted. Protocols have been developed to differentiate insulin-producing β-cells from various stem cell types, and preclinical investigations have led to clinical trials [46]. de Klerk and Hebrok [47] recently published a concise review on stem cell–based clinical trial for diabetes mellitus, where the authors have provided a detailed list of clinical trials which have employed stem cells for the management of diabetes. Mesenchymal stem cells (MSCs) have been studied broadly in the stem cell–based therapies for T1DM. MSCs of different origins have been reported to have potential to generate insulin-producing cells. Although MSCs appear to be a promising source for both autologous and allogenic stem cell therapies [48], their therapeutic application in managing T1DM is highly controversial based on the clinical trial outcomes so far. Broadly MSCs have been used in managing diabetes based on the following hypotheses: (a) MSC-derived pancreatic progenitor in vitro, which were later believed to differentiate into insulin-producing β-cells; (b) undifferentiated MSCs which are expected to transdifferentiate into β-cells in vivo when transplanted into the pancreas; and (c) MSCs as supporting cells for the survival of islet in the pancreas without any differentiation into pancreatic progenitor cells. Even though the strategy of employing MSCs is effective for T2DM management, its direct effect on T1DM management is controversial because of some critical factors including the poor differentiation of MSCs in vitro and the failure of transdifferentiation in vivo. Since clinical trials have failed to produce clear evidence to support the hypothesis of MSC differentiation into β-cells and rather MSCs were shown to have mostly immune modulatory effects, investigators use MSCs as immune-protecting/immune-modulating supporting cells for β-cells [47]. The immunomodulatory properties of MSCs and their use as a strategy to evade immune response have been discussed later in this review under the “Immune-Modulation Approaches” section.
Human embryonic stem cell (hESC)–derived β-cells have been explored as another precursor source of β-cells. Although studies have shown success in deriving insulin-producing cells from hESC, transplantation of the resultant β-cells in patients requires immune suppression as these allogenic cells are known to trigger host immune reaction. The immune reaction is mainly caused by class I HLA molecule on their surface, and the existence of variations in this molecule adds another layer of complication, and hence using hESCs requires HLA-type stem cell banks [49]. On the other hand, removal of HLA molecule results in the immune attack by natural killer (NK) cells and therefore, warrants further investigations on how to overcome these issues for successful employment of these pluripotent stem cells in T1DM management. As an alternate to hESCs, induced pluripotent stem cells (iPSCs) generated from the somatic cells by induction of stem cell–related genes have been investigated. iPSCs were shown to have some advantages including safety and immune compatibility. However, the use of iPSCs has technical challenges in deriving insulin-producing cells, as the protocol needs to be adjusted according to the patient’s somatic cell properties. iPSC technology–based generation of pancreatic β-cells is complicated and time-consuming as it involves derivation of iPSCs first and then differentiation into insulin-producing β-cells. In addition to the patient-specific nature of these iPSCs, their genetic stability is still questionable. Moreover, the ability of iPSCs to differentiate into functional β-cells has not reached the same level as what has been observed with that of hESCs [50], which suggests that the stem cell–based technology development should be focused on alterations in the immunogenic properties of ESCs, including induction of immune tolerance and generation of “cloaked” ESCs which are invisible to host immune system. While, induction of immune tolerance have been studied using tolerogenic cytokines and immunomodulatory proteins such as CTLA-4 and PD-L1 [51], the “cloaked” cell approach has been attempted by modifying HLA protein expression on the surface of hESCs [52,53,54]. Recently, Gornalusse et al. [55] have generated hESCs expressing less variable HLA type (HLA-E), which provides the cloaking effect to the hESCs, and these cells have good potential as suitable allogeneic cells in several stem cell–based technologies including T1DM management for any patient without immune suppression, and therefore, the authors referred to these cloaked cells as “universal stem cells.” However, this technology requires further validation and characterization before being employed in clinical trials for stem cell–based therapies in T1DM.
Tissue-Based Therapies
Pancreatic islet is known to be composed of other cell types in addition to β-cells, and the choice of pancreatic tissue replacement (whole pancreas or pancreatic islet) appears to be a more natural and viable alternative compared to cell-based therapy [56]. Whole pancreas transplantation has been shown to improve the quality of life in T1DM patients as it stabilizes or improves diabetes-associated complications such as nephropathy, neuropathy, retinopathy, and macrovascular complications [57, 58]. The first whole pancreas transplantation was reported at the University of Minnesota, USA, in 1967 [59] and ever since, with the improvements in the surgical techniques and advancements in immunotherapies for T1DM, has led to an increase in the number of pancreas transplantations according to the International Pancreas Transplant Registry (IPTR) [60,61,62]. Pancreas transplantation has been performed under one of the following schemes: (a) pancreas transplant alone; (b) simultaneous pancreas and kidney transplant; (c) pancreas after kidney transplant; and (d) transplanting pancreas from deceased donor simultaneously with live donor kidney [63]. Pancreas transplantation is a complicated procedure associated with significant levels of mortality and morbidity. The major limitation of this approach is the critical post-operative complications of pancreas transplantation including graft rejection, vascular thrombosis, hemorrhage, pancreatitis, peripancreatic fluid accumulation, and exocrine leaks [64]. Another limitation of this procedure is the ratio between the volume of functional tissue and the nonfunctional associated tissue. Of note, only 1–2% of the pancreas is made up of the functional units referred to as “islets,” as the parenchyma is predominantly made up of the exocrine tissue.
Pancreatic islet transplantation as opposed to whole pancreas transplantation is an evolving and promising therapeutic approach for the management of T1DM. In this approach, the pancreatic islets are isolated from the pancreas, purified from any extraneous tissues, and transplanted into the recipient. The concept of islet transplantation was successfully demonstrated by Ballinger and Lacy in 1972, where the isolated islets were infused through intraportal vein in to STZ-induced diabetic rats [65]. Later, the same approach was successfully replicated in human subjects where the isolated autologous islets were successfully transplanted [66]. While the development of the Ricordi chamber provided an improved islet isolation method [67], the Edmonton study optimized both the islet isolation procedure and the post-transplantation care in clinical trial [68••]. The Edmonton protocol has been adopted globally as a standardized protocol for clinical studies on islet transplantation and has led to the establishment of 36 centers worldwide for Collaborative Islet Transplant Registry (CITR) as of 2020. As a result, there has been a considerable improvement in islet transplantation during the past two decades with many refinements in the pre- and post-transplant procedures [69, 70]. However, there are still significant challenges in islet transplantation for the treatment of T1DM including the occurrence of instant blood–mediated inflammatory reaction (IBMIR) immediately after transplantation, loss of islet mass due to cold ischemia, apoptosis of islets, and the detrimental side effects of immunosuppressive agents on islets [71, 72]. Therefore, strategies are being developed to improve the outcome of the islet transplant transplantation for the treatment of T1DM. Among these strategies, the encapsulation of islets to circumvent the use of immunosuppressive agents is a significant milestone, which we will now discuss in the following sections of this review article.
Islet-Based Approach vs Exogenous Insulin Therapy
The standard treatment option of exogenous insulin administration to treat hyperglycemia causes in T1DM patients some undesirable effects including severe hypoglycemic episodes, lifelong dependency on exogenous insulin, subsequent insulin resistance, mild obesity, and even psychiatric conditions [73,74,75]. Interestingly, studies have demonstrated that T1DM patients presenting with remnant β-cells as demonstrated by detectable C-peptide in circulation are less prone to developing microvascular complications compared to those who are completely C-peptide deficient [76]. This has led to investigations of the biological effects of C-peptides as well as a series of studies to assess the clinical benefits of C-peptide administration in T1DM patients who lack the peptide. The outcome from these studies was an apparent demonstration that C-peptide replacement at physiological levels resulted in significant improvement in various T1DM-induced functional abnormalities [77,78,79,80,81]. This subsequently has led to thorough investigations on the biological role of C-peptides that have provided vital information including the membrane binding of the peptide and intracellular signaling mechanisms [82]. Therefore, C-peptide that was earlier considered as an inert byproduct of insulin processing has now been shown to have critical physiological functions including the prevention of microvascular damage, kidney, and nerves [83,84,85] and may thus be considered as a previously missed therapeutic biomolecule in the treatment of T1DM [86].
As mentioned in the “Alternative Approaches” section, the other secretions of pancreatic islets such as glucagon and GLPs have been reported to play critical role in the tight regulation of blood glucose, thereby ameliorating the complications associated with chronic hyperglycemia. Similarly, there may be other putative, yet to be discovered, biomolecules produced by islet cells that may still be missing in the current exogenous insulin-based therapies. This highlights the advantages of islet-based therapies over the insulin-based therapies. Even though islet transplantation is a minimally invasive, clinically available, and preferred approach to treat patients with labile diabetes (uncontrolled T1DM), this islet-based approach still faces two critical challenges including the limited availability of human islets for transplantation due to donor shortage and the histocompatibility issue associated with lifelong dependency on immunosuppressive drugs. The later has been reported to cause detrimental effects on the transplanted pancreatic tissues such as direct β-cell toxicity and impaired islet viability and functionality [87,88,89,90,91]. Therefore, approaches such as islet encapsulation have been developed to provide immune isolation for the transplanting islets in T1DM cases.
Islet Immune Isolation (Encapsulation) Strategies
Islets of Langerhans, the functional endocrine unit of the pancreas as depicted in Fig. 1, comprise 20% with glucagon-producing α cells, 70% with insulin-producing β-cells, 5% with somatostatin-producing δ cells, 1–2% with pancreatic polypeptide–producing F cells, and the remaining portion made up of substance P–producing enterochromaffin cells and ghrelin-producing ε cells [92]. The composition of islets varies from region to region within the pancreas, and islets constitute 1–2% mass of the pancreas. There have been various isolation techniques developed to obtain the islets. Islets are known for losing function under long ischemia duration or prolonged hypoxic conditions. Since T1DM is a condition where the β-cells are completely destroyed, they may be replaced by islets from allogenic source, which requires either the use of immunosuppressive agents or the development of immune isolation techniques to avoid use of immunosuppressive agents [93].

Schematic of immune-isolating islets. Pancreatic islets enclosed in hydrogel with permselective pore size allow the diffusion of gases, nutrients, and islet secretions while blocking the entry of immune cells or their antibodies. A Pancreatic islet composed of different cells types; B schematic of immune isolation; C dithizone-stained islet encapsulated in alginate microcapsule
Scientific Rationale behind Encapsulation of Islets
To circumvent the use of immunosuppressive agents in islet transplantation, immune isolation strategies such as encapsulation have been developed. Cellular immune isolation concept is based on the principle of separating the transplanted cells/tissues from the host immune system using a selectively permeable membrane to coat the cells [94, 95]. The membrane or selectively permeable pore-sized encapsulation materials allow neither the entry of inflammatory cells nor the entry of large immune modulatory molecules such as antibodies and some cytokines, and therefore as shown in Fig. 1B, such permselective membrane-protected islet tissues are generally referred to as bioartificial pancreas (BAP) (Fig. 1B and C). The immune isolation technology solves two major obstacles in the clinical application of islet transplantation: (a) the need for immunosuppressive agents and (b) expansion of pancreas donor sources as it facilitates the use of xenogeneic islets [68••].
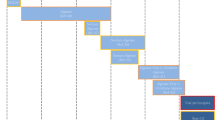
The concept of immune isolation dates back to 1933 when Vincenzo Bisceglie described successful encapsulation of tumor cells in a polymer [96], and since then several different devices and designs have been developed [97,98,99,100,101,102] and studied in both preclinical models [103,104,105,106,107,108] and clinical studies [109,110,111]. Encapsulation is an immune isolation technique as well as a bioengineering technology, where the therapeutic cells or tissues are encased in a permselective biomaterial to evade the host immune reaction. In general, encapsulation devices can be classified into the following categories as shown in Fig. 2: (a) intravascular device, (b) extravascular macroencapsulation device, (c) extravascular microencapsulation device, and (d) nanoencapsulation (islet surface coating) or conformal coating. Classification as intravascular or extravascular device depends on whether or not it is connected directly to the blood circulation. Similarly, the macro- or microencapsulation classification depends on the number of islets enclosed in the device. While clubbing many islets together as a single construct during the encapsulation process is referred to as macroencapsulation, encapsulating a few individual islets (usually <3) in a selectively permeable microsphere is referred to as microencapsulation. Several hydrogel materials have been used to encapsulate islets by different groups and have reported with success in lowering the blood glucose level. Among various materials that have been used, alginate have been identified as an ideal material for its superior qualities over others.

Different types of encapsulation to immune-isolate islets. a Intravascular macroencapsulation approach where a bunch of islets are encapsulated in a selectively permeable cylindrical device and wrapped around the blood vessels. b Extravascular approach in which more than one islet is encapsulated in a selectively permeable sealed tubes, sheets, or slabs. c Microencapsulation encases 1–3 individual islets in a permselective microsphere. d Nanoencapsulation coats the surface of islets with selectively permeable membranous materials providing conformal nano-coat around the islets
Earlier Form of Encapsulation—Intravascular Macroencapsulation
Intravascular encapsulation contains a design with a small chamber that is directly connected to the recipient’s vascular system [112, 113]. The main biomaterial used in this encapsulation is composed of copolymer polyacrylonitrile-polyvinyl chloride (PAN-PVC) [114]. Originally, this approach was applied in autologous islet transplantation and reported to be successful in rodent and nonhuman primate models [115]. Later, it was modified and tested for allogenic islets [116, 117]. However, such an intravascular encapsulation system has never been developed for clinical conditions. The intravascular encapsulation system provides an advantage to the islets because of close contact with the blood stream allowing for fast exchange of glucose and insulin and therefore, rapid control of circulating levels of glucose. The major drawback of this approach is the requirement of a major surgical procedure to implant the encapsulated islets. In addition, like any other type of vascular prostheses, this encapsulation approach also poses some risks such as thrombosis, infections, and primary or secondary intimal hyperplasia at the venous anastomosis (Table 1). In addition, to prevent blood clotting and cellular adhesion in this approach, it requires (a) anticoagulation agents, (b) use of large lumen device, and (c) high flow rate through the macroencapsulation device. The drawbacks in the current designs in this approach makes it not suitable for clinical use in treating T1DM patients.
Modern Era of Encapsulation—Extravascular Encapsulations
Extravascular encapsulation has been shown to be a much safer approach than the intravascular approach for the islet delivery. The encapsulated islets can be implanted with minor surgical procedure and depending upon the site of implantation can be readily retrieved in case of any complications associated with the implanted islets. The superior qualities of the extravascular encapsulation devices appear to be suitable for clinical use and hence they continue to be investigated with various modifications and improvements. With advancement in various aspects of this approach, studies in extravascular islet encapsulation devices are considered to constitute the modern era of encapsulation. In this category, till date three different types of encapsulation have been developed and investigated. The three forms of extravascular encapsulation systems, which are discussed in this section, are (1) macroencapsulation, (2) microencapsulation, and (3) nanoencapsulation.
Macroencapsulation
In this approach, a multitude of islets are packed in a biomaterial such as PAN-PVC and implanted at a site which may contain capillary network. The initial studies with extravascular macroencapsulation devices containing a group of islets enveloped in one or several large capsules were unsuccessful. The main reason for the failure has been attributed to the aggregation of islets into large clumps that led to necrotic cores with limited diffusion of nutrients and gases [118]. Improvement in the design have been brought about by immobilizing the islets in a matrix before encapsulating them in macrocapsules, and the outcome was encouraging in an animal study with a survival rate in rats reported to be for up to 200 days post-implantation in the peritoneal cavity [119]. Similarly, some level of success has been reported in a human study after implanting the microencapsulated islets subcutaneously [120••]. The macroencapsulation device was structurally weak and could rupture easily during the implantation procedure. To overcome the problem in structural vulnerability, a sheet type device was made (Fig. 2B) that could be handled easily [121], and this improvement was believed to accommodate this approach for clinical application. However, an inherent drawback in the macroencapsulation approach is the relatively large surface-to-volume ratio of macrocapsules, which interferes with the diffusion of essential nutrients and gases. To ensure adequate supply of nutrients to the islet cells, the islet density inside the macrocapsules is kept very low and never exceeds 5–10% of the volume fraction. As a consequence, very large macroencapsulation devices need to be implanted to meet the therapeutic demand. It is highly impractical to implant such large devices in conventional transplantation sites such as the liver, kidney capsules, or spleen [122]. Even the large peritoneal space is not sufficient enough to implant such large volumes of microencapsulated islets for long-term performance. In addition, the relatively large surface-to-volume ratio in this approach also interferes with optimum regulation of blood glucose due to the slow exchange glucose and insulin in these macrocapsules.
Microencapsulation
Current insights point toward microencapsulation as the preferred approach to transplant islets in diabetic individuals as microcapsules offer optimum volume-to-surface ratio that aids fast exchange of nutrients and hormones. The principle of microencapsulation is based on enveloping individual islets into microspheres using suitable polymer (Fig. 1B and C; Fig. 2C). The polymer used in microencapsulation should not affect the viability and function of the encapsulated cells and tissues. In addition, it should meet essential criteria of forming scaffolds that are flexible, yet soft enough, are mechanically strong, and allow the diffusion of nutrients into the capsules and therapeutic hormone (insulin) out of the capsules into the recipient’s blood stream. Owing to their flexible and tunable nature, hydrogels are used in fabricating microcapsules. Over the past three decades, several hydrogels including alginate [123], poly(hydroxyethyl methacrylate-methyl methacrylate), agarose [124], polyethylene glycol (PEG) [125], acrylonitrile copolymers, and chitosan [126] have been frequently used in microencapsulation techniques. Till date, the most desirable material for microencapsulation is alginate, which forms liquid when reconstituted in aqueous solution and then gets gelled into rigid microspheres when crosslinked with divalent cations.
Alginate (the anhydrous form of alginic acid), a collective term used for a family of polysaccharides synthesized in seaweeds and bacteria, is composed of two monomers, namely α-L-guluronic acid (G unit) and β-D-mannuronic acid (M unit) [127]. Alginate as a biomaterial exists with a varying gelling property due to the difference in the compositions of G and M units. Existence of more G units results in a stiffer and stronger gel, while abundance of M unit yields a softer gel. Further, the choice of divalent cation also is a determining factor on the stiffness of the gel. In general, the divalent cations used for microencapsulating cells and tissues include calcium (Ca++), strontium (Sr++), and barium (Ba++). Alginate hydrogels formed by crosslinking with Sr++ are stronger and stiffer than Ca++-crosslinked gels [128]. Similarly, Ba++ yields a stiffer gel compared to Sr++ and Ca++ [129, 130]; however, the use of Ba++ for encapsulating cells and tissue has at times been debated due to their potential toxicity [131,132,133] and hence avoided in most studies. The porosity or stiffness of the alginate gel depends on the following parameters: (a) composition of G and M units in alginate; (b) concentration of alginate used for microencapsulation; (c) choice of crosslinking divalent cation; and (d) concentration of crosslinking divalent cations [134, 135].
Devices used for microencapsulation have also evolved since the technique was first introduced. Originally, microencapsulation devices consisted of a design with an extrusion of islet-laden alginate into droplets and collected a divalent cation crosslinker (calcium chloride (CaCl2) solution) bath, as shown in Fig. 3A [136••]. Several improvements have been made in the design of extrusion-based microencapsulation devices to obtain desired characteristics of the islet microcapsules [137]. Since devices based on the initial model extrude alginate through a nozzle into a single file of islet-laden alginate stream that uses gravity as the shear force to cut it into droplets, it creates a heterogeneous population of microcapsules with varying sizes ranging from 300 to 1000 μm in diameter. Often, more than one islet end up within a large-sized microcapsule with a lot of empty capsules in this approach. However, the size of the microcapsules can be adjusted with the needle sizes that are used as nozzles in these devices. When a coaxial airflow has been used as a shearing force in the design to cut the file of islet-laden alginate stream as depicted in Fig. 3B, it aided in generating homogeneity in microcapsule size with most beads containing a single islet and only occasional empty beads.

Schematic of microencapsulation devices. Extrusion devices (A–D) produce droplets that are crosslinked by divalent cations to create hydrogel microcapsules. A Simple droplet generator uses gravity as force to form the alginate-islet droplets and microcapsules; B coaxial air channel converging at the extrusion nozzle acts as a shear force to generate homogenous microcapsules; C electrostatic potential between the extrusion nozzle and crosslinker bath electrospray beads of reduced size; D inclusion of two input channels (alginate and islet delivery through different channels) helps to create microcapsules with alginate sheath and liquid core; E microfluidic chip uses single channel of oil or two channels of oil (F) as shearing force to generate microbeads within the device; G separate channels for islets, alginate, and oil generate microbeads with liquid core and alginate sheath
Many groups (including ours) developed their microencapsulation device design based on this principle, and the generation of empty beads can be avoided by adjusting the number of islets per mL of alginate suspension used. Similarly, the sizes of the microcapsules produced can be maintained as small as 300 μm by controlling the flow rate of islet-laden alginate through the nozzle and pressure of airflow (Fig. 1C) in addition to adjusting the needle size [138, 139]. Similarly, electrostatic potential has also been used as shearing force to create homogenous smaller microcapsules (Fig. 3C) [140, 141]. In one approach, the investigators included a liquid core harboring the islets and an alginate sheath around it by modifying the design, as shown in Fig. 3D [142]. Alternatively, microfluidic designs have been developed on chips using technologies such as photolithography and threedimensional (3D) printing [143]. These chip-based microfluidic devices are very tunable to achieve the desirable microcapsule profile by making a few alterations in their designs as depicted in Fig. 3E–G [144,145,146]. The advantages of microfluidic devices in general include the ability to control microcapsule size with a possibility of obtaining microcapsules as small as 100 μm and the uniformity in the generated beads [147]. In addition, the microfluidic approach permits high throughput manufacture, which is not available in extrusion-based devices [148, 149]. Further, the microfluidic chip microencapsulation design provides room for internal crosslinking where the islet-laden alginate solution is mixed with inactive form of crosslinking cations and then activated within the device allowing the crosslinking process to occur from inside-out direction in the microbeads instead of outside-in direction in conventional design [147]. It also avoids any microencapsulation process–induced stress on the very sensitive islets.
The immune isolation property of alginate microcapsules is determined by the molecular permeability of the alginate hydrogel used in microencapsulation. In turn, the molecular permeability of alginate depends on the porosity of the hydrogel itself and the biochemical characteristics of the molecules involved such as size, shape of the molecule, molecular weight, and presence of charged group. The porosity of the alginate hydrogel ranges from 5 to 200 nm [150, 151], depending on the four parameters mentioned earlier such as (a) composition of G and/or M unit; (b) concentration of alginate solution; (c) type of divalent cation used for crosslinking; and (d) concentration of cation. This range of porosity would allow molecules less than 650 kDa (650,000 Da) to diffuse through it including oxygen (~16 Da), carbon dioxide (~44 Da), urea (60 Da), glucose (180 Da), insulin (5.7 kDa), and other macromolecules [152]. In some studies, it has been reported that alginate permits only proteins less than ~ 25 kDa including insulin and restrict macromolecules such as antibodies [153, 154]. However, in other studies, it has been reported that the alginate hydrogel may be permeable to proteins up to ~250 kDa and polysaccharides up to ~ 50 kDa [155, 156]. The variation in the permeability could be attributed to the type of crosslinking cation with its eventual effect on the porosity of the alginate hydrogel used in these studies. Hence, the porosity of the alginate hydrogel needs to be adjusted appropriately to provide immune isolation.
Further, the use of polycationic molecules such as poly-L-Lysine (PLL) or poly-L-Ornithine (PLO) for semi-selective coating of alginate hydrogel microbeads has been shown to provide immune isolation for encapsulated cells [157,158,159,160,161,162]. It is the poly-anionic nature of alginate that allows the application of poly-cationic materials (PLL or PLO) as coatings on the external surface of the microcapsules. To circumvent any immune reaction induced by the positively charged polycationic coating, a second layer of alginate is applied as the final coating on top of the polycationic semipermeable membrane in the microcapsule design (Fig. 4G–I). Thus, the layer-by-layer encapsulation approach yields multilayered microcapsules referred to as alginate-PLO/PLL-alginate (APA) microcapsules [159, 160]. In general, encapsulation increases the diffusion length of essential materials such as nutrients and gases for the islets from the extracellular fluid (ECF). Even though the size of islets ranges from ~50 to ~250 μm, when encapsulated an increased size (~500–800 μm) of homogenous microcapsules occurs. Since each islet is of a different size and the microcapsules are approximately of the same size, the diffusion length of alginate around the islet also varies from one encapsulated islet construct to another. In addition, the performance of encapsulated islets varies with transplant sites. For instance, when transplanted in the peritoneal space, the lack of vascularization and the requirement of large quantities of encapsulated islets not only to correct the hyperglycemic condition in T1DM, but also to compensate any necrotic loss, are considered as major limitations of microencapsulated islet transplants.

Some of the strategies to improve the functionality of microencapsulated cells. A–E Incorporation of POGS (CPO and SPO) in the alginate, while encapsulating islets to supplement oxygen have shown an increase in viability (B and D) and an enhancement in insulin expression (C and E) (adapted from McQuilling et al. [163] with permission). F–I Modification in the microcapsule design including the APA design (G), liquification of the core harboring islets (H), and incorporation of growth factors in the outer shell of APA microcapsules (I). J and K Calcium precipitation observed in Ca++-crosslinked microcapsules that were retrieved 90 days post-transplantation (J) has been rectified by the substitution of Ca++ with Sr++ (K) (adapted from Sittadjody et al. [160] with permission). L–U Incorporation of ECM materials have demonstrated an improved microcapsule structural integrity and islet function (adapted from Enck et al. [147] with permission). CPO, calcium peroxide; SPO, sodium peroxide; MTS, (3-(4,5-dimethylthiazol-2-yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium); qPCR, quantitative polymerase chain reaction; INS, insulin; CASP-3, caspase -3; PLO, poly-L-Ornithine; SrCl2, strontium chloride; ECM, extracellular matrix of pancreas; GSI, glucose stimulation index
Nanoencapsulation
Nanoencapsulation or conformal coating is an emerging technique in encapsulation where thin films of hydrogel are placed onto the surface of islets (Fig. 2d) by interfacial polymerization [164,165,166]. Different combinations of nano-coating compounds that were attempted as hydrogels include (a) streptavidin and biotin-PEG derivatives [167, 168]; (b) complement receptor 1 and heparin [169]; and (c) PEG-lipid and poly(vinyl alcohol) [170, 171]. However, commonly used hydrogels for nanoencapsulation are acrylate-based polymers such as acrylate polyethylene glycol (PEG) which is referred to as “PEGylation” [172, 173]. The original method of nanoencapsulation was developed at the University of Texas [174] and involves thin layers of polymers applied on to the surface of islets and the polymerization activated by light in order to provide a conformal coating around the islets on a nanoscale. Briefly, photo-initiator eosin Y is applied to the surface of islets, followed by adding a mixture of acrylate PEG, n-vinylpyrrolidone (NVP) monomers, and a polymerization accelerant compound triethanolamine (TEA), and then finally exposed to ultraviolet (UV) light to crosslink the acrylate PEG and NVP and in order to form a thin film of hydrogel around the islets [175]. Other than the PEGylation approach of nanoencapsulation, layer-by-layer encapsulation method also has been employed in conformal coating [167,168,169,170,171, 176,177,178,179,180]. Conformal coating solves the problem of diffusion length as it provides the same diffusion length for all nano-capsules. Another advantage of nanoencapsulation is the improvement in the surface-to-volume ratio, which allows for implanting increased number of islets in contrast to other encapsulation approaches. However, the major limitation in nanoencapsulation is the difficulty in clinical application. It is also challenging to retrieve or remove the transplanted islets (in the case of nonfunctional implants), since there is no control over the location of individual nanoencapsulated islets in this approach [181, 182]. Further, in some cases, islets get exposed due to incomplete coating during the nanoencapsulation process, which can trigger immune reactions in the host and lead to graft rejection [168]. The use of certain components in nanoencapsulation technology such as PEG, TEA, and UV light also contributes to cytotoxicity and compromises the viability of islets [183, 184]. Therefore, additional investigations are required to develop less immunoreactive formulations to allow for a safer nanoencapsulation technology to achieve the desired goal and meet the physiological demands of islet transplants.
Encapsulated Islets in Preclinical Studies and Clinical Trials
Islet encapsulation technology provides immune isolation for the transplanted islets by utilizing immune-protecting biomaterials to create selectively permeable scaffold and membrane around the islets. Such immune-isolating device that harbors islets and support their long-term survival and function is referred to as “bioartificial pancreas.” Following various in vitro analysis and characterization, the encapsulated islets have been studied in preclinical animal models and clinical trials to assess their therapeutic potentials. The following section discusses some of the important studies that have evaluated the efficacy of various forms of encapsulated islets in vivo.
Macroencapsulated Islets
Macroencapsulation-based devices at the macroscopic scale (> 1 mm) mostly come in either circular or planar designs with islets embedded in hydrogels and placed within semipermeable chambers. An initial preclinical study in diabetic dogs with multilayered alginate sheet encapsulating islets (central layer containing islets sandwiched by two empty alginate layers) demonstrated excellent graft survival and achieved normoglycemia for 12 weeks [121]. A similar design by Dufrane et al. that comprises a central islet-embedded alginate layer covered on both side by collagen matrices was used to encapsulate porcine islets and implanted subcutaneously into diabetic monkeys. The macroencapsulated xeno-islets were shown to correct hyperglycemia for up to 6 months without any immunosuppression. Even though a strong immune response was detected in this NHP study, the alginate layer was found to be impermeable to immunoglobulin G (IgG) up to 20 weeks post-transplantation [185].
The major drawback of macroencapsulation, poor oxygen diffusion through the graft due to the size of the device, has compromised the viability and function of implanted islets. To address this issue, Beta-O2 Technologies Limited has developed a macroencapsulation device referred to as “β-Air” with an oxygen diffusion channel which can supply oxygen through an external tubing system [186]. Macroencapsulation device in this design can be fabricated in different sizes ranging from 31.3 mm × 7 mm to 68 mm × 18 mm suitable for preclinical investigation or clinical trial, respectively [186, 187]. Preclinical studies with diabetic pigs transplanted with allogenic islets were reported to have blood glucose regulated in the normal range for several months without exogenous insulin [187, 188].
Similarly, the Diabetes Research Institute of Miami has developed an injectable macroencapsulation system to solve the low oxygen diffusion problem with a device named “BioHub.” This device has been developed to increase the vasculature around graft and thereby improve the functional efficiency of the transplanted islets [189]. After achieving the desirable outcome in preclinical small animal models [190], the group moved into a NHP study with cynomolgus monkeys and has also reported encouraging results. The allogenic islets injected using BioHub system into the omentum of diabetic monkeys with immunosuppressive drugs have progressively reduced the dependency on exogenous insulin with well-preserved islet morphology and abundant graft vasculature as revealed in post-implant analysis [190].
Another approach to address the oxygen diffusion issue is a slender thread designed alginate encapsulation, where an islet embedded in alginate hydrogel layer is placed around a nano-porous calcium-releasing nylon thread. This device can be scaled up according to the recipient organism but still retrievable through a minimally invasive procedure, and this type of macroencapsulated device is referred to as “TRAFFIC” (Thread-Reinforced Alginate Fiber For Islet enCapsulation). TRAFFIC devices have been tested in small animal and preclinical models such as mice and dogs and have been shown to restore normoglycemia while providing immune protection up to 3 months [191].
In spite of the fact that there have been a good number of designs of macroencapsulated devices that were developed and tested in preclinical models, only a few clinical trials have been carried out using these devices. Following a preclinical NHP study and its encouraging outcome [185], Dufrane et al. proceeded to a clinical study where the “monolayer cellular device” encapsulated with allogenic islets was implanted subcutaneously into a 74-year-old T1DM patient [192]. In this pilot study, blood glucose levels were controlled for almost 1 year (361 days) post-transplantation with minimal hypoglycemic episodes. When the macroencapsulated device was retrieved after the study period, the integrity of the device was revealed without any sign of inflammation or immunization against the implanted islets.
The β-Air device developed by Beta-O2 Technologies has also been tested in a pilot clinical study, where a 63-year-old T1DM patient was transplanted with (2100 IEQ/kg body weight) allogenic islets encapsulated in the β-Air device. The study showed graft function for 10 months of insulin secretion and controlled blood glucose levels without any immune suppression treatments. In the next phase clinical trial, four T1DM patients were transplanted with 1800–4600 IEQ/kg B.W. allogenic islets and monitored for the following 3–6 months. The results validated the findings of the preliminary study demonstrating that β-Air devices are safe and provide protection to the transplanted islets from the host immune attack through immune isolation. However, the β-Air device has failed to provide a long-term insulin independence due to limited function of implanted islets [186].
The BioHub macroencapsulation device has been evaluated in a pilot study, where a 43-year-old female T1DM patient was transplanted with a total of 600,000 allogenic IEQ in her omentum. This study provided encouraging results such as the restoration of glucose homeostasis in the T1DM patient without exogenous insulin dependence for at least 1 year [193, 194]. Although the hydrogels used in macroencapsulation provide physical support in maintaining the 3D structure, keeping the islets apart to prevent aggregation and thus improving their viability and function, often they are fragile and unable to support long-term survival of the implanted islets [195]. In addition, the major limitation of macroencapsulation is the insufficient diffusion of oxygen and nutrients due to the increased diffusion length between the encapsulated islet and the ECF [196]. Further, cellular adherence and fibrous growth around the implanted microencapsulated devices due to their size, shape, physicochemical properties of the materials such as chemical composition, level of hydrophobicity, roughness, and pore size are other challenging issues associated with macroencapsulation [197]. Therefore, it requires a lot of improvements with regard to surface properties and designs of the macroencapsulation devices to achieve a desirable outcome in long-term clinical trials.
Microencapsulated Islets
Following the initial in vivo studies of Lim and Sun [136••] with microencapsulated islets in rats, many studies were carried out to improve the technology to treat T1DM. Some of the main modifications include (a) identifying a divalent cation that generates a reduced pore-sized alginate hydrogel to evade immune attack and (b) the inclusion of polycation coating to provide immune-isolating semipermeable membrane. Hence, alginate hydrogel crosslinked with the divalent cation, Ba++, has shown less permeability of compounds of higher molecular weights including immunoglobulin G (IgG) compared to calcium-crosslinked microcapsules [130]. However, Ba++-crosslinked microcapsules have been found to be susceptible to fibrotic overgrowth around the implanted microcapsules [181]. As alternative to Ba++ crosslinking, alginate microcapsules have been coated with polycationic molecules such as the polyallylamines, PLL, PLO, or polyvinylamine [161, 174] to create a semipermeable membrane around the microcapsules. It has been shown that PLL coating around microcapsules induced immune reactions due to the exposed layer of positively charged material [198]. As mentioned earlier in the “Microencapsulation” section, the immune provoking reactions by polycationic coating has been addressed by adding a final external layer of the polyanionic alginate around the polycation semipermeable membrane to create APA microcapsules (Fig. 4G) [199]. However, in addition to cytotoxicity associated with PLL coating, as previously mentioned [198] the degradation of this polymer appears to lead to the compromise of the immune protection [200], and therefore an alternative choice of PLO for permselective coating of alginate microbeads [161] has gained much attention for further studies including clinical trials [201, 202]. Such improved microcapsules with islets have been reported to restore normoglycemia in NHP studies (diabetic cynomolgus monkeys) with improved islet viability compared to previous studies [103].
Clinical studies with APA microcapsules gained momentum in 1994 with the study by Soon-Shiong et al., where microencapsulated allogenic islets were transplanted into the peritoneum of immunosuppressed T1DM patients. The outcome of this study showed that the islet grafts in microcapsules provided a tight regulation on glucose metabolism without any exogenous insulin for 9 months [109]. Later in another study by the Calafiore group, intraperitoneally implanted microencapsulated human islets without immunosuppression and caused a decreased use of exogenous insulin after a few weeks post-transplantation. Further, there was no evidence of immune reaction or sensitization on the recipients [111].
In 2009, Tuch et al. performed a small clinical trial of Ba++-crosslinked alginate microcapsules with allogenic islets in four diabetic patients transplanted in the peritoneal cavity without immunosuppression agents and reported a decrease in blood glucose, but not enough to be independent of exogenous insulin [110]. Even though this earlier study used human islets for therapeutic purpose, in later studies this group advanced to the use of xenogeneic (porcine) islets in order to address the shortage of human pancreatic islets for transplantation [203]. In this encapsulated xeno-islet approach, Living Cell Technologies (LCT) Limited (Auckland, New Zealand) also conducted a clinical trial (NCT01739829) using microencapsulated porcine islets referred to as “DIABECELL®,” where eight T1DM patients (aged between 21 and 68) were transplanted with varying doses of islets ranging from 5000 to 10,000 islet equivalent per kilogram body weight (IEQ/kg B.W.). Six out of eight patients displayed a long-term improvement in their blood glucose management as reflected by both the reduction of their daily exogenous insulin requirements and their levels of glycosylated hemoglobin (HbA1c%) for up to 8 months. Two of them were totally independent of exogenous insulin use to manage their blood glucose level, and this study demonstrated the potential of microencapsulation-based islet therapy as a safe and effective alternative approach for exogenous insulin therapy in T1DM management [203].
Other Forms of Encapsulated Islets in Clinical Studies
An initial in vivo study with the transplantation of 5000–8000 nanoencapsulated porcine islets was reported to decrease the blood glucose level in diabetic rats [204], and it led to a nonhuman primate (NHP) study with five baboons by Novocell, Inc. that showed improvements with the nanoencapsulation approach. The preclinical NHP study was successful, as 60% of baboons transplanted with allogenic islets became insulin independent up to a period of 20 months. Encouraged by the success of the NHP study, Novocell, Inc. entered into a phase I/II clinical trial in the USA. In this FDA-approved clinical study, 12 patients enrolled for the trial, but only two of them qualified for the study after screening for the inclusion and exclusion criteria. Nanoencapsulated allogenic islets were implanted subcutaneously into the back and abdomen region without the use of any long-term immunosuppressive agents. Even though the recipients experienced a decline in the number of hyperglycemic (> 300 mg/dL) and hypoglycemic (< 70 mg/dL) episodes, none of them was reported to achieve insulin independence during the first 4 to 6 months post-transplantation [174, 203]. Following the unsuccessful outcome, the clinical trials with nanoencapsulated islets were discontinued until recommended improvements or investigations were carried out to make the nanoencapsulation technology available for further clinical trials.
Summary of Current Status of Encapsulated Islet Technologies
Among all the islet/β-cell delivery systems that have been actively investigated for their therapeutic potentials in T1DM, the islet microencapsulation approach meets all the essential prerequisites for clinical translation with high potential to provide desirable outcomes. Various preclinical studies have demonstrated the efficacy of alginate-based islet microencapsulation in diabetic models, and the data from clinical trials also suggest that this approach of delivering islet for the treatment of T1DM is promising. Although the preclinical studies and clinical trials so far have all shown measurable function of encapsulated islets for a short duration, their long-term survival and function remain to be determined. Despite the fact that the technology has been investigated and evaluated for almost 35 years, no clinical therapeutic product has been released in the market yet. While there are several factors that contribute to the roadblock, some of the critical ones are discussed in the following section along with proposed strategies to overcome the problems.
Limitations in Encapsulated Islet Technologies and Current Strategies for Improvement
Even though encapsulated islets have shown functional efficacy based on the studies with some success up to 12 months in preclinical large animal models [199, 205] and in clinical trials [109,110,111, 174, 186, 193, 194, 203], a common and persistent problem of graft failure with BAP in its long-term function has been observed. Several obstacles still need to be overcome before the BAP approach becomes a clinical reality. The limiting factors to the success of this BAP technology in clinic have been identified as alterations in islet function and the immune reactions from the graft host recipient.
Causes of Encapsulated Islet Dysfunction
Insufficient quantity and poor quality of transplanted islets are the prime factors for the limited success in clinical studies. Diminished viability and endocrine function of islets within the encapsulated devices over time are the next set of contributing factors. Since islets by their native architecture are cluster of cells, it is natural that the cells at the center of the islets suffer from hypoxia due to limited diffusion. Islets are known for their high oxygen demand compared to other cell types [206, 207], and hypoxia poses a serious threat to the viability of the islets. In addition, alterations in the encapsulating biomaterials with time contribute to apoptosis or necrosis of islets within the hydrogel capsules by causing debris around the devices leading to limited diffusion. Accumulation or precipitation of calcium salts inside the APA microcapsules has been reported as a contributing to the failure of encapsulated cell functions [160]. In addition, displacement of Ca++ ion by other monovalent cation such as sodium ion (Na+) compromises the tight packing of alginate hydrogel and leads to the swelling of macro- and microcapsules. When the hydrogel material swells, the diffusion length also increases correspondingly, contributing to the necrosis of the encapsulated islets. Another phenomenon observed with some of the biomaterials used for encapsulation is the biodegradation of hydrogels over time post-transplantation. Biodegradation compromises the immune protection property of the encapsulation devices, eventually leading to host immune destruction.
Host Immune Reactions toward Transplanted Graft
Similar to the apoptosis/necrosis of islet and the associated dysfunction, the host reaction against the encapsulated islet grafts is also a major contributing factor to the failure of this approach in treating T1DM. In unencapsulated islets, intrahepatic transplantation induces instant blood–mediated inflammatory reaction (IBMIR) [208]. With encapsulation, the host reaction has been identified against two components of encapsulated islet: (1) the reaction against the biomaterials used for encapsulation and (2) the reactions against the allogenic or xenogeneic cell-derived bio-factors and antigens that leak out of the capsules. The inflammatory response against the materials used for the encapsulation in the form of pericapsular fibrotic overgrowth (PFO) interferes with the supply of gases and nutrients to the encapsulated islets leading to cell necrosis in the transplanted tissue. With advancement in the technology, these shortcomings can be successfully addressed by certain processes such as purification of the materials [94, 209]. Some biomaterials, including alginate, contain impurities associated with their preparation that are recognized as pathogen-associated molecular patterns (PAMPs) by the pattern recognition receptors (PRRs) in the immune system [210, 211]. This results in the release of proinflammatory cytokines causing adverse anti-capsular immune response [212]. Toll-like receptors (TLRs) found on the cell surface or in the endosomal compartment are one such PRR that can recognize the PAMPs in biomaterials such as alginate. Some of the common PAMPs that are recognized by TLRs of immune system include lipopolysaccharides (recognized by TLR4) [213], peptidoglycans and lipoteichoic acid (recognized by TLR2) [210], and small poly-M residues (recognized by both TLR2 and TLR4) [214]. These data highlight the importance of high-quality purification of alginate during preparation, and in recent times many groups have used ultrapure alginates in their studies to mitigate the PAMP-associated immune reactions [210].
Also, the transplanted tissue-secreted bio-factors cause chronic conditions including PFO induced by macrophages and lymphocytes. The encapsulated cells induce immune reaction by a process called antigen shedding and secretion of soluble immune mediators [215]. In addition, the encapsulated cells can also respond to immune mediators of the host immune system as well. Some of the metabolic products of encapsulated cells such as advanced glycation end (AGE) products and uric acid can be recognized as damage-associated molecular patterns (DAMPs) by the host immune system [216, 217]. Other compounds released by any apoptotic cells including nucleic acids and chromosomal fragments can also serve as DAMPs [218]. Finally, the transplanted microcapsules themselves can attract various types of cells from the host including macrophages, NK cells, CD4+ T-cells, B-cells, granulocytes, and myofibroblasts, which adhere to the surface of the capsules forming the PFO. The PFO blocks the diffusion of essential nutrients and gases and suffocate the encapsulated islets leading to the failure of the graft. This highlights the importance of sustained viability of the encapsulated islets and need for permselectivity in the microcapsule design. Our current understanding of these factors has led to improvement in the choice of biomaterials, design, and bio-fabrication process, leading to strategies for a better outcome of encapsulated islet–based therapy for T1DM.
Potential Strategies to Improve Graft Function
Some strategies that can be employed to circumvent graft failure are discussed in this section and include: (1) Improved isolation procedures with minimized ischemia time and shorter isolation procedure/period to minimize shock to the islets may improve the quantity and quality of islets; (2) inclusion of oxygen-supplying designs or oxygen-generating materials in the isolation and encapsulation reagents would minimize the hypoxia-induced shock to the islets during the ex vivo handling; (3) incorporating angiogenic growth factor to accelerate vascularization of the implanted islets; (4) replacement of Ca++ cation with a more stable cation such as Sr++ could diminish the hydrogel swelling due to Ca++ displacement by physiological cations or calcium precipitation within the microcapsules; (5) liquefaction of the core in the APA microcapsule design to facilitate diffusion; (6) functionalizing alginate with RGD sequence or including pancreatic ECM components to augment the optimum function of encapsulated islets; (7) co-encapsulating islets with immune-evading stem cells such as MSCs or immune-modulating molecules such as HMGB1 proteins. We will now discuss a few of these issues based on the available data.
Strategies to Circumvent Hypoxia
Islets begin to experience hypoxia from the moment circulation severed from the pancreas of the donor until the period of completion of the neo-vasculature blood supply to the transplanted islets. Certain measures have been taken to avoid hypoxia during the islet handling period ex vivo, as well as the immediate period after transplantation prior to resumption of circulation at the transplanted site. It may take anywhere from 7 to 14 days for the resumption of blood supply to the transplanted islets, and this is a critical period during which most of the encapsulated islets die [219]. Various strategies have been investigated to meet the oxygen demand of transplanted islets. One such approach is the utilization of particulate oxygen-generating substances (POGS). These are chemicals that can generate oxygen when activated by addition to aqueous medium or by other chemical agents. Some of the POGS that have been investigated for various tissue engineering applications include calcium peroxide (CPO), magnesium peroxide (MPO), and sodium peroxide (SPO) (Fig. 4A–E) [163, 220, 221]. An in vitro study with POGS-incorporated microcapsules have shown an improved viability and function of encapsulated islets demonstrating the potential benefit of POGS in BAP technology [163]. CPO, when combined with hemoglobin, has also been reported to restore the viability and endocrine function of neonate porcine islets in a study by Mouré et al. [221].
Oxygen-perfused approaches employed in β-Air devices aimed to circumvent the prevailing hypoxia inside macrocapsules have shown improved function in clinical studies [186], demonstrating the importance of oxygenation of islets. However, it is known that islets also exposed to reactive oxygen species (ROS) during the grafting process or from excessive oxygen-supplementing systems may suffer dysfunction. Inclusion of antioxidants in reagents during the ex vivo handling islets have been shown to ameliorate the adverse effects of ROS and associated cell toxicity [222]. The antioxidant, bilirubin, with cyto-protective effects against oxygen tension, has been shown at physiological concentrations to prevent apoptotic pathways by downregulating apoptotic genes such as TNF-α, while upregulating anti-apoptotic genes including bcl-2 and HO-1 [223,224,225]. It is also known to downregulate the release of DAMPs from the encapsulated islets that are known to induce host immune reaction [224]. Various other strategies have been suggested and discussed in the literature about how to combat hypoxia in encapsulated islets, including hemoglobin crosslinking, photosynthetic oxygen generators, and hyperbaric oxygen therapy [226, 227]. These methods have been proposed and tested with promising results to provide protection against oxygen tension and have good potential for therapeutic application.
Promoting Vasculature at the Transplant Site
Similar to the oxygen-supplementing strategy to improve encapsulated islet survival and function, investigators have studied the incorporation of angiogenic factors to facilitate vasculature and thereby improve nutrient and oxygen supply to the islet graft (Fig. 4I). In this approach, the growth factors studied include VEGF, FGF 1, and FGF 2 [162, 228,229,230,231,232]. Apart from incorporating angiogenic factors in the hydrogels of encapsulated devices, islets pretreated with growth factors and hormones prior to encapsulation also have been shown to promote longevity. Ludwig et al. [233] have demonstrated an improved function of islets, when they were pretreated with growth hormone–releasing hormone (GHRH) prior to microencapsulation and subcutaneous transplantation. In another study by Vaithilingam et al. [234], the desferrioxamine-pretreated islets showed an increased expression of VEGF. The bioactive hydrogel approach developed by BioHub was designed to promote vascularization around the transplanted islets [196]. Therefore, researchers are actively aiming to improve the survival and function of encapsulated islets through facilitation of vasculature and thus improve the transplant outcomes.
Reengineering Encapsulation Matrix
The survival and function of encapsulated islets are greatly impacted by the diffusion property of the microcapsules. The use of APA design of microcapsules with the semipermeable polycation membrane, not only masks the exposure of islet-released DAMPs but blocks PFO on the surface of microcapsules. However, the addition of an outer layer of alginate could hinder the diffusion of essential nutrients and gases. The inner core of APA microcapsules could be liquified by cation chelating agents such as citrate or ethylenediaminetetraacetic acid (EDTA), leaving the outer alginate shell intact (Fig. 4H). This step is carried out between the polycation (PLL or PLO) coating and the addition of outer alginate layer during the synthesis of APA microcapsules [235]. As discussed earlier, the pore size of hydrogel is a determining factor for the permeability of molecules including nutrients, gases, secreted insulin, and mediators of immune system. Therefore, the choice of crosslinking cation plays a crucial role in adjusting the hydrogel pore size that favors only the diffusion of essential materials for the survival and function of islets while restricting the permeability of immune system components without compromising the integrity of the hydrogel. Earlier studies have shown that the substitution of Ca++ with Ba++ decreased the pore size of the hydrogel restricting the infiltration of immune-related components. However, its potential toxicity [131,132,133] restricts the employment of Ba++ as crosslinking agent among the researchers. Another possible choice of bivalent cation is Sr++, which has been used in encapsulation techniques. Substituting Ca++ with Sr++ solves some of the problems including the swelling of hydrogel due to leaching out of Ca++ from alginate hydrogel, reduces the pore size due to compact crosslinking [135], provides a stiffness closer to the native tissue with reduced concentration of Sr++ compared to Ca++ (Fig. 4U) [128], and prevents the precipitation inside the APA microcapsules in contrast to Ca++ (Fig. 4J and K) [160].
Mimicking the composition of native tissue has been reported to improve the function of bioengineered tissues. In that aspect, in addition to recapitulating the stiffness of the native pancreas for islets encapsulated with Sr++-crosslinked alginate, incorporating decellularized ECM of human pancreas in the encapsulating hydrogel is another approach that has been used to mimic the native microenvironment of islets. (Fig. 4L–T). In a study where the hydrogel mimicking the natural microenvironment of the pancreatic scaffold was used for encapsulating human islets, it was found that it enhanced islet function compared to islets without ECM materials [128]. Investigators have also incorporated components of the pancreatic ECM, rather than using the decellularized pancreatic ECM [236], and have also demonstrated an improved function of encapsulated islets. Similarly, attaching the functional units of ECM such as arginine-glycine-aspartate (RGD) sequence to alginate molecule referred to as “functionalized-alginate” is another approach that has been investigated and shown to improve the functions of encapsulated cells [237,238,239,240].
Immune-Modulation Approaches
While the bio-fabrication process (encapsulation) has improved tremendously, there appears to be still some yet to-be-completely elucidated factors that may cause some adverse immune reactions against encapsulated islets in vivo. Various strategies are being studied to address these emerging immune reactions. Co-encapsulation of HMGB1 A box protein (an inflammation receptor antagonist) with islets provided protection against the host immune reaction and demonstrated a two-fold improved survival and function of encapsulated islets [241]. In a related study, 16 anti-inflammatory small molecules were screened for their protective effects against PFO formation over microcapsules. Among the 16 screened compounds, dexamethasone and curcumin have shown encouraging outcomes in a diabetic mice study [242].
Also, incorporating immunomodulatory compounds or co-encapsulating immune-modulating stem cells such as MSCs along with islets and therapeutic cells has been investigated for improved functions and immune-protecting effects [159]. In a study by Vaithilingam, MSCs were treated with cytokines such as IFN-γ and TNF-α and co-encapsulated with islets and reported to result in an improved islet function and less inflammatory cytokines compared the islet only encapsulated group [243]. In another study, MSCs have not only been shown to provide immune protection but also augmented the induction of blood vessel formation due to the angiogenic effect of MSCs [244]. MSC co-encapsulated with islet also have demonstrated a reduction in Th1 cytokines in addition to improved blood glucose regulation [245]. Consistent with these data, the incorporation of autologous stem cells along with islets transplanted in T1DM patients have resulted in a long-term sustained insulin independence, which had not been achieved in previous clinical studies [246]. Results from such studies have provided encouragements in the direction of using stem cells in encapsulated islet–based therapies for T1DM.
Conclusion and Future Perspectives
Although the microencapsulation technology has been investigated all around the world by various academic institutions and biotechnology companies, the technology remains to be perfected [110, 111, 247, 248], probably due to lack of coordination and consensus among the investigators. Among several variabilities, the differences in the raw materials used for bio-fabrication would be a prime factor. The next issue is the use of various preclinical models to assess the biocompatibility and safety that are often not translatable to the clinic. Finally, there is the problem of significant inconsistency in the results of studies from various groups even using the same approach and study models. Collaboration is vital in order to succeed in the clinical cell therapy of T1DM using islet delivery. A good step in this direction is the Collaborative Islet Transplant Registry (CITR), which was created in 2004 with the mission to not only expedite the progress of the technology but also to promote safety in islet transplantation through collection, analysis, and communication of the data among various centers [249]. Despite some success in clinical trials, the slow progress in the field of islet encapsulation and the inconsistency in the results of clinical studies threaten to dampen enthusiasm.
Till date, no other cell-based therapeutic approach has been more thoroughly investigated than islet encapsulation, which presents both unique opportunities and challenges as well. Even though the recent development of immune evading “universal stem cells” appears to have lot of potentials in this field as discussed in the “(Stem) Cell–Based Therapies” section, it requires further studies before possible application in managing T1DM. On the other hand, studies have advanced in the potential utilization of xenogeneic sources of islets for T1DM. Some of the variations in the outcome of this approach are due to differences in the processes used by different groups including the encapsulation devices used, the islet source, and dose of islets transplanted. To achieve a clinically successful bioartificial pancreas would require advancement and collaboration in several areas including biomaterials, cell source, genetic engineering, growth factor delivery, and scaffold mimicking the native ECM. Even though the current status of the microencapsulated islet technology is that it has not yet provided permanent independence from exogenous insulin, it is advancing in the right direction with a strong hope for a successful outcome in the near future, which will pave way for its application in the clinical management of diabetes.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Bullard KM, et al. Prevalence of diagnosed diabetes in adults by diabetes type - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(12):359–61.
International Diabetes Federation, IDF Diabetes Atlas. 2019: Brussels, Belgium.
CDC report, National Diabetes Statistics Report. 2020: Atlanta, GA, USA.
Diagnosis and classification of diabetes mellitus. Diabetes Care, 2009. 32 Suppl 1(Suppl 1): p. S62-7.
Mobasseri M, et al. Prevalence and incidence of type 1 diabetes in the world: a systematic review and meta-analysis. Health Promot Perspect. 2020;10(2):98–115.
Maahs DM, et al. Epidemiology of type 1 diabetes. Endocrinol Metab Clin North Am. 2010;39(3):481–97.
JDRF, Type 1 Diabetes Facts 2020.
Liese AD, et al. The burden of diabetes mellitus among US youth: prevalence estimates from the SEARCH for Diabetes in Youth Study. Pediatrics. 2006;118(4):1510–8.
Dabelea D, et al. Incidence of diabetes in youth in the United States. Jama. 2007;297(24):2716–24.
Banting FG, Best CH. Pancreatic extracts. 1922. J Lab Clin Med. 1990;115(2):254–72 This is the original paper that describes the discovery of insulin by Banting and Best in Canada.
Pathak V, et al. Therapies for type 1 diabetes: current scenario and future perspectives. Clin Med Insights Endocrinol Diabetes. 2019;12:1179551419844521.
REPOSE Study Group. Relative effectiveness of insulin pump treatment over multiple daily injections and structured education during flexible intensive insulin treatment for type 1 diabetes: cluster randomised trial (REPOSE). BMJ 2017. 356: p. j1285. https://doi.org/10.1136/bmj.j1285.
Abramson A, et al. An ingestible self-orienting system for oral delivery of macromolecules. Science. 2019;363(6427):611–5.
Boughton CK, Hovorka R. Is an artificial pancreas (closed-loop system) for type 1 diabetes effective? Diabet Med. 2019;36(3):279–86.
Kambe N, et al. Impact of newly developed, next-generation artificial endocrine pancreas. J Med Invest. 2015;62(1-2):41–4.
Slover RH, et al. Accuracy of a fourth-generation continuous glucose monitoring system in children and adolescents with type 1 diabetes. Diabetes Technol Ther. 2018;20(9):576–84.
Jacobs PG, et al. Randomized trial of a dual-hormone artificial pancreas with dosing adjustment during exercise compared with no adjustment and sensor-augmented pump therapy. Diabetes Obes Metab. 2016;18(11):1110–9.
Haidar A, et al. Outpatient overnight glucose control with dual-hormone artificial pancreas, single-hormone artificial pancreas, or conventional insulin pump therapy in children and adolescents with type 1 diabetes: an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2015;3(8):595–604.
Weisman A, et al. Effect of artificial pancreas systems on glycaemic control in patients with type 1 diabetes: a systematic review and meta-analysis of outpatient randomised controlled trials. Lancet Diabetes Endocrinol. 2017;5(7):501–12.
Bergenstal RM, et al. Safety of a hybrid closed-loop insulin delivery system in patients with type 1 diabetes. JAMA. 2016;316(13):1407–8.
Bekiari E, et al. Artificial pancreas treatment for outpatients with type 1 diabetes: systematic review and meta-analysis. Bmj. 2018;361:k1310.
Anonymous. Cyclosporin-induced remission of IDDM after early intervention. Association of 1 yr of cyclosporin treatment with enhanced insulin secretion. The Canadian-European Randomized Control Trial Group. Diabetes, 1988. 37(11): p. 1574-82.
Russell G, et al. Mechanisms of action of cyclosporine and effects on connective tissues. Semin Arthritis Rheum. 1992;21(6 Suppl 3):16–22.
Martin S, et al. Natural course of remission in IDDM during 1st yr after diagnosis. Diabetes Care. 1992;15(1):66–74.
Ludvigsson J. Therapies to preserve β-cell function in type 1 diabetes. Drugs. 2016;76(2):169–85.
Gitelman SE, et al. Antithymocyte globulin therapy for patients with recent-onset type 1 diabetes: 2 year results of a randomised trial. Diabetologia. 2016;59(6):1153–61.
Moran A, et al. Interleukin-1 antagonism in type 1 diabetes of recent onset: two multicentre, randomised, double-blind, placebo-controlled trials. Lancet. 2013;381(9881):1905–15.
Visperas A, Vignali DA. Are regulatory T cells defective in type 1 diabetes and can we fix them? J Immunol. 2016;197(10):3762–70.
Takemoto N, et al. Coaggregates of regulatory T cells and islet cells allow long-term graft survival in liver without immunosuppression. Transplantation. 2015;99(5):942–7.
Bluestone JA, et al. Type 1 diabetes immunotherapy using polyclonal regulatory T cells. Sci Transl Med. 2015;7(315):315–189.
Singha S, et al. Peptide-MHC-based nanomedicines for autoimmunity function as T-cell receptor microclustering devices. Nat Nanotechnol. 2017;12(7):701–10.
Clemente-Casares X, et al. Expanding antigen-specific regulatory networks to treat autoimmunity. Nature. 2016;530(7591):434–40.
Millar PJ, et al. Beneficial metabolic actions of a stable GIP agonist following pre-treatment with a SGLT2 inhibitor in high fat fed diabetic mice. Mol Cell Endocrinol. 2016;420:37–45.
van Baar MJB, et al. SGLT2 inhibitors in combination therapy: from mechanisms to clinical considerations in type 2 diabetes management. Diabetes Care. 2018;41(8):1543–56.
Tahara A, et al. Effects of sodium-glucose cotransporter 2 selective inhibitor ipragliflozin on hyperglycaemia, oxidative stress, inflammation and liver injury in streptozotocin-induced type 1 diabetic rats. J Pharm Pharmacol. 2014;66(7):975–87.
Cheng ST, et al. The effects of empagliflozin, an SGLT2 inhibitor, on pancreatic β-cell mass and glucose homeostasis in type 1 diabetes. PLoS One. 2016;11(1):e0147391.
McCrimmon RJ, Henry RR. SGLT inhibitor adjunct therapy in type 1 diabetes. Diabetologia. 2018;61(10):2126–33.
Pathak VI, N, Flatt PR, The enteroinsular axis – contribution to obesity-diabetes and its treatments, in nutrition and diabetes: pathophysiology and management, E.C.D.-J. Opara, S., Editor. CRC Press: Boca Raton, FL. 2019, p. 41-56.
Frandsen CS, et al. Twelve-week treatment with liraglutide as add-on to insulin in normal-weight patients with poorly controlled type 1 diabetes: a randomized, placebo-controlled, double-blind parallel study. Diabetes Care. 2015;38(12):2250–7.
Traina AN, et al. Once-weekly exenatide as adjunct treatment of type 1 diabetes mellitus in patients receiving continuous subcutaneous insulin infusion therapy. Can J Diabetes. 2014;38(4):269–72.
Pocai A. Action and therapeutic potential of oxyntomodulin. Mol Metab. 2014;3(3):241–51.
Pathak NM, et al. Stable oxyntomodulin analogues exert positive effects on hippocampal neurogenesis and gene expression as well as improving glucose homeostasis in high fat fed mice. Mol Cell Endocrinol. 2015;412:95–103.
Irwin N, et al. Sustained treatment with a stable long-acting oxyntomodulin analogue improves metabolic control and islet morphology in an experimental model of type 1 diabetes. Diabetes Obes Metab. 2015;17(9):887–95.
Khan D, et al. Differential expression of glucagon-like peptide-2 (GLP-2) is involved in pancreatic islet cell adaptations to stress and beta-cell survival. Peptides. 2017;95:68–75.
Khan D, et al. Islet distribution of peptide YY and its regulatory role in primary mouse islets and immortalised rodent and human beta-cell function and survival. Mol Cell Endocrinol. 2016;436:102–13.
Chen S, Du K, Zou C. Current progress in stem cell therapy for type 1 diabetes mellitus. Stem Cell Res Ther. 2020;11(1):275.
de Klerk E, Hebrok M. Stem cell-based clinical trials for diabetes mellitus. Front Endocrinol (Lausanne). 2021;12:631463.
Song N, Scholtemeijer M, Shah K. Mesenchymal stem cell immunomodulation: mechanisms and therapeutic potential. Trends Pharmacol Sci. 2020;41(9):653–64.
Taylor CJ, et al. Generating an iPSC bank for HLA-matched tissue transplantation based on known donor and recipient HLA types. Cell Stem Cell. 2012;11(2):147–52.
Kondo Y, et al. iPSC technology-based regenerative therapy for diabetes. Journal of Diabetes Investigation. 2018;9(2):234–43.
El Khatib MM, et al. β-Cell-targeted blockage of PD1 and CTLA4 pathways prevents development of autoimmune diabetes and acute allogeneic islets rejection. Gene Ther. 2015;22(5):430–8.
Figueiredo C, Blasczyk R. A future with less HLA: potential clinical applications of HLA-universal cells. Tissue Antigens. 2015;85(6):443–9.
Koga K, Wang B, Kaneko S. Current status and future perspectives of HLA-edited induced pluripotent stem cells. Inflammation and Regeneration. 2020;40(1):23.
Lee J, et al. Abrogation of HLA surface expression using CRISPR/Cas9 genome editing: a step toward universal T cell therapy. Sci Rep. 2020;10(1):17753.
Gornalusse GG, et al. HLA-E-expressing pluripotent stem cells escape allogeneic responses and lysis by NK cells. Nat Biotechnol. 2017;35(8):765–72.
Swanson KJ, et al. Incidence and outcomes of significant weight changes after pancreas transplant alone. Transplant Direct. 2020;6(3):e539.
Robertson P, et al. Pancreas transplantation in type 1 diabetes. Diabetes Care. 2004;27(Suppl 1):S105.
Hampson FA, et al. Pancreatic transplantation: surgical technique, normal radiological appearances and complications. Insights Imaging. 2010;1(5-6):339–47.
Kelly WD, et al. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery. 1967;61(6):827–37.
Troppmann C. Complications after pancreas transplantation. Curr Opin Organ Transplant. 2010;15(1):112–8.
Gruessner AC, Sutherland DE. Pancreas transplant outcomes for United States (US) cases as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Registry (IPTR). Clin Transpl. 2008:45–56.
Gruessner AC. 2011 update on pancreas transplantation: comprehensive trend analysis of 25,000 cases followed up over the course of twenty-four years at the International Pancreas Transplant Registry (IPTR). Rev Diabet Stud. 2011;8(1):6–16.
Dholakia S, et al. Advances in pancreas transplantation. J R Soc Med. 2016;109(4):141–6.
Liong SY, et al. Complications following pancreatic transplantations: imaging features. Abdom Imaging. 2011;36(2):206–14.
Ballinger WF, Lacy PE. Transplantation of intact pancreatic islets in rats. Surgery. 1972;72(2):175–86.
Sutherland DE, et al. Transplantation of dispersed pancreatic islet tissue in humans: autografts and allografts. Diabetes. 1980;29(Suppl 1):31–44.
Ricordi C, et al. Automated method for isolation of human pancreatic islets. Diabetes. 1988;37(4):413–20.
Shapiro AM, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med. 2000;343(4):230–8 This paper may be described as the dawn of new era of clinical islet transplantation as it reported extended periods of insulin independence for the first time in several patients after intraportal allo-islet transplantation.
Johansson H, et al. Tissue factor produced by the endocrine cells of the islets of Langerhans is associated with a negative outcome of clinical islet transplantation. Diabetes. 2005;54(6):1755–62.
Koh A, et al. Insulin-heparin infusions peritransplant substantially improve single-donor clinical islet transplant success. Transplantation. 2010;89(4):465–71.
Bottino R, et al. The Future of Islet Transplantation Is Now. Front Med (Lausanne). 2018;5:202.
McCall M, Shapiro AM. Update on islet transplantation. Cold Spring Harb Perspect Med. 2012;2(7):a007823.
Yeh HC, et al. Comparative effectiveness and safety of methods of insulin delivery and glucose monitoring for diabetes mellitus: a systematic review and meta-analysis. Ann Intern Med. 2012;157(5):336–47.
Jacobson AM, et al. The long-term effects of type 1 diabetes treatment and complications on health-related quality of life: a 23-year follow-up of the Diabetes Control and Complications/Epidemiology of Diabetes Interventions and Complications cohort. Diabetes Care. 2013;36(10):3131–8.
Priya G, Kalra S. A review of insulin resistance in type 1 diabetes: is there a place for adjunctive metformin? Diabetes Ther. 2018;9(1):349–61.
Panero F, et al. Fasting plasma C-peptide and micro- and macrovascular complications in a large clinic-based cohort of type 1 diabetic patients. Diabetes Care. 2009;32(2):301.
Johansson BL, et al. C-peptide improves autonomic nerve function in IDDM patients. Diabetologia. 1996;39(6):687–95.
Johansson BL, et al. Beneficial effects of C-peptide on incipient nephropathy and neuropathy in patients with type 1 diabetes mellitus. Diabet Med. 2000;17(3):181–9.
Johansson BL, et al. Influence of combined C-peptide and insulin administration on renal function and metabolic control in diabetes type 1. J Clin Endocrinol Metab. 1993;77(4):976–81.
Johansson BL, Linde B, Wahren J. Effects of C-peptide on blood flow, capillary diffusion capacity and glucose utilization in the exercising forearm of type 1 (insulin-dependent) diabetic patients. Diabetologia. 1992;35(12):1151–8.
Johansson BL, Sjöberg S, Wahren J. The influence of human C-peptide on renal function and glucose utilization in type 1 (insulin-dependent) diabetic patients. Diabetologia. 1992;35(2):121–8.
Hills CE, Brunskill NJ. C-Peptide and its intracellular signaling. Rev Diabet Stud. 2009;6(3):138–47.
Wahren J, Ekberg K, Jörnvall H. C-peptide is a bioactive peptide. Diabetologia. 2007;50(3):503–9.
Sima AA, et al. Sequential abnormalities in type 1 diabetic encephalopathy and the effects of C-peptide. Rev Diabet Stud. 2009;6(3):211–22.
Luppi P, Cifarelli V, Wahren J. C-peptide and long-term complications of diabetes. Pediatr Diabetes. 2011;12(3 Pt 2):276–92.
Wahren J, Kallas Å, Sima AAF. The clinical potential of C-peptide replacement in type 1 diabetes. Diabetes. 2012;61(4):761–72.
Vantyghem MC, et al. Effects of non-steroid immunosuppressive drugs on insulin secretion in transplantation. Ann Endocrinol (Paris). 2007;68(1):21–7.
Froud T, et al. Resolution of neurotoxicity and beta-cell toxicity in an islet transplant recipient following substitution of tacrolimus with MMF. Cell Transplant. 2006;15(7):613–20.
Zhang N, et al. Sirolimus is associated with reduced islet engraftment and impaired beta-cell function. Diabetes. 2006;55(9):2429–36.
Niclauss N, et al. Rapamycin impairs proliferation of transplanted islet β cells. Transplantation. 2011;91(7):714–22.
Hyder A, Laue C, Schrezenmeir J. Effect of the immunosuppressive regime of Edmonton protocol on the long-term in vitro insulin secretion from islets of two different species and age categories. Toxicol In Vitro. 2005;19(4):541–6.
Mense MG, Rosol TJ, Chapter 35 - endocrine pancreas, in Boorman's pathology of the rat (second edition), A.W. Suttie, Editor. Academic Press: Boston.2018, p. 695-704.
Opara EC, Kendall WF Jr. Immunoisolation techniques for islet cell transplantation. Expert Opin Biol Ther. 2002;2(5):503–11.
de Vos P, Hamel AF, Tatarkiewicz K. Considerations for successful transplantation of encapsulated pancreatic islets. Diabetologia. 2002;45(2):159–73.
de Vos P, van Schilfgaarde R. In: Kühtreiber WM, Lanza RP, Chick WL, editors. Biocompatibility issues, in cell encapsulation technology and therapeutics. Boston, MA: Birkhäuser Boston; 1999. p. 63–75.
Bisceglie V. Über die antineoplastische Immunität. Zeitschrift für Krebsforschung. 1934;40(1):122–40.
Aebischer P, et al. Functional recovery in hemiparkinsonian primates transplanted with polymer-encapsulated PC12 cells. Exp Neurol. 1994;126(2):151–8.
Wong H, Chang TM. Bioartificial liver: implanted artificial cells microencapsulated living hepatocytes increases survival of liver failure rats. Int J Artif Organs. 1986;9(5):335–6.
Cieslinski DA, David Humes H. Tissue engineering of a bioartificial kidney. Biotechnol Bioeng. 1994;43(7):678–81.
Chang TM. Semipermeable microcapsules. Science. 1964;146(3643):524–5.
Koo J, Chang TM. Secretion of erythropoietin from microencapsulated rat kidney cells: preliminary results. Int J Artif Organs. 1993;16(7):557–60.
Prehn RT, Weaver JM, Algire GH. The diffusion-chamber technique applied to a study of the nature of homograft resistance. J Natl Cancer Inst. 1954;15(3):509–17.
Elliott RB, et al. Transplantation of micro- and macroencapsulated piglet islets into mice and monkeys. Transplant Proc. 2005;37(1):466–9.
Dufrane D, et al. Six-month survival of microencapsulated pig islets and alginate biocompatibility in primates: proof of concept. Transplantation. 2006;81(9):1345–53.
Abalovich AG, et al. Pig pancreatic islet transplantation into spontaneously diabetic dogs. Transplant Proc. 2009;41(1):328–30.
Wang T, et al. Successful allotransplantation of encapsulated islets in pancreatectomized canines for diabetic management without the use of immunosuppression. Transplantation. 2008;85(3):331–7.
Meyer T, Höcht B, Ulrichs K. Xenogeneic islet transplantation of microencapsulated porcine islets for therapy of type I diabetes: long-term normoglycemia in STZ-diabetic rats without immunosuppression. Pediatr Surg Int. 2008;24(12):1375–8.
Foster JL, et al. Differentiation of transplanted microencapsulated fetal pancreatic cells. Transplantation. 2007;83(11):1440–8.
Soon-Shiong P, et al. Insulin independence in a type 1 diabetic patient after encapsulated islet transplantation. Lancet. 1994;343(8903):950–1.
Tuch BE, et al. Safety and viability of microencapsulated human islets transplanted into diabetic humans. Diabetes Care. 2009;32(10):1887–9.
Calafiore R, et al. Microencapsulated pancreatic islet allografts into nonimmunosuppressed patients with type 1 diabetes: first two cases. Diabetes Care. 2006;29(1):137–8.
Scharp DW, Mason NS, Sparks RE. Islet immuno-isolation: the use of hybrid artificial organs to prevent islet tissue rejection. World J Surg. 1984;8(2):221–9.
Lanza RP, Hayes JL, Chick WL. Encapsulated cell technology. Nat Biotechnol. 1996;14(9):1107–11.
Colton CK, Avgoustiniatos ES. Bioengineering in development of the hybrid artificial pancreas. J Biomech Eng. 1991;113(2):152–70.
Chick WL, Like AA, Lauris V. Beta cell culture on synthetic capillaries: an artificial endocrine pancreas. Science. 1975;187(4179):847–9.
Maki T, et al. Treatment of diabetes by xenogeneic islets without immunosuppression. Use of a vascularized bioartificial pancreas. Diabetes. 1996;45(3):342–7.
Maki T, et al. Treatment of severe diabetes mellitus for more than one year using a vascularized hybrid artificial pancreas. Transplantation. 1993;55(4):713–7 discussion 717-8.
Lacy PE, et al. Maintenance of normoglycemia in diabetic mice by subcutaneous xenografts of encapsulated islets. Science. 1991;254(5039):1782–4.
Jain K, et al. Glucose control and long-term survival in biobreeding/Worcester rats after intraperitoneal implantation of hydrophilic macrobeads containing porcine islets without immunosuppression. Transplantation. 1999;68(11):1693–700.
Scharp DW, et al. Protection of encapsulated human islets implanted without immunosuppression in patients with type I or type II diabetes and in nondiabetic control subjects. Diabetes. 1994;43(9):1167–70 This is one of the first reports of encapsulation as an effective strategy for islet immunoisolation in clinical transplantation.
Storrs R, et al. Preclinical development of the islet sheet. Ann N Y Acad Sci. 2001;944:252–66.
van Suylichem PT, et al. Insulin secretion by rat islet isografts of a defined endocrine volume after transplantation to three different sites. Diabetologia. 1992;35(10):917–23.
de Vos P, et al. Alginate-based microcapsules for immunoisolation of pancreatic islets. Biomaterials. 2006;27(32):5603–17.
Iwata H, et al. Evaluation of microencapsulated islets in agarose gel as bioartificial pancreas by studies of hormone secretion in culture and by xenotransplantation. Diabetes. 1989;38(Suppl 1):224–5.
Cruise GM, et al. In vitro and in vivo performance of porcine islets encapsulated in interfacially photopolymerized poly(ethylene glycol) diacrylate membranes. Cell Transplant. 1999;8(3):293–306.
Zielinski BA, Aebischer P. Chitosan as a matrix for mammalian cell encapsulation. Biomaterials. 1994;15(13):1049–56.
Haug A, Larsen B, A study on the constitution of alginic acid by partial acid hydrolysis, in Proceedings of the fifth international seaweed symposium, Halifax, August 25–28, 1965, E.G. Young and J.L. McLachlan, Editors. Pergamon. 1966, p. 271-277.
Enck, K., et al., Effect of alginate matrix engineered to mimic the pancreatic microenvironment on encapsulated islet function. Biotechnol Bioeng, 2020.
Zhang J, et al. Influence of divalent cations on the biofouling behaviors of alginate hydrogels. Biomed Mater. 2019;15(1):015003.
Mørch YA, et al. Effect of Ca2+, Ba2+, and Sr2+ on alginate microbeads. Biomacromolecules. 2006;7(5):1471–80.
Tao H, et al. Inconceivable hypokalemia: a case report of acute severe barium chloride poisoning. Case Reports in Medicine. 2016;2016:2743134.
Bhoelan BS, et al. Barium toxicity and the role of the potassium inward rectifier current. Clinical Toxicology. 2014;52(6):584–93.
Struyk AF, Cannon SC. Paradoxical depolarization of BA2+- treated muscle exposed to low extracellular K+: insights into resting potential abnormalities in hypokalemic paralysis. Muscle & Nerve. 2008;37(3):326–37.
Brady SA, et al. Optimisation of a novel glass-alginate hydrogel for the treatment of intracranial aneurysms. Carbohydr Polym. 2017;176:227–35.
Kang S-M, et al., Alginate microencapsulation for three-dimensional In vitro cell culture. ACS Biomaterials Science & Engineering, 2020.
Lim F, Sun AM. Microencapsulated islets as bioartificial endocrine pancreas. Science. 1980;210(4472):908–10 This is the first report that described microencapsulated islets as a bioartificial pancreas and demonstrated its efficacy in streptozotocin-induced diabetic rats.
Rabanel JM, et al. Progress technology in microencapsulation methods for cell therapy. Biotechnol Prog. 2009;25(4):946–63.
Wolters GH, et al. A versatile alginate droplet generator applicable for microencapsulation of pancreatic islets. J Appl Biomater. 1991;3(4):281–6.
Opara EC, McQuilling JP, Farney AC. Microencapsulation of pancreatic islets for use in a bioartificial pancreas. Methods Mol Biol. 2013;1001:261–6.
Omer A, et al. Long-term normoglycemia in rats receiving transplants with encapsulated islets. Transplantation. 2005;79(1):52–8.
Liaudanskaya V, et al. Assessing the impact of electrohydrodynamic jetting on encapsulated cell viability, proliferation, and ability to self-assemble in three-dimensional structures. Tissue Eng Part C Methods. 2015;21(6):631–8.
Ma M, et al. Core-shell hydrogel microcapsules for improved islets encapsulation. Adv Healthc Mater. 2013;2(5):667–72.
Weibel DB, Diluzio WR, Whitesides GM. Microfabrication meets microbiology. Nat Rev Microbiol. 2007;5(3):209–18.
Choi JK, et al. The crucial role of mechanical heterogeneity in regulating follicle development and ovulation with engineered ovarian microtissue. Biomaterials. 2014;35(19):5122–8.
Headen DM, et al. Microfluidic-based generation of size-controlled, biofunctionalized synthetic polymer microgels for cell encapsulation. Adv Mater. 2014;26(19):3003–8.
Weaver JD, et al. Synthetic poly(ethylene glycol)-based microfluidic islet encapsulation reduces graft volume for delivery to highly vascularized and retrievable transplant site. Am J Transplant. 2019;19(5):1315–27.
Enck K, et al. Design of an adhesive film-based microfluidic device for alginate hydrogel-based cell encapsulation. Ann Biomed Eng. 2020;48(3):1103–11.
Tendulkar S, et al. A scalable microfluidic device for the mass production of microencapsulated islets. Transplant Proc. 2011;43(9):3184–7.
Tendulkar S, et al. A three-dimensional microfluidic approach to scaling up microencapsulation of cells. Biomed Microdevices. 2012;14(3):461–9.
Boontheekul T, Kong HJ, Mooney DJ. Controlling alginate gel degradation utilizing partial oxidation and bimodal molecular weight distribution. Biomaterials. 2005;26(15):2455–65.
Ashimova, A., et al., Cell encapsulation within alginate microcapsules: immunological challenges and outlook. Frontiers in Bioengineering and Biotechnology, 2019. 7(380).
Lanza RP, et al. Xenotransplantation of porcine and bovine islets without immunosuppression using uncoated alginate microspheres. Transplantation. 1995;59(10):1377–84.
Cui H, et al. Long-term metabolic control of autoimmune diabetes in spontaneously diabetic nonobese diabetic mice by nonvascularized microencapsulated adult porcine islets. Transplantation. 2009;88(2):160–9.
Paredes-Juarez GA, et al. DAMP production by human islets under low oxygen and nutrients in the presence or absence of an immunoisolating-capsule and necrostatin-1. Sci Rep. 2015;5:14623.
Vaithilingam V, et al. Characterisation of the xenogeneic immune response to microencapsulated fetal pig islet-like cell clusters transplanted into immunocompetent C57BL/6 mice. PLoS One. 2013;8(3):e59120.
Vaithilingam V, et al. Effect of prolonged gelling time on the intrinsic properties of barium alginate microcapsules and its biocompatibility. J Microencapsul. 2011;28(6):499–507.
Kendall WF Jr, Opara EC. Polymeric materials for perm-selective coating of alginate microbeads. Methods Mol Biol. 2017;1479:95–109.
de Vos P, Hoogmoed CG, Busscher HJ. Chemistry and biocompatibility of alginate-PLL capsules for immunoprotection of mammalian cells. J Biomed Mater Res. 2002;60(2):252–9.
Sittadjody S, et al. Encapsulation of mesenchymal stem cells in 3D ovarian cell constructs promotes stable and long-term hormone secretion with improved physiological outcomes in a syngeneic Rat model. Ann Biomed Eng. 2020;48(3):1058–70.
Sittadjody S, et al. In vivo transplantation of 3D encapsulated ovarian constructs in rats corrects abnormalities of ovarian failure. Nat Commun. 2017;8(1):1858.
Darrabie MD, Kendall WF Jr, Opara EC. Characteristics of poly-L-ornithine-coated alginate microcapsules. Biomaterials. 2005;26(34):6846–52.
Pareta R, et al. Long-term function of islets encapsulated in a redesigned alginate microcapsule construct in omentum pouches of immune-competent diabetic rats. Pancreas. 2014;43(4):605–13.
McQuilling JP, et al. Applications of particulate oxygen-generating substances (POGS) in the bioartificial pancreas. Biomater Sci. 2017;5(12):2437–47.
Krol S, et al. Multilayer nanoencapsulation. New approach for immune protection of human pancreatic islets. Nano Lett. 2006;6(9):1933–9.
Kozlovskaya V, et al. Ultrathin polymeric coatings based on hydrogen-bonded polyphenol for protection of pancreatic islet cells. Adv Funct Mater. 2012;22(16):3389–98.
Zhi ZL, Khan F, Pickup JC. Multilayer nanoencapsulation: a nanomedicine technology for diabetes research and management. Diabetes Res Clin Pract. 2013;100(2):162–9.
Wilson JT, et al. Noncovalent cell surface engineering with cationic graft copolymers. J Am Chem Soc. 2009;131(51):18228–9.
Wilson JT, Cui W, Chaikof EL. Layer-by-layer assembly of a conformal nanothin PEG coating for intraportal islet transplantation. Nano Lett. 2008;8(7):1940–8.
Luan NM, Teramura Y, Iwata H. Layer-by-layer co-immobilization of soluble complement receptor 1 and heparin on islets. Biomaterials. 2011;32(27):6487–92.
Tatsumi K, et al. The non-invasive cell surface modification of hepatocytes with PEG-lipid derivatives. Biomaterials. 2012;33(3):821–8.
Teramura Y, Kaneda Y, Iwata H. Islet-encapsulation in ultra-thin layer-by-layer membranes of poly(vinyl alcohol) anchored to poly(ethylene glycol)-lipids in the cell membrane. Biomaterials. 2007;28(32):4818–25.
Shih H, Mirmira RG, Lin CC. Visible light-initiated interfacial thiol-norbornene photopolymerization for forming islet surface conformal coating. J Mater Chem B. 2015;3(2):170–5.
Lee DY, et al. Optimization of monomethoxy-polyethylene glycol grafting on the pancreatic islet capsules. J Biomed Mater Res. 2002;62(3):372–7.
Scharp DW, Marchetti P. Encapsulated islets for diabetes therapy: history, current progress, and critical issues requiring solution. Adv Drug Deliv Rev. 2014;67-68:35–73.
Teramura Y, Iwata H. Bioartificial pancreas microencapsulation and conformal coating of islet of Langerhans. Adv Drug Deliv Rev. 2010;62(7-8):827–40.
Zhi ZL, et al. Polysaccharide multilayer nanoencapsulation of insulin-producing beta-cells grown as pseudoislets for potential cellular delivery of insulin. Biomacromolecules. 2010;11(3):610–6.
Teramura Y, Iwata H. Improvement of graft survival by surface modification with poly(ethylene glycol)-lipid and urokinase in intraportal islet transplantation. Transplantation. 2011;91(3):271–8.
Kizilel S, et al. Encapsulation of pancreatic islets within nano-thin functional polyethylene glycol coatings for enhanced insulin secretion. Tissue Eng Part A. 2010;16(7):2217–28.
Miura S, Teramura Y, Iwata H. Encapsulation of islets with ultra-thin polyion complex membrane through poly(ethylene glycol)-phospholipids anchored to cell membrane. Biomaterials. 2006;27(34):5828–35.
Veerabadran NG, et al. Nanoencapsulation of stem cells within polyelectrolyte multilayer shells. Macromol Biosci. 2007;7(7):877–82.
Vaithilingam V, Bal S, Tuch BE. Encapsulated islet transplantation: where do we stand? Rev Diabet Stud. 2017;14(1):51–78.
O'Sullivan ES, et al. Islets transplanted in immunoisolation devices: a review of the progress and the challenges that remain. Endocr Rev. 2011;32(6):827–44.
Phelps EA, et al. Maleimide cross-linked bioactive PEG hydrogel exhibits improved reaction kinetics and cross-linking for cell encapsulation and in situ delivery. Adv Mater. 2012;24(1):64–70 2.
Hwang PT, et al. Progress and challenges of the bioartificial pancreas. Nano Converg. 2016;3(1):28.
Dufrane D, Goebbels RM, Gianello P. Alginate macroencapsulation of pig islets allows correction of streptozotocin-induced diabetes in primates up to 6 months without immunosuppression. Transplantation. 2010;90(10):1054–62.
Ludwig B, et al. Transplantation of human islets without immunosuppression. Proc Natl Acad Sci U S A. 2013;110(47):19054–8.
Ludwig B, et al. Improvement of islet function in a bioartificial pancreas by enhanced oxygen supply and growth hormone releasing hormone agonist. Proc Natl Acad Sci U S A. 2012;109(13):5022–7.
Neufeld T, et al. The efficacy of an immunoisolating membrane system for islet xenotransplantation in minipigs. PLoS One. 2013;8(8):e70150.
Farina M, et al. Cell encapsulation: overcoming barriers in cell transplantation in diabetes and beyond. Adv Drug Deliv Rev. 2019;139:92–115.
Berman DM, et al. Bioengineering the endocrine pancreas: intraomental islet transplantation within a biologic resorbable scaffold. Diabetes. 2016;65(5):1350–61.
An D, et al. Designing a retrievable and scalable cell encapsulation device for potential treatment of type 1 diabetes. Proc Natl Acad Sci U S A. 2018;115(2):E263–e272.
Dufrane DM, M, Goffin E, Aouassar N, Gianello P, Vandeleene B. A simple and safe clinical procedure for human encapsulated islet transplantation in the subcutaneous tissue for diabetes treatment. Transplantation. 2013;96:S43.
Espona-Noguera A, et al. Review of advanced hydrogel-based cell encapsulation systems for insulin delivery in type 1 diabetes mellitus. Pharmaceutics. 2019;11(11):597.
Kepsutlu B, et al. Design of bioartificial pancreas with functional micro/nano-based encapsulation of islets. Curr Pharm Biotechnol. 2014;15(7):590–608.
Skrzypek K, et al. Pancreatic islet macroencapsulation using microwell porous membranes. Scientific Reports. 2017;7(1):9186.
Dufrane D, Gianello P. Macro- or microencapsulation of pig islets to cure type 1 diabetes. World J Gastroenterol. 2012;18(47):6885–93.
Thevenot P, Hu W, Tang L. Surface chemistry influences implant biocompatibility. Curr Top Med Chem. 2008;8(4):270–80.
Strand BL, et al. Poly-L-lysine induces fibrosis on alginate microcapsules via the induction of cytokines. Cell Transplant. 2001;10(3):263–75.
Sun Y, et al. Normalization of diabetes in spontaneously diabetic cynomolgus monkeys by xenografts of microencapsulated porcine islets without immunosuppression. J Clin Invest. 1996;98(6):1417–22.
Duvivier-Kali VF, et al. Complete protection of islets against allorejection and autoimmunity by a simple barium-alginate membrane. Diabetes. 2001;50(8):1698–705.
Shimoda M, Matsumoto S. Update regarding xenotransplantation in Japan. Xenotransplantation. 2019;26(1):e12491.
Basta G, Montanucci P, Calafiore R, Microencapsulation of cells and molecular therapy of type 1 diabetes mellitus: the actual state and future perspectives between promise and progress. J Diabetes Investig, 2020.
Qi M. Transplantation of encapsulated pancreatic islets as a treatment for patients with type 1 diabetes mellitus. Adv Med. 2014;2014:429710.
Hill RS, et al. Immunoisolation of adult porcine islets for the treatment of diabetes mellitus. The use of photopolymerizable polyethylene glycol in the conformal coating of mass-isolated porcine islets. Ann N Y Acad Sci. 1997;831:332–43.
Soon-Shiong P, et al. Successful reversal of spontaneous diabetes in dogs by intraperitoneal microencapsulated islets. Transplantation. 1992;54(5):769–74.
Dionne KE, Colton CK, Yarmush ML. Effect of hypoxia on insulin secretion by isolated rat and canine islets of Langerhans. Diabetes. 1993;42(1):12–21.
Sato Y, et al. Cellular hypoxia of pancreatic beta-cells due to high levels of oxygen consumption for insulin secretion in vitro. J Biol Chem. 2011;286(14):12524–32.
Hilbrands R, et al. Differences in baseline lymphocyte counts and autoreactivity are associated with differences in outcome of islet cell transplantation in type 1 diabetic patients. Diabetes. 2009;58(10):2267–76.
De Vos P, et al. Improved biocompatibility but limited graft survival after purification of alginate for microencapsulation of pancreatic islets. Diabetologia. 1997;40(3):262–70.
Paredes-Juarez GA, et al. A technology platform to test the efficacy of purification of alginate. Materials (Basel). 2014;7(3):2087–103.
Krishnan R, et al. Immunological challenges facing translation of alginate encapsulated porcine islet xenotransplantation to human clinical trials. Methods Mol Biol. 2017;1479:305–33.
Dorrington MG, Fraser IDC. NF-κB signaling in macrophages: dynamics, crosstalk, and signal integration. Front Immunol. 2019;10:705.
Vaure C, Liu Y. A comparative review of toll-like receptor 4 expression and functionality in different animal species. Front Immunol. 2014;5:316.
Flo TH, et al. Involvement of toll-like receptor (TLR) 2 and TLR4 in cell activation by mannuronic acid polymers. J Biol Chem. 2002;277(38):35489–95.
Hu S, de Vos P. Polymeric approaches to reduce tissue responses against devices applied for islet-cell encapsulation. Front Bioeng Biotechnol. 2019;7:134.
Matzinger P. The danger model: a renewed sense of self. Science. 2002;296(5566):301–5.
Matzinger P. Friendly and dangerous signals: is the tissue in control? Nat Immunol. 2007;8(1):11–3.
Kono H, Rock KL. How dying cells alert the immune system to danger. Nat Rev Immunol. 2008;8(4):279–89.
Fullagar B, et al. Nano-encapsulation of bilirubin in pluronic F127-chitosan improves uptake in β cells and increases islet viability and function after hypoxic stress. Cell Transplant. 2017;26(10):1703–15.
Suvarnapathaki S, et al. Breathing life into engineered tissues using oxygen-releasing biomaterials. NPG Asia Materials. 2019;11(1):65.
Mouré A, et al. Extracellular hemoglobin combined with an O(2) -generating material overcomes O(2) limitation in the bioartificial pancreas. Biotechnol Bioeng. 2019;116(5):1176–89.
Stiegler P, et al. Prevention of oxidative stress in porcine islet isolation. J Artif Organs. 2010;13(1):38–47.
Wang H, et al. Bilirubin can induce tolerance to islet allografts. Endocrinology. 2006;147(2):762–8.
Adin CA, et al. Physiologic doses of bilirubin contribute to tolerance of islet transplants by suppressing the innate immune response. Cell Transplant. 2017;26(1):11–21.
Adin CA, Croker BP, Agarwal A. Protective effects of exogenous bilirubin on ischemia-reperfusion injury in the isolated, perfused rat kidney. Am J Physiol Renal Physiol. 2005;288(4):F778–84.
Krishnan RK, D, Tucker T, Opara E, Foster CE, Imagawa D, et al. Strategies to combat hypoxia in encapsulated islet transplantation. Surgery Curr Res. 2016;6(2):259.
Papas KK, et al. Oxygenation strategies for encapsulated islet and beta cell transplants. Adv Drug Deliv Rev. 2019;139:139–56.
Khanna O, et al. Synthesis of multilayered alginate microcapsules for the sustained release of fibroblast growth factor-1. J Biomed Mater Res A. 2010;95(2):632–40.
Lembert N, et al. Encapsulation of islets in rough surface, hydroxymethylated polysulfone capillaries stimulates VEGF release and promotes vascularization after transplantation. Cell Transplantation. 2005;14(2-3):97–108.
Sigrist S, et al. Induction of angiogenesis in omentum with vascular endothelial growth factor: influence on the viability of encapsulated rat pancreatic islets during transplantation. J Vasc Res. 2003;40(4):359–67.
Trivedi N, et al. Improved vascularization of planar membrane diffusion devices following continuous infusion of vascular endothelial growth factor. Cell Transplant. 2000;9(1):115–24.
Weaver JD, et al. Design of a vascularized synthetic poly(ethylene glycol) macroencapsulation device for islet transplantation. Biomaterials. 2018;172:54–65.
Ludwig B, et al. Agonist of growth hormone-releasing hormone as a potential effector for survival and proliferation of pancreatic islets. Proc Natl Acad Sci U S A. 2010;107(28):12623–8.
Vaithilingam V, et al. Beneficial effects of desferrioxamine on encapsulated human islets--in vitro and in vivo study. Am J Transplant. 2010;10(9):1961–9.
Opara EC, et al. Design of a bioartificial pancreas(+). J Investig Med. 2010;58(7):831–7.
Smink AM, de Vos P. Therapeutic strategies for modulating the extracellular matrix to improve pancreatic islet function and survival after transplantation. Curr Diab Rep. 2018;18(7):39.
Llacua LA, de Haan BJ, de Vos P. Laminin and collagen IV inclusion in immunoisolating microcapsules reduces cytokine-mediated cell death in human pancreatic islets. J Tissue Eng Regen Med. 2018;12(2):460–7.
Yan J, Chen F, Amsden BG. Cell sheets prepared via gel-sol transition of calcium RGD-alginate. Acta Biomater. 2016;30:277–84.
Kang SW, et al. The effect of conjugating RGD into 3D alginate hydrogels on adipogenic differentiation of human adipose-derived stromal cells. Macromol Biosci. 2011;11(5):673–9.
Kreeger PK, et al. The in vitro regulation of ovarian follicle development using alginate-extracellular matrix gels. Biomaterials. 2006;27(5):714–23.
Jo EH, Hwang YH, Lee DY. Encapsulation of pancreatic islet with HMGB1 fragment for attenuating inflammation. Biomater Res. 2015;19:21.
Dang TT, et al. Enhanced function of immuno-isolated islets in diabetes therapy by co-encapsulation with an anti-inflammatory drug. Biomaterials. 2013;34(23):5792–801.
Vaithilingam V, et al. Co-encapsulation and co-transplantation of mesenchymal stem cells reduces pericapsular fibrosis and improves encapsulated islet survival and function when allografted. Scientific Reports. 2017;7(1):10059.
Fransson M, et al. Mesenchymal stromal cells support endothelial cell interactions in an intramuscular islet transplantation model. Regen Med Res. 2015;3:1.
Hamilton DC, et al. A silk-based encapsulation platform for pancreatic islet transplantation improves islet function in vivo. J Tissue Eng Regen Med. 2017;11(3):887–95.
Cantú-Rodríguez OG, et al. Long-term insulin independence in type 1 diabetes mellitus using a simplified autologous stem cell transplant. J Clin Endocrinol Metab. 2016;101(5):2141–8.
Jacobs-Tulleneers-Thevissen D, et al. Sustained function of alginate-encapsulated human islet cell implants in the peritoneal cavity of mice leading to a pilot study in a type 1 diabetic patient. Diabetologia. 2013;56(7):1605–14.
Basta G, et al. Long-term metabolic and immunological follow-up of nonimmunosuppressed patients with type 1 diabetes treated with microencapsulated islet allografts: four cases. Diabetes Care. 2011;34(11):2406–9.
Close N, et al. NIH-supported National Islet Transplantation Registry. Cell Biochem Biophys. 2004;40(3 Suppl):9–18.
Acknowledgements
The authors would like to thank all the students and fellows that have worked with Dr. Opara in the microencapsulation technology over the years as their findings have contributed to the knowledge shared in this review article.
Author information
Authors and Affiliations
Contributions
Sittadjody S performed the literature search and generated a draft of the manuscript. Opara EC conceived the idea, generated the outline for the review, and critically edited the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Artificial Tissues
Rights and permissions
About this article

Cite this article
Sittadjody, S., Opara, E.C. Encapsulation Strategies for Pancreatic Islet Transplantation without Immune Suppression. Curr Stem Cell Rep 7, 49–71 (2021). https://doi.org/10.1007/s40778-021-00190-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40778-021-00190-w